Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Mass Casualty Shootings and Emergency Preparedness: A Multidisciplinary Approach for an Unpredictable Event
Authors Melmer P, Carlin M, Castater CA, Koganti D, Hurst SD, Tracy BM, Grant AA, Williams K ![]() , Smith RN, Dente CJ, Sciarretta JD
, Smith RN, Dente CJ, Sciarretta JD
Received 16 September 2019
Accepted for publication 21 November 2019
Published 10 December 2019 Volume 2019:12 Pages 1013—1021
DOI https://doi.org/10.2147/JMDH.S219021
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Patrick Melmer,1 Margo Carlin,2 Christine A Castater,2 Deepika Koganti,2 Stuart D Hurst,2 Brett M Tracy,2 April A Grant,2 Keneeshia Williams,2 Randi N Smith,2 Christopher J Dente,2 Jason D Sciarretta2
1Grand Strand Medical Center, University of South Carolina, Myrtle Beach, SC 29572, USA; 2Grady Memorial Hospital, Emory University School of Medicine, Atlanta, GA 30303, USA
Correspondence: Jason D Sciarretta Tel +1 404 251-8914
Fax +1 404 523-3931
Email [email protected]
Abstract: Mass casualty events (MCE) are an infrequent occurrence to most daily healthcare systems however these incidents are the causation for new hospital preparedness and the development of coordinated emergency services. The broad support and operational plans outside the hospital include emergency medical services, local law enforcement, government agencies, and city officials. Modern-day hospital disaster preparedness goals include scheduled training for healthcare personnel to ensure effective and accurate triage for a high-volume of injured patients. This MDT collaboration strengthens the emergency response to optimize the delivery of life-saving care during MCEs. This review identifies the clinical importance of the interdisciplinary team interactions and the lessons learned from past MCE experiences, strengthening healthcare system readiness for such critical incidents.
Keywords: mass casualty, multidisciplinary, mass shooting
Introduction
A mass casualty event (MCE) is characterized by multiple fatalities and a sudden temporal surge of injured patients necessitating emergency services.1 Emergency resources are saturated within hours as critically injured patients arrive to the nearby hospitals. Current MCEs are an epidemic culminating from mass shootings, bombings, or other atrocities against human life. In the United States (US), mass shootings are the most common and most closely tracked type of MCE.2 Also referred to as “mass killings”, this type of MCE is rather defined as three or more killings in a single event, while others reference it as greater than four.
Modern-day hospital disaster preparedness goals include scheduled training for healthcare personnel to ensure effective and accurate triage for a high-volume of injured patients. Accurate triage is essential in these circumstances of multiple critically ill patients with limited resources. Those hospital facilities closest to the incident may receive a disproportionate share of injured patients, and although MCEs remain infrequent to daily healthcare systems, emergency departments (ED) and trauma centers worldwide are establishing protocols to prepare for such events. Our objective is to review and discuss emergency response, hospital preparedness, and the multidisciplinary approach necessary to provide immediate emergency care to the injured during a critical incident following a mass shooting.
Mass Casualty Team Collaboration
Local hospital operations require a team leader to effectually coordinate and communicate with various healthcare disciplines and hospital departments. The broad support and operational plans outside the hospital include emergency medical service (EMS), local law enforcement, government agencies, and city officials. Integrated clinical-alert system through community healthcare systems enhance the response of all neighboring hospitals. Following any type of MCE, internal and external communication with community leaders and partners (EMS, healthcare personnel, public health officers, law enforcement and government agencies) is essential. Interfacility communication in conjunction with management systems help coordinate all participating team members to help optimize acute care needs. This multidisciplinary team (MDT) collaboration strengthens the emergency response to optimize the delivery of life-saving care.
All patients presenting via EMS will be rapidly triaged. Commonly, surgical intervention is required for the critically injured. Operating room personnel should not only anticipate an acute surge of patients directly from the ED but also prepare for multiple and simultaneous procedures. Collaboration with the anesthesia team, OR staff, and surgical specialist (ie, trauma team, vascular and orthopedics) is crucial for improved outcomes. An MDT approach to a polytrauma patient can provide a reduction in anesthesia time, maximize OR availability, and shorten overall hospitalization. Coordinated surgical care with surgeons operating in parallel provides operating room efficiency and surgical stabilization of the injured.3
Emergency Response and Triage
Historically, triage methods during wartime conflicts improved patient outcomes and survivability. The field triage process effectively utilizes acuity levels for the injured at a designated area. Optimal field triage by first responders requires pre-incident training. The goal is to identify and prioritize the injured before emergency transport. Traditional mass casualty triage systems involve Sort, Assess, Lifesaving Intervention, Treatment/Transport (SALT) and Simple Triage and Rapid Treatment (START) triage methodologies. Triage systems commonly assign each victim to green (minimal), yellow (delayed), red (immediate), or black (dead) categories. These colored designations can be changed at any time due to clinical status; however, focus should remain on a rapid assessment. Primary triage systems are not built for determining resource allocation.4 First responders should transfer stable patients to an ancillary or non-hospital facility for immediate resource allocation to critical patients. Smaller hospitals experiencing a nearby MCE may not be able to care for all patients, especially outside the urban metropolitan area.
Below is a brief summary of notable mass casualty shootings, and Table 1 demonstrates the world’s deadliest mass casualty shootings in the last 35 years.
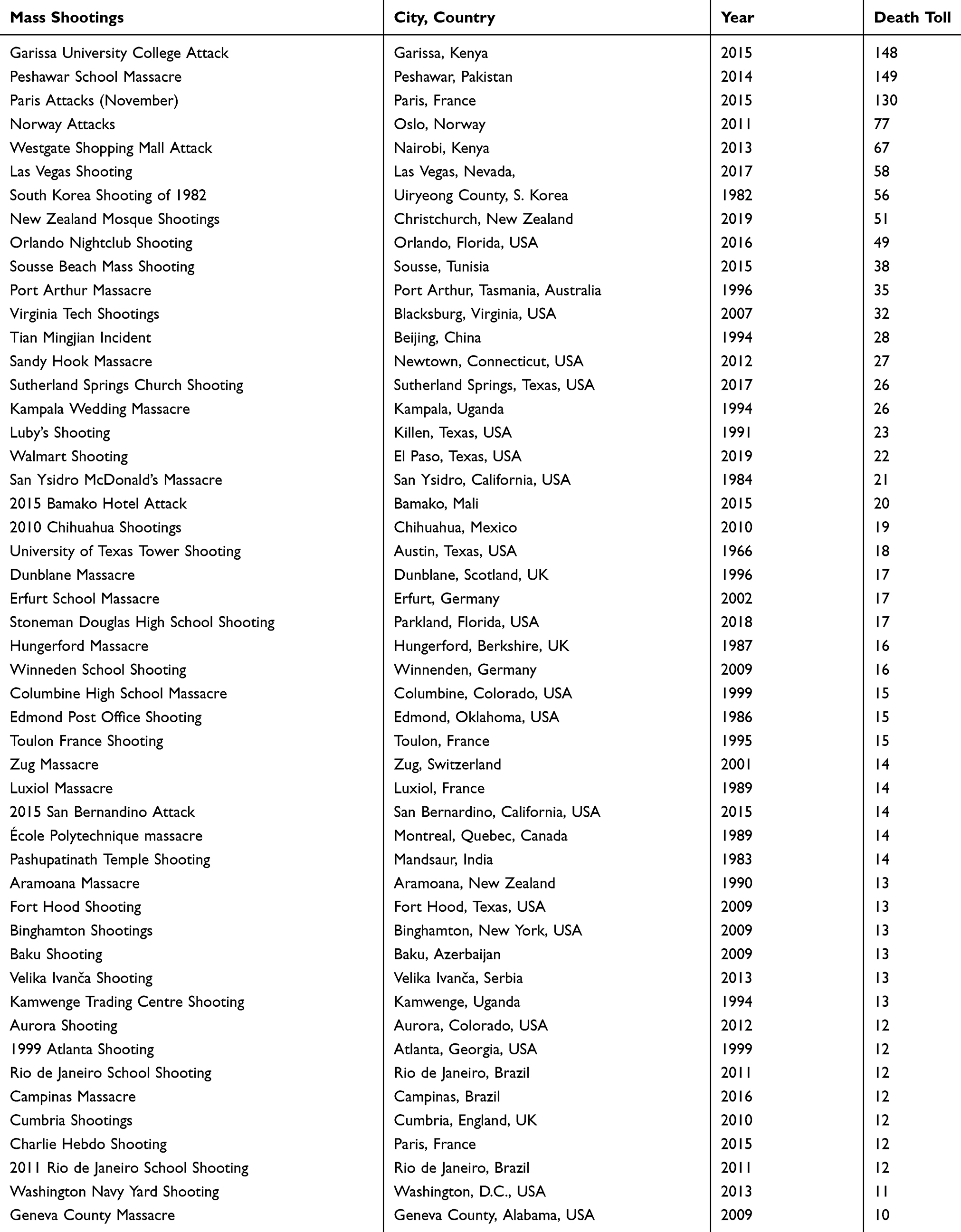 |
Table 1 Deadliest Mass Casualty Shootings |
1. Boston Marathon Bombing: April 15, 2013, Boston, Massachusetts
The Boston Marathon Bombing resulted in 5 deaths and 264 injuries. Two explosions, separated by one block apart, occurred in downtown Boston during the annual Boston Marathon. Each explosion killed at least one individual, while wounding over 200 hundred others and causing pandemonium. A well-publicized manhunt was undertaken for the suspects, Dzhokhar and Tamerlan Tsarnaev. Multiple agencies, including police, rescue workers, medical personnel, and other organizations, were part of a city-wide response to the crisis.5
2. Pulse Nightclub Shooting: June 12, 2016, Orlando, Florida
The Pulse Nightclub Shooting resulted in 49 deaths and 53 injured. A security guard, Omar Mateen, opened fire inside of a busy nightclub. At the time, this event marked the deadliest mass shooting by a single shooter in US history (later surpassed by the Las Vegas Shooting). It remains the deadliest attack against the LGBTQ+ community in the US.6 Due to the nature of the close quarters in the nightclub, and the complexity of the incident with hostage-taking by the shooter, the initial tactical response of the police were questioned and investigated.7,8 The US Department of Justice released a report highlighting that while the local agencies acted well given the circumstances, further training would be needed in order to prepare for such future possible terrorist attacks.8
3. Charleston Church Massacre: June 17, 2015, Charleston, South Carolina
The Charleston Church Massacre resulted in 9 deaths and 3 injured. At one of the most historic churches in the United States, a white supremacist attacked African American churchgoers during a service. Before being surpassed in 2017 and 2018 by the Sutherland Springs Church Shooting and Pittsburgh Synagogue Shooting, respectively, the Charleston Massacre was the deadliest MCE at a place of worship in America.9 Despite swift local response, the majority of victims died on scene. Coordinated action by the police and other authorities resulted in the arrest of the perpetrator in North Carolina. The Federal Bureau of Investigation denounced the Charleston Massacre as a hate crime which sparked an intense nationwide discussion regarding domestic terrorism.10
4. Las Vegas Massacre: October 1, 2017, Las Vegas, Nevada
The Las Vegas Massacre resulted in 58 killed and 422 injured. This event is the deadliest mass shooting in the history of the United States. The massacre occurred during the 2017 Route 91 Harvest Music Festival on the Las Vegas Strip. Stephen Paddock killed 58 and injured over 800 others, both as a direct result of gunfire and the pandemonium that ensued.11 Hundreds of victims were transported to multiple surrounding hospitals, quickly overwhelming and disrupting care across the city.12 This event was notable for the volume of injured patients and potentially worse outcomes had law-enforcement been unable to reach the shooter. As seen following other mass shootings, national debate on gun laws proliferated. Bump stocks, the accessory the shooter used to increase his rate of rifle fire, were heavily criticized and ultimately banned by states and the United States Justice Department.13 Multiple aspects of the multi-healthcare system response continue to be studied, such as the utilization of blood products.14
5. Marjory Stoneman Douglas High School Shooting: February 14, 2018, Parkland, Florida
The Marjory Stoneman Douglas High School shooting resulted in 17 killed and 17 injured. Expelled student, Nikolas Cruz, opened fire in Parkland, Florida. The event surpassed the Columbine High School Massacre as the deadliest high school shooting in the history of the United States. Occurring only a few months after the Las Vegas Shooting, public outcry was particularly fierce. The police department responding to the shooting was heavily criticized for its ineffectiveness and lack of response.15 The young age of the high school victims galvanized efforts at political reform regarding gun control and school safety.16
6. Christchurch Mosque Shootings: March 15, 2019, Christchurch, New Zealand
The Christchurch Mosque Shooting resulted in 51 killed and 49 injured. Though mass shootings have been widely noted to be increasing in frequency in the United States, the 2019 Christchurch shootings in New Zealand marked a rise in MCEs on a global scale.17 A total of 100 victims were killed or injured in two consecutive shootings at mosques in the country’s first mass shooting in over 20 years at the time.18 Emergency response was swift and coordinated, with the local hospital systems activating their mass-casualty plan.19 Following the attacks, gun control issues were raised across New Zealand, which has some laws akin to those in the United States, such as non-tracking of purchased firearms.20 International comparisons were made to New Zealand’s neighbor, Australia, which after the 1996 Port Arthur Shooting in Tasmania, sparked the largest gun violence reducing efforts in the world, complete with severe purchase restrictions.20
7. Sandy Hook Elementary School Shooting: December 4, 2012, Newtown Connecticut
The Sandy Hook Elementary School shooting resulted in 27 killed and 2 injured. The deadliest mass shooting at a grade school in United States history, the Sandy Hook Massacre was notable for the very young age of its victims, the majority between six and seven years of age. Adam Lanza killed his mother and 26 other victims before committing suicide in Newtown, Connecticut. Investigations following the incident focused on mental health and learning disorders after noting a diagnosis of Asperger’s in the shooter.21 Further reporting by the state of Connecticut’s Office of the Child Advocate described the shooter as having a history of antisocial tendencies and a myriad of developmental and behavioral health problems.22
8. El Paso and Dayton Shootings: August 3, 2019
The El Paso shooting resulted in 22 killed and 24 injured. The Dayton, Ohio shootings resulted in 9 killed and 27 injured. These events both occurred after a gunmen opened fire on dozens of civilians in popular shopping areas. Occurring on the 216th day of the year, these events marked more mass shootings in 2019 than days of the year at that point in time.23 Both cities saw coordinated efforts at care for the critically injured at local trauma centers. As details continue to emerge about these events, the recent spur of increasing MCEs continues to fuel intense debate on gun legislation.24
The Aftermath: Social Services and Family Support
A community’s ability to handle any MCE depends on the critical demand and capabilities of the treating healthcare facility. Lessons learned from previous MCEs include the aftermath support necessary to guide and inform the victims, their families and all professional personnel involved during the incident. Following the 2013 Washington, D.C., Navy Yard shooting, the after action report highlighted the necessary notification and communication process for victim families and advocated for the collaboration and structured processes during a critical incident.25 Establishing a family assistance center (FAC) in the aftermath of an MCE is crucial to hospital strategic planning in the aftermath of an MCE. This platform provides social workers, counselors, and volunteer community support groups to those in need of assistance. Similarly, the after action report of the 2013 Boston Marathon bombing recommended that a plan FAC be established prior to any MCE so that jurisdictions can quickly establish necessary services for victims and their families.26 The San Bernardino terrorist shooting incident report advocated for a FAC location where amenities such as food, water, and charging stations were provided for victims while they waited to receive updated information.27
Mass shootings are associated with negative psychological outcomes in survivors and community members. FACs may also offer assistance with mental health, pastoral care, and a variety of short-term and longer-term needs for affected family members. This interdisciplinary team provides the skills and services by both medical (MSW) and occupational (OSW) social workers. MSWs will care for patients and families who have encountered a life-altering trauma, while OSWs use similar skills to act in response to mental health needs of their healthcare colleagues that may arise following the disaster response.28 The mental health consequences, including post-traumatic stress, require a coordinated effort to arrange readily accessible mental health services for those affected. Immediate interventions may include psychological debriefing, community outreach and coping strategies in an effort to diminish any psychological repercussions extended to the community.
Discussion
While many hospital facilities will never experience such an event, this has been an unfortunate reality for some US healthcare systems. In 2017, 11 mass shootings were reported in the United States, more than in any other year in recorded history.2 Of all recorded shootings occurring in 2017, there were 117 fatalities and 587 casualties.2 Almost 50% of all fatalities and more than 90% of the casualties occurred on October 1, 2017, at a music festival in Las Vegas where a gunman opened fire on the crowd.2
Even as recently as producing this manuscript, MCEs continue to dominate the global news market. Within 24 hrs, two separate mass shootings occurred in Dayton, Ohio and El Paso, Texas, with at least 29 dead and 27 more injured on August 3, 2019. Following these two events, 251 recorded mass shootings occurred in the United States in 216 days, a sobering milestone in US history. To date, more than 520 people have died in mass shootings and at least 2000 have been injured (Table 1).23 Recently at the Gilroy Garlic Festival in Northern California, 3 people were killed and 15 wounded. On May 31, 2019, 12 people were killed and 4 others wounded by a city worker at a Virginia Beach government municipal center.29,30
Blood Bank Preparedness
MCEs challenge the utilization of resources at all levels, with blood being no exception. Damage control resuscitation (DCR) has become a key concept that has been adopted from military to civilian practice.31,32 These principles include hemorrhage control (ie, the use of tourniquets,tranexamic acid) within the first 3 hrs and transfusion of 1:1 or 3:2 ratios of red blood cells to fresh frozen plasma.33–35 While crystalloid was initially the product used in resuscitation, blood products are now considered the gold standard in DCR even in pre-hospital settings.36
While patient outcomes have improved with the use of blood, the logistics of obtaining, storing, and supplying blood are much more complicated than intravenous fluids. While crystalloids can be given to any patient, blood must obviously be group O until the patient’s blood type is known. Moreover, crystalloids can be stored for years, while blood products have a limited shelf life. Finally, the administration of blood, unlike crystalloid, is limited by its availability, which is tested during MCEs as many patients require the use of massive transfusion protocol. Based on prior MCEs, the highest demand for blood is during the initial 4 hrs when the most gravely injured patients are brought to the hospital, using two-thirds of the total blood transfused.36–38
There is no standardized protocol for the preparation of blood products in MCE; however, several countries have published their individual experiences and subsequent recommendations. Israel has experienced over 1600 terrorist attacks between 2000 and 2005, finding that 6.7 units of blood and 4.5 units of components were needed per one moderately or severely injured patient. The National Blood Services in Israel is a national, non-profit organization that manages the supply and distribution of blood and has been successfully able to provide products as needed with the development of a national preparedness blood program.39 A study using a computerized simulation model of a UK major trauma center found that even small volume MCEs could overwhelm trauma centers’ blood supplies and restocking would be necessary. The authors also suggest a central supplier for blood as a solution for the massive demand for blood during MCE.37,38
Review of the Las Vegas mass shooting showed that over 500 units of blood were used. Local stock in the treating hospitals along with United Blood Services and American Red Cross contributions allowed for an adequate amount of transfusion products without the need for public donation.14 As MCEs increase in number and lethality, the ability to provide blood products in the pre-hospital and hospital setting is of paramount importance to reduce mortality. Creation of national, or even international, protocols may help create a more organized system for storage, delivery, and utilization of blood during MCE. For now, relying on the blood banks of local hospitals as well as national organizations appears to be universal practice.
Lessons Learned
The intensifying epidemic of violence resulting in mass casualty incidents has promoted the development of effective and coordinated response protocols. Affected centers have published their institution’s debriefing and analysis of quality improvement recommendations. These personal accounts provide not only a platform for the development of institutional mass casualty response protocols but also offers a component of experience to those that have not been faced with such an event. Acknowledging the pros and cons of tactics employed in the face of an MCE also helps other facilities prevent similar mistakes. Lessons learned from previous incidents include, but are not limited to, securing the emergency department, using remote damage control approach to guide resources, evaluation of the complex trauma patient, and management of the aftermath.40–43 It is essential to fundamentally appreciate the magnitude of these high-pressure, high-volume events in order to develop an institutional response protocol.
Establishment of a partial lockdown early in the response is essential to maintaining the efficiency and safety of the response system.41 Complete lockdown prevents entry of medical personnel; however, it is important to consider ambulances as a potential threat. As these vehicles are capable of carrying up to 4000 pounds in explosives, designated ambulance checkpoints a safe distance from the hospital are recommended.41 A facility’s ability to receive or provide information may be inhibited by overloaded or shut down telephone systems in law enforcement’s attempts to prevent remote detonation of an explosive.41,42 Real-time communication may be provided to hospital personnel through social media at predetermined time intervals.41 Prearranged teams of medical personnel should be stationed within the emergency department with back-up teams at a distance, in the event the primary team is compromised. Consideration of primary and secondary blast effects should be based on the building’s architecture when planning evacuation.41 Furthermore, the chain of command should be well established and easily referenced, as one facility identified disruption of patient flow as multiple “leaders” tried to implement simultaneous and potentially contradictory plans.41
Coordination of care of the critically injured patient in immediate need of intervention is supply and personnel intensive. The appropriate triage of high volumes of injured patients is essential for resource allocation after a mass casualty incident. Evaluation of complex injury patterns includes concomitant blast and crush injury, penetrating and blunt visceral injury and neurologic and orthopedic injury. Rapid triage, anticipated clinical course and complications of this injury complex are best determined by mature judgment.41–43 Reviewing and continued reassessment of the patient, management plans, and imaging helps optimize patient care and prevent complications associated with missed injuries.40 Mass transportation of those patients not requiring immediate life-sustaining interventions to nearby facilities clears the responding trauma centers for critically ill patients.43 This maintenance of clinical capacity is essential to the MCE response. A designated individual (ie, trauma medical director) should coordinate all operating room personnel, cancel all elective cases, prepare for simultaneous operations and need for delayed second-look operations.40
It is essential to maintain close supervision and documentation of time limits in provider care. Hospital staff may experience physical and emotional exhaustion in caring for injured patients in a crisis.40 Residents who served at Orlando Regional Medical Center during the Pulse Night Club Shooting experienced burnout, major depression, or post-traumatic stress disorder (PTSD) lasting 6 months after the crisis had ended.40 On November 13, 2015, Paris suffered four suicide bomber attacks within 40 mins resulting in 495 wounded and 130 dead.40 Providers followed 840 firefighters with a psychological check-up within 4 weeks of the incident, 1/3 followed up 3 months later, all underwent repeated PTSD screening.40 Furthermore, facilities should anticipate media attention and plan accordingly. Recommendations include establishing regular conferences, creating an official website, setting up a call center with a hotline and designating a family gathering area.40 This organized response to anticipated media attention and its consequences prevents distractions from the care of patients and ensures a unified hospital message.40
Simulation Exercises
There have been many suggestions about ways to improve the performance of providers and hospitals during an MCE. One thing that can be helpful is simulation exercises and drills. Advantages of these practices include identification of deficiencies, developing and implementing solutions, and increasing confidence in practiced and learned strategies.44,45 After the Sandy Hook shooting, the Hartford Consensus conducted a number of surveys and released reports focused on enhancing survivability from both active shooter and MCEs. One key point was that simulation and training events can help to avoid delays in reaction time. In addition, all simulation exercises should include both practice and conversations about evacuation policies and procedures.46
Recent reviews of the events after the Boston Marathon bombing identified planning and simulation exercises as a key part of the successful triage and treatment of victims.44,47 SimWars is one example of a simulation exercise that focuses on teams participating in an identical and observed mass casualty exercise followed by a group discussion and debrief. Participants are assigned roles and are tasked with triaging patients while observers complete a checklist on each patient. Results show that both participants and observers develop new understanding about how to triage patients in MCE.48 Another technique is to utilize one hour computer-based simulations to assess management and self-efficacy. By the end of multiple sessions, participants exhibit improved abilities to triage and treat trauma and in-hospital patients.49 Another recent simulation involving an active shooter in a hospital showed a 70% improvement in knowledge and preparation for an MCE.50
Overall, simulation exercises provide many advantages to first responders. They improve knowledge of emergency activities and improve competence and confidence in a potential MCE.51 One major advantage to simulation exercises that has been seen across multiple studies is the ability to identify gaps or limitations in plans, protocols or procedures so that solutions can be implemented. Simulation exercises have been shown to produce stress in participants, with the most stress being seen with those responsible for triage. Despite this stress, participants have performed effectively and efficiently despite any reported higher stress level.52 Long-term retention of skills learned during simulation exercises is an area that is both lacking and conflicting in current research. This is most likely only due to difficulties in longitudinal follow-up; however, it remains an area of concern. Overall, there are different options for simulation exercises that exist and there is little doubt that these are helpful in the setting of a real MCE.
Stop the Bleed
The Stop the Bleed Campaign is a national effort by the American College of Surgeons to reduce morbidity and mortality in hemorrhage. The initiative is based on the realization that civilian bystanders are the true first responders. Empowering the public to provide life-sustaining support with simple clinical skills has enormous potential to decrease morbidity and mortality following an MCE. Objectives of the training programs are to motivate learners to act when faced with a hemorrhagic emergency, teach learners how to distinguish life-threatening from non-life-threatening bleeding and to apply pressure.53 A follow-up study questioned the retention and application of clinical skills of those citizens trained in Stop the Bleed. Pasley et al found that 60% were successful at tourniquet placement after training.54 This means that 6 of 10 people in that particular group were theoretically able to respond to and control hemorrhage. It is essential that there is a firm understanding of the psychological impact of these events on all those involved and interval requalification is necessary for preservation of skills. Courses are provided by the American College of Surgeons Committee on Trauma and are offered throughout the country. Locations of training include churches, gun clubs, libraries, and high schools.
Gun Violence and Mortality
Gun violence is a national epidemic. At this point in the history of the United States, both intentional and unintentional gunshot injuries are both socioeconomically and psychologically devastating. In 2010, of deaths resulting from gun violence in high-income countries, 90% of the women, 91% of the children aged 0–14 years, and 92% of the young adults aged 15–24 years occurred in the United States.55 In 2015, the overall firearm death rate was 11.4 times higher in the US than in other high-income countries with the rate increasing between 2003 and 2015.12 Although healthcare providers have been attempting to debrief and optimize therapy following an MCE, there has been an exponential increase in deaths resulting from firearms. Refining our trauma systems and enabling the public as first responders may preserve the critical golden hour after trauma, but it is not a solution to this public health crisis. With the continued attempts to optimize preservation of life following a MCE, our conversations must also focus on prevention. Compromise is not only essential for regulation of access to firearms but also necessary to maintain the balance of protecting our citizens from our constitution, where a right to bear arms does not undermine the right to life.
Conclusion
Although all hospitals should support a mass casualty strategic plan, no hospital can administer all emergency care during a large-scale incident independently. Hospital preparedness and emergency response are increasingly coordinated with the collaboration of different healthcare systems, EMS, emergency management, and public health agencies. This multidisciplinary approach to any mass casualty incidents provides practical and effective triage methods while providing critical emergency care for the injured.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. DuPree C, Pinnola A, Gibson S, Muertos K, Davis JM, Sciarretta JD. Can planned traffic patterns improve survival among the injured during mass casualty motorcycle rallies? J Surg Res. 2019;234:262–268. doi:10.1016/j.jss.2018.09.014
2. 2018 National Crime Victims’ Rights Week (NCVRW) Resource Guide: Mass Casualty Shootings Fact Sheet. Office of Justice Programs; 2018.
3. Oh JS, Humphries AE. Management of Dismounted Complex Blast Injury Patients at a Role V Military Treatment Facility: Special Considerations. Managing Dismounted Complex Blast Injuries in Military & Civilian Settings; 2018:259–267.
4. Clarkson L, Williams M. EMS, Mass Casualty Triage. Treasure Island, FL: StatPearls; 2019.
5. Levs J, Plott M, Terrorism Strikes Boston Marathon as Bombs Kill 3, Wound Scores. CNN; 2013.
6. Meyer D. Violence Against Queer People: Race, Class, Gender, and the Persistence of Anti-LGBT Discrimination. Rutgers University Press; 2015.
7. Hayes C, Harris D, Tziperman Lotan G, Doornbos C. New Pulse review from Orlando police reveals details, lessons learned. Orlando Sentinel. 2017.
8. Gal Tziperman L. Federal Report on Pulse: Authorities performed well but more training needed. Orlando Sentinel. 2017.
9. Beyer L. C.R., 9 dead in shooting at historic Charleston African American church. Police chief calls it ‘hate crime.’. The Washington Post, 2015.
10. Niquette M. South Carolina governor backs removal of confederate flag. Bloomberg; 2015.
11. Romo V. FBI Finds No Motive in Las Vegas Shooting, Closes Investigation. NPR, 2019.
12. Grinshteyn E, Hemenway D. Violent death rates in the US compared to those of the other high-income countries, 2015. Prev Med. 2019;123:20–26. doi:10.1016/j.ypmed.2019.02.026
13. Del Valle L. Massachusetts becomes first state to ban bump stocks since Vegas massacre. CNN, 2017.
14. Lozada MJ, Cai S, Li M, Davidson SL, Nix J, Ramsey G. The Las Vegas Shooting: an analysis of blood component administration and blood bank donations. J Trauma Acute Care Surg. 2019;86(1):128–133. doi:10.1097/TA.0000000000002089
15. Fleshler D. Broward Sheriff’s sergeant called an ‘absolute, total failure’ as Parkland shooting panel slams agency. Sun-Sentinel, 2018.
16. Turkewitz J. Hartocollis A, Highlights: students call for action across nation; Florida lawmakers fail to take up assault rifle bill. The New York Times., 2018.
17. Fattalf I. New Zealand went more than 20 years between mass shootings. NPR, 2019.
18. Saldivia G. Number of dead rises to 50 in New Zealand Mass Shooting. NPR, 2019.
19. Deadly mass shooting at New Zealand mosques. BBC News. 15 March 2019. Archived from the original on 15 March 2019. Retrieved August 19, 2019.
20. Cave D, Stevens M. New Zealand’s Gun Laws Draw Scrutiny After Mosque Shootings. The New York Times, 2019.
21. Park A. Don’t Blame Adam Lanza’s Violence on Asperger’s. Time, 2014.
22. Advocate, T.O.o.t.C., Shooting at Sandy Hook Elementary School: Report of the Office of the Child Advocate. Office of the Child Advocate: State of Connecticut, 2014.
23. Miller S. El Paso, Dayton make 251 mass shootings in the US in 216 days, more shootings than days in the year. USA Today, 2019.
24. King L. After Newtown, pulse, Vegas stirred little change, gun-control advocates hope latest shootings push tougher laws. USA Today, 2019. doi:10.3310/hta23120
25. After Action Report. Washington, DC: Washington Navy Yard; 2014:1–83.
26. Massachusetts Emergency Management Agency. After Action Report for the Response to the 2013 Boston Marathon Bombings. 2014. pp. 1–130. Massachusetts Department of Public Health.
27. Braziel R, Straub F, Hoops R. Bringing Calm to Chaos: a Critical Review of the San Bernadino Public Safety Response to the December 2, 2015 Terrorist Shooting Incident at the Inland Regional Center. U. S. Department of Justice. Office of Community Oriented Policing Services; 2015.
28. Sabbath EL, Shaw J, Stridsen A, Hashimoto D. Protecting mental health of hospital workers after mass casualty events: a social work imperative. Soc Work. 2018;63:272–275. doi:10.1093/sw/swy029
29. Adami C, Cimini K, Cuevas E, Lam K. ‘Incredibly disheartening’: 3 killed, 15 wounded in Gilroy Garlic Festival shooting. USA Today, 2019.
30. Andrews K, Mele C, Eligon J. 12 Killed in Rampage at Municipal Center in Virginia. The New York Times, 2019.
31. Duchesne JC, McSwain NE
32. Holcomb JB, Jenkins D, Rhee P, et al. Damage control resuscitation: directly addressing the early coagulopathy of trauma. J Trauma. 2007;62(2):307–310. doi:10.1097/TA.0b013e3180324124
33. Holcomb JB, Wade CE, Michalek JE, et al. Increased plasma and platelet to red blood cell ratios improves outcome in 466 massively transfused civilian trauma patients. Ann Surg. 2008;248(3):447–458. doi:10.1097/SLA.0b013e318185a9ad
34. Davenport R, Curry N, Manson J, et al. Hemostatic effects of fresh frozen plasma may be maximal at red cell ratios of 1:2. J Trauma. 2011;70(1):
35. Roberts I, Shakur H, Collaborators, C. et al. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. Lancet. 2011;377(9771):
36. Campion EM, Pritts TA, Dorlac WC, et al. Implementation of a military-derived damage-control resuscitation strategy in a civilian trauma center decreases acute hypoxia in massively transfused patients. J Trauma Acute Care Surg. 2013;75(2 Suppl 2):S221–S227. doi:10.1097/TA.0b013e318299d59b
37. Glasgow S, Davenport R, Perkins Z, Tai N, Brohi K. A comprehensive review of blood product use in civilian mass casualty events. J Trauma Acute Care Surg. 2013;75(3):468–474. doi:10.1097/TA.0b013e318298efb9
38. Glasgow S, Vasilakis C, Perkins Z, Brundage S, Tai N, Brohi K. Managing the surge in demand for blood following mass casualty events: early automatic restocking may preserve red cell supply. J Trauma Acute Care Surg. 2016;81(1):50–57. doi:10.1097/TA.0000000000001101
39. Shinar E, Yahalom V, Silverman BG. Meeting blood requirements following terrorist attacks: the Israeli experience. Curr Opin Hematol. 2006;13(6):452–456. doi:10.1097/01.moh.0000245691.32085.66
40. Russo RM, Galante JM, Holcomb JB, et al. Mass casualty events: what to do as the dust settles? Trauma Surg Acute Care Open. 2018;3(1):e000210. doi:10.1136/tsaco-2018-000210
41. Hojman H, Rattan R, Osgood R, Yao M, Bugaev N. Securing the emergency department during terrorism incidents: lessons learned from the Boston Marathon Bombings. Disaster Med Public Health Prep. 2019;1–8. doi:10.1017/dmp.2019.51
42. Lesaffre X, Tourtier JP, Violin Y, et al. Remote damage control during the attacks on Paris: lessons learned by the Paris Fire Brigade and evolutions in the rescue system. J Trauma Acute Care Surg. 2017;82(6S Suppl 1):S107–S113. doi:10.1097/TA.0000000000001438
43. Sheridan RL, Friedstat J, Votta K. Lessons learned from burn disasters in the post-9/11 era. Clin Plast Surg. 2017;44(3):435–440. doi:10.1016/j.cps.2017.02.003
44. Vandenberg SL, Davidson SB. Preparation for mass casualty incidents. Crit Care Nurs Clin North Am. 2015;27(2):157–166. doi:10.1016/j.cnc.2015.02.008
45. Sloan HM. Responding to a multiple-casualty incident: room for improvement. J Emergency Nurs. 2011;37(5):484–486. doi:10.1016/j.jen.2010.07.013
46. Jacobs LM, Burns KJ. The Hartford consensus: survey of the public and healthcare professionals on active shooter events in hospitals. J Am Coll Surg. 2017;225(3):435–442. doi:10.1016/j.jamcollsurg.2017.06.009
47. Biddinger PD, Baggish A, Harrington L, Dhemecourt P, Hooley J, Dyer KS. Be prepared - The Boston Marathon and mass-casualty events. N Engl J Med. 2013;368(21):1958–1960. doi:10.1056/NEJMp1305480
48. Bentley S, Iavicoli L, Agriantonis G, Dilos B. A simulated mass casualty incident triage exercise: SimWars. MedEdPORTAL. 2019;15. doi:10.15766/mep_2374-8265.10823
49. Jonson CO, Pettersson J, Rybing J, Nilsson H, Prytz E. Short simulation exercises to improve emergency department nurses self-efficacy for initial disaster management: controlled before and after study. Nurse Educ Today. 2017;55:20–25. doi:10.1016/j.nedt.2017.04.020
50. Sanchez L, Young VB, Baker M. Active shooter training in the emergency department: a safety initiative. J Emergency Nurs. 2018;44(6):598–604. doi:10.1016/j.jen.2018.07.002
51. Skryabina E, Reedy G, Amlôt R, Jaye P, Riley P. What is the value of health emergency preparedness exercises? A scoping review study. Int J Disaster Risk Reduct. 2017;21:274–283. doi:10.1016/j.ijdrr.2016.12.010
52. Fernández-Pacheco AN, Delgado RC, González PA, et al. Analysis of performance and stress caused by a simulation of a mass casualty incident. Nurse Educ Today. 2018;62:52–57. doi:10.1016/j.nedt.2017.12.016
53. Goolsby C, Jacobs L, Hunt R, et al. Stop the bleed education consortium: education program content and delivery recommendations. J Trauma Acute Care Surg. 2017;84:205–210. doi:10.1097/TA.0000000000001732
54. Pasley AM, Parker BM, Levy MJ, et al. Stop the bleed: does the training work one month out? Am Surg. 2018;84(10):1635–1638.
55. Gerstein N, Sanders J, McCunn M, et al. The gun violence epidemic: time for perioperative physicians to act. J Cardiothorac Vasc Anesth. 2018;32(3):1097–1100. doi:10.1053/j.jvca.2018.03.002
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.