Back to Journals » Nature and Science of Sleep » Volume 18

Mandibular Advancement for Obstructive Sleep Apnea: Efficacy and the Trade-off of Expiratory Velopharyngeal Obstruction During Sleep Endoscopy – An Exploratory Observational Study
Authors Lo SC ![]() , Hsu YS
, Hsu YS ![]() , Lin YH
, Lin YH ![]() , Kuo YE, Chen TY
, Kuo YE, Chen TY ![]() , Yang CC
, Yang CC ![]()
Received 23 January 2026
Accepted for publication 23 May 2026
Published 11 June 2026 Volume 2026:18 598380
DOI https://doi.org/10.2147/NSS.S598380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Shih-Chieh Lo,1,2,* Ying-Shuo Hsu,3– 5,* Yun-Hsuan Lin,1 Yu-En Kuo,1,5 Tien-Yu Chen,5– 7 Cheryl CH Yang1,5,8,9
1Institute of Brain Science, National Yang Ming Chiao Tung University, Taipei, Taiwan; 2Department of Administer/Dentistry, Leading Dental Group, Taipei, Taiwan; 3Department of Otolaryngology, Shin Kong Wu-Ho-Su Memorial Hospital, Taipei, Taiwan; 4School of Medicine, Fu Jen Catholic University, New Taipei City, Taiwan; 5Sleep Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan; 6Department of Psychiatry, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan; 7Department of Psychiatry, College of Medicine, National Defense Medical University, Taipei, Taiwan; 8Brain Research Center, National Yang Ming Chiao Tung University, Taipei, Taiwan; 9Department of Education and Research, Taipei City Hospital, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Cheryl CH Yang, Institute of Brain Science, National Yang Ming Chiao Tung University, No. 155, Sec. 2, Linong Street, Beitou District, Taipei, 112304, Taiwan, Tel +886-2-2826-7058, Fax +886-2-28273123, Email [email protected] Tien-Yu Chen, Department of Psychiatry, Tri-Service General Hospital, National Defense Medical University, Taipei, Taiwan, Tel +886-2-8792-3311, Email [email protected]
Purpose: Mandibular advancement devices (MADs) are effective alternatives for obstructive sleep apnea (OSA), yet robust predictors of response are lacking, and the phenomenon of device-induced expiratory velopharyngeal obstruction (EVO) remains overlooked. This study conducted an exploratory clinical simulation to compare the efficacy and airway dynamics of a custom-fitted, maximally protrusive advanced MAD simulator versus a conventional edge-to-edge oral appliance (OA) during drug-induced sleep endoscopy (DISE).
Patients and Methods: In this prospective observational study, 75 adults with OSA underwent target-controlled infusion DISE. Upper airway obstruction (VOTE classification) and EVO were assessed in supine and head-rotated positions under three conditions: baseline, conventional OA, and advanced MAD simulator. A monitored subset (n=18) underwent simultaneous home sleep apnea testing to quantify apnea–hypopnea index (AHI) and lowest oxygen saturation (SpO2). The primary outcome was the change in upper airway obstruction severity at each VOTE anatomical site.
Results: Compared to the conventional OA, the advanced MAD simulator resolved complete velum obstruction in 34.8% of cases (supine, P = 0.015) and achieved 80.0% resolution for epiglottic obstruction during head rotation (P < 0.001). Velum responders in the supine position were younger and had a lower body mass index (BMI) and lower baseline AHI compared to non-responders (P < 0.05). In the monitored subset, the advanced simulator reduced AHI and improved lowest SpO2 compared to the conventional OA (P < 0.05). The incidence of EVO was higher with the advanced device (64.0% vs 41.3% in supine, P < 0.001), showing no significant association with tongue pressure.
Conclusion: While the advanced MAD simulator effectively resolves inspiratory obstruction at the velum and epiglottis, it significantly increases EVO. This exploratory simulation highlights a critical mechanical trade-off between inspiratory patency and expiratory resistance. These hypothesis-generating results warrant further longitudinal research to determine the net clinical impact on long-term treatment adherence and sleep quality.
Keywords: endoscopy, orthodontic appliances, obstructive sleep apnea, expiratory velopharyngeal obstruction
Introduction
Obstructive sleep apnea (OSA) is a common subtype of sleep-disordered breathing characterized by recurrent episodes of upper airway obstruction during sleep, leading to reduced airflow (hypopnea) or complete cessation of airflow (apnea) despite ongoing respiratory efforts. OSA affects nearly 1 billion adults globally and is strongly associated with serious comorbidities, including hypertension,1 type 2 diabetes,2 cardiovascular events,3 and excessive daytime sleepiness.4 Given its high prevalence and systemic impact, OSA is regarded as a major public health issue worldwide. While its hallmark is biomechanical collapse, contemporary evidence emphasizes a multifactorial etiology involving neurobiological, genetic, and metabolic contributions.5,6 Recent research indicates that elevated serum dopamine levels and the DRD2 rs1800497 polymorphism act as independent modulators of disease severity, hypopnea, and arousal thresholds.7 Furthermore, metabolic factors such as vitamin D and uric acid levels have been linked to sleep fragmentation and autonomic instability, particularly in patients with comorbid hypertension.8 While continuous positive airway pressure (CPAP) therapy remains the gold standard and first-line treatment for OSA,9 poor adherence is common, and many patients find CPAP intolerable, necessitating alternative therapeutic approaches.
Mandibular advancement devices (MADs) have emerged as important and viable alternatives to CPAP, particularly for patients with mild to moderate OSA who exhibit poor CPAP compliance.10–12 By advancing the lower jaw, MADs enlarge the upper airway space and reduce the tendency for airway collapse during sleep, in contrast to CPAP, which maintains airway patency by delivering continuous positive pressure through a mask.
Although MADs are generally more comfortable and better tolerated, treatment success varies considerably among patients, and reliable predictive factors for treatment response remain elusive.10–12 To determine suitable treatment modalities for specific individuals and to better phenotype patterns of upper airway collapse, drug-induced sleep endoscopy (DISE) has become increasingly important in clinical decision-making.13–16
DISE is now recognized as a valuable and critical tool for evaluating upper airway dynamics and guiding personalized treatment strategies.9,17,18 It allows real-time assessment of airway obstruction patterns and therapeutic maneuvers under conditions that closely mimic natural sleep, thereby elucidating the pathophysiological mechanisms underlying specific collapse sites and configurations.14–16 Recent methodological advances, including target-controlled infusion (TCI), positional maneuvers such as head rotation, intraoral negative airway pressure, and the application of noncustomized oral appliances, have further enhanced the clinical utility of TCI-DISE and improved its accuracy in forecasting surgical outcomes, particularly in tongue base collapse.13 Building on these developments, several studies have examined the predictive value of DISE for MAD therapy, showing that patients with complete improvement of upper airway obstruction during DISE with MAD or simulation bite in situ are more likely to respond to MAD treatment, with reported positive predictive values ranging from approximately 69% to 91%.16,19,20
Expanding upon these insights, contemporary clinical practice has transitioned toward systematic, individualized titration rather than fixed edge-to-edge advancement. Standard, non-customized oral appliances (OA) are defined as fixed-position devices typically utilized for initial response screening.21,22 While previous work established the utility of fixed edge-to-edge advancement, a critical knowledge gap remains regarding the upper physiological limit of airway expansion and the potential adverse effects on expiratory flow during aggressive titration.17,18
The clinical rationale for comparing maximal protrusion against standard advancement serves as an anatomical stress test. This approach allows clinicians to determine the therapeutic window, identifying the maximum inspiratory gain achievable before triggering expiratory velopharyngeal obstruction (EVO), which is essential for optimizing individualized MAD titration strategies. Current practice guideline from the American Academy of Sleep Medicine (AASM) and the American Academy of Dental Sleep Medicine (AADSM)10 indicate that while advancement may start at 30%–50%, the optimal therapeutic window is typically achieved between 50% and 75% of the patient’s maximum comfortable protrusion (MCP).23,24 These devices enlarge the cross-sectional area by mechanically advancing the tongue and mandible, thereby reducing peripharyngeal muscle relaxation.25 However, while DISE has been validated for establishing the physiological ceiling of inspiratory expansion,26–28 the specific behavior of the expiratory airway under differing levels of mechanical protrusion remains underexplored.
Previous work has demonstrated correlations between oral breathing patterns and the severity of sleep-disordered breathing, leading to the identification of EVO, a soft‑palate–related narrowing at the velopharynx during expiration that impedes nasal airflow, as an important therapeutic consideration.29–32 In our patient population, despite various interventions aimed at reducing mouth breathing, such as mouth taping, a phenomenon termed “mouth puffing” emerged in a substantial proportion of patients, suggesting complex interactions between oral breathing and upper airway structure.30–32 Prior TCI-DISE studies in these patients revealed that, when the mouth was taped or forcibly closed, some individuals exhibited EVO due to soft palate movement, resulting in obstruction of the oropharyngeal–nasal pathway during expiration and potentially influencing treatment outcomes.13,30–32 Although oral appliances can improve expiratory airflow, conventional OAs used in earlier TCI-DISE research typically employed a fixed edge-to-edge advancement length, which may not fully reflect the therapeutic potential of larger, individualized mandibular protrusion.16,19
Different degrees of mandibular advancement in OAs may yield varying effects on both inspiratory airway patency and EVO. Unlike previous DISE–MAD studies that excluded patients without improvement and thus focused primarily on positive predictive value, the present study included all patients regardless of DISE outcomes to evaluate both positive and negative predictive values. In this study, the distance of mandibular advancement was targeted to reach each patient’s MCP, determined while awake by simulating a forward mandibular position, and then reproduced during TCI-DISE using an advanced MAD simulator.13,16,19,20,33 This position was prioritized within the 50%–75% range of the patient’s MCP.
We hypothesized that an advanced MAD simulator, customized to the MCP, would yield superior inspiratory airway patency compared to conventional OAs, but might concomitantly increase the risk of EVO due to the aggressive anatomical reconfiguration of the velopharynx. To test this hypothesis, the aim of this study was to compare the effectiveness of an advanced MAD simulator with conventional OAs during DISE, assess its impact on upper airway patency and expiratory airflow restriction, and identify baseline patient characteristics that predict favorable treatment response and risk of EVO, thereby improving patient selection and optimizing treatment outcomes in clinical practice.
Materials and Methods
Study Design and Participants
This prospective observational study included consecutive patients with obstructive sleep apnea who underwent drug-induced sleep endoscopy in the Division of Otolaryngology at a tertiary medical center between August 2022 and June 2024. Patients were diagnosed with OSA by physicians using either standard polysomnography (PSG) or home sleep testing (HST). Inclusion criteria were: age 20–80 years, confirmed OSA diagnosis, ability to understand the study purpose and content, and provision of written informed consent. Exclusion criteria were: severe cardiovascular or cerebrovascular diseases, uncontrolled diabetes or other severe metabolic diseases, chronic obstructive pulmonary disease or other respiratory diseases requiring long-term oxygen therapy, vulnerable populations, and patients deemed unsuitable by the investigators. The study protocol was approved by the Institutional Review Board of Shin Kong Wu Ho-Su Memorial Hospital (IRB No. 20231105R) and complied with STROBE guidelines for observational studies. Figure 1 presents the participant flow diagram illustrating the screening, enrollment, and analysis process.
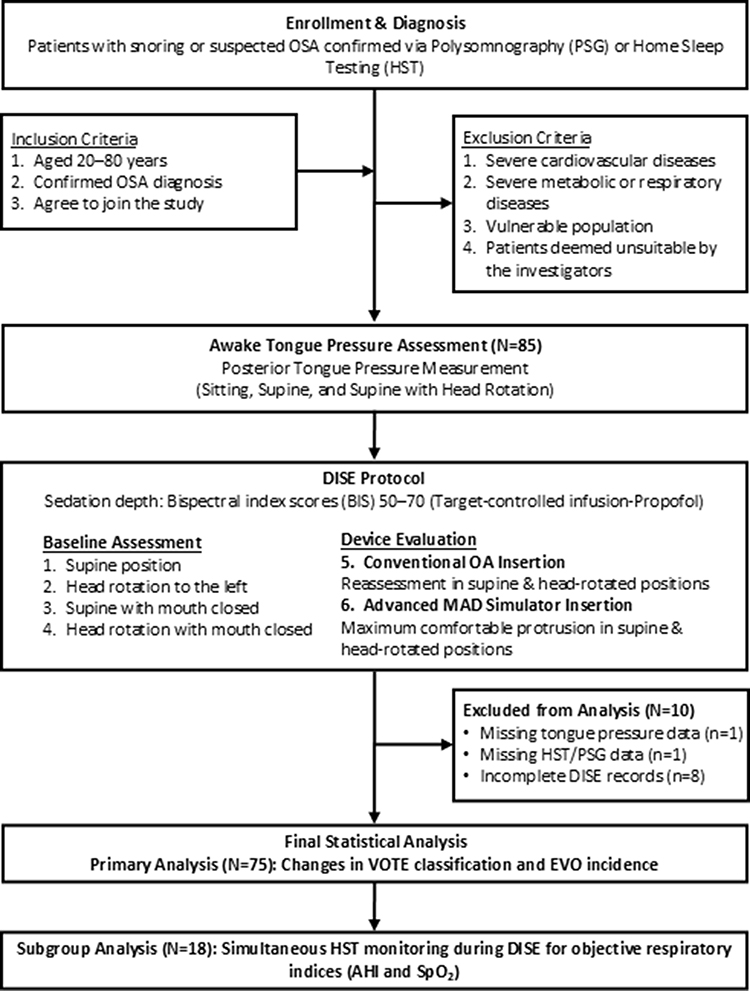 |
Figure 1 Flowchart illustrating the screening, enrollment, intervention, and analysis stages of the study in accordance with STROBE guidelines. Primary analysis included 75 patients, while a monitored subgroup of 18 patients underwent simultaneous objective respiratory monitoring. |
Sleep Studies
Patients underwent either in-laboratory PSG using the Compumedics Grael system (Compumedics Limited) or HST using the ApneaLink Air device (ResMed Ltd)., based on participant preference. The ApneaLink Air device has been validated against standard polysomnography, demonstrating high sensitivity (97.4%) and specificity (100%) for diagnosing moderate-to-severe OSA,34 with a strong correlation in AHI measurements.35 Sleep parameters, including apnea–hypopnea index (AHI), oxygen desaturation index (ODI), and lowest oxygen saturation during sleep, were recorded and scored according to the 2012 American Academy of Sleep Medicine definitions.36 In a subset of participants, the ApneaLink Air device was also used during DISE to monitor AHI and lowest oxygen saturation continuously, allowing objective assessment of respiratory events and desaturations across different airway conditions and positional changes.
Tongue Pressure Assessment
Maximum posterior tongue pressure was assessed before DISE using the IOPI Tongue Pressure/Lip Pressure Assessment and Training System (IOPI Medical LLC, Carnation, WA, USA), a clinically validated device for quantifying orofacial muscle strength and endurance in neuromuscular and swallowing disorders. Measurements were performed with the air-filled bulb positioned against the posterior tongue, and patients were instructed to press the bulb as hard as possible for approximately 2–3 seconds in three standardized postures: seated upright, supine, and head-rotated to the left. For each posture, three trials were recorded, and the highest value was taken as the maximum tongue pressure (kPa). All measurements were obtained prior to sedative administration for DISE to avoid the confounding effects of sedation on tongue muscle performance.
Device Specifications
Conventional Oral Appliance
The conventional OA (Somnoguard®, Tomed GmbH, Köln, Germany) is a prefabricated, commercially available mandibular advancement device with an edge-to-edge configuration and a central breathing hole to facilitate airflow (Supplementary Figure 1). It is designed as a one-size-fits-all device and is widely used in the management of mild to moderate OSA.
Advanced MAD Simulator
The advanced mandibular advancement device simulator was custom-fabricated using Regidur (Bielefelder Dentalsilicone GmbH & Co KG, Bielefeld, Germany), a fast-curing, super-hard dental silicone commonly used for bite registration (Supplementary Figure 2). During DISE, Regidur was molded intraorally to each patient’s maximum comfortable mandibular protrusion while awake, creating a patient-specific monoblock without a breathing hole to optimally simulate maximal mandibular advancement. Specifically, the advancement was targeted to reach each patient’s most comfortable level, representing a position within 50%–75% of their MCP. This range was selected based on clinical titration standards which suggest that the therapeutic effect is maximized in this window, while advancements exceeding 75% are frequently associated with significant temporomandibular joint discomfort and muscle fatigue. This custom simulator provided a stable occlusal model tailored to each patient, enabling real-time evaluation of its effectiveness in improving upper airway obstruction during DISE.
DISE Protocol
DISE was performed in an outpatient setting using a target-controlled infusion system to administer sedatives, with sedation depth monitored by maintaining Bispectral index scores (BIS) between 50 and 70. Upper airway obstruction was evaluated using the VOTE classification system (velum, oropharynx lateral wall, tongue base, epiglottis) to document the level, configuration, and degree of collapse.13 Once the target sedation level (BIS 50–70) was reached, patients were placed in the supine position. A flexible endoscope was introduced through the nasal cavity to evaluate the nasal passages, nasopharynx, velum, oropharynx, tongue base, epiglottis, and larynx. The primary goal was to assess upper airway obstruction during inspiration and detect the presence of EVO. Airway dynamics were assessed sequentially in the following positions, each maintained for at least 1 minute:
- Baseline assessment in the supine position (Figure 2A).
- Head rotation to the left, simulating the lateral sleep position (Figure 2B).
- Mouth forcibly closed with jaw support in the supine position (Figure 2C).
- Head rotation to the left with the mouth forcibly closed (Figure 2D).
- Insertion of the conventional OA, followed by reassessment in supine and head-rotated positions (Figure 2E and F).
- Insertion of the advanced MAD simulator at maximum comfortable protrusion, followed by reassessment in supine and head-rotated positions (Figure 2G and H).
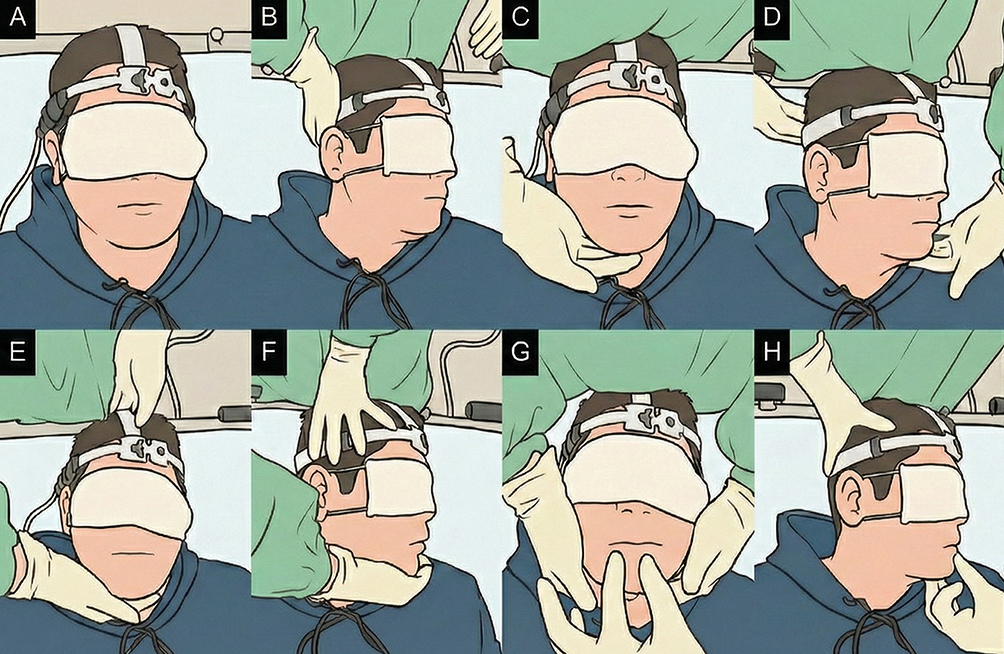 |
Figure 2 Clinical Demonstration of DISE Protocol. Sequential evaluation of airway dynamics during DISE. (A) Supine position. (B) Head tilted left. (C) Mouth forcibly closed. (D) Head tilted left with mouth closed. (E) Conventional OA. (F) Head tilted left with Conventional OA. (G) Advanced MAD simulator. (H) Head tilted left with advanced MAD simulator. |
To assess EVO, the endoscope tip was positioned in the velopharyngeal region. EVO was documented when posterior displacement and narrowing of the soft palate were observed during exhalation, leading to difficulty expelling air through the nasal passages; this phenomenon was recorded when it occurred repeatedly (more than twice) and persisted for at least 1 minute in each condition.
Outcome Measures
Primary Outcomes
The primary outcomes were changes in upper airway obstruction severity at each VOTE anatomical site (velum, oropharynx lateral wall, tongue base, epiglottis) when comparing the conventional OA with the advanced MAD simulator during DISE. Obstruction severity was graded according to the VOTE system, and improvement was defined as a shift from complete or partial obstruction to less obstruction, or from partial obstruction to no obstruction.
Secondary Outcomes
Secondary outcomes included baseline patient characteristics associated with treatment response, defined as improvement in obstruction severity at any VOTE site when using the advanced MAD simulator compared with the conventional OA. Additionally, the incidence of EVO under different positional and device conditions was evaluated. In the subset with simultaneous HST monitoring, changes in AHI and lowest oxygen saturation (SpO2) across interventions (no device, conventional OA, advanced MAD simulator) and positions (supine, head-rotated) were also analyzed.
Statistical Analysis
An a priori sample size calculation was performed for the primary outcome using McNemar’s test. Assuming an odds ratio of 4.0 and a discordant pair proportion of 0.35 in favor of the advanced MAD simulator, a minimum of 58 patients was required to achieve 80% statistical power at a two-sided alpha level of 0.05. Changes in obstruction severity at each VOTE site between the conventional OA and the advanced MAD simulator were compared using the McNemar–Bowker test. For analyses based on responder status, baseline characteristics between treatment responders and non-responders were compared using Fisher’s exact test for categorical variables and independent t-tests for continuous variables. The proportion of patients exhibiting increased EVO before and after application of the advanced MAD simulator was compared using McNemar’s test. Generalized Estimating Equations (GEE) were used to analyze AHI, ODI, and lowest oxygen saturation across intervention conditions, accounting for the repeated measures design. Pairwise comparisons were based on Estimated Marginal Means (EMM) with Sequential Bonferroni correction for multiple comparisons. Statistical significance was set at P < 0.05. Missing data were handled using complete case analysis for categorical variables, while the Generalized Estimating Equations (GEE) model intrinsically accommodated missing continuous data points in the monitored subset without requiring explicit multiple imputation techniques. All statistical analyses were performed using SPSS version 25.0 (IBM SPSS Inc., Chicago, IL, USA).
Results
Patient Characteristics
During the study period, patients with suspected or confirmed OSA were assessed for eligibility. As detailed in the participant flow diagram (Figure 1), after excluding patients based on the predefined criteria, a total of 85 eligible patients were enrolled for awake assessments. Subsequently, 10 patients were excluded from the final analysis due to missing data or incomplete records. A final cohort of 75 adult OSA patients (82.7% male, mean age 44.5 ± 11.5 years) was included in the primary statistical analysis. Mean BMI was 26.5 ± 4.3 kg/m2, baseline AHI, derived mainly from level 3 HST, was 27.5 ± 19.7 events/h, and minimum oxygen saturation was 77.5 ± 9.0%. Tongue pressure measurements were generally low across all positions (45.4–47.7 kPa), below the normal adult range of 80 kPa (Table 1).
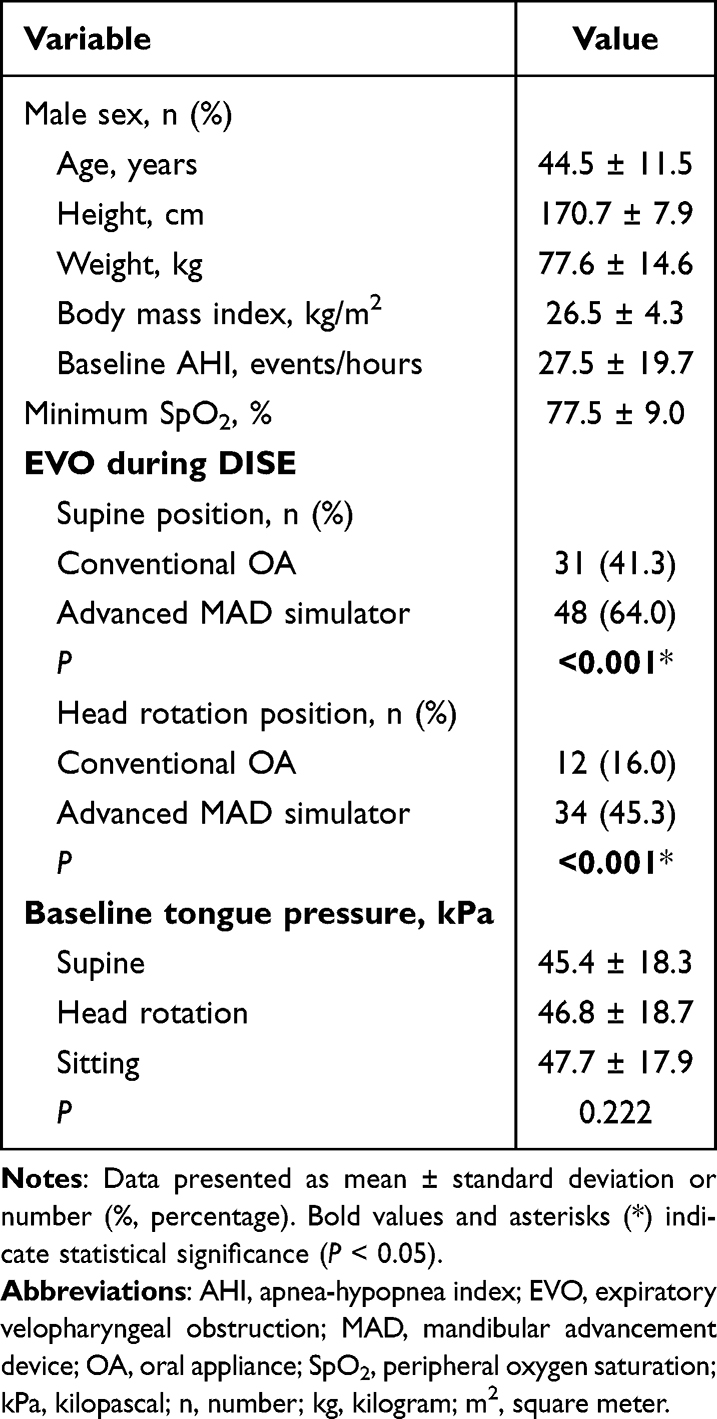 |
Table 1 Demographics and Clinical Characteristics of Study Participants (N = 75) |
Treatment Efficacy Comparison
The advanced MAD simulator demonstrated superior efficacy compared to conventional oral appliances across multiple anatomical sites, as evaluated by overall transition for clinical improvement, as detailed in Table 2. The clinical effect sizes, expressed as paired odds ratios with Haldane-Anscombe correction, are detailed in Supplementary Table 1.
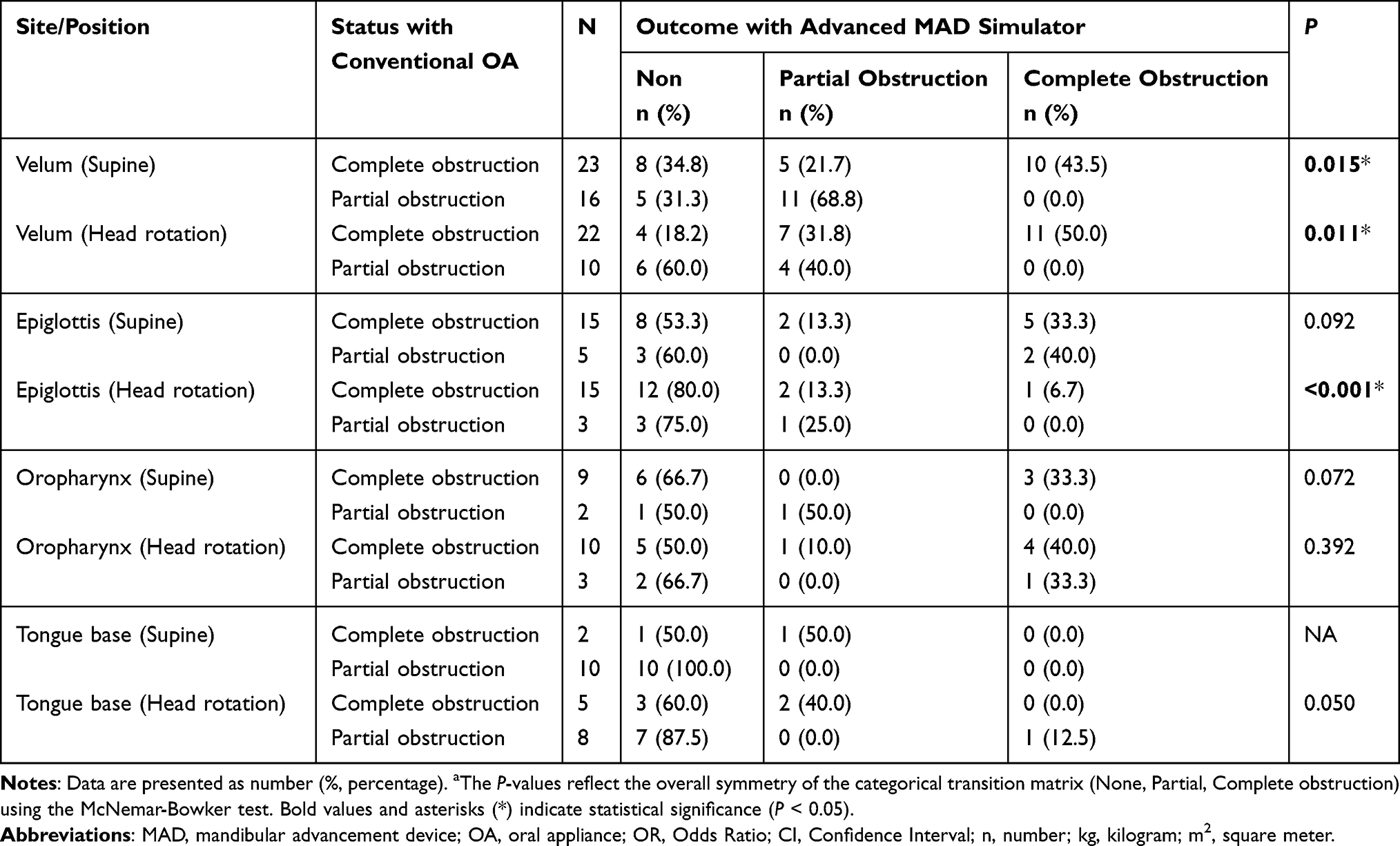 |
Table 2 Comparison of Upper Airway Obstruction Severity by VOTE Classification Between Conventional OA and Advanced MAD Simulator |
Velum (Soft Palate) Obstruction
In the supine position, the advanced MAD simulator demonstrated a significant rescue effect at the velum (overall transition P = 0.015, Table 2). Among patients who experienced persistent complete obstruction with the conventional OA (n=23), 34.8% achieved complete resolution and an additional 21.7% improved to partial obstruction with the advanced MAD simulator. During head rotation, improvement was even more pronounced (overall transition P = 0.011, Table 2). Among 22 patients with complete velum obstruction, 50% experienced improvement to partial or no obstruction. Additionally, 60% of patients with partial obstruction achieved complete resolution.
Epiglottis Obstruction
The most distinct advantage was observed at the epiglottis during head rotation (overall transition P < 0.001). Remarkably, 80.0% (12/15) of patients who remained completely obstructed with the conventional OA achieved full patency (no obstruction) when switched to the advanced MAD simulator.
Oropharynx and Tongue Base
Although a trend toward improvement was observed at the oropharyngeal and tongue base sites following intervention with the advanced MAD simulator, these changes did not reach statistical significance in either the supine or head rotation positions (oropharynx supine, overall P = 0.072; head rotation, P = 0.392; tongue base supine, NA). Notably, improvement at the tongue base in the head rotation position showed a trend toward improvement (overall P = 0.050), suggesting a possible treatment effect in this subgroup. It should be noted, however, that the relatively small number of patients with partial or complete obstruction at these anatomical sites may have limited the statistical power, and these results should therefore be interpreted with caution (Table 2).
Predictive Factors for Treatment Response
Analysis of baseline characteristics associated with treatment response revealed distinct patterns for different anatomical sites (Tables 3–6).
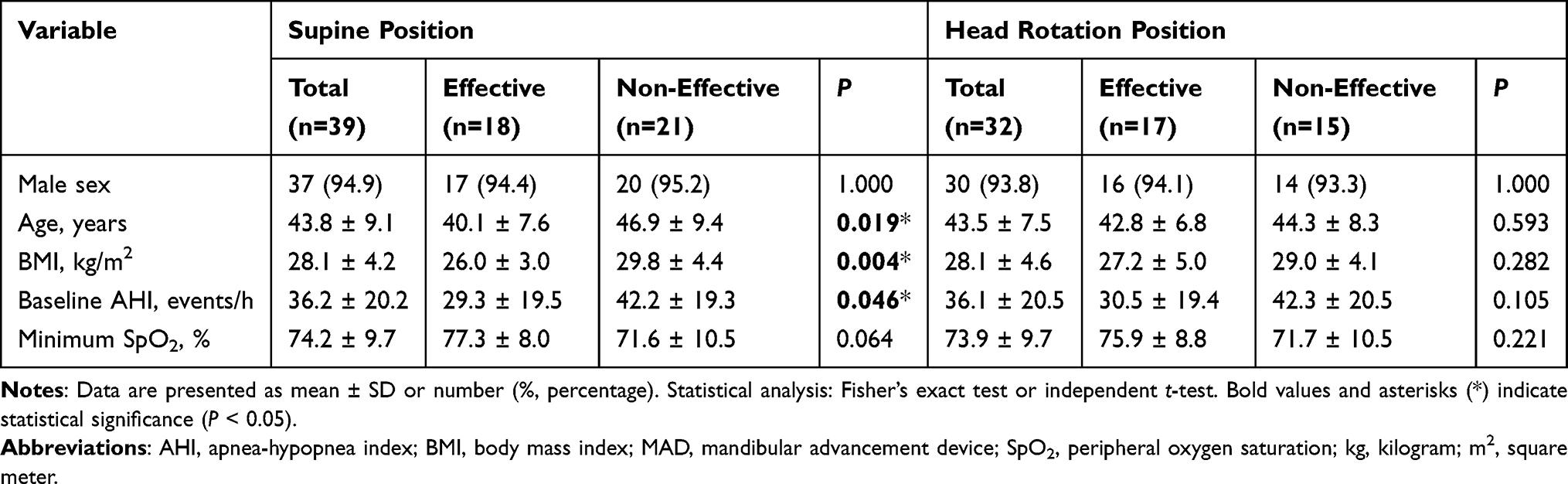 |
Table 3 Baseline Characteristics for Velum Obstruction Response to Advanced MAD Simulator |
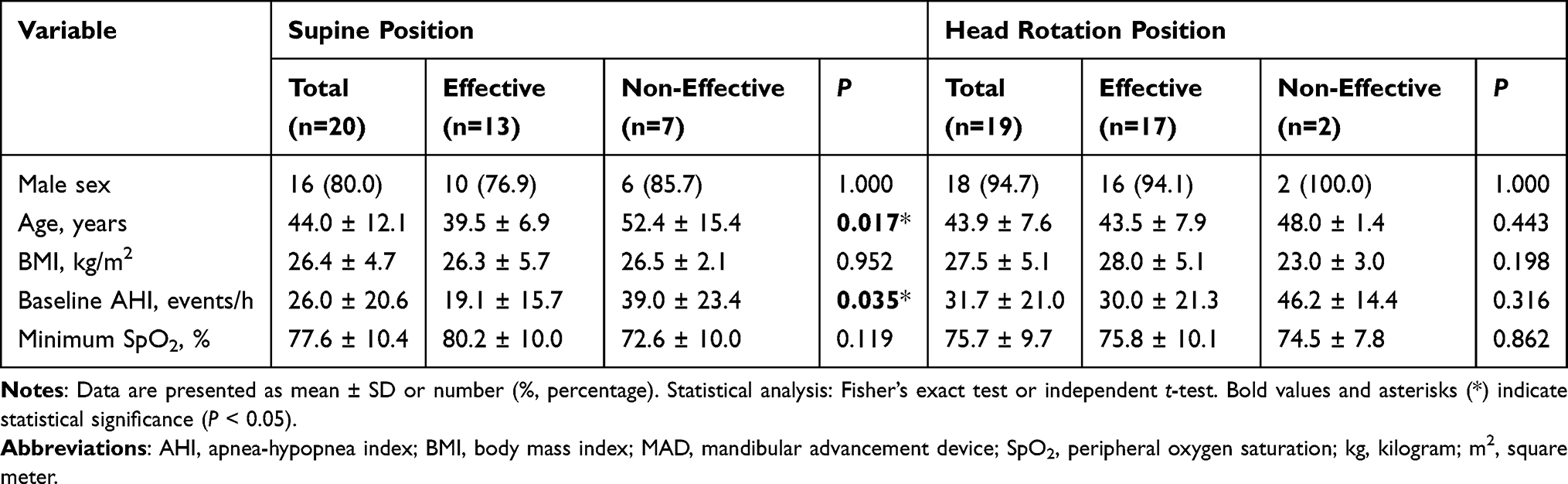 |
Table 4 Baseline Characteristics for Epiglottis Obstruction Response to Advanced MAD Simulator |
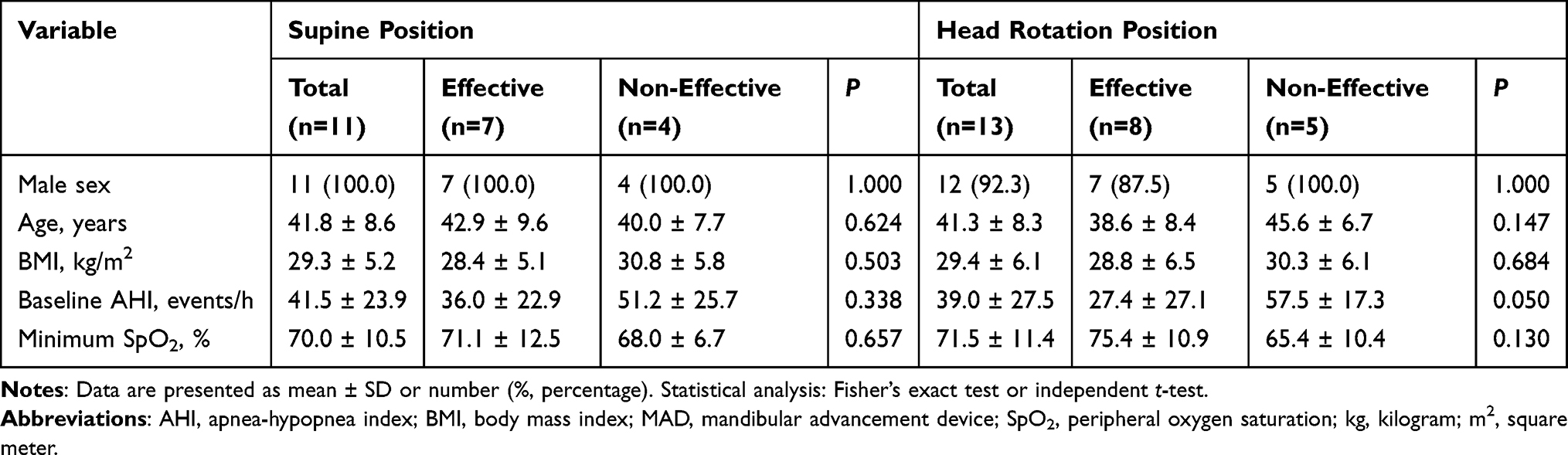 |
Table 5 Baseline Characteristics for Oropharynx Obstruction Response to Advanced MAD Simulator |
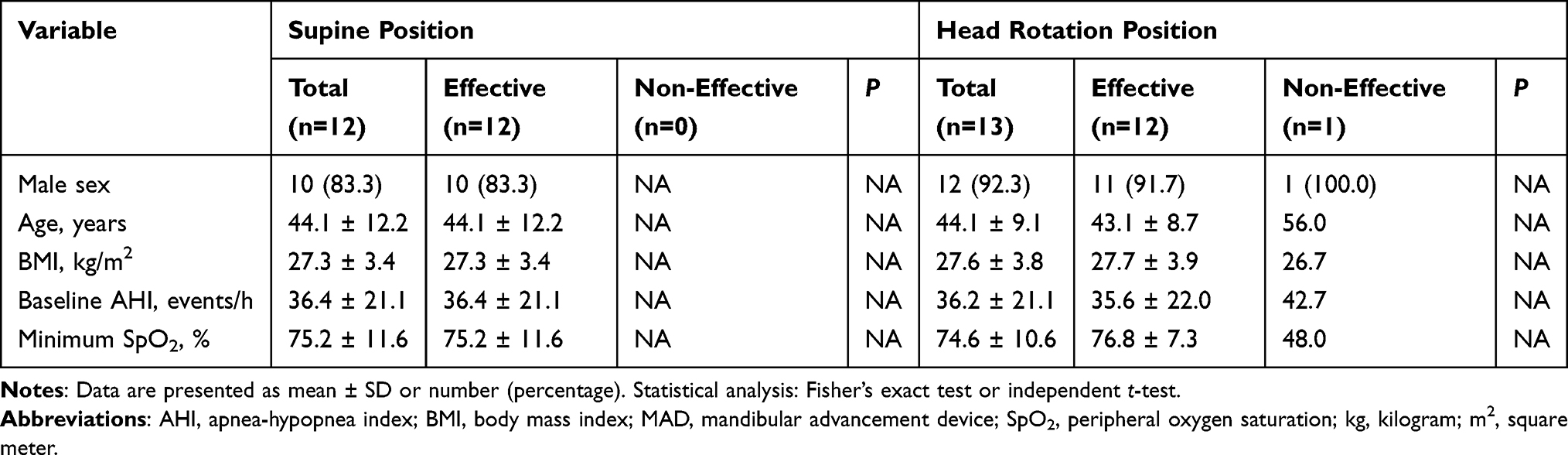 |
Table 6 Baseline Characteristics for Tongue Base Obstruction Response to Advanced MAD Simulator |
Velum Obstruction Response
In supine position, patients who responded favorably to advanced MAD simulator treatment were characterized by significantly different baseline characteristics compared to non-responders, with a younger age (40.1 ± 7.6 vs 46.9 ± 9.4 years, P = 0.019), lower BMI (26.0 ± 3.0 vs 29.8 ± 4.4 kg/m2, P = 0.004), and lower baseline AHI (29.3 ± 19.5 vs 42.2 ± 19.3 events/h, P = 0.046; Table 3). During head rotation, these differences were attenuated and did not reach statistical significance, suggesting positional factors may influence treatment response prediction.
Epiglottis Obstruction Response
For epiglottis obstruction in the supine position, treatment responders were younger (39.5 ± 6.9 vs 52.4 ± 15.4 years, P = 0.017) and had a lower baseline AHI (19.1 ± 15.7 vs 39.0 ± 23.4 events/h, P = 0.035) compared with non‑responders, as shown in Table 4. These findings suggest that milder disease severity and younger age may favor epiglottic improvement with the advanced MAD simulator (Table 4).
Oropharynx and Tongue Base Response
For oropharynx obstruction, patients with higher baseline AHI showed poorer response during head rotation (27.4 ± 27.1 vs 57.5 ± 17.3 events/h, P = 0.050, Table 5). Tongue base obstruction showed near-universal improvement, limiting meaningful predictive factor analysis (Table 6).
Representative endoscopic views demonstrate the effects of no intervention, conventional OA, and advanced MAD on velopharyngeal patency in the supine position (Figure 3). EVO was substantially more frequent with the advanced MAD simulator than with the conventional oral appliance (Table 1). In supine position, 64.0% of patients using advanced MAD simulator experienced EVO compared to 41.3% with conventional OA (P < 0.001). During head rotation, the rates were 45.3% versus 16.0% respectively (P < 0.001).
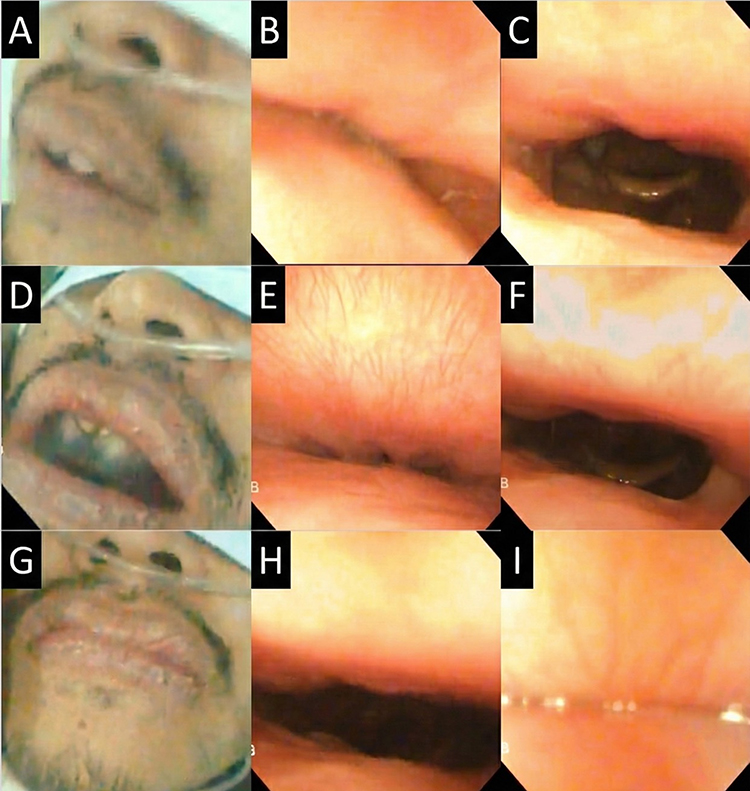 |
Figure 3 Effects of no intervention, conventional OA, and advanced MAD on velopharyngeal patency in the supine position. (A–C) show the patient without an oral appliance: facial view (A), velopharyngeal airway during inspiration (B), and during expiration (C). (D–F) show the patient wearing a conventional OA: facial view (D), velopharyngeal airway during inspiration (E), and during expiration (F). Despite the use of the conventional OA, persistent velopharyngeal narrowing is observed during inspiration. (G–I) show the patient wearing an advanced MAD simulator: facial view (G), velopharyngeal airway during inspiration (H), and during expiration (I). With the advanced MAD simulator, the inspiratory velopharyngeal airway becomes patent, whereas velopharyngeal obstruction is shifted to expiration. |
Tongue pressure measurements did not significantly differ between patients with and without EVO across different positions and devices (P = 0.222), suggesting anatomical rather than functional factors may predominate.
Subgroup Analysis of AHI and Oxygen Saturation During DISE
In the monitored subset of 18 participants, minor missing data occurred during data collection. For the repeated respiratory measures, transient signal loss resulted in missing AHI and ODI data for 2 participants, and missing SpO2 data for 1 participant during the device intervention phases. As predetermined, the Generalized Estimating Equations (GEE) model intrinsically accommodated these unbalanced repeated measures without requiring multiple imputation. The analysis compared the Estimated Marginal Means (EMM) across conditions. In the supine position, the advanced MAD simulator significantly reduced the AHI to an EMM of 4.41 ± 5.16 events/h, compared to 40.36 ± 5.16 events/h in the no intervention condition (P < 0.001). In the head rotation position, the advanced MAD simulator demonstrated superior efficacy. The AHI decreased to 0.00 ± 5.59 events/h, which was significantly lower than the conventional OA and no intervention groups. Similarly, the lowest oxygen saturation (SpO2) in the head rotation position was significantly higher with the advanced MAD simulator (92.98 ± 1.97%) compared to the conventional OA and no interventional groups. These findings suggest that the advanced MAD simulator provides greater therapeutic benefit, particularly when combined with head rotation (Figure 4 and Supplementary Table 2).
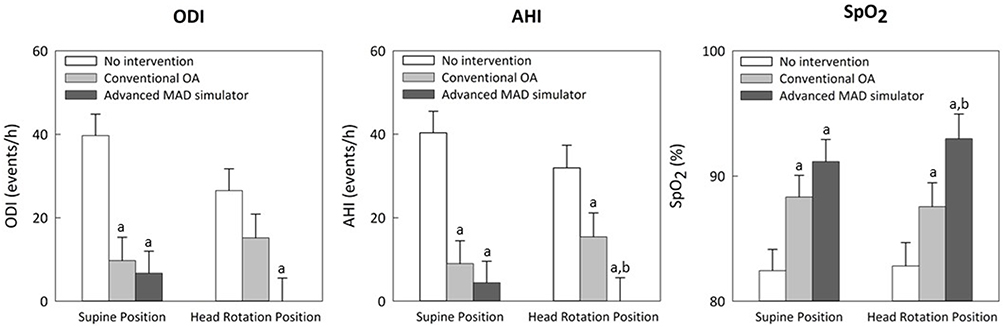 |
Figure 4 Comparison of AHI, ODI, and Lowest SpO2 across conditions and positions during DISE. Data are presented as Estimated Marginal Means (EMM) with error bars representing the Standard Error (SE) derived from the GEE model. No intervention: Baseline; Conventional OA: Conventional Oral Appliance; Advanced MAD simulator: Custom Oral Appliance. Statistical significance is indicated by letters: a, p < 0.05 vs No Intervention; b, p < 0.05 vs Conventional OA. The p-values for these comparisons were adjusted using the Sequential Bonferroni method. |
Discussion
This study represents the first comprehensive evaluation comparing different oral appliance designs in terms of upper airway obstruction patterns during DISE while simultaneously integrating objective respiratory indices such as AHI and lowest oxygen saturation. By including all patients irrespective of DISE improvement, the study allowed assessment of both positive and negative predictive values for MAD effectiveness, in contrast to prior work that focused mainly on responders. The advanced MAD simulator, which achieved greater mandibular advancement than a conventional edge-to-edge OA, provided superior treatment efficacy for upper airway obstruction—particularly at the velum and epiglottis—yet was also associated with a higher incidence of EVO in a subset of patients.
Superior Resolution of Velum and Epiglottis Obstruction
Our results demonstrate that the advanced MAD simulator acts as a powerful therapeutic intervention for patients who remain obstructed with a conventional device. As shown in Table 2, the advanced simulator achieved a significant “rescue effect”, resolving complete velum obstruction in over one-third of non-responders in the supine position and half during head rotation. Even more striking is the response at the epiglottis: during head rotation, 80% of patients with complete obstruction achieved full patency. This finding is clinically pivotal, as epiglottic collapse is traditionally considered difficult to treat with oral appliances.
Regarding the epiglottis, our findings highlight a significant synergistic benefit between mandibular protrusion and head rotation. Previous studies have indicated that head rotation alone can reduce epiglottic collapse by shifting the gravitational vector away from the airway.37,38 Our group’s prior research also confirmed that head rotation is among the most effective non-surgical treatments for anteroposterior epiglottic collapse.17 In the current exploratory simulation, the high-resolution rate (80.0%) suggests that the advanced MAD simulator provides additional mechanical stabilization. Protrusion exerts forward traction on the genioglossus and suprahyoid muscles, which may in turn tighten the hyo-epiglottic ligament.39,40 This mechanical tension could make it more responsive to the positional benefits of head rotation. However, we acknowledge that the resolution cannot be attributed to the device alone; rather, it represents an optimized clinical scenario where mechanical and positional therapies coincide.17,41 These short-term DISE findings suggest that a combined phenotypic approach—aggressive MAD titration alongside positional modification—holds potential for patients with predominant epiglottic collapse who fail conventional single-modality treatments, and warrants further validation in prospective longitudinal trials.17,28
The concurrent improvement in quantitative respiratory indices (AHI and SpO2, Supplementary Table 2) in our monitored subset further validates these endoscopic observations, confirming that the anatomical patency achieved by the advanced simulator translates into physiological benefits.
Phenotypes for Precision Treatment
A key contribution of this study is the identification of robust predictors for treatment success (Table 3 and Table 4). We found that responders to the advanced MAD simulator at the velum and epiglottis were significantly younger, had lower BMI, and presented with lower baseline AHI compared to non-responders. This aligns with the concept that “anatomical compromise” in severe OSA or obesity may overwhelm the mechanical advantage provided by mandibular advancement. These data suggest that patient selection is critical: rather than applying MADs universally, clinicians can use these anthropometric markers to identify ideal candidates who are most likely to achieve optimal airway patency with aggressive protrusion.
Design Considerations and Role of DISE-Guided MAD Screening
The advanced MAD simulator represents an important innovation in the context of TCI-DISE, enabling real-time testing of patient-specific maximum comfortable protrusion rather than relying solely on standardized edge-to-edge advancement. Previous DISE studies using interim MADs have shown that complete resolution of upper airway obstruction under MAD simulation confers a markedly higher likelihood of long-term treatment response, though statistical significance was sometimes limited by small sample sizes.20 More recent work has also demonstrated that new-generation interim MADs can serve as effective screening tools, with comparable effects between non-custom and custom devices.19 The present findings extend this literature by demonstrating that DISE-guided, maximally protrusive MAD simulation can reveal not only potential benefits (reversal of velum and epiglottis obstruction, AHI and SpO2 improvement) but also risks (induction or worsening of EVO) within the same session. Importantly, patient feedback indicated that, outside of DISE conditions, using the advanced MAD simulator without completely sealing the mouth could allow adequate airflow and effectively reduce snoring and breathing difficulty, suggesting that clinical performance may differ from that observed under forced mouth closure or tape. This observation is consistent with reports that interim MADs can give patients an immediate “trial experience” of both advantages and potential drawbacks before committing to a custom-made device.19 Together, these results argue for DISE-based MAD screening protocols that explicitly evaluate both inspiratory and expiratory phases and test different mandibular positions and oral sealing conditions rather than focusing solely on inspiratory collapse.
The Trade-Off: Inspiratory Gain vs Expiratory Resistance
While the advanced MAD simulator excelled in maintaining inspiratory patency, this benefit came with a trade-off. We observed a significantly higher incidence of EVO compared to the conventional OA. We hypothesize that this phenomenon is primarily mechanical: greater mandibular advancement enhances inspiratory airway patency but simultaneously increases the contact area between the soft palate and the posterior pharyngeal wall. This observation suggests a potential mechanism where an anatomical seal is created, hindering expiratory flow, which aligns with previous observations of “mouth puffing” and EVO.32,42 Our findings extend these observations. While previous work identified external mouth taping as a trigger for this obstruction, our current data reveal that aggressive mandibular advancement itself can internally reconfigure the soft palate geometry, creating a similar “sealed” environment independent of external taping.29 Although the absence of a breathing hole in our simulator could theoretically contribute to resistance, we believe the observed EVO is primarily driven by anatomical reconfiguration. Aggressive mandibular advancement likely increases tension on the palatoglossal arch, mechanically pulling the soft palate posteriorly against the pharyngeal wall. This creates a structural seal that hinders expiratory flow, a mechanism distinct from simple mouth closure. Crucially, our data indicate that the therapeutic benefit of maintaining inspiratory patency outweighs the functional cost of expiratory obstruction. Despite the higher incidence of EVO, the advanced MAD simulator achieved superior improvements in AHI and oxygen saturation (Supplementary Table 2), suggesting that the physiological gain may remain positive despite expiratory impedance during short-term observation. However, these findings are strictly hypothesis-generating. Future prospective longitudinal trials incorporating real-world device use, objective adherence monitoring, and patient-centered outcomes are essential to confirm whether the inspiratory benefits definitively outweigh the expiratory drawbacks. Therefore, clinical titration must aim for a “sweet spot” that maximizes inspiratory width without crossing the threshold that triggers expiratory limitation.
Limitations and Future Directions
Several limitations must be acknowledged. First, the two devices compared in this exploratory simulation are structurally non-equivalent. The conventional OA is a prefabricated device featuring a central breathing hole, while the advanced MAD simulator is a custom-molded monoblock lacking an anterior airway channel. This structural asymmetry prevents the isolation of mandibular advancement distance as the sole independent variable. Furthermore, because the MAD simulator lacks a breathing hole, which does not fully reflect many clinically used devices, it forces obligate nasal expiration. This likely acts as a significant confounder, mechanically contributing to the increased EVO observed as a device-related artifact. Therefore, the observed EVO should be interpreted as a combined biomechanical response to both the patient’s anatomy and the specific closed-mouth device design, rather than a purely intrinsic physiological phenomenon. Second, although OSA diagnosis was allowed by either PSG or HST, most patients underwent HST because of convenience. Combining these two modalities without accounting for their differential impact introduces a potential misclassification bias. Specifically, because HST estimates the AHI based on total recording time rather than electroencephalogram-confirmed total sleep time, it tends to systematically underestimate baseline OSA severity compared to PSG. However, our study focused on the relative change in airway dynamics and respiratory indices within the same individual under controlled DISE conditions rather than absolute diagnostic classification. The utility of HST for detecting therapeutic trends in AHI and SpO2 in this context is well-supported, providing a valid metric for comparing device efficacy. Third, this study focused on immediate DISE findings and short-term physiological responses during a single session, without long-term follow-up of nightly MAD use, adherence, or clinical outcomes; previous work has reported treatment response rates of around 51% after several months of interim MAD therapy, underscoring the importance of longitudinal data.19 Fourth, the advanced MAD simulator was fabricated without a breathing hole due to procedural and material constraints, limiting direct comparability to many commercially available MADs that incorporate breathing channels to improve airflow.43–45 While the absence of a breathing hole was a design constraint, it inadvertently served as a stress test for the velopharyngeal airway. It demonstrated that without an anterior relief channel (breathing hole), the posterior airway space alone is often insufficient to handle expiratory flow during maximal mandibular advancement. Fifth, the sample sizes within specific anatomical subgroups, particularly the tongue base and oropharynx, were highly limited. This small sample size inherently restricts the statistical power to detect significant differences and increases the margin of error for these specific anatomical sites. Consequently, the subgroup analyses regarding these regions, such as the observed trends toward improvement at the tongue base during head rotation, should not be overinterpreted. These specific findings must be viewed strictly as exploratory and require future validation in larger, adequately powered cohorts. Sixth, our protocol did not incorporate awake objective imaging (eg, lateral cephalograms or cone-beam computed tomography) to evaluate baseline structural differences or quantify the static dimensional expansion of the upper airway provided by the devices. While DISE remains essential for capturing dynamic collapse,46–48 the absence of static imaging limits our ability to correlate awake anatomy with dynamic functional responses. Finally, individual anatomical variations—such as tongue size, palatal length and thickness, lateral wall collapsibility, and craniofacial structure—were not systematically quantified, which may have contributed to heterogeneity in both obstruction patterns and expiratory resistance. Future research should aim to refine MAD designs that preserve the inspiratory benefits of greater mandibular advancement while minimizing EVO, for example by incorporating pressure‑relief valves or active expiratory channels, optimizing breathing-hole geometry, and adjusting vertical opening or other structural parameters. Prospective studies that combine detailed anatomical imaging, DISE phenotyping, and long-term clinical outcomes will be crucial for establishing robust, data-driven algorithms for MAD selection and titration. In parallel, interdisciplinary collaboration among dentists, otolaryngologists, sleep physicians, and primary care providers will be essential to translate these mechanistic insights into practical, individualized treatment pathways that improve both efficacy and tolerability across diverse OSA populations.
Conclusion
In this exploratory simulation, the advanced, maximally protrusive MAD simulator demonstrated a potential for enhanced resolution of upper airway obstruction compared to the conventional OA, particularly at the velum and epiglottis, with corresponding improvements in respiratory indices. Younger age, lower BMI, and milder baseline AHI severity were identified as potential predictors of response, supporting the hypothesis for DISE-guided, phenotype-based patient selection. However, aggressive advancement was associated with a significant increase in the incidence of EVO. These preliminary findings suggest that optimal management therefore requires balancing inspiratory patency with expiratory airflow preservation, which must be further validated in prospective longitudinal clinical trials.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, TY Chen and CCH Yang, upon reasonable request.
Ethics Approval and Consent to Participate
This study complies with the highest ethical standards, having obtained IRB approvals (IRB No. 20231105R) from Shin Kong Wu-Ho-Su Memorial Hospital, and was conducted according to the Declaration of Helsinki and STROBE guidelines. Informed consent was obtained, and all data were anonymized.
Author Contributions
Shih-Chieh Lo and Ying-Shuo Hsu contributed equally as first Authors.
Tien-Yu Chen and Cheryl C. H. Yang contributed equally as Corresponding Authors.
Shih‑Chieh Lo: Conceptualization, Methodology, Formal analysis, Writing - original draft, Writing - review & editing.
Ying‑Shuo Hsu: Conceptualization, Methodology, Formal analysis, Writing - original draft, Writing - review & editing.
Yun‑Hsuan Lin: Conceptualization, Data curation, Formal analysis, Writing - original draft, Writing - review & editing.
Yu‑En Kuo: Conceptualization, Data curation, Formal analysis, Writing - original draft, Writing - review & editing.
Tien‑Yu Chen: Conceptualization, Methodology, Formal analysis, Funding acquisition, Supervision, Writing - original draft, Writing - review & editing.
Cheryl C. H. Yang: Conceptualization, Methodology, Formal analysis, Supervision, Writing - original draft, Writing - review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Science and Technology Council (NSTC), Taiwan [Grant No. 2024NSTCADR003]; Shin Kong Wu Ho-Su Memorial Hospital [Grant No. 2025SKHADR024]; and the Tri-Service General Hospital Research Foundation [Grant No. TSGH-D-115148]. We gratefully acknowledge their support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Peppard PE, Young T, Palta M, Skatrud J. Prospective study of the association between sleep-disordered breathing and hypertension. N Engl J Med. 2000;342(19):1378–16. doi:10.1056/NEJM200005113421901
2. Reichmuth KJ, Austin D, Skatrud JB, Young T. Association of sleep apnea and type II diabetes: a population-based study. Am J Respir Crit Care Med. 2005;172(12):1590–1595. doi:10.1164/rccm.200504-637OC
3. Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med. 2005;353(19):2034–2041. doi:10.1056/NEJMoa043104
4. Engleman HM, Douglas NJ. Sleep. 4: sleepiness, cognitive function, and quality of life in obstructive sleep apnoea/hypopnoea syndrome. Thorax. 2004;59(7):618–622. doi:10.1136/thx.2003.015867
5. Maniaci A, Iannella G, Cocuzza S, et al. Molecular determinants of obstructive sleep apnea. Sleep Med. 2021;80:11–21. doi:10.1016/j.sleep.2021.01.032
6. Strausz S, Ruotsalainen S, Ollila HM, et al. Genetic analysis of obstructive sleep apnoea discovers a strong association with cardiometabolic health. Eur Respir J. 2021;57(5):2003091. doi:10.1183/13993003.03091-2020
7. Smardz J, Martynowicz H, Dratwa-Kuzmin M, et al. The importance of dopamine levels and single-nucleotide polymorphism within COMT, DRD1 and DRD2 genes in obstructive sleep apnoea. Ann Med. 2025;57(1):2548386. doi:10.1080/07853890.2025.2548386
8. Kanclerska J, Wieckiewicz M, Nowacki D, et al. Sleep architecture and vitamin D in hypertensives with obstructive sleep apnea: a polysomnographic study. Dent Med Probl. 2024;61(1):43–52. doi:10.17219/dmp/172243
9. Kushida CA, Littner MR, Hirshkowitz M, et al. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep-related breathing disorders. Sleep. 2006;29(3):375–380. doi:10.1093/sleep/29.3.375
10. Ramar K, Dort LC, Katz SG, et al. Clinical practice guideline for the treatment of obstructive sleep apnea and snoring with oral appliance therapy: an update for 2015. J Clin Sleep Med. 2015;11(7):773–827. doi:10.5664/jcsm.4858
11. Uniken Venema JAM, Doff MHJ, Joffe-Smole D, et al. Long-term obstructive sleep apnea therapy: a 10-year follow-up of mandibular advancement device and continuous positive airway pressure. J Clin Sleep Med. 2020;16(3):353–359. doi:10.5664/jcsm.8204
12. Doff MH, Hoekema A, Wijkstra PJ, et al. Oral appliance versus continuous positive airway pressure in obstructive sleep apnea syndrome: a 2-year follow-up. Sleep. 2013;36(9):1289–1296. doi:10.5665/sleep.2948
13. Chiu FH, Chang Y, Liao WW, et al. Post-operative sleep endoscopy with target-controlled infusion after palatopharyngoplasty for obstructive sleep apnea: anatomical and polysomnographic outcomes. Nat Sci Sleep. 2021;13:1181–1193. doi:10.2147/NSS.S311702
14. Croft CB, Pringle M. Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci. 1991;16(5):504–509. doi:10.1111/j.1365-2273.1991.tb01050.x
15. Safiruddin F, Koutsourelakis I, de Vries N. Upper airway collapse during drug induced sleep endoscopy: head rotation in supine position compared with lateral head and trunk position. Eur Arch Otorhinolaryngol. 2015;272(2):485–488. doi:10.1007/s00405-014-3215-z
16. Cavaliere M, De Luca P, De Santis C, et al. Drug-induced sleep endoscopy (DISE) with simulation bite to predict the success of oral appliance therapy in treating obstructive sleep apnea/hypopnea syndrome (OSAHS). Transl Med UniSa. 2020;23(4):58–62. doi:10.37825/2239-9747.1011
17. Shih HW, Chen YL, Lin HC, et al. Potential treatments for epiglottic collapse in obstructive sleep apnea: how modified drug-induced sleep endoscopy help? Otolaryngol Head Neck Surg. 2024;170(3):792–799. doi:10.1002/ohn.572
18. Lin HC, Wu CH, Kuo TBJ, et al. Upper airway surgery or weight control? Modified drug-induced sleep endoscopy for obstructive sleep apnea. Otolaryngol Head Neck Surg. 2023;169(5):1300–1307. doi:10.1002/ohn.364
19. Bosschieter PFN, Uniken Venema JAM, Vonk PE, et al. An interim oral appliance as a screening tool during drug-induced sleep endoscopy to predict treatment success with a mandibular advancement device for obstructive sleep apnea. Sleep Breath. 2023;27(3):1045–1053. doi:10.1007/s11325-022-02689-w
20. Vroegop AV, Vanderveken OM, Dieltjens M, et al. Sleep endoscopy with simulation bite for prediction of oral appliance treatment outcome. J Sleep Res. 2013;22(3):348–355. doi:10.1111/jsr.12008
21. Bosschieter PFN, Uniken Venema JAM, Vonk PE, et al. Equal effect of a noncustom vs a custom mandibular advancement device in treatment of obstructive sleep apnea. J Clin Sleep Med. 2022;18(9):2149–2157. doi:10.5664/jcsm.10058
22. Johal A, Aarab G. Ready-made versus custom-made mandibular advancement appliances in obstructive sleep apnea: a systematic review and meta-analysis. J Sleep Res. 2018;27(6):e12660. doi:10.1111/jsr.12660
23. Suzuki Y, Finkel A, Kim E, et al. The most effective amount of forward movement for oral appliances for obstructive sleep apnea: a systematic review. Int J Environ Res Public Health. 2019;16(18):3248. doi:10.3390/ijerph16183248
24. Marklund M, Verbraecken J, Randerath W. Non-CPAP therapies in obstructive sleep apnoea: mandibular advancement device therapy. Eur Respir J. 2012;39(5):1241–1247. doi:10.1183/09031936.00144711
25. Bamagoos AA, Cistulli PA, Sutherland K, et al. Dose-dependent effects of mandibular advancement on upper airway collapsibility and muscle function in obstructive sleep apnea. Sleep. 2019;42(6):zsz049. doi:10.1093/sleep/zsz049
26. Bosschieter PFN, Vonk PE, de Vries N. The predictive value of drug-induced sleep endoscopy for treatment success with a mandibular advancement device or positional therapy for patients with obstructive sleep apnea. Sleep Breath. 2022;26(3):1153–1160. doi:10.1007/s11325-021-02501-1
27. Fernández-Sanjuán P, Alvarez M, Blanco G, et al. Modifications in upper airway collapsibility during sleep endoscopy with a mandibular positioner: study in snorers and obstructive sleep apnea patients. J Clin Med. 2024;13(5):1184. doi:10.3390/jcm13051184
28. Thurnheer E, Dieltjens M, Vroegop AE, et al. Effect of mandibular advancement device treatment on the site-specific degree of upper airway collapse during drug-induced sleep endoscopy. J Clin Med. 2025;14(22):8142. doi:10.3390/jcm14228142
29. Hsu YS, Kuo YK, Kuo TBJ, et al. Expiratory velopharyngeal obstruction: sleep endoscopy-guided treatment strategies to prevent oral breathing during sleep. Otolaryngol Head Neck Surg. 2024;171(5):1234–1242. doi:10.1002/ohn.902
30. Jau JY, Kuo TBJ, Li LPH, et al. Mouth puffing phenomenon and upper airway features may be used to predict the severity of obstructive sleep apnea. Nat Sci Sleep. 2023;15:153–164. doi:10.2147/NSS.S384387
31. Lee YC, Lu CT, Cheng WN, Li HY. The impact of mouth-taping in mouth-breathers with mild obstructive sleep apnea: a preliminary study. Healthcare. 2022;10(9):1755. doi:10.3390/healthcare10091755
32. Jau JY, Kuo TBJ, Li LPH, et al. Mouth puffing phenomena of patients with obstructive sleep apnea when mouth-taped: device’s efficacy confirmed with physical video observation. Sleep Breath. 2023;27(1):153–164. doi:10.1007/s11325-022-02588-0
33. Kuo YH, Liu TJ, Chiu FH, et al. Novel intraoral negative airway pressure in drug-induced sleep endoscopy with target-controlled infusion. Nat Sci Sleep. 2021;13:2087–2099. doi:10.2147/NSS.S327770
34. Erman MK, Stewart D, Einhorn D, Gordon N, Casal E. Validation of the ApneaLink for the screening of sleep apnea: a novel and simple single-channel recording device. J Clin Sleep Med. 2007;3(4):387–392. doi:10.5664/jcsm.26861
35. Cho JH, Kim HJ. Validation of ApneaLink™ Plus for the diagnosis of sleep apnea. Sleep Breath. 2017;21(3):799–807. doi:10.1007/s11325-017-1532-3
36. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring respiratory events in sleep: update of the 2007 AASM manual for the scoring of sleep and associated events. Deliberations of the sleep apnea definitions task force of the American academy of sleep medicine. J Clin Sleep Med. 2012;8(5):597–619. doi:10.5664/jcsm.2172
37. Marques M, Grote L, Schwarz EI, et al. Effect of sleeping position on upper airway patency in obstructive sleep apnea is determined by the pharyngeal structure causing collapse. Sleep. 2017;40(3):zsx005. doi:10.1093/sleep/zsx005
38. Tsuiki S, Kim JM, Kim J, et al. Head rotation improves airway obstruction, especially in patients with less severe obstructive sleep apnea without oropharyngeal collapse. PLoS One. 2022;17(5):e0268455. doi:10.1371/journal.pone.0268455
39. Katori K, Watanabe T, Yanagisawa M, et al. A newly discovered tendon between the genioglossus muscle and epiglottic cartilage identified by histological observation of the pre-epiglottic space. Dysphagia. 2023;38(1):285–292. doi:10.1007/s00455-022-10469-7
40. Amatoury J, Kairaitis K, Wheatley JR, Bilston LE, Amis TC. Peripharyngeal tissue deformation, stress distributions, and hyoid bone movement in response to mandibular advancement. J Appl Physiol. 2015;118(3):282–291. doi:10.1152/japplphysiol.00668.2014
41. Borggreven AMEH, Vonk PE, de Vries N. Drug-induced sleep endoscopy: the effect of different passive maneuvers on the distribution of collapse patterns of the upper airway in obstructive sleep apnea patients. Sleep Breath. 2018;22(4):1121–1127. doi:10.1007/s11325-018-1732-5
42. Azarbarzin A, Sands SA, Marques M, et al. Palatal prolapse as a signature of expiratory flow limitation and inspiratory palatal collapse in patients with obstructive sleep apnoea. Eur Respir J. 2018;51(2):1701419. doi:10.1183/13993003.01419-2017
43. Clark GT. Mandibular advancement devices and sleep disordered breathing. Sleep Med Rev. 1998;2(3):163–174. doi:10.1016/s1087-0792(98)90019-3
44. Marklund M, Franklin KA, Sahlin C, Lundgren R. The effect of a mandibular advancement device on apneas and sleep in patients with obstructive sleep apnea. Chest. 1998;113(3):707–713. doi:10.1378/chest.113.3.707
45. Lei H, Wang Z, Yang Y, Chen M. The development of a novel bidirectional fine-tuning mandibular advancement device. BMC Oral Health. 2024;24(1):865. doi:10.1186/s12903-024-04619-6
46. Vroegop A, Eijsvogel D, Zhang C. The clinical application progress and potential of drug-induced sleep endoscopy in obstructive sleep apnea. Ann Med. 2022;54(1):3109–3120. doi:10.1080/07853890.2022.2134586
47. Peng D, Kim JS, Hong SJ. Obstruction patterns during drug-induced sleep endoscopy vs natural sleep endoscopy in patients with obstructive sleep apnea. JAMA Otolaryngol Head Neck Surg. 2019;145(8):723–731. doi:10.1001/jamaoto.2019.1437
48. Certal VF, Pratas R, Guimarães L, et al. Awake examination versus DISE for surgical decision making in patients with OSA: a systematic review. Laryngoscope. 2016;126(3):768–774. doi:10.1002/lary.25722
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.