Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Management of Glucocorticoid-Induced Hyperglycemia
Authors Shah P, Kalra S, Yadav Y, Deka N, Lathia T, Jacob JJ, Kota SK, Bhattacharya S, Gadve SS, Subramanium K, George J, Iyer V, Chandratreya S, Aggrawal PK, Singh SK ![]() , Joshi A, Selvan C, Priya G, Dhingra A, Das S
, Joshi A, Selvan C, Priya G, Dhingra A, Das S
Received 22 October 2021
Accepted for publication 9 February 2022
Published 23 May 2022 Volume 2022:15 Pages 1577—1588
DOI https://doi.org/10.2147/DMSO.S330253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Parag Shah,1 Sanjay Kalra,2 Yogesh Yadav,3 Nilakshi Deka,4 Tejal Lathia,5 Jubbin Jagan Jacob,6 Sunil Kumar Kota,7 Saptrishi Bhattacharya,8 Sharvil S Gadve,9 KAV Subramanium,10 Joe George,11 Vageesh Iyer,12 Sujit Chandratreya,13 Pankaj Kumar Aggrawal,14 Shailendra Kumar Singh,15 Ameya Joshi,16 Chitra Selvan,17 Gagan Priya,18 Atul Dhingra,19 Sambit Das20
1Department of Endocrinology, Gujarat Endocrine Centre, Ahmedabad, Gujarat, India; 2Department of Endocrinology, Bharti Hospital & B.R.I.D.E, Karnal, Haryana, India; 3Department of Endocrinology, MAX Super Specialty Hospital, Dehradun, Uttarakhand, India; 4Department of Endocrinology, Apollo Hospital & Dispur Polyclinic and Nursing Home, Guwahati, West Bengal, India; 5Department of Endocrinology, Apollo Hospital, Mumbai, Maharashtra, India; 6Department of Endocrinology, CMC Hospital, Ludhiana, Punjab, India; 7Department of Endocrinology, Diabetes and Endocrine Clinic, Berhampur, Orissa, India; 8Department of Endocrinology, OeHealth Diabates & Endocrinology Centre, Delhi, Delhi, India; 9Department of Endocrinology, Excel Endocrine Centre, Kolhapur, Maharashtra, India; 10Department of Endocrinology, Visakha Diabates & Endocrine Centre, Vishakhapatnam, Andhra Pradesh, India; 11Department of Endocrinology, Endodiab Clinic, Calicut, Kerala, India; 12Department of Endocrinology, St.John’s Medical College & Hospital, Bangalore, Karnataka, India; 13Department of Endocrinology, Endocare Clinic, Nashik, Maharashtra, India; 14Department of Endocrinology, Hormone Care & Research Centre, Ghaziabad, Uttar Pradesh, India; 15Department of Endocrinology, Endocrine Clinic, Varanasi, Uttar Pradesh, India; 16Department of Endocrinology, Endocrine and Diabetes Clinic, Mumbai, Maharashtra, India; 17Department of Endocrinology, Ramaiah Memorial Hospital, Bangalore, Karnataka, India; 18Department of Endocrinology, IVY Hospital, Chandigarh, Punjab, India; 19Department of Endocrinology, Bansal Hospital, Sri Ganganagar, Rajasthan, India; 20Department of Endocrinology, Endeavour Clinic, Bhubaneshwar, Orissa, India
Correspondence: Sanjay Kalra, Kunjpura Road, Model Town, Near State Bank of India, Sector 12, Karnal, Haryana, 132001, India, Tel +9215848555, Email [email protected]
Abstract: Glucocorticoids are potent immunosuppressive and anti-inflammatory drugs used for various systemic and localized conditions. The use of glucocorticoids needs to be weighed against their adverse effect of aggravating hyperglycemia in persons with diabetes mellitus, unmask undiagnosed diabetes mellitus, or precipitate glucocorticoid-induced diabetes mellitus appearance. Hyperglycemia is associated with poor clinical outcomes, including infection, disability after hospital discharge, prolonged hospital stay, and death. Furthermore, clear guidelines for managing glucocorticoid-induced hyperglycemia are lacking. Therefore, this consensus document aims to develop guidance on the management of glucocorticoid-induced hyperglycemia. Twenty expert endocrinologists, in a virtual meeting, discussed the evidence and practical experience of real-life management of glucocorticoid-induced hyperglycemia. The expert group concluded that we should be proactive in terms of diagnosis, management, and post-steroid care. Since every patient has different severity of underlying disease, clinical stratification would help understand patient profiles and determine the treatment course. Patients at home with pre-existing diabetes who are already on oral or injectable therapy can continue the same as long as they are clinically stable and eating adequately. However, depending on the degree of hyperglycemia, modification of doses may be required. Initiating basal bolus with correction regimen is recommended for patients in non-intensive care unit settings. For patients in intensive care unit, variable rate intravenous insulin infusion could be temporarily used, but under supervision of diabetes inpatient team, and patients can be transitioned to subcutaneous insulin once stable baseline assessment and continual evaluation are crucial for day-to-day decisions concerning insulin doses. Glycemic variability should be carefully monitored, and interventions to treat patients should also aim at achieving and maintaining euglycemia. Rational use of glucose-lowering drugs is recommended and treatment regimen should ensure maximum safety for both patient and provider. Glucovigilance is required as the steroids taper during transition, and insulin dosage should be reduced subsequently. Increased clinical and economic burden resulting from corticosteroid-related adverse events highlights the need for effective management. Therefore, these recommendations would help successfully manage GC-induced hyperglycemia and judiciously allocate resources.
Keywords: corticosteroids, insulin, steroid-induced hyperglycemia, steroid-induced diabetes, stress hyperglycemia, diabetes
Introduction
Glucocorticoids (GCs) are potent immunosuppressive and anti-inflammatory drugs and the recent COVID-19 pandemic has highlighted an urgent need to develop clear guidance on how to manage GC-induced hyperglycemia. GCs may be used as replacement therapy in people with adrenal insufficiency. But more commonly, they are used for their immunosuppressive and immunomodulatory properties for a wide variety of systemic and localized conditions (Table 1). The use of GCs needs to be weighed against their adverse effects of aggravating hyperglycemia in persons with diabetes mellitus (DM), unmask undiagnosed DM, or precipitate GC-induced DM appearance.1 The incidence of GC-induced hyperglycemia is 12%, and a recent meta-analysis suggested that the rate of GC-induced diabetes and hyperglycemia was 18.6% and 32.3%, respectively.2,3 In patients with organ transplant, who undergo GC treatment, the prevalence of abnormal glucose metabolism is between 17% and 32%.4
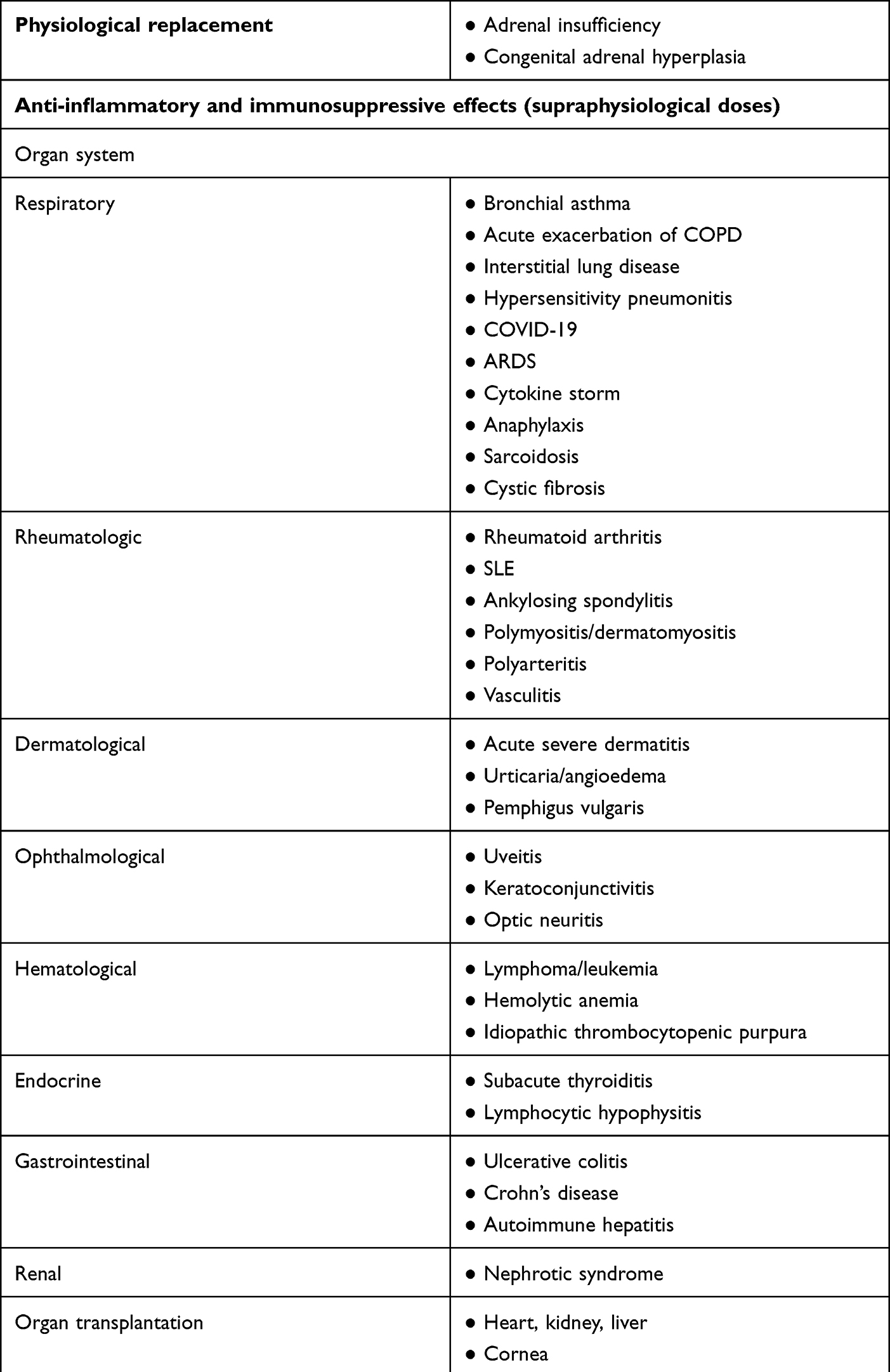 |
Table 1 Common Indications for Use of Glucocorticoid Therapy |
The pattern of glycemic excursions that are seen with GC use is associated with the type of GC used, its dose and regimen. While replacement doses cause the least amount of hyperglycemia, hyperglycemia can be marked in those on moderate to high doses, such as 7.5–30 and 30 mg per day prednisolone, respectively. When intermediate acting GCs are administered once daily (in the morning), hyperglycemia is more marked after 4–6 hours of the dose (seen mostly in late afternoon and evening time). However, when they are administered in 2–3 divided doses or with the use of long-acting GCs, hyperglycemia usually persists throughout the day. In addition, GCs cause a greater degree of post prandial hyperglycemia due to insulin resistance.5,6 Therefore, fasting blood glucose may be misleading and normal with a significant amount of hyperglycemia through the rest of the day.
GC-induced hyperglycemia should be controlled since hyperglycemia is associated with poor clinical outcomes, including infection, disability after hospital discharge, prolonged hospital stay, and death. Therefore, careful monitoring of glucose levels is recommended for reducing severity. Hyperglycemia screening for hospitalized COVID-19 patients: all admitted patients need to be evaluated for hyperglycemia at admission with at least 2 capillary blood glucose (CBG) values (1 pre-meal and 1 post-meal value) by a glucometer. Every patient with diabetes should be on a diabetic diet. Also, need to monitor the CBG values and titrate oral anti-hyperglycemic drugs (OAD)/insulin based on the protocols.47
Definition and Classification
The standard definitions for hyperglycemia have been described in Box 1.7–11
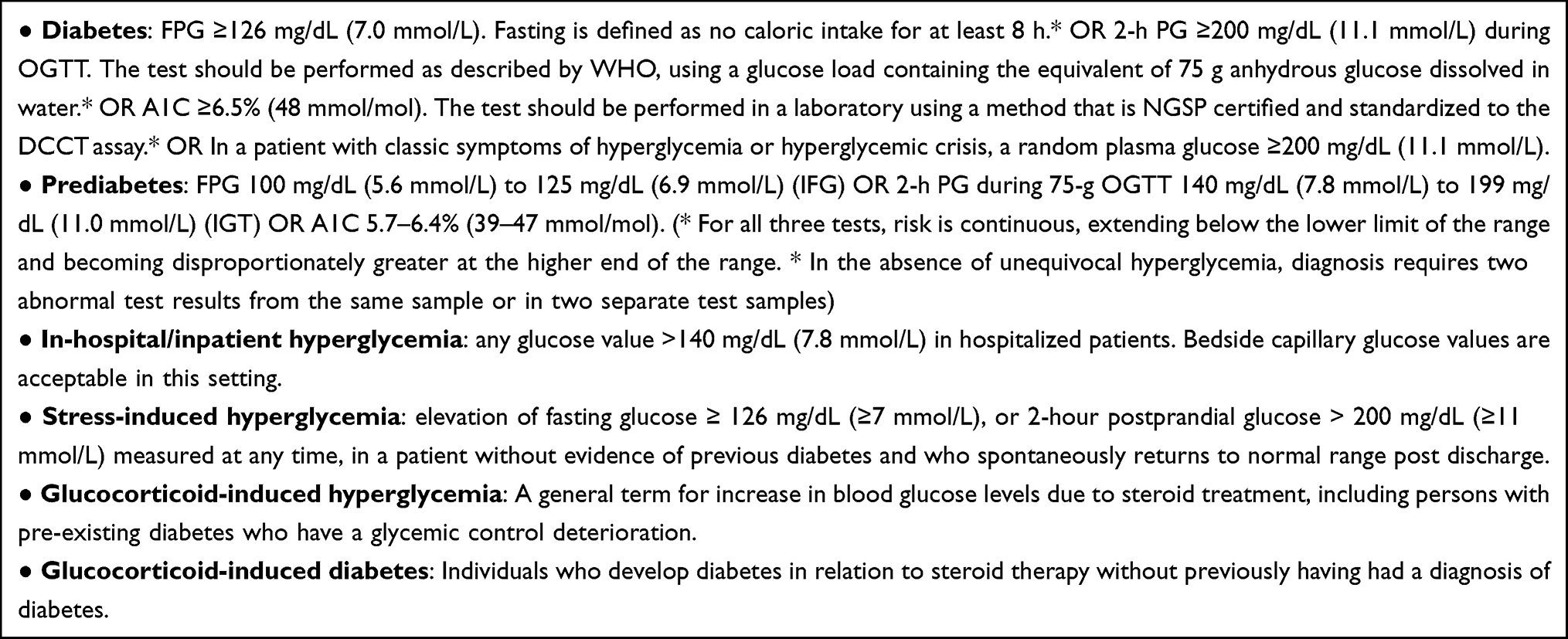 |
Box 1 Standard definitions for hyperglycemia |
This consensus document aims to develop guidance on the management of GC-induced hyperglycemia. Twenty expert endocrinologists, in a virtual meeting, discussed the evidence and practical experience of real-life management of GC-induced hyperglycemia. Regular contact was made over social media and email. Multiple interactions were done until consensus was reached. Published literature was compiled and presented to the expert group for review, and the discussions were used to prepare this document. Increased clinical and economic burden resulting from corticosteroid-related adverse events highlights the need for effective management.16 Therefore, these recommendations would help successfully manage GC-induced hyperglycemia and judiciously allocate resources.
Patient Clinical Considerations
Since every patient has different severity of underlying disease, clinical stratification helps understand patient profiles and determine treatment course. Clinical stratification can be based upon either management setting or the use of steroids. The risk of hyperglycemia depends on underlying profiles. Several factors need to be considered when managing hyperglycemia associated with the use of GCs, such as the underlying indication for the use of GCs, clinical severity of the disease, type of GC used, dose potency being used, and expected duration of use of GCs (Table 2). Other factors that need consideration include prior history of diabetes or steroid-induced hyperglycemia, background antidiabetic therapy, family history of diabetes, nutritional status, organ dysfunction, general well-being, and concomitant medications.
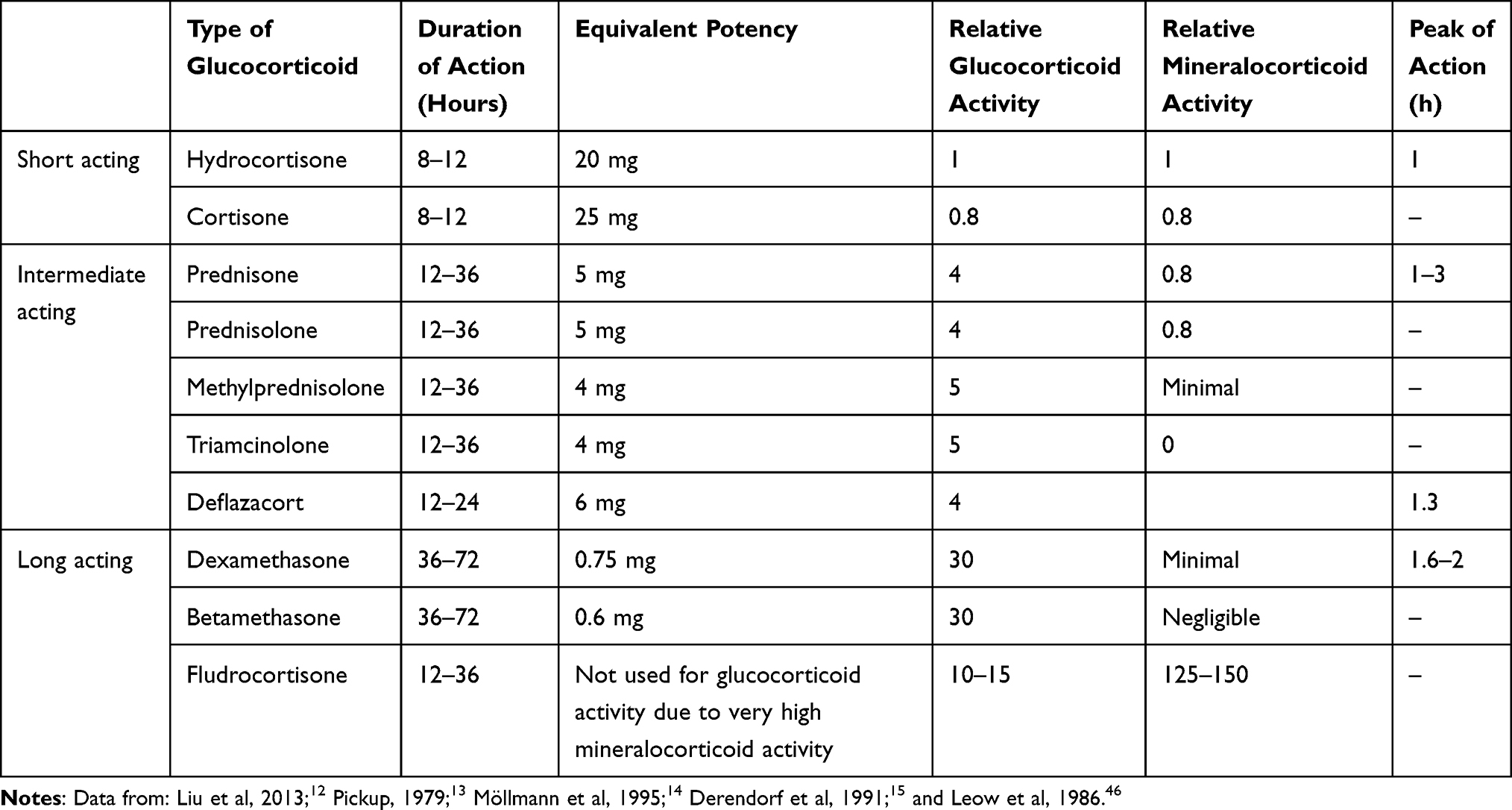 |
Table 2 Glucocorticoids in Clinical Use: Preparations and Equivalent Potency |
Management Setting
Home
GCs may be used in stable patients at home for a variety of conditions including some patients of COVID-19. The usual GC regimens being used in domiciliary care include prednisolone or methylprednisolone once daily (preferably in the morning) or twice daily or dexamethasone (once daily). Patients with adrenal insufficiency may be on hydrocortisone administered in three divided doses or once daily prednisolone. According to guidelines by the Joint British Diabetes Societies for inpatient care, taking steroid medications at home could elevate blood glucose levels, which require treatment. Individuals should be advised to monitor capillary blood glucose (CBG) regularly at home with a glucometer. Monitoring should not be restricted to only fasting blood glucose but should include post prandial and evening glucose values.18
Non-Intensive Care Unit/Ward
In the case of patients who are hospitalized in general ward areas and who are initiated on GC therapy, regular monitoring of CBG levels is advised.18 The usual dose regimens in the ward setting are similar to those used in domiciliary care. The pattern of glucose monitoring should include fasting as well as post-meal monitoring.
Intensive Care Unit
GCs are usually administered in high doses such as methylprednisolone 1–2 mg/kg/day or higher or dexamethasone 6 mg/day. This can result in significant hyperglycemia throughout the day. In addition, the type of nutrition and concomitant medications might also influence glycemia. Patients on enteral (Ryles tube) rather than oral feed have more marked hyperglycemia.19–23 Some centers administer RT feed as continuous feed with few hours of discontinuation at night, while others use bolus feeds administered every 2–3 hours. Monitoring should take into consideration the type of enteral feed. Parenteral nutrition may have a high glucose load and results in significant sustained hyperglycemia. Concomitant use of inotropes may also add to hyperglycemia. Intensive care unit (ICU) patients usually require blood glucose monitoring at 1–2 hourly intervals.
When there are resource constraints and in select patients where BG has been stable for over 24 hours, monitoring can be reduced to 3–4 hourly intervals. For patients on parenteral feed, the experts recommended glucose monitoring every 4 to 6 hours.24 Furthermore, if the patient is receiving intravenous insulin, blood glucose monitoring should be more frequent, ranging from 30 min to every 2 hours. Glucometer readings must be reliable in ICU patients, and blood from arterial or central venous lines can be used for bedside glucometer testing. If the capillary glucose does not match the clinical picture, a confirmatory lab sample should be sent.25
Baseline Assessment and Evaluation
Upon admission, the patient’s family history, concomitant medication, and clinical status, including illness severity, changes in the trajectory of glucose measures, concomitant medications, nutritional status, which could affect glucose levels, should be noted and included in day-to-day decisions concerning insulin doses.24 Random CBG should be performed at the time of hospital admission. Next, a pre-meal and 2-hour post-meal CBG should be performed with the first major meal in the hospital. If lab facilities are available, then blood samples should be sent for fasting plasma glucose (FPG) and glycosylated hemoglobin (HBA1c) the next morning. CBG should be monitored before each meal and, if possible, after meal as well for at least 2 days for underlying hyperglycemia if any of the test values are high (ie, Random CBG ≥ 180 mg/dL [10 mmol/L], Pre-meal ≥140 mg/dL [7.8 mmol/L], Post-meal ≥180 mg/dL [10 mmol/L], FPG ≥ 110 mg/dL [6.1 mmol/L], HbA1c ≥6.0%). Pharmacotherapy should be initiated if any of the test values meet the glycemic thresholds (ie, Random CBG ≥ 250 mg/dL [13.9 mmol/L], Pre-meal ≥150 mg/dL [8.3 mmol/L], 2 hours Post-meal ≥200 mg/dL [11.1 mmol/L]). HBA1c test should be performed at the time of diagnosis wherever possible. This would help detect pre-existing unknown diabetes and also provide information about the prior glycemic control in persons with known diabetes. It also assists in patient counseling and risk stratification. ADA recommends that A1C should be performed on all hospital-admitted patients with diabetes or hyperglycemia (blood glucose >140 mg/dL [7.8 mmol/L]) if not performed in the prior 3 months.24
Risk factors for GC-induced diabetes include a higher dose of steroids (prednisolone >20 mg, hydrocortisone >50 mg, dexamethasone >4 mg), as well as longer duration of steroids. Other risk factors include advanced age, higher BMI, previous glucose intolerance or impaired glucose tolerance, personal history of gestational diabetes or previous GC-induced hyperglycemia, family history of DM, HbA1C ≥6%.5
Monitoring and Therapeutic Targets
Glucose variability is reported to be an independent predictor of mortality in critically ill patients. Nevertheless, the role of intervention to control glycemic variability in improving outcomes is unknown.24 However, glycemic management can be challenging due to the variable nutritional status and consciousness level of a patient, which affects glycemic monitoring and overall patient safety. Therefore, glucose targets in hospital settings are modestly higher than commonly advised for persons with diabetes in outpatient settings.24,26 Optimal blood glucose targets should be <140 mg/dL (7.8 mmol/L) for pre-meal values and <180 mg/dL (10.0 mmol/L) for post-meal values. For ICU, target should be 140–180 mg/dL (7.8–10.0 mmol/L).
Optimal glycemic control improves outcomes. However, too aggressive lowering to near-normoglycemia has not been shown to be beneficial and significantly increases hypoglycemia risk.27 Glycemic targets according to AACE guidelines have been described in Box 2.24
 |
Box 2 Glycemic Targets (AACE) |
Choice of Therapy
The importance of matching glycemic profile of the GC administered with insulin has been highlighted in a previous study, where the experimental group received a “correctional insulin” that matched with the GC’s glycemic profile administered with or without “background” basal-bolus insulin. The study reported significantly lower mean blood glucose and glycemic variability in the experimental group.28 In patients receiving high-dose GC therapy, glucose monitoring for minimum of 48 hours and initiating insulin therapy, as appropriate, is recommended. For patients who are already undergoing hyperglycemia treatment, early adjustment of insulin dose is advised. Continuous glucose monitoring in real-time (rtCGM) or intermittently (iCGM) facilitates monitoring the “time in range” and is a potential tool for adjusting insulin doses.29 Hyperglycemia can be managed with different approaches depending on the patient’s clinical status (Table 3). The high load of hyperglycemia in hospitals creates challenges for health-care professionals. Administering GCs with maximum provider safety is challenging, but crucial. In overburdened wards, it may be difficult for health-care providers to administer insulin at the exact time.
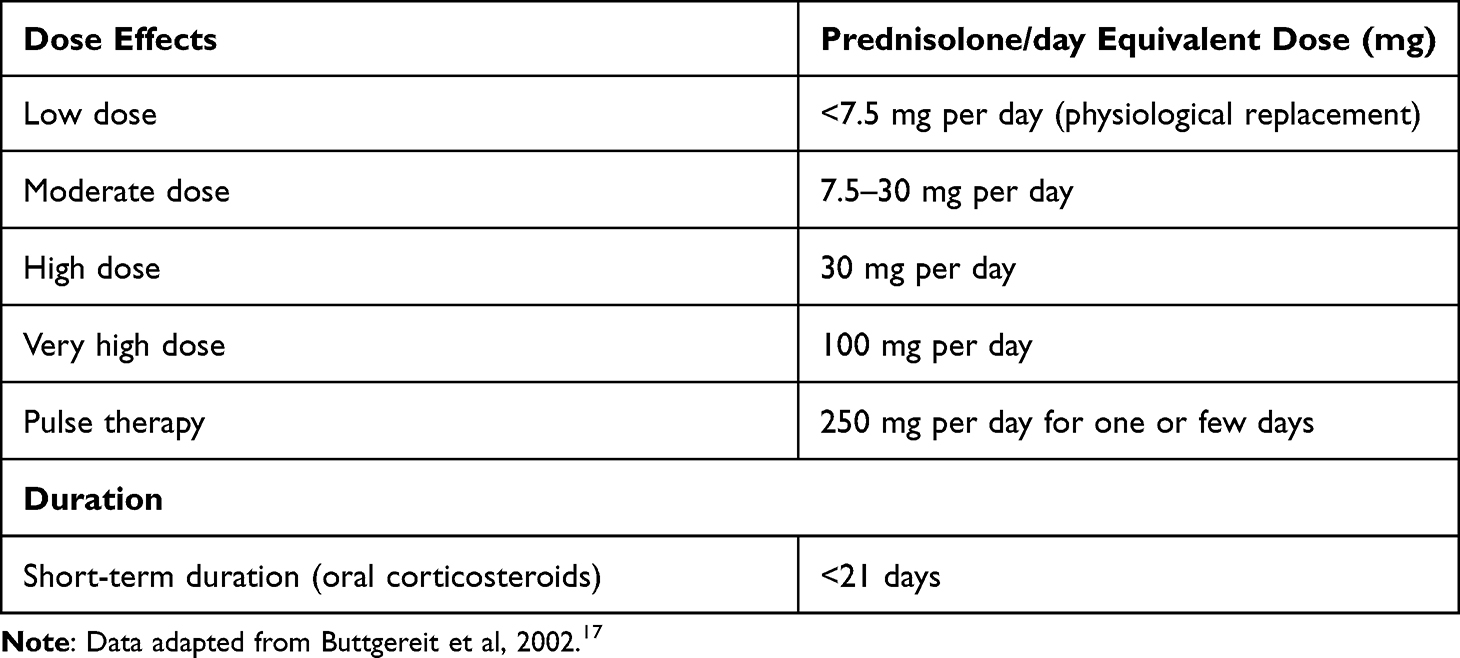 |
Table 3 Dose Treatment Regimens and Duration |
Insulin therapies for morning once-daily oral steroid-associated glucose excursion could include morning administration of basal human insulin. If hyperglycemia is present throughout the day till evening, basal analog insulin could be considered, and administration of basal insulin in the morning is recommended.18,30 The choice of insulin formulation and regimen should be based on the pharmacokinetic properties (especially dose and duration of action of the GC being used) and the pattern of hyperglycemia. For patients on once-daily prednisolone in the morning, hyperglycemia is usually seen in the noon and evening time. In such cases, the glucose-lowering profile of NPH insulin closely mimics the hyperglycemia pattern caused by intermediate-acting GC. Hence, NPH administered in the morning is considered a good choice. In patients who continue to have significant hyperglycemia, mealtime insulin can be added as required. In patients where intermediate-acting GCs are used in multiple divided doses or long-acting GCs are used, hyperglycemia usually persists over 24 hours. Therefore, a basal-bolus insulin regimen is the preferred choice.28
The dose of insulin should be based on the dose of GC. If the dose of prednisolone (or its equivalent dose of GC) is 10, 20, 30, or 40 mg, then the dose of NPH or basal insulin should be 0.1, 0.2, 0.3, 0.4 U/kg per day, respectively, as previously reported.5
Management of Patients in Domiciliary Care (Home)
Patients with pre-existing diabetes who are already on oral or injectable therapy can continue the same as long as they are clinically stable and eating adequately. However, depending on the degree of hyperglycemia, modification of doses may be required. Metformin, dipeptidyl peptidase-4 (DPP-4) inhibitors, sodium/glucose cotransporter-2 (SGLT2) inhibitors, pioglitazone, Glucagon-like peptide 1 receptor agonist (GLP1Ra), and existing insulin regimens should be continued. The dose of sulfonylurea can be increased if needed. Short-acting sulfonylurea or meglitinides can be added if the patient is not already on sulfonylureas. Other drugs usually take a longer time to act, so they will not help address acute hyperglycemia. In all such cases, insulin initiation should be considered. In the case of patients who are not eating reliably, oral antidiabetics should be discontinued, and the patient switched to insulin. The safety and efficacy of dapagliflozin have been evaluated in the DARE-19 trial, where, in non-critically ill patients hospitalized with COVID-19, no significant decrease in organ dysfunction or death, or improvement in recovery was observed compared with the placebo group.31
The British guidelines suggest that in people without a pre-existing diagnosis of diabetes, glucose should be monitored at least once daily, preferably before lunch or evening meal, or 1–2 hours after lunch or evening meal.
- If initial blood glucose is <216 mg/dL (12 mmol/L), testing should continue once before or following lunch or evening meal.
- If subsequent blood glucose >216 mg/dL (12 mmol/L), the frequency of testing should be increased to 4 times daily (before meals and before bed).
- If capillary glucose is consistently >216 mg/dL (12 mmol/L) (ie, on two occasions in 24 hours), the treatment algorithm for steroid-induced diabetes should be introduced.18
The group of experts agreed that, in OPD, glucose should be monitored before starting and then once or twice weekly post-lunch. In patients with no prior diabetes, monitoring before starting and daily pre- or post-lunch is recommended. In patients with prior diabetes, monitoring before starting and four times daily is recommended. The expert group also agreed that existing or current therapy should be continued in such patients.
The committee recommended initiating 10 units of basal human insulin with a daily dose increase of 10% to 20% to blood glucose level; however, some individuals may require up to 40% dose increments, as shown in some studies.18,26
Management with Long-Term Use of GCs
Persons on long-term steroid therapy should be monitored regularly and treatment should be given, as discussed. In case there is a change in dosage of corticosteroids, fluctuation in glucose control should be anticipated and managed proactively.
Management of Patients in Non-Intensive Care Unit Settings/Wards
The experts recommended initiating basal bolus with correction regimen. In the case of multiple daily doses of steroids, such as oral or intravenous dexamethasone, methylprednisolone or hydrocortisone or oral prednisolone, hyperglycemic effects can occur throughout the day. For patients who are clinically stable and eating orally, oral antidiabetic agents can be continued. For majority patients, subcutaneous insulin with basal or multiple daily injection regimens under the supervision of health care team is recommended. In case if once-daily insulin is insufficient in controlling hyperglycemia, twice daily premixed or basal bolus is recommended. Premix is associated with more hypoglycemia than basal bolus but has the benefit of fewer daily injections and better post prandial glucose control than the basal bolus.32–34 For patients on total parenteral nutrition more complex insulin regimen would be required. Blood glucose monitoring should be carefully monitored along with early interventions to prevent prolonged symptomatic hyperglycemia.35
If not feasible, initiating a combination of premix and oral therapy, including metformin, with or without short-acting sulfonylureas, meglitinides, DPP-4 inhibitors, at lunch is recommended. DPP-4 inhibitors inhibit glucagon secretion and promote insulin secretion, which is considered beneficial for treating GC-induced diabetes, and their use is also suggested in ICMR guidelines.36,37 Newer medications like GLP1ra can also be considered.35
Management During Pregnancy
Special situations may be encountered in pregnancy when antenatal corticosteroid (ACS) therapy has to be administered. ACS is recommended for women at risk of pre-term, irrespective of diabetes status, except in the case of medical conditions that could worsen with corticosteroid therapy. The nature and frequency of monitoring depend on the nature of diabetes, and medical nutrition is advised for patients receiving ACS regardless of previous glycemic status. Supplementary insulin could be proactively added for a minimal negative effect of hyperglycemia on mother and fetus. However, the therapy should be individualized for better management.38
Management of Patients in Intensive Care Unit
Oral non-insulin therapies might not be effective to achieve glucose control in acutely unwell hospital inpatients having significant hyperglycemia; in such cases, variable rate intravenous insulin infusion (VRIII) could be temporarily used but under the supervision of diabetes inpatient team.18 Patients on insulin infusion can be transitioned to subcutaneous insulin once stable. The approach should be to use a basal-bolus regimen with additional correction doses of insulin to be added to correct residual hyperglycemia. The sliding scale approach of insulin is retroactive and does not perform as well as the basal-bolus approach. A combination of basal insulin and correction insulin reportedly helps achieve a mean glucose value of 160 mg/dL (8.9 mmol/L). Similar results have been reported in another study that randomized patient group to receive only SSI; however, for 48% of patients, glycemic target could be achieved by the addition of intermediate-acting insulin.24,39 If not feasible, basal supported correction dose was recommended by the experts (Table 4).
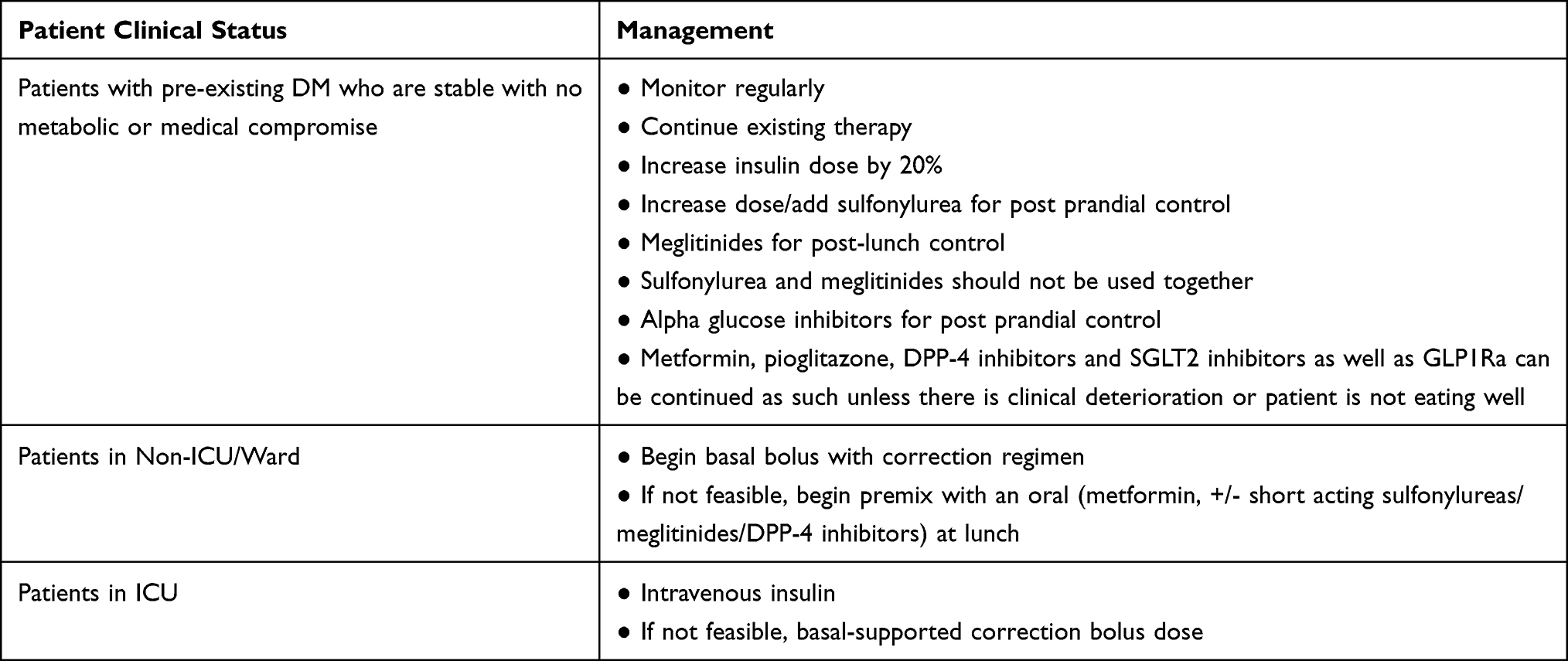 |
Table 4 Management of Glucocorticoid-Induced Hyperglycemia |
Transition Care
Patient education and staff training and hospital protocols for prevention, early detection, and prompt management of hypoglycemia are a must. The expert team recommended that, when a patient is discharged from the hospital on steroid therapy, proper education should be given regarding diabetes management, lifestyle, hyper- and hypoglycemia-associated risks, and the importance of blood glucose monitoring and the need to check blood glucose in the late afternoon or evening.18 Patients should be empowered to proactively adjust their insulin dose.
Patient empowerment should focus on nutrition, monitoring, insulin injection technique and storage, how to interpret BG values, insulin self-titration (eg, insulin sliding scale and titration scheme), prevention of hypoglycemia, warning symptoms and signs of hypoglycemia and how to correct hypoglycemia, and need for frequent contact (tele or otherwise) with the diabetes care team.
If steroids have been used for a shorter time, tapering is not required. Importantly, glucovigilance is recommended as the steroids get tapered, and insulin dosage should be proactively adjusted to avoid hypoglycemia.24 Blood glucose should be continuously monitored after steroid therapy and corresponding blood-glucose-lowering medication have been stopped, as returning to pre-steroid therapy blood-glucose levels is anticipated. HbA1c test 3 months post steroid therapy is recommended to check diabetes status.10 In some cases, retinopathy and other microvascular complications can occur even after normoglycemia is achieved; therefore, diabetes-related complications should be screened.40
Patients with hyperglycemia, who have been on steroid therapy, should be regularly monitored post-discharge to assess the status of the original disease for which steroids were given and also to assess if there is any long-term impact of steroids. This is especially important for persons who have had a significant medical illness and in those who have received a high dose of steroids for a relatively longer duration, such as patients with connective tissue disorders or after organ transplantation. Patients with diabetes taking oral glucose-lowering agents at the time of admission could follow the same medications on discharge, but with regular follow-up. DPP-4 inhibitors, including low-cost gliptins such as vildagliptin, are a safe option and associated with improved clinical outcomes in COVID-19 infected patients and decreased length of hospital stay.41,42 DPP-4 inhibitors decrease glycemic variability in patients with GC-induced diabetes and have shown significant improvements in post-prandial glucose levels after lunch and supper, as well as glycemic profiles, determined by CGM. In patients with GC-induced diabetes, DPP-4 inhibitors can minimize the risk of hypoglycemia.36 DPP-4 inhibitors could be safe and effective antidiabetic drugs for GC-induced diabetes. In patients with T2DM, DPP-4 inhibitors have shown higher improvement in glucose metabolism with less adverse events compared with metformin.43 Similarly, another study by Filozof et al has also reported DPP-4 inhibitors to be safe and effective for GC-induced diabetes.44 Once-daily pioglitazone could be appropriate for managing steroid-induced hyperglycemia provided there are no contraindications, such as fluid retention and heart failure. The role of GLP1Ra is unclear, but these could have a potential role in managing diabetes.45
The Joint British Diabetes Societies for inpatient care recommend that in patients without a previous diagnosis of diabetes before steroid use, hyperglycemia treatment should be titrated based on the decrease in steroid dose. Not all patients would need insulin and if the glycemic levels are not very high, initiating an OHS like DPP-4 inhibitor can be an option.43 For example, a weekly 5 mg reduction of prednisolone from 20 mg may require a 20–25% reduction in insulin dose, or a 40 mg reduction in gliclazide.18 In the case where GC treatment is stopped in the hospital, and hyperglycemia is resolved, post-discharge CBG could be discontinued. However, if GC treatment is stopped before discharge and hyperglycemia persists, then monitoring should be continued until normal glycemia is achieved or diabetes-specific test is undertaken (FBG, oral glucose tolerance test [OGTT], or HBA1c). Patients who do not have diabetes before steroid use should continue getting SMBG done until all glucose lowering therapy is stopped. Post that HbA1c should be done 3 monthly till normal and then annually. Annual testing should preferably include OGTT (if not, HbA1c and postprandial) as some patients may not have fasting hyperglycemia. Patients should also be advised to report if there are any osmotic symptoms. Patients with diabetes before steroid use should follow the Standard of Care.
Summary: Rational Pharmacotherapy
The expert group concluded that we should be proactive in terms of diagnosis, management, and post-steroid care. Insulin should be selected based on the steroid’s duration of action and frequency of administration, and the type of steroid and type of insulin should match. Replacement doses can lead to least amount of hyperglycemia; however, hyperglycemia can be marked in moderate to high doses. Fasting blood glucose could be misleading and normal even if there is significant hyperglycemia throughout the day. Key factors such as disease severity, underlying indication for GC use, as well as type, dose potency, and duration of GC used should be considered for hyperglycemia management. For ICU patients with persistent hyperglycemia, insulin therapy should be initiated at a maximum threshold of 180 mg/dL (10.0 mmol/L). After initiating insulin therapy, for most ICU patients, glucose range between 140 and 180 mg/dL (7.8–10.0 mmol/L) is recommended. Intravenous insulin infusions are advised for glycemic control in ICU patients, although care should be taken to follow validated protocols that have demonstrated safety and efficacy, and have low rates of hypoglycemia. Frequent glucose monitoring is recommended with IV insulin to minimal hypoglycemia chances and for optimal glucose control.
For majority of the insulin-treated non-ICU patients, premeal BG should be <140 mg/dL (<7.8 mmol/L) along with random BG values <180 mg/dL (<10.0 mmol/L), if these can be safely achieved. In stable patients, more stringent glycemic targets could be appropriate, whereas for patients with comorbidities or terminally ill patients, less stringent targets could be more appropriate. Glucose control can be best achieved and maintained by scheduled subcutaneous administration of insulin, along with basal, nutritional, and correction components. Continuing only SSI therapy is not recommended. For most hospitalized patients, who require therapy for hyperglycemia, non-insulin anti-hyperglycemic agents are not appropriate. Glucovigilance is required as the steroids taper during transition, and insulin dosage should be reduced subsequently.24
Abbreviations
GCs, glucocorticoids; DM, diabetes mellitus; CBG, capillary blood glucose; ICU, intensive care unit; GLP1Ra, Glucagon-like peptide 1 receptor agonist; DPP-4, dipeptidyl peptidase-4; SGTL2, sodium/glucose cotransporter-2; ACS, antenatal corticosteroid; VRIII, variable rate intravenous insulin infusion; FBG, fasting blood glucose; OGTT, oral glucose tolerance test; HBA1c, glycosylated hemoglobin; OAD, oral antihyperglycemic drug.
Acknowledgment
We also sincerely acknowledge the help of Harold Koenig, Duke University Medical Center and King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia, in revising and editing the second draft of this manuscript.
Editorial support in the development of this manuscript was provided by Eris Pharmaceuticals.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
Prof. Dr. Jubbin Jagan Jacob reports grants, personal fees from Novo Nordisk, grants, personal fees from Sanofi India Ltd, grants, personal fees from Biocon. The authors report no other conflicts of interest in this work.
References
1. Perez A, Jansen-Chaparro S, Saigi I, Bernal-Lopez MR, Miñambres I, Gomez-Huelgas R. Glucocorticoid-induced hyperglycemia. J Diabetes. 2014;6(1):9–20. doi:10.1111/1753-0407.12090
2. Blackburn D, Hux J, Mamdani M. Quantification of the risk of corticosteroid-induced diabetes mellitus among the elderly. J Gen Intern Med. 2002;17(9):717–720. doi:10.1046/j.1525-1497.2002.10649.x
3. Liu X, Zhu X, Miao Q, Ye H, Zhang Z. Hyperglycemia induced by glucocorticoids in nondiabetic patients: a meta-analysis. Ann Nutr Metab. 2014;65(4):324–332. doi:10.1159/000365892
4. Kwon S, Hermayer KL, Hermayer K. Glucocorticoid-induced hyperglycemia. Am J Med Sci. 2013;345(4):274–277. doi:10.1097/MAJ.0b013e31828a6a01
5. Suh S, Park MK. Glucocorticoid-induced diabetes mellitus: an important but overlooked problem. Endocrinol Metab. 2017;32(2):180–189. doi:10.3803/EnM.2017.32.2.180
6. Clore JN, Thurby-Hay L. Glucocorticoid-induced hyperglycemia. Endocr Pract. 2009;15(5):469–474. doi:10.4158/EP08331.RAR
7. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes—2021 | diabetes care. Available from: https://care.diabetesjournals.org/content/44/Supplement_1/S15.
8. Farrokhi F, Smiley D, Umpierrez GE. Glycemic control in non-diabetic critically ill patients. Best Pract Res Clin Endocrinol Metab. 2011;25(5):813–824. doi:10.1016/j.beem.2011.05.004
9. Kamceva G, Vavlukis M, Kitanoski D, Kedev S. Newly diagnosed diabetes and stress glycaemia and its’ association with acute coronary syndrome. Open Access Maced J Med Sci. 2015;3(4):607–612. doi:10.3889/oamjms.2015.103
10. Roberts A, James J, Dhatariya K; Joint British Diabetes Societies (JBDS) for Inpatient Care. Management of hyperglycaemia and steroid (glucocorticoid) therapy: a guideline from the Joint British Diabetes Societies (JBDS) for Inpatient Care group. Diabet Med. 2018;35(8):1011–1017. doi:10.1111/dme.13675
11. Castilla-Guerra L, Fernández-Moreno MC, Hewitt J. Treatment of hyperglycemia in patients with acute stroke. Revista Clínica Española. 2016;216(2):92–98. doi:10.1016/j.rceng.2015.08.002
12. Liu D, Ahmet A, Ward L, et al. A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. Allergy Asthma Clin Immunol. 2013;9(1):30. doi:10.1186/1710-1492-9-30
13. Clinical pharmacokinetics of prednisone and prednisolone - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/378499/.
14. Möllmann H, Hochhaus G, Rohatagi S, Barth J, Derendorf H. Pharmacokinetic/pharmacodynamic evaluation of deflazacort in comparison to methylprednisolone and prednisolone. Pharm Res. 1995;12(7):1096–1100. doi:10.1023/a:1016287104656
15. Derendorf H, Möllmann H, Barth J, Möllmann C, Tunn S, Krieg M. Pharmacokinetics and oral bioavailability of hydrocortisone. J Clin Pharmacol. 1991;31(5):473–476. doi:10.1002/j.1552-4604.1991.tb01906.x
16. Manson SC, Brown RE, Cerulli A, Vidaurre CF. The cumulative burden of oral corticosteroid side effects and the economic implications of steroid use. Respir Med. 2009;103(7):975–994. doi:10.1016/j.rmed.2009.01.003
17. Buttgereit F, da Silva J a P, Boers M, et al. Standardised nomenclature for glucocorticoid dosages and glucocorticoid treatment regimens: current questions and tentative answers in rheumatology. Ann Rheum Dis. 2002;61(8):718–722. doi:10.1136/ard.61.8.718
18. JBDS management of hyperglycaemia and steriod therapy_0.pdf. Available from: https://www.diabetes.org.uk/resources-s3/2017-09/JBDS%20management%20of%20hyperglycaemia%20and%20steriod%20therapy_0.pdf.
19. Gosmanov AR, Umpierrez GE. Management of hyperglycemia during enteral and parenteral nutrition therapy. Curr Diab Rep. 2013;13(1):155–162. doi:10.1007/s11892-012-0335-y
20. Pleva M, Mirtallo JM, Steinberg SM. Hyperglycemic events in non-intensive care unit patients receiving parenteral nutrition. Nutr Clin Pract. 2009;24(5):626–634. doi:10.1177/0884533609339069
21. Rosmarin DK, Wardlaw GM, Mirtallo J. Hyperglycemia associated with high, continuous infusion rates of total parenteral nutrition dextrose. Nutr Clin Pract. 1996;11(4):151–156. doi:10.1177/0115426596011004151
22. Arinzon Z, Shabat S, Shuval I, Peisakh A, Berner Y. Prevalence of diabetes mellitus in elderly patients received enteral nutrition long-term care service. Arch Gerontol Geriatr. 2008;47(3):383–393. doi:10.1016/j.archger.2007.09.001
23. Pancorbo-Hidalgo PL, García-Fernandez FP, Ramírez-Pérez C. Complications associated with enteral nutrition by nasogastric tube in an internal medicine unit. J Clin Nurs. 2001;10(4):482–490. doi:10.1046/j.1365-2702.2001.00498.x
24. Moghissi ES, Korytkowski MT, DiNardo M, et al. American Association of Clinical Endocrinologists and American Diabetes Association Consensus Statement on inpatient glycemic control. Diabetes Care. 2009;32(6):1119–1131. doi:10.2337/dc09-9029
25. Rice MJ, Smith JL, Coursin DB. Glucose measurement in the ICU: regulatory intersects reality. Crit Care Med. 2017;45(4):741–743. doi:10.1097/CCM.0000000000002274
26. Rodbard HW, Blonde L, Braithwaite SS, et al. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the management of diabetes mellitus. Endocr Pract. 2007;13(Suppl 1):1–68. doi:10.4158/EP.13.S1.1
27. Vaaler S. Optimal glycemic control in type 2 diabetic patients. Does including insulin treatment mean a better outcome? Diabetes Care. 2000;23(Suppl 2):B30–34.
28. Lakhani OJ, Kumar S, Tripathi S, Desai M, Seth C. Comparison of two protocols in the management of glucocorticoid-induced hyperglycemia among hospitalized patients. Indian J Endocrinol Metab. 2017;21(6):836–844. doi:10.4103/ijem.IJEM_226_17
29. Danne T, Nimri R, Battelino T, et al. International consensus on use of continuous glucose monitoring. Diabetes Care. 2017;40(12):1631–1640. doi:10.2337/dc17-1600
30. Dashora UK, Taylor R. Maintaining glycaemic control during high-dose prednisolone administration for hyperemesis gravidarum in Type 1 diabetes. Diabet Med. 2004;21(3):298–299. doi:10.1046/j.1464-5491.2003.01026_21_3.x-i1
31. DARE-19: dapagliflozin in high-risk patients hospitalized with COVID-19. American College of Cardiology. Available from: https://www.acc.org/latest-in-cardiology/articles/2021/05/12/19/08/http%3a%2f%2fwww.acc.org%2flatest-in-cardiology%2farticles%2f2021%2f05%2f12%2f19%2f08%2fsun-8am-dare-19-acc-2021.
32. Bellido V, Suarez L, Rodriguez MG, et al. Comparison of basal-bolus and premixed insulin regimens in hospitalized patients with type 2 diabetes. Diabetes Care. 2015;38(12):2211–2216. doi:10.2337/dc15-0160
33. Ilag LL, Kerr L, Malone JK, Tan MH. Prandial premixed insulin analogue regimens versus basal insulin analogue regimens in the management of type 2 diabetes: an evidence-based comparison. Clin Ther. 2007;29(6 Pt 1):1254–1270. doi:10.1016/j.clinthera.2007.07.003
34. Garber AJ, Ligthelm R, Christiansen JS, Liebl A. Premixed insulin treatment for type 2 diabetes: analogue or human? Diabetes Obes Metab. 2007;9(5):630–639. doi:10.1111/j.1463-1326.2006.00654.x
35. Use of variable rate intravenous insulin infusion in medical inpatients_0.pdf. Available from: https://www.diabetes.org.uk/resources-s3/2017-09/Use%20of%20variable%20rate%20intravenous%20insulin%20infusion%20in%20medical%20inpatients_0.pdf.
36. Yata Y, Hosojima M, Kabasawa H, et al. The assessment of the efficacy of dipeptidyl peptidase-4 inhibitors in patients with glucocorticoid-induced diabetes by continuous glucose monitoring. Intern Med. 2017;56(19):2555–2562. doi:10.2169/internalmedicine.8296-16
37. ICMR_GuidelinesType2diabetes2018_0.pdf. Available from: https://main.icmr.nic.in/sites/default/files/guidelines/ICMR_GuidelinesType2diabetes2018_0.pdf.
38. Kalra S, Kalra B, Gupta Y. Glycemic management after antenatal corticosteroid therapy. N Am J Med Sci. 2014;6(2):71–76. doi:10.4103/1947-2714.127744
39. Korytkowski MT, Salata RJ, Koerbel GL, et al. Insulin therapy and glycemic control in hospitalized patients with diabetes during enteral nutrition therapy: a randomized controlled clinical trial. Diabetes Care. 2009;32(4):594–596. doi:10.2337/dc08-1436
40. Diabetes in remission - Hillson - 2017 - practical diabetes - Wiley online library. Available from: https://wchh.onlinelibrary.wiley.com/doi/10.1002/pdi.2087.
41. Nafakhi H, Alareedh M, Al-Buthabhak K, Shaghee F, Nafakhi A, Kasim S. Predictors of adverse in-hospital outcome and recovery in patients with diabetes mellitus and COVID-19 pneumonia in Iraq. Diabetes Metab Syndr. 2021;15(1):33–38. doi:10.1016/j.dsx.2020.12.014
42. Gupta Y, Goyal A, Kubihal S, Golla KK, Tandon N. A guidance on diagnosis and management of hyperglycemia at COVID care facilities in India. Diabetes Metab Syndr. 2021;15(1):407–413. doi:10.1016/j.dsx.2021.01.015
43. Yanai H, Masui Y, Yoshikawa R, Kunimatsu J, Kaneko H. Dipeptidyl peptidase-4 inhibitor for steroid-induced diabetes. World J Diabetes. 2010;1(3):99–100. doi:10.4239/wjd.v1.i3.99
44. Filozof C, Schwartz S, Foley JE. Effect of vildagliptin as add-on therapy to a low-dose metformin. World J Diabetes. 2010;1(1):19–26. doi:10.4239/wjd.v1.i1.19
45. López-Carmona MD, Gómez-Huelgas R, Corpas E. Chapter 17 - diabetes mellitus in the elderly. In: Corpas E, editor. Endocrinology of Aging. Elsevier; 2021:547–576. doi:10.1016/B978-0-12-819667-0.00017-2
46. Loew D, Schuster O, Graul EH. Dose-dependent pharmacokinetics of dexamethasone. Eur J Clin Pharmacol. 1986;30(2):225–320. doi: 10.1007/BF00614309
47. Clinical Guidance on Diabetes Management at COVID-19 Patient Management Facility; Version 1.0. AIIMS; 2020. Available from: https://covid.aiims.edu/wp-content/uploads/2020/07/Diabetes-management-at-COVID-facility..pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.