Back to Journals » Patient Preference and Adherence » Volume 17
Managing Medications and Medication Adherence Among US Adults During the Early Phase of the COVID-19 Pandemic
Authors Bartlett Ellis RJ ![]() , Andrews A, Elomba CD, Remy LM, Ruggeri SY
, Andrews A, Elomba CD, Remy LM, Ruggeri SY ![]() , Russell CL, Ruppar TM
, Russell CL, Ruppar TM ![]()
Received 17 October 2022
Accepted for publication 25 January 2023
Published 11 February 2023 Volume 2023:17 Pages 369—383
DOI https://doi.org/10.2147/PPA.S393749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Johnny Chen
Rebecca J Bartlett Ellis,1 Angela Andrews,2 Charles D Elomba,1 Laura M Remy,3 Sunny Yoo Ruggeri,4 Cynthia L Russell,4 Todd M Ruppar5
1Science of Nursing Care Department, Indiana University, Indianapolis, IN, USA; 2Primary Care and Health Systems, Southern Illinois University-Edwardsville, Edwardsville, IL, USA; 3Optum Infusion Services, Kansas City, MO, USA; 4School of Nursing and Health Studies, Kansas City, Missouri, University of Missouri-Kansas City, Kansas City, MO, USA; 5Department of Adult Health and Gerontological Nursing, Rush University, Chicago, IL, USA
Correspondence: Rebecca J Bartlett Ellis, Science of Nursing Care Department, Indiana University, 600 Barnhill Drive, NU 120, Indianapolis, IN, 46202, USA, Tel +1 317 274 0047, Email [email protected]
Purpose: Before the COVID-19 pandemic and the disruptions it brought, medication adherence was already a challenging and complex health behavior. The purpose of this study was to describe patients’ interactions in clinic, pharmacy, and home contexts and associated medication management and adherence during the early phase of the COVID-19 pandemic.
Patients and Methods: A survey questionnaire was developed using the Medication Adherence Context and Outcomes framework and distributed via social media between May and July 2020 targeting adults taking a daily prescribed medication. Survey questions assessed sociodemographics, interactions with healthcare providers, clinics, pharmacies, medication management experiences, habit strength, and life chaos perceptions during the pandemic. Medication adherence was assessed by the self-report BAASIS© scale to measure implementation, discontinuation, and overall nonadherence.
Results: A total of 134 adults from the United States, mean age 50.0 (SD 16.1) years were included in this analysis. Respondents took a median of 3.50 (interquartile range 4) daily medications. Delays in seeing a provider were reported by 47 (35.1%). Pharmacy encounters were impacted; 25 (18.7%) indicated their method for obtaining medication changed. Medication nonadherence was reported among 62 (46.3%) and was significantly greater among those who delayed prescription refills (p=0.032), pillbox users (p=0.047), and those who experienced greater life chaos (p=0.040) and lower habit strength (p< 0.001) in the early phase of the pandemic.
Conclusion: Although the early phase of the pandemic affected access to care for nearly one-third of the sample, distance-accessible care options and strategies to obtain needed services without being in-person supported respondents medication management. Helpful strategies included provider accessibility, telehealth, home delivery/mail-order, drive-thru’s, 90-day supplies, and online/automatic refills. Methods to develop and reestablish habits are critical. Care providers in clinic and pharmacy settings can educate and remind patients about services like distance-accessible technologies and online ordering of medications and establishing routines to support medication adherence.
Keywords: COVID-19, habits, medication adherence, medication non-adherence, pandemics
Introduction
In the United States (US), more than two-thirds of the population takes at least one prescription medication and more than 70% of health-care visits involve initiating drug therapy.1 Despite the importance of medications, approximately 50% of people experience nonadherence to medication regimens, based on research literature published before the coronavirus disease of 2019 (COVID-19) pandemic.2–4 Medication nonadherence leads to poor clinical outcomes, unnecessary health care costs,5 and increased risk for morbidity and mortality.6
In March 2020, the World Health Organization (WHO) declared the COVID-19 outbreak a pandemic.7 Internationally, protective measures were put in place as the outbreak threatened public health. The US responded with city and state protective measures that altered US citizens mobility behaviors such as stay-at home orders, masking, and social distancing and quarantining procedures to slow the spread of the virus.8
The COVID-19 pandemic and protective measures to slow the spread of the virus significantly disrupted9 life and impacted the healthcare system. COVID-19 protective measures broadly affected daily routines and how and where people accessed work, school, and healthcare including their healthcare providers visits in clinics and pharmacies. To reduce the spread of COVID-19 and alleviate fear of spreading the virus, outpatient appointments were cancelled or converted to telehealth appointments10 and nonemergent and elective procedures were canceled to free healthcare providers availability and hospital beds for COVID-19 surges.11 Outpatient clinics and pharmacies changed their hours, further disrupting health care services and access. Alongside changes in healthcare were changes in business leading to businesses closing or moving to online and remote work. Employment changes resulted in loss of work and health insurance changes. The unemployment rate reached an all-time high of 14.8%, and more than 25 million Americans lost their health insurance.12
The unprecedented disruptions brought on by the pandemic made managing and adherence to medications more complex. Several studies have investigated the effects of the pandemic on nonadherence. Some studies demonstrate increased nonadherence occurred during the pandemic,13–15 yet others suggest that medication taking improved and adherence increased,15,16 while other studies suggest that rates of nonadherence remained relatively unchanged.17 These studies used a variety of adherence measures and focused on disease-specific populations, which might account for the noted differences in adherence findings. Some studies used global measures of adherence which make thorough understanding of the adherence problems difficult and do not provide insight into the adherence phases of initiation, implementation, discontinuation, and persistence. Furthermore, it is unclear how the contexts of clinics, pharmacies, and home were associated with experiences of managing medications and subsequent adherence. Medication adherence requires individuals to engage in multiple behaviors that take place in the context of clinics, pharmacies, and home18,19 as individuals engage in processes that affect their adherence. Clinics, pharmacies, and home are all contexts that were affected by the pandemic.17
Understanding people’s experiences managing medications in clinic, pharmacy, and home contexts in the early phases of the pandemic, when the greatest disruptions occurred, can inform development of durable interventions to supporti adherence in situations that disrupt healthcare delivery and routines. The purpose of this study was to describe US adults’ interactions with healthcare providers within the clinic and pharmacy settings and their home management of prescribed medications and adherence, including implementation and persistence phases of adherence during the early phases of the COVID-19 pandemic.
Materials and Methods
Design/Sample
This descriptive study was conducted via a survey questionnaire delivered by social media and responses obtained between May and July 2020, which was in the early phase of the pandemic. The overall goal of this descriptive study was to recruit 2000 participants over the course of the pandemic. This number was selected based on the number of questions in the survey and the rule of thumb of having at least 10 responses per item.20 Data were collected by a one-time, web-based survey questionnaire delivered by Research Electronic Data Capture (REDCap).21 Study data were collected and managed using the REDCap electronic data capture tools hosted by Indiana University.22,23 REDCap is a widely used secure, web-based application to support investigators to build and deliver online surveys. This study complies with ethical practices including the Declaration of Helsinki24,25 and institutional review board approval was obtained prior to recruitment. This study was approved as an exempt study 2004518613 by the Indiana University Institutional Review Board.
A convenience sample was recruited by social media using targeted Facebook advertisements and organic sharing through social media. We used paid advertisement and recruitment advertisements were shown in US Facebook feeds with the goal of boosting link clicks. Based on Facebook analytics, paid advertisement resulted in 129 link clicks with a total cost of $71.83. The content of the advertisement indicated we were interested in learning how people were managing their medicines during the Coronavirus COVID-19 pandemic. We also encouraged wide sharing and participation for people taking prescribed medication and 18 years of age and older. A button to learn more was included which linked interested individuals to our study information sheet and pre-screening questionnaire link that was a REDCap survey. Prior to accessing the survey questions reported herein, respondents were presented with a study information sheet describing the purpose of the study, identifying the voluntary nature of the survey, the inclusion criteria, anticipated time to complete the study (no more than 30 minutes), the study team members, and contacts for questions or concerns related to the study. A pre-screening questionnaire was created along with the study information sheet. For respondents to progress to the study survey questions, they needed to select a response option that indicated they consented to participate and that they agreed that they were at least 18 years of age, were able to read and understand English language, and had been prescribed any medication by a healthcare provider.
Inclusion and Exclusion Criteria
Participants were included in this study if their self-reported responses indicated that they were taking a daily prescribed oral medication, reported being at least 18 years of age or older. All individuals in this study reported living in the United States. If individuals did not affirm the above inclusion criteria, the survey closed.
Development and Pre-Testing of Survey
The questions used in the survey were developed and/or selected by the study team based on the conceptual framework guiding this study. The survey was designed to be “open” which means anyone with the link could access the survey. Prior to fielding the questionnaire, the study team tested the functionality in a test environment. The full survey questionnaire, including the screening questionnaire, consisted of 135 variable fields, with 12 conditionally displayed based on prior response options. Completing every item in the survey was not required or enforced. A button was available on each page for participants to review prior responses and to save and return later if needed. There were 12 pages in the full survey, designed to help organize the survey questions by content and ease participant burden. The participation rate was 69.4% (n=134) based on individuals who clicked on the initial study information and screening page (n=193) and who then proceeded forward to the survey questionnaire. At the conclusion of the survey, respondents who were interested in entering their name in a drawing for a chance to win one Kindle fire tablet were redirected to a separate REDCap survey. The separate survey to collect personal information for the drawing was created to keep identifiable data separated from the survey data. Of the 113 individuals who clicked on the link to submit their contact information to be entered into a drawing, 91.2% (n=103), did so. We did not collect IP addresses in this study.
Conceptual Framework
Development of the survey questions and selected measures was guided by the Medication Adherence Context and Outcomes (MACO) framework.18,19 This framework reflects that managing medications occurs across three contexts: clinic, pharmacy, and day-to-day home management. Clinic contexts include the communication between patient and provider as people are prescribed new medications or seek to learn more about medications. Pharmacy encounters occur when a patient initially obtains prescribed medications by filling or refilling them. Day-to-day home management encompasses managing, organizing, and taking medications in the context of daily living. See Figure 1.
 |
Figure 1 The conceptual framework based on the MACO framework. Notes: Adapted from Bartlett Ellis RJ, Ruppar TM. (2018 Oct. 4). The Medication Adherence Context and Outcomes Framework Image. Creative Commons Attribution 4.0 International License.26 |
Survey Questionnaire
The survey questionnaire was comprised of individual questions developed by the investigators for this study as well as validated measures (habit strength, chaos, and medication adherence), all described below.
Respondent, Pandemic and Medication Related Characteristics
We included items for individuals to self-report sociodemographic, pandemic, and medication-related characteristics. Sociodemographic characteristics included gender, race, ethnicity, education level, relationship status, employment status, and age. Pandemic-related characteristics included social distancing and masking practices. Medication-taking characteristics included the number of daily oral medications taken.
Clinic Context Independent Variables
Three questions were designed to assess interactions between respondents and their healthcare providers during the pandemic. These questions assessed if respondents had 1) talked with a healthcare provider since beginning social distancing, 2) if respondents had delayed seeking care because of pandemic related concerns, and 3) whether any new medications were prescribed in the last 30 days. Response options were yes/no. For respondents who indicated they had visited a healthcare provider, they were also asked if it was an in-person visit, on the phone, or using telehealth with internet and video. For respondents reporting they delayed visiting a healthcare provider, they were asked for the reasons, with response options of unable to get to the provider office, healthcare provider hours changed, had change in job/insurance and focused on saving money, or afraid to leave home.
Open-Ended Clinic Questions
Respondents were asked three additional open-ended questions about their pandemic experience with clinic services. First, respondents were asked to share if their interactions with their healthcare provider or office had changed related to the COVID-19 pandemic and social distancing measures. Second, they were asked what was helpful for managing medications during social distancing measures. Third, they were asked what they needed to better manage medications during social distancing in relation to their provider and clinic services.
Pharmacy Context Independent Variables
Pharmacy-related questions were designed to assess respondents’ pharmacy interactions and experiences obtaining medications during the pandemic. Respondents were asked if they had obtained a prescription medication, either a new medication or refill, since the beginning of the pandemic. Response options were “yes” or “no”. If they responded “yes”, they were asked to select all options that applied to how they obtained their medications with options of “picked up from pharmacy by self”, “picked up by someone else”, “delivered by pharmacy”, “mail-order” or “other”. Three additional “yes/no” response options were asked, to include 1) if the method for obtaining medications had changed due to the pandemic, 2) if the interaction with the pharmacist or pharmacy changed because of the pandemic, and 3) if respondents had delayed refilling their prescriptions due to the pandemic. For those indicating they “had delayed obtaining a prescription”, they were prompted to respond to the cause of the delay with responses, “unable to get to pharmacy”, “pharmacy hours changed”, “medication not available”, “had a change in job/insurance and cannot afford medication”, “worry about losing job/insurance”, and “afraid to leave home”. Respondents were also asked if they had stopped taking any medications due to inability to refill the medication related to the pandemic, with a “yes/no” response option. For those who indicated “yes”, they were prompted to identify the reason with the same response options provided for those who indicated they had delayed filling a prescription.
Open-Ended Pharmacy Context Questions
Two additional open-ended questions were asked. First, respondents were asked what was helpful from pharmacy and pharmacy services to support managing medications during the pandemic. Second, they were asked whether they had what they needed from the pharmacy or pharmacy services that they did not have during the pandemic.
Home Context Independent Variables
To assess the home context, measures with evidence of validity and reliability for measuring habit strength and interruptions in daily routines (ie, life chaos) in the home were selected. To further assess home management, one single-item question was developed by the team to assess whether respondents used pillboxes or organizers for managing their medications. To assess habit strength, the Self-Report Habit Index,27 shortened to 11 items,28 was used to assess habit of medication taking. This scale measures habits and repetition of behaviors on a Likert-style scale ranging from strongly disagree (=1) to strongly agree (=5) with higher scores indicating stronger habits. Items were reworded to reflect taking medications during the pandemic. Evidence of reliability of the 11-items is reflected in the Cronbach’s alpha coefficient of 0.796 for the present study. To assess life daily routine consistency, we used the 15-item Confusion, Hubbub, and Order Scale (CHAOS) scale.29 This scale was originally developed for parents to assess their children’s home environment29 and has been shown to be associated with medication adherence in other studies.30 Responses were recorded on a 5-point Likert scale with response options strongly agree (=5) to strongly disagree (=1) and summed to a total scale score with lower scores (range 15 to 75) representing greater home chaos and less consistency in daily routines. Respondents were asked to respond to the CHAOS scale reflecting on daily routines before the beginning of the pandemic and at the time of completing the survey to assess the change related to the pandemic. In the present study, Cronbach’s alpha for the 15-item scale was 0.895. Respondents were asked if they used an organizer like a pillbox or dosette to manage medications with response options yes/no.
Dependent Variable: Medication Adherence
The self-report BAASIS© scale31 was used to measure the implementation and persistence phases of medication adherence. This self-report measure has been used to measure adherence in several chronic conditions and validated with electronic monitoring.32–36 This measure was selected for this study because it aligns with the ABC taxonomy definition of adherence37 and can measure implementation and persistence phases of adherence. The implementation phase was assessed by 4 items that focus on taking adherence, timing adherence, drug holidays, and reduction in doses. All items are dichotomous with response options “yes/no” and each item has a follow-up question to assess the frequency of problems occurring with implementation (ie, once, twice, 3 times, or more than 3 times in the past 4 weeks). Any response of “yes” indicates implementation phase problems and is thus classified as nonadherence. Persistence is defined as the duration of time between when a person begins taking medication and when they stop. This was assessed with one dichotomous item (yes/no response) that asks if medication was stopped without consulting provider. Items are summarized individually as the proportion of respondents scoring “yes” to each item.38 If a respondent scored “yes” to any item implementation and persistence items, then they were classified as nonadherent.
Data Analysis
Prior to exporting data from REDCap into SPSS version 27 for data analysis, quality checks were performed within REDCap to identify incorrect data types, out-of-range field validation error and other types of invalid values or incorrect values. Finding no discrepancies beyond missingness and blank values, data were recoded and missingness examined using Missing Values Analysis and data assumed missing completely at random. Sample sizes are reported for each analysis. Normality was assessed using Q-Q plots and the Shapiro–Wilks test. Data were summarized by sociodemographic, medication-taking, and pandemic related characteristics, and clinic, pharmacy, and home context variables based on the MACO contexts. Categorical-level data were summarized using counts and percentages (n/%). Continuous data were presented using means (± standard deviations), and in cases where the Shapiro–Wilks was significant, medians (interquartile range). Differences in self-reported nonadherence and adherence were examined across all variables. For categorical-level variables, the chi-square test was used, and for continuous scale variables independent t-tests and paired t-tests, or the non-parametric alternatives, Mann–Whitney U and Wilcoxon matched-pair signed rank tests were used to examine differences in socio-demographic, pandemic, and medication-related characteristics and MACO framework context-specific variables/measures. Alpha level was set at 0.05. Qualitative responses to open-ended items were organized thematically by content analysis and summarized as counts for each theme. The results are summarized by contexts of medication management that include clinic context variables, pharmacy context variables, home context variables and the primary outcome of interest, medication adherence.
Results
A total of 134 respondents indicated taking at least one prescribed daily oral medication and were included in the analysis. Table 1 shows the sample sociodemographics, medication-taking, and pandemic characteristics. As reflected in Table 1, on average, the sample was middle-aged, white, female, educated at the college level or beyond, married or in a relationship, and most reported working either full-time or part-time at the time they completed the survey. Respondents managed a median of 3.0 (4.0) (minimum 1, maximum 18) prescription medications daily.
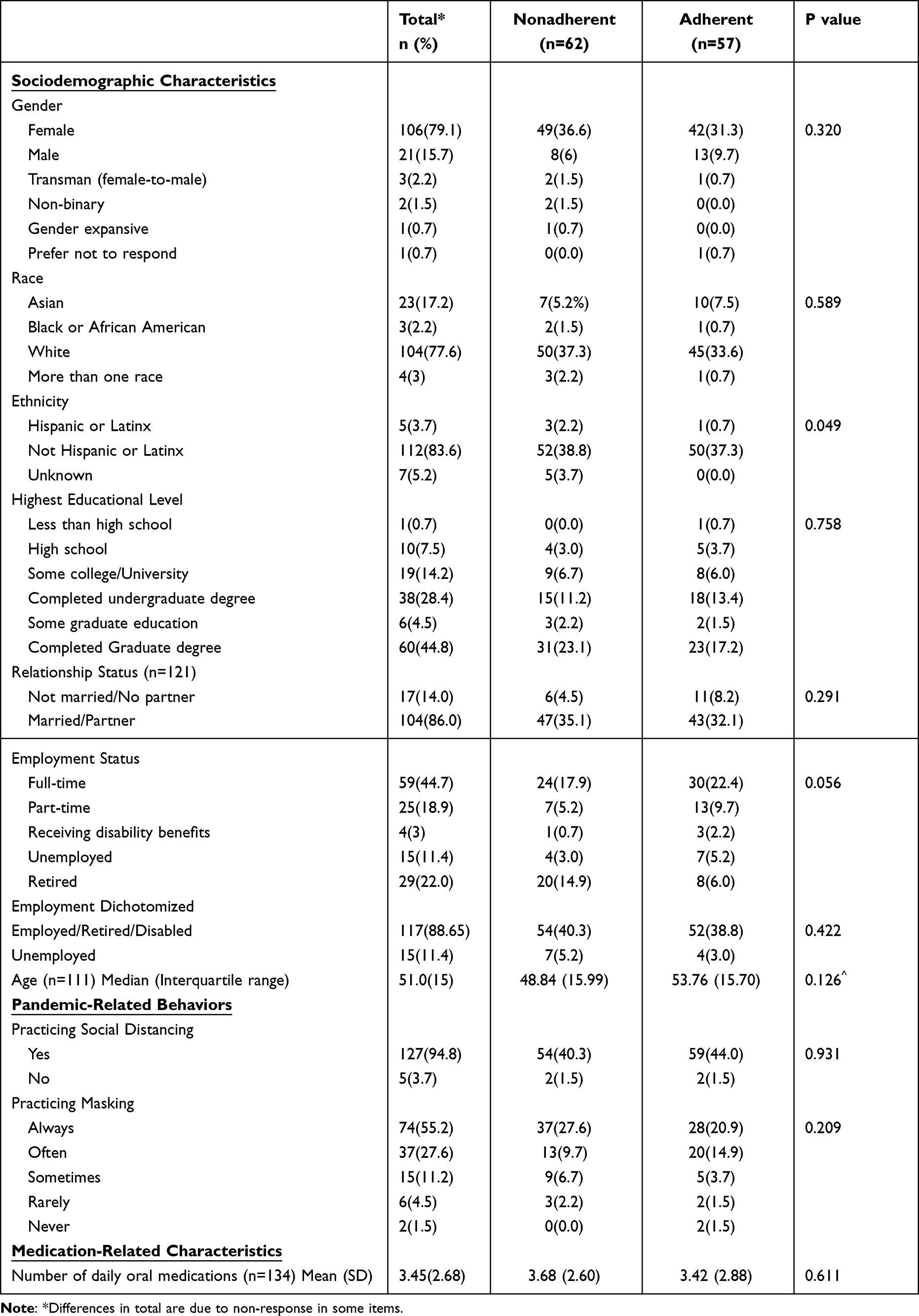 |
Table 1 Sociodemographic, Pandemic, and Medication-Related Characteristics |
Pandemic Experiences Across Medication-Related Contexts
Table 2 summarizes descriptive statistics for context-specific experiences reported in this sample. Each context variable aligned with the MACO framework (ie, clinic, pharmacy, and home) and associated findings are summarized in the context below.
 |
Table 2 Context-Specific Experiences and Medication Adherence Outcomes |
Clinic Context
A majority of the sample reported that they had not talked with their health care provider since the beginning of the pandemic (49.3%, n=66). Of 41.8% (n=56) respondents who indicated they had visited a provider, they reported how they visited their provider with 32.1% (n=18) doing so in person, 30.4% (n=17) by phone, and 37.5% (n=21) using telehealth. Delay in seeing a provider was reported by 35.1% (n=47). The reasons reported for delay included inability to get to provider office (5.2%, n=7), provider hours changed (1.55%, n=2), provider not seeing patients in the office (14.2%, n=19), change in job/insurance and affordability (0.7%/n=1), and fear of leaving house (11.2%/n=15). New medication was prescribed to 19.4% (n=26) of the sample.
A total of 39 (29.1%) individuals provided responses to the open-ended question about how interactions with healthcare providers or staff changed because of social distancing. Thirty responses included comments indicating no changes were noted or that no healthcare was not needed during this timeframe. For those reporting changes in clinic interactions, three main themes emerged within their comments to include “Care delays or cancellations” (n=27), “Use of distance-accessible care” (n=29), and “In-person safety precautions” (n=14).
Comments categorized as “Care delays or cancellations” experienced rescheduling of appointments or cancellations, sometimes by providers or the healthcare system and sometimes by patients to avoid increased risk from COVID exposure. For example, one respondent wrote,
I take warfarin and should have re-checked my INR in mid/late March. I have been on the same dose of warfarin for years, and my INR is fairly stable I felt that it was riskier to go to the hospital to check my INR rather than staying home and not checking it.
Interactions with clinics and providers were facilitated through the “Use of Distance-Accessible Care” using telehealth services such as video and phone calls and use of patient portals, that was a change due to the pandemic. One respondent shared, “we usually meet in person but now we’re meeting over the phone”. Another shared,
It’s actually improved. We’ve been using written messages through his office’s on-line portal, and I feel so much better communicating myself fully and precisely that way.
Clinic interactions changes with “In-Person Safety Precautions” included use of masking, social distancing in the waiting room, inability to bring support persons into appointments and in one case, a respondent indicated providers were seeing patients in the parking lot.
Among the 44 (32.8%) respondents who provided open-ended responses about what was helpful to them for managing medications during social distancing, three main themes emerged: “Accessible Care and Communication” (n=31), “Access to Medication” (n=26), and “Self-Management” (n=12). Accessible Care and Communication included the ability for providers to prescribe without being seen in-person, being able to connect with a provider with telephone and telehealth accessibility was collectively mentioned 13 times, and accessible communication available through web platforms and patient portals, where respondents indicated they could message providers or clinic staff. “Access to Medication” included helpful measures like providing 90-day/3-month supplies of medications or 12-month prescriptions, and automatic refills through the pharmacy. Self-management was a theme that included comments that indicated individuals managed well on their own, had knowledge to support their own self-management and took control of their medication management. Some self-management strategies identified included “making sure I have refills earlier than usual, to make sure I had extra time to get them”, and having a “regular routine”. Two comments indicated that the pandemic resulted in improved medication taking with one indicating “Less distractions resulted in taking meds more regularly”, and “I’m traveling less so I now rarely forget my medicine”.
Of the 50 (37.3%) respondents who made comments about what they needed from their provider and clinic services, their needs included, “Habit support or reminders” (n=3), “Supplies of medication” (n=6), “Access to care” (n=10), and “Medication instruction” (n=1). Examples of “Habit support or reminders” included, “Reminders. I need a routine to remember things like appointments or refills and since my routine has been disrupted, I totally forgot to make an appointment before running out of my medication” and “My routine is off so I periodically miss meds”. Those that reported a need for “supplies of medications” included getting refills, 3-month supplies, drive-thru, access to rare medications, and getting medications mail ordered. The theme “Access to care” included comments about telehealth, ability to see desired care provider and in timely fashion, and better communication from providers about accessibility. Example comments, “I’m in a COVID-19 hotspot and my doctor had been very backed up, so one refill was late”, and “To see my doctor not just a doctor in the practice”.
Pharmacy Context
A majority of the sample indicated they had obtained a prescription medication from the pharmacy since the beginning of the pandemic (77.6%, n=104). Respondents indicated they used a variety of ways to obtain medications and could select more than one option to report how they picked up medications. Picking up prescriptions from the pharmacy was reported by 59.7% (n=80); 15.7% (n=21) reported someone else obtained medications, 6.7% (n=9) had them delivered by the pharmacy, and 13.4% (n=18) reporting using mail-order. For those obtaining medications during this period, 18.7% (n=25) reported that their usual method for obtaining medications changed due to the pandemic, whereas the majority indicated no change (68.7%, n=92). The pharmacy interaction due to the pandemic was changed for 23.1% (n=31) of the respondents.
Delay and stopping medications were reported by a few respondents. Delay in refilling medication was reported by 6.7% (n=9). Reasons for the delay were reported by seven individuals, which included fear of leaving the house reported by 71.4% (n=5), and inability to get to the pharmacy 14.3% (n=1) and medication not being available 14.3% (n=1). A small proportion of individuals reported they stopped taking a medication altogether due to the inability to refill a medication due to the pandemic (4.5%, n=6). Of the four (66.7%) individuals reporting reasons, 50% (n=3) indicated they were afraid to leave their home and 25% (n=1) indicated they were worried about losing their job or insurance.
Among the 56 (41.8%) open-ended responses about pharmacy services that helped with medication management, themes included “Home delivery” (n=16), “Drive-thru” (n=15), “Digital Technology Support” (n=8), “Access” (n=6), “Online and automatic refills” (n=4), “Planning ahead” (n=3), Pharmacists (n=3), 90-day supplies (n=1), and phone availability (n=1). Home delivery options included mail-order as well as local pharmacy delivery as noted in this comment, “I was not able to pick up a prescription and the pharmacy delivered for free”. The theme “Digital Technology Support” included apps as noted in comments, “Health plan medication app” and “Pharmacy app”, as well as use of text message reminders and online payment options. The theme “Planning ahead” included comments like, “Delivery has been delayed so we order early” and “I call before I pick up. I don’t want to wait in store to get my meds”.
Sixty comments (44.8%) were made about needed pharmacy or pharmacy services and themes included “Home delivery” (n=2), “Better communication” (n=2), “Reminders” (n=1), “Access to Medications” (n=5) and “Affordability” (n=3). “Better Communication” was noted in comments like, “Better communication between pharmacy and clinicians. Having everyone working from home makes communication difficult”, and “Needed better communication and a method for picking up medications” “Access to medications” included lack of stock in pharmacies, or back-ordered medications, as well as limited hours and need for specific medications.
Home Management Context
The average consistency in home routine, measured by pre-pandemic chaos, was 54.78 (±7.02); median 53.0 (10.5). Pandemic life chaos in the sample averaged 54.33 (±7.68); median 54.0 (12.0). The differences in pre-pandemic life chaos compared with these scores in the early phase of the pandemic were not significantly different, p=0.540, related-samples Wilcoxon Signed-Rank test. Habit strength in the early phase of the pandemic was 55.02 (±12.49), median 56.0 (19.5). Of the total sample, 43.3% (n=58) reported using an organizer like a pillbox to manage their medications. There was no significant difference in pre-pandemic life chaos (55.36 [±7.97]; median 54 (13), p=0.431), pandemic life chaos (54.23 [±8.75]; median 54 (15), p=0.766 or habit strength (52.9 [±11.5]; median 53 (18.0, p=0.108) among those using a pillbox, Independent samples Mann–Whitney U-test.
Medication Adherence
Table 3 shows the frequencies of self-reported medication adherence and nonadherence for each item of the medication adherence scale. Much of the sample reported that they adhered to the implementation phase of taking their medications. A majority reported they had remembered to take their doses of medications over the prior 4 weeks, took their medications on time, and took their prescribed amount of medication. Medications were taken early or late among nearly one-quarter of the sample, and less than 10% reported altering the amount of their medications. Persistence in this sample was high, with only a few respondents indicating they had discontinued their medications without talking with their provider.
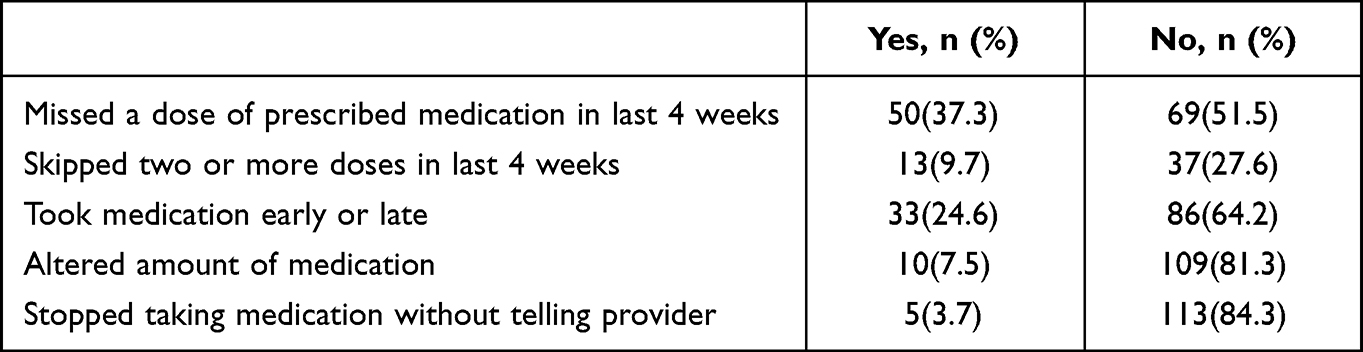 |
Table 3 Frequencies of Adherence and Nonadherence |
Nonadherence was reported among 46.3% (n=62) of the sample, determined by those responding “yes” to any of the adherence scale items. We found no differences in socio-demographic, social distancing/masking practices or medication-related characteristics among those classified as adherent compared with those nonadherent as reflected in Table 1. Among the medication management context variables, we found that nonadherence was significantly greater among those reporting they delayed getting a refill in the pharmacy (p=0.032), used a medication organizer like a pillbox (p=0.047), experienced more pandemic life chaos (p=0.040), and those with lower habit strength (p<0.001), as reflected in Table 2. Among those classified with nonadherence (n=62), 80.6% (n=50) reported missing a dose of their medications over the prior four weeks and among those who reported missing a medication, 21% (n=13) skipped taking two or more doses.
Discussion
This descriptive study was conducted in the early phases of the pandemic to understand individuals’ medication management experiences and adherence, focusing on contexts of the clinic, pharmacy, and home with survey questions developed and selected using the MACO framework. Less than half of the sample visited with a healthcare provider in this early phase of the pandemic; however, changes in interactions included a greater use of distance-accessible care options such as telephone and telehealth. Care was also delayed or cancelled, but having 90-day/3-month supplies of medications was helpful. The way in which individuals interacted with their pharmacies changed for nearly one-quarter of the sample; however, the majority reported that their usual method of obtaining medications from the pharmacy did not change. Home delivery of medications like mail order as well as drive-thru options at the pharmacy helped them obtain their medications. A relatively low number of individuals reported that fear of leaving their home affected their medication management during this period. A majority of the sample reported adherence to implementation and persistence phases of managing their medication; however, nonadherence was noted among nearly one-half of the sample. In the pharmacy context, those who reported they delayed getting their medications refilled, also experienced significantly greater nonadherence. All the home management context variables, including habit strength, pandemic-related home chaos, and pillbox use, were associated with self-reported nonadherence.
The proportion of individuals self-reporting nonadherence issues (52%) was consistent with pre-pandemic medication adherence patterns. For example, other studies that utilized the same self-report scale found nonadherence rates ranging from 38% to 64%.39,40 Even though our sample did not target a specific disease process, our findings are consistent with pre-pandemic adherence rates reported in the literature before 2020 that document approximately 50% of people on average are nonadherent among the general population.3 Other studies conducted during the pandemic have reported nonadherence ranging from 14.8%17 to 51% which included different chronic conditions.41 Like many others, our study relied on self-report, which tends to overestimate adherence.
Our study did not find a difference in adherence among those prescribed new medications in the early phases of the pandemic. The group prescribed new medication was relatively adherent based on self-report. This finding was surprising given that medication access issues are common during the initiation phase of medication and access barriers are often associated with nonadherence.3,42 Other studies evaluating medication adherence during the pandemic found access barriers to healthcare providers associated with non-adherence.41 Access to healthcare providers using distance-accessible care options such as telephone, telehealth, and online portals was used and found to be beneficial for managing medications in our study. Some also felt the communication with their providers increased during this time. Our findings indicate that among those who visited with providers, nearly 40% used telehealth. Literature suggests that the telehealth utilization was 7–18% before the COVID-19 pandemic and increased to 54–72% after the pandemic started.43 Other studies conducted in early phases of the pandemic reflect that telehealth enhanced communication and satisfaction.44,45 It is likely that alternative ways of accessing providers and pharmacies supported adherence.
In the home context, nonadherence was more likely when habits were not strong and there was inconsistency in routines. This finding further adds to the body of literature indicating that habit strength is associated with nonadherence.46,47 This phenomenon has been found in other studies, where adherence was improved when linking medication to existing habits such as meals and hygiene rituals. Habits remove the necessity of relying on memory and motivation alone, thereby improving adherence.47,48 Additionally, the qualitative comments in our study supported this finding and respondents reported they used routines to help support taking medications, while some reported that they needed greater habit and reminder support from their providers and clinic services. Interventions like the SystemCHANGE(TM) intervention, which has shown promising results in kidney transplant recipients, focus on changing routines to improve adherence49 and may be a habit formation intervention that could improve adherence for other populations. No studies to our knowledge examined the aspects of day-to-day home management, habits and routines in the early phases of the pandemic, which is a unique contribution of this study in the early pandemic phase literature.
A surprising finding in this study was that self-reported nonadherence was significantly greater among those who reported using a pill organizer, like a pillbox. Studies conducted pre-pandemic have shown mixed results on the effects of pillboxes on medication adherence as reported in a review of reviews.50 In one of the meta-analyses included in this review, investigators found that packaging interventions that included pillboxes were associated with increased medication adherence.51 In that same meta-analysis, moderator analyses revealed that these packaging interventions were associated with larger effect sizes when medication adherence measures were focused on pharmacy refill measures versus self-report measures,51 suggesting the way that medication adherence is measured might affect conclusions drawn on intervention effectiveness. Investigators have called for more studies to understand the mechanisms underlying pillboxes as an intervention.52,53
Limitations of this study include the cross-sectional design, and relatively homogenous and small sample size. Because this was a cross-sectional study, baseline medication adherence or pre-pandemic adherence is unknown for respondents. Medication adherence was obtained by self-report, which may have biased the results toward higher reported adherence, which is a known limitation of using self-reported adherence measures. The survey timing was also early in the pandemic, so disruptions in medication supplies may not have been observed during this period. Likewise, medication cost is a considerable barrier to medication adherence, and the economic impact from the pandemic may not have been fully realized. Given this was an online survey, it is likely that findings may not be representative of the general US population, especially those who do not access social media. Lastly, the study had a small sample size, including a homogeneous sample, so generalizability of findings should be considered cautiously.
Despite study limitations, there are strengths of this study and findings that have implications for practice, policy, and future research. While our sample size was small, the strengths of the study include assessment of people’s experiences managing and adhering to medication with data collection occurring in the early phase of the pandemic, nation-wide outreach and a patient-centered framework guiding survey development. This study also added measures with evidence of reliability and validity to self-reported habit strength, routine consistency, and medication adherence. We used the ABC taxonomy37 to select the self-report adherence measure used in this study and report adherence to enhance interpretation of study findings related to measures of implementation, discontinuation, and overall nonadherence. Other descriptive survey questions were designed specifically to align with the MACO framework contexts so that findings can be informative to clinic, pharmacy, and home contexts. Additionally, adding qualitative responses to the survey questions provided opportunities for respondents to share what was helpful to them and what they needed in the early phase of the pandemic. These lend to developing implications for practice, policy, and research to improve the patient experience in managing medications and future intervention development.
Implications for Practice
Implications for practice include the importance of interventions to improve medication adherence, especially during a pandemic when daily routines are altered. Interventions such as increasing access to care and medications can assist not only during a pandemic but also in non-pandemic times. Minimizing disruptions in obtaining medications from pharmacies and supporting individuals to consider ways in which they can incorporate their medication-taking in daily routines when medications are prescribed may improve medication adherence. It is crucial to discuss with patients access issues related to medication and supporting patients across all phases of medication adherence including initiation, implementation, and persistence. Providing prescriptions with longer refill times was noted as being helpful and may support medication implementation and persistence, especially when patients’ access to medications becomes problematic. Making this a standard of practice when prescribing, if possible, may help improve access to medications as well as help alleviate disruptions should another pandemic occur. As described above, interventions that support habit formation delivered by providers can help support adherence.
Policy Implications
Access to telehealth and telephone services was helpful to respondents in this study. Ensuring access to these services is critical to ensure equitable access to care for all patients. While several respondents indicated that they used some form of telehealth which was helpful, others mentioned that having this access was needed. This finding suggests that not all people have the same access to services. Additionally, ensuring broader access to mail-order and home delivery options may improve access to medications, which is a known barrier to adherence. While policy has changed to improve access to expanded telehealth services, more advocacy and access to these services is needed to ensure that all populations can benefit equally from these services.
Research Implications
The extent to which pillboxes support habit strength and managing medications in life chaos should be further examined. Pillboxes are often thought of as strategies for planning and organizing medications. However, we did not find that habit strength was significantly better among pillbox users. It is possible that pillbox users were simply more aware of their missed doses due to the inherent adherence monitoring that comes with pillbox use. Possible mechanisms of action in pillboxes should be explored in future studies as well as more research evaluating interventions that support habit formation, like testing SystemCHANGE™ in other populations.
Conclusion
The early phases of the pandemic affected access to care and how individuals received care in this sample. Distance-accessible care options and strategies to obtain needed services without being in-person supported respondents medication management, interactions with providers and pharmacy services. Helpful strategies included use of telehealth and telephone access to care, access to medication including home delivery, mail-order, online and automatic refills, and digital technology support. Habit and routine disruptions were associated with nonadherence in this sample early in the pandemic. Care providers in clinic and pharmacy settings can enhance care and better prepare patients for disruptions through education and reminders about additional services available to support medication management adherence including use of distance-accessible technologies, portals, online ordering, home delivery and enhancing communication between patients, clinic, and pharmacy settings. Advocacy efforts are needed to ensure equitable access to helpful services when disruptions occur, such as occurred in the early phases of the pandemic.
Disclosure
Dr Rebecca J Bartlett Ellis reports a patent US 10857070. (This patent is for a device designed to be used as a smart pillbox. This is not directly related to the present study but is designed to measure medication adherence). The authors report no conflicts of interest in this work.
References
1. Georgetown University HPI. Prescription drugs: Georgetown University Health Policy Institute; 2022. Available from: https://hpi.georgetown.edu/rxdrugs/.
2. Brown MT, Bussell JK. Medication Adherence: WHO Cares? Mayo Clinic Proceedings. Elsevier; 2011.
3. Sabaté E, Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003.
4. Gokoel SR, Gombert-Handoko KB, Zwart TC, van der Boog PJ, Moes DJA, de Fijter JW. Medication non-adherence after kidney transplantation: a critical appraisal and systematic review. Transplant Rev. 2020;34(1):100511. doi:10.1016/j.trre.2019.100511
5. Cutler RL, Fernandez-Llimos F, Frommer M, Benrimoj C, Garcia-Cardenas V. Economic impact of medication non-adherence by disease groups: a systematic review. BMJ open. 2018;8(1):e016982. doi:10.1136/bmjopen-2017-016982
6. Walsh CA, Cahir C, Tecklenborg S, Byrne C, Culbertson MA, Bennett KE. The association between medication non‐adherence and adverse health outcomes in ageing populations: a systematic review and meta‐analysis. Br J Clin Pharmacol. 2019;85(11):2464–2478. doi:10.1111/bcp.14075
7. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta Bio Medica. 2020;91(1):157. doi:10.23750/abm.v91i1.9397
8. Lee M, Zhao J, Sun Q, et al. Human mobility trends during the early stage of the COVID-19 pandemic in the United States. PLoS One. 2020;15(11):e0241468. doi:10.1371/journal.pone.0241468
9. Horsley A, Brightling C, Davies J, et al. Early-phase clinical trials in a pandemic: learning from the response to COVID-19. Lancet Respir Med. 2022;10(7):625–627. doi:10.1016/S2213-2600(22)00062-5
10. Barnett ML, Mehrotra A, Landon BE. Covid-19 and the upcoming financial crisis in health care. NEJM Catal Innov Care Deliv. 2020;1:2.
11. Kaye AD, Okeagu CN, Pham AD, et al. Economic impact of COVID-19 pandemic on healthcare facilities and systems: international perspectives. Best Pract Res Clin Anaesthesiol. 2021;35(3):293–306. doi:10.1016/j.bpa.2020.11.009
12. Nguyen A, Guttentag A, Li D, Meijgaard J. The impact of job and insurance loss on prescription drug use: a panel data approach to quantifying the health consequences of unemployment during the covid-19 pandemic. Int J Health Services. 2022;2022:00207314221078749.
13. Shimels T, Asrat Kassu R, Bogale G, et al. Magnitude and associated factors of poor medication adherence among diabetic and hypertensive patients visiting public health facilities in Ethiopia during the COVID-19 pandemic. PLoS One. 2021;16(4):e0249222. doi:10.1371/journal.pone.0249222
14. Subathra G, Rajendrababu SR, Senthilkumar VA, Mani I, Udayakumar B. Impact of COVID-19 on follow-up and medication adherence in patients with glaucoma in a tertiary eye care centre in south India. Indian J Ophthalmol. 2021;69(5):1264. doi:10.4103/ijo.IJO_164_21
15. Menon S, Sander JW. Effects of the COVID-19 pandemic on medication adherence: in the case of antiseizure medications, A scoping review. Seizure. 2021;93:81–87. doi:10.1016/j.seizure.2021.10.009
16. Kaye L, Theye B, Smeenk I, Gondalia R, Barrett MA, Stempel DA. Changes in medication adherence among patients with asthma and COPD during the COVID-19 pandemic. J Allergy Clin Immunol Pract. 2020;8(7):2384. doi:10.1016/j.jaip.2020.04.053
17. Rebić N, Park JY, Garg R, et al. Rapid review of medication taking (adherence) among patients with rheumatic diseases during the COVID‐19 pandemic. Arthritis Care Res. 2021;74:1961.
18. Bartlett Ellis RJ, Welch JL. Medication‐taking behaviours in chronic kidney disease with multiple chronic conditions: a meta‐ethnographic synthesis of qualitative studies. J Clin Nurs. 2017;26(5–6):586–598. doi:10.1111/jocn.13588
19. Bartlett Ellis RJ, Haase J, Ruppar T Understanding Processes, Outcomes, and Contexts in Medication Adherence. Patient Preference and Adherence. 2023;17:239–248.
20. Cappelleri JC, Lundy JJ, Hays RD. Overview of classical test theory and item response theory for the quantitative assessment of items in developing patient-reported outcomes measures. Clin Ther. 2014;36(5):648–662. doi:10.1016/j.clinthera.2014.04.006
21. Patridge EF, Bardyn TP. Research electronic data capture (REDCap). JMLA. 2018;106(1):142. doi:10.5195/jmla.2018.319
22. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
23. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
24. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2014;81(3):14–18.
25. The Belmont report: ethical principles and guidelines for the protection of human subjects of research: Department of Health, Education, and Welfare. National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research; 1978.
26. Bartlett Ellis RJ, Ruppar TM (2018 Oct. 4). The Medication Adherence Context and Outcomes Framework Image. Available from: https://hdl.handle.net/1805/30882.
27. Verplanken B, Orbell S. Reflections on past behavior: a self‐report index of habit strength 1. J Appl Soc Psychol. 2003;33(6):1313–1330. doi:10.1111/j.1559-1816.2003.tb01951.x
28. Orbell S, Verplanken B. The strength of habit. Health Psychol Rev. 2015;9(3):311–317. doi:10.1080/17437199.2014.992031
29. Matheny JAP, Wachs TD, Ludwig JL, Phillips K. Bringing order out of chaos: psychometric characteristics of the confusion, hubbub, and order scale. J Appl Dev Psychol. 1995;16(3):429–444. doi:10.1016/0193-3973(95)90028-4
30. Zullig LL, Shaw RJ, Crowley MJ, et al. Association between perceived life chaos and medication adherence in a postmyocardial infarction population. Circ Cardiovasc Qual Outcomes. 2013;6(6):619–625. doi:10.1161/CIRCOUTCOMES.113.000435
31. Dobbels F, Berben L, De Geest S, et al. The psychometric properties and practicability of self-report instruments to identify medication nonadherence in adult transplant patients: a systematic review. Transplantation. 2010;90(2):205–219. doi:10.1097/TP.0b013e3181e346cd
32. Abraham I, Van Camp Y, Villa L, et al. Hierarchical modeling of patient and physician determinants of blood pressure outcomes in adherent vs nonadherent hypertensive patients: pooled analysis of 6 studies with 14,646 evaluable patients. J Clin Hyper. 2013;15(9):663–673. doi:10.1111/jch.12163
33. Cajita MI, Denhaerynck K, Berben L, et al. Is degree of chronic illness management in heart transplant centers associated with better patient survival? Findings from the intercontinental BRIGHT study. Chronic Illn. 2022;18(4):806–817. doi:10.1177/17423953211039773
34. Villa L, Sun D, Denhaerynck K, et al. Predicting blood pressure outcomes using single-item physician-administered measures: a retrospective pooled analysis of observational studies in Belgium. Br J Gen Pract. 2015;65(630):e9–e15. doi:10.3399/bjgp15X683101
35. Delameillieure A, Wuyts WA, Pironet A, Dobbels F. Electronically monitored medication adherence in idiopathic pulmonary fibrosis: prevalence, predictors and outcomes. ERJ Open Res. 2022;8(3):00030–2022. doi:10.1183/23120541.00030-2022
36. Belaiche S, Décaudin B, Caron A, et al. Medication non‐adherence after allogeneic hematopoietic cell transplantation in adult and pediatric recipients: a cross sectional study conducted by the Francophone Society of Bone Marrow Transplantation and Cellular Therapy. Fundam Clin Pharmacol. 2021;35(2):435–445. doi:10.1111/fcp.12593
37. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
38. DeGeest S. The Basel Assessment of Sdherence to Immunsuppressive Medications Scale (BAASIS©) – EXPLANATION; 2021.
39. Gustavsen MT, Midtvedt K, Lønning K, et al. Evaluation of tools for annual capture of adherence to immunosuppressive medications after renal transplantation–a single‐centre open prospective trial. Transplant Int. 2019;32(6):614–625. doi:10.1111/tri.13412
40. Shemesh Y, Peles‐Bortz A, Peled Y, et al. Feelings of indebtedness and guilt toward donor and immunosuppressive medication adherence among heart transplant (HT x) patients, as assessed in a cross‐sectional study with the Basel Assessment of Adherence to Immunosuppressive Medications Scale (BAASIS). Clin Transplant. 2017;31(10):e13053. doi:10.1111/ctr.13053
41. Ismail H, Marshall VD, Patel M, Tariq M, Mohammad RA. The impact of the COVID-19 pandemic on medical conditions and medication adherence in people with chronic diseases. J Am Pharm Assoc. 2022;62(3):834–9. e1. doi:10.1016/j.japh.2021.11.013
42. Peh KQE, Kwan YH, Goh H, et al. An adaptable framework for factors contributing to medication adherence: results from a systematic review of 102 conceptual frameworks. J Gen Intern Med. 2021;36(9):2784–2795. doi:10.1007/s11606-021-06648-1
43. Lonergan PE, Washington Iii SL, Branagan L, et al. Rapid utilization of telehealth in a comprehensive cancer center as a response to COVID-19: cross-sectional analysis. J Med Internet Res. 2020;22(7):e19322. doi:10.2196/19322
44. Harkey LC, Jung SM, Newton ER, Patterson A. Patient satisfaction with telehealth in rural settings: a systematic review. Int J Telerehabilitation. 2020;12(2):53. doi:10.5195/ijt.2020.6303
45. Orlando JF, Beard M, Kumar S. Systematic review of patient and caregivers’ satisfaction with telehealth videoconferencing as a mode of service delivery in managing patients’ health. PLoS One. 2019;14(8):e0221848. doi:10.1371/journal.pone.0221848
46. Alison Phillips L, Leventhal H, Leventhal EA. Assessing theoretical predictors of long-term medication adherence: patients’ treatment-related beliefs, experiential feedback and habit development. Psychol Health. 2013;28(10):1135–1151. doi:10.1080/08870446.2013.793798
47. Conn VS, Ruppar TM, Enriquez M, Cooper P. Medication adherence interventions that target subjects with adherence problems: systematic review and meta-analysis. Res Soc AdministratPharm. 2016;12(2):218–246. doi:10.1016/j.sapharm.2015.06.001
48. Conn VS, Ruppar TM. Medication adherence outcomes of 771 intervention trials: systematic review and meta-analysis. Prev Med. 2017;99:269–276. doi:10.1016/j.ypmed.2017.03.008
49. Russell CL, Hathaway D, Remy LM, et al. Improving medication adherence and outcomes in adult kidney transplant patients using a personal systems approach: systemCHANGE results of the MAGIC randomized clinical trial. Am J Transplant. 2020;20(1):125–136. PubMed PMID: 31291507; PMCID: PMC7179766. doi:10.1111/ajt.15528
50. Anderson LJ, Nuckols TK, Coles C, et al. A systematic overview of systematic reviews evaluating medication adherence interventions. Am J Health Syst Pharm. 2020;77(2):138–147. doi:10.1093/ajhp/zxz284
51. Conn VS, Ruppar TM, Chan KC, Dunbar-Jacob J, Pepper GA, De Geest S. Packaging interventions to increase medication adherence: systematic review and meta-analysis. Curr Med Res Opin. 2015;31(1):145–160. doi:10.1185/03007995.2014.978939
52. Schwartz JK. Pillbox use, satisfaction, and effectiveness among persons with chronic health conditions. Assist Technol. 2017;29(4):181–187. doi:10.1080/10400435.2016.1219884
53. Ellis RJB, Knisely MR, Boyer K, Pike C. Pillbox intervention fidelity in medication adherence research: a systematic review. Nurs Outlook. 2017;65(4):464–476. doi:10.1016/j.outlook.2016.12.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence Evaluated Through Electronic Monitors During the 2020 COVID-19 Pandemic Lockdown in Switzerland: A Longitudinal Analysis
Bandiera C, Pasquier J, Locatelli I, Niquille A, Wuerzner G, Dotta-Celio J, Hachfeld A, Wandeler G, Wagner AD, Csajka C, Zanchi A, Cavassini M, Schneider MP
Patient Preference and Adherence 2022, 16:2313-2320
Published Date: 25 August 2022
Impact of the COVID-19 Pandemic on Adherence to Most Costly Chronic Disease Medications in British Columbia, Canada: A Population-Based Interrupted Time Series Analysis
Rebić N, Sayre EC, Law MR, Cragg JJ, Brotto LA, De Vera MA
Patient Preference and Adherence 2025, 19:2493-2504
Published Date: 15 August 2025