Back to Journals » Clinical Ophthalmology » Volume 17
Mapping the Burden of Visual Impairment Due to Onchocerciasis Infection in Central Africa from 1990 to 2019
Authors Fan X, Li J, Yundendorj G, Duan Y, Liu S, Jiao J ![]() , Liu L
, Liu L ![]()
Received 22 July 2023
Accepted for publication 27 October 2023
Published 6 November 2023 Volume 2023:17 Pages 3373—3377
DOI https://doi.org/10.2147/OPTH.S431911
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Xiaoe Fan,1,* Junying Li,2,* Gantugs Yundendorj,3 Yajian Duan,4 Shunming Liu,5 Jinghua Jiao,6,7 Lei Liu5
1Department of Ophthalmology, Jincheng People’s Hospital, Jincheng, People’s Republic of China; 2Department of Cataract Surgery, Baotou Chaoju Eye Hospital, Baotou, Inner Mongolia, People’s Republic of China; 3Department of Health Policy, School of Public Health, Mongolian National University of Medical Sciences, Ulaanbaatar, Mongolia; 4Department of Ophthalmology, Shanxi Bethune Hospital, Shanxi Academy of Medical Science, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China; 5Guangdong Eye Institute, Department of Ophthalmology, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 6Department of Anesthesiology, Guangzhou Eighth People’s Hospital, Guangzhou Medical University, Guangzhou, People’s Republic of China; 7Department of Anesthesiology, Central Hospital Affiliated to Shenyang Medical College, Shenyang, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoe Fan, Department of Ophthalmology, Jincheng People’s Hospital, Jincheng, People’s Republic of China, Email [email protected] Jinghua Jiao, Department of Anesthesiology, Guangzhou Eighth People’s Hospital, Guangzhou Medical University, Guangzhou, People’s Republic of China, Email [email protected]
Background
Human onchocerciasis, also known as river blindness, mainly occurs (more than 99% of infected people globally) in 31 countries of the tropical areas of sub-Saharan Africa. The disease is transmitted by the bite of a black fly of the species Simulium and caused by infection from the filarial nematode (roundworm), Onchocerca volvulus. It is responsible for permanent blindness and one of the tropical, traveling diseases prioritized by the World Health Organization (WHO) for prevention and control. To eliminate onchocerciasis-associated blindness, it is important to identify areas where there is still high ongoing disease burden. Although the recent study has emerged highlighting the prevention and overall burden of onchocerciasis in Africa,1,2 there is no evidence on the prevalence and burden of onchocerciasis-associated blindness and vision loss (BVI) as well as its severity throughout this region in detail.
Methods
In order to fill these gaps, global burden of disease 2019 (GBD 2019) dataset, which provided cause-specific BVI data in the Global Health Data Exchange (http://ghdx.healthdata.org/gbd-results-tool), was used to map the regional and national burden of BVI from 1990 to 2019. The regional prevalence and years lived with disability (YLDs) of BVI attributable to onchocerciasis were reported for the African region, using the methodological framework and analytical strategies adopted by GBD 2019.3–5 The present study used the data on number (thousand), and age-standardized rate (ASR, per 100,000) of BVI prevalence and YLDs estimates to assess the burden. The estimates were all reported as counts, and age-standardised rates, along with their corresponding 95% uncertainty intervals (UIs). Also, the average annual percentage changes (AAPC) with its 95% confidence interval (95% CI) were used to represent the trends of ASR. If the AAPC value as well as its 95% CI are all higher or lower than 0, it will be identified as statistically significant.
Results
In 2019, the highest number of BVI attributable to onchocerciasis were observed in the Western Sub-Saharan Africa region, with an estimated 446.7 thousand BVI (95% UI: 392.3 to 508.7) and 35.3 thousand YLDs (95%UI: 24.6 to 49.5), which were decreased by 36% and 43% compared with 1990, respectively. The highest ASR of prevalence and YLDs of BVI were 588.2 (95%UI: 518 to 670.1) and 41.1 (95%UI: 28.2 to 57) in Central Sub-Saharan Africa in 2019, respectively. During past three decades, the ASR of prevalence and YLDs of BVI attributable to onchocerciasis decreased largely with AAPC of −3.95 (95% CI: −4.16 to −3.74) and −4.39 (95% CI: −4.77 to −4) in the Western Sub-Saharan Africa region, respectively (Table 1). The ASR of prevalence and YLDs in males was higher than that in females, and both the highest prevalence and YLD rates were found in the 65–69 age groups in 2019. At national level, South Sudan (2606.1, 95%UI: 2343.7 to 2893.8) and Niger (0.2, 95%UI: 0.2 to 0.3) had the highest and lowest ASR of BVI related prevalence attributable to onchocerciasis in 2019, respectively (Figure 1A). In terms of burden, South Sudan (220, 95%UI: 153.7 to 308.2) also had the highest ASR of YLD on onchocerciasis related BVI (Figure 1B). During study period, only South Sudan (AAPC: 0.67, 95% CI: 0.55 to 0.79) and Chad (AAPC: 0.58, 95% CI: 0.37 to 0.78) had increasing trends of ASR of prevalence. Cote d’Ivoire, Guinea-Bissau, Burkina Faso, Niger, Mali were top five countries with decreasing trends of prevalence (Figure 1C). In terms of YLDs, only South Sudan showed upward trends (AAPC: 0.41, 95% CI: 0.27 to 0.55). Furthermore, Cote d’Ivoire, Guinea-Bissau, Burkina Faso, Niger, and Ghana were top five countries with downward trends of YLDs (Figure 1D). In 2019, South Sudan had the highest ASR of prevalence and YLD of moderate, severe vision loss, and blindness, respectively.
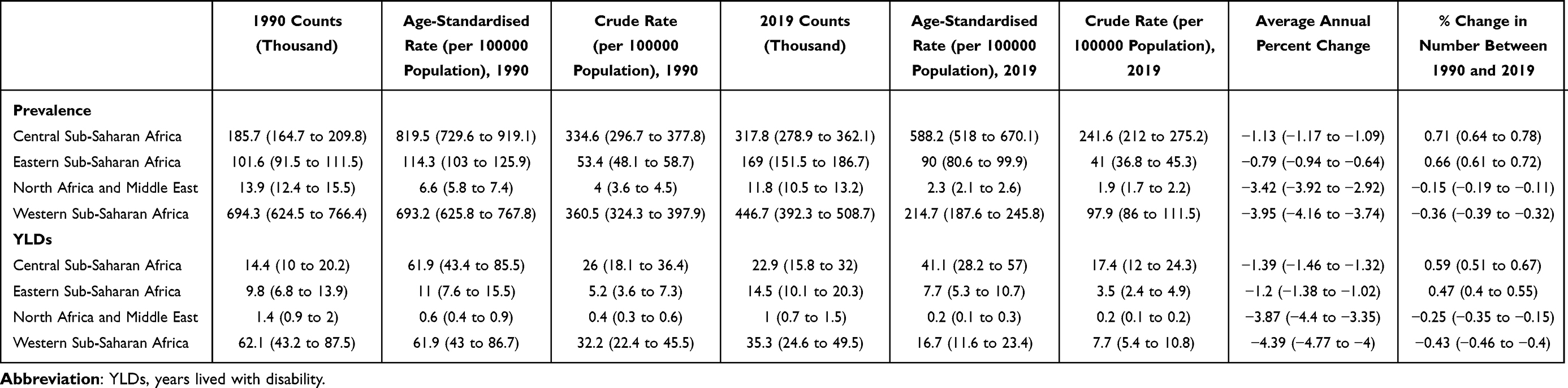 |
Table 1 Burden of Blindness and Vision Loss Attributable to Onchocerciasis in Africa Region from 1990 to 2019 |
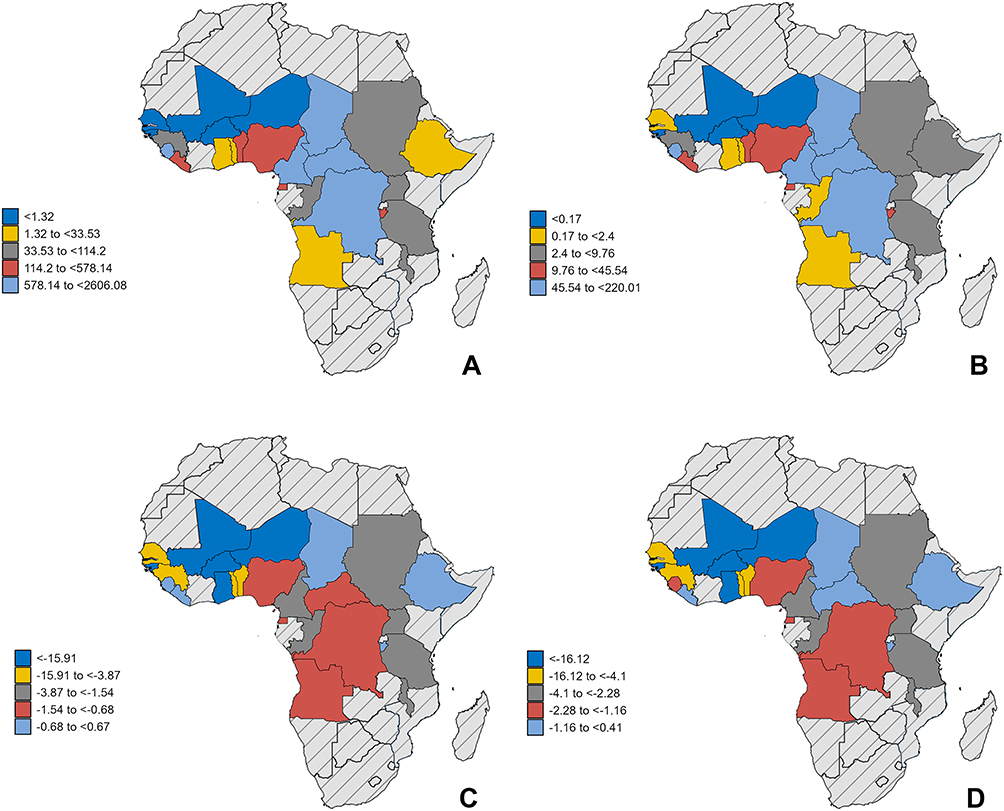 |
Figure 1 Regional map of onchocerciasis-related vision impairment burden. Geographic distribution of age-standardized prevalence (per 100,000 population) in nations with onchocerciasis-related vision impairment in 2019 (A); geographic distribution of age-standardized years lived with disability (YLDs, per 100,000 population) in nations with onchocerciasis-related vision impairment in 2019 (B); average annual percentage changes (AAPC) of age-standardized prevalence in nations with onchocerciasis-related vision impairment from 1990 to 2019 (C); AAPC of age-standardized YLDs in nations with onchocerciasis-related vision impairment from 1990 to 2019 (D). |
Discussion
In recent decades, through vector control (larviciding) and using mass drug administration (MDA) with ivermectin, such as the Community-Directed Treatment with Ivermectin (CDTI) strategy,6 and alternative treatment strategies (ATS) including ground larviciding,7 there was a significant reduction in the age-standardised prevalence and YLD rate of BVI attributable to onchocerciasis over the period 1990 to 2019 in Africa, particularly in Western Sub-Saharan Africa region. This is in accordance with a regional reduction in the onchocerciasis infection over the last two decades throughout western and central Africa.1 Due to the major public health concern on onchocerciasis, large-scale control programmes were performed previously with strategies for its control and prevention while in recent years strategies have been directed at its elimination. The Onchocerciasis Control Programme (OCP) aerial larviciding, the African Programme for Onchocerciasis Control (APOC) by Ivermectin mass drug administration (MDA), and alternative treatment strategies including enhanced community-directed treatment with ivermectin (CDTI), community-directed treatment (CDT) with drug combinations or new drugs and test-and-treat (TNT) strategies led to the control of onchocerciasis as a public health problem. Notably, Western Sub-Saharan Africa had the largest number of cases, while Central Sub-Saharan Africa had the highest ASR of disease burden. Moreover, there were also age, and gender differences in onchocerciasis-related BVI burden. Males with higher disease burden may be related to more involved in outdoor activities, exposing themselves to infective blackfly bites. Therefore, improved protection and ivermectin treatments should be performed for males. It is interesting that both the ASR of prevalence and YLDs increased with age, indicating that improved, longitudinal intervention strategies might overcome the disease burden. In 2019, the proportion of all BVI attributable to onchocerciasis varied markedly by country (from 0.2 to 2601.1). South Sudan had the highest burden in 2019 and faster annual increases in BVI due to onchocerciasis. This may be related to the lower ivermectin treatment coverage, the existence of abundant breeding sites of biting black flies in central Africa, and long-standing civil strife for several years. However, previous estimates showed particularly high burden in the Congo according to Rapid Epidemiological Mapping of Onchocerciasis (REMO) data. The African Programme for Onchocerciasis Control (APOC) or preventive chemotherapy with MDA are important for the control of onchocerciasis and elimination of transmission.2 Potential limitations related to onchocerciasis estimated in GBD studies were described previously, including coverage rate, data quality and availability. Further well-designed and population-based study are still needed to estimate the disease burden.
Conclusions
In sum, the ASR of prevalence and YLDs of onchocerciasis-related BVI in the African region have decreased over the past three decades. Closer prenatal monitoring is recommended for countries and territories, particularly those countries with higher disease burden. Further reduction can be facilitated by policy interventions targeted on the improvement of ivermectin treatment coverage, the landscape as well as living environment, and increasing public awareness.
Abbreviation
BVI, blindness and vision loss; GBD, global burden of disease; YLDs, years lived with disability; MDA, mass drug administration; CDTI, Community-Directed Treatment with Ivermectin; REMO, Rapid Epidemiological Mapping of Onchocerciasis; APOC, African Programme for Onchocerciasis Control; ASR, age-standardized rate; UIs, uncertainty intervals; AAPC, average annual percentage changes; CI, confidence interval.
Data Sharing Statement
The data that support the findings of this study are available from the Global Health Data Exchange (http://ghdx.healthdata.org/gbd-results-tool), which were used under license for this study, and so are publicly available. All data associated with this paper will be made available upon reasonable request from corresponding author (LL).
Ethics Approval and Consent to Participate
The protocol for this study was approved by the Research Ethics Committee of the Guangdong Provincial People`s Hospital (KY-Q-2022-495-01).
Funding
This study was supported by Guangdong Provincial People`s Hospital Supporting Fund for Talent Program (Grant No. KY0120220263), Health Commission of Shanxi Province (No. 2020146), the Youth Talent Support Program of Liaoning Province (XLYC2203192), National Natural Science Foundation of China (Grant No. 82003882), and Science and Technology Department of Shanxi Province (No. 202103021223014).
Disclosure
The authors declare that they have no competing interests.
References
1. Schmidt CA, Cromwell EA, Hill E, et al. LBD 2019 neglected tropical diseases collaborators; hay si. The prevalence of onchocerciasis in Africa and Yemen, 2000–2018: a geospatial analysis. BMC Med. 2022;20(1):293. doi:10.1186/s12916-022-02486-y
2. Vinkeles Melchers NVS, Stolk WA, van Loon W, et al. The burden of skin disease and eye disease due to onchocerciasis in countries formerly under the African Programme for Onchocerciasis Control mandate for 1990, 2020, and 2030. PLoS Negl Trop Dis. 2021;15(7):e0009604. doi:10.1371/journal.pntd.0009604
3. GBD 2019 Demographics Collaborators. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: a comprehensive demographic analysis for the global burden of disease study 2019. Lancet. 2020;396:1160–1203. doi:10.1016/S0140-6736(20)30977-6
4. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396:1223–1249. doi:10.1016/S0140-6736(20)30752-2
5. Vollset SE, Goren E, Yuan CW, et al. Fertility, mortality, migration, and population scenarios for 195 countries and territories from 2017 to 2100: a forecasting analysis for the Global Burden of Disease Study. Lancet. 2020;396:1285–1306. doi:10.1016/S0140-6736(20)30677-2
6. Lawrence J, Sodahlon YK, Ogoussan KT, Hopkins AD. Growth, Challenges, and solutions over 25 years of mectizan and the impact on onchocerciasis control. PLoS Negl Trop Dis. 2015;9(5):e0003507. doi:10.1371/journal.pntd.0003507
7. Ekanya R, Obie ED, Hamill L, et al. The preparatory phase for ground larviciding implementation for onchocerciasis control in the Meme River Basin in South West Cameroon: the COUNTDOWN consortium alternative strategy implementation trial. Parasit Vectors. 2022;15(1):219. doi:10.1186/s13071-022-05300-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Underutilization of Mental Health Care Services in the Lives of People with Blindness or Visual Impairment: A Literature Review on Rehabilitation Factors Toward Provision

Richardson CG
Clinical Ophthalmology 2024, 18:953-980
Published Date: 29 March 2024
Global, Regional, and National Burden of Iodine Deficiency in Reproductive Women From 1990 to 2019, and Projections to 2035: A Systematic Analysis for the Global Burden of Disease Study in 2019
Lin J, Tan HL, Ge H
International Journal of Women's Health 2025, 17:1863-1875
Published Date: 21 June 2025
Global, Regional and National Burden of Low Back Pain in Adolescents Aged 10–19 years, 1990–2021: A Systematic Analysis of the Global Burden of Disease Study 2021
Wang S, Zhang S, Li M, Chen S, Chen Y, Song Y, Zhang X
Journal of Pain Research 2025, 18:3171-3183
Published Date: 26 June 2025