Back to Journals » Infection and Drug Resistance » Volume 19
Management of Diabetic Foot Infections Using Phage Therapy
Authors Nazari M, Shokoohizadeh L
Received 29 October 2025
Accepted for publication 30 January 2026
Published 4 February 2026 Volume 2026:19 577526
DOI https://doi.org/10.2147/IDR.S577526
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Mohsen Nazari,1 Leili Shokoohizadeh2
1Department of Microbiology, School of Medicine, Hamadan University of Medical Sciences, Hamadan, Iran; 2Infectious Disease Research Center, Avicenna Institute of Clinical Sciences, Avicenna Health Research Institute, Hamadan University of Medical Sciences, Hamadan, Iran
Correspondence: Leili Shokoohizadeh, Infectious Disease Research Center, Avicenna Institute of Clinical Sciences, Avicenna Health Research Institute, Hamadan University of Medical Sciences, P.O.Box: 6517838678, Hamadan, Iran, Tel +989335068305, Fax +98-8118276299, Email [email protected]
Abstract: Diabetic foot infections (DFIs) represent a major and increasing complication of diabetes mellitus, often leading to hospitalization, osteomyelitis, and lower limb amputation. The rising prevalence of multidrug-resistant pathogens in DFIs has limited the effectiveness of conventional antibiotic therapy, emphasizing the need for alternative or adjunctive approaches. Bacteriophage therapy has emerged as a promising strategy due to its specificity to target bacteria, ability to penetrate and disrupt biofilms, and activity against multidrug-resistant organisms, while generally demonstrating a favorable safety profile with minimal effects on host tissues. This review critically evaluates current evidence for phage therapy in DFIs, which is dominated by in vitro studies, animal models, and a limited number of compassionate use and small clinical series. Reported outcomes show effectiveness against key pathogens including Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella pneumoniae, Acinetobacter baumannii, Escherichia coli, and Enterococcus species, with preliminary evidence of reduced bacterial burden and improved wound healing in select patients. Despite these encouraging findings, clinical translation is challenged by narrow phage host ranges, the need for rapid phage-pathogen matching, standardization of production, regulatory hurdles, and incomplete understanding of pharmacokinetics and host immune interactions. Therefore, while phage therapy represents a potentially safe and effective adjunct to conventional DFI management, further well-designed preclinical studies and randomized clinical trials, alongside optimized delivery systems and regulatory frameworks, are required to fully establish its clinical utility.
Keywords: diabetic foot infections, phage therapy, antibiotics
Introduction
Diabetes mellitus (DM) is an increasingly prevalent chronic condition, affecting millions globally.1 As of 2019, approximately 436 million people were living with DM, and this number is projected to rise to 578 million by 2030.2 This rapid increase in DM prevalence is paralleled by a surge in complications and hospitalizations, placing an immense burden on healthcare systems worldwide.3 Among these complications, diabetic foot infections (DFIs) have emerged as one of the most serious, accounting for a significant portion of diabetes-related hospitalizations.4 Individuals with DM face a hospitalization risk for DFIs that is 50 times higher than those without the condition.5
Chronic wounds in people with diabetes encompass a heterogeneous spectrum of pathological entities. Diabetic foot ulcers represent open lesions of the skin and underlying tissue that typically arise from neuropathy, ischemia, or mechanical trauma, whereas diabetic foot infections refer specifically to the microbial invasion of these ulcers or adjacent tissues, often characterized by local and systemic inflammatory responses.6 This distinction is clinically relevant, as not all diabetic foot ulcers are infected, yet progression to infection markedly increases morbidity, treatment complexity, and the risk of limb loss.7
The clinical management of DFIs is particularly challenging due to the high rate of infectious complications.8 Around 60% of diabetic foot ulcers (DFUs) progress to infection, with osteomyelitis being one of the most common and severe outcomes.9 Osteomyelitis is not only difficult to treat but is also associated with alarmingly high rates of amputation, occurring in 10–15% of patients with moderate infections and in 50–60% of those with severe infections.10 The conventional treatment approach typically involves prolonged antibiotic regimens or, in severe cases, amputation.11 However, these strategies come with significant limitations. Extended antibiotic use can promote antimicrobial resistance, severely limiting future treatment options and exacerbating a growing global health crisis.11,12 Amputation, on the other hand, carries profound psychological and physical consequences, including significant anxiety and reduced quality of life.13,14 The growing prevalence of multidrug resistant organisms in this setting further constrains therapeutic options and is now recognized as a major driver of treatment failure and recurrence.15
Given these challenges, there is an urgent need for innovative therapies that can more effectively manage DFIs while mitigating the risks associated with current treatment modalities. Bacteriophages (phages), naturally occurring viruses that specifically target and kill bacteria, represent a promising alternative. First used therapeutically in 1919, phage therapy lost prominence with the advent of antibiotics, which were initially easier to produce and administer and less prone to resistance.16 However, the escalating crisis of antibiotic resistance has reignited global interest in phage therapy.17,18
Phage therapy has shown considerable promise in treating a wide range of infections, including chronic wounds, with minimal adverse effects.19,20 Notably, phages are capable of penetrating and degrading biofilms, which are often implicated in the chronicity and antibiotic resistance of DFIs.21,22 This unique ability to overcome biofilm-related treatment failures positions phage therapy as a potentially transformative approach in the management of DFIs.23 Preliminary clinical observations have suggested reductions in bacterial burden and improved wound healing in select patients; however, robust randomized controlled trials remain scarce, and the overall quality of clinical evidence is still limited.24
This review employs a narrative synthesis methodology, incorporating findings from recent preclinical and clinical studies to provide a comprehensive overview of the application of phage therapy in DFIs. By synthesizing current evidence systematically, this approach allows the reader to understand the efficacy, limitations, and potential clinical implications of phage therapy in managing these complex infections. The purpose of this review is to critically evaluate the current evidence on the application of phage therapy in managing DFIs. By exploring its potential benefits, limitations, and clinical implications, this review aims to underscore the importance of integrating phage therapy into the treatment arsenal for DFIs, potentially offering a more effective and sustainable solution to this growing global health challenge.
Microbial Composition in Diabetic Foot Infections
DFIs are typically polymicrobial, involving a complex community of aerobic and anaerobic bacteria. The most commonly isolated pathogens include Staphylococcus aureus and Pseudomonas aeruginosa, along with other Gram-positive and Gram-negative bacteria.5,25,26
Staphylococcus aureus
S. aureus is a Gram-positive bacterium known for causing a wide range of infections, including severe wound infections, skin and soft tissue infections, and osteomyelitis, due to its evolving strains.27 S. aureus frequently colonizes the skin and mucosal surfaces, particularly in children, as well as in individuals with HIV or diabetes, who are more susceptible to colonization by this pathogen.28–30 Hospital-acquired methicillin-resistant S. aureus (MRSA) strains are prevalent in clinical settings and typically infect immunocompromised patients, whereas community-associated MRSA strains can cause infections in otherwise healthy children and adults.31–33
Diabetic patients are at a higher risk of MRSA colonization and infection, which can significantly impact their clinical outcomes. A meta-analysis by Stacey et al revealed that the prevalence of MRSA colonization among diabetic patients is notably higher than in non-diabetics, with a pooled colonization rate of 9.2% among 11,577 diabetic patients. Furthermore, MRSA prevalence in DFIs was reported to be 16.78% among 10,994 cases, underscoring the importance of targeted screening and alternative therapeutic strategies.34 Similarly, a systematic review by Zhou et al analyzed MRSA prevalence in DFUs across 20 countries, reporting an overall prevalence of 17%, with notable regional differences: 61% in South America, 20% in North America, 19% in Europe, 13% in Africa, and 11% in other regions.35
Although vancomycin-resistant S. aureus (VRSA) remains rare, its emergence poses an additional therapeutic challenge, emphasizing the need for continuous surveillance.36,37
S. aureus is the most common DFI isolate, often delaying wound healing and increasing amputation risk.38,39 In patients with DFIs, MRSA infections are particularly concerning. Qi et al reported that among hospitalized patients with MRSA infections, 46.9% developed osteomyelitis and 40.8% underwent amputation or experienced disability, significantly higher than in patients infected with other pathogens.40 Saltoglu et al observed that MRSA accounted for 19.4% of isolates, and inappropriate initial therapy was associated with reinfection and adverse outcomes.41 Gramberg et al reported a hazard ratio (HR) for amputation of 0.7 (95% CI: 0.39–1.1) and HR for mortality of 0.89 (95% CI: 0.49–1.6) for S. aureus infections, indicating a moderate but clinically significant impact on patient outcomes.42 Methicillin-resistant S. epidermidis (MRSE) and MRSA from DFUs also exhibit high multidrug resistance (MDR).43
Pseudomonas aeruginosa
P. aeruginosa is a Gram-negative bacterium that plays a significant role in the pathogenesis of DFUs.44 Saltoglu et al found that 18.2% of P. aeruginosa isolates were MDR, and Gramberg et al reported that Gram-negative infections, including P. aeruginosa, were associated with a HR for amputation of 1.3 (95% CI: 0.78–2.1) and HR for mortality of 2.6 (95% CI: 1.4–4.8), highlighting their contribution to severe clinical outcomes and higher morbidity.41
Garousi et al conducted a global analysis of P. aeruginosa in DFU infections. Their systematic review identified a global prevalence of 16.6% for P. aeruginosa in DFUs, with the rates varying by region: 18.5% in Asia, 16.3% in Africa, and 11.1% in Western countries.45 However, a recent systematic review and meta-analysis by Makeri et al focused on the prevalence of P. aeruginosa and S. aureus in DFUs across Africa, revealing that S. aureus (19.9%) is more frequently isolated than P. aeruginosa (11.8%). Despite this, P. aeruginosa isolates demonstrated a concerning MDR rate of 41.8%, emphasizing the need for antimicrobial stewardship and alternative therapeutic approaches.46
In patients with DM, the presence of P. aeruginosa in DFUs is associated with prolonged wound healing, increased risk of complications, and higher rates of morbidity.47 Despite its importance, P. aeruginosa is often overtreated empirically. Veve et al found it in only 9% of DFU cultures, suggesting that antipseudomonal coverage should be reserved for patients with specific risk factors, such as prior treatment failure or immunocompromise.48 Intrinsic resistance mechanisms of P. aeruginosa include low outer membrane permeability and efflux pumps, conferring resistance to many beta-lactams (except antipseudomonal penicillins, ceftazidime, cefepime, and carbapenems excluding ertapenem), aminoglycosides, and fluoroquinolones.49
Klebsiella pneumoniae
K. pneumoniae is a Gram-negative bacterium that has become an increasingly important pathogen in DFIs.50 Although it is typically a part of the normal microbiota in the human gastrointestinal tract, it can transform into a highly pathogenic opportunistic organism, particularly in patients with diabetes due to impaired immunity, poor tissue perfusion, and delayed wound healing.51,52
In the study by Sultana et al, K. pneumoniae was identified as a prevalent Gram-negative bacterium in DFUs, though the specific prevalence rate within their study is not directly provided. The study, which included data from 73 studies across 12 Asian countries, highlighted that K. pneumoniae is part of the 77% of DFU infections attributed to Gram-negative bacteria.53
Recent evidence further indicates that K. pneumoniae infections in DFIs are associated with more severe disease outcomes compared to other Gram-negative pathogens. These infections have been linked to prolonged wound healing, higher incidence of osteomyelitis, and increased rates of lower-limb amputation in affected patients.54 For example, in a study of 122 DFU patients, K. pneumoniae isolates demonstrated high resistance to commonly used antibiotics, including carbapenems, which limited therapeutic options and was associated with more complicated clinical courses.
A major challenge in treating K. pneumoniae infections in DFUs is the emergence of MDR strains. According to the study by Yang et al the prevalence of MDR K. pneumoniae in DFUs was found to be 3.50% (95% CI: 2.31–4.91%).15 Many strains of K. pneumoniae have developed resistance to multiple antibiotics, including those commonly used to treat DFIs. This resistance is often due to the production of extended-spectrum beta-lactamases (ESBLs) and carbapenemases, enzymes that break down a wide range of antibiotics, rendering them ineffective.55 The presence of these resistant strains significantly limits treatment options and increases the likelihood of complications such as osteomyelitis (bone infection) and, in severe cases, the need for amputation.56 Additionally, extensively drug-resistant (XDR) K. pneumoniae strains have been increasingly reported in chronic wounds, displaying near-total resistance to ampicillin, amoxicillin, and nitrofurantoin, with only relative susceptibility to amikacin, highlighting the clinical threat posed by these pathogen.57,58
The pathogenicity of K. pneumoniae in DFIs is driven by several virulence factors. These include adhesins, which facilitate bacterial attachment to host tissues; capsules, which protect bacteria from phagocytosis; and siderophores, which enable iron acquisition essential for bacterial proliferation.59 Moreover, robust biofilm formation by K. pneumoniae contributes to persistent infection, resistance to host defenses and antibiotics, and the chronicity of DFIs. These factors collectively explain why highly pathogenic K. pneumoniae infections often result in more severe clinical outcomes, delayed wound healing, and increased risk of amputation.60
Acinetobacter baumannii
A. baumannii is a Gram-negative bacterium that has gained notoriety as a highly resilient and opportunistic pathogen, particularly in healthcare settings.61 It is increasingly implicated in DFIs, where it poses significant challenges due to its ability to survive in harsh conditions and its resistance to multiple antibiotics.33,62 A. baumannii is known as one of the microorganisms associated with a higher incidence of amputation.63 In diabetic patients, A. baumannii can exploit the compromised immune system, poor circulation, and delayed wound healing that are characteristic of diabetes.64 These factors create a favorable environment for the bacterium to colonize and cause infection in DFUs.65 A significant concern with A. baumannii infections in DFIs is the notorious resistance of the bacterium to antibiotics. Many strains of A. baumannii are MDR, often displaying resistance to a wide range of antibiotics, including carbapenems, which are typically used as a last resort in treating severe bacterial infections.66 This resistance is largely due to the bacterium’s ability to acquire and express various resistance genes, often through mobile genetic elements such as plasmids, transposons, and integrons.67 The emergence of these MDR strains severely limits the available treatment options, increasing the risk of complications such as osteomyelitis, sepsis, and, in extreme cases, the need for amputation.68
Escherichia coli
E. coli, a Gram-negative bacterium commonly found in the gastrointestinal tract, is emerging as a significant pathogen in DFIs.69,70 In studies by Idrees et al and Jain et al, E. coli was found in 41.6% of 180 samples and 20% of 150 diabetic patients with foot ulcers, respectively.71,72 Traditionally associated with urinary tract infections and gastrointestinal illnesses, E. coli is now increasingly recognized for its role in DFIs, particularly in polymicrobial infections, where it can worsen wound severity and complicate treatment.73 In DFUs, E. coli often colonizes wounds alongside other Gram-negative and Gram-positive bacteria.74
A major determinant of therapeutic failure in E. coli associated DFIs is the production of extended spectrum beta lactamases, which represents the principal resistance mechanism in this species.75 Saltoglu et al reported that 38.5% of E. coli isolates were ESBL producers, and reinfections were more common in patients with inadequate initial therapy.41 Zambelli et al found that E. coli accounted for 8.3% of isolates and was associated with polymicrobial infections, which increase the risk of complications, treatment failure, and chronicity.76
The compromised immune system in diabetic patients, coupled with poor circulation and delayed wound healing, creates an environment that fosters the growth and persistence of E. coli and other pathogens.77 This bacterium is especially problematic in chronic and deep infections, where it contributes to the complexity and chronicity of the infection.78
Enterococcus spp
Enterococcus spp., particularly E. faecalis and E. faecium, are significant pathogens in DFIs. Perzon et al focused on the prevalence and impact of Enterococcal infections in DFUs. Their study, conducted at the Hadassah Medical Center, found that enterococci were present in 35% of DFUs. These infections were predominantly polymicrobial and were associated with higher rates of amputation and longer hospital stays compared to non-Enterococcal infections.79 Gramberg et al reported that Enterococcus infections were associated with HR for amputation of 0.73 (95% CI: 0.38–1.4) and HR for mortality of 0.73 (95% CI: 0.38–1.4), indicating moderate influence on severe outcomes compared to Gram-negative pathogens.42
In DFIs, Enterococcus spp. are often found in polymicrobial infections, coexisting with other pathogens such as S. aureus, P. aeruginosa, and various anaerobes.80,81 The presence of Enterococcus spp. complicates treatment, as these bacteria frequently exhibit resistance to multiple antibiotics, including vancomycin, a major concern in clinical settings.38 Saltoglu et al additionally found vancomycin-resistant Enterococcus in 7% of isolates, complicating treatment and prolonging hospital stay.41
Biological Phages
Phages, or bacteriophages, are the most abundant biological entities on Earth.82 They are ubiquitous, found in soil, seawater, and on various surfaces, including extreme environments with very high or low temperatures. Additionally, they are present in hospitals, wastewater, and wherever bacteria are found, including animal and human tissues.83 Thousands of phages have been described and classified based on their morphological characteristics, nucleic acid content, typical habitats, and the bacterial species they infect.84
Phages are commonly classified according to their tail structures and biological cycles.85 This classification divides phages into two main groups: lytic (virulent) and lysogenic (temperate) phages. In the lytic cycle, phages attach to and invade bacterial cells, but they can only bind to specific bacterial receptors that match their tail structures (Figure 1). Due to the high rate of mutations in both phages and bacterial receptors, often mediated by the phages themselves, each phage can infect a limited number of bacterial strains or sometimes only a single strain.86 This specificity explains the precise targeting of phages. Once inside the bacterial cell, the phage hijacks the bacterial machinery to produce its own genome and proteins. The phage then assembles and packages new virions before lysing the host cell to release these new phages, which can infect other bacterial cells.86 The burst size, or the number of new phages produced, can vary depending on the characteristics of the phage, the pathogens it targets, and the environmental conditions.87
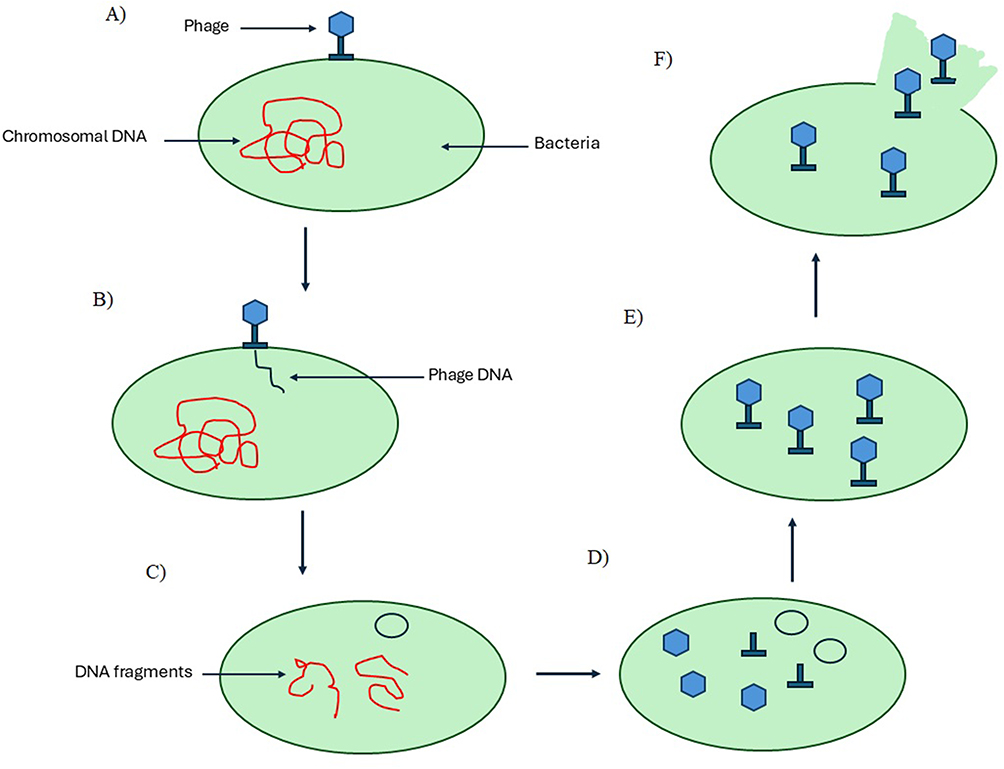 |
Figure 1 Mechanism of phage therapy. (A) The bacteriophage first attaches firmly to the surface of the bacterial host, recognizing specific receptors on the bacterial cell wall, which ensures host specificity. (B) Next, the bacteriophage injects its viral genome into the bacterial cell, transferring the genetic instructions necessary for viral replication directly into the host cytoplasm. (C) Once inside, the bacteriophage genome triggers the degradation of the bacterial host’s DNA, effectively shutting down the host’s normal cellular functions and redirecting resources toward viral production. (D) The host machinery is then hijacked to synthesize viral components, including structural proteins and nucleic acids, allowing the replication of new phage particles. (E) These newly produced components self-assemble into complete, mature bacteriophages, ready for release. (F) Finally, the bacterial cell undergoes lysis, breaking open its membrane and releasing the newly formed bacteriophages into the environment to infect additional bacterial cells, continuing the cycle. |
In contrast, the lysogenic cycle involves the integration of the phage’s genetic material into the host’s genome. During cell division, the viral DNA is replicated along with the bacterial DNA and passed to daughter cells. The phage remains dormant within the bacterial genome and only rarely exits this state to enter the lytic cycle.88 Due to their ability to precisely target and kill bacteria, only lytic phages are used for therapeutic purposes.
Advantages of Phages Therapy
Phages offer several theoretical and practical advantages over traditional antibiotics in treating bacterial infections. One notable benefit is that, theoretically, no bacterium is immune to all phages. While antibiotics often have broad spectra of activity, no single antibiotic can eradicate every bacterial species. The most compelling attribute of phages is their specificity; they target only the bacteria they are designed to recognize and infect.89
Phages have a narrow spectrum of activity, which helps avoid one of the major drawbacks of antibiotics: disruption of the entire microbiome. Antibiotics can kill not only harmful bacteria but also beneficial ones, leading to secondary infections and the emergence of resistant strains.90 Studies have shown that phages can be used without adversely affecting the microbiota. For instance, research with mice demonstrated that oral administration of T4-like phages targeting E. coli associated with diarrhea did not harm non-pathogenic E. coli strains.91 Similarly, a study by Sarker et al found that administering an oral cocktail of nine T4-like E. coli phages to healthy adults for two days did not alter gut microbiota composition, despite the presence of phages in feces.92
Compared to antibiotics, phages offer several additional benefits. They are generally considered safer and better tolerated because they replicate only within target bacteria and do not infect mammalian cells. This safety profile is supported by historical use in Eastern Europe and recent studies in animals and humans, which have not reported significant adverse effects following phages therapy.93 Furthermore, phages may require fewer doses and can remain in the body for longer periods, reducing the need for frequent administration, unlike antibiotics that often require multiple doses over several days.94,95 Phages are also effective at targeting infections in areas difficult for antibiotics to reach, such as certain body organs or systems. For example, the lytic phage EC200 (PP), effective against the fatal neonatal meningitis strain of E. coli, successfully treated infected pups in a meningitis model even with low phage titers in the central nervous system.96
Advancements in cost-effective DNA sequencing and synthesis technologies have enabled the engineering of phages to address some limitations of antibiotics. For instance, phages can be engineered to disrupt biofilms, which are resistant to standard antibiotic treatments even when the bacteria are susceptible to the drugs.97 An in vitro study demonstrated that a biofilm-degrading enzyme incorporated into a phages reduced bacterial biofilm cell counts by approximately 99.9%.98 Additionally, genetic modifications in phages can combat bacterial resistance to antibiotics. For example, Edgar et al introduced genes into lysogenic phages that conferred sensitivity to streptomycin and nalidixic acid in resistant strains, significantly reducing their minimal inhibitory concentrations.99
Finally, phages may be a more cost-effective alternative to antibiotics, especially for treating MDR pathogens. A study by Miedzybrodzki et al found that phage therapy significantly reduced healthcare costs for patients with MRSA infections.100
Phage Therapy for Diabetic Foot Infections
DFIs represent a significant challenge in clinical management due to the persistent presence of MDR bacterial pathogens. With the growing limitations of antibiotics, phage therapy has emerged as a promising alternative for treating chronic wounds associated with diabetes. Recent studies have demonstrated the efficacy of bacteriophages in targeting key bacterial pathogens, reducing biofilm formation, and accelerating wound healing (Table 1).
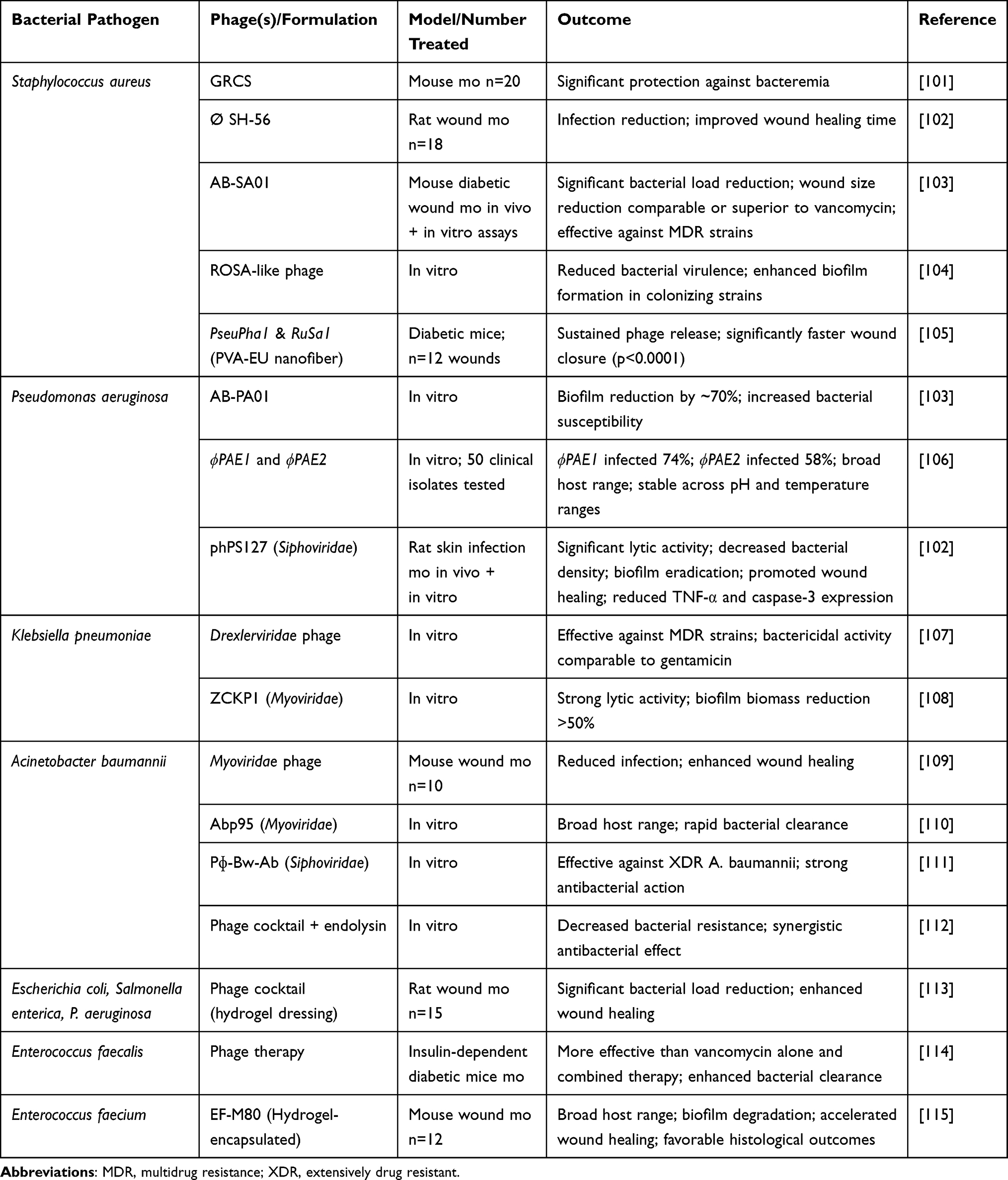 |
Table 1 Phage Therapy and Their Therapeutic Outcomes Against Bacterial Pathogens in Diabetic Foot Infections (DFIs) |
Advances in Preclinical and Animal Studies
Preclinical investigations have consistently demonstrated the therapeutic potential of phage therapy in DFIs. For instance, Sunagar et al evaluated the efficacy of phage GRCS in diabetic and non-diabetic mice with S. aureus bacteremia. A single phage administration achieved survival rates of 90% in diabetic mice and 100% in non-diabetic mice, compared to 0% in untreated controls, alongside substantial reductions in bacterial load.101
In a diabetic rat excision wound model, Kumar et al tested the broad-host-range phage Ø SH-56 against MRSA. Phage treatment significantly decreased infection levels, shortened the period of epithelization, and improved wound contraction compared to Clindamycin-treated and control groups.102 While Sunagar et al reported nearly complete survival, Kumar et al demonstrated substantial but comparatively lower reductions in bacterial burden, highlighting variability in efficacy across phages, bacterial strains, and animal models.
Further innovative delivery systems have been explored to enhance phage therapy outcomes. Suchithra et al incorporated two phages, PseuPha1 and RuSa1, targeting P. aeruginosa and S. aureus, into a polyvinyl alcohol–eudragit (PVA-EU†) nanofiber matrix. This formulation enabled sustained antibacterial release, effectively reduced bacterial abundance, and promoted rapid wound closure in diabetic mice.105 Similarly, Shiue et al developed a 3D-printed porous hydrogel dressing containing a cocktail of phages against Salmonella enterica, E. coli, and P. aeruginosa. Application of this dressing in diabetic mice led to significant bacterial reduction (37–79%) and improved wound healing ratios after 14 days compared to controls.113
Phage therapy has also shown promise against MDR K. pneumoniae. Kelishomi et al identified a lytic phage from the Drexlerviridae family that effectively cleared infections in mice, exhibiting comparable efficacy to gentamicin, with treated mice maintaining better overall health.107 Additionally, Taha et al characterized ZCKP1, a Myoviridae phage with a 150.9 kb dsDNA genome, which showed significant in vitro and in vivo bactericidal activity, reducing bacterial counts and biofilm biomass by over 50%.108
For A. baumannii, Shivaswamy et al investigated the therapeutic efficacy of a Myoviridae phage isolated from hospital sewage. Using an uncontrolled diabetic rat wound infection model, they compared five groups: non-infected controls, infected untreated rats, infected rats treated with the phage, infected rats treated with colistin, and non-infected rats treated with phage alone. Phage treatment led to a significant reduction in bacterial infection, faster wound epithelization, and improved wound contraction compared to both the antibiotic-treated and control groups.109 Huang et al similarly described Abp95, a broad-host-range Myoviridae phage that facilitated rapid wound recovery in diabetic mouse models.110 Additionally, Torabi et al evaluated the Siphoviridae phage Pɸ-Bw-Ab against extensively drug-resistant A. baumannii, demonstrating potent antibacterial activity under optimal temperature and pH conditions.111 While preclinical studies provide strong evidence for phage efficacy, they cannot fully replicate human immune responses, comorbidities, or wound microenvironments. Therefore, these findings should be considered indicative rather than definitive.
Clinical Insights into Phage Therapy for DFIs
The translation of phage therapy into clinical practice has shown promising potential for managing DFIs, particularly in the context of rising antibiotic resistance. Young et al reported a prospective case series involving ten patients with chronic DFIs treated with a personalized anti-staphylococcal phage cocktail, resulting in significant clinical improvement or complete resolution in nine out of ten cases, underscoring the feasibility of compassionate phage use for persistent infections.116 Similarly, Mendes et al conducted a clinical study evaluating topically applied phage cocktails for treating S. aureus and P. aeruginosa infections in diabetic patients. The treatment yielded notable reductions in bacterial counts and visible wound healing improvements, indicating that phage therapy, when combined with standard debridement, could be an effective adjunct in chronic wound care.117
Beyond these clinical insights, extensive preclinical studies strengthen the translational foundation. For instance, Kifelew et al investigated the efficacy of AB-SA01, a cGMP-grade phage cocktail comprising three Myoviridae phages, which has already undergone two Phase I clinical trials for MDR S. aureus infections. In a diabetic mouse model, AB-SA01 treatment significantly reduced bacterial burden and wound size compared with saline controls, performing comparably or better than vancomycin. Importantly, no adverse events related to phage application were observed, and post-mortem examination revealed no systemic pathology, supporting its safety and clinical readiness for DFUs.103 Likewise, Kamer et al characterized phage phPS127, a Siphoviridae family member, targeting P. aeruginosa, a key opportunistic pathogen in DFIs. Detailed in vitro and in vivo analyses confirmed that phPS127 efficiently reduced bacterial load, disrupted biofilms, lowered pro-inflammatory cytokines (TNF-α), and decreased apoptosis markers (caspase-3), culminating in significant wound healing acceleration in a rat skin infection model.118 Clinical translation requires standardized phage production, rigorous quality control, and compliance with regulatory frameworks. Variability in phage preparations and dosing strategies currently limits broader clinical adoption.
Some evidence also suggests that phages may modulate bacterial pathogenicity. For example, the ROSA-like prophage identified by Messad et al reduced bacterial virulence but enhanced biofilm formation, indicating that phage effects can be complex and context-dependent.104
Focusing on P. aeruginosa, which remains a major concern for antibiotic resistance, Mohamed et al isolated two potent phages, ϕPAE1 and ϕPAE2, from sewage samples. Both phages showed broad host ranges, infecting over half of clinical isolates, and remained active under diverse temperature and pH conditions. Their stability and host specificity, alongside resistance to common organic solvents and prolonged storage resilience, highlight their promise as robust anti-Pseudomonas agents for chronic wounds.106
Phage therapy is also being explored for resistant Gram-positive pathogens beyond S. aureus. Oli et al demonstrated that phage treatment outperformed vancomycin alone in controlling vancomycin-resistant E. faecalis (VREF) infections in an insulin-dependent diabetic mice model. This suggests a potential role for phages as an alternative or supplement to last-line antibiotics in immunocompromised patients.114 Extending this, Khazani Asforooshani et al characterized the E. faecium phage EF-M80, which showed a broad host range, biofilm degradation capacity, and genomic stability. When formulated in a hydrogel, EF-M80 significantly improved wound healing markers, including enhanced collagen deposition, neovascularization, and tissue regeneration, further supporting the promise of advanced delivery platforms for phage therapy.115
Synergistic Effects of Phage Therapy in Combination with Other Compounds
Phage-antibiotic synergy, observed between phages and antibiotics, has generated significant interest due to its potential to enhance bacterial eradication.119,120 Initially, this term described the phenomenon where sublethal concentrations of antibiotics stimulated phage replication, leading to an improved antimicrobial effect. Today, it broadly refers to any scenario where combined use of phages and antibiotics results in synergistic antimicrobial effects.89
Current understanding indicates that this synergy arises through several complementary biological processes. Antibiotics may alter bacterial cell morphology, metabolism, or division rates, thereby increasing phage adsorption, intracellular replication, and burst size.121 Conversely, phage infection can resensitize bacteria to antibiotics by selecting for resistance mutations that impair efflux pumps, membrane integrity, or virulence determinants, creating evolutionary trade-offs that restore antimicrobial susceptibility.122 In addition, phage-mediated lysis disrupts bacterial biofilm architecture and releases extracellular polymeric substances, enhancing antibiotic penetration into previously protected microbial communities.123
This synergy is particularly important in the treatment of DFUs, where antibiotic resistance is common (Table 2). Several studies have highlighted the potential of phage-antibiotic synergy in treating infections. For instance, Liu et al focused on P. aeruginosa infections in DFUs, demonstrating that phage APTC-PA18, when combined with ciprofloxacin, exhibited synergistic effects against both planktonic and biofilm forms of the bacteria.124 Mubeen et al reported that combining phages with antibiotics like meropenem significantly enhanced bacterial killing against P. aeruginosa compared to either treatment alone.125 Mubeen et al reported that combining phages with antibiotics like meropenem significantly enhanced bacterial killing against P. aeruginosa compared to either treatment alone.126 Oliveira et al explored phage therapy in combination with honey against E. coli, showing that combining E. coli-specific phages with honey significantly enhanced biofilm disruption, resulting in severe membrane disruption, collapse of bacterial cells, and prevention of biofilm formation.127
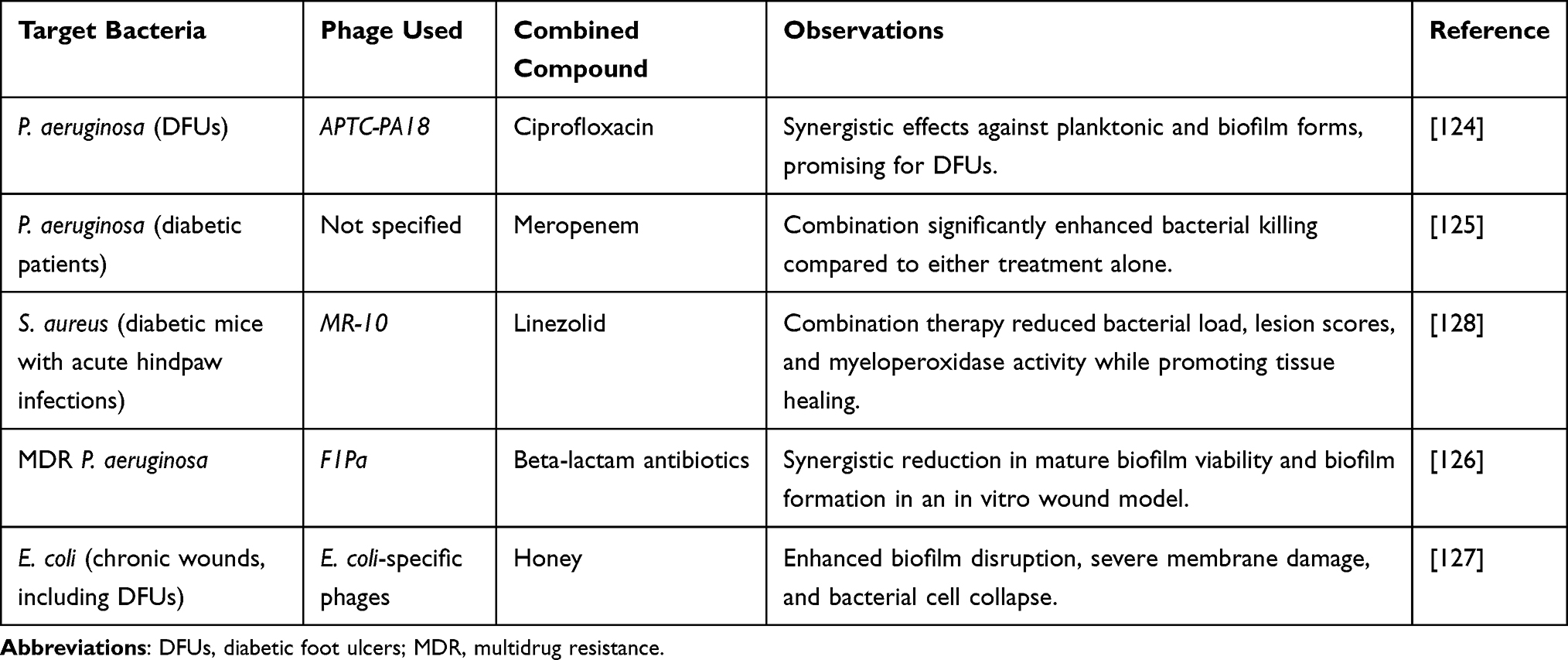 |
Table 2 Synergistic Effects of Phage Therapy in Combination with Other Compounds for Treating Diabetic Infections |
In animal model studies that reflect clinical relevance, Chhibber et al investigated diabetic mice induced with acute hindpaw infections using S. aureus ATCC 43300. The researchers found that a single administration of phage MR-10 was as effective as linezolid alone in resolving the infection. However, combination therapy of MR-10 with linezolid proved significantly more effective in reducing bacterial load, lesion scores, and foot myeloperoxidase activity, as well as in promoting faster tissue healing. Importantly, this combined approach also reduced the likelihood of resistant mutant emergence.128 Although current clinical data on phage-antibiotic synergy in diabetic foot infections remain limited, these findings from animal models provide strong translational potential for combined therapy to overcome resistant bacterial strains, improve treatment outcomes, and reduce the need for high-dose antibiotics that may cause adverse effects.129
Limitations of Phage Therapy
DFUs are often complicated by infections caused by multiple bacterial species.69 One of the primary limitations of phage therapy in this context is the narrow spectrum of bacteriophage activity due to their high specificity, which restricts their effectiveness against diverse bacterial populations commonly found in DFUs.130 Additionally, lysogenic bacteriophages, which can integrate into bacterial genomes, may further complicate treatment by inhibiting other phages’ lytic activities and possibly transferring harmful genes, such as those for antibiotic resistance, to the bacteria involved in the infection.131
An important consideration in translating phage therapy to clinical practice is the mode of administration. Topical application remains the most practical approach for diabetic foot infections, as it delivers high concentrations of phages directly to the wound site with minimal systemic exposure and is easy to integrate into routine wound care. However, a major limitation is that phages can be rapidly cleared from the wound surface due to exudate, and their penetration into deeper infected tissues is limited.132 Recent studies have explored encapsulating phages in hydrogels to address these issues, showing that such formulations can prolong phage residence time, maintain activity, and enhance wound healing outcomes in animal models.133 For deeper infections, such as osteomyelitis, systemic administration may be required, though this approach carries risks of immune neutralisation and rapid clearance from circulation. Alternatively, intralesional or subcutaneous injections could provide higher local tissue concentrations while avoiding systemic exposure.
The lack of standardized policies and regulatory frameworks for phage therapy presents another significant challenge in treating DFUs. Without clear standards for phage isolation, purification, and clinical application, there is considerable variability in the efficacy of phage preparations, which can lead to inconsistent treatment outcomes.134,135 This variability is particularly problematic for managing complex infections like those seen in DFUs.135
An additional major limitation of phage therapy in DFIs is the capacity of bacteria to develop resistance to bacteriophages through multiple molecular and phenotypic mechanisms. These include modification or loss of bacterial surface receptors required for phage adsorption, activation of intracellular defense systems such as restriction–modification and CRISPR–Cas immunity, abortive infection pathways that terminate phage replication, and superinfection exclusion systems encoded by prophages.136–139 Moreover, bacteria residing within biofilms, which are common in chronic diabetic wounds, can exhibit increased tolerance to phages due to reduced metabolic activity, physical shielding by extracellular polymeric substances, and spatial heterogeneity, thereby limiting phage penetration and efficacy.140 Phase variation and phenotypic heterogeneity further contribute to transient phage insensitivity, enabling bacterial persistence under therapeutic pressure and increasing the risk of treatment failure or relapse.141 Additionally, the pharmacokinetic properties of phages, including their absorption, distribution, metabolism, and excretion, are not well understood, making it difficult to determine the appropriate dosages and administration methods for effective treatment.142,143 This challenge is compounded by the body’s ability to degrade phages, which makes it difficult to maintain therapeutic concentrations at the infection site.144,145
Finally, interactions between bacteriophages and the human body during treatment can have adverse effects, such as the release of bacterial toxins during lysis, which may exacerbate infections or lead to septic conditions in DFUs patients.146,147 There is also a risk of immune reactions to phage proteins, although such occurrences are generally rare.148 Despite the potential benefits of phage therapy, the lack of data from double-blind randomized controlled trials limits its current application in treating DFIs.149
Conclusion
The escalating prevalence of DFIs and the global rise in antimicrobial resistance underscore the urgent need for innovative and effective therapeutic strategies. Phage therapy, owing to its host specificity, ability to penetrate and disrupt biofilms, and activity against MDR pathogens, represents a promising adjunct or alternative to conventional antibiotic treatment. The studies reviewed in this article highlight encouraging in vitro, animal, and early clinical evidence supporting the efficacy of phages alone or in combination with antibiotics in targeting key DFI pathogens. However, despite these promising findings, the translation of phage therapy into routine clinical practice has been hindered by a limited number of large-scale randomized controlled trials (RCTs). Several factors appear to underlie this stagnation, including regulatory uncertainty regarding phage classification and approval pathways, difficulties in standardizing phage production under good manufacturing practice conditions, and the personalized nature of phage therapy that requires rapid pathogen phage matching, which is difficult to accommodate within conventional trial designs. Additional obstacles include restricted commercial incentives, intellectual property constraints, incomplete understanding of phage pharmacokinetics and host immune responses, and concerns regarding the emergence of phage-resistant bacterial variants during treatment. The polymicrobial character of many DFIs, challenges in recruiting patients with microbiologically confirmed infections, and ethical concerns related to placebo-controlled designs in limb-threatening disease further complicate the execution of rigorous RCTs, helping to explain why current clinical evidence is largely derived from compassionate-use cases, small observational cohorts, and early-phase studies rather than definitive trials. Future research efforts should therefore prioritize the development of adaptive and pragmatic clinical trial designs tailored to personalized antimicrobial strategies, alongside harmonized regulatory frameworks and standardized manufacturing pipelines. Optimization of phage selection, dosing strategies, formulation technologies, and delivery platforms remains essential to ensure reproducible and clinically meaningful outcomes. In addition, although phage bioengineering has demonstrated potential in enhancing bactericidal activity, broadening host range, and mitigating resistance in other infectious contexts, its application in DFIs remains largely unexplored and warrants focused investigation. Clinically, phage therapy may be considered in patients with DFIs who present with chronic, non-healing wounds, infections caused by multidrug-resistant pathogens, or infections complicated by biofilm formation, particularly when conventional antibiotic therapy has failed. Early integration of phages into the treatment plan may enhance bacterial clearance, reduce the risk of amputation, and improve wound healing outcomes. As the global health community continues to confront the mounting burden of antibiotic resistance, the thoughtful integration of phage therapy, potentially including engineered phages, into multidisciplinary DFI management strategies may ultimately represent a significant advance in limb salvage, infection control, and patient outcomes.
Acknowledgments
The authors would like to acknowledge the Vice-Chancellor of Hamadan University of Medical Sciences for the support of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests.
References
1. Arokiasamy P, Salvi S, Selvamani Y. Global burden of diabetes mellitus. In: Handbook of Global Health. Springer; 2021:1–16.
2. Grover A, Sharma K, Gautam S, Gautam S, Gulati M, Singh SK. Diabetes and its complications: therapies available, anticipated and aspired. Current Diabetes Rev. 2021;17(4):397–420. doi:10.2174/1573399816666201103144231
3. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):1–11. doi:10.1038/s41598-019-56847-4
4. Liu W, Song L, Sun W, Fang W, Wang C. Distribution of microbes and antimicrobial susceptibility in patients with diabetic foot infections in South China. Front Endocrinol. 2023;14:1113622. doi:10.3389/fendo.2023.1113622
5. Dörr S, Freier F, Schlecht M, Lobmann R. Bacterial diversity and inflammatory response at first-time visit in younger and older individuals with diabetic foot infection (DFI). Acta Diabetologica. 2021;58:181–189. doi:10.1007/s00592-020-01587-5
6. Jais S. Various types of wounds that diabetic patients can develop: a narrative review. Clin Pathol. 2023;16:2632010x231205366. doi:10.1177/2632010x231205366
7. Wang Q, Liu C, An J, Liu J, Wang Y, Cai Y. Mechanisms of microbial infection and wound healing in diabetic foot ulcer: pathogenicity in the inflammatory-proliferative phase, chronicity, and treatment strategies. Front Endocrinol. 2025;16(1657928). doi:10.3389/fendo.2025.1657928
8. Cortes-Penfield NW, Armstrong DG, Brennan MB, et al. Evaluation and management of diabetes-related foot infections. Clinl Infect Dis. 2023;77(3):e1–e13. doi:10.1093/cid/ciad255
9. Aicale R, Cipollaro L, Esposito S, Maffulli N. An evidence based narrative review on treatment of diabetic foot osteomyelitis. Surgeon. 2020;18(5):311–320. doi:10.1016/j.surge.2020.01.007
10. Lázaro Martínez JL, García Álvarez Y, Tardáguila-García A, García Morales E. Optimal management of diabetic foot osteomyelitis: challenges and solutions. Diab Metabol Syndr Obesit. 2019;Volume 12:947–959. doi:10.2147/DMSO.S181198
11. Baig MS, Banu A, Zehravi M, et al. An overview of diabetic foot ulcers and associated problems with special emphasis on treatments with antimicrobials. Life. 2022;12(7):1054. doi:10.3390/life12071054
12. Alikhani MS, Nazari M, Hatamkhani S. Enhancing antibiotic therapy through comprehensive pharmacokinetic/pharmacodynamic principles. Front Cell Infect Microbiol. 2025;15:1521091. doi:10.3389/fcimb.2025.1521091
13. Roșca AC, Baciu CC, Burtăverde V, Mateizer A. Psychological consequences in patients with amputation of a limb. An interpretative-phenomenological analysis. Front Psychology. 2021;12:537493. doi:10.3389/fpsyg.2021.537493
14. Nazari M, Shokoohizadeh L, Taheri M. Natural products in the treatment of diabetic foot infection. Eur J Med Res. 2025;30(1):1–17. doi:10.1186/s40001-024-02255-y
15. Yang S, Hu L, Zhao Y, Meng G, Xu S, Han R. Prevalence of multidrug-resistant bacterial infections in diabetic foot ulcers: a meta-analysis. Int Wound J. 2024;21(4):e14864. doi:10.1111/iwj.14864
16. Chanishvili N. Phage therapy—history from Twort and d’Herelle through Soviet experience to current approaches. Advanc Virus Res. 2012;83:3–40.
17. Międzybrodzki R, Hoyle N, Zhvaniya F, et al. Current updates from the long-standing phage research centers in Georgia, Poland, and Russia. Bacteriophages. 2021;921–951.
18. Nikolic N, Anagnostidis V, Tiwari A, Chait R, Gielen F. Droplet-based methodology for investigating bacterial population dynamics in response to phage exposure. Front Microbiol. 2023;14:1260196. doi:10.3389/fmicb.2023.1260196
19. Uyttebroek S, Chen B, Onsea J, et al. Safety and efficacy of phage therapy in difficult-to-treat infections: a systematic review. Lancet Infect Dis. 2022;22(8):e208–e20. doi:10.1016/S1473-3099(21)00612-5
20. Clarke AL, De Soir S, Jones JD. The safety and efficacy of phage therapy for bone and joint infections: a systematic review. Antibiotics. 2020;9(11):795. doi:10.3390/antibiotics9110795
21. Tkhilaishvili T, Lombardi L, Klatt A-B, Trampuz A, Di Luca M. Bacteriophage Sb-1 enhances antibiotic activity against biofilm, degrades exopolysaccharide matrix and targets persisters of Staphylococcus aureus. Int J Antimicrob Agents. 2018;52(6):842–853. doi:10.1016/j.ijantimicag.2018.09.006
22. Nazari M, Taheri M, Nouri F, Bahmanzadeh M, Alikhani MY. Time-kill curve analysis of fucoidan combination with conventional antibiotics against biofilms formation of methicillin-resistant Staphylococcus aureus and Acinetobacter baumannii clinical isolates. Chemotherapy. 2024;70:1–18.
23. Pouget C, Dunyach-Remy C, Pantel A, Schuldiner S, Sotto A, Lavigne J-P. Biofilms in diabetic foot ulcers: significance and clinical relevance. Microorganisms. 2020;8(10):1580. doi:10.3390/microorganisms8101580
24. Yang L, Rong GC, Wu QN. Diabetic foot ulcer: challenges and future. World J Diabetes. 2022;13(12):1014–1034. doi:10.4239/wjd.v13.i12.1014
25. Rajha H, Alsheikh R, Zar A, Mohsen S, Zughaier SM. Microbiology and Antimicrobial resistance in diabetic foot infections. 2024.
26. Abdulwaha DA, Mansour RA. The microbiological landscape of diabetic foot infections: implications for treatment and prevention. Int J Med Sci Dental Health. 2024;10(02):65–85. doi:10.55640/ijmsdh-10-02-12
27. Tigabu A, Getaneh A. Staphylococcus aureus, ESKAPE bacteria challenging current health care and community settings: a literature review. Clin Lab. 2021;67. doi:10.7754/Clin.Lab.2020.200930
28. Von Eiff C, Becker K, Machka K, Stammer H, Peters G. Nasal carriage as a source of Staphylococcus aureus bacteremia. N Engl J Med. 2001;344(1):11–16. doi:10.1056/NEJM200101043440102
29. Wertheim HF, Vos MC, Ott A, et al. Risk and outcome of nosocomial Staphylococcus aureus bacteraemia in nasal carriers versus non-carriers. Lancet. 2004;364(9435):703–705. doi:10.1016/S0140-6736(04)16897-9
30. Shettigar K, Murali TS. Virulence factors and clonal diversity of Staphylococcus aureus in colonization and wound infection with emphasis on diabetic foot infection. Eur J Clin Microbiol Infect Dis. 2020;39(12):2235–2246. doi:10.1007/s10096-020-03984-8
31. Post V, Pascoe B, Mourkas E, et al. Multiple hypervirulent methicillin-sensitive Staphylococcus aureus lineages contribute towards poor patient outcomes in orthopedic device-related infections. medRxiv. 2022;2022.
32. Li M, Diep BA, Villaruz AE, et al. Evolution of virulence in epidemic community-associated methicillin-resistant Staphylococcus aureus. Proc Natl Acad Sci. 2009;106(14):5883–5888. doi:10.1073/pnas.0900743106
33. Nazari M, Taheri M, Nouri F, Bahmanzadeh M, Alikhani MY. The antimicrobial and antibiofilm effects of gentamicin, imipenem, and fucoidan combinations against dual-species biofilms of Staphylococcus aureus and Acinetobacter baumannii isolated from diabetic foot ulcers. Ann Clinic Microbiol Antimicrob. 2024;23(1):101. doi:10.1186/s12941-024-00760-w
34. Stacey HJ, Clements CS, Welburn SC, Jones JD. The prevalence of methicillin-resistant Staphylococcus aureus among diabetic patients: a meta-analysis. Acta Diabetologica. 2019;56(8):907–921. doi:10.1007/s00592-019-01301-0
35. Zhou S, Hu X, Wang Y, Fei W, Sheng Y, Que H. The global prevalence of methicillin-resistant Staphylococcus aureus in patients with diabetic foot ulcers: a systematic review and meta-analysis. Diabet Metabol Syndr Obesit. 2024;17:563–574. doi:10.2147/DMSO.S446911
36. Sreejisha M, Mulki SS, Shenoy S, Dhanashree B, Chakrapani M, Bhat G. Heterogeneous vancomycin intermediate Staphylococcus aureus infections in diabetic and non-diabetic patients–A hospital-based comparative study. Infect Drug Resist. 2023;16:9. doi:10.2147/IDR.S393415
37. Tosh PK, Agolory S, Strong BL, et al. Prevalence and risk factors associated with vancomycin-resistant Staphylococcus aureus precursor organism colonization among patients with chronic lower-extremity wounds in Southeastern Michigan. Infect Control Hosp Epidemiol. 2013;34(9):954–960. doi:10.1086/671735
38. Neves JM, Duarte B, Pinto M, Formiga A, Neves J. Diabetic foot infection: causative pathogens and empiric antibiotherapy considerations—the experience of a tertiary center. Int J Lower Extrem Wound. 2019;18(2):122–128. doi:10.1177/1534734619839815
39. Abbas ZG. Managing the diabetic foot in resource-poor settings: challenges and solutions. Chronic Wound Care Manage Res. 2017;4:135–142. doi:10.2147/CWCMR.S98762
40. Qi C, Luo X, Huang J, et al. Prevalence of S. aureus and/or MRSA in hospitalized patients with diabetic foot and establishment of LAMP methods for rapid detection of the SCCmec gene. BMC Microbiol. 2024;24(1):36. doi:10.1186/s12866-024-03196-6
41. Saltoglu N, Surme S, Ezirmik E, et al. The effects of antimicrobial resistance and the compatibility of initial antibiotic treatment on clinical outcomes in patients with diabetic foot infection. Int J Low Extrem Wounds. 2023;22(2):283–290. doi:10.1177/15347346211004141
42. Gramberg M, Mahadew SKN, Lissenberg-Witte BI, et al. The association between bacteria and outcome and the influence of sampling method, in people with a diabetic foot infection. Infection. 2023;51(2):347–354. doi:10.1007/s15010-022-01884-x
43. Galkowska H, Podbielska A, Olszewski WL, et al. Epidemiology and prevalence of methicillin-resistant Staphylococcus aureus and Staphylococcus epidermidis in patients with diabetic foot ulcers: focus on the differences between species isolated from individuals with ischemic vs. neuropathic foot ulcers. Diabetes Res Clin Pract. 2009;84(2):187–193. doi:10.1016/j.diabres.2009.02.008
44. Srivastava P, Sivashanmugam K. Combinatorial drug therapy for controlling Pseudomonas aeruginosa and its association with chronic condition of diabetic foot ulcer. Int J Lower Extrem Wound. 2020;19(1):7–20. doi:10.1177/1534734619873785
45. Garousi M, MonazamiTabar S, Mirazi H, Farrokhi Z, Khaledi A, Shakerimoghaddam A. Epidemiology of Pseudomonas aeruginosa in diabetic foot infections: a global systematic review and meta-analysis. Germs. 2023;13(4):362. doi:10.18683/germs.2023.1406
46. Makeri D, Odoki M, Eilu E, Agwu E. Update on prevalence and antimicrobial resistance of Staphylococcus aureus and Pseudomonas aeruginosa isolated from diabetic foot ulcers in Africa: a systematic review and meta-analysis. Bull Natl Res Cent. 2023;47(1):145. doi:10.1186/s42269-023-01119-5
47. Afonso AC, Oliveira D, Saavedra MJ, Borges A, Simões M. Biofilms in diabetic foot ulcers: impact, risk factors and control strategies. Int J Mol Sci. 2021;22(15):8278. doi:10.3390/ijms22158278
48. Veve MP, Mercuro NJ, Sangiovanni RJ, Santarossa M, Patel N. Prevalence and predictors of Pseudomonas aeruginosa among hospitalized patients with diabetic foot infections. In: Open Forum Infectious Diseases. Vol. 9. Oxford University Press; 2022:ofac297.
49. Jurado-Martín I, Sainz-Mejías M, McClean S. Pseudomonas aeruginosa: an audacious pathogen with an adaptable arsenal of virulence factors. Int J Mol Sci. 2021;22(6):3128. doi:10.3390/ijms22063128
50. Sannathimmappa MB, Nambiar V, Aravindakshan R, et al. Diabetic foot infections: profile and antibiotic susceptibility patterns of bacterial isolates in a tertiary care hospital of Oman. J Educ Health Promot. 2021;10:10. doi:10.4103/jehp.jehp_225_20
51. Opoku-Temeng C, Malachowa N, Kobayashi SD, DeLeo FR. Innate host defense against Klebsiella pneumoniae and the outlook for development of immunotherapies. J Innate Immun. 2022;14(3):167–181. doi:10.1159/000518679
52. Khanam A, Hithamani G, Naveen J, Pradeep SR, Barman S, Srinivasan K. Management of invasive infections in diabetes mellitus: a comprehensive review. Biologics. 2023;3(1):40–71. doi:10.3390/biologics3010004
53. Sultana R, Ahmed I, Saima S, Salam MT, Sultana S. Diabetic foot ulcer-a systematic review on relevant microbial etiology and antibiotic resistance in Asian countries. Diabetes Metab Syndr. 2023;17(6):102783. doi:10.1016/j.dsx.2023.102783
54. Reddy S, Singh CD, Kumar S, Muthusamy R. Prevalence and antibiotic resistance of Klebsiella pneumoniae in diabetic foot ulcer. Cureus. 2024;16(8):e67824. doi:10.7759/cureus.67824
55. Fatima H, Goel N, Sinha R, Khare SK. Recent strategies for inhibiting multidrug-resistant and β-lactamase producing bacteria: a review. Colloids Surf B. 2021;205:111901. doi:10.1016/j.colsurfb.2021.111901
56. Hawkins BK, Barnard M, Barber KE, et al. Diabetic foot infections: a microbiologic review. Foot. 2022;51:101877. doi:10.1016/j.foot.2021.101877
57. Ajigbewu OH, Adeyemi FM, Wahab AA, Oyedara OO, Yusuf-Omoloye NA, Ajigbewu FA. Occurrence of extremely drug-resistant Klebsiella and multidrug-resistant Enterobacter species in chronic wound patients. Microb Infect Dis. 2025;6(1):342–354.
58. Hassan MA, Abd El-Aziz S, Elbadry HM, Samy A, Tamer TM. Prevalence, antimicrobial resistance profile, and characterization of multi-drug resistant bacteria from various infected wounds in North Egypt. Saudi J Biol Sci. 2022;29(4):2978–2988. doi:10.1016/j.sjbs.2022.01.015
59. Riwu KHP, Effendi MH, Rantam FA, Khairullah AR, Widodo A. A review: virulence factors of Klebsiella pneumonia as emerging infection on the food chain. Vet World. 2022;15(9):2172–2179. doi:10.14202/vetworld.2022.2172-2179
60. Hanoon E, Alammar M, Sobhanimonfared F. Molecular detection of some virulence factors of hypervirulent Klebsiella pneumonia that associated with pathogenicity. Magaz Al-Kufa Univer Biol. 2023;15(2).
61. Nazari M, Azizi O, Solgi H, Fereshteh S, Shokouhi S, Badmasti F. Emergence of carbapenem resistant Acinetobacter baumannii clonal complexes CC2 and CC10 among fecal carriages in an educational hospital. Int J Environ Health Res. 2022;32(7):1478–1488. doi:10.1080/09603123.2021.1892036
62. Nazari M, Youzbashi Z, Khaledi M, Fathi J, Afkhami H. Detection of carbapenem resistance and virulence genes among Acinetobacter baumannii isolated from hospital environments in center of Iran. J Curr Biomed Rep. 2021;2(1):14. doi:10.52547/JCBioR.2.1.14
63. Cardoso NA, Cisneiros LDL, Machado CJ, Cenedezi JM, Procópio RJ, Navarro TP. Bacterial genus is a risk factor for major amputation in patients with diabetic foot. Revista do Colégio Brasileiro de Cirurgiões. 2017;44(02):147–153. doi:10.1590/0100-69912017002007
64. Mottola C. Virulence characterization and antimicrobial resistance of major bacterial genera from diabetic foot infections. In: Universidade de. Lisboa (Portugal); 2017.
65. Moretta A, Scieuzo C, Petrone AM, et al. Antimicrobial peptides: a new hope in biomedical and pharmaceutical fields. Front Cell Infect Microbiol. 2021;11:668632. doi:10.3389/fcimb.2021.668632
66. Ibrahim S, Al-Saryi N, Al-Kadmy IM, Aziz SN. Multidrug-resistant Acinetobacter baumannii as an emerging concern in hospitals. Mol Biol Rep. 2021;48(10):6987–6998. doi:10.1007/s11033-021-06690-6
67. Pagano M, Martins AF, Barth AL. Mobile genetic elements related to carbapenem resistance in Acinetobacter baumannii. Braz J Microbiol. 2016;47:785–792. doi:10.1016/j.bjm.2016.06.005
68. Pouget C, Dunyach-Remy C, Pantel A, et al. Alternative approaches for the management of diabetic foot ulcers. Front Microbiol. 2021;12:747618. doi:10.3389/fmicb.2021.747618
69. Sadeghpour Heravi F, Zakrzewski M, Vickery K, Armstrong D, Hu H. Bacterial diversity of diabetic foot ulcers: current status and future prospectives. J Clin Med. 2019;8(11):1935. doi:10.3390/jcm8111935
70. Ebrahimi MT, Nazari M, Mobarezpour N, Afkhami H, Fereshteh S. Analysis of β-lactams and carbapenem heteroresistance in extra-intestinal pathogenic Escherichia coli from blood samples in Iran. J Med Microbiol Infect Dis. 2021;9(3):170–177. doi:10.52547/JoMMID.9.3.170
71. Idrees M, Khan I, Ullah A, et al. Bacterial spectrum from diabetic foot ulcers: a study of antibiotic resistance patterns and phylogenetic diversity. J King Saud Univ Sci. 2024;36(8):103320. doi:10.1016/j.jksus.2024.103320
72. Jain SK, Barman R. Bacteriological profile of diabetic foot ulcer with special reference to drug-resistant strains in a tertiary care center in North-East India. Indian J Endocrinol Metab. 2017;21(5):688–694. doi:10.4103/ijem.IJEM_546_16
73. Husain M, Agrawal YO. Antimicrobial remedies and emerging strategies for the treatment of diabetic foot ulcers. Current Diabetes Rev. 2023;19(5):5–17.
74. Thanganadar Appapalam S, Muniyan A, Vasanthi Mohan K, Panchamoorthy R. A study on isolation, characterization, and exploration of multiantibiotic-resistant bacteria in the wound site of diabetic foot ulcer patients. Int J Lower Extrem Wound. 2021;20(1):6–14. doi:10.1177/1534734619884430
75. Husna A, Rahman MM, Badruzzaman ATM, et al. Extended-Spectrum β-Lactamases (ESBL): challenges and opportunities. Biomedicines. 2023;11(11):2937. doi:10.3390/biomedicines11112937
76. Zambelli R, Santos AF, Moreira LR, et al. Bacterial profile and antimicrobial resistance in diabetic foot ulcer infections: a 10-year retrospective cohort study. Braz J Infect Dis. 2025;29(5):104570. doi:10.1016/j.bjid.2025.104570
77. Tehrany PM, Rahmanian P, Rezaee A, et al. Multifunctional and theranostic hydrogels for wound healing acceleration: an emphasis on diabetic-related chronic wounds. Environ Res. 2023;238(Pt 1):117087. doi:10.1016/j.envres.2023.117087
78. Robineau O, Nguyen S, Senneville E. Optimising the quality and outcomes of treatments for diabetic foot infections. Exp Rev Anti-Infective Ther. 2016;14(9):817–827. doi:10.1080/14787210.2016.1214072
79. Perzon O, Cahn A, Gellman YN, et al. Enterococci in diabetic foot infections: prevalence, clinical characteristics, and outcomes. In: Open Forum Infectious Diseases. Vol. 10. Oxford University Press US; 2023:ofad238.
80. Citron DM, Goldstein EJ, Merriam CV, Lipsky BA, Abramson MA. Bacteriology of moderate-to-severe diabetic foot infections and in vitro activity of antimicrobial agents. J Clin Microbiol. 2007;45(9):2819–2828. doi:10.1128/JCM.00551-07
81. Jneid J, Lavigne J, La Scola B, Cassir N. The diabetic foot microbiota: a review. Human Microbiome J. 2017;5:1–6. doi:10.1016/j.humic.2017.09.002
82. Węgrzyn G. Should bacteriophages be classified as parasites or predators? Polish J Microbiol. 2022;71(1):3–9. doi:10.33073/pjm-2022-005
83. Clokie MR, Millard AD, Letarov AV, Heaphy S. Phages in nature. Bacteriophage. 2011;1(1):31–45. doi:10.4161/bact.1.1.14942
84. Székely AJ, Breitbart M. Single-stranded DNA phages: from early molecular biology tools to recent revolutions in environmental microbiology. FEMS Microbiol Lett. 2016;363(6):fnw027. doi:10.1093/femsle/fnw027
85. Fauquet C, Pringle C. Abbreviations for bacterial and fungal virus species names. Arch Virol. 2000;145(1):197. doi:10.1007/s007050050017
86. Young R. Phage lysis: do we have the hole story yet? Curr Opin Microbiol. 2013;16(6):790–797. doi:10.1016/j.mib.2013.08.008
87. Weinbauer MG. Ecology of prokaryotic viruses. FEMS Microbiol Rev. 2004;28(2):127–181. doi:10.1016/j.femsre.2003.08.001
88. Salmond GP, Fineran PC. A century of the phage: past, present and future. Nat Rev Microbiol. 2015;13(12):777–786. doi:10.1038/nrmicro3564
89. Liu C, Hong Q, Chang RYK, Kwok PCL, Chan H-K. Phage–Antibiotic therapy as a promising strategy to combat multidrug-resistant infections and to enhance antimicrobial efficiency. Antibiotics. 2022;11(5):570. doi:10.3390/antibiotics11050570
90. Domingo-Calap P, Delgado-Martínez J. Bacteriophages: protagonists of a post-antibiotic era. Antibiotics. 2018;7(3):66. doi:10.3390/antibiotics7030066
91. Chibani-Chennoufi S, Sidoti J, Bruttin A, Kutter E, Sarker S, Brüssow H. In vitro and in vivo bacteriolytic activities of Escherichia coli phages: implications for phage therapy. Antimicrob Agents Chemother. 2004;48(7):2558–2569. doi:10.1128/AAC.48.7.2558-2569.2004
92. Sarker SA, McCallin S, Barretto C, et al. Oral T4-like phage cocktail application to healthy adult volunteers from Bangladesh. Virology. 2012;434(2):222–232. doi:10.1016/j.virol.2012.09.002
93. Kakasis A, Panitsa G. Bacteriophage therapy as an alternative treatment for human infections. A comprehensive review. Int J Antimicrob Agents. 2019;53(1):16–21. doi:10.1016/j.ijantimicag.2018.09.004
94. Bogovazova G, Voroshilova N, Bondarenko V. The efficacy of Klebsiella pneumoniae bacteriophage in the therapy of experimental Klebsiella infection. Zhurnal mikrobiologii epidemiologii iimmunobiologii. 1991;(4):5–8.
95. Bogovazova G, Voroshilova N, Bondarenko V, et al. Immunobiological properties and therapeutic effectiveness of preparations from Klebsiella bacteriophages. Zhurnal mikrobiologii epidemiologii i immunobiologii. 1992;(3):30–33.
96. Pouillot F, Chomton M, Blois H, et al. Efficacy of bacteriophage therapy in experimental sepsis and meningitis caused by a clone O25b: H4-ST131 Escherichia coli strain producing CTX-M-15. Antimicrob Agents Chemother. 2012;56(7):3568–3575. doi:10.1128/AAC.06330-11
97. Eghbalpoor F, Gorji M, Alavigeh MZ, Moghadam MT. Genetically engineered phages and engineered phage-derived enzymes to destroy biofilms of antibiotics resistance bacteria. Heliyon. 2024;10(15):e35666. doi:10.1016/j.heliyon.2024.e35666
98. Lu TK, Collins JJ. Dispersing biofilms with engineered enzymatic bacteriophage. Proc Natl Acad Sci. 2007;104(27):11197–11202. doi:10.1073/pnas.0704624104
99. Edgar R, Friedman N, Molshanski-Mor S, Qimron U. Reversing bacterial resistance to antibiotics by phage-mediated delivery of dominant sensitive genes. Appl. Environ Microbiol. 2012;78(3):744–751. doi:10.1128/AEM.05741-11
100. Weber-Dąbrowska B, Górski A, Weber-Dabrowska B, Górski A. Phage therapy of staphylococcal infections (including MRSA) may be less expensive than antibiotic treatment. Postepy Hig Med Dosw. 2007;61:461–465.
101. Sunagar R, Patil SA, Chandrakanth RK. Bacteriophage therapy for Staphylococcus aureus bacteremia in streptozotocin-induced diabetic mice. Res Microbiol. 2010;161(10):854–860. doi:10.1016/j.resmic.2010.09.011
102. Kumar V, Srinivasa H, Basavarajappa K, Patil U, Bandekar N, Patil R. Abrogation of Staphylococcus aureus wound infection by bacteriophage in diabetic rats. Int J Pharmaceut Sci Drug Res. 2011;202–207. doi:10.25004/IJPSDR.2011.030307
103. Kifelew LG, Warner MS, Morales S, et al. Efficacy of phage cocktail AB-SA01 therapy in diabetic mouse wound infections caused by multidrug-resistant Staphylococcus aureus. BMC Microbiol. 2020;20:1–10. doi:10.1186/s12866-020-01891-8
104. Messad N, Prajsnar TK, Lina G, et al. Existence of a colonizing Staphylococcus aureus strain isolated in diabetic foot ulcers. Diabetes. 2015;64(8):2991–2995. doi:10.2337/db15-0031
105. Suchithra KV, Hameed A, Surya S, Mahammad S, Arun AB. Dual phage-incorporated electrospun polyvinyl alcohol-eudragit nanofiber matrix for rapid healing of diabetic wound infected by Pseudomonas aeruginosa and Staphylococcus aureus. Drug Delivery Transl Res. 2024;15:1–17.
106. Mahdy M, Askora AA, Mahdy MMH, El-Hussieny EA, Abu-Shady HM. Isolation and characterization of bacteriophages active against Pseudomonas aeruginosa strains isolated from diabetic foot infections. Arch Razi Inst. 2022;77(6):2187. doi:10.22092/ARI.2022.359032.2357
107. Kelishomi FZ, Nikkhahi F, Amereh S, et al. Evaluation of the therapeutic effect of a novel bacteriophage in the healing process of infected wounds with Klebsiella pneumoniae in mice. J Global Antimicrob Resist. 2024;36:371–378. doi:10.1016/j.jgar.2024.01.018
108. Taha OA, Connerton PL, Connerton IF, El-Shibiny A. Bacteriophage ZCKP1: a potential treatment for Klebsiella pneumoniae isolated from diabetic foot patients. Front Microbiol. 2018;9:2127. doi:10.3389/fmicb.2018.02127
109. Shivaswamy VC, Kalasuramath SB, Sadanand CK, et al. Ability of bacteriophage in resolving wound infection caused by multidrug-resistant Acinetobacter baumannii in uncontrolled diabetic rats. Microb Drug Resist. 2015;21(2):171–177. doi:10.1089/mdr.2014.0120
110. Huang L, Huang S, Jiang L, et al. Characterisation and sequencing of the novel phage Abp95, which is effective against multi-genotypes of carbapenem-resistant Acinetobacter baumannii. Sci Rep. 2023;13(1):188. doi:10.1038/s41598-022-26696-9
111. Torabi LR, Doudi M, Naghavi NS, Monajemi R. Isolation, characterization, and effectiveness of bacteriophage Pɸ-Bw-Ab against XDR Acinetobacter baumannii isolated from nosocomial burn wound infection. Iran J Basic Med Sci. 2021;24(9):1254. doi:10.22038/ijbms.2021.57772.12850
112. Jasim HN, Hafidh RR, Abdulamir AS. Formation of therapeutic phage cocktail and endolysin to highly multi-drug resistant Acinetobacter baumannii: in vitro and in vivo study. Iran J Basic Med Sci. 2018;21(11):1100. doi:10.22038/IJBMS.2018.27307.6665
113. Shiue SJ, Wu MS, Chiang YH, Lin HY. Bacteriophage‐cocktail hydrogel dressing to prevent multiple bacterial infections and heal diabetic ulcers in mice. J Biomed Mater Res Part A. 2024;112(11):1846–1859. doi:10.1002/jbm.a.37728
114. Oli AK, Shivshetty N, Ahmed L, Chavadi M, Kambar RN, Kelmani Chandrakanth R. Efficacy of bacteriophage therapy against vancomycin-resistant Enterococcus feacalis in induced and non-induced diabetic mice. bioRxiv. 2021.
115. Khazani Asforooshani M, Elikaei A, Abed S, et al. A novel Enterococcus faecium phage EF-M80: unveiling the effects of hydrogel-encapsulated phage on wound infection healing. Front Microbiol. 2024;15:1416971. doi:10.3389/fmicb.2024.1416971
116. Young MJ, Hall LM, Merabishvilli M, Pirnay J-P, Clark JR, Jones JD. Phage therapy for diabetic foot infection: a case series. Clin Ther. 2023;45(8):797–801. doi:10.1016/j.clinthera.2023.06.009
117. Mendes JJ, Leandro C, Mottola C, et al. In vitro design of a novel lytic bacteriophage cocktail with therapeutic potential against organisms causing diabetic foot infections. J Med Microbiol. 2014;63(8):1055–1065. doi:10.1099/jmm.0.071753-0
118. Kamer AMA, Abdelaziz AA, Nosair AM, Al-Madboly LA. Characterization of newly isolated bacteriophage to control multi-drug resistant Pseudomonas aeruginosa colonizing incision wounds in a rat model: in vitro and in vivo approach. Life Sci. 2022;310:121085. doi:10.1016/j.lfs.2022.121085
119. Lin Y, Chang RYK, Britton WJ, Morales S, Kutter E, Chan H-K. Synergy of nebulized phage PEV20 and ciprofloxacin combination against Pseudomonas aeruginosa. Int J Pharm. 2018;551(1–2):158–165. doi:10.1016/j.ijpharm.2018.09.024
120. Lin Y, Quan D, Chang RYK, et al. Synergistic activity of phage PEV20-ciprofloxacin combination powder formulation—A proof-of-principle study in a P. aeruginosa lung infection model. Eur J Pharm Biopharm. 2021;158:166–171. doi:10.1016/j.ejpb.2020.11.019
121. Bulssico J, Panigrahi S, Matveeva M, Ginet N, Ansaldi M. Antibiotic-induced morphological changes enhance phage predation. PLoS Pathog. 2025;21(10):e1013546. doi:10.1371/journal.ppat.1013546
122. Hasan M, Ahn J. Evolutionary dynamics between phages and bacteria as a possible approach for designing effective phage therapies against antibiotic-resistant bacteria. Antibiotics. 2022;11(7). doi:10.3390/antibiotics11070915
123. Topka-Bielecka G, Dydecka A, Necel A, et al. Bacteriophage-derived depolymerases against bacterial biofilm. Antibiotics. 2021;10(2). doi:10.3390/antibiotics10020175
124. Liu S, Goonetilleke S, Hon K, et al. Bacteriophage in combination with ciprofloxacin against Pseudomonas aeruginosa infections in diabetic foot ulcer patients. bioRxiv. 2023;2023.
125. Mubeen S, Ullah K, Kanwal R, et al. Phage-antibiotic synergism against Pseudomonas aeruginosa isolated from diabetic wounds. J Popul Ther Clin Pharmacol. 2024.
126. Santamaría-Corral G, Aguilera-Correa JJ, Esteban J, García-Quintanilla M. Bacteriophage therapy on an in vitro wound model and synergistic effects in combination with beta-lactam antibiotics. Antibiotics. 2024;13(9):800. doi:10.3390/antibiotics13090800
127. Oliveira A, Ribeiro HG, Silva AC, et al. Synergistic antimicrobial interaction between honey and phage against Escherichia coli biofilms. Front Microbiol. 2017;8:2407. doi:10.3389/fmicb.2017.02407
128. Chhibber S, Kaur T, Kaur S. Co-therapy using lytic bacteriophage and linezolid: effective treatment in eliminating methicillin resistant Staphylococcus aureus (MRSA) from diabetic foot infections. PLoS One. 2013;8(2):e56022. doi:10.1371/journal.pone.0056022
129. Lu H, Li Z, Elbaz A, Ni S-Q. Synergistic action of phages and lytic proteins with antibiotics: a combination strategy to target bacteria and biofilms. BMC Microbiol. 2023;23(1):149. doi:10.1186/s12866-023-02881-2
130. Hyman P, Abedon ST. Bacteriophage host range and bacterial resistance. Adv Appl Microbiol. 2010;70:217–248.
131. Carascal MB, Dela Cruz-Papa DM, Remenyi R, Cruz MCB, Destura RV. Phage revolution against multidrug-resistant clinical pathogens in Southeast Asia. Front Microbiol. 2022;13:820572. doi:10.3389/fmicb.2022.820572
132. Pinto AM, Cerqueira MA, Bañobre-Lópes M, Pastrana LM, Sillankorva S. Bacteriophages for chronic wound treatment: from traditional to novel delivery systems. Viruses. 2020;12(2):235. doi:10.3390/v12020235
133. Loh B, Gondil VS, Manohar P, Khan FM, Yang H, Leptihn S. Encapsulation and delivery of therapeutic phages. Appl Environ Microbiol. 2021;87(5):e01979–20. doi:10.1128/AEM.01979-20
134. Fauconnier A. Phage therapy regulation: from night to Dawn. Viruses. 2019;11(4):352. doi:10.3390/v11040352
135. Verbeken G, Pirnay J-P, Lavigne R, et al. Call for a dedicated European legal framework for bacteriophage therapy. Archivum immunologiae et therapiae experimentalis. 2014;62(2):117–129. doi:10.1007/s00005-014-0269-y
136. Atterbury RJ, Dillon E, Swift C, et al. Correlation of Campylobacter bacteriophage with reduced presence of hosts in broiler chicken ceca. Appl Environ Microbiol. 2005;71(8):4885–4887. doi:10.1128/AEM.71.8.4885-4887.2005
137. Hagens S, Loessner MJ. Application of bacteriophages for detection and control of foodborne pathogens. Appl Microbiol Biotechnol. 2007;76(3):513–519. doi:10.1007/s00253-007-1031-8
138. Oot R, Raya RR, Callaway TR, Edrington TS, Kutter EM, Brabban AD. Prevalence of Escherichia coli O157 and O157: H7‐infecting bacteriophages in feedlot cattle feces. Lett Appl Microbiol. 2007;45(4):445–453. doi:10.1111/j.1472-765X.2007.02211.x
139. Callaway TR, Edrington TS, Brabban AD, et al. Bacteriophage isolated from feedlot cattle can reduce Escherichia coli O157: H7 populations in ruminant gastrointestinal tracts. Foodborne Pathogens Dis. 2008;5(2):183–191. doi:10.1089/fpd.2007.0057
140. Zhao A, Sun J, Liu Y. Understanding bacterial biofilms: from definition to treatment strategies. Front Cell Infect Microbiol. 2023;13(1137947). doi:10.3389/fcimb.2023.1137947
141. Raatz M, Shah S, Chitadze G, Brüggemann M, Traulsen A. The impact of phenotypic heterogeneity of tumour cells on treatment and relapse dynamics. PLoS Comput Biol. 2021;17(2):e1008702. doi:10.1371/journal.pcbi.1008702
142. Merril CR. Interaction of Bacteriophages with Animals. Cambridge, UK:Cambridge University Press;2008:332–352
143. Gill J, Pacan J, Carson M, Leslie K, Griffiths M, Sabour P. Efficacy and pharmacokinetics of bacteriophage therapy in treatment of subclinical Staphylococcus aureus mastitis in lactating dairy cattle. Antimicrob Agents Chemother. 2006;50(9):2912–2918. doi:10.1128/AAC.01630-05
144. Huh H, Wong S, Jean JS, Slavcev R. Bacteriophage interactions with mammalian tissue: therapeutic applications. Adv Drug Delivery Rev. 2019;145:4–17. doi:10.1016/j.addr.2019.01.003
145. Zelasko S, Gorski A, Dabrowska K. Delivering phage therapy per os: benefits and barriers. Exp Rev Anti-Infective Ther. 2017;15(2):167–179. doi:10.1080/14787210.2017.1265447
146. Tetz GV, Ruggles KV, Zhou H, Heguy A, Tsirigos A, Tetz V. Bacteriophages as potential new mammalian pathogens. Sci Rep. 2017;7(1):7043. doi:10.1038/s41598-017-07278-6
147. Górski A, Borysowski J, Międzybrodzki R. Beata-Weber-Dąbrowska B-W-D. Bacteriophages Med. 2007.
148. Sulakvelidze A. Phage therapy: an attractive option for dealing with antibiotic-resistant bacterial infections. Drug Discovery Today. 2005;12(10):807–809. doi:10.1016/S1359-6446(05)03441-0
149. Górski A, Borysowski J, Międzybrodzki R. Phage therapy: towards a successful clinical trial. Antibiotics. 2020;9(11):827. doi:10.3390/antibiotics9110827
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.