Back to Journals » Clinical Interventions in Aging » Volume 15
Marked Reduction in 28-day Mortality Among Elderly Patients with Severe Community-acquired Pneumonia: Post Hoc Analysis of a Large Randomized Controlled Trial
Authors Liu Y ![]() , Zhang C
, Zhang C ![]() , Li C, Bai C, Shang H
, Li C, Bai C, Shang H ![]()
Received 30 June 2020
Accepted for publication 6 October 2020
Published 9 November 2020 Volume 2020:15 Pages 2109—2115
DOI https://doi.org/10.2147/CIA.S268140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yan Liu, 1,* Chi Zhang, 2,* Chengyu Li, 1 Chunxue Bai, 3 Hongcai Shang 1
1Key Laboratory of Chinese Internal Medicine of Ministry of Education and Beijing, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Institute for Brain Disorders, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3Department of Respiratory Medicine, Zhongshan Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongcai Shang
Key Laboratory of Chinese Internal Medicine of Ministry of Education and Beijing, Dongzhimen Hospital, Beijing University of Chinese Medicine, 5 Haiyuncang, Dongcheng District, Beijing 100700, People’s Republic of China
Email [email protected]
Background: There were few studies on the case mortality of severe community-acquired pneumonia (CAP) in elderly people. Improved outcomes with XueBiJing (XBJ) injection vs placebo have been shown in overall trial populations. We investigated the efficacy and safety of XBJ vs placebo in subjects with severe CAP stratified by age (< 65 and ≥ 65 years).
Methods: This post hoc analysis of a large randomized trial compared data from elderly and nonelderly patients with XBJ, 100 mL, q 12 h, or a visually indistinguishable placebo for five-to-seven days.
Results: Among subjects ≥ 65 years (n=291), 23 (16.0%) XBJ recipients and 41 (27.9%) placebo recipients (P=0.014) died within 28 days. Among subjects < 65 years (n=360), XBJ still had lower mortality (XBJ 15.6% vs placebo 22.8%; P=0.082), without significantly statistical difference. Total duration of ICU stay and the time of mechanical ventilation were similar in both groups (P> 0.05). XBJ also had a favorable safety profile, with no clinically relevant differences between the two groups. The overall incidence of adverse events was similar in both groups.
Conclusion: XBJ was safe and effective for reduction in 28-day mortality among elderly patients with severe CAP. Additional confirmatory trials involving elderly patients are needed to further confirm the present results.
Trial Registration: http://www.chictr.org.cn/index.aspx. ChiCTR-TRC-13003534.
Keywords: severe community-acquired pneumonia, randomized controlled trial, post hoc analysis, 28-day mortality rate, XueBiJing injection
Corrigendum for this paper has been published
Background
Community-acquired pneumonia (CAP) represents an important threat to the health of elderly adults.1 Like other respiratory infections, people at the extremes of age are at greatest risk and have worse outcomes. In adults, the incidence of CAP and related hospitalization and mortality increase steadily with age, even when these rates are adjusted for chronic health problems such as lung or heart conditions.2,3 The incidence of CAP in adults increases with age, with a dramatic rise after the age of 65. In developed countries, almost one half of the total hospitalizations for CAP occur in patients over 65 years old and pneumonia is a leading cause of death among this age group.4 The severity of CAP also increases with age, primarily due to age-related immune dysfunction, and greater likelihood of underlying comorbid factors in elderly patients.5
However, despite the recognized importance of CAP in the elderly, there is little information about the precise etiology and prognosis factors affecting older patients admitted to an intensive care unit (ICU) for severe CAP although such knowledge seems basic to the most appropriate management of elderly patients.6 American Thoracic Society guidelines suggest that three criteria can be used to define appropriate empirical treatment of CAP: the severity of pneumonia at presentation, the presence of underlying disease, and age.7 As a result, different antimicrobial strategies are proposed for outpatients according to age and/or underlying condition. Conversely, all patients with severe CAP are included in the same therapeutic group whatever their age, and the potential implications of advanced age on antimicrobial management are not mentioned. Given the morbidity and mortality of severe CAP in the elderly, new therapeutic options would be valuable.8
XueBiJing (XBJ), an herbal-based intravenous preparation approved by the National Medical Products Administration (NMPA) China in 2004, has been incorporated into routine sepsis care in China.9,10 Pharmacological studies have shown that XBJ has an antagonistic effect on endotoxin, and an inhibitory effect on the uncontrolled release of endogenous inflammatory mediators produced by endotoxin-stimulated monocytes/macrophages. XBJ also can improve the coagulation disorder in DIC, increase the activity of superoxide dismutase, regulate hypersensitive or hyposensitive immune response, and prevent the development of organ dysfunction in acute insults. The main pharmacological effects of XBJ might be summarized as follows: (1) antagonizing endotoxin; (2) inhibiting inflammatory cytokines; (3) regulating immune function; (4) improving the balance of coagulation; and (5) protecting organ damage.11–13 A recent well-done large randomized study showed XBJ effective in patients with severe CAP.14 This large randomized controlled trial is more than quintuple the size of a trial in severe CAP.15 Impressive benefit with this herbal-based medication was an 8.8% absolute reduction in mortality in patients who received XBJ.
Few clinical trials have examined the safety or impact of new therapeutic options on mortality rate in an older high-risk cohort with severe CAP, data in individuals with severe CAP in this age group is largely lacking. The present analysis evaluated the effects of XBJ and placebo in two age groups (≥65, <65 years) using data from the XBJ trial. Subjects aged 65 years may represent older patients of greatest concern to clinicians. This study provides information to clinicians on the efficacy and safety of XBJ in the elderly subjects with severe CAP.
Methods
Design Overview
A post hoc analysis was carried out using data from the main multicenter randomized controlled trial (RCT) “XueBiJing injection versus placebo for critically ill patients with severe community-acquired pneumonia: a randomized controlled trial”.14 Details of the XBJ trial have been previously published. The protocol is consistent with the principles of the Declaration of Helsinki, was approved by the Medical Ethics Committee of Zhongshan Hospital, Fudan University 2011–38(3) and the participants gave their written informed consent. The trial included 710 severe CAP patients, randomly assigned to receive XBJ (n=334), or placebo (n=341). The participants received the solvent only (normal saline, 200 mL, q 12 h) in the placebo group and the solvent plus XBJ (normal saline 100 mL+XBJ 100 mL, q 12 h) in the XBJ group. Both groups received a standard therapy (such as antibiotics) chosen by the attending physician according to the 2007 ATS/IDSA guideline. The primary outcome was eight-day improvement in the pneumonia severity index (PSI) risk rating. Main secondary outcomes were 28-day mortality rate, duration of mechanical ventilation and total duration of ICU stay. In this post hoc analysis of the XBJ study the primary outcome was 28-day mortality. Other secondary endpoints were the time of mechanical ventilation, total duration of ICU stay.
Statistical Analyses
Primary outcome analysis was a simple categorical frequency comparison by use of the chi-squared test. For time-to-event variables, Kaplan–Meier estimates were used and the groups were compared with a log rank test. HR and associated 95%CIs were estimated from the Cox proportional hazards model. The secondary outcome for the time of mechanical ventilation was analyzed by t-test or the Wilcoxon rank sum test as appropriate. The same analysis was used for other continuous variables, such as total duration of ICU stay. Categorical variables were compared using the chi-squared test or Fisher's exact test. Descriptive statistics (number and frequency) were used to summarize all safety outcomes for each group. Safety outcomes included serious, nonserious adverse events, and laboratory measurements. All outcomes were analyzed in the intent-to-treat population, which included all patients as randomized. Statistical analyses were performed using SAS version 9.4 (SAS Institute Inc.), with a two-sided P-value of less than 0.05 considered significant.
Results
Demographic characteristics stratified according to age group and treatment arms are summarized in Table 1. The mean age of elderly patients (n=291) was 70.47±3.23 years; and n=190, 65.29% were male. The mean age of nonelderly patients (n=360) was 49.76±11.63 years; and n=253, 70.28% were male. BMI did not differ between the treatment or age groups at baseline (≥65 years P=0.929, <65 years P=0.749). Differences between age groups in baseline comorbidities, PSI score or other biological parameters were not significant.
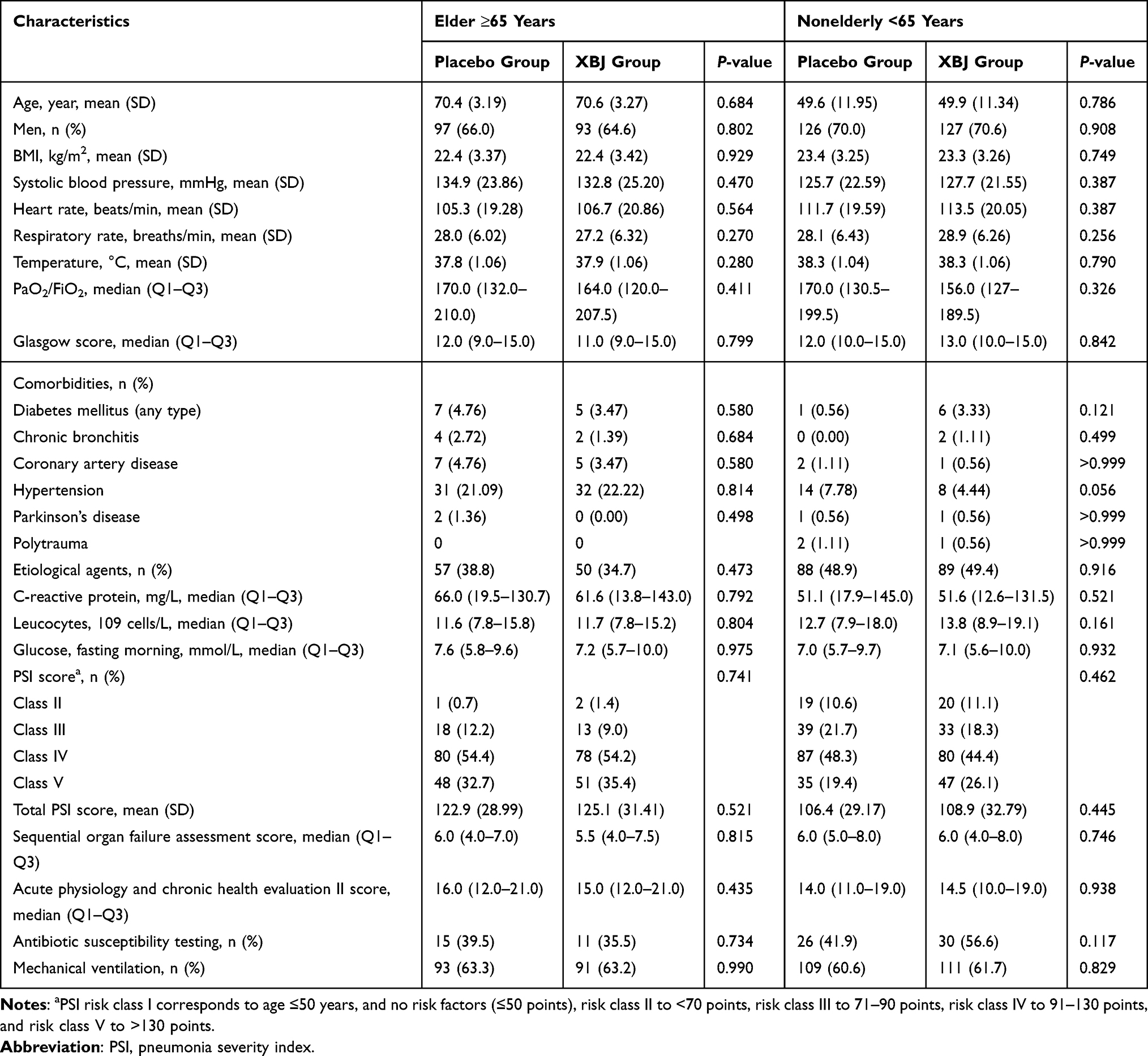 |
Table 1 Comparison of Demographic and Basal Clinical Characteristics of Patients Between XueBiJing Injection and Placebo Groups |
Rate of patients with acute respiratory distress syndrome (ARDS) and septic shock, the baseline settings of mechanical ventilation, and the frequency of antimicrobial prescriptions in each age group are listed in Table 2. There were no significant differences in antimicrobial treatment (beta-lactam, quinolones, glycopeptide, oxazolidinones, antifungal agents, tetracyclines, macrolide, aminoglycoside, nitroimidazoles, antivirals, lincomycin, and sulfanilamide) or patient parameters (septic shock and ARDS at baseline and on study) between the XBJ and placebo groups in each age group. In addition, microbiologic identification was similar in both study groups (all P>0.05) (Supplementary Material Table S1).
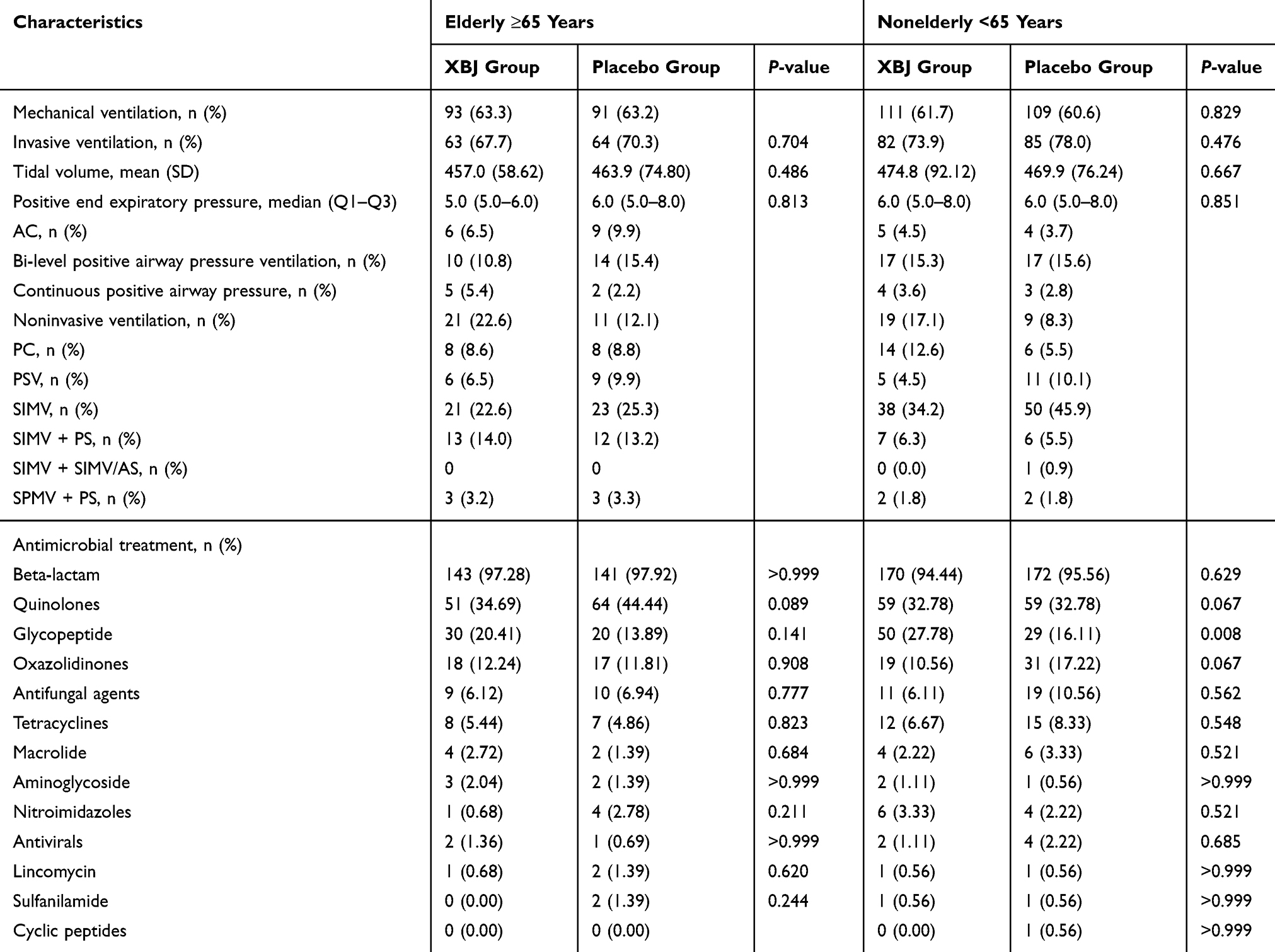 |
Table 2 Rate of Patients with Acute Respiratory Distress Syndrome and Septic Shock, The Baseline Settings of Mechanical Ventilation, and the Frequency of Antimicrobial Prescriptions for XueBiJing Group vs Placebo Group Using Descriptive Statistics for the Intention-to-treat Populations |
Among elderly patients (n=291), 28-day mortality was significantly lower in those who received XBJ vs those who received placebo (P=0.014) (Table 3). Elderly patients with XBJ had a significantly inferior overall survival to those with placebo. The HR of was 0.57 (95%CI, 0.34–0.95; P =0 0.029) (Figure 1). No statistically significant difference in mortality between the two groups was seen in younger patients (P=0.082). About the time of mechanical ventilation and total duration of ICU stay, there were decreased tendency without statistic difference between elderly and nonelderly patients in XBJ and placebo group. Some secondary outcomes are listed in Supplementary Material Table S2. Among elderly patients, the XBJ group had a significantly lower pneumonia severity index (PSI) (96.0±26.18) than the control group (106.9±28.92) (P=0.001) at day eight.
 |
Table 3 The Primary and Two Secondary Outcomes |
 |
Figure 1 Kaplan–Meier survival curve of overall survival after XueBiJing (XBJ) and placebo for patients in (A) elderly group: patients with XBJ had a significantly inferior overall survival to those who with placebo. The HR of was 0.57 (95%CI, 0.34–0.95; P=0 0.029), (B) nonelderly group: the HR was 0.67 (95%CI, 0.41–1.08; P=0 0.0949). |
Adverse events (AEs) that occurred with a frequency of >1% are summarized in Supplementary Material Table S3. Overall, XBJ demonstrated a similar overall safety profile among the subgroups of patients aged <65 and ≥65 years. In particular, very similar incidences of low red blood cell count (7.22% vs 5.56%) and elevated aspartate amino transferase (5.56% vs 7.64%) were seen in the subgroups aged <65 and ≥65 years, respectively. No severe AEs occurred either in elderly or nonelderly patients after XBJ therapy.
Discussion
The overall results of this large trial showed that XBJ is an effective and well-tolerated therapy for patients with severe CAP.14 With high efficacy and good tolerability, XBJ compares favorably with the placebo, especially as there was an 8.8% absolute reduction in mortality in patients who received XBJ. In addition, with improved PSI risk score.
In the current analysis, XBJ showed a similar favorable safety profile in older and younger patients alike, and the high efficacy of XBJ was preserved in older patients. No clinically relevant differences in safety profile were observed between the subgroups of patients aged <65 years and ≥65 years. These results suggest that there is no a priori need for upfront dose reductions when prescribing XBJ to elderly patients. Prospectively planned ongoing trial is further evaluating the efficacy and safety benefits of XBJ in older patients.
CAP seems more severe in older than in younger patients. Fine and colleagues’ have demonstrated that being aged over 65 years was one of the five predisposing factors for a complicated course.15 In most prognosis studies, age is a strong predictor of mortality.16 Consequently, the mortality rate of such pulmonary infection seems high in older people. Among elderly hospitalized patients overall, the death rate was about 30%.17,18 When patients were admitted to an ICU, mortality was even higher.19 In Rello’s study, the mortality rate was 40%.18 In the present work, 94.07% of the participants were from ICUs, the 28 day mortality rate among older patients with XBJ was 16.0%. This rate was significantly lower than the rate observed in placebo group (27.9%).
Although efficacy was not the primary end point of the original study, efficacy comparisons were undertaken to allow for a more clinically meaningful comparison of the tolerability profiles and to explore any clinically relevant differences in efficacy between younger and older patients. One recently presented study has evaluated use of hydrocortisone in patients with severe CAP in the ICU setting.20 Among patients with a mean age of 62 years, a continuous infusion of hydrocortisone did not result in lower 28-day mortality than placebo. We believe that this analysis is particularly intriguing: in fact, this result on mortality overcomes one of the main limitations of our previous study.
XBJ has pharmacological effects on antagonizing endotoxin, inhibiting inflammatory mediators, improving coagulation function, protecting endothelial cells, improving microcirculation, and regulating immune response. XBJ can obviously protect vascular endothelial cells by inhibiting the expression of early/late inflammatory cytokines, attenuate the interaction between inflammation system and coagulation system, and prevent the development of multiple organ dysfunction.21–23 Meanwhile, it markedly improves the hyperactive state of the natural immune response during the early stage of sepsis and alleviates the gradually aggravated immunosuppressive state, thereby comprehensively modulating systemic inflammation, coagulopathy and immune dissonance in the development of sepsis.22 Taken together, these results might suggest the integrated regulation of herbal medicine on multicomponents, multipathways, and multitargets.
All herbal therapy requires active supervision, particularly for elderly patients, who could have other illnesses and be receiving concomitant medications.23 Elderly patients could also be at greater risk of experiencing toxicity, particularly if their renal function is impaired. Unlike tablets at home, XBJ IV therapy is administered in the hospitals and the clinician has an active role in treatment administration and the management of any toxicity.
The results of our study come with some limitations. First, the analyses were planned post hoc, so the results cannot be considered confirmative. Also, the number of patients included in each age group was relatively small and did not allow multivariate analysis involving backward stepwise logistic regression in each group to show the exact level of significance. The balance in baseline characteristics in subgroups illustrates that the balancing effect of randomization may persist after the subgrouping and, consequently, the results may be unbiased. The strengths of this study are the strict methodology and high quality of the data of the original RCT, which minimized the risk of bias and random findings.
Conclusions
Recognizing the methodological limitations of post hoc analyses, marked reduction in 28-day mortality was observed in older XBJ users with severe CAP. As the analyses were planned post hoc and the power is reduced compared to the original trial result, the results of our analysis needs to be confirmed by a large, well-designed, and appropriately focused randomized clinical trial in an elderly population.
Abbreviations
AE, adverse event; APACHE, acute physiology and chronic health evaluation; ARDS, acute respiratory distress syndrome; CAP, community-acquired pneumonia; ICU, intensive care unit; K-M curve, Kaplan–Meier curve; NMPA, national medical products administration; PSI, pneumonia severity index; RCT, randomized controlled trial; SIRS, systemic inflammatory response syndrome; SOFA, sequential organ failure assessment; XBJ, XueBiJing injection.
Data Sharing Statement
All data generated or analyzed during this study are included in the published article.14
Ethics Approval
The original study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Zhongshan Hospital, Fudan University (2011–2038 [3]).
Acknowledgments
The authors appreciate all the participants for making contributions to this work. Yan Liu and Chi Zhang are equally contributing co-first authors.
Funding
This work was supported by National High-level Personnel of Special Support Program (W02020052).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brown RB. Community-acquired pneumonia: diagnosis and therapy of older adults. Geriatrics. 1993;48(2):43–50.
2. Loeb MB. Community-acquired pneumonia in older people: the need for a broader perspective. J Am Geriatr Soc. 2003;51(4):539–543. doi:10.1046/j.1532-5415.2003.51165.x
3. Neupane B, Walter SD, Krueger P, et al. Predictors of inhospital mortality and re-hospitalization in older adults with community-acquired pneumonia: a prospective cohort study. BMC Geriatr. 2010;10(1):22. doi:10.1186/1471-2318-10-22
4. Kelly E, MacRedmond RE, Cullen G, et al. Community-acquired pneumonia in older patients: does age influence systemic cytokine levels in community-acquired pneumonia? Respirology. 2009;14(2):210–216. doi:10.1111/j.1440-1843.2008.01423.x
5. Vila-Corcoles A, Ochoa-Gondar O, Rodriguez-Blanco T, et al. Epidemiology of community-acquired pneumonia in older adults: a population-based study. Respir Med. 2009;103(2):309–316. doi:10.1016/j.rmed.2008.08.006
6. Fung HB, Monteagudo-Chu MO. Community-acquired pneumonia in the elderly. Am J Geriatr Pharmacother. 2010;8(1):47–62. doi:10.1016/j.amjopharm.2010.01.003
7. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72.
8. Fleischmann C, Scherag A, Adhikari NK, et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am J Respir Crit Care Med. 2016;193(3):259–272. doi:10.1164/rccm.201504-0781OC
9. Qi F, Liang ZX, She DY, et al. A clinical study on the effects and mechanism of xuebijing injection in severe pneumonia patients. J Tradit Chin Med. 2011;31(1):46–49.
10. Li C, Wang P, Zhang L, et al. Efficacy and safety of Xuebijing injection (a Chinese patent) for sepsis: a meta-analysis of randomized controlled trials. J Ethnopharmacol. 2018;224:512–521.
11. Jiang M, Zhou M, Han Y, et al. Identification of NF-κB inhibitors in Xuebijing injection for sepsis treatment based on bioactivity-integrated UPLC-Q/TOF. J Ethnopharmacol. 2013;147(2):426–433.
12. Wang Q, Wu X, Tong X, et al. Xuebijing ameliorates sepsis-induced lung injury by downregulating HMGB1 and RAGE expressions in Mice. Evid Based Complement Alternat Med. 2015;2015(264):860259.
13. Liu Y, Tian X, Cui M, et al. Safflower yellow inhibits angiotensin II-induced adventitial fibroblast proliferation and migration. J Pharmacol Sci. 2014;126(2):107.
14. Song Y, Yao C, Yao Y, et al. XueBiJing injection versus placebo for critically ill patients with severe community-acquired pneumonia: a randomized controlled trial. Crit Care Med. 2019;47(9):e735–e743.
15. Fine MJ, Smith DN, Singer DE. Hospitalization decision in patients with community-acquired pneumonia: a prospective cohort study. Am J Med. 1990;89(6):713–721. doi:10.1016/0002-9343(90)90211-U
16. Marrie TJ, Haldane EV, Faulkner RS, et al. Community-acquired pneumonia requiring hospitalization. Is it different in the elderly? J Am Geriatr Soc. 1985;33(10):671–680.
17. Kaplan V, Angus DC, Griffin MF, et al. Hospitalized community-acquired pneumonia in the elderly: age- and sex-related patterns of care and outcome in the United States. Am J Respir Crit Care Med. 2002;165(6):766–772.
18. Rello J, Rodriguez R, Jubert P, et al. Severe community-acquired pneumonia in the elderly: epidemiology and prognosis. Study group for severe community-acquired pneumonia. Clin Infect Dis. 1996;23(4):723–728.
19. Venkatesh B, Finfer S, Cohen J, et al. Adjunctive glucocorticoid therapy in patients with septic shock. N Engl J Med. 2018;378(9):797–808.
20. Agbabiaka T, Wider B, Watson LK, et al. Concurrent use of prescription drugs and herbal medicinal products in older adults: a systematic review protocol. Syst Rev. 2016;5(1):65. doi:10.1186/s13643-016-0244-2
21. Liu MW, Wang YH, Qian CY, Li H. Xuebijing exerts protective effects on lung permeability leakage and lung injury by upregulating Toll-interacting protein expression in rats with sepsis. Int J Mol Med. 2014;34(6):1492–504.
22. Liu LW, Shi YY, Li ZL, Zuo LH, Sun Z. Metabolomic Insights Into the Synergistic Effect of Biapenem in Combination With Xuebijing Injection Against Sepsis. Front Pharmacol. 2020;11.
23. Agbabiaka T, Wider B, Watson LK, Goodman C. Concurrent use of prescription drugs and herbal medicinal products in older adults: a systematic review protocol. Syst Rev. 2016;5:65.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.