Back to Journals » Advances in Medical Education and Practice » Volume 17
Mapping Biomedical Engineering Education and Research in Sub-Saharan Africa: A Bibliometric and Systematic Analysis
Authors Dirisu JO ![]() , Dzogbewu TC, De Beer DJ
, Dzogbewu TC, De Beer DJ
Received 24 December 2025
Accepted for publication 14 March 2026
Published 8 April 2026 Volume 2026:17 591352
DOI https://doi.org/10.2147/AMEP.S591352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Joseph O Dirisu,1– 3 Thywill Cephas Dzogbewu,1,2 Deon Johan De Beer1,2
1Department of Mechanical and Mechatronics Engineering, Central University of Technology, Bloemfontein, Free State, South Africa; 2Centre for Rapid Prototyping and Manufacturing, Central University of Technology, Bloemfontein, Free State, South Africa; 3Department of Mechanical Engineering, Covenant University, Ota, Nigeria
Correspondence: Joseph O Dirisu, Email [email protected]
Abstract: Biomedical engineering (BME) education is critical to the growth of engineering-driven healthcare entrepreneurs and the enhancement of health systems globally. This study examines the evolution of BME education research over the past 20 years, with a focus on Sub-Saharan Africa (SSA), using a mixed-methods approach that includes bibliometric analysis and a systematic literature review. Between 2000 and 2025, there were almost 370,000 BME-related publications indexed in PubMed alone. Bibliometric data indicates a large global growth, mostly because of advances in artificial intelligence and digital health. However, compared to major producers like the US and China, SSA is notably underrepresented, and African contributions account for a very small percentage of overall output. These differences are further contextualized by the systematic review of literature that is indexed in PubMed, Web of Science, and Scopus. Important findings include chronic financing constraints, restricted growth of specialized sub-disciplines, poor infrastructure, and inconsistent research productivity across SSA nations. SSA suffers structural obstacles that limit academic progress and technical advancement, in contrast to technologically advanced regions that are distinguished by robust research capability, innovation ecosystems, and sophisticated medical device development. The study emphasizes the critical need for improved policy frameworks, long-term funding, the growth of research capacity, and the updating of BME teaching and learning methodologies. By filling these gaps, stakeholders will be able to promote long-term sectoral growth and inclusive innovation, which will ultimately align clinical practice, technological advancement, and societal demands in SSA and other low- and middle-income settings.
Keywords: biomedical engineering education, bibliometric analysis, Sub-Saharan Africa, healthcare technology innovation, smart prostheses
Introduction
Global Evolution of Biomedical Engineering
The concept of Biomedical Engineering (BME) had its roots in the early attempts to use tools and scientific expertise in medicine, but it was formally established in the middle of the last century, when the development of electronics, materials science and computing changed the nature of healthcare.1–5 The need of prostheses, monitoring systems and life-support technologies, generated after World War II, stimulated the emergence of specialized university courses and professional associations. Medical imaging (CT, MRI, PET), implantation devices, tissue engineering, and medical robotics were medical breakthroughs in subsequent decades.6–20
Medicine Genomics, nanotechnology, digital health, artificial intelligence, and additive manufacturing have transformed BME in the twenty-first century.21–32 The 3D-printed implants, smart prosthetics, organ-on-chip, and AI-driven diagnostics are some of the innovations that indicate a transition to data-driven, individualized, and minimally invasive care.33,34 The world has now turned to BME to modernize health care, especially in the process of meeting the needs of the ageing populations, chronic diseases and the need to produce technologies that are accessible and cost effective.35,36 Although the field is solidly established in high-income nations, the establishment of the field is still lopsided in low- and middle-income (LMI) countries, including Sub-Saharan Africa (SSA), wherein program structures, research ecosystems, and regulatory frameworks continue to develop.33–36
Importance of BME for Healthcare Innovation in SSA
BME has a lot of potential in making healthcare systems stronger in SSA by having a locally relevant innovation.37,38 The area experiences high burdens of infectious diseases, maternal and child health issues, trauma and there is an alarmingly rising prevalence of non-communicable diseases.39–41 Solutions that are engineered like point-of-care diagnostics, portable imaging systems, telemedicine systems, solar-powered medical devices, and affordable prosthetics can enhance service delivery in resource-constrained settings.42
On top of that leading to the development of devices, BME has a role to play in clinical engineering capacity, such as installation, maintenance, and lifecycle management of medical equipment, in which many facilities have found a challenge with non-functional infrastructure.43–45 Remote monitoring and early disease detection are also provided by digital health, AI-diagnostics, and mobile technologies.46–49
Further development is, however, curtailed by disjointed training platforms, inadequate laboratory facilities, unreliable regulatory frameworks, ineffective university-industry networks, and inadequate commercialization services.50–55 Nevertheless, with these limitations, there is an increasing interest in digital health, local production, innovation centre, and biotechnology policies, so BME might be not only a contributor to health care provision but also to the workforce and economic diversification.56–68
Scope of Biomedical Engineering
BME is multidisciplinary by nature, which combines engineering, physical sciences, computing, and life sciences to tackle the problem of diagnosing, treating, and rehabilitating. Bioinstrumentation, biomaterials, biomechanics, medical imaging, clinical engineering, bioinformatics, systems physiology, telehealth and regulatory science are the core subfields.69–74
Biomedical engineers work in various hospitals, research centre, medical device companies and pharmaceutical groups around the world. It is a research intensive and translational field that involves high levels of cooperation among academia, clinical setup, and industries to develop innovations on laboratories into clinical solutions.75–77
Biomedical engineers are also in demand in SSA as the healthcare systems attempt to enhance performance, diagnostic capacity, and therapeutic outcomes of equipment used. Nonetheless, the educational system and research performance differ greatly in countries. Figure 1 below presents the key issues in BME.78–86 This number demonstrates the BME multidisciplinary nature by showing the essence and emerging sub-fields, including bioinstrumentation, biomaterials, biomechanics, tissue engineering, medical imaging, and digital health.87–91 It helps identify the purpose of the study as it gives background on the thematic areas that are evaluated throughout the bibliometric and systematic review of BME education and research in Sub-Saharan Africa.92,93
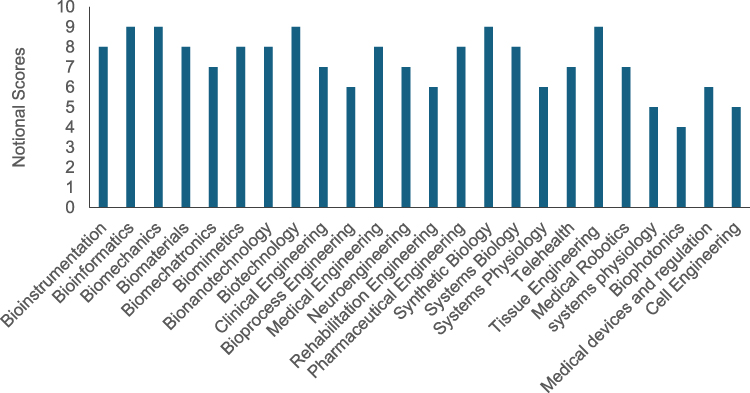 |
Figure 1 BME Subject Area. |
Conceptual Framework and Research Gap
The development of BME in SSA can be understood through the interaction of three interconnected dimensions:
- Healthcare demand: high disease burdens requiring affordable and context-sensitive technologies.94–98
- Technological innovation: development of reliable, cost-effective devices and digital solutions.99–102
- Capacity-building systems: education, research infrastructure, regulation, and industry partnerships.103–105
The successful incorporation of these dimensions is what can and will decide whether BME can positively empower health systems. Conceptual discourses on BME in Africa are growing, however there are still big gaps in the empirical evidence.106–108 Published research tends to concentrate on the isolated technology or the prototype, and little assessment has been performed with regards to long-term clinical implications, sustainability, or even commercialization prospects.109–112 Moreover, little research has been done in terms of systematic evidence mapping productivity of research, thematic development, institutional contribution, and network of collaborations throughout SSA. In comparison to other LMIC regions of the world, including elements of South Asia and Latin America, where bibliometric measures and other organized innovation systems are more well-developed, SSA does not feature any in-depth mapping research that examines not only the educational systems, but also the research output in BME. The BME growth in SSA is hampered by inadequate infrastructure, lack of funds and uneven research capacity, despite the increasing interest. There are also distinct differences in program allocation, research partnerships, and fit to local healthcare priorities in SSA.112–118 Such lack of organized evidence inhibits strategic investment, harmonization of curricula and alignment of regional policies and it was found necessary to map out BME education and research in the region.119,120
Rationale for Bibliometric and Systematic Assessment
Although BME education has expanded across SSA during the last 20 years, curricula vary widely in terms of structure, specialization, and alignment with national health priorities.121–123 Although many institutions concentrate on the foundations of engineering, they do not offer advanced laboratory access, organized clinical experience, or expertise in high-impact sectors such as medical imaging, biomaterials, or digital health. The substantial variations in national policy and regulatory frameworks have an impact on medical device approval processes and professional certification.124,125 By identifying structural gaps, understudied topics, and chances for curricular reform and strategic investment, mapping goes beyond descriptive statistics. A combined bibliometric and systematic approach provides an evidence-based means of evaluating:
- Research productivity trends and growth patterns126–135
- Thematic focus areas and emerging technologies136–138
- Institutional and regional research distribution136–139
- Collaboration networks and interdisciplinarity136–139
- Alignment between research output and regional healthcare priorities136–139
Scope and Objectives of the Review
This research aims to map biomedical engineering research and education in Sub-Saharan Africa using a combination of bibliometric and systematic analytics. This study adds systematic evidence to support long-term healthcare innovation planning in SSA, research prioritization, capacity-building tactics, and curriculum creation by offering a thorough regional assessment.
It aims to:
- Quantify the growth and distribution of BME research across SSA.
- Identify dominant and emerging research themes and technologies.
- Analyze institutional productivity and collaboration networks.
- Examine alignment between educational programs, research output, and regional healthcare needs.
- Emphasize strategic paths for policy development, innovative ecosystems, and BME capacity enhancement.
Methodology of the Bibliometric Assessment
Databases and Search Strategy
Three key databases Scopus, Web of Science (WoS Core Collection) and PubMed were used to carry out a structured bibliometric analysis of Biomedical Engineering (BME) research in Sub-Saharan Africa (SSA). The reason behind the selection of these databases is that they are widely covered in terms of peer-reviewed engineering, medical and interdisciplinary research.
The search method was a combination of controlled vocabulary and free-text terms with Boolean operators (AND, OR). The main disciplinary terms were:
Bioengineering OR Biomedical Engineering OR Medical Engineering OR Healthcare Technology or Clinical Engineering or Tissue Engineering. These were joined with geographical identifiers such as: Sub-Saharan Africa OR country names of the SSA countries.
The search was narrowed down to 2000 to 2025 because of the modern trends. To ensure inclusion of peer-reviewed journal articles, review papers, conference proceedings, and book chapters only were considered. News articles, letters, commentary articles and editorials were omitted. The original dataset had 154, 981 records before the screening and refinement.
Inclusion-Exclusion Criteria
To ensure relevance and geographic specificity, studies were included if they:
- Focused on BME subfields (eg., medical devices, biomaterials, clinical engineering, health technologies, biomedical education).
- Had at least one author affiliated with an SSA institution or explicitly addressed healthcare or technological challenges within SSA.
- Were published in English within the defined study period.
Studies were excluded if they:
- Lacked an engineering component (purely biological or clinical without technological integration),
- Were non-research publications (editorials, letters, commentaries),
- Contained incomplete bibliographic data,
- Were not indexed in the selected databases.
This screening ensured a geographically and thematically focused dataset representative of BME research and educational trends in SSA.
Bibliometric Indicators and Analytical Tools
This study adds organized evidence to support long-term healthcare innovation planning in SSA, research prioritization, capacity-building tactics, and curriculum creation by offering a thorough regional assessment.
Performance Indicators:
I. Annual publication growth trends
II. Total publications and institutional productivity
III. Country contributions
IV. Total citations, average citations per paper
V. h-index
Science Mapping Indicators:
I. Co-authorship networks (institutional and international collaboration)
II. Co-citation networks
III. Keyword co-occurrence analysis
IV. Thematic clustering and evolution
V. Burst detection to identify emerging research frontiers
Three specialized tools were used:
I. CiteSpace for identifying citation bursts, intellectual turning points, and research frontiers.
II. Bibliometrix (R package) for quantitative performance analysis and thematic evolution.
III. VOSviewer for visualizing co-authorship, co-citation, and keyword networks.
Integration of Bibliometric and Systematic Review Approaches
As the bibliometric analysis gives a quantitative measure of the trends of publications, citation impact, collaboration networks and thematic development, the systematic review element offers the qualitative insight and contextual interpretation. Namely, evidence regarding the structure of the curriculum, policy frameworks, implementation issues, regulatory contexts, and innovation systems are systematically reviewed in SSA. In contrast to bibliometric techniques where trends and research interests are discovered, the systematic review analyzes the material, applicability and usefulness of chosen studies. It is the combination of these two approaches that thus make it possible to evaluate more thoroughly- a structural mapping of the scientific production and a contextual evaluation of the developmental processes of education and healthcare innovation possibilities in the area.
Limitations
There are a few methodological issues with this study. First, research published in local or non-indexed African publications may be underrepresented because the bibliometric study was limited to Scopus, Web of Science, and PubMed. Second, there may have been linguistic prejudice because only English-language publications were considered. Third, older publications and internationally collaborative work may be favoured by bibliometric metrics like citation counts and h-index, undervaluing new or regionally focused research.
Additionally, keyword-based search strategies may not capture all relevant interdisciplinary studies, particularly those not explicitly labelled under “biomedical engineering.” Variations in institutional naming conventions and incomplete metadata may also influence affiliation-based analysis. While the systematic review provides qualitative insights, interpretation of thematic content may involve some degree of subjectivity despite the use of predefined inclusion criteria. These limitations should be considered when interpreting the findings and their implications for regional policy and strategic planning.
Research Output Trends in BME in SSA
Annual Publication Trends
Web of Science, Scopus, and PubMed was searched thoroughly for papers from 2000 to 2025 using the key phrases “BME” and its synonyms in SSA. For analysis, bibliometric data such as titles, authors, journals, abstracts, and references were exported in CSV and RIS formats. Beaudry and Mouton140 agree that over the past 20 years, BME research in SSA has continuously increased, according to annual publication patterns. Due to limited institutional capability, inadequate research funding, and emerging BME programs, early contributions were restricted. Nonetheless, the creation of postgraduate programs, research teams, and BME departments progressively increased academic production. Multidisciplinary research in digital health, point-of-care diagnostics, biomaterials, and custom medical device creation has been a major driver of recent growth. Increased international cooperation, better funding, and improved research infrastructure have all contributed to this expansion. The increasing publishing trends show a growing regional commitment to using BME to address local healthcare issues as well as a developing research ecosystem.
Contribution by Different Categories for BME Globally
A search on Scopus for “BME practiced worldwide” turned 131,771 publications, illustrating the interdisciplinary and rapidly growing subject of BME. Figures 2–8, which display the distribution of these publications by year, authorship, sources, countries, document types, subject areas, and funding sponsors, provide a comprehensive picture of worldwide research activity. The high citation counts of these works attest to their important contributions to scientific advancement, influence on healthcare policy, and support of sustainability and global health goals. Citation performance demonstrates the applicability and significance of BME developments as a measure of the calibre and significance of research.141 This strong scholarly engagement, which has attracted continued interest from scholars, decision-makers, and commercial stakeholders, further demonstrates the field’s global relevance.
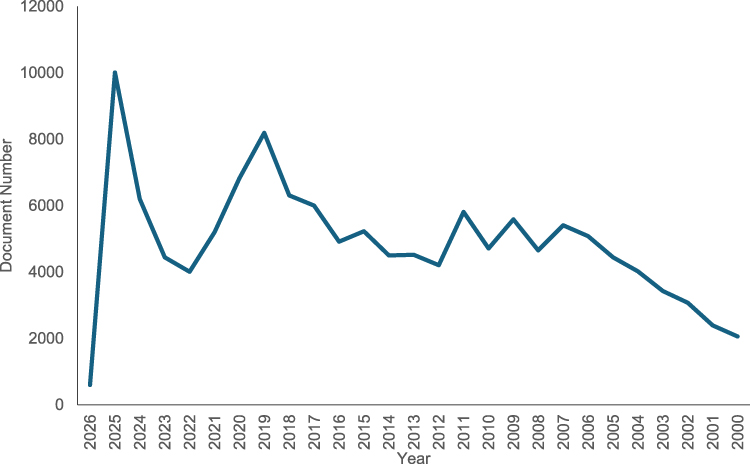 |
Figure 2 Document by year for BME. |
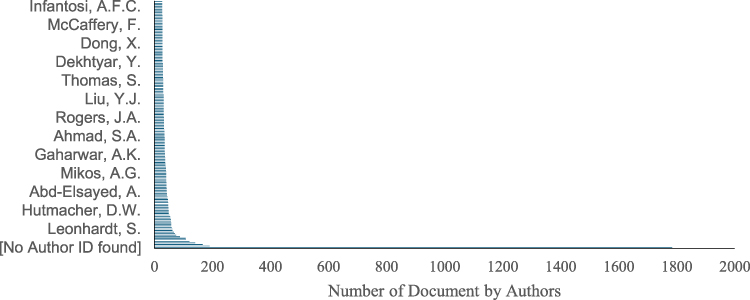 |
Figure 3 Distribution of Documents by Authors in Global BME Practice. |
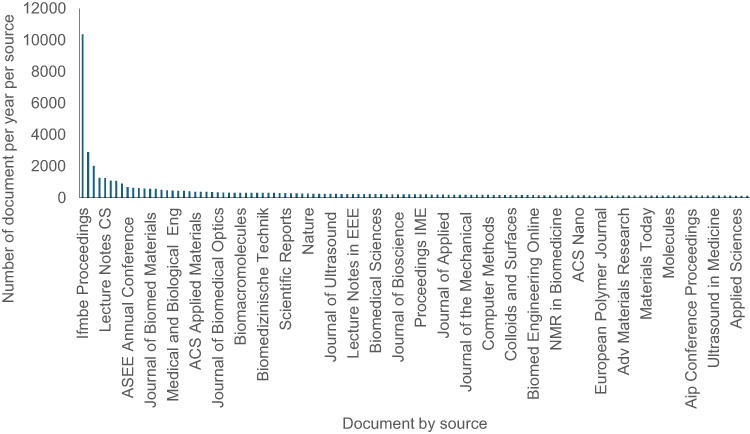 |
Figure 4 Document per year per source. |
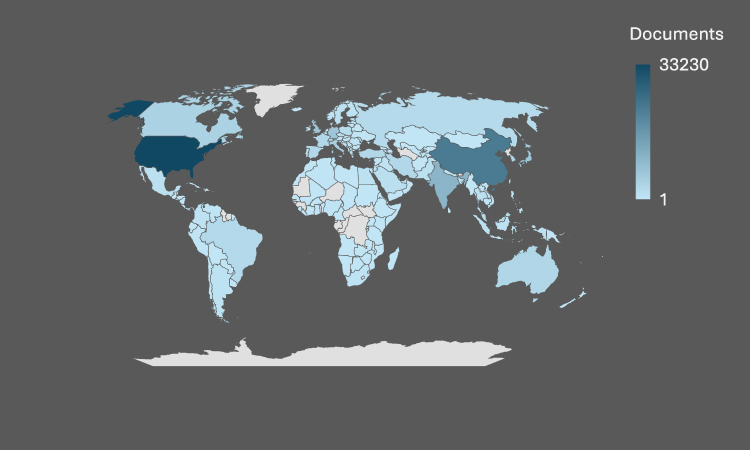 |
Figure 5 Document by Countries. |
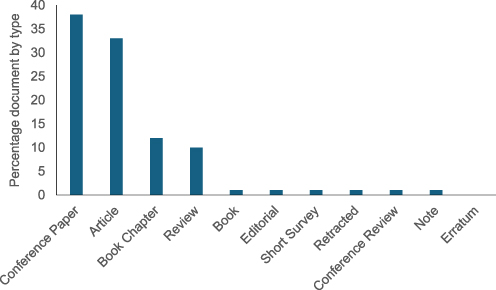 |
Figure 6 Document by type. |
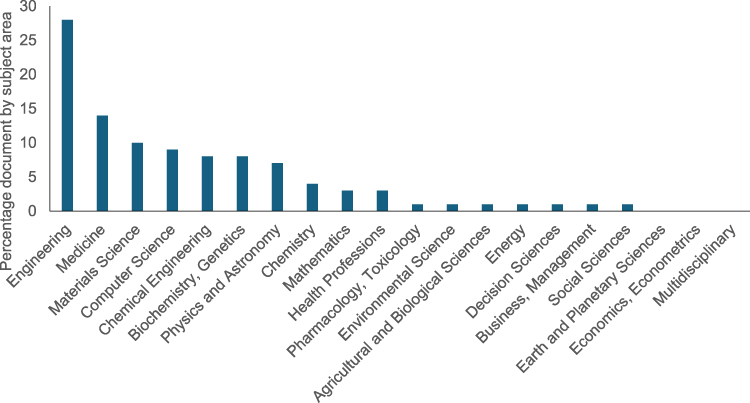 |
Figure 7 Document by subject Area. |
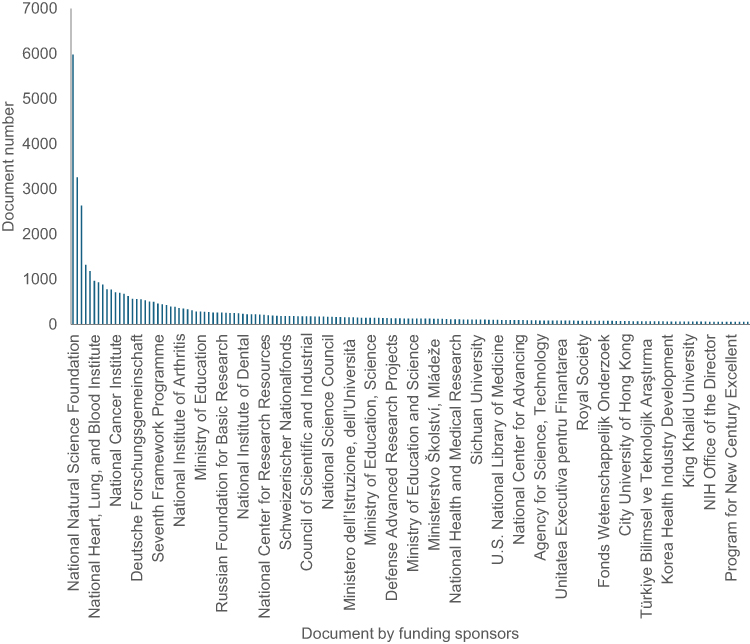 |
Figure 8 Document by funding sponsors. |
The annual publishing trends in BME research show notable shifts over time from Figure 2. The steady rise in output between 2000 and 2007 demonstrates the early development of modern BME and the increasing recognition of its significance in healthcare innovation, particularly in biomaterials, medical devices, and diagnostic technologies. The COVID-19 pandemic caused disruptions to international collaboration, laboratory access, and research funding, which led to a sharp decline in publication output after 2019.142 Despite this setback, BME research recovered and peaked in 2025. As seen by recent growth, the industry has swiftly adopted cutting-edge technology such as artificial intelligence (AI), machine learning (ML), artificial neural networks (ANNs), and data-driven healthcare solutions.
Figure 4 shows that the number of authors per document rarely surpasses 200, regardless of the substantial volume of publications overall. This pattern reflects the highly technical and specialized nature of BME research, where dogged proficiency is imperative, in contrast to several other scientific disciplines with big, concerted teams. Despite the moderate team size, these specialist teams’ high research productivity contributes to large production.
Geographically, the United States leads the globe in BME research production, closely followed by China, thanks to its well-established departments, robust research infrastructure, and steady financing. Growing investments in healthcare technology and technical education are making India a major contributor. Nonetheless, BME research production remains low in Argentina, Brazil, and African countries, highlighting the urgent need for funding, capacity building, and the establishment of specialized BME programs. Supporting local research ecosystems would allow for context-specific solutions to regional healthcare problems in addition to improving global fairness.143
As seen in Figure 6, the most prominent documents in this field of study are “conference papers,” “articles,” and “book chapters.”
The study of prosthesis design, biomaterials, medical devices, and implant technologies, which rely on a solid engineering basis and collaboration with the computer science endeavour, is visible in a large portion of literature on BME, which is applicable to the field of engineering, such as chemical engineering, materials science, and general engineering (Figure 7). The highly multidisciplinary nature of BME, in which the different disciplinary perceptions come together to promote healthcare innovation, is further illuminated by the input of non-engineering disciplines, including life sciences, medicine, physics, and social sciences.
Funding patterns according to which most of financial aid is provided by China and the United States (Figure 8) indicate the importance of regular investment in the further development of high-impact biomedical research. Advanced infrastructure, interdisciplinary cooperation, and research continuity are made possible by strong funding.144 BME is a convergent field that integrates knowledge, methods, and resources from other disciplines to address complex healthcare concerns, as further demonstrated by the multidisciplinary linkages shown in Figure 9. Figure 9 displays the co-occurrence of terms because of the search. The keywords’ co-occurrence suggests that this specific research issue is broad and spans multiple fields, especially given its significance to the continent and the entire world.
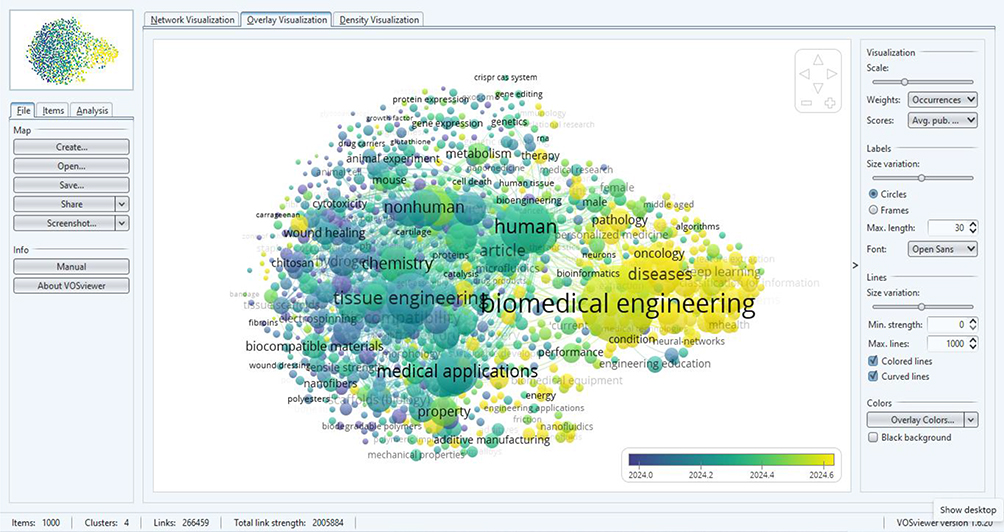 |
Figure 9 Co-occurrence of keywords linked to BME. |
Contribution by Different Categories for BME in SSA (Scopus)
SSA’s BME research output shows notable geographical differences as well as new areas of interest.145 With South Africa, Nigeria, Kenya, Uganda, and Zambia producing most publications, productivity is concentrated in a small number of nations (Figure 10). Due to its robust institutions, specialized laboratories, well-developed research infrastructure, steady funding for science, technology, and health research, and deep integration into international research networks all of which improve output and international visibility South Africa leads by a significant margin.
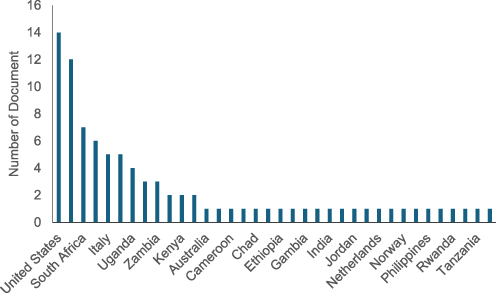 |
Figure 10 Document by Country. |
BME research in SSA is concentrated in a few important countries, with South Africa, Nigeria, and Kenya generating most publications, due to growing universities, increasing postgraduate enrolment in engineering programs, and more donor-supported activities, this aligns with the findings of Agbeyangi & Lukose.146 The examples of the emerging contributors are Ethiopia, Tanzania, Cameroon, and Chad, which illustrate the results of regional efforts, capacity-building initiatives, and more readily available access to foreign investment (Figure 10). Even with such developments total regional cooperation remains low as compared to world leaders such as the US and the UK, highlighting continued problems with finance, laboratory facilities, skilled workforce, and industry-academia engagement. To enhance cross-border collaboration, research facilities, and training, regional plans need to be synchronized.
The outcome of research is highly influenced by funding. Tropical Health and Education Trust (THET) are the most common sponsors (Figure 11) with regular investment in health research and health capacity building. The United States and the United Kingdom continue to be the most leading sources of funding globally and they offer access to state of the art facilities, interdisciplinary skills as well as international networks that elevate the level, scope and publicity of research. Personal researcher leadership, as indicated by Pecchia (Figures 12 and 13) highlights the significance of ongoing academic participation, although institutional affiliation has less predictive value of influencing research, demonstrating BME research as having a network basis. BME study in the region is greatly multidisciplinary. Engineering dominates the fields particularly in energy systems, medical devices, biomaterials, and prosthetics. Healthcare innovation, workforce development, policymaking, and technology management are supported by intersections with life sciences, medicine, and computer science. In line with worldwide trends in diagnostics and intelligent healthcare devices, thematic and chronological analyses (Figures 14–16) show a growing integration of emerging technologies, such as artificial intelligence, machine learning, and data-driven medical solutions. International partnerships have greatly improved research quality, exposure, and methodological rigor, especially with the US, UK, Australia, and India (Figures 17–24).
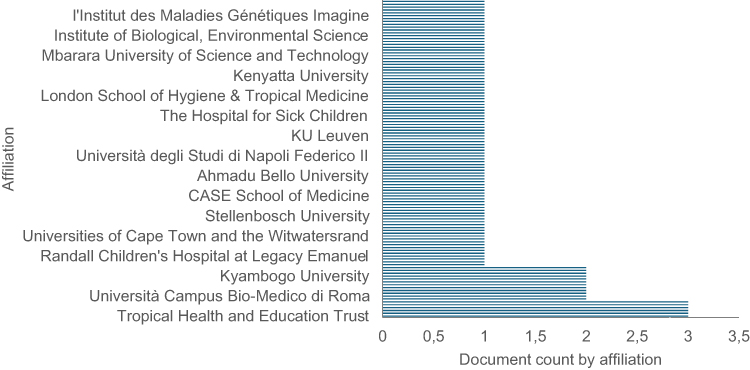 |
Figure 11 Document count by affiliation. |
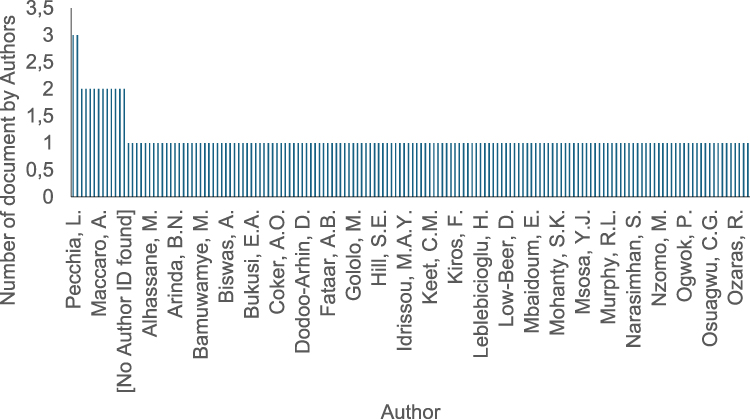 |
Figure 12 Document by Authors. |
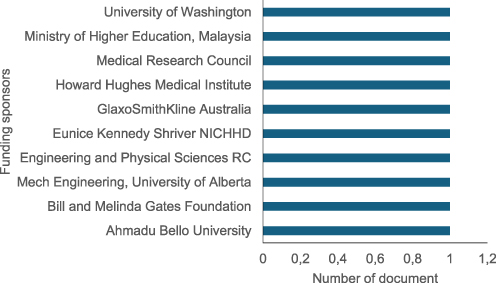 |
Figure 13 Document by funding. |
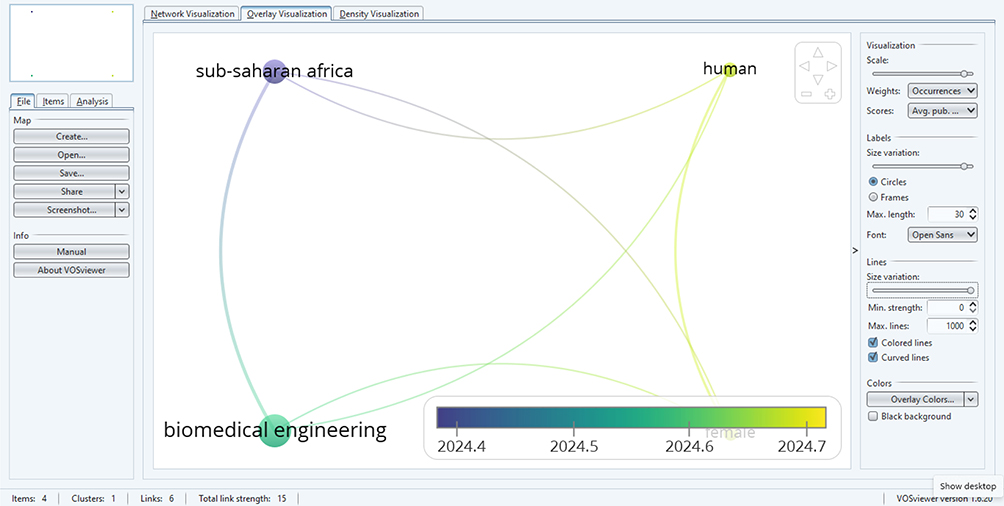 |
Figure 14 BME in SSA. |
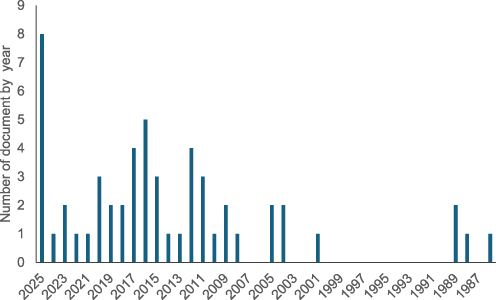 |
Figure 15 Document by year. |
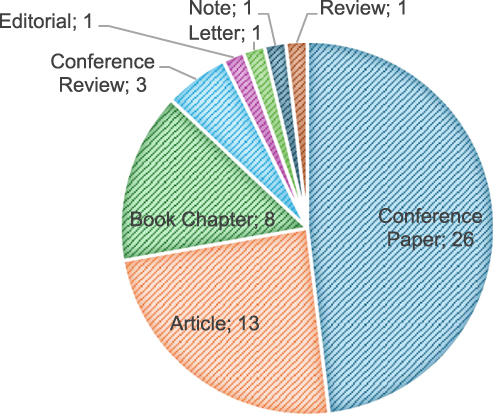 |
Figure 16 Document by type. |
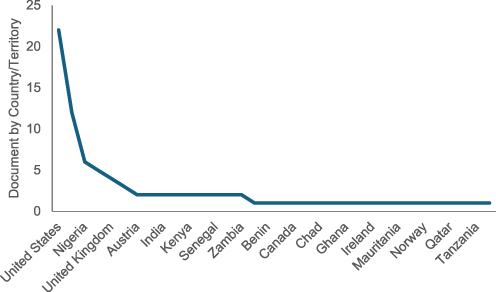 |
Figure 17 Document by country. |
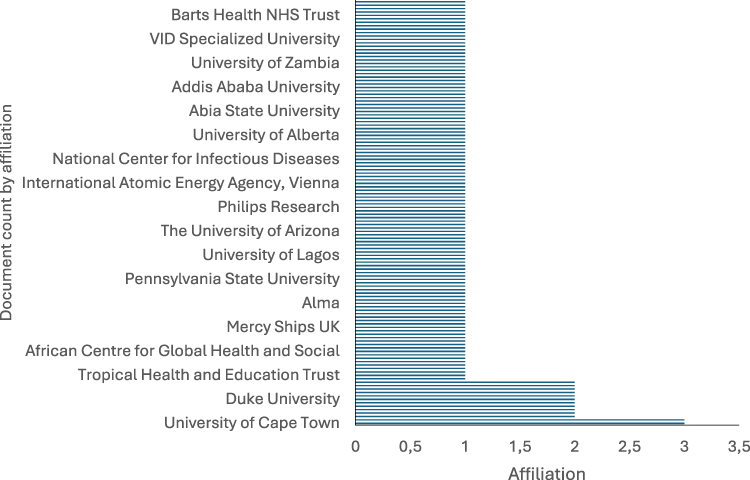 |
Figure 18 Document by affiliation. |
 |
Figure 19 Document by funding sponsor. |
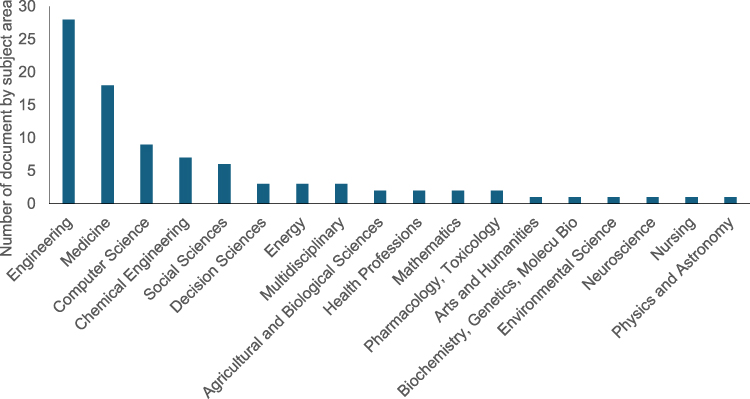 |
Figure 20 Document by subject area. |
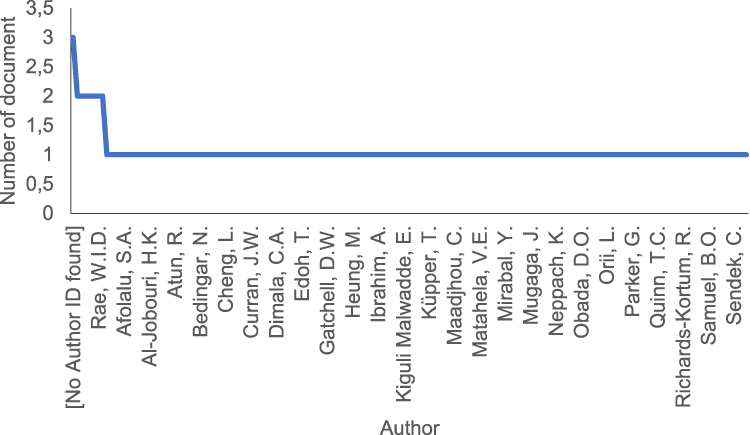 |
Figure 21 Document by Author. |
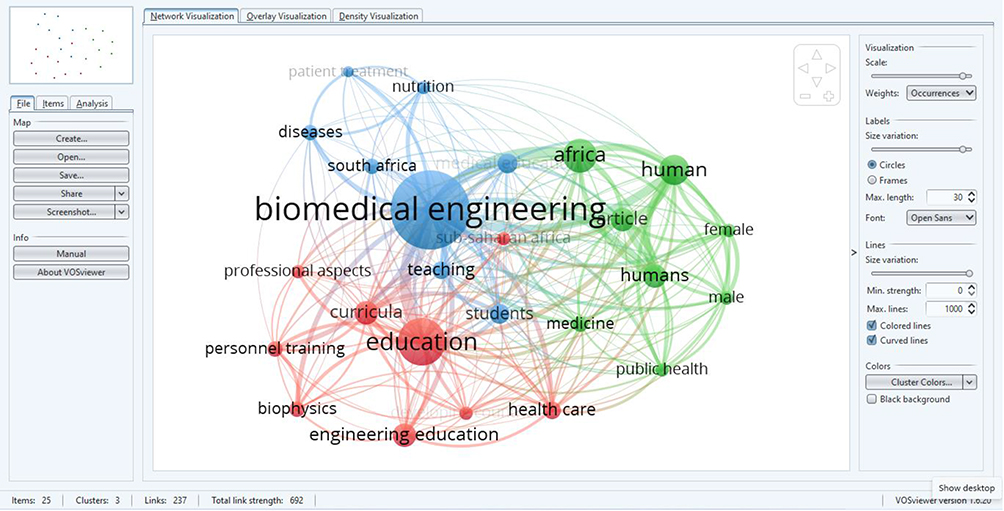 |
Figure 22 BME Education in Africa Based on Scopus Data. |
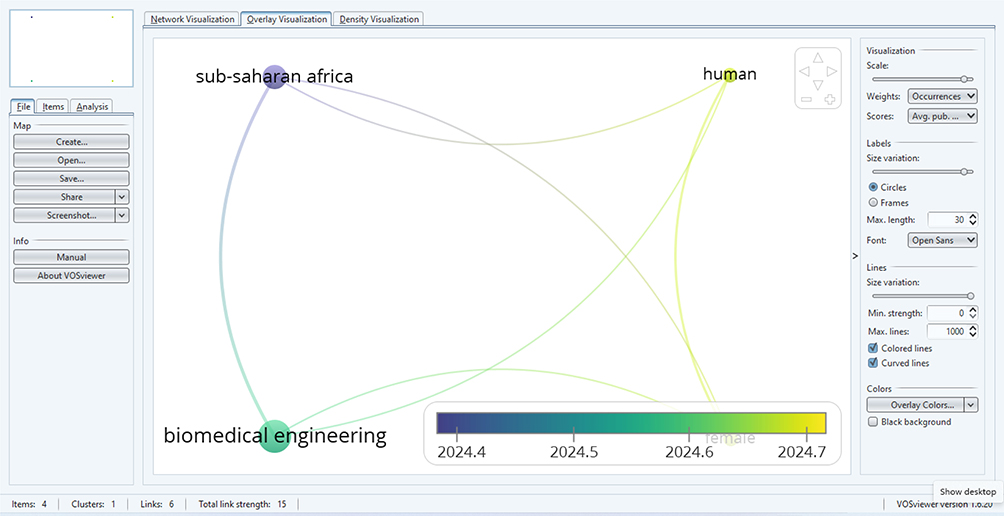 |
Figure 23 BME Education in SSA Based on Scopus Data. |
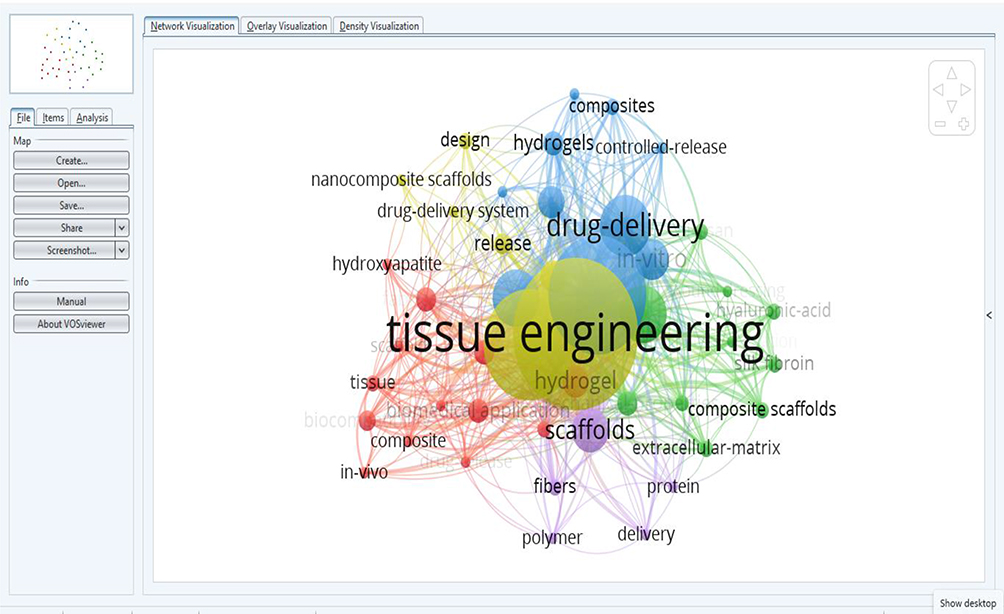 |
Figure 24 Link among education, BME and other subdivisions. |
Education remains a key component of the BME ecology. Links between biomedical education, BME programs, and tissue engineering training encourage long-term growth in research, innovation, and healthcare application throughout SSA.147
Web of Science Account of BME Document by Different Categories
Upon initially searching the Web of Science (WOS) database with the term “BME,” 34,899 entries were found. The search results of WOS are narrowly matched as the search strategy is focused, whereas Scopus uses synonyms and other related words automatically. The search was then furthered to 477,725 records of the WOS Core Collection to be able to cover more relevant keywords and phrases. This expanded dataset reflects the complexity and the variety of BME which incorporates biotechnology, biomaterials, medical devices, bioinformatics, clinical engineering, and healthcare systems. The results show the importance of paying close attention to the specificity versus breadth of bibliometric searches: although larger queries are needed to fully capture research activity in a rapidly emerging and interdisciplinary field, narrower searches increase accuracy (Figure 25).
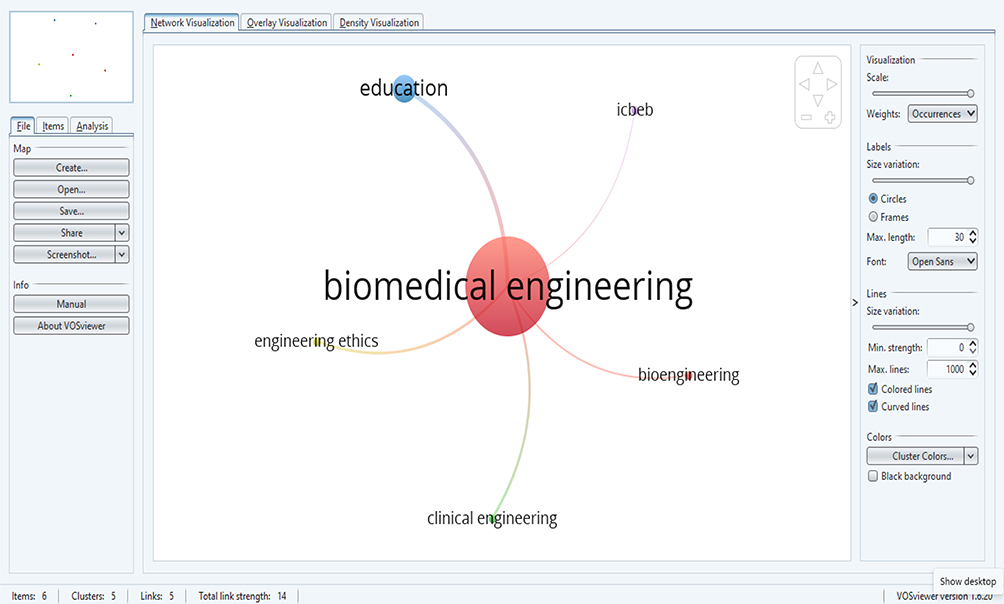 |
Figure 25 BME search. |
BME in Africa
Only two papers were discovered when the keyword “BME” was only typed in the Web of Science Core Collection, demonstrating the database’s dependence on exact search terms rather than assumed subject expansion. A more thorough dataset with 182,304 records was generated by inserting extra applicable keywords. This large upsurge highlights the value of cautiously choosing and merging keywords in bibliometric analyses. It also exhibits the scope and cross disciplinary nature of BME research, which embraces a wide range of subjects and may be understated by overly limited or unstructured search strategies.
There are very different citation patterns in the BME literature due to a small number of works with disproportionately high citations (Figure 26). The direction of research and regional health goals have been impacted by these widely referenced articles, which are frequently on basic subjects like BME, biotechnology, and policy-relevant studies on healthcare, capacity building, and innovation in SSA.148 As theoretical frameworks, methodological guidelines, or empirical evidence that other researchers commonly utilize, their citation intensity demonstrates their intellectual importance. High citation counts also show how important this research is to politicians, medical professionals, and other stakeholders looking for evidence-based solutions for urgent biomedical and public health issues. Using terms like “health technology education,” “Africa,” “Sub-Saharan Africa,” and “medical engineering,” an extensive bibliometric search centred on BME education yielded 396,054 documents from the Web of Science Core Collection (Figure 27). The vast expansion of biomedical and health technology education in SSA is reflected in this wide and multidisciplinary body of work, which covers engineering, medical sciences, pedagogy, policy, and capacity building. To adequately capture the range of scholarly output in biological education and training, these findings emphasize the significance of well-crafted keyword combinations. Only 20,000 of the 131,623 papers that were obtained from Scopus could be exported in RIS format for additional analysis because of Scopus export restrictions. Figure 28 displays bibliometric maps and visualizations of these entries created by VOSviewer. The organization and focus of the area are revealed by these visualizations, which highlight the relationships, structure, and thematic distribution of research in BME education.
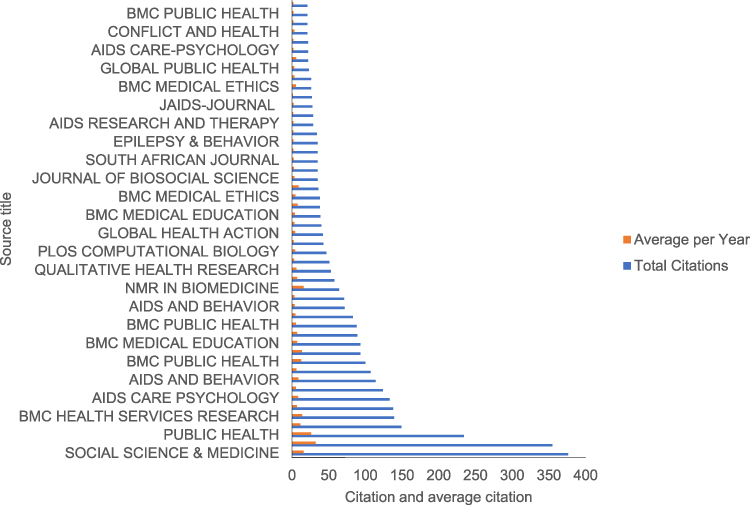 |
Figure 26 Source title Citation and average citation per year. |
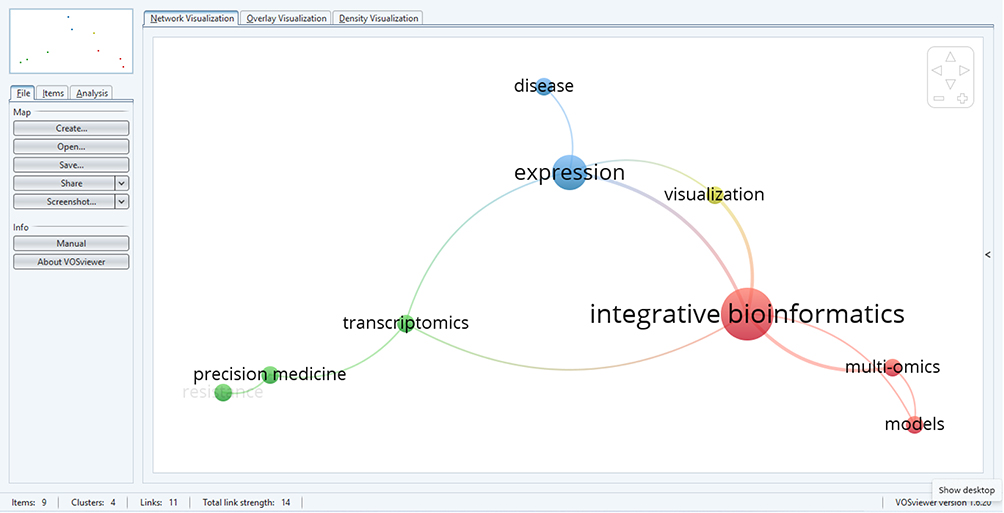 |
Figure 27 BME in Africa with added keywords. |
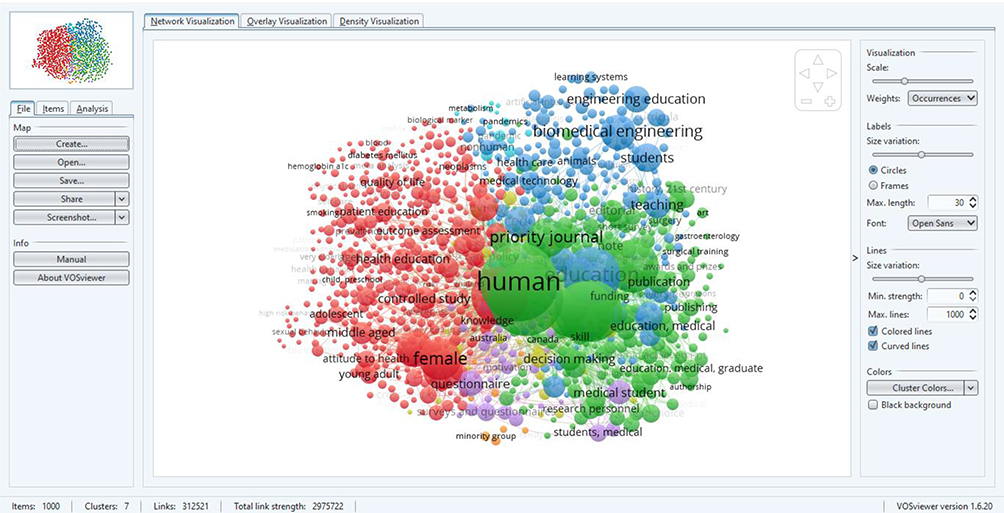 |
Figure 28 BME education and added keywords. |
Results of Bibliometric Data Extraction and Network Visualization
The PubMed search on the topic BME in the period between 2000 and 2025 returned 370,601 results, which proves that it is a multidisciplinary sphere. The automatic addition of relevant terms in PubMed allowed a huge amount of data, however, it can be exported in a 10,000 filler. The data were organized by Zotero and were exported in the RIS file to be analyzed by bibliometrics, and the four targeted subject areas were worldwide BME, BME in Africa, BME education in Africa, and BME education in SSA. A network and co-occurrence analysis with VOSviewer show thematic groups, relationships and intellectual organizations (Figures 29–32) stronger conceptual or citation relationships are also marked by physical proximity.
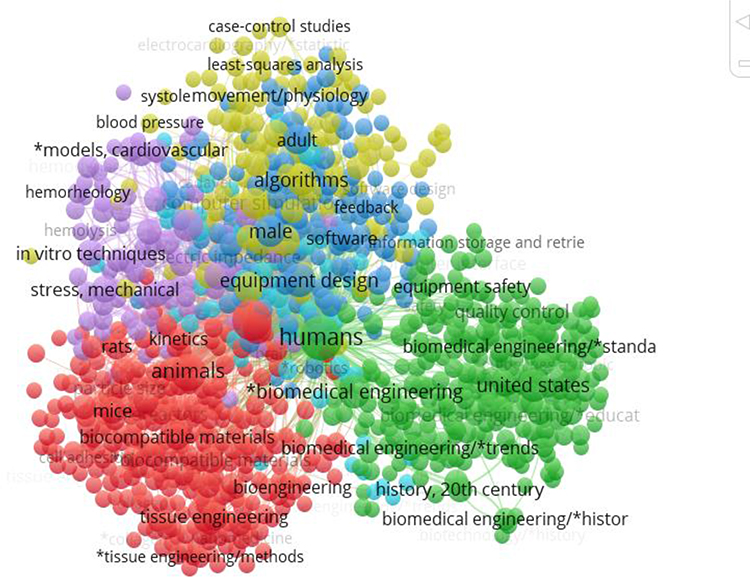 |
Figure 29 BME globally. |
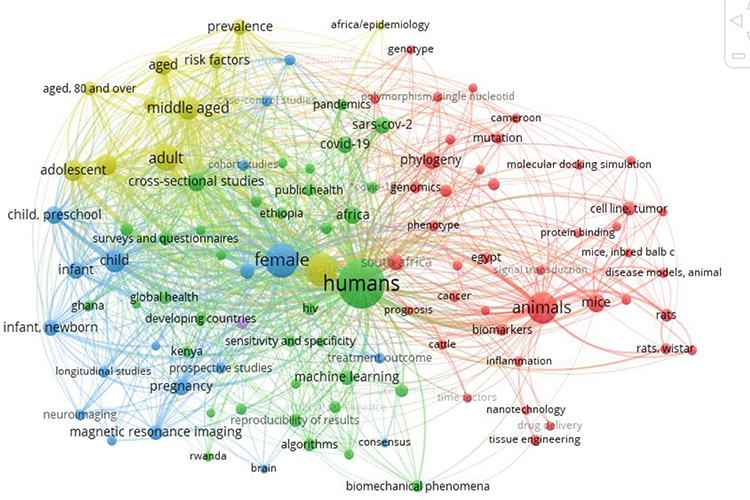 |
Figure 30 BME in Africa. |
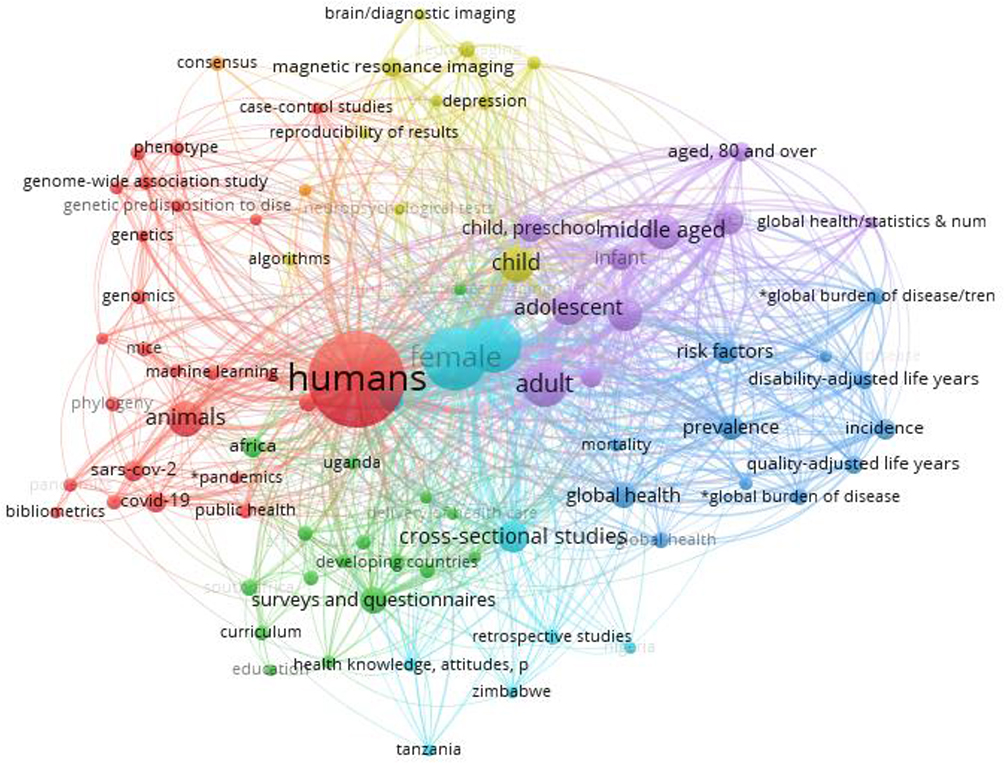 |
Figure 31 BME Education in Africa Based on PubMed Data. |
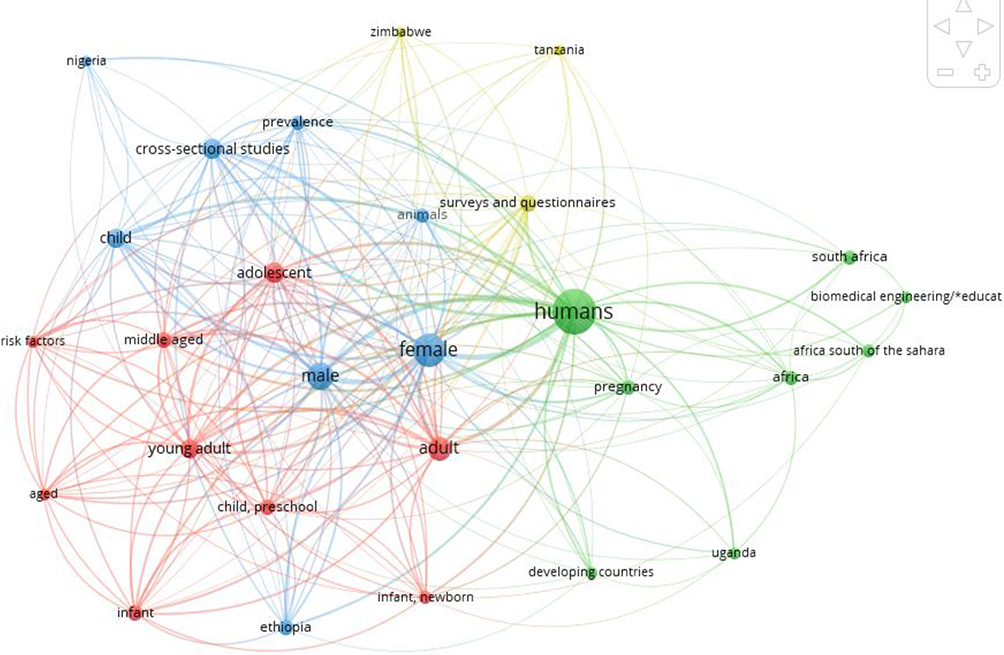 |
Figure 32 BME education in SSA. |
The search only found two articles as the SSA was used, but when Africa was searched in general, 2,333 articles were found; 435 records were found in BME education in Africa, and 102 in SSA. This paucity underscores such long-standing problems as bad funding, ragged institutional structures, lack of postgraduate training, and indexing of regional research. The low visibility of work in the regions negatively affects evidence-based policymaking, contributing to the need to be more dependent on foreign technologies and prevent the translation of biological progress into healthcare.143
The findings confirm that shared policy actions are immediately needed to expand research capacity, standardize BME education, and foster regional and global cooperation. The strategic investments to enhance the competitiveness of industries and free movement of labour should encompass specialized finance, centres of excellence equipped with state-of-the art laboratories and prototyping units, regulatory support, and standardized education.149 Making more visible, more productive and creative research can be done by fostering international and intra-African partnerships via co-supervised postgraduate research, mobility, and joint funding. Scholars, business, and health care institutions should work together to transform research into locally produced medical innovations, reduce dependency on imported goods, and enhance healthcare delivery. Such actions are essential for establishing sustainable innovation ecosystems and presenting SSA as an active participant in international BME research.
Thematic Research Areas in BME Within the SSA Region
A broad but uneven distribution of research interests influenced by regional healthcare demands and infrastructure constraints is revealed by a thematic analysis of BME research in SSA. Biomedical signal and image processing, medical equipment, biomaterials and prostheses, healthcare systems, and clinical engineering are some of the leading fields. The pressing need for resource-sensitive, context-appropriate healthcare solutions is the main driving force behind these sectors. New research directions are rapidly being influenced by emerging technologies like machine learning, artificial intelligence, and data-driven healthcare. Despite being less organized, digital health, telemedicine, and mobile health have grown quickly, reflecting issues with workforce, access, and geography.
Disability and post-trauma care are addressed under resource restrictions through research in assistive technology and rehabilitation engineering, such as inexpensive prostheses and orthotic devices. However, high-tech fields such as bioinformatics, tissue engineering, robotics, and smart prosthetics remain ignored due to poor financing, insufficient lab facilities, and dearth of crossdisciplinary partnership. There is also a dearth of research on policy and education, with professional practice, accreditation, and curriculum creation. This suggests a mismatch between academic training, industry demands, and healthcare priorities. There are still plenty of chances to go into high-impact, technology-intensive fields even with the heavy focus on applied, problem-driven innovation. To close theme gaps, promote BME research and education, and enhance healthcare outcomes in the area, targeted funding, capacity building, and supporting policies are crucial (Figure 33).
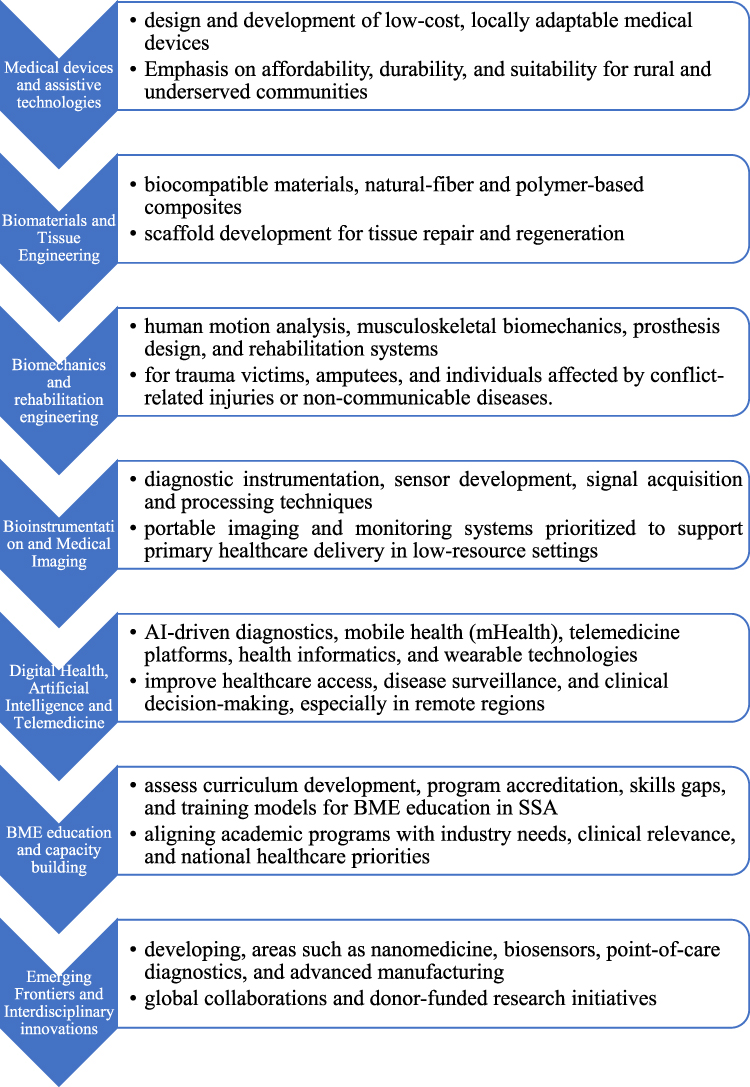 |
Figure 33 Thematic Research Areas in BME. |
The distribution and connections of BME research in SSA are highlighted in the thematic map, which also identifies gaps and strengths. Biomaterials and prosthetics, biomedical signal and image processing, medical devices, healthcare systems, and clinical engineering are examples of prominent clusters that concentrate on applied and need-driven research. AI, machine learning, digital health, telemedicine, and mobile health technologies are gradually being integrated into emerging clusters.150 On the other hand, policy and educational research including professional practice, curriculum development, and BME training is hardly represented, and advanced subjects like robotics, bioinformatics, tissue engineering, and intelligent prosthetic systems are still developing.
Accessibility, affordability, and contextual fit are given top priority in medical device and assistive technology research, which focuses on low-cost diagnostic, rehabilitative, prosthetic, and orthotic solutions. These inventions are loosely connected to intelligent, AI-enabled systems, even though they serve local needs relating to trauma, handicap, and resource constraints. The creation of prosthetics and medical devices is aided by biomaterials research, but tissue engineering and regenerative therapies are underrepresented because of multidisciplinary, budgetary, and infrastructure limitations. Additive manufacturing, biofabrication, and regenerative technologies present opportunities to grow these fields.
Cost-effective diagnostic tools and signal processing for radiology, cardiology, and point-of-care applications are the main topics of bioinstrumentation and imaging research. Nevertheless, there are still few links to multimodal imaging, wearable sensors, and AI-based picture analysis. Similar to this, biomechanics and rehabilitation engineering deal with low-cost rehabilitation devices, musculoskeletal modeling, and gait analysis; nevertheless, robotics-assisted therapy, predictive modeling, and AI-based motion tracking are understudied. With a focus on data-driven healthcare, remote monitoring, and decision support systems, BME and IT research prioritizes telemedicine, digital health, and AI-enabled care. Implementation is hampered by inadequate infrastructure, a lack of finance, and skills vacuum despite growing expansion. Wearable sensors, nanomedicine, lab-on-a-chip technologies, smart implants, and nanoscale drug delivery systems are examples of high-impact but underrepresented fields. These developments have the potential to revolutionize healthcare delivery, remote monitoring, and tailored medication, but they also call for skill development, interdisciplinary cooperation, and strategic investment. With significant opportunities in high-tech, data-driven, and transdisciplinary research sectors that might satisfy regional healthcare needs, the theme analysis reveals a highly applied, problem-driven, but unevenly developed BME environment in SSA.151
BME Education and Curriculum Landscape
Overview of BME Academic Programs in SSA
The experience of SSA over the last 20 years suggests that there has been a consistent increase in the number of BME courses in the region that may be attributed to the growing awareness of the importance of the field in enhancing healthcare and advancing local innovation.152,153 Undergraduate courses in BME or other related programs such as medical or clinical engineering are now offered as well as advanced courses such as master and doctoral courses focusing on medical devices, biomaterials and health care technology management. The diverse nature of the industry makes it extremely important that programs specifically identify potential career paths and areas of concentration in which the graduate can work. Nevertheless, many programs are hampered by the lack of finance, and this results in a lack of experience in staff, lack of laboratory equipment and a lack of curriculum.
Other formal BME education programs have been instituted in several countries such as South Africa, Nigeria, Kenya, and Ghana. Such courses usually blend basic engineering knowledge with biological and medical sciences. Working with clinical facilities, laboratory activity and practical and project-based learning are often mentioned. Nevertheless, these developments do not mean that there are no significant disparities between schools in duration of programs, curriculum content, certification procedures, and research incorporation, which points out variations in funding, academic capability, and resource. Lack of proper funding of research and innovation, outdated infrastructure, ineffective collaboration between industries and universities, and unskilled employees further hinder development.
Some of the emerging technologies that tend to be underrepresented in the curriculum are wearable technology, digital health platforms, and AI-enabled systems. This would graduate graduates ill equipped to take up the latest BME jobs. However, there is some local effort at developing a qualified manpower that can generate low-cost prosthetics, rehabilitation equipment, and a long-lasting medical machinery. To add capacity to BME, improve graduate skills and promote locally relevant innovation in health care, it would be required to strengthen educational programs by adding funding, developing international partnerships, training the faculty and revising curricula.
Figure 34 shows the geographic distribution and development of BME programs in SSA, providing crucial information about the current state of education in the area. BME initiatives are concentrated in a small number of countries, particularly South Africa, Ghana, Nigeria, and Kenya. The most well-established programs, which often offer both undergraduate and graduate degrees, are found in these countries. Due to the higher investments in infrastructures and research capacities as well as faculty availability, these countries are regional centre of education in BME. Nonetheless, the majority of other SSA countries (marked with light grey) have limited or no official BME programs.
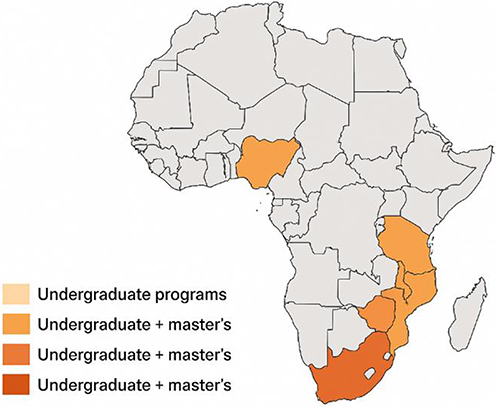 |
Figure 34 Distribution of BME academic programs in SSA. |
Inequality in access to specialized engineering training exists globally, which is a sign of more severe issues including lack of funding, shortage of skilled workforce, and the lack of institutional readiness to undertake BME curriculum. The expansion of the program is region-based; the transition of the program to master and doctoral degree programs is expressed by darker orange and red colours. The absence of post-graduate education funding also limits the opportunities to conduct research, advance knowledge, and become innovative.
In Southern and West Africa BME education is common compared to Central and some parts of East Africa because of the prospects of economic development, government policies, financing of higher education and foreign academic engagement. The map emphasizes the need to allocate funds to specific areas, to work together as a region, and to develop capacity to spread knowledge of BME education across SSA. It also outlines the prospects of initiating or expanding projects in developing countries, which may be critical in solving the problems faced by the region in terms of healthcare and the advancement of medical equipment, prostheses, diagnostics, and healthcare technologies. In general, the graph shows the existence of both systematic gaps and significant potential of development and fair promotion of BME education across the region.
Curriculum Structure and Comparison with Global Benchmarks
Most BME programs in SSA employ integrated curricula that incorporate foundational engineering sciences with biological and medical training. Essential subjects typically include mathematics, physics, programming, circuits, mechanics, materials science, anatomy, physiology, and preliminary BME topics. Many programs also comprise industrial training or capstone projects to offer partial practical experience.
Compared with globally benchmarked curricula affiliated with ABET, EUR-ACE, and foremost BME programs in North America, Europe, and Asia, considerable variations persist. International programs combine biology and engineering design beforehand, offer massive laboratory and prototyping experiences, highlight clinical immersion, and uphold strong industry engagement. Contrariwise, many SSA programs remain centred on traditional engineering content, with limited biomedical laboratory access, medical device prototyping, and structured clinical exposure.
Globally accredited curricula progressively accentuate crossdisciplinarity and evolving areas such as biomedical imaging, biomaterials, biomechanics and rehabilitation engineering, tissue engineering, bioinstrumentation, artificial intelligence in healthcare, digital health, regulatory science, and medical device standards. While some SSA programs comprise elements of these topics often as electives their depth, consistency, and specialization are constrained, and advanced tracks or modular curricular flexibility are mainly lacking.
Affiliation with frameworks for quality assurance and accreditation is another significant difference. Outcome-based education with clearly specified graduate traits, such as problem-solving, ethical responsibility, teamwork, communication, and lifelong learning, is commonly used in internationally certified programs. Despite the emergence of outcome-based approaches in SSA, their implementation is still inconsistent because of resource constraints and differences in country accrediting systems.
Despite these shortcomings, SSA BME initiatives demonstrate high contextual significance by emphasizing locally appropriate healthcare solutions, such as appropriate medical devices and technologies for contexts with low resources. This problem-driven approach gives SSA programs a strategic opportunity to establish a distinctive international reputation and supports the global precedent for socially responsive engineering education. Graduate competency, mobility, and global effectiveness would increase if the remaining obstacles were addressed through curriculum modernization, faculty development, international alliances, and cooperation with global benchmarks. A comparison of ABET-aligned programs with standard SSA BME curriculum is provided in Table 1.
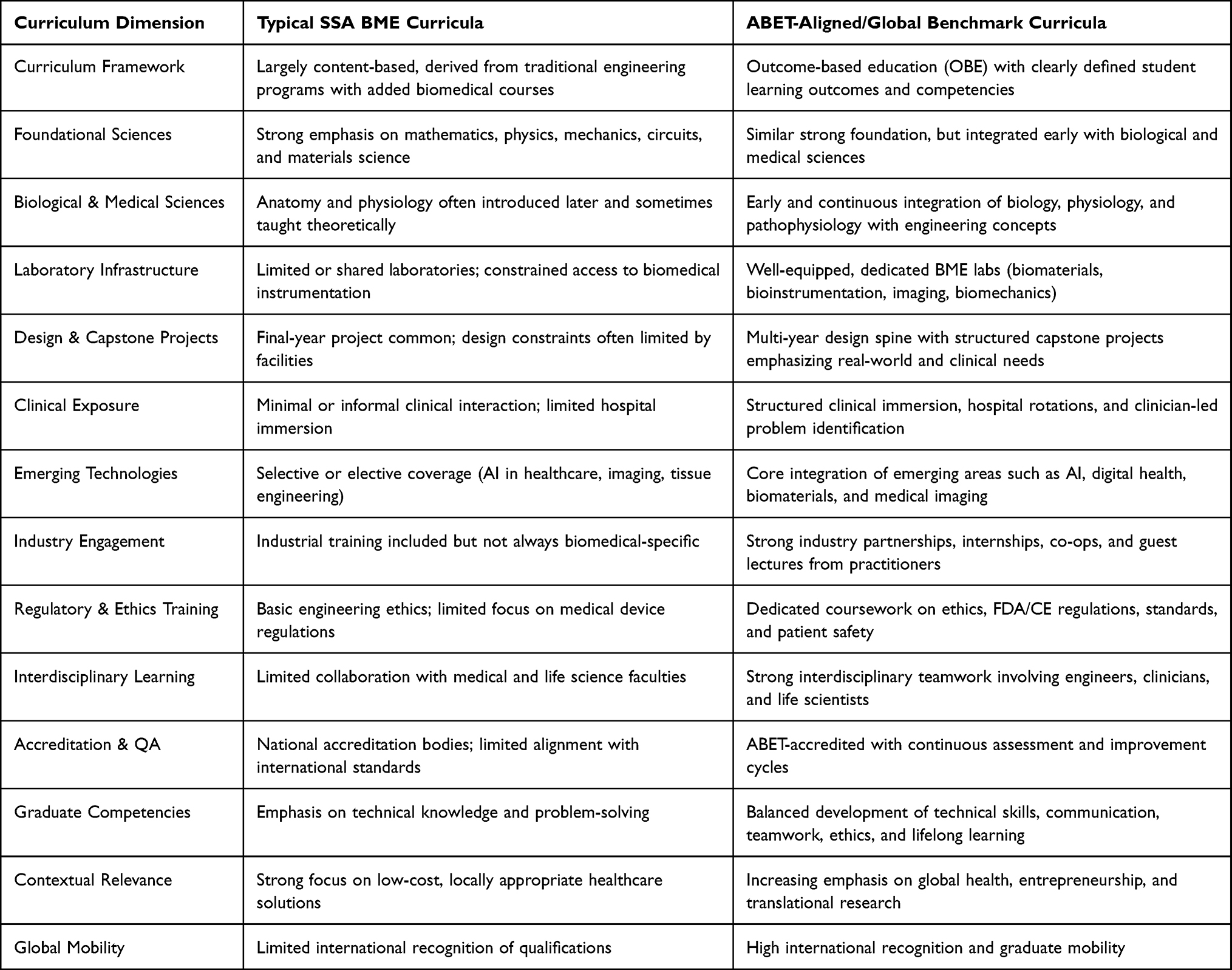 |
Table 1 Comparative Table Contrasting Typical BME and Curricula in SSA with ABET-Aligned BME Curricula |
Significant shortcomings persist even though the majority of SSA BME programs are affiliated with ABET-accredited core engineering science courses. These have been insufficiency of exposure to new biomedical technology, laboratory and prototyping facilities, inconsistency in the certification process, inadequacy of outcome-based education implementation, and clinical integration. Simultaneously, the focus on the locally related, resource-adjusted healthcare solutions constitutes another strength of SSA programs. This contextual advantage may be exploited to enhance the quality and impact of programs with targeted curriculum modernization, capacity building and closer association with international standards of accreditation. Table 2 is framed from a policy and accreditation viewpoint to guide funding agencies, accrediting bodies, and policymakers. Rather than serving only as an academic comparison, it detects important gaps, systemic risks, and important intervention areas needed to improve BME education in SSA and advance alignment with global standards.
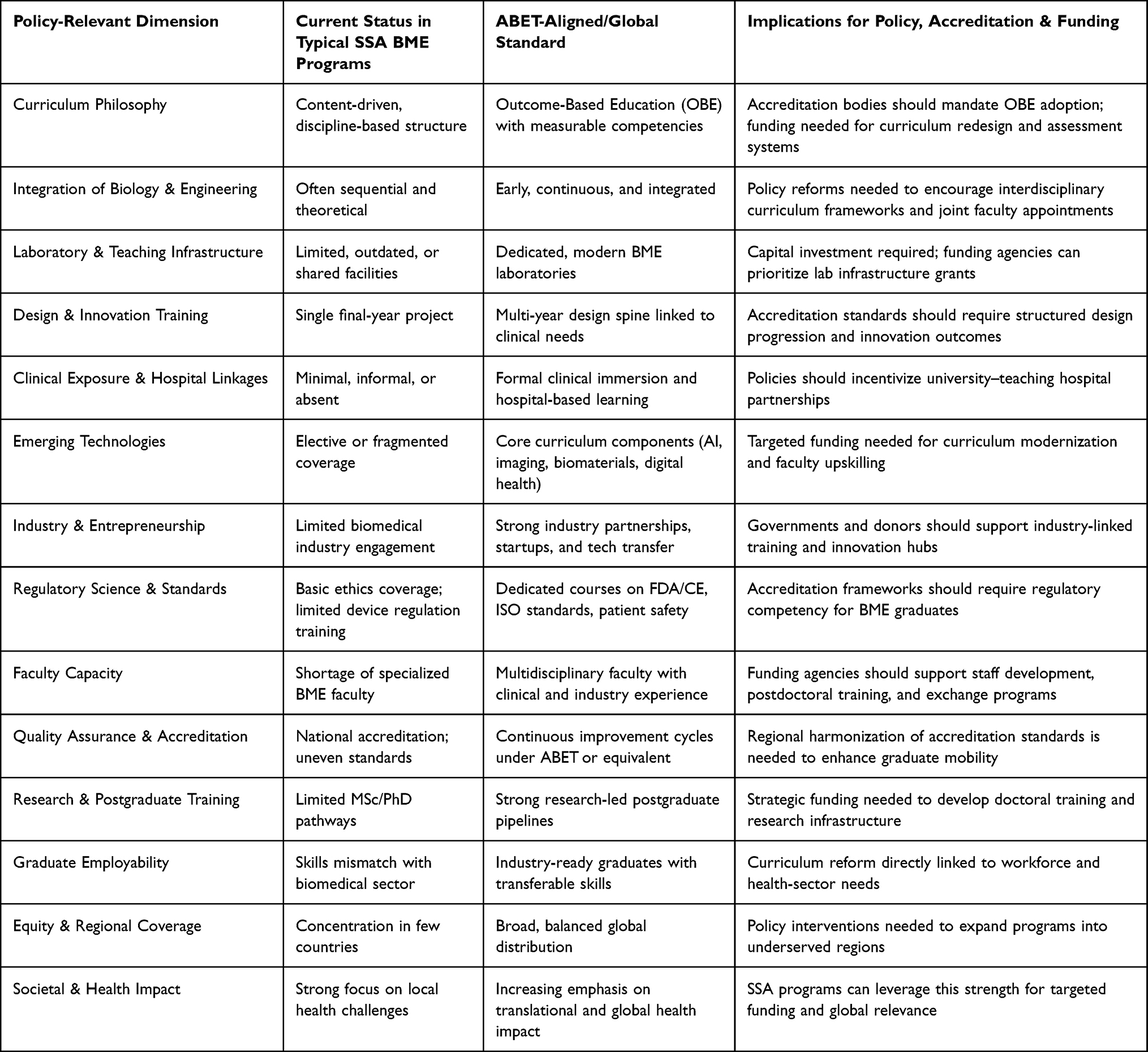 |
Table 2 Policy-Oriented and Accreditation Focused to Funding Support |
Policymakers should prioritize consistent national and regional BME education strategies that support healthcare requests with industrial development, while consolidating university–hospital–industry collaboration through focused policy and funding mechanisms. Developing BME programs beyond current regional hubs is vital. Accreditation bodies should increasingly support national standards with international outcome-based frameworks such as ABET, highlighting noticeable proficiencies in design, clinical relevance, ethics, and regulatory alertness, and sustaining continuous development through external benchmarking.
Funding agencies and development partners should intentionally finance faculty development, postgraduate training, laboratory and prototyping infrastructure, and curriculum modernization that incorporates promising technologies and digital health. Support for pilot centres of excellence is crucial to serve as regional hubs for BME education, research, and innovation. While SSA BME programs show strong contextual significance, operational misalignment with global accreditation standards continues. Workforce preparedness, healthcare innovation, and technology independence would all be significantly improved by focused investment in outcome-based curriculum, infrastructure, faculty capacity, and clinical integration. To support accreditation evaluations, policy creation, and funding justification, Table 3 connects SSA BME curricula to ABET Student Outcomes (1–7).
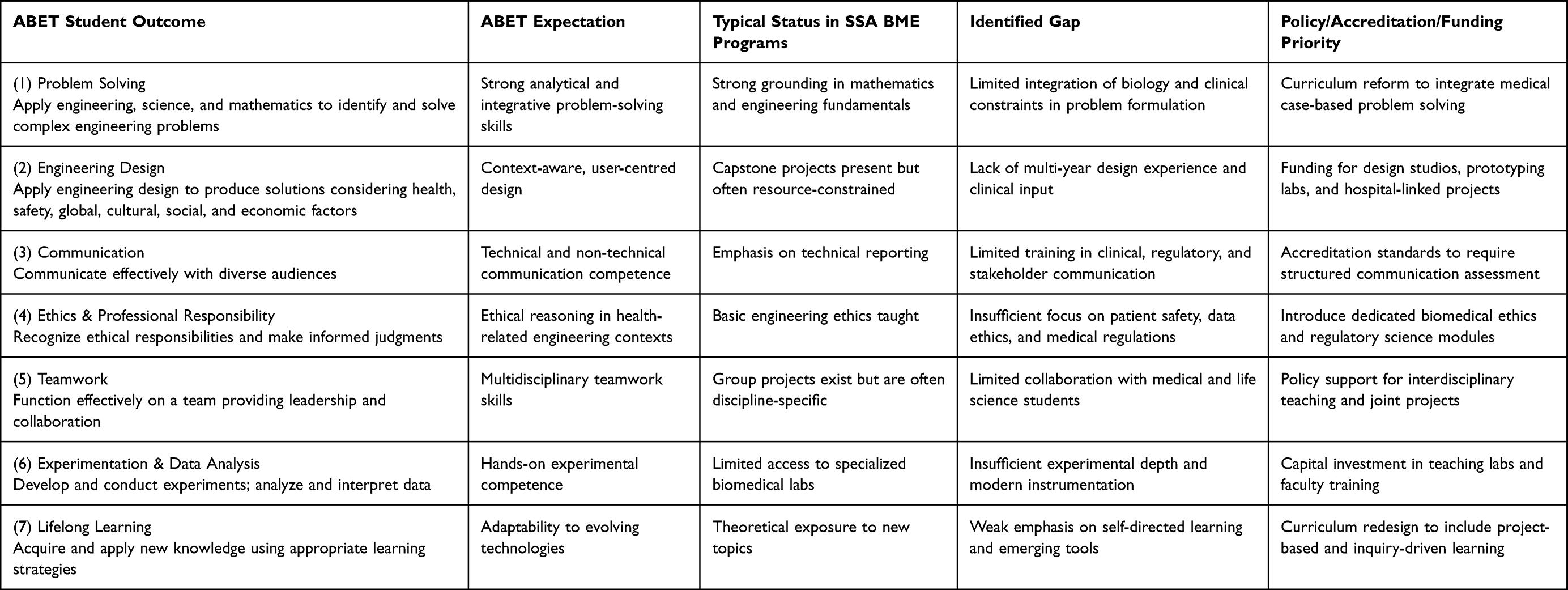 |
Table 3 Mapping of SSA BME Curricula with ABET Student Outcomes |
For accreditation organizations in SSA, ABET Student Outcomes (1–7) offer a useful benchmarking framework to direct phased alignment, especially in enhancing design capability, clinical relevance, and continuous improvement. By incorporating outcome-based education into national engineering standards and providing incentives for university-hospital collaboration to foster the development of design, teamwork, and experimental abilities, policymakers can facilitate this process. The support of laboratory infrastructure, faculty training, and international collaborations that promote design, experimentation, ethics, and lifelong learning should be highlighted by funding agencies. By resolving the long-standing gaps in design thinking, experimental expertise, moral accountability, and flexibility, the systematic compatibility with ABET objectives would promote graduate employment and accreditation readiness.
Most BME programs in SSA are accepted at the national level but not very in line with the international systems such as ABET, EUR-ACE, or the Washington Accord. These programs are yet to be formally accredited on different levels. External audit and internal quality assurance are not always effectively conducted to gauge laboratory capacity, clinical integration, and research participation. Some of the significant gaps in accreditation are poor laboratory and clinical infrastructure, insufficient interdisciplinary faculty, weak implementation of outcome-based education, limited exposure to international ethical and regulatory standards as well as weakly institutionalized processes of continuous improvement. Competency-based evaluation, focused investments in faculty and infrastructure, improved clinical relationships, regional accreditation cooperation, and methodical tracking of student outcomes, employability, and research performance can all help close these disparities. To create globally competitive graduates, ensure the safety of medical technology developed in a specific area and region, focus financial resources, and build regional facilities of excellence in sustainable BME education and innovation in SSA, accreditation and quality assurance is required.154
Accreditation Status and Quality Assurance
The national level approval of BME programs in SSA is primarily done through engineering councils or higher education organizations and the programs are being at varying levels of formal accreditation.155,156 Even though national accreditation ensures that academic standards at the lowest level are met, it often fails to align with international models that put greater emphasis on outcome-based learning, competency assessment, and constant enhancement like ABET, EUR-ACE, or Washington Accord. The number of institutions that want to get partial international recognition has been limited depending on the level of funds, level of regulations and development of programs.155–157
Even though they are in place, there is not always the use of internal quality assurance procedures such as program committees, curriculum reviews, and student feedback. In external audits of agencies conducted by the national agencies, laboratory capacity, clinical integration, research capabilities, and interdisciplinary collaboration is not always adequately evaluated. Some of the key drawbacks include limited practice training, absence of interdisciplinary faculty, absence of exposure to global ethical and regulatory standards, and insufficient adoption of outcome-based education in accordance with ABET student outcomes. Such inadequacies restrict the employability, global comparability and mobility of graduates. Besides being in accordance with global standards, the possibilities of improving accreditation are specialized investment in clinical and laboratory centre, faculty, and clinical collaboration. Applicability of the programs and transparency could be enhanced through establishment of quantifiable student outcomes, competency-based assessment, strict monitoring of graduate performance and research publications. Regional cooperation and global alliances are also useful in the process of benchmarking resources sharing and quality alignment. Enhanced accreditation and quality assurance are the key to improving graduate competency, ensuring the safety of medical technology developed locally, developing regional centres of excellence, and enhancing the competitiveness of SSA on the global BME market.158,159
Industry–Academia Linkage in Curriculum Development
For SSA BME programs to address changing healthcare requirements, developing technology, and labour demands, strong industry-academia ties are crucial.160 There are not many partnerships now, and most of the courses are still academic and provide little exposure to biomedical problems, clinical procedures, or device development. As a result, graduates are technically capable but unprepared for positions driven by the industry. By recognizing new skills, technological trends, and regulatory requirements, industry advisory committees can provide guidance for curriculum design. Structured internships, co-ops, and capstone projects with hospitals, research facilities, and biomedical corporations are ways to obtain real-world experience. To promote applied interdisciplinary learning, teachers and industry professionals can collaborate in workshops to jointly build modules in digital health, medical imaging, regulatory compliance, and biomedical data analytics.
These partnerships facilitate the transfer of knowledge: industry gains from competent graduates and research results, while universities gain access to industrial knowledge and equipment. These collaborations can be further strengthened by supportive policies, such as targeted funding, tax breaks, and acknowledgment of industry mentorship. Graduates who participate in these partnerships gain useful skills, regulatory knowledge, and creative abilities that are in line with both local healthcare requirements and international norms, supporting the development of a sustainable biomedical technology ecosystem in SSA.160,161
Identified Gaps in Research, Training and Infrastructure
Research Output Gaps vs Health Priorities in the SSA Region
Although BME research in SSA is expanding, it is still insufficient to address important healthcare issues. Bibliometric analyses reveal deficits in addressing infectious illnesses, maternity and child health, low-cost diagnostics, assistive technology, and healthcare delivery in locations with limited resources, despite an increase in publications on biomaterials, medical devices, and digital health.162,163 Context-relevant research is hampered by structural constraints in clinical and laboratory infrastructure, a lack of professors, and insufficient financing.
There is a gap between findings and workable remedies since many initiatives place more emphasis on international cooperation or academic measures than on local health needs. Translation into workable prototypes and inventions is further hampered by poor industry-academia collaborations and little technology transfer. The emphasis on postgraduate and doctoral programs in a small number of institutions also hinders long-term innovation. To increase societal impact, advance SDG, and strengthen sustainable healthcare systems throughout SSA, strategic investments in applied research infrastructure, capacity building, industry engagement, and technology transfer are essential, as is alignment with national and regional health priorities.164
Skills and Curriculum Gaps
Although basic curricula in SSA BME programs have improved, deficiencies in skills and curriculum design continue to hinder graduate preparation for regional and international biological responsibilities.165,166 While integration of biological sciences, clinical practice, and multidisciplinary problem-solving is frequently minimal, many schools emphasize classic engineering courses like mathematics, physics, mechanics, and materials science. As a result, graduates possess excellent analytical abilities but lack practical experience in clinical procedures, patient care, medical device development, and laboratory experimentation.
Wearable sensors, digital health platforms, medical imaging, telemedicine, regenerative medicine, and AI-driven solutions are examples of emerging healthcare technology that are not always integrated. Some schools provide electives, but they sometimes do not cover enough ground, leaving graduates unprepared for cutting-edge biological advancements. Gaps in lifelong learning, design thinking, regulatory compliance, ethical reasoning, and interdisciplinary teamwork are caused by inconsistent use of outcome-based frameworks that are in line with international standards (such as ABET Student Outcomes).
Employability is further hampered by limited clinical experience, business collaborations, and entrepreneurial training. SSA BME graduates will be equipped with the technical, clinical, and creative skills necessary to address local healthcare issues and make a global impact through the integration of contemporary technologies, organized lab and clinical skills, and clear outcome-based objectives, as well as faculty development and industry collaboration.167
Limited Laboratory, Prototyping and Testing Facilities
Inadequate, well-equipped testing, prototyping, and laboratory facilities are a key obstacle in SSA BME education.168 The infrastructure for biomaterials, bioinstrumentation, biomechanics, medical imaging, and tissue engineering is limited in most institutions, which limits students’ ability to develop practical skills and engage in hands-on learning. Students’ ability to convert ideas like wearable sensors, medical devices, or diagnostic tools into workable solutions is hampered by outdated or shared facilities, which further limit experimentation, prototype creation, and exposure to contemporary biomedical technologies.
The lack of clinical trial sites and hospital-based laboratories further limits experiential learning in patient safety, device usability, regulatory compliance, and clinical processes. These deficiencies lower research productivity, graduation quality, and industry and healthcare workforce preparedness. Strategic investments in cutting-edge lab and prototyping technology, academic capacity building, and solid industry collaborations are all necessary to close these gaps. Increased access to contemporary facilities would encourage creativity, improve hands-on learning, and strengthen the calibre, applicability, and competitiveness of SSA BME programs throughout the region.169
Underfunding and Low Commercialization Capacity
The lack of funding and commercialization opportunities for BME programs in SSA has a detrimental impact on research output and teaching quality. Insufficient funding makes it difficult to set up labs, buy cutting-edge equipment, and hire and train staff, which limits opportunities for hands-on learning in device testing, design, and evaluation. The transformation of research findings and prototypes into useful medical equipment, diagnostics, or healthcare solutions is further restricted by inadequate channels for technology transfer, intellectual property management, and industry participation, leaving many inventions limited to academic settings.170 Governments and development partners must make targeted investments in infrastructure, funds for research, and human resources to address these issues. Research may be transformed into commercially viable products more quickly by establishing innovation hubs, fortifying university-industry ties, and setting up efficient technology transfer offices.170 These measures would boost local healthcare systems, expand access to capital and commercialization opportunities, improve graduate employability, promote contextually applicable medical innovations, and increase the practical impact of BME programs across SSA.
Regulatory and Policy Limitations
Regulations and guidelines have a big impact on what can be taught and learned in biology, medicine, and BME. Students’ comprehension of compliance, safety, and ethical obligations is hampered by SSA’s disjointed, inconsistent, or poorly implemented policies on medical device development, clinical testing, and technology approval. The integration of biomedical, medical, and engineering skills is further hampered by inadequate institutional support for curriculum creation, funding, and university-industry collaboration. Many governments and academic institutions fail to match their programs with business demands or public health concerns, which leads to fragmented curriculum, unequal funding for research, and a lack of incentives for innovation or technology transfer.170,171 Regional variations in licensing, quality assurance, and approval procedures hinder the implementation of global best practices, including as outcome-based education and hospital-based experiential learning, as well as collaboration, benchmarking, and workforce mobility. Clear, enforced standards for medical equipment, focused funding for research and innovation, and universal accrediting processes for biomedical and medical programs are all necessary to close these disparities. Governments, academic institutions, and industry associates must work mutually to expand omission, update curricula, and further joint innovation. Patient safety, biomedical innovation, educational quality, and program alignment with national healthcare regulations and international standards will all advance with better regulatory and policy frameworks.172
Opportunities for Growth and Strategic Development
Strengthening Regional Centres of Excellence
Strategic local hubs can significantly enhance BME education, research, and innovation in SSA by pooling expertise, resources, and facilities at key institutions.173 These hubs reduce the unequal distribution of BME programs in the area by acting as hubs for state-of-the-art training, interdisciplinary collaboration, and excellent research. By pooling their resources, they provide access to state-of-the-art labs, clinical cooperation areas, and prototype facilities that could be challenging for individual universities to maintain. Targeted investments in graduate programs, lab equipment, technology transfer, faculty development, and scholarships are crucial for optimum impact. Hubs can foster business-academia collaboration, offer training tailored to regional healthcare needs, and encourage innovation in medical equipment and digital health.
Additionally, they facilitate curriculum harmonization, cross-institutional collaboration, and benchmarking international standards to enhance the quality, applicability, and global competitiveness of BME education. By promoting research networks, student mobility, and shared infrastructure, local hubs can address educational gaps, boost capacity, and accelerate the translation of results into practical healthcare solutions throughout SSA.173,174
Curriculum Modernization Towards Industry-Ready Skills
To give graduates integrated knowledge and practical abilities for contemporary healthcare, SSA’s BME curricula must be upgraded. Conventional schools emphasize engineering, math, and the fundamental sciences, but they often provide students with minimal exposure to clinical practice, the living sciences, and cutting-edge technologies, making them theoretically strong but practically unprepared.175,176 Modern courses should address topics including digital health, biomedical imaging, tissue engineering, medical device development, regulatory compliance, and entrepreneurship. Outcome-based learning ensures measurable abilities in moral decision-making, teamwork, communication, and project management. Practical experience that links theory to real-world application is provided by clinical rotations, internships, capstone projects, and industrial collaborations. Program relevance is increased and creativity is fostered through ongoing curriculum modifications that consider technological advancements, regulatory changes, and changing healthcare demands in conjunction with partnerships with hospitals, research institutes, and enterprises.176,177 In addition to producing graduates who are technically proficient, adaptable, and capable of managing local and international healthcare issues, these reforms help the region establish a sustainable biomedical technology ecosystem.
Leveraging Additive Manufacturing, AI, and Low-Cost Medical Device Innovation
SSA is still plagued by health problems, including a lack of medical supplies, a dependence on expensive foreign technologies, and a lack of capability for local production. BME schools may reduce these gaps by integrating affordable medical device design, artificial intelligence, and 3D printing into research, teaching, and prototyping. 3D printing reduces dependency on imports by enabling the rapid and local production of lab equipment, surgical models, prosthetics, and diagnostic instruments.178 AI enables improved diagnosis, predictive care, individualized treatment planning, and remote patient monitoring, especially in areas with limited resources. Students gain the practical skills required to develop safe, affordable, and context-appropriate medical solutions by incorporating these technologies into their curriculum. Collaboration with businesses, governmental organizations, and healthcare facilities enhances innovation, usability, and compliance even more. In general, AI, 3D printing, and low-cost device development into SSA BME programs enhances worker readiness, healthcare delivery, and local innovation capacity.
Funding, Partnerships and Collaborative Research Networks
Sufficient funding, collaboration, and active research networks are necessary for BME to progress in SSA.179 Financial constraints continue to limit investments in labs, modern technology, teacher development, graduate training, and student experiential learning. Governments, development partners, and businesses must provide focused support in order to enhance infrastructure, promote applied research, and transform results into practical healthcare solutions.180 Internships, clinical experience, prototype possibilities, and research alignment with national health priorities are made possible by strategic partnerships between universities, hospitals, businesses, and governmental organizations. Cooperative local and international research networks enhance knowledge sharing, interdisciplinary projects, and the development of technologies such as digital health solutions, low-cost medical equipment, and 3D-printed healthcare items. SSA BME programs may promote innovation, make research a reality, and provide graduates with the skills necessary to solve regional and global health issues by combining funding, cooperation, and coordinated research activities.
Public–Private Partnership Opportunities
By using corresponding means and knowledge, governments, academic institutions, and businesses can launch planned partnerships that could greatly progress BME in SSA. Industry contributes technological know-how, regulatory expertise, and innovative talent; however, governments and universities frequently face challenges related to funding, laboratory infrastructure, faculty development, and clinical training opportunities.181 Judiciously thought-out partnerships can fund internships, laboratory and prototyping resources, and curriculum development, giving students real-world, employable proficiencies. These group efforts also encourage invention and practical research in fields like digital health, 3D printing, and reasonable medical products that meet regional prerequisites. Technology transfer and commercialization are expedited by industry input, which assures that research and educational programs are aligned with healthcare primacies and market anticipations. Besides supporting skill development and augmenting resource usage, regional cooperation through shared centre of excellence, standard rules, and cross-border deals speeds up the training of competent biomedical engineers. These partnerships can increase the calibre, pertinency, and social effect of BME education and research through the region by fusing government, academic, and business undertakings.182,183
Expanding BME Entrepreneurship and Commercialization Pathways
BME programs in SSA must incorporate entrepreneurship and technology transfer market into their curricula to convert research into practical healthcare results.184 These days, many programs place more importance on academic achievement than financial literacy, which curbs students’ capability to start and manage medical technology businesses. Through training in financial acquirement, intellectual property supervision, regulatory compliance, and business expansion, graduates gain needed entrepreneurial capacities. Creating technology transfer offices in enterprises can help with commercialization by safeguarding inventions, boosting the creation of start-ups, and linking researchers with investors. Additionally, government-industry partnerships and business incubators provide firsthand medical businesses coaching, start-ups capital, and regulatory assistance.185–187 The local biomedical industry can profit from policies like tax exceptions, financial inducements, and furthered product endorsement measures. Consolidating these commercialization avenues inspires the making of sensibly priced, locally made medical apparatus, minimizes dependence on imports, reassures regional innovation, and creates employment and economic development.
Policy Recommendations
National and Regional Policy Directions
Coherent national and regional policies are the future of BME in SSA education and innovation. To promote the collaboration between industry and universities, national governments need to establish BME programs that would not violate the needs of healthcare on the region and international standards. To translate research into practical solutions there must be policies that promote entrepreneurship like tax exemptions and financial incentive on the start-ups in BME. Several methods to facilitate cross-border cooperation, mutual resource sharing, and dissemination of information at a regional level can be developed: establishing innovation centre, coordinated investments in research and prototyping centers and unified educational standards. Such schemes aid multidisciplinary partnership, make certain free mobility of workforce, and step up commercialization of medical inventions. Leverage investment and policy will enhance health outcomes, spur innovation in technology in the long term, and build the BME workforce in the region.
Standardization and Harmonization of BME Curricula
The curricula of BME in SSA should be harmonized to allow the graduates to be able to work, move, and get education. The current diversity of curricula is explained by the availability of various institutional resources, the level of financing, and regulations in the country, and it is rather difficult to follow the international standards such as ABET. The integrated courses must include fundamental engineering, biological sciences, clinical experience, new technology and outcome-based training. Standardization also guarantees that graduates get skills required in business and medical care as well as easing credit transfer, dual degrees, and local study options. To achieve this, governments, universities, businesses and certification organizations need to join efforts of formulating learning objectives, creating assessment tools and pooling resources. Implementing standardized curricula can improve the level of labour preparedness, quality control, and innovation capability through SSA BME programs.
Strategies for Sustainable Funding
Funding Sustainable funding is essential to the development and influence of BME education, research, and innovation in SSA. Financial shortage decreases graduates’ readiness and innovation in healthcare by hindering investments in laboratories, prototype centres, personnel increase, curriculum development, and practical student training. The national and regional policies are to aim at a diverse range of sources of funds, such as corporate sponsorship, state grants, international assistance, and philanthropic donation. Professional training, short courses, consulting, patent commercialization, and incubators are also sources of money for the universities. Open financial administration enables money to be invested in such essential sectors as labs, research, and clinical associations. Through the fusion of domestic, corporate, and international resources, SSA BME efforts can offer sustainable funding, facilitate research and teaching, and create long-term innovation ecosystems that can meet the healthcare requirements of the region.
Regulatory Frameworks for Medical Devices Produced Locally
Strong regulatory frameworks are necessary for locally produced medical devices in SSA to be safe, efficient, and profitable The current constraints, which are occasionally inadequate, fragmented, or applied inconsistently, limit clinical testing, commercialization, and technological transfer. In accordance with international standards (ISO, WHO, FDA/CE), governments should establish comprehensive, locally adaptable frameworks for device design, testing, certification, and post-market monitoring. Harmonized regional legislation can enhance cross-border cooperation, production scale, and market access. Graduates of BME programs are ensured to be ethically pure, compliant, and capable of fostering innovation by including regulatory training. Improved healthcare access, local biomedical advancements, startup financing, and the creation of sustainable medical technology bionetwork are all preceded by supported regulatory frameworks.
Conclusion
The bibliometric and systematic analysis reveals that South Africa, Nigeria, Kenya, and Ghana lead BME program development and research output in SSA, despite collective contributions still falling short of global trends. Even though research is growing but geographically focused, there are gaps in addressing pressing regional health issues such infectious diseases, pregnancy and child health, and readily accessible diagnostics. Emerging areas of influence include 3D printing, AI-enabled healthcare solutions, and inexpensive medical equipment.
Short-term recommendations include strategic investments in clinical and laboratory infrastructure, faculty development, outcome-driven courses, and strengthening industry-academia partnerships to boost research productivity, innovation, and local relevance.
Long-term recommendations include the creation of standardized accreditation, integrated curricula, regional centers of excellence, sustainable financing sources, and public-private partnerships to promote translational research, graduate mobility, and quality assurance. This work provides the first thorough bibliometric and systematic mapping of BME in SSA to guide curriculum development, research priorities, and policy initiatives. Ultimately, by enhancing healthcare service delivery, creating a skilled BME workforce, and strengthening the biomedical innovation ecosystem, these projects can enable regional self-sufficiency in medical technology and capacity-building for sustainable healthcare.
Abbreviations
ABET, Accreditation Board for Engineering and Technology; AI, Artificial Intelligence; BME, BME; CSV, Comma-Separated Values; CT, Computed Tomography; GDP, Gross Domestic Product; ICT, Information and Communication Technology; MRI, Magnetic Resonance Imaging; OBE, Outcome-Based Education; PPP, Public–Private Partnership; QA, Quality Assurance; R&D, Research and Development; SDG, Sustainable Development Goal; SSA, Sub-Saharan Africa; WHO, World Health Organization; EUR-ACE, European Accreditation of Engineering Programmes; ISO, International Organization for Standardization; FDA, Food and Drug Administration; CE, Conformité Européenne.
Data Sharing Statement
All data are included in this manuscript.
Acknowledgments
This study was supported by the National Research Foundation of South Africa and the South African Research Chairs Initiative of the Department of Science and Technology (Grant No. PSTD250326306545).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Finch J. The ancient origins of prosthetic medicine. The Lancet. 2011;377(9765):548–39. doi:10.1016/S0140-6736(11)60190-6
2. Joseph F. Ancient High Tech: The Astonishing Scientific Achievements of Early Civilizations. Simon and Schuster; 2020.
3. Thayer MC. A Historical Overview of How Battlefield Medicine and Surgery Have Accelerated the Advancement of Medical Technology Through the Ages. Chapman University; 1974.
4. Marin E, Boschetto F, Pezzotti G. Biomaterials and biocompatibility: an historical overview. J Biomed Mater Res Part A. 2020;108(8):1617–1633. doi:10.1002/jbm.a.36930
5. Ackerknecht EH. A Short History of Medicine. JHU press; 2016.
6. Kichura DB, Sobechko IB. Biomaterials for Medical Purposes Progress Parallel with the Development of Civilization. Publishing House “Baltija Publishing”; 2025.
7. Sturdy S, Cooter R. Science, scientific management, and the transformation of medicine in Britain c. 1870–1950. History Sci. 1998;36(4):421–466. doi:10.1177/007327539803600402
8. Laufman H. Are engineers unsung heroes of medical progress? The historic bond between physics, engineering, and medicine. Biomed Instrument Technol. 2002;36(5):325–334.
9. Rayan AM, Adam A, Al-Arabi G, Ahmed MR. The applications of X-ray technology in medical imaging: advances, challenges, and future perspectives (A review). J Sustainable Food Water Energy Environ. 2025;1(2):39–61. doi:10.21608/jsfw.2025.409882.1003
10. Parthiban K, Deepthi D, Ahmed GS, Al-Salman HNK, Shari FH. Advanced Biomedical Technology. COSMAS Scientific Publications; 2024.
11. Foord DJ. Making hands: a history of scientific research and technological innovation in the development of myoelectric upper limb prostheses, 1945 to 2010; 2013.
12. Staros A. Rehabilitation engineering and the growth of prosthetics/orthotics practice. Int Rehabil Med. 1984;6(2):79–84. doi:10.3109/03790798409166765
13. Enderle J, Bronzino J, Eds. Introduction to BME. Academic press; 2012.
14. National Research Council, Division on Earth, Life Studies, Board on Life Sciences, & Committee on A Framework for Developing a New Taxonomy of Disease. Toward precision medicine: building a knowledge network for biomedical research and a new taxonomy of disease; 2011.
15. Nebeker F. Golden accomplishments in BME. IEEE Eng Med Biol Magazine. 2002;21(3):17–47. doi:10.1109/MEMB.2002.1016851
16. Weerarathna IN, Kumar P, Luharia A, Mishra G. Engineering with biomedical sciences changing the horizon of healthcare-A review. Bioengineered. 2024;15(1):2401269. doi:10.1080/21655979.2024.2401269
17. Akhtar Z. Exploring BME (BME): advances within accelerated computing and regenerative medicine for a computational and medical science perspective exploration analysis. J Emerg Med OA. 2024;2:1–23. doi:10.33140/JEMOA.02.01.06
18. Dixit S, Gupta S, Sharma A. Surgical devices for biomedical implants. In: Additive Manufacturing for Biomedical Applications: Recent Trends and Challenges. Singapore: Springer Nature Singapore; 2024:195–218.
19. Jaafari A, Rahmani Z, Zolfagharizadeh A, Amoozegar H. Innovations in BME: A Comprehensive Review of Emerging Trends and Technologies. 2025.
20. Regala JZ, Rahman KKM. An overview of the specializations in BME: definitions, scopes, constraints, and job opportunities. Available at SSRN 5159118. 2024.
21. da Ana PA, Lombello CB. BME: history and areas of expertise. In: Current Trends in BME. Cham: Springer International Publishing; 2023:1–13.
22. Yadav A, Rathore R, Suhag D, Thakur P, Thakur A. Nanobiology of Infectious Diseases. In: Advancements in Nanobiology. CRC Press; 2025:176–196.
23. Habeeb M, Thirumalai Vengateswaran H, Suseela P, Grace XF, Rani TS. Artificial intelligence and machine learning in cancer drug discovery, nanomedicine, and precision oncology. Nanomed Precision Oncol. 2025.
24. Fortune A, Aime A, Raymond D, Kumar S. Nanotechnology in medicine: a double-edged sword for health outcomes. Health Nanotechnol. 2025;1(1):9. doi:10.1186/s44301-025-00008-2
25. Aithal S. A review on anticipated breakthrough technologies of 21st century; 2015.
26. Srinivasan VA, Annalakshmi M, Priya C. Innovations in healthcare and biotechnology driven by Industry 5.0. In: Utilizing Renewable Energy, Technology, and Education for Industry. Vol. 5. IGI Global; 2024:258–274.
27. Jane Osareme O, Muonde M, Maduka CP, Olorunsogo TO, Omotayo O. Demographic shifts and healthcare: a review of aging populations and systemic challenges. Int J Sci Res Arch. 2024;11:383–395. doi:10.30574/ijsra.2024.11.1.0067
28. Khan HT, Addo KM, Findlay H. Public health challenges and responses to the growing ageing populations. Public Health Challenges. 2024;3(3):e213. doi:10.1002/puh2.213
29. Chakravarty S, Knorringa P.Enabling inclusive technological change through transformative policies: Frugal innovations from medical device manufacturing firms in South Africa; 2021.
30. De Maria C, Díaz Lantada A, Jämsä T, Pecchia L, Ahluwalia A. BME in low-and middle-income settings: analysis of current state, challenges and best practices. Health Technol. 2022;12(3):643–653. doi:10.1007/s12553-022-00657-8
31. Chakravarty S. Resource constrained innovation in a technology intensive sector: Frugal medical devices from manufacturing firms in South Africa. Technovation. 2022;112:102397. doi:10.1016/j.technovation.2021.102397
32. Joshi P. Inclusive Health: Medtech Innovations for the Early Detection of Cancer in India. Open University (United Kingdom); 2023.
33. Raxworthy M, Ssekitoleko R, Makobore PN. BME as a driver for healthcare improvements in East Africa; 2022.
34. Simiyu KW. Commercialization of Health Products from Sub-Saharan Africa: Challenges and Opportunities(Doctoral dissertation); 2011.
35. Thimbleby H. Technology and the future of healthcare. J Public Health Res. 2013;2(3):jphr–2013. doi:10.4081/jphr.2013.e28
36. Thielst CB. The future of healthcare technology. J Healthcare Manage. 2007;52(1):7–9. doi:10.1097/00115514-200701000-00003
37. Signé L. Strategies for Effective Health Care for Africa in the Fourth Industrial Revolution. Brookings; 2021.
38. Wahbi A, Khaddouj K, Aziz H, Naoufal L, Mkik M, Hebaz A. Digital health transformation and decision-making in Africa. In:
39. Lawal GS. AI-enabled early detection systems for low-resource oncology settings using cost-efficient IoT sensors; 2025.
40. Al-Worafi YM. Technology for health: overview. In: Handbook of Medical and Health Sciences in Developing Countries: Education, Practice, and Research. 2023:1–23.
41. Johnson EGT. AI-driven healthcare modernization in data-scarce regions: a quality-assured integrated maintenance management system with deep transfer learning and cybersecurity threat intelligence. Int J Multidisciplin Res Sci Eng Technol Manage. 2025;1(02):19–26.
42. Kelvin-Agwu MC, Adelodun MO, Igwama GT, Anyanwu EC. Innovative approaches to the maintenance and repair of biomedical devices in resource-limited settings. Int J Front Med Surg Res. 2024.
43. Woldeyohanins AE, Molla NM, Mekonen AW, Wondimu A. The availability and functionality of medical equipment and the barriers to their use at comprehensive specialized hospitals in the Amhara region, Ethiopia. Front Health Services. 2025;4:1470234. doi:10.3389/frhs.2024.1470234
44. Kabeta SH, Chala TK, Tafese F. Medical equipment management in general hospitals: experience of tulu bolo general hospital, south west shoa zone, Central Ethiopia. Med Devices Evidence Res. 2023;16:57–70. doi:10.2147/MDER.S398933
45. Sewagegn N, Tilahun T, Dessie G, Bezabih B. Assessment of the operational status of medical equipment in public hospitals in the Amhara region, Ethiopia: a sub-national study. Discover Health Syst. 2025;4(1):1–13. doi:10.1007/s44250-025-00312-9
46. Hussain SA, Bresnahan M, Zhuang J. Can artificial intelligence revolutionize healthcare in the Global South? A scoping review of opportunities and challenges. Digital Health. 2025;11:20552076251348024. doi:10.1177/20552076251348024
47. Tripathi D, Hajra K, Mulukutla A, Shreshtha R, Maity D. Artificial intelligence in BME and its influence on healthcare structure: current and future prospects. Bioengineering. 2025;12(2):163. doi:10.3390/bioengineering12020163
48. Twiringiyimana R. Fostering knowledge space actor interactions in an emerging place-based innovation ecosystem: The case of Kigali Innovation City (Doctoral dissertation, UCL (University College London)); 2025.
49. Onyancha OB, Nwagwu WE, Kwanya T. Knowledge mobilization for maximized research impact in centers of excellence in three countries in sub-Saharan Africa: insights from content analysis. Inform Develop. 2025;02666669251336561. doi:10.1177/02666669251336561
50. Agyei E, Kumah E. Navigating the complex terrain of healthcare systems in Sub-Saharan Africa: challenges and opportunities for progress. Discov Health Syst. 2024;3(1):39. doi:10.1007/s44250-024-00108-3
51. Peprah E, Wonkam A. Biomedical research, a tool to address the health issues that affect African populations. Global Health. 2013;9(1):50. doi:10.1186/1744-8603-9-50
52. Ahmed SN, Judd T. Clinical/BME & medical device trainings capacity assessment survey in Somaliland. Int J Health Technol Innov. 2025;4(01):19–30. doi:10.60142/ijhti.v4i01.04
53. Rushmer R. Medical Engineering: Projections for Health Care Delivery. Elsevier; 2012.
54. Nummi J. University–industry collaboration in medical devices development: case study of the Oulu Region in Finland. Innov Univ Competitive Regions. 2007;214(2007):95.
55. Kleiner-Schaefer T, Schaefer KJ. Barriers to university–industry collaboration in an emerging market: firm-level evidence from Turkey. J Technol Transfer. 2022;47(3):872–905. doi:10.1007/s10961-022-09919-z
56. Amaral C, Paiva M, Rodrigues AR, Veiga F, Bell V. Global regulatory challenges for medical devices: impact on innovation and market access. Appl Sci. 2024;14(20):9304. doi:10.3390/app14209304
57. Rimpi, Verma SJ, Pinky, Baldi A. Evidence-based recommendations for comprehensive regulatory guidelines in medical devices: the imperative for global harmonization. Naunyn-Schmiedeberg’s Arch Pharmacol. 2025;398(7):7697–7711.
58. Kulkov I, Ivanova-Gongne M, Bertello A, et al. Technology entrepreneurship in healthcare: challenges and opportunities for value creation. J Innov Knowledge. 2023;8(2):100365. doi:10.1016/j.jik.2023.100365
59. Ibeneme S, Karamagi H, Muneene D, Goswami K, Chisaka N, Okeibunor J. Strengthening health systems using innovative digital health technologies in Africa. Front Digital Health. 2022;4:854339. doi:10.3389/fdgth.2022.854339
60. Adekola AP. Digital health innovations: transforming healthcare access in sub-Saharan Africa. J Law Soc Development. 2025;22.
61. Arefin S. Leveraging AI for Healthcare Advancement in Africa. Acad J Sci Technol. 2024;7(1):1–11.
62. Lawanson OM, Abu-Halimeh A, Ajiferuke O. Leveraging advanced technologies to improve telemedicine delivery in Nigeria. World J Adv Res Rev. 2025;25(3):1698–1707. doi:10.30574/wjarr.2025.25.3.0902
63. Hubner S, Maloney C, Phillips SD, et al. The evolving landscape of medical device regulation in east, central, and Southern Africa. Global Health. 2021;9(1):136–148. doi:10.9745/GHSP-D-20-00578
64. de Jager K, Chimhundu C, Douglas TS. The medical device development landscape in South Africa: institutions, sectors and collaboration. South Afr J Sci. 2017;113(5–6):1–8. doi:10.17159/sajs.2017/20160259
65. Chikunichawa TA, Grobbelaar SS, Persson M. Research landscape and future agenda for health technology assessment of medical devices in low-and middle-income countries. South Afr J Indust Eng. 2025;36(4):115–133.
66. Okyere DO, Lomazzi M, Peri K, Moore M. Investing in health system resilience: a scoping review to identify strategies for enhancing preparedness and response capacity. Population Med. 2024;6(February):1–21. doi:10.18332/popmed/183661
67. Haldane V, De Foo C, Abdalla SM, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964–980. doi:10.1038/s41591-021-01381-y
68. Hanefeld J, Mayhew S, Legido-Quigley H, et al. Towards an understanding of resilience: responding to health systems shocks. Health Policy Plan. 2018;33(3):355–367. doi:10.1093/heapol/czx183
69. Saltzman WM. BME: Bridging Medicine and Technology. Cambridge University Press; 2009.
70. Olsztynska S, Komorowska M, Eds. BME: Trends, Research and Technologies. BoD–Books on Demand; 2011.
71. Mishra S. Artificial intelligence: a review of progress and prospects in medicine and healthcare. J Electronics Electromed Eng Med Informatics. 2022;4(1):1–23. doi:10.35882/jeeemi.v4i1.1
72. Fermin JL, Tan MJ. The need for the establishment of BME (BME) as an academic and professional discipline in the Philippines—a quantitative argument. IEEE Access. 2020;9:3097–3111. doi:10.1109/ACCESS.2020.3046655
73. Bamigboye AA, Bello KA. BME in Nigeria: the genesis, present and the future. Clin Rev Opin. 2021;10(1):1–4. doi:10.5897/CRO2019.0120
74. Miculescu M, Ion OA. Regulation and certification of (Bio) medical engineers: a case study on Romania. Int J Environ Res Public Health. 2022;19(15):9004. doi:10.3390/ijerph19159004
75. Ibrahim F, Thio THG, Faisal T, Neuman M. The application of BME techniques to the diagnosis and management of tropical diseases: a review. Sensors. 2015;15(3):6947–6995. doi:10.3390/s150306947
76. Hu CS, Wu QH, Hu DY, Tkebuchava T. Treatment of chronic heart failure in the 21st century: a new era of BME has come. Chronic Dis Transl Med. 2019;5(02):75–88. doi:10.1016/j.cdtm.2018.08.005
77. Nanthakumar R, Sivakumaran N. Role of BME for diagnose and treatment. Biomed J Sci Tech Res. 2018;4:94–112.
78. Rege K, Medintz IL. Methods in Bioengineering: Nanoscale Bioengineering and Nanomedicine. Artech House; 2009.
79. Siripurapu S, Darimireddy NK, Chehri A, et al. Technological advancements and elucidation gadgets for healthcare applications: an exhaustive methodological review-part-II (robotics, drones, 3D-printing, internet of things, virtual/augmented and mixed reality). Electronics. 2023;12(3):548. doi:10.3390/electronics12030548
80. Weber WA, Czernin J, Phelps ME, Herschman HR. Technology Insight: novel imaging of molecular targets is an emerging area crucial to the development of targeted drugs. Nat Clin Pract Oncol. 2008;5(1):44–54. doi:10.1038/ncponc0982
81. Rudin M, Weissleder R. Molecular imaging in drug discovery and development. Nat Rev Drug Discovery. 2003;2(2):123–131. doi:10.1038/nrd1007
82. Pang Z, Yang G, Khedri R, Zhang YT. Introduction to the special section: convergence of automation technology, BME, and health informatics toward the healthcare 4.0. IEEE Rev BME. 2018;11:249–259.
83. Melchor-Martínez EM, Torres Castillo NE, Macias-Garbett R, Lucero-Saucedo SL, Parra-Saldívar R, Sosa-Hernández JE. Modern world applications for nano-bio materials: tissue engineering and COVID-19. Front Bioeng Biotechnol. 2021;9:597958. doi:10.3389/fbioe.2021.597958
84. Akhtar ZB. Accelerated computing a BME and medical science perspective. Ann Acad Roman Sci Series Biol Sci. 2023;12(2):138–164. doi:10.56082/annalsarscibio.2023.2.138
85. Al Asif MR, Roy S, Abdullah A, Raihan M, Akter R, Hossain MZ. Role and impact of BME discipline for developing country perspective. Int J Innov Res Comput Sci Technol. 2018;6(4).
86. Houssein A, Lefor AK, Veloso A, et al. BMC BME: a home for all BME research. BMC BME. 2019;1(1):1.
87. Huang H, Feng W, Chen Y. Two-dimensional biomaterials: material science, biological effect and BME applications. Chem Soc Rev. 2021;50(20):11381–11485. doi:10.1039/d0cs01138j
88. Cai W, Ed. Engineering in Translational Medicine. Berlin, Germany: Springer; 2014.
89. Trebuňová M, Mezencevová V, Živčák J. BME–part of medicine. Acta Simulatio. 2017;3(2):1–6.
90. Jo H, Jun HW, Shin J, Lee S, Eds. BME: Frontier Research and Converging Technologies. Vol. 9. Springer;2015.
91. Alsuwairi HM, Alanazi YW, Alsayegh AA, et al. BME as a catalyst for healthcare quality, safety, and technology integration: a comprehensive review. Rev Diabetic Studies. 2025;285–296.
92. Lee HY, Oh BH. Paradigm shifts of heart failure therapy: do we need another paradigm? Int J Heart Fail. 2020;2(3):145. doi:10.36628/ijhf.2020.0010
93. Lander B, Atkinson-Grosjean J. Translational science and the hidden research system in universities and academic hospitals: a case study. Soc Sci Med. 2011;72(4):537–544. doi:10.1016/j.socscimed.2010.11.019
94. Ahluwalia A, Atwine D, De Maria C, et al. Open BME education in Africa. In:
95. Pecchia L, Maccaro A, Stavrianou K. Ethics and BME: Facing Global Health Emergencies. CRC Press; 2024.
96. Emicke R, Shepherd A, Powell D. Exploring the opportunities and challenges of healthcare innovation in UK higher education: a narrative review. Nurs Rep. 2025;15(5):171. doi:10.3390/nursrep15050171
97. Willie MM. Enhancing healthcare accessibility in South African medical schemes: applying Willie’s service innovation enabler framework. In: Health Promotion-From Knowledge to Action. IntechOpen; 2025.
98. Owusu MF, Adu J, Gyamfi S, Martin-Yeboah E, Dortey BA. Tackling the non-communicable disease epidemic: a framework for policy action in low-and middle-income countries. Pan Afr Med J. 2024;47(1).
99. Dovlo D. People and their health systems: the right to universal health coverage and the SDGs in Africa. Sustain Dev Goals Human Rights. 2020;2(3):53–71.
100. Defo BK. Beyond the ‘transition’frameworks: the cross-continuum of health, disease and mortality framework. Global Health Action. 2014;7(1):24804. doi:10.3402/gha.v7.24804
101. Gautam D, Sahney R. Reprocessing and reuse of single-use medical devices and the role of interprofessional collaboration: a literature review. Curr Med Res Pract. 2020;10(2):70–74. doi:10.1016/j.cmrp.2020.03.001
102. Balakrishnan K, Velusamy D, Hinkle HE, et al. Artificial intelligence in rural healthcare delivery: bridging gaps and enhancing equity through innovation. arXiv preprint arXiv:2508.11738. 2025.
103. Krishnan S. Project-based learning with international collaboration for training biomedical engineers. In:
104. De Maria C, Mazzei D, Ahluwalia A. Improving African healthcare through open source BME. Int J Adv Life Sci. 2015;7(1–2):10–19.
105. Bashir E, Gad K, Hammad M, Allam E. An IT-driven conceptual framework for research capacity building in integrated academic health systems. Discov Health Syst. 2025;4(1):135. doi:10.1007/s44250-025-00320-9
106. El Arab RA, Abu-Mahfouz MS, Abuadas FH, et al. Bridging the gap: from AI success in clinical trials to real-world healthcare implementation—A narrative review. Healthcare. 2025;13(7):701. doi:10.3390/healthcare13070701
107. Samenjo KT. Circular Medical Device Design for Low Resource Settings in sub-Saharan Africa; 2025.
108. Samenjo KT, Ji S. Realizing accessible and environmentally sustainable medical devices in low-resource healthcare settings in Sub-Saharan Africa personal narrative of the designer’s roles and competencies. She Ji J Design Econom Innov. 2025;11(1):99–122.
109. Costa V, Custodio MG, Gefen E, Fregni F. The relevance of the real-world evidence in research, clinical, and regulatory decision making. Front Public Health. 2025;13(1512429). doi:10.3389/fpubh.2025.1512429
110. Zhang XY. BME for health research and development. European Review for Medical & Pharmacological Sciences. 2015;19(2).
111. Kaill N, Bibb R. Perceived barriers and opportunities for adopting the circular economy in medical devices and the disparity between academia and industry. Design J. 2025;1–22. doi:10.1080/14606925.2025.2510800
112. Mehta SS. Commercializing Successful Biomedical Technologies. Cambridge University Press; 2022.
113. Nasir N, Molyneux S, Were F, Aderoba A, Fuller SS. Medical device regulation and oversight in African countries: a scoping review of literature and development of a conceptual framework. BMJ Global Health. 2023;8(8):e012308. doi:10.1136/bmjgh-2023-012308
114. Dube-Mwedzi S, Kniazkov S, Nikiema JB, et al. A rapid assessment of the National Regulatory Systems for medical products in the Southern African Development Community. J Pharm Policy and Practice. 2020;13(1):64. doi:10.1186/s40545-020-00255-x
115. Nyazema NZ, Chanyandura JT, Kumar PO. Nanomedicine and regulatory science: the challenges in Africa. Front Biomater Sci. 2023;2:1184662. doi:10.3389/fbiom.2023.1184662
116. Ndomondo-Sigonda M, Azatyan S, Doerr P, Agaba C, Harper KN. Best practices in the African medicines regulatory harmonization initiative: perspectives of regulators and medicines manufacturers. PLOS Global Public Health. 2023;3(4):e0001651. doi:10.1371/journal.pgph.0001651
117. de Jager K, Chimhundu C, Saidi T, Douglas TS. Medical device innovation in South Africa: evolution of collaboration networks (2001-2013). South Afr J Industrial Eng. 2019;30(2):26–44. doi:10.7166/30-2-1977
118. Chettri B, Ravi R. A comparative study of medical device regulation between countries based on their economies. Expert Rev Med Devices. 2024;21(6):467–478. doi:10.1080/17434440.2024.2360979
119. Bolo M. Strengthening research: industry collaborations in Africa; 2020.
120. UNICEF, & World Health Organization. Stakeholders’ Meeting on Strengthening Research Partnerships for Neglected Diseases of Poverty (No. TDR/GEN/EN/10.2). World Health Organization; 2010.
121. Ahluwalia A, María CD, Díaz Lantada A, et al. BME project based learning: Euro-African design school focused on medical devices. International. Journal of Engineering Education. 2018;34(5):1709–1722.
122. Lustick DR, Zaman MH. BME education and practice challenges and opportunities in improving health in developing countries. In:
123. White JA, Gaver DP, Butera RJ, et al. Core competencies for undergraduates in bioengineering and BME: findings, consequences, and recommendations. Ann BME. 2020;48(3):905–912.
124. Datta G, Gupta SK, Singh S. Revolutionizing design-centric business education. In:
125. Miao G, Ranaraja I, Grundy S, Brown N, Belkina M, Goldfinch T. Project-based learning in Australian & New Zealand universities: current practice and challenges. Australasian J Eng Educ. 2024;29(2):102–114. doi:10.1080/22054952.2024.2358576
126. Javaid M, Haleem A, Singh RP, Suman R. Sustaining the healthcare systems through the conceptual of BME: a study with recent and future potentials. Biomed Technol. 2023;1:39–47. doi:10.1016/j.bmt.2022.11.004
127. Oyejide AJ, Abodunrin OD, Atoyebi EO, et al. Landscape of BME and Technology in Nigeria: a Perspective. BME Educ. 2025;1–12.
128. Breneol S, Curran JA, Marten R, et al. Strategies to adapt and implement health system guidelines and recommendations: a scoping review. Health Res Policy Syst. 2022;20(1):64. doi:10.1186/s12961-022-00865-8
129. Kilmarx PH, Maitin T, Adam T, et al. A mechanism for reviewing investments in health research capacity strengthening in low-and middle-income countries. Ann Global Health. 2020;86(1):92. doi:10.5334/aogh.2941
130. Bartels HG. Promoting Access to Medical Technologies and Innovation: Intersections Between Public Health, Intellectual Property and Trade. World Health Organization; 2020.
131. Bhimavarapu U. AI in technology transfer developing sustainable models through university-industry collaboration. In: Bridging Technology and Development for Sustainable Innovation and Geopolitical Dynamics. IGI Global Scientific Publishing; 2025:67–86.
132. Pandey N, De Coninck H, Sagar AD. Beyond technology transfer: innovation cooperation to advance sustainable development in developing countries. Wiley Interdisciplin Rev: Energy Environ. 2022;11(2):e422. doi:10.1002/wene.422
133. Malik A, Sharma P, Pereira V, Temouri Y. From regional innovation systems to global innovation hubs: evidence of a Quadruple Helix from an emerging economy. J Bus Res. 2021;128:587–598. doi:10.1016/j.jbusres.2020.12.009
134. Nan M, Huang L. Innovation ecosystems: a cross-industry examination of knowledge flows and collaboration dynamics. J Knowledge Econ. 2025;16(1):26–64. doi:10.1007/s13132-024-01986-x
135. Stephen S, Aigbavboa C. Enhancing academia–industry partnerships for sustainable building: a change framework for research and innovation integration in Sub-Saharan Africa. Sustainability. 2025;17(9):3863. doi:10.3390/su17093863
136. Qian Y, Siau KL. Advances in IoT, AI, and sensor-based technologies for disease treatment, health promotion, successful ageing, and ageing well. Sensors. 2025;25(19):6207. doi:10.3390/s25196207
137. Huang G, Chen X, Liao C. AI-driven wearable bioelectronics in digital healthcare. Biosensors. 2025;15(7):410. doi:10.3390/bios15070410
138. Akila K, Gopinathan R, Arunkumar J, Malar BSB. The role of artificial intelligence in modern healthcare: advances, challenges, and future prospects. EurJ Cardiovasc Med. 2025;15:615–624.
139. Schee Genannt Halfmann S, Evangelatos N, Kweyu E, Van der Merwe A, Steinhausen K, Brand A. Best practice guidance for creation and management of innovations in health care and information and communications technologies. Omics J Integrat Biol. 2022;26(2):106–114. doi:10.1089/omi.2021.0043
140. Beaudry C, Mouton J. The Next Generation of Scientists in Africa. African Minds; 2018.
141. Arbaugh JB, Hwang A, McNally JJ, Fornaciari CJ, Burke-Smalley LA. Discerning citation patterns in dominant BME literature streams: lessons for BME scholars. Organ Manage J. 2021;18(3–4):145–172. doi:10.1108/OMJ-06-2020-0967
142. Abramo G, D’Angelo CA, Mele I. Gendered impact of COVID-19 pandemic on research production: a cross-country analysis. arXiv preprint arXiv:2102.05360. 2021.
143. Behague D, Tawiah C, Rosato M, Some T, Morrison J. Evidence-based policy-making: the implications of globally-applicable research for context-specific problem-solving in developing countries. Soc Sci Med. 2009;69(10):1539–1546. doi:10.1016/j.socscimed.2009.08.006
144. Lyall C, Bruce A, Marsden W, Meagher L. The role of funding agencies in creating interdisciplinary knowledge. Sci Public Policy. 2013;40(1):62–71. doi:10.1093/scipol/scs121
145. Greysen SR, Dovlo D, Olapade-Olaopa EO, Jacobs M, Sewankambo N, Mullan F. Medical education in sub-Saharan Africa: a literature review. Med Educ. 2011;45(10):973–986. doi:10.1111/j.1365-2923.2011.04039.x
146. Agbeyangi AO, Lukose JM. Telemedicine adoption and prospects in sub-Sahara Africa: a systematic review with a focus on South Africa, Kenya, and Nigeria. Healthcare. 2025;13(7):762. doi:10.3390/healthcare13070762
147. Ahluwalia A, Atwine D, De Maria C, et al. Open biomedical engineering education in Africa. In:
148. Danhoundo G. A scoping review of researchers’ involvement in health policy dialogue in Africa. Syst Rev. 2021;10(1). doi:10.1186/s13643-021-01745-y
149. Mathipa-Mdakane MG. Supporting innovation to address South Africa’s socio-economic challenges: a strategic framework. South Afr J Sci. 2025;121(9–10):1–4. doi:10.17159/sajs.2025/21836
150. Mbunge E, Batani J. Application of deep learning and machine learning models to improve healthcare in sub-Saharan Africa: emerging opportunities, trends and implications. Telematics Info Rep. 2023;11:100097. doi:10.1016/j.teler.2023.100097
151. Dash S, Shakyawar SK, Sharma M, Kaushik S. Big data in healthcare: management, analysis and future prospects. J Big Data. 2019;6(1):54. doi:10.1186/s40537-019-0217-0
152. Ploss B, Reichert W. Part I. the emergence of degree-granting biomedical engineering programs in sub-Saharan Africa. Ann Biomed Eng. 2017;45(10):2265–2268. doi:10.1007/s10439-017-1897-2
153. Coker A, Akintayo F, Achi C, Odeniyi M, Akano AOD. Recent developments in biomedical engineering education in Africa: a focus on Nigeria and the University of Ibadan. J Biomed Eng Educ. 2019;5(2):123–135.
154. Atwine D, Karanja YW, Ahluwalia A, et al. Nurturing next-generation biomedical engineers in Africa: the impact of innovators’ summer schools. Global Health. 2020;3(2):4.
155. Mohamedbhai G. Engineering Education in Sub-Saharan Africa: Quest for Quality. Int J Afr High Educ. 2016;2(1). doi:10.6017/ijahe.v2i1.9259
156. Hayward FM. Quality assurance and accreditation of higher education in Africa. In:
157. King R. Governing Universities Globally: Organizations, Regulation and rankings. Edward Elgar Publishing; 2009.
158. Al-Worafi YM. Quality and accreditation: overview. In: Handbook of Medical and Health Sciences in Developing Countries: Education, Practice, and Research. 2024:1–21.
159. Sims D, Zingela Z, Mokhachane M, et al. Medical education, reflections and perspectives from South Africa: a review. BMC Med Educ. 2025;25(1):370. doi:10.1186/s12909-025-06910-8
160. Ogu MI, Gabriel-Ugwu CF, Franklin S, et al. Industry Academia partnerships; models and strategies. In:
161. Carter KF, Nyemba WR. Industry-academia engagements: benchmarking the UK experience on Southern Africa. SAJET.
162. Maulana S, Iqhrammullah M, Pratama R, Tjandra S, Mulya IC, Haroen H. Bibliometric analysis and ChatGPT-Assisted identification of key strategies for improving primary maternity care based on a decade of collective research. Int J Women’s Health. 2025;17:53–66. doi:10.2147/IJWH.S494922
163. Sibanda K, Ndayizigamiye P, Twinomurinzi H. Industry 4.0 technologies in maternal health care: bibliometric analysis and research agenda. JMIR Pediatr Parent. 2024;7:e47848. doi:10.2196/47848
164. Kshatriya M, Syal R, Als D, et al. Implementation of health and health-related sustainable development goals: progress, challenges and opportunities—a systematic literature review update. BMJ Global Health. 2026;11(2):e021623. doi:10.1136/bmjgh-2025-021623
165. González SA, Vásquez JA. Higher education and professional performance: gaps and opportunities for developing professional skills in marine biologist graduates. J Biol Educ. 2024;58(5):1481–1503. doi:10.1080/00219266.2023.2255198
166. Eko F, Ajayi OO, Olatunji GI. An Interdisciplinary training and education model for STEM equity: integrating biomedical engineering and community engagement. J Adv Multidisciplin Res Studies. 2023;3(1):1404–1415. doi:10.62225/2583049X.2023.3.1.5055
167. DiMeo AJ, Afamefuna CJ, Ward SJ, et al. Biomedical engineering professional skills development: the RADx SM tech impact on graduates and faculty. IEEE Open Journal of Engineering in Medicine and Biology. 2021;2:163–169. doi:10.1109/OJEMB.2021.3070831
168. Oyejide AJ, Abodunrin OD, Atoyebi EO, et al. Landscape of biomedical engineering and technology in nigeria: a perspective: AJ Oyejide et al. Biomed Eng Educ. 2025;5(2):203–214. doi:10.1007/s43683-025-00187-5
169. Akindele BO. Application of design-based research in innovative education: western African education perspectives. In: Global Perspectives and Implementations of Design-Based Research. IGI Global Scientific Publishing; 2025:101–134.
170. Van Norman GA, Eisenkot R. Technology transfer: from the research bench to commercialization: part 1: intellectual property rights—basics of patents and copyrights. Basic Transl Sci. 2017;2(1):85–97. doi:10.1016/j.jacbts.2017.01.003
171. Graff G, Heiman A, Zilberman D. University research and offices of technology transfer. California Manage Rev. 2002;45(1):88–115. doi:10.2307/41166155
172. Falade IM, Gyampoh GKS, Akpamgbo EO, et al. A comprehensive review of effective patient safety and quality improvement programs in healthcare facilities. Med Res Arch. 2024;12(7).
173. Dosso M. Research and innovation: learning and Innovation strategies for sub-Saharan Africa. New Visions High Educ Towards. 2022;2030:474–482.
174. Olatunji G, Emmanuel K, Osaghae OW, Timilehin I, Aderinto N, Abdulbasit MO. Enhancing clinical and translational research in Africa: a comprehensive exploration of challenges and opportunities for advancement. J Clin Transl Res. 2023;9(5):357–368.
175. Simpson E. An Evaluation of the Equitable Practices for STEM Education to Prepare All Students for the 21st Century; 2024.
176. Cunningham CM. Engineering in Elementary STEM Education: Curriculum Design, Instruction, Learning, and Assessment. Teachers College Press; 2017.
177. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
178. Borthakur PP. The role and future directions of 3D printing in custom prosthetic design. Eng Proc. 2025;81(1):10.
179. Simpkin V, Namubiru-Mwaura E, Clarke L, Mossialos E. Investing in health R&D: where we are, what limits us, and how to make progress in Africa. BMJ Global Health. 2019;4(2):e001047. doi:10.1136/bmjgh-2018-001047
180. Al-Worafi YM. Research and Development in Developing Countries: achievements and Challenges. In: Handbook of Medical and Health Sciences in Developing Countries: Education, Practice, and Research. 2024:1–23.
181. Mazzoleni R, Nelson RR. The roles of research at universities and public labs in economic catch-up (No. 2006/01). LEM Working Paper Series; 2005.
182. Cheetham M, Redgate S, van der Graaf P, Humble C, Hunter D, Adamson A. ‘What I really want is academics who want to partner and who care about the outcome’: findings from a mixed-methods study of evidence use in local government in England. Evidence Policy. 2023;19(1):74–94. doi:10.1332/174426421X16535820632215
183. Elnasr Sobaih A, Jones E. Bridging the hospitality and tourism university–industry research gap in developing countries: the case of Egypt. Tourism Hospitality Res. 2015;15(3):161–177. doi:10.1177/1467358415578188
184. Omaswa F, Kiguli-Malwadde E, Donkor P, et al. The medical education partnership initiative (MEPI): innovations and lessons for health professions training and research in Africa. Ann Global Health. 2018;84(1):160. doi:10.29024/aogh.8
185. Nwoye MI, George S. TRIPLE HELIX MODEL: Role of Industry, Government and Academia. Shineeks Publishers; 2026.
186. Ramjee S. Comparing the Cost of Delivering Hospital Services Across the Public and Private Sectors in South Africa. The Hospital Association of South Africa, University of Cape Town; 2013.
187. Komape LJ. Exploring Public Perceptions of South African Private and Public Hospitals and Preferences for Health Care Providers. University of the Witwatersrand, Johannesburg (South Africa); 2013.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.