Back to Journals » Patient Preference and Adherence » Volume 10
Managing neurogenic bowel dysfunction: what do patients prefer? A discrete choice experiment of patient preferences for transanal irrigation and standard bowel management
Authors Nafees B, Lloyd AJ, Ballinger R, Emmanuel A
Received 10 September 2015
Accepted for publication 28 November 2015
Published 17 February 2016 Volume 2016:10 Pages 195—204
DOI https://doi.org/10.2147/PPA.S96082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Beenish Nafees,1 Andrew J Lloyd,2 Rachel S Ballinger,2 Anton Emmanuel3
1Health Outcomes Research, Nafees Consulting Limited, London, 2Patient-Reported Outcomes Research, ICON plc, Oxford, 3Department of Gastroenterology and Nutrition, University College Hospital, London, UK
Background: Most patients with bowel dysfunction secondary to neurological illness are managed by a range of nonsurgical methods, including dietary changes, laxatives, and suppository use to transanal irrigation (TAI). The aim of the present study was to explore individuals’ preferences regarding TAI devices and furthermore investigate willingness to pay (WTP) for attributes in devices in the UK.
Methods: A discrete choice experiment survey was conducted to evaluate the patients’ perceived value of TAI devices. Attributes were selected based upon a literature review and input from clinicians. Interviews were conducted with three clinicians and the survey was developed and finalized with the input from both patients and professionals. The final attributes were “risk of urinary tract infections” (UTIs), “risk of fecal incontinence” (FI), “frequency of use”, “time spent on toilet”, “ease of use”, “level of control/independence”, and “cost”. Participants were recruited by a patient panel of TAI device users in the UK. Data were analyzed using the conditional logit model whereby the coefficients obtained from the model provided an estimate of the (log) odds ratios (ORs) of preference for attributes. WTP was also estimated for each attribute.
Results: A total of 129 participants were included in the final analyses. Sixty two percent of the participants had suffered from three UTIs in the preceding year and 58% of patients reported currently experiencing FI using their current device. All attributes were significant predictors of choice. The most important attributes for participants were the “risk of FI”, “frequency of use”, and “risk of UTIs”.
Conclusion: Participants with bowel dysfunction regarded “risk of FI”, “frequency of use”, and “avoiding UTIs” as the most important features of a TAI device. These preferences are valuable in informing decision makers and clinicians regarding different bowel management solutions as well as for development of future devices.
Keywords: neurogenic bowel dysfunction, UK, transanal irrigation, patient preference, discrete choice
Introduction
Damage to the central nervous system (either brain or spinal cord) can have a significant impact on the function of the bowel and the patients’ ability to maintain fecal continence. Neurogenic bowel dysfunction (NBD) affects ~80% of spinal cord injury (SCI) patients to some degree1 and is also prevalent among patients with other neurological conditions such as multiple sclerosis (MS) and spina bifida (SB).2 Up to 30% of MS patients can experience fecal incontinence (FI).3
Bowel dysfunction can affect patients’ psychological, physical, and social well-being because of constipation, FI, the extended time spent on defecation, and the social restrictions that bowel dysfunction imposes on the patient.4,5 Liu et al6 evaluated the health status of 128 participants with spinal cord injuries (SCIs) using the Short Form 12 (SF-36) and a NBD score. Almost 50% of participants had moderate to severe NBD (moderate score 10–13, and severe dysfunction score ≥14) and this was associated with poorer physical functioning. Coggrave et al7 also showed that NBD had an impact on longer duration of care, more frequent episodes of FI, more frequent management, and more than one intervention was used including stimulant laxatives, osmotics, and bulk formers. Furthermore, 58% of the participants spent up to 30 minutes on each bowel care episode.7
Approaches to management of NBD include dietary changes, digital anal stimulation, laxatives and suppositories, manual evacuation, and transanal irrigation (TAI).8,9 The majority of bowel management methods can be time consuming, which increases the burden for patients.10
TAI is designed to assist the evacuation of feces from the bowel by introducing water into the rectum via a manual pump. TAI devices are commercially available and can be offered as part of a bowel management program to patients. TAI has been shown to be a significantly efficient health technology for improving constipation, FI, and symptom-related quality of life in adult SCI patients when compared to conservative bowel management.11 TAI has also been shown to improve bowel function in children SB.12,13
However, evidence suggests that as many as 40% of the patients who start TAI have discontinued within 3 years.14,15 Adherence may be better understood by identifying the value that patients place on the features and benefits of TAI. This could also potentially guide patient selection and future development of TAI devices. Patient preference surveys can be used to assess the value of different features of a device. The discrete choice experiment (DCE) methodology has been widely used to elicit preferences for this purpose.16 This method can capture benefits in terms of willingness to pay (WTP), which is an estimation of the maximum amount a user may be willing to pay out of pocket in order to receive the benefits of the device. DCEs identify the key characteristics of a product (referred to as “attributes”) with different levels associated with each attribute. Levels describe the various aspects of each attribute, eg, a device could be easy to use, or require several steps and each of these would be a level of the attribute. Hypothetical choices are then presented to participants in pairs, which feature distinct levels of each attribute. Participants are asked to indicate their choice of preference, and regression models can be used to understand the influence of each of the study attributes on participants’ choices.
The aim of the present study was to elicit the preferences of patients with NBD (related to SCI, MS, and SB) with regard to TAI as well as other standard approaches to bowel management.
Materials and methods
Identification of attributes
To determine which aspects of using TAI may be most important to people with NBD, information on currently available bowel management approaches was reviewed. This included studies regarding best practice of TAI in adults and the cost-effectiveness of using this approach compared with standard bowel management.15,17 The information was used to develop a list of potential device attributes and levels which could be included in a DCE.
Seven key attributes were selected in order to ensure that the survey was not too long or burdensome for participants but was still able to capture information regarding different features of the device. The attributes reflected the different aspects of currently available treatments and the studies that showed the impact of devices on daily functioning. Selected attributes and levels identified by the study team, were explored by clinician and patient interviews (as described in the following section), and are shown in Table 1.
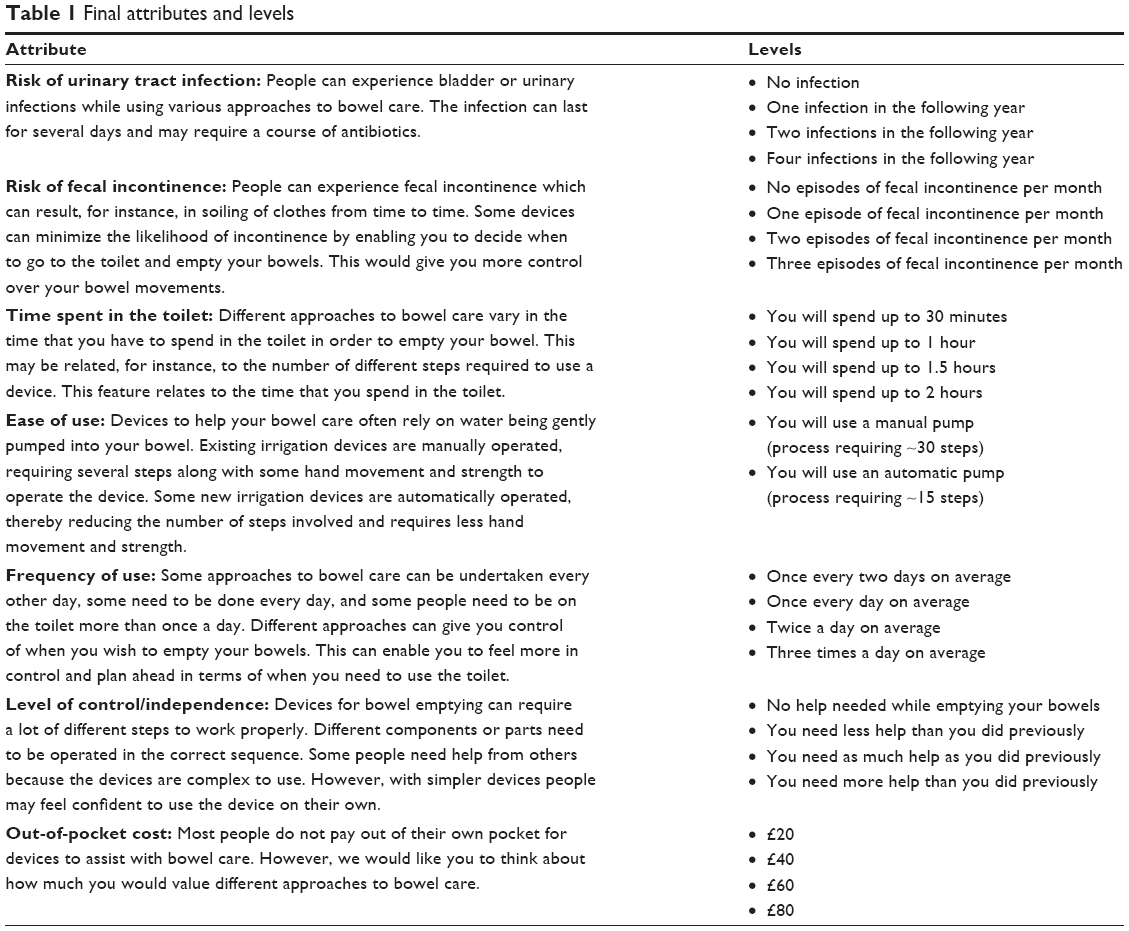 | Table 1 Final attributes and levels |
Development of DCE survey
The attributes and levels were combined into choice sets using a published orthogonal array (http://neilsloane.com/oadir/). An orthogonal fractional factorial design was used to identify the minimum specification of the DCE experimental design in order to fairly represent combinations of the attributes and levels. These combinations were paired using a fold-over design. Each choice question presented two TAI devices (device A or B) and participants were asked to indicate their choice of preference. In addition, participants were also presented with a third choice, which was designed to reflect a standard or conventional approach to bowel management, which did not include anal irrigation. The conventional approach relied upon the use of suppositories and laxatives, or antidiarrheal products; active monitoring of diet and fluid intake; use of incontinence pads on a daily basis; and some use of digital evacuation to empty the bowel. The third option remained constant in each choice question in the survey.
The survey included 17 pairs of choice sets (each also combined with the conventional approach). This included 16 choices from the statistical design plus an additional choice to permit an assessment of consistency. The consistency check involved device A, which was better than device B on every attribute. In addition, participants were asked to state whether they would choose their selected device over their current bowel care plan.
Background information regarding sociodemographics, experience of current device, medical history, and health-related quality of life (HRQL) assessed using EuroQoL-5D (EQ-5D-3L),18 was collected. The EQ-5D-3L categorizes participants into health states based upon five domains (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and provides an estimate of each person’s health state utility (ranging from 1 which is full health through 0 which is dead). Participants also completed the St Mark’s FI score which is a validated self-reported measure of the severity of FI.19 Each domain has a score of 0–4 and the total score is a sum of all domain scores where 0 is perfect continence and 24 is totally incontinent. The Cleveland Clinic Constipation Scoring System was also completed by participants to evaluate the severity of constipation in the sample.20 The total score is a sum of all domain scores from 0–4, with a maximum score of 30. Higher scores represent significant constipation.
An electronic version of the DCE survey in a format appropriate for administration via the web was developed. This was designed to be user-friendly. Prior to patient interviews and main online survey, all study documentation was approved by a US Institutional Review Board (Salus IRB) (REF OXO-0649-0016). Online consent was obtained from all participants before they completed the survey.
Expert interviews
Semi-structured telephone interviews with three clinical experts in the field of bowel management were undertaken. The identified attributes and levels were discussed with the three clinical specialists (gastroenterologist and specialists in bowel care) in order to explore their views on their appropriateness.
Patient interviews
Telephone-based interviews with three individuals in UK suffering from NBD were conducted to explore their understanding of the survey questions. The individuals were asked to complete the survey and participate in a cognitive debrief exercise in which they could comment on the clarity of the questions, the response options, and ease of completion of the overall survey.
Overall, the participants found that the survey was easy to understand and complete and some minor inputs were implemented in the final DCE survey. Descriptions of the attributes were programmed into the online survey so that participants could refer back if needed. Some changes were made to the descriptions of each feature of the device to make them easier to understand.
Main study
Sample
Participants were recruited through a panel of patients in the UK who have used TAI products of one manufacturer (Coloplast; Humlebaek, Denmark) at some stage. Inclusion criteria included participants who: 1) had a diagnosis of SCI, MS, or SB; 2) had used a bowel management program for a minimum of 3 months; 3) had used a bowel management program previously or currently including a TAI device; 4) were aged between 18 and 85 years; 5) had access to the internet; and 6) were currently residing in the UK. Exclusion criteria included an acute illness or cognitive impairment that in the opinion of the interviewer would interfere with the study requirements. All potential participants were required to provide online consent before access to the DCE survey. Participants received a small compensation at the completion of the online survey.
Data analysis
Sociodemographic and medical information were analyzed as means, standard deviations (SDs), and frequencies or percentages. The EQ-5D-3L was scored using standard UK preference weights, whereby full health has a value of 1.0 and dead has a value of 0.
The choice data were analyzed using a conditional logit model to explore the impact of each attribute on participants’ choices.21 The conditional logit model evaluates choice responses after conditioning them on the attributes of the other alternatives available within the choice set. Hence, if, for example, “device option A” is preferred in the choice set 1, this preference is conditional on the attributes of “device option B”. The coefficients obtained from the logit model provide an estimate of the (log) odds ratios (ORs) of preference for attributes. Within each attribute one level was set as a reference point and participants’ strength of preference for achieving other levels of the attribute was estimated (Table 5). WTP was calculated by dividing the estimated coefficients for each attribute by the coefficient for out-of-pocket cost (so-called marginal rates of substitution).
Results
Participant characteristics
A total of 143 participants completed the study questionnaires, of which 14 participants were excluded due to failure on the consistency check. This resulted in a data set of 129 participants of which 48 were diagnosed with SCI, 69 with MS, and 12 with SB.
Table 2 presents the sociodemographic profile of the sample. The mean overall duration of having a condition was 18.7 years. By condition, the participants suffering from SB had an average of 44 years (range: 20–66 years) for this lifelong condition, whereas those suffering from SCI and MS reported having their condition for an average of 15 (range: 1–48) and 17 (range: 1–44) years (data not shown), respectively. Eighty-three percent of the participants had not used an anal irrigation system for bowel management prior to the current one, but laxatives/suppositories had been used by 68% of the sample. “Insufficient effect”, “bowel incontinence”, and “emptying bowel takes too long” were the three main reasons for discontinuing previous bowel management approach. HRQL (as assessed by the EQ-5D index score) for the total data set was 0.37 (SD =0.32), but for the participants with SB it was 0.52 (data not shown). This study also reports data from the St Mark’s Fecal Incontinence measure and Cleveland Clinic Constipation Scoring System, and these data indicate a moderate level of problems on both of these scales. Table 3 presents the clinical history/bowel care approach of the data set. All except two participants had a bowel care plan, which was discussed with a health care professional. The majority of participants currently used various methods, such as TAI, laxatives/suppositories, FI pads, abdominal massage, etc, to empty their bowel.
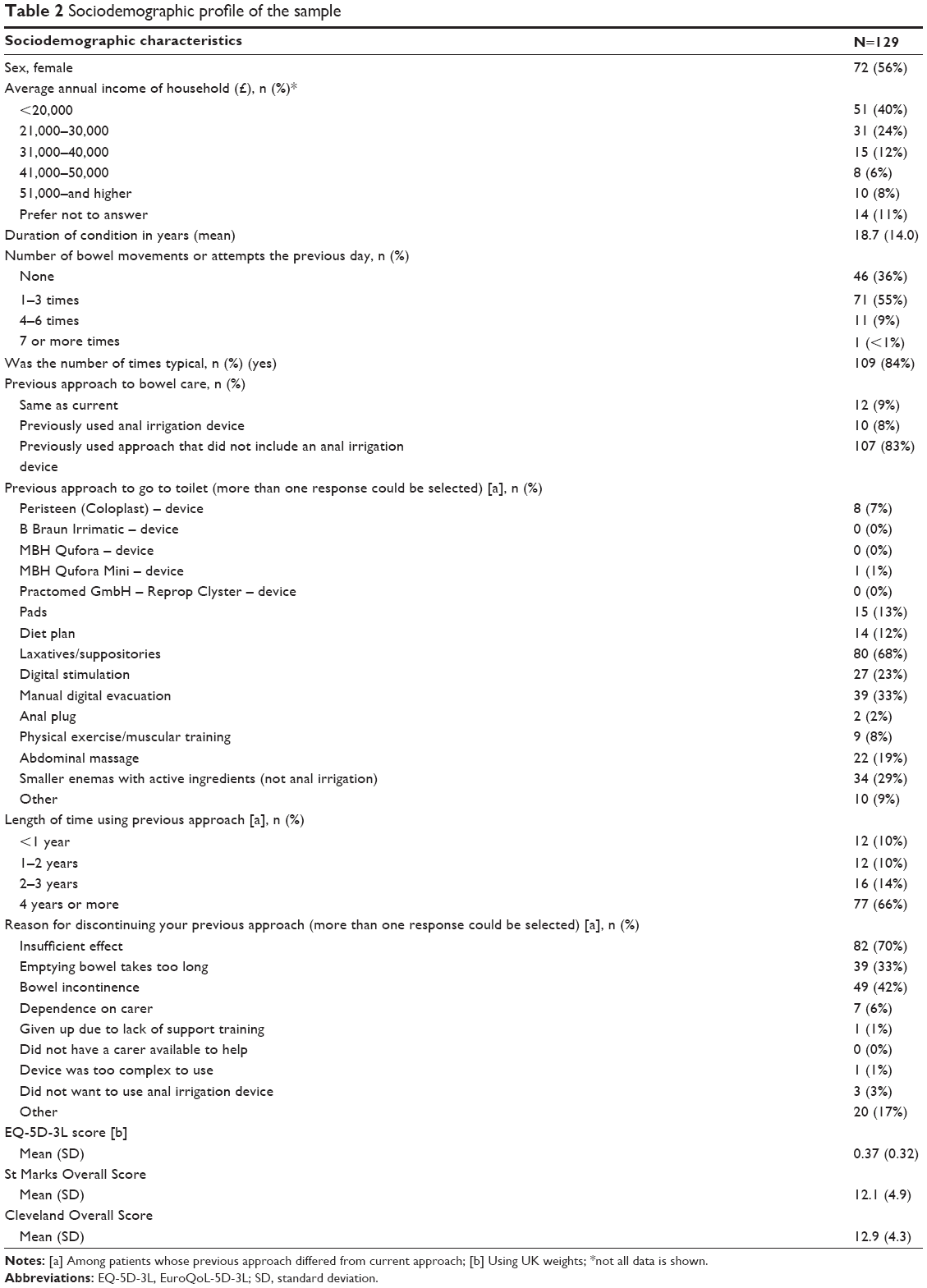 | Table 2 Sociodemographic profile of the sample |
 | Table 3 Clinical profile of the sample |
Participants were asked to describe their current TAI device in relation to the attributes of the DCE (Table 4). Sixty two percent of the participants had experienced a urinary tract infection (UTI) in the previous year and on average they had just over three UTIs requiring antibiotics in the previous year. Fifty eight percent of the participants reported experiencing FI using their current device. However, 33% of those had not experienced any FI during the previous month and 43% had experienced one or two episodes of FI during the previous month. The majority (89%) of the participants used a manually operated device. Most participants emptied their bowel on the toilet (Table 3), 59% used the toilet once every 2 days, and 71% did not require help when going to the toilet. The majority (90%) of the participants did not pay out of pocket for the bowel care and those that had an out-of-pocket cost paid an average of £19 per month.
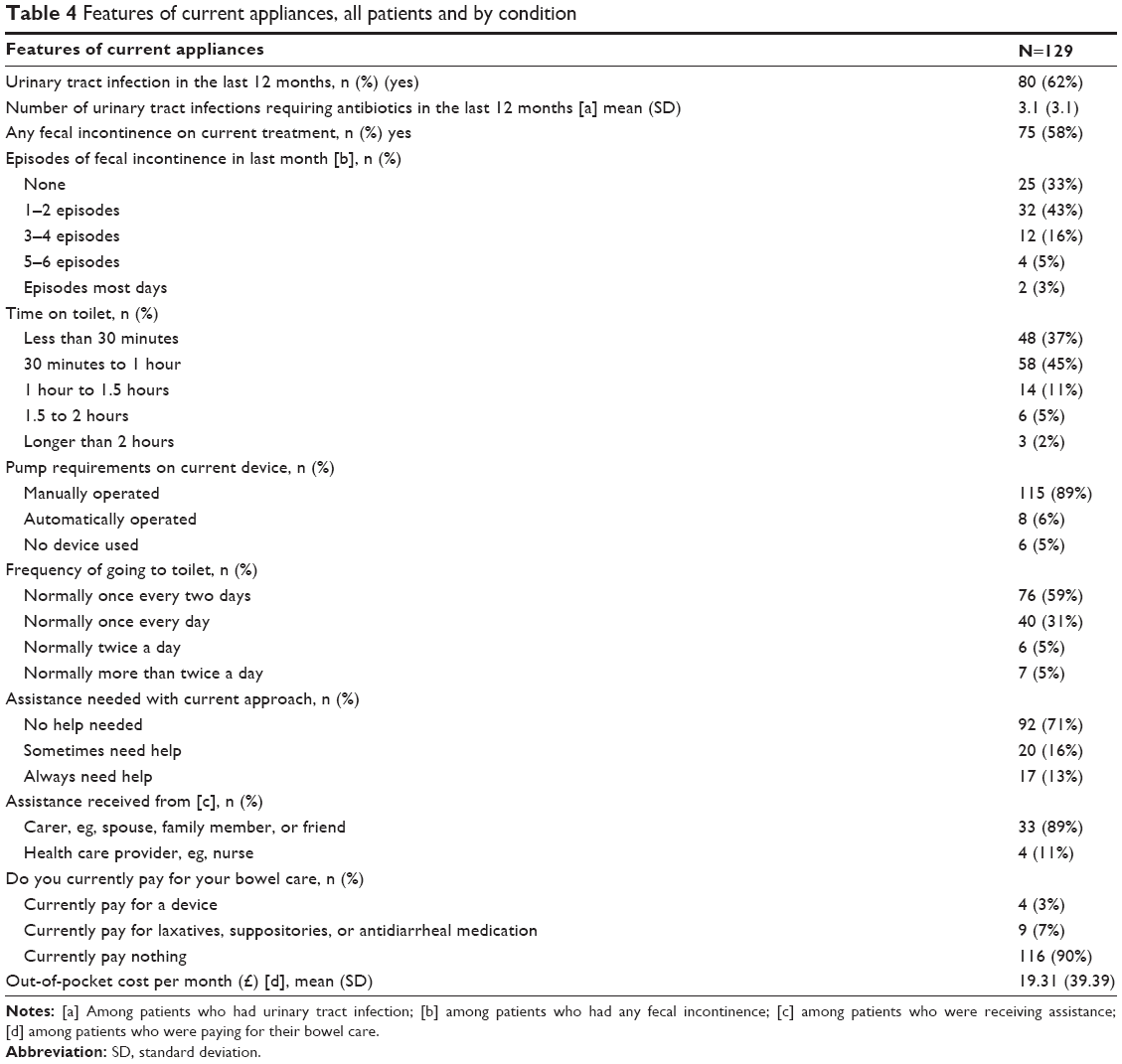 | Table 4 Features of current appliances, all patients and by condition |
DCE findings
All attributes were significant predictors of choice (Table 5) except two levels of “level of control/independence” (“less help than previously” and “as much help as previously”). This means that all of the significant attributes and levels were independent and important drivers of people’s choice. The most highly valued attributes were risk of FI (OR =5.18) and frequency of use (OR =4.69). The OR means that all other attributes being equal, participants in the survey were five times more likely to prefer a device that was associated with no episodes of FI compared with a device that was likely to cause three episodes of FI per month. Participants preferred a device that led to going to the toilet once in every 2 days rather than three times a day (OR =4.69). Participants also preferred a device that avoided the risk of UTIs completely, than a device that led to four UTIs in the following year (OR =3.43). Participants preferred to minimize the amount of time they spent on the toilet. Compared to spending 2 hours on the toilet, participants strongly preferred reducing this to 30 minutes (OR =2.66). The attribute “ease of use” was designed to understand patients’ preference for an automatic pump compared with a manual pump. The results showed that overall people preferred a manual pump than an automatic pump or no pump (OR =0.88 and 0.30 respectively). Out-of-pocket cost was also a significant attribute, which meant that participants were trading improvements in device attributes against increases in cost.
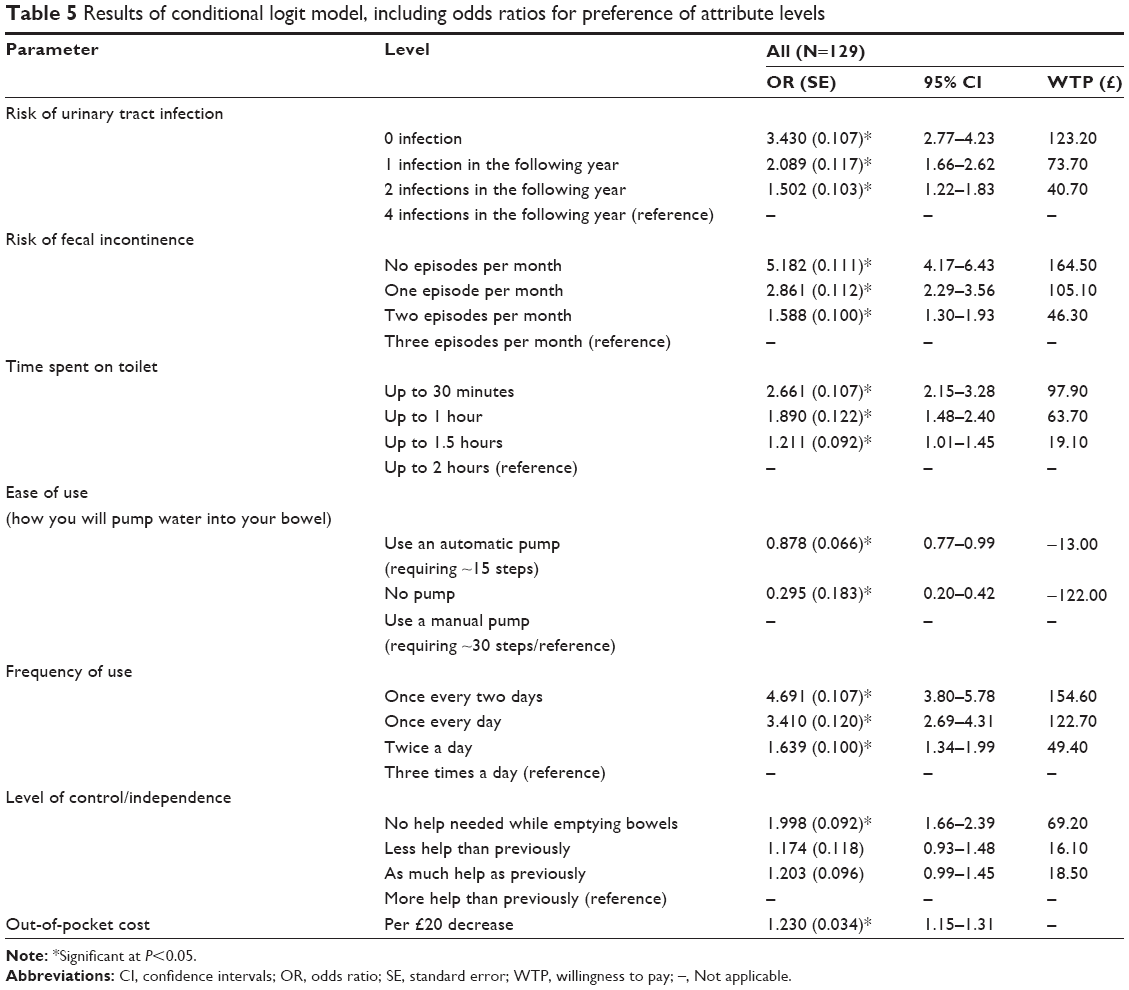 | Table 5 Results of conditional logit model, including odds ratios for preference of attribute levels |
Participants were willing to pay £164.50 and £123.20 per month for a device that could eliminate the risk of FI episodes and avoid all UTIs, respectively. Participants were willing to pay £154.60 for a device that could reduce the frequency of use to once every 2 days. Participants also placed significant value on reducing time spent on the toilet. To reduce the time spent each day from 2 hours to 30 minutes, participants were willing to pay £97.90 per month. Some other device features were valued slightly less highly. For example, participants placed less value (compared to other attributes) on a device that would allow them to be fully independent for bowel management.
An interaction model was explored to see whether preferences varied by condition (SCI, MS, or SB) whereby the reference case was the SCI group. The results showed that there were only differences in patient groups in the attributes “level of control/independence” and “cost” (results are not shown). The SCI group placed significantly more value than the MS group on devices that required “less help than previously” (P<0.05). The MS group were more willing to accept higher out-of-pocket cost compared with the SCI group (P<0.03). The results showed that all three patient groups placed similar value on the other attributes when choosing devices.
Discussion
The key original message emerging from this study is that it reflects user’s perceived value and their WTP for TAI devices. The study used the methodology of a DCE in a group of UK-based patients with neurological disease and secondary bowel dysfunction. The survey explored the importance that users place on seven selected features of a bowel care plan/device.
The majority of the participants had experienced FI and were currently on a bowel care plan, which included a TAI device. Most of the participants were able to empty their bowel on the toilet and did not require any assistance. The sample reported poor HRQL as reflected by low EQ-5D scores. Pinder et al22 conducted a DCE in which they explored preferences of people who use intermittent self-catheterization (ISC) devices in the UK, France, and the Netherlands. People using ISC reported EQ-5D scores between 0.40 and 0.56 in each country which were marginally higher than the current sample. Participants reported moderately severe scores regarding their experience of incontinence and constipation in Pinder et al.22
The seven attributes explored were “risk of UTI”, “risk of FI”, “time spent on toilet”, “ease of use”, “frequency of use”, “level of control/independence”, and “cost”. All attributes were significant predictors of choice except some degrees of “level of control/independence”, demonstrating the relevance of the chosen items to the patient group when considering a new device. TAI therapy, by its nature, requires active patient involvement, in terms of self-administration of the therapy for an intimate function. The relative low priority of independence may reflect that the majority of the sample was independent (only 29% were dependent on a carer to manage their bowel). This is similar to other cohorts with a similar patient population where complete assistance was required by 22.8%.7
Avoiding the risk of FI was the most important attribute for participants. This is consistent with the observation that the prevalence of FI significantly impacts HRQL.9 SCI has a significant impact on bowel function and these changes result in a high risk of FI and constipation.10,23 It is thought that up to 30% of patients with MS can develop regular FI.3 The other most important attributes for participants were the “frequency of use” and “risk of UTIs”. The majority of the sample (62%) reported that they had experienced a UTI in the last 12 months. Taken together, these observations reflect the importance of using patient-related outcomes and defining therapy on a case-by-case basis employing those metrics of patient preference which can transform health care.24
Frequency of use was a very important attribute of choice. Participants preferred a bowel frequency of once every 2 days rather than the traditionally used metric of a daily bowel action.10,23 More than 40% of participants reported a bowel frequency of once a day or more often, and almost two-thirds spent more than 30 minutes on each attempted bowel action. As such, it is not surprising that patients prioritize minimizing the number of bowel movements they have.
Cost was also an important driver of choice for participants. This was an interesting observation given that in the UK, treatment via health care service is free at the point of delivery to patients. Given that people were trading other attributes against cost, it is possible to estimate WTP for significant attributes and levels. The ensuing results indicated how important attributes were in terms of WTP, and also gave an indication of the amounts that participants were willing to pay every month for a device with improved functionality on different attributes. In particular, the results of this study showed that a cost of up to £165 per month was deemed acceptable for a treatment that would eliminate the risk of FI.
There were some important limitations to remember when interpreting this study. Participants were recruited from a panel that included people who had used Coloplast products at some stage, which could result in possible bias in their experience of TAI devices. However, participants did report using a wide range of devices and bowel care plans, and the frequency of use of medications and devices was similar to that in other studies.23 The current study also relied on people completing the survey online, which excluded some users who did not have access to the internet. However, all efforts were made to recruit a representative sample across the UK, including consideration of social stratum. In addition, it should also be noted that the sample size is relatively limited. While the aggregate results are largely clear, the sample is too small for reliably exploring differences between the three neurological diseases. As such, these analyses, which have explored differences between SCI, MS, and SB patients, should be treated as exploratory only. It is also worth commenting that the vast majority of the sample does not currently pay for their TAI devices and associated bowel care. Therefore, this may bias the estimates of WTP because the participants do not have experience of making such purchases. There are, however, examples in the literature where participants in DCE surveys are asked to make choices based upon hypothetical treatments for which they do not currently pay.25
Conclusion
This study assessed users’ preferences regarding TAI devices. “Risk of FI” and “frequency of use” were the most important attributes of devices. The DCE method allows clinicians to identify important features of devices and understand the relative importance of attributes in terms of WTP. Such data are also important in helping care management decisions in an increasingly hard-pressed and complex financial environment of health care funding.
Acknowledgments
This study was supported by research funding from Coloplast A/S to ICON plc. However, no restrictions were placed on the design of the study, the choice of included data sources, the presentation of results, or the content of the final manuscript. Frederikke Bruun Andersen and Zenia M Størling contributed with data interpretation and critical scientific review of the manuscript.
Disclosure
AE has participated on advisory boards for Coloplast, Hollister, and Wellspect, all of whom are developing or have developed TAI devices. BN, AJL, and RB have conducted this study on behalf of Coloplast. The authors report no other conflicts of interest in this work.
References
Krogh K, Nielsen J, Djurhuus JC, Mosdal C, Sabroe S, Laurberg S. Colorectal function in patients with spinal cord lesions. Dis Colon Rectum. 1997;40(10):1233–1239. | ||
Chia YW, Fowler CJ, Kamm MA, Henry MM, Lemieux MC, Swash M. Prevalence of bowel dysfunction in patients with multiple sclerosis and bladder dysfunction. J Neurol. 1995;242(2):105–108. | ||
Rao SS, Tuteja AK, Vellema T, Kempf J, Stessman M. Dyssynergic defecation: demographics, symptoms, stool patterns, and quality of life. J Clin Gastroentrerol. 2004;38(8):680–685. | ||
Glickman S, Kamm MA. Bowel dysfunction in spinal-cord-injury patients. Lancet. 1996;347(9016):1651–1653. | ||
Lynch AC, Wong C, Anthony A, Dobbs BR, Frizelle FA. Bowel dysfunction following spinal cord injury: a description of bowel function in a spinal cord-injured population and comparison with age and gender matched controls. Spinal Cord. 2000;38(12):717–723. | ||
Liu CW, Huang CC, Yang YH, Chen SC, Weng MC, Huang MH. Relationship between neurogenic bowel dysfunction and health-related quality of life in persons with spinal cord injury. J Rehabil Med. 2009;41(1):35–40. | ||
Coggrave M, Norton C, Wilson-Bartnett J. Management of neurogenic bowel dysfunction in the community after spinal cord injury: a postal survey in the United Kingdom. Spinal Cord. 2009;47(4):323–333. | ||
Del Popolo G, Mosiello G, Pilati C, et al; Treatment of neurogenic bowel dysfunction using transanal irrigation: a multicenter Italian study. Spinal Cord. 2008;46(7):517–522. | ||
National Institute for Health and Clinical Excellence. Faecal Incontinence: The Management of Faecal Incontinence in Adults. London: NICE; 2007. Available from: www.nice.org.uk/CG49. Accessed August 1, 2014. | ||
Coggrave M. Transanal irrigation after spinal cord injury. Nurs Times. 2007;103:44–46. | ||
Christensen P, Bazzocchi G, Coggrave M, et al; Outcome of transanal irrigation for bowel dysfunction in patients with spinal cord injury. J Spinal Cord Med. 2008;31(5):560. | ||
Shandling B, Gilmour RF. The enema continence catheter in spina bifida: successful bowel management. J Pediatr Surg. 1987;22(3):271–273. | ||
Eire PF, Cives RV, Gago MC. Faecal incontinence in children with spina bifida: the best conservative treatment. Spinal Cord. 1998;36:774–776. | ||
Christensen P, Andreasen J, Ehlers L. Cost-effectiveness of transanal irrigation versus conservative bowel management for spinal cord injury patients. Spinal Cord. 2009;47:138–143. | ||
Emmanuel AV, Krogh K, Bazzocchi G, et al; Consensus review of best practice of transanal irrigation in adults. Spinal Cord. 2013;51(10):732–738. | ||
Ryan M, Gerard K. Using discrete choice experiments to value health care programmes: current practice and future research reflections. Appl Health Econ Health Policy. 2003;2(1):55–64. | ||
Christensen P, Krogh K, Buntzen S, Payandeh F, Laurberg S. Long-term outcome and safety of transanal irrigation for constipation and fecal incontinence. Dis Colon Rectum. 2009;52(2):286–292. | ||
EuroQol Group. EuroQol – a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199–208. | ||
Vaizey CJ, Carapeti E, Cahill JA, Kamm MA. Prospective comparison of faecal incontinence grading systems. Gut. 1999;44(1):77–80. | ||
Agachan F, Chen T, Pfeifer J, Reissman P, Wexner SD. A constipation scoring system to simplify evaluation and management of constipated patients. Dis Colon Rectum. 1996;39(6):681–685. | ||
Hosmer DW, Lemeshow S. Applied Logistic Regression. New York: Wiley; 1989. | ||
Pinder B, Lloyd AJ, Nafees B, Elkin EP, Marley J. Patient preferences and willingness to pay for innovations in intermittent self-catheters. Patient Prefer Adherence. 2015;9:381–388. | ||
Preziosi G, Raptis DA, Storrie J, Raeburn A, Fowler CJ, Emmanuel A. Bowel biofeedback treatment in patients with multiple sclerosis and bowel symptoms. Dis Colon Rectum. 2011;54(9):1114–1121. | ||
Black N. Patient reported outcome measures could help transform healthcare. BMJ (Clin Res Ed). 2013;346:f167. | ||
Johnson FR, Mohamed AF, Özdemir S, Marshall DA, Phillips KA. How does cost matter in health-care discrete-choice experiments? Health Econ. 2011;20(3):323–330. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.