Back to Journals » Clinical Ophthalmology » Volume 14
Masquerades of Acquired Dacryocystocele
Authors Bothra N, Wagh RD ![]() , Ali MJ
, Ali MJ ![]()
Received 3 May 2020
Accepted for publication 23 June 2020
Published 2 July 2020 Volume 2020:14 Pages 1855—1858
DOI https://doi.org/10.2147/OPTH.S261098
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Nandini Bothra, Richa Dharap Wagh, Mohammad Javed Ali
Govindram Seksaria Institute of Dacryology, L.V. Prasad Eye Institute, Hyderabad 500034, Telangana, India
Correspondence: Nandini Bothra
Govindram Seksaria Institute of Dacryology, L.V. Prasad Eye Institute, Road No. 2, Banjara Hills, Hyderabad 500034, Telangana, India
Email [email protected]
Introduction: Dacryocystocele can be congenital or acquired and acute or chronic, based on underlying pathology. An inferomedial anterior orbital mass lesion can masquerade an acquired dacryocystocele with similar symptomatology; however, the treatment varies. Hence, a careful examination of the swelling to differentiate these masquerades is needed to ensure rightful treatment.
Patients and Methods: A retrospective, interventional study was performed on consecutive patients from January 2017 to October 2019 who presented with swelling in the lacrimal sac area of varying durations. They underwent computed tomography scans followed by surgical intervention. Their relation to the lacrimal drainage apparatus was explored.
Results: During the study period, 5 such patients were found in the records. The radiology was consistent with anterior orbital mass lesions, not involving the lacrimal sac. Histopathology after surgical excision was consistent with three of the lesions being dermoid cysts, one was cavernous hemangioma and one was a solitary fibrous tumor.
Conclusion: Inferomedial anterior orbital mass lesions can present as masquerades of acquired dacrycystoceles. Careful examination and high degree of suspicion is needed to distinguish these lesions and ensure correct treatment.
Keywords: dacryology, dacryocystocele, lacrimal, medial orbital dermoid, solitary fibrous tumor of the lacrimal sac
Introduction
Dacryocystocele is a gross dilatation of the lacrimal sac, presenting as a swelling below the medial canthal tendon as a result of combined proximal and distal obstructions at the level of common canalicular opening and the nasolacrimal duct, respectively.1 These swellings can be congenital or acquired and acute or chronic, based on the underlying pathology.1,2 The treatment for these lesions is determined by the age at onset and the presentation, and can include irrigation and probing, marsupialization or a dacryocystorhinostomy when indicated. Orbital masses arising from the anterior orbit and lying in the inferomedial area can present as swellings in the lower eyelid and medial canthal area, without much proptosis. Such lesions can be potentially misdiagnosed as lacrimal sac swelling in the absence of a careful examination. The current series reflect the presentation and management of five cases with inferomedial swellings located below the medial canthal tendon, mimicking acquired dacryocystoceles. The study conforms to the Tenets of Declaration of Helsinki. Written informed consent for the publication of case details and photographs have been obtained by the patient.
Case Report
Retrospective chart reviews were performed for patients presenting at the Dacryology Services from January 2017 to October 2019. This study is approved by the L V Prasad Eye Institute’s Institutional Ethics Committee. A total of 5 cases were found to present with lesions masquerading as acquired dacryocystocele. All the five cases presented with a painless, gradually progressing mass lesion in the lacrimal sac area, not extending above the medial canthal tendon. Of the five patients, only one of them presented with complaints of epiphora. None of them had any history of trauma. On examination, all five patients had swelling in the lacrimal sac area which was firm on palpation, non-tender and the posterior extent of the lesion was not palpable (Figure 1). Case 2 (Table 1) also showed mid-canalicular block involving the lower canaliculus of the affected right eye, however there was no history of trauma in the past or any other ocular surface disorder or systemic disease. No history of usage of topical medications. Case 5 (Table 1, Panel E) in addition to above findings, showed increased pigmentation of the overlying skin. Irrigation was freely patent in all 5 cases. Computed tomography scans of the orbits were performed in all cases (Table 1, Figure 1). All patients underwent excision under general anaesthesia, either by transconjunctival or an external approach. Due care to protect the proximal lacrimal passages was taken by inserting a Bowman’s lacrimal probe in the canaliculus throughout the duration of the surgery.
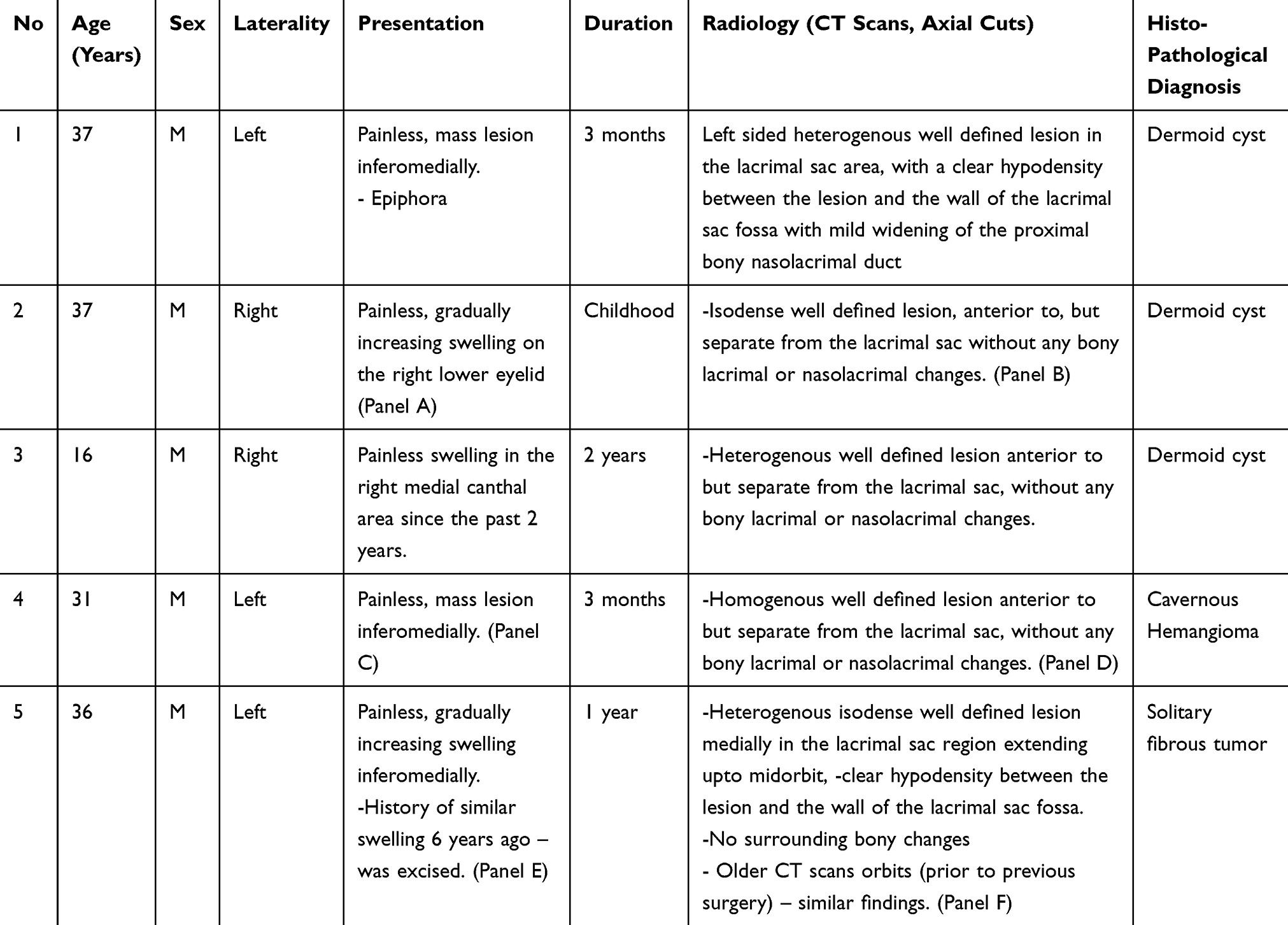 |
Table 1 Clinical symptoms and signs. |
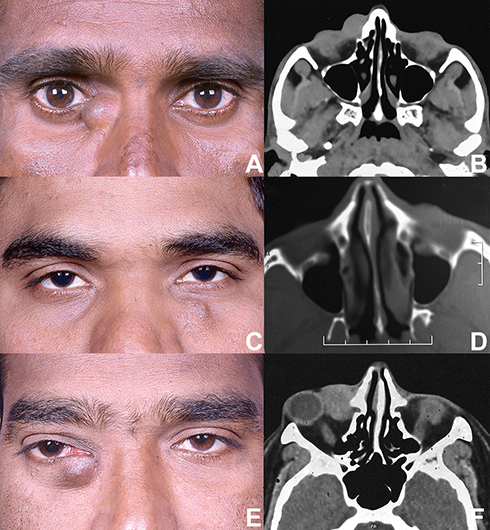 |
Figure 1 Clinical photograph (Case 2) showing swelling in the right lacrimal sac region, extending till the medial canthal region (A). Computed tomography scan, axial cut of the same patient showing isodense well-defined lesion, anterior to, but separate from the lacrimal sac (B). Clinical photograph (Case 4) demonstrating swelling the left lower eyelid in the anterior lacrimal crest region (C). Computed tomography, axial scan of the same patient demonstrating homogenous, well-defined lesion anterior to and separate from the lacrimal sac (D). Clinical photograph of the right eye (Case 5) showing swelling and increased pigmentation In the lacrimal sac region below the medial canthal tendon (E). Computed tomography axial scan of the same patient showing heterogenous, well-defined lesion, separate from the lacrimal sac (F). |
Intraoperatively, in a single case (Case 2, Table 1), the lesion was firmly adherent to the anterior wall of the lacrimal sac, from which it was dissected and the resultant small laceration in the sac wall was repaired with 6-0 polyglactin sutures. In addition, the mid-canalicular obstruction involving the lower canaliculus was trephined followed by a mini-monka stent intubation for 4 weeks.
The excised mass lesions were sent for histopathological analysis. On histopathology, the diagnosis in three cases was dermoid cyst, one was cavernous hemangioma and the last one was a solitary fibrous tumor (see Table 1). At 6-weeks post-operative follow-up, all the patients were relieved of their mass lesions and epiphora. The patient with mid-canalicular obstruction achieved anatomical and functional patency. Case 5 was scheduled for radiotherapy owing to the recurrence of the mass in the orbit.
Discussion
Dacryocystocele is mostly a clinical diagnosis based on history and examination. The most common presentation includes history of epiphora, swelling inferomedial to the medial canthus, and occasional acute inflammation.1 Imaging of acquired dacryocystocoele demonstrates fluid filled structure with thin rim enhancement, without any solid internal structures.3 Lacrimal sac malignancy can also present with similar clinical features.3 Inferomedial orbital masses in the anterior orbit can present as swellings in the lower eyelid and lacrimal sac area, without much proptosis. Symptomatically, these cases may or may not have epiphora. They generally do not have any history of acute inflammation in the past. Irrigation of the lacrimal passages is usually patent unless the mechanical effect of the lesion is gross upon the canaliculus or the lacrimal sac. Imaging in these cases shows the swelling to be separate from the lacrimal sac by a thin hypodense line. However, we would need serial imaging cuts to separate the lesion from the lacrimal sac, as these lesions may compress the lacrimal sac and make it harder to distinguish them from each other. CT-DCG will be a better modality in these cases as it will dilate the lacrimal sac due to the passage of the dye and also help to confirm a patent lacrimal system and thus, help to differentiate the mass from the lacrimal sac.
Differential diagnosis of medial canthal lesions would include lacrimal drainage and non-lacrimal ones. The lacrimal drainage lesions include congenital and acquired dacryocystocele, lacrimal sac diverticulum and lacrimal sac tumors. The non-lacrimal drainage lesions include dermoid and epidermoid cysts, encephalocele, benign fibrous histiocytoma, cavernous hemangioma, skin tumors, hygroma, sinus mucoceles, ectopic lacrimal gland and glial heterotropia.1,3,4 The treatment for these conditions varies from that of a dacryocystocele and thus, differentiation between them is needed.
Dermoid cyst represents 3–9% of all orbital masses.5 “Medial” superficial dermoids usually refer to a superomedial location lying lateral to the root of the nose and above the medial canthal tendon. Inferomedial superficial dermoid cysts are very rare, with only five cases being reported in literature.5 Owing to the proximity to the lacrimal sac, the potential to damage the lacrimal passages is very high. Two such cases with intraoperative damage to the lacrimal passages have been reported.3,5 In our series, intraoperative trauma to the lacrimal sac was noted in one case, which was successfully repaired. Orozco-Covarrubias et al6 reported a dermoid cyst having an accessory canaliculus, with lacrimal secretions as contents. An orbital septate dermoid cyst masquerading as a lacrimal sac diverticulum has also been reported.7 The possible etiology for the close adherence of the cyst to the lacrimal passages was considered to be inflammation in the cyst at some point in time.7 Hence, a meticulous dissection is warranted to prevent injuries to the lacrimal passages.
Extraconal presentations of cavernous hemangioma, are uncommon. Imaging demonstrates a well-defined lesion with moderate contrast enhancement.8 The present series found a similar presentation in the inferomedial orbit, close to the lacrimal passages, masquerading as lacrimal sac mass, without demonstrable dystopia of the globe.
Solitary fibrous tumors (SFT) are spindle cell tumors derived from the fibroblasts or mesenchymal cells, commonly seen involving the pleura. Orbit is a rare site and the imaging usually reveals a well-circumscribed mass with moderate to intense contrast enhancement.9 SFT can arise from the lacrimal sac or lie in close proximity to the lacrimal passages.9 In the present series, the SFT was in close proximity to the lacrimal sac, involving ant to mid orbit without much dystopia of the orbit, and a patent lacrimal system.
In conclusion, a high index of suspicion is needed when examining a mass over the lacrimal sac area with a patent lacrimal drainage system. Appropriate pre-operative counselling with regards to possibility of damage to the lacrimal passage and resultant epiphora should be discussed. The intra-operative placement of Bowman’s probe within the canaliculus and meticulous dissection of the mass from the lacrimal passage can help prevent injury and its further consequences. Patency of the lacrimal apparatus must be confirmed during and after the surgery.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Davies R, Watkins WJ, Kotecha S, Watts P. The presentation, clinical features, complications, and treatment of congenital dacryocystocele. Eye (Lond). 2018;32(3):522–526. doi:10.1038/eye.2017.235
2. Singh S, Ali MJ. Congenital dacryocystocele: a major review. Ophthalmic Plast Reconstr Surg. 2019;35(4):309–317. doi:10.1097/IOP.0000000000001297
3. Debnam JM, Esmaeli B, Ginsberg LE. Imaging characteristics of dacryocystocele diagnosed after surgery for sinonasal cancer. Am J Neuroradiol. 2007;28(10):1872–1875. doi:10.3174/ajnr.A0709
4. Ali MJ, Kamal S, Vemuganti GK, Naik MN. Glial heterotopia or ectopic brain masquerading as a dacyrocystocele. Ophthalmic Plast Reconstr Surg. 2015;31(2):e26–8. doi:10.1097/IOP.0000000000000050
5. Sherman RP, Rootman JA, Lapointe JS. Orbital dermoids: clinical presentation and management. Br J Ophthalmol. 1984;68:642–652. doi:10.1136/bjo.68.9.642
6. Orozco‐Covarrubias MD, Salazar‐Leon JA, Tamayo‐Sanchez L, Duran‐McKinster C, Ruiz‐Maldonado R. Dermoid cyst connected with the lacrimal canaliculum. Pediatr Dermatol. 1993;10:69–70. doi:10.1111/j.1525-1470.1993.tb00019.x
7. Ali MJ. Septate dermoid cyst mimicking septate lacrimal sac diverticulum. Ophthalmic Plast Reconstr Surg. 2019;35:e53. doi:10.1097/IOP.0000000000001226
8. Haaris GJ, Jakobiec FA. Cavernous hemangioma of the orbit. J Neurosurg. 1979;51:219–228. doi:10.3171/jns.1979.51.2.0219
9. Morawala A, Bothra N, Dendukuri G, Ali MJ. Solitary fibrous tumors of the lacrimal drainage system with variable orbital and sinonasal extensions: combined external and endoscopic surgical approach [published online ahead of print, 2020 Jan 23]. Ophthalmic Plast Reconstr Surg. 2020. doi:10.1097/IOP.0000000000001596
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.