Back to Journals » Clinical Ophthalmology » Volume 20
Management of Post-Operative Inflammation After Cataract Surgery with Intracanalicular Dexamethasone Implant and Topical Ketorolac
Authors Gannamaneni K, Shapiro JN, Levine H ![]() , Reddy K
, Reddy K ![]() , Armenti ST, Mian SI
, Armenti ST, Mian SI
Received 10 December 2025
Accepted for publication 24 February 2026
Published 5 March 2026 Volume 2026:20 584501
DOI https://doi.org/10.2147/OPTH.S584501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Bharat Gurnani
Kartik Gannamaneni,1 Jeremy N Shapiro,2 Harry Levine,3 Karthik Reddy,3,4 Stephen T Armenti,5 Shahzad I Mian3
1Indiana University School of Medicine, Indianapolis, IN, USA; 2Department of Ophthalmology, Johns Hopkins University, Baltimore, MD, USA; 3Department of Ophthalmology and Visual Sciences, University of Michigan, Ann Arbor, MI, USA; 4University of Michigan Medical School, Ann Arbor, MI, USA; 5Department of Ophthalmology, University of Pennsylvania, Philadelphia, PA, USA
Correspondence: Shahzad I Mian, Department of Ophthalmology and Visual Sciences, University of Michigan, 1000 Wall Street, Ann Arbor, MI, 48105, USA, Tel +1 734-764-6468, Email [email protected]
Purpose: To determine the safety of an intracanalicular dexamethasone ophthalmic insert (IDOI) and topical Ketorolac tromethamine 0.5% (ketorolac) versus ketorolac and topical prednisolone acetate 1% (PA) over the first month after cataract surgery (POM1).
Patients and Methods: Retrospective study of uncomplicated cataract surgeries between June 2020 and March 2023 at the University of Michigan. Patients received either IDOI and ketorolac or PA and ketorolac (control) during POM1. Outcomes included breakthrough inflammation necessitating additional anti-inflammatory drops, cystoid macular edema, and increased intraocular pressure at POM1.
Results: 100 eyes of 78 patients were included in the IDOI/ketorolac group, and 102 eyes of 83 individuals in the control group. Demographics, ocular comorbidities, and baseline IOP were comparable between groups. There were no differences between groups in the distribution of race (p = 0.137), the preoperative presence of epiretinal membrane (43.5% vs 57.83%; p = 0.88), or history of diabetic retinopathy (19.23% vs 15.6%; p = 0.59) in the surgical eyes. There were no differences in the rates of postoperative rebound inflammation in the IDOI/ketorolac compared to the PA/ketorolac group (2.0% vs 2.0%; p = 1.00) or in the development of cystoid macular edema (2.0% vs 2.9%; p = 1.00). There were no cases of increased IOP > 10 mmHg at POM1 compared with baseline in either group.
Conclusion: There was no difference in the rate of rebound inflammation or CME in the IDOI/ketorolac regimen compared to the PA/ketorolac regimen. IDOI can be a safe and effective dropless alternative to PA/ketorolac therapy after cataract surgery in patients susceptible to inflammation.
Keywords: cataract, dexamethasone insert, postoperative inflammation, ketorolac, iritis
Introduction
Postoperative inflammation prophylaxis is an essential consideration in cataract surgery. Cataract surgery is the most commonly performed surgical procedure in the United States, with approximately 3.7 million cases annually.1 Uncontrolled postoperative inflammation after cataract surgery has been known to lead to a multitude of adverse outcomes. The severity of inflammation can vary case by case, with long-term complications including uveitis, posterior synechiae, and secondary glaucoma.1 Postoperative inflammation can manifest in the immediate postoperative period with breakthrough inflammation (BI) of the anterior chamber or in a more delayed fashion with cystoid macular edema (CME).2 Each has distinct mechanisms and implications for patient outcomes. BI has been reported to have an incidence of anterior chamber inflammation ranging from 0.32% to 1.75% of cases, and CME ranging from 1% to 19%.2,3 Given variations in patient risk for postoperative inflammation and in the rate of development of long-term complications, optimizing the selection of each patient’s anti-inflammatory prophylactic regimen is essential.
Approaches to postoperative inflammation prophylaxis vary among clinicians, but common strategies include corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), or a combination of both. For cataract surgery patients at low/normal risk of postoperative inflammation, single-agent prophylaxis is typically preferred. Studies suggest that NSAIDs have gained increasing favor in being more effective in preventing CME compared to steroids.4 For patients with risk factors for inflammation, a combination of steroids and NSAIDs can be used for drug synergism, albeit with the added risk of side effects from either medication. Multiple studies have demonstrated that combination therapy can offer superior control of inflammation and better visual outcomes compared to monotherapy alone.5 Several patient-related factors have been shown to increase the likelihood and severity of postoperative inflammation, including age, diabetic status, and history of previous ocular inflammation or surgery.1,6 Pre-existing immune dysregulation in both systemic and ocular settings can exacerbate the postoperative inflammatory response.6
The traditional route of administration for these medications is via patient self-administered topical drops; however, nonadherence remains a significant concern. Nonadherence is often related to cognitive disability, vision-related disability, or physical disability in elderly patients.7,8 Studies have shown that between 20–30% of cataract patients do not use their eyedrops as prescribed after surgery.8
The FDA approval of the intracanalicular dexamethasone insert (DII) for postoperative inflammation in ocular surgery in 2018 provided an alternative to corticosteroid drops, thereby eliminating the need for patient adherence to complex drop regimens.9,10 The DII is a sustained-release dexamethasone insert placed into the upper or lower canaliculus during surgery, delivering a 0.4 mg dose of dexamethasone for 30 days after insertion.10 The DII is equal in effectiveness to topical steroid drops in managing postoperative inflammation after cataract surgery, with comparable rates of BI.11 Additionally, multiple small randomized controlled trials have found that most patients prefer the DII to topical steroid drop regimens.10–12
Management of postoperative inflammation following cataract surgery requires a multifactorial approach, particularly with patients who are suspected to be at a higher risk of uncontrolled inflammation. The benefits of combination steroid and NSAID therapy have been shown when compared with monotherapy for higher-risk patients. However, extensive studies have not compared the efficacy of a postoperative regimen of combination steroid and NSAID drops to a combination of dropless steroids (eg, DII) and NSAID drops. This study aims to compare these two treatment modalities among a cohort of patients at higher risk of postoperative inflammation.
Materials and Methods
The study protocol was approved by the University of Michigan Institutional Review Board (IRBMED, HUM00272654). As the study involved retrospective, secondary analysis of existing health information, the requirement for informed consent was waived. The study adhered to the principles outlined in the Declaration of Helsinki, and HIPAA regulations were strictly followed. It was designed as a retrospective chart review of consecutive patients who underwent extracapsular cataract extraction with phacoemulsification and implantation of a posterior chamber intraocular lens performed by five surgeons. Data regarding demographics, ocular and systemic comorbidities, surgical history, post-operative medications, and follow-up were obtained.
The intervention group consisted of individuals who had a 0.4 mg dexamethasone ophthalmic insert placed intraoperatively in the lower canaliculus or, if insertion in the lower canaliculus was not feasible, in the upper canaliculus. The decision to use DII for a patient’s cataract surgery was made through shared decision-making between the provider and the patient. The control group was composed of individuals that were started on a regimen of topical prednisolone acetate (PA) 1% (1 mg/mL) eyedrops tapered weekly in the following manner: 4 drops per day during the first week, three drops per day during the second week, two drops per day during the third week, and one drop per day during the fourth week postoperatively. Both the intervention and control groups received a regimen of topical ketorolac 0.5% following a similar taper to the steroid drops, as well as intraoperative intracameral cefuroxime 1 mg/0.1 mL or moxifloxacin 0.5 mg/0.1 mL.
Individuals were excluded if they had a history of uveitis, ocular infection, glaucoma, intraoperative complications such as posterior capsular rupture, vitreous prolapse, retained lens fragments, or if their cataract surgery was combined with another type of procedure (eg, corneal transplant).
All patients were seen in the clinic at 1 day postoperatively, had a 1-week postoperative telephone visit, and were scheduled for a 1-month final postoperative visit (POM1). For this study, a visit was considered acceptable as the POM1 visit if it occurred between postoperative days 21 and 56. Patients with no visits in that window were excluded from the study. All postoperative eyes were examined under a slit lamp at each clinic visit. Baseline preoperative IOP and IOP at the POM1 visit were measured for each eye using rebound tonometry (iCare, Icare Finland Oy). Breakthrough inflammation was defined in this study as the presence of trace or more anterior chamber cells on exam, necessitating the addition of supplemental topical anti-inflammatory medication between postoperative day 3 and the POM1 visit. CME was defined as the development of macular thickening due to the accumulation of fluid clinically or by OCT imaging.
Data was collected and reviewed between May 2024 and May 2025. Statistical analyses were performed using SPSS version 28.0 (IBM Corp). Independent two-tailed Student’s t-test, Chi-square, and Fisher’s exact tests were used, as appropriate, to compare variables of interest between groups. A p-value less than .05 was considered statistically significant.
Results
The eyes of 161 patients met the inclusion criteria, and data were collected and analyzed from their medical records. 100 eyes of 78 patients were in the DII + ketorolac group, and 102 eyes of 83 patients were in the PA + ketorolac group. The demographic and comorbidities of the included patients are presented in Table 1, showing no statistically significant differences between the two groups in terms of patient demographics and comorbidities.
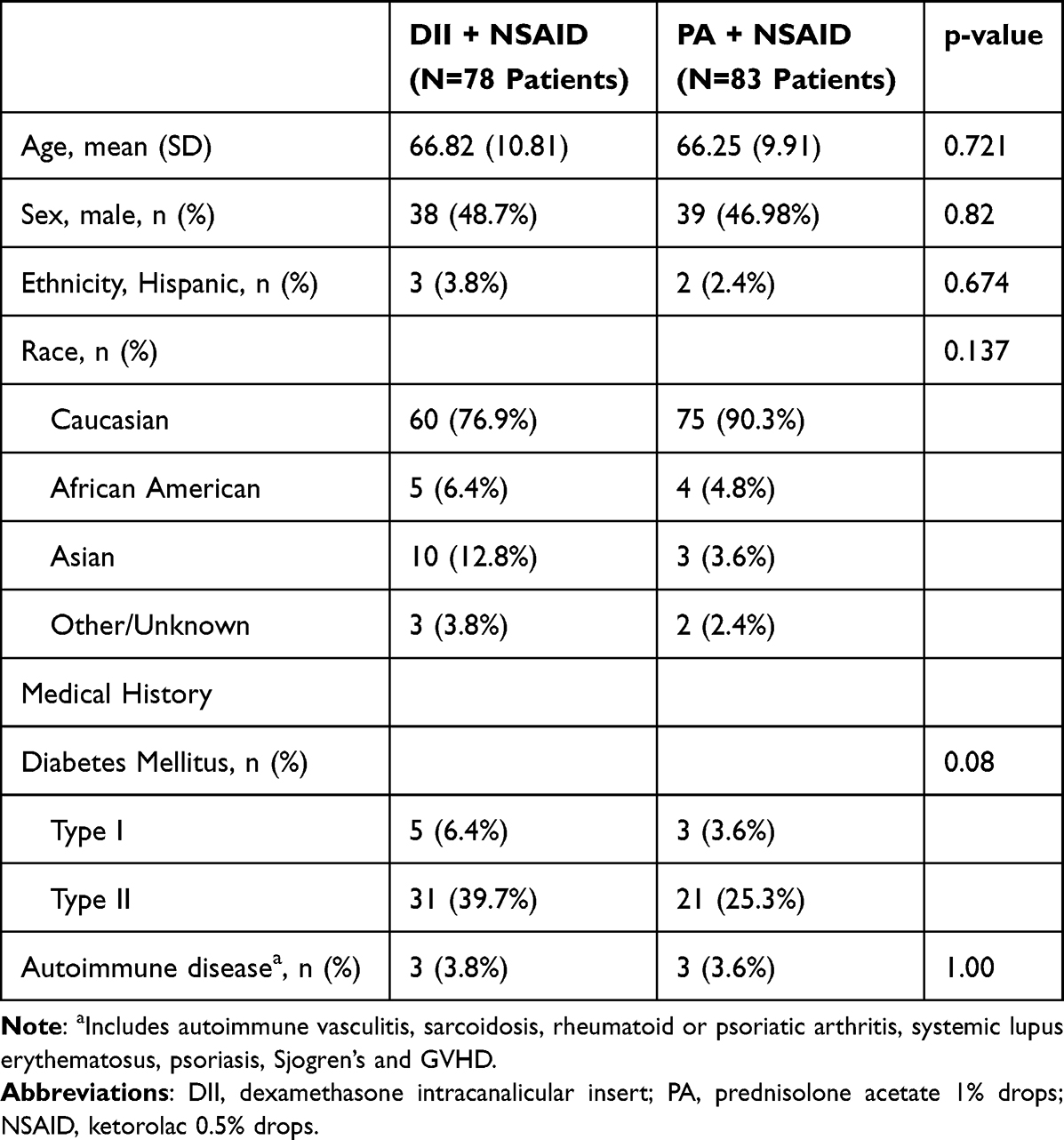 |
Table 1 Demographics and Comorbidities of Patients Receiving Either the Dexamethasone Intracanalicular Insert + Topical NSAIDs or Steroid Drops + Topical NSAIDs |
There were no differences between groups in preoperative indications for surgery, including the presence of epiretinal membrane (43.5% vs 57.8%; p = 0.88) or a history of diabetic retinopathy (19.2% vs 15.6%; p = 0.59) in the surgical eyes. There were no differences in the rates of postoperative BI in the DII + NSAID compared to the PA + NSAID group (2.0% vs 2.0%; p = 1.00) or in the development of cystoid macular edema (2.0% vs 2.9%; p = 1.00). There were no cases of increased IOP greater than 10 mmHg at POM1 compared to baseline in either group, as shown in Table 2.
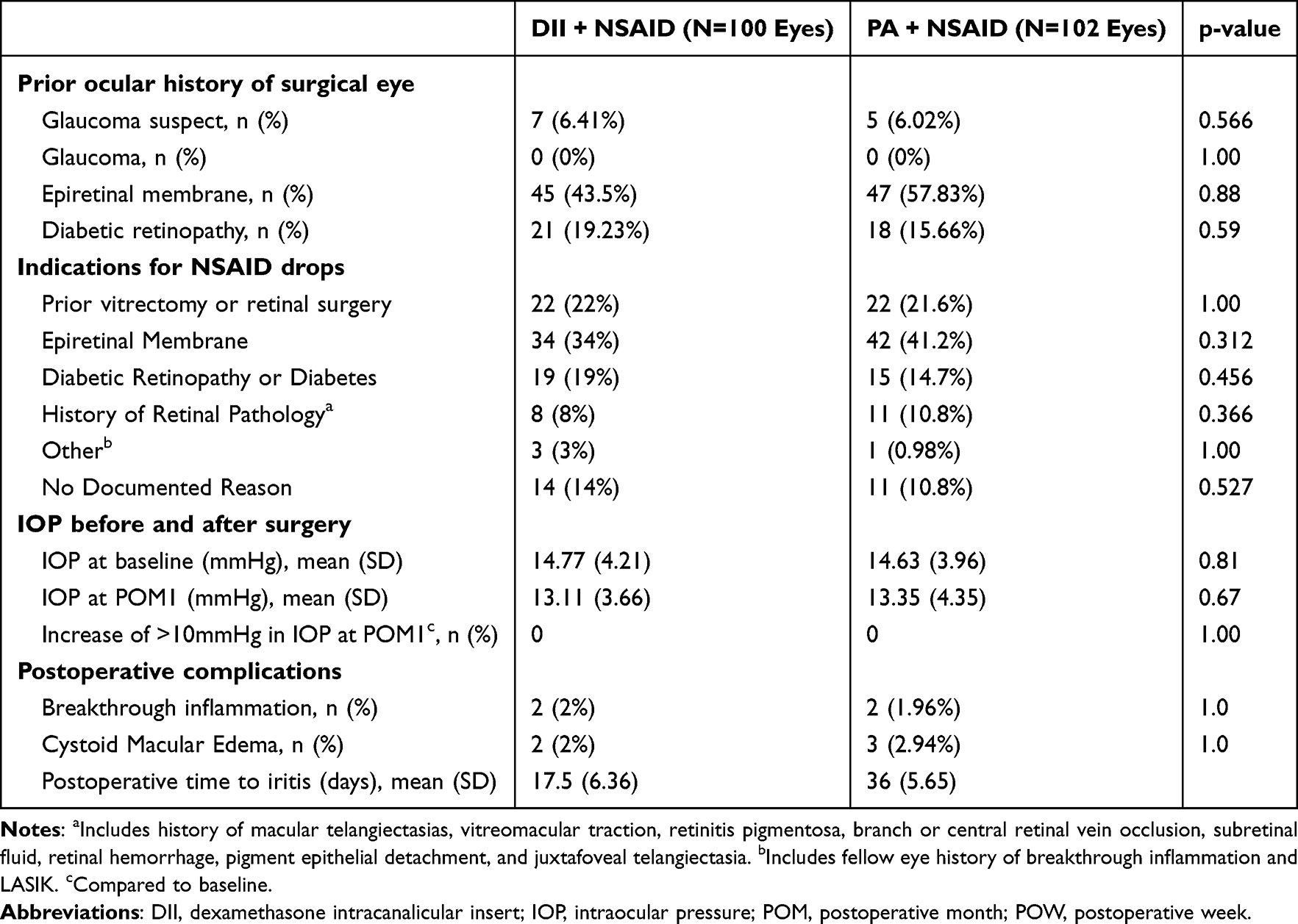 |
Table 2 Ocular Baseline Characteristics and Postoperative Outcomes of Eyes Receiving the Dexamethasone Intracanalicular Insert or Steroid Drops After Cataract Surgery |
Discussion
This study presents data from a single institution on 202 uncomplicated cataract surgeries that received either combination DII + NSAID drops or topical steroid drops + NSAID drops. The rates of both CME and BI were not significantly different between groups. Similarly, no differences were found in IOP elevation rates at postoperative month one compared with baseline preoperative IOP.
There is minimal large-scale research assessing rates of postoperative inflammation after cataract surgery in patients taking combination DII and NSAIDs. To our knowledge, only one study directly compares DII + NSAID drops and topical steroid drops + NSAID drops.12 This study reported similar rates of postoperative inflammation between interventions, as well as greater than 90% of patient preference for the DII.12 However, it is essential to note that the patients in this study were undergoing refractive lens exchange rather than uncomplicated cataract surgery, and the sample size was limited to 20 patients.12
Combination steroid and NSAID therapy has gained favor in the prophylaxis of postoperative inflammation following cataract surgery, particularly for patients with higher ocular comorbidities and risk factors for inflammation. Provider preference plays a significant role in NSAID use for prophylaxis, with some clinicians reserving them for patients with specific risk factors—such as diabetic retinopathy, prior retinal pathology or surgery, and history of ocular inflammation—while others use them universally as routine prophylaxis.13 This study corroborates this, as 92.5% of cases had a specific documented indication for NSAID use, with the majority being for the presence of an ERM (37.6%), prior retinal surgery (21.7%), and diabetic retinopathy or diabetes (16.8%). The growing trend of combination therapy has been bolstered by both clinical experience and multiple studies demonstrating a lower incidence of macular edema after one month postoperatively in patients who received combination topical steroids and NSAIDs compared to monotherapy.13 The rates of BI and CME found in this study are in line with the numbers reported in the literature.2 This helps to suggest that the DII may be a suitable alternative to topical steroid drops for patients at risk of inflammation who are receiving a combination of steroid and NSAID postoperative regimen. The combination of these two drug classes can offer a synergistic effect, providing broader anti-inflammatory coverage and has been suggested to provide better pain control than either drug alone.
The usage of steroids and NSAIDs for postoperative inflammation control is not without risk. For example, chronic topical steroid use has been shown to predispose patients to elevated postoperative IOP, increasing the risk of optic nerve damage.14 Likewise, chronic topical NSAID use has been associated with an increased risk of corneal melt, a severe complication that can lead to corneal perforation and loss of vision.15 Multiple studies have suggested, however, that with close postoperative monitoring and consideration of patient risk factors for increased IOP, combination steroid and NSAID therapy after cataract surgery does not have higher risks of IOP elevation than a regimen lacking steroids.5,16
This is also an essential factor in clinical decision-making, given the benefits of steroid therapy in reducing macular edema rates and controlling inflammation compared with other medications. Extensive research has been done evaluating IOP elevation in topical steroid drops individually or in conjunction with NSAIDs; however, not in comparison with a combination DII therapy. In this study, neither treatment group experienced an IOP elevation greater than 10 mmHg within the period of observation (POM1). This helps support the tolerability of both treatments and their equivalent safety profiles in terms of IOP sensitivity.
Given the increased risk of postoperative inflammation in patients with risk factors for such inflammation, including previous history of uveitis, intraoperative excessive iris manipulation, and posterior capsular rupture, proper prophylaxis is imperative. Some studies have shown the efficacy of combination topical steroid drops and NSAID drops in these populations; however, ours is the first to compare dropless steroids in conjunction with NSAID drops to a regimen of steroid drops in conjunction with NSAID drops. This study suggests that the DII may serve as an alternative to topical steroid drops for patients requiring combination therapy, without compromising efficacy or tolerability.
Several limitations should be considered when evaluating the findings of this study. As a retrospective study, the data are vulnerable to potential selection and information bias. Additionally, the study population was primarily composed of older, white individuals seeking care at a specialized hospital, which may limit the applicability of the findings to other groups. Other limitations of this study include the use of 1% prednisolone acetate as the comparator, which precludes direct comparison with other dexamethasone-based regimens that may vary in potency and clinical effect. Additionally, ketorolac 0.5% was administered to both groups to reflect routine practice, which may have reduced detectable differences and precluded conclusions regarding steroid-only effects. Finally, this retrospective pilot study had a small sample size and lacked an a priori sample size calculation, so it may be underpowered to detect small differences and should be interpreted cautiously. Future studies, particularly more extensive randomized controlled trials involving different populations, can be done to verify these findings more robustly. Future research can also help further streamline clinical decision-making by comparing the DII with other modern dropless steroid regimens for prophylaxis against postoperative inflammation in high-risk patients.
Conclusion
Our study identified no significant differences in the occurrence of rebound inflammation or cystoid macular edema between patients receiving an intracanalicular dexamethasone ophthalmic insert and a ketorolac regimen versus a ketorolac and topical prednisolone acetate 1% regimen. Neither treatment group experienced an increase in intraocular pressure greater than 10 mmHg. This suggests that intracanicular prophylaxis may be as effective as the ketorolac and 1% topical prednisolone acetate regimen for inflammatory prophylaxis after cataract surgery; however, future studies are needed to validate these findings.
Data Sharing Statement
Available upon reasonable request to the corresponding author.
Acknowledgment
An abstract consisting of preliminary analyses was presented as a poster at the 2025 American Society of Cataract and Refractive Surgery Annual Meeting.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Dr. Shahzad Mian is a research investigator for KOWA and receives Up-to-date royalties for work unrelated to the contents of this manuscript. All other authors report no potential conflicts of interest that would influence this work, including consulting, royalties, or research support.
References
1. Moshirfar M, Milner D, Patel BC. Cataract surgery. In: StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2025.
2. Padidam S, Skopis G, Lai MM. Prevalence of cystoid macular edema after cataract surgery in eyes with previous macular surgery. Clin Ophthalmol. 2022;16:423–6. doi:10.2147/OPTH.S333754
3. Neatrour K, McAlpine A, Owens TB, Trivedi RH, Poole Perry LJ. Evaluation of the etiology of persistent iritis after cataract surgery. J Ophthalmic Inflamm Infect. 2019;9(1):4. doi:10.1186/s12348-019-0170-2
4. Kessel L, Tendal B, Jorgensen KJ, et al. Post-cataract prevention of inflammation and macular edema by steroid and nonsteroidal anti-inflammatory eye drops: a systematic review. Ophthalmology. 2014;121(10):1915–1924. doi:10.1016/j.ophtha.2014.04.035
5. Haddad JE, Sabbakh NA, Macaron MM, et al. NSAIDs and corticosteroids for the postoperative management of age-related cataract surgery: a systematic review and meta-analysis. Am J Ophthalmol. 2024;260:1–13. doi:10.1016/j.ajo.2023.09.027
6. Low L, Shah V, Norridge CFE, Donachie PHJ, Buchan JC. Royal college of Ophthalmologists’ National Ophthalmology Database, report 10: risk Factors for post-cataract surgery endophthalmitis. Ophthalmology. 2023;130(11):1228–1230. doi:10.1016/j.ophtha.2023.07.021
7. Nouraeinejad A. Factors of noncompliance with prescribed eye drops in patients undergoing cataract surgery. J Med Access. 2023;7:27550834231152341. doi:10.1177/27550834231152341
8. Vandenbroeck S, De Geest S, Dobbels F, Fieuws S, Stalmans I, Zeyen T. Prevalence and correlates of self-reported nonadherence with eye drop treatment: the Belgian Compliance Study in Ophthalmology (BCSO). J Glaucoma. 2011;20(7):414–421. doi:10.1097/IJG.0b013e3181f7b10e
9. Ibach MJ, Zimprich L, Wallin DD, Olevson C, Puls-Boever K, Thompson V. In clinic optometrist insertion of Dextenza (Dexamethasone Ophthalmic Insert 0.4mg) prior to cataract surgery: the PREPARE Study. Clin Ophthalmol. 2022;16:2609–2615. doi:10.2147/OPTH.S374405
10. Gira JP, Sampson R, Silverstein SM, Walters TR, Metzinger JL, Talamo JH. Evaluating the patient experience after implantation of a 0.4 mg sustained release dexamethasone intracanalicular insert (Dextenza): results of a qualitative survey. Patient Prefer Adherence. 2017;11:487–494. doi:10.2147/PPA.S126283
11. Shapiro JN, Armenti ST, Levine H, Hood CT, Mian SI. Dexamethasone intracanalicular insert versus standard topical steroids for the prophylaxis of inflammation after cataract surgery. Am J Ophthalmol. 2024;268:174–180. doi:10.1016/j.ajo.2024.07.030
12. Larsen J, Whitt T, Parker B, Swan R. A randomized, controlled, prospective study of the effectiveness and safety of an intracanalicular dexamethasone ophthalmic insert (0.4 Mg) for the treatment of post-operative inflammation in patients undergoing Refractive Lens Exchange (RLE). Clin Ophthalmol. 2021;15:2211–2217. doi:10.2147/OPTH.S311070
13. Hoffman RS, Braga-Mele R, Donaldson K, et al. Cataract surgery and nonsteroidal antiinflammatory drugs. J Cataract Refract Surg. 2016;42(9):1368–1379. doi:10.1016/j.jcrs.2016.06.006
14. Malik A, Sadafale A, Gupta YK, Gupta A. A comparative study of various topical nonsteroidal anti-inflammatory drugs to steroid drops for control of post cataract surgery inflammation. Oman J Ophthalmol. 2016;9(3):150–156. doi:10.4103/0974-620X.192268
15. Rigas B, Huang W, Honkanen R. NSAID-induced corneal melt: clinical importance, pathogenesis, and risk mitigation. Surv Ophthalmol. 2020;65(1):1–11. doi:10.1016/j.survophthal.2019.07.001
16. Erichsen JH, Holm LM, Forslund Jacobsen M, Forman JL, Kessel L. Prednisolone and ketorolac vs ketorolac monotherapy or sub-tenon prophylaxis for macular thickening in cataract surgery: a randomized clinical trial. JAMA Ophthalmol. 2021;139(10):1062–1070. doi:10.1001/jamaophthalmol.2021.2976
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
0.2% Betamethasone Sodium Phosphate: A Multicenter, Randomized, Double-Masked Study to Compare Its Ocular Safety, Tolerability, and Efficacy to Vehicle in Cataract Surgery Subjects
Hosseini K, Gollamudi S, Reiser H, Walters T, Lindstrom RL
Clinical Ophthalmology 2023, 17:2219-2230
Published Date: 5 August 2023