Back to Archived Journals » Chronic Wound Care Management and Research » Volume 6
Management of chronic wounds in patients with pemphigus
Authors Grada A ![]() , Obagi Z, Phillips T
, Obagi Z, Phillips T
Received 8 May 2019
Accepted for publication 19 July 2019
Published 30 August 2019 Volume 2019:6 Pages 89—98
DOI https://doi.org/10.2147/CWCMR.S141948
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Marco Romanelli
Ayman Grada,1 Zaidal Obagi,2 Tania Phillips1
1Department of Dermatology, Boston University School of Medicine, Boston, MA, USA; 2University of Toledo College of Medicine and Life Sciences, Toledo, OH, USA
Correspondence: Ayman Grada
Department of Dermatology, Boston University School of Medicine, Boston, MA 02118, USA
Tel +1 317 525 5247
Email [email protected]
Abstract: Pemphigus is a group of chronic IgG-mediated autoimmune blistering diseases that involves both the skin and mucous membranes. It is caused by autoantibodies disrupting intercellular keratinocyte adhesion. Loss of epidermal integrity clinically manifests as flaccid thin-walled blisters, erosions, and crusts on the skin, and painful mucosal erosions. Pemphigus vulgaris and pemphigus foliaceus are the two most common types of pemphigus. Although rare, pemphigus can be life-threatening. Substantial morbidity and mortality can occur as a result of complications of these diseases and their treatments. In general, pemphigus often results in extensive skin loss, leading to scar formation and adherence of articular skin folds, limiting joint and limb movements. The primary goal of treatment is to induce durable remission, decrease blister formation, prevent infections and promote healing of blisters and erosions. The mainstay of treatment for pemphigus is systemic corticosteroids combined with an adjuvant immunosuppressant and wound care. We performed PubMed and Google Scholar searches of the English-language literature for pemphigus disease and wound management for blistering disease (1966–2019). In this review, we discuss wound care in patients with pemphigus disease.
Keywords: pemphigus, chronic wounds, blisters, dressing, wound healing, infection
Introduction
Pemphigus is a group of rare yet potentially fatal IgG-mediated blistering autoimmune diseases affecting the skin and mucous membranes.1 The term pemphigus was derived from the Greek word “pemphix” meaning bubble or blister.2 Pemphigus can be grouped into four major types: vulgaris, foliaceus, paraneoplastic, and IgA pemphigus. Pemphigus vulgaris (PV) is the most prevalent of the autoimmune bullous diseases in the pemphigus family. In PV, the blister occurs in the deeper part of the epidermis, just above the basal layer, and in pemphigus foliaceus (PF), also called superficial pemphigus, the blister occurs in the granular layer. PV is characterized by the presence of circulating IgG autoantibodies against desmoglein, a keratinocyte cell surface molecule, leading to disruption of normal cell adhesion between keratinocytes, and hence separation and rounding up of epidermal cells (acantholysis) and intraepidermal clefting leading to blister formation. The target antigens in PV are desmoglein (Dsg) 1 and 3. In the mucocutaneous type, autoantibodies against Dsg1 and Dsg3 are present, whereas the mucosal-dominant type of PV is caused by autoantibodies against Dsg3. PF is characterized by cutaneous involvement only and is caused by autoantibodies directed against Dsg1, leading to subcorneal blisters.3
The incidence rate of PV is estimated to be between 0.1 and 0.5 per 100,000 people per year. Pemphigus is more common in adults but can occur at any age. The average age of onset is 40–60 years for PV and nonendemic PF.4 Overall, the sex ratio for PV and PF appears to be equivalent or close to equivalent.5 It is rare in young people.
Clinical manifestations
The disease has a chronic course. The primary lesion of PV is a flaccid blister, which may occur anywhere on the skin surface, but typically not the palms and soles.6 The skin lesions in PV can be pruritic or painful. Because the blister is forming in the epidermis, it is flaccid and easily ruptured and hence, the most common skin lesions observed in patients are moist erosions resulting from broken blisters.7 These erosions are often quite large, as they tend to spread at their periphery. Large areas of the epidermis can denude, creating risk for bacterial infection and sepsis. Some patients will only have mucosal involvement, usually in the oral cavity.6 In the mouth, short-lived bullae quickly rupture to involve most of the mucosa with slow-healing painful erosions. A characteristic finding in pemphigus patients is that erosions can be extended into visibly normal skin by pulling the remnant of the blister wall or rubbing at the periphery of active lesions; additionally, erosions can be induced in normal-appearing skin distant from active lesions by lateral pressure or mechanical shear force. This phenomenon is known as the Nikolsky sign.1 This sign helps differentiate pemphigus from other blistering diseases of the skin such as pemphigoid; however, similar findings also can be elicited in staphylococcal scalded skin syndrome, Stevens-Johnson syndrome, and toxic epidermal necrolysis. Exposure to ultraviolet radiation may intensify disease activity.8
PF typically presents in a seborrheic distribution. The scalp, face, and trunk are common sites of involvement.9 Lesions usually start on the trunk. The skin lesions typically consist of small, scattered superficial blisters that rapidly evolve into scaly, crusted erosions. Because the blisters are superficial, patients often appear to have impetiginized eczema of the face and upper trunk. Nikolsky sign is often present in active disease. The lesions may remain localized or may coalesce to cover large areas of skin. In its most severe form, PF progresses to involve the entire skin surface as an exfoliative erythroderma.10 The erosions may cause local pain and/or burning sensation.9 Unlike PV, PF very rarely has mucosal lesions. Systemic symptoms are usually absent. Key clinical and laboratory findings in different types of pemphigus are listed in (Table 1).2,3,11
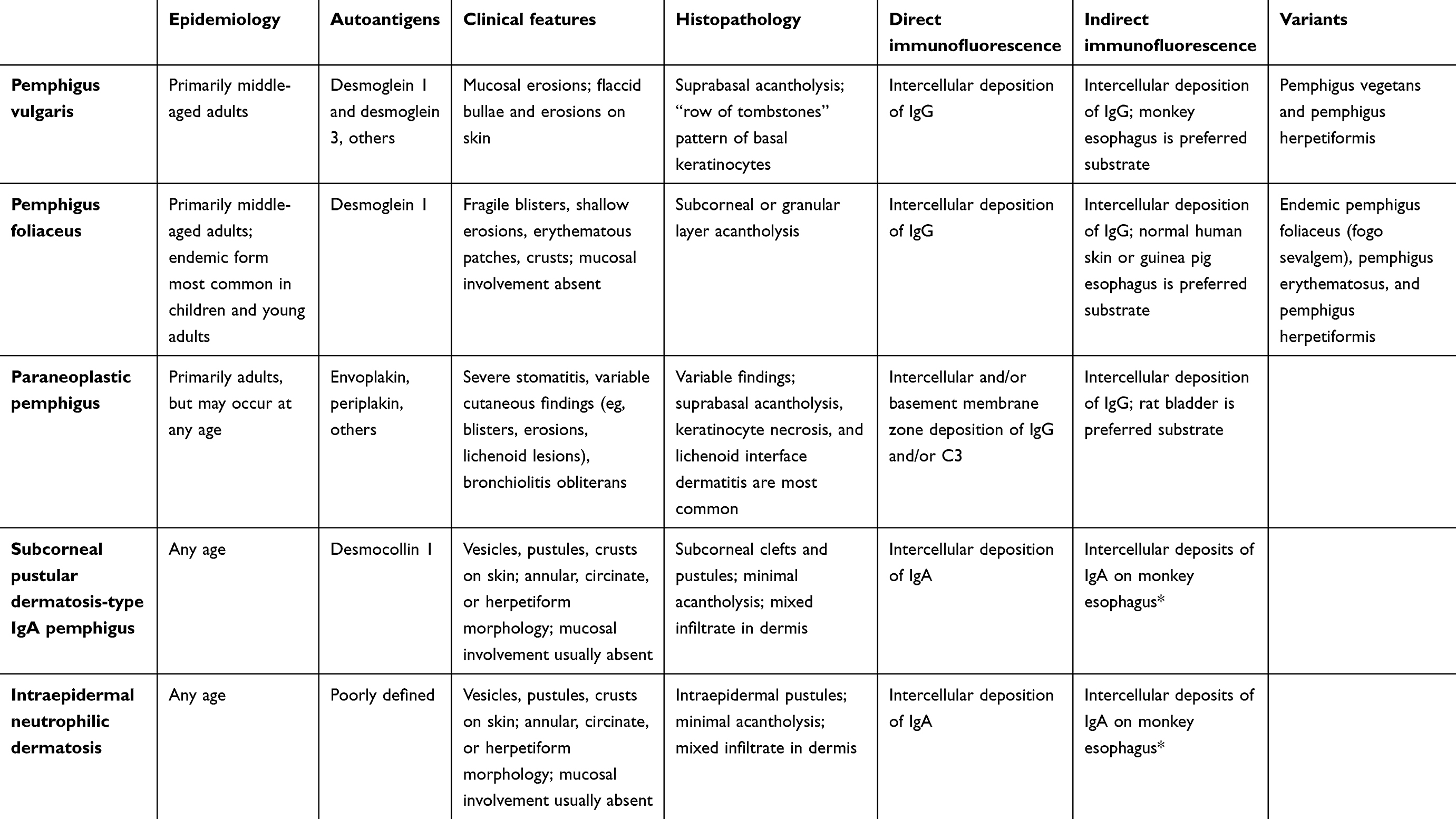 |
Table 1 Key clinical and laboratory findings in pemphigus disease |
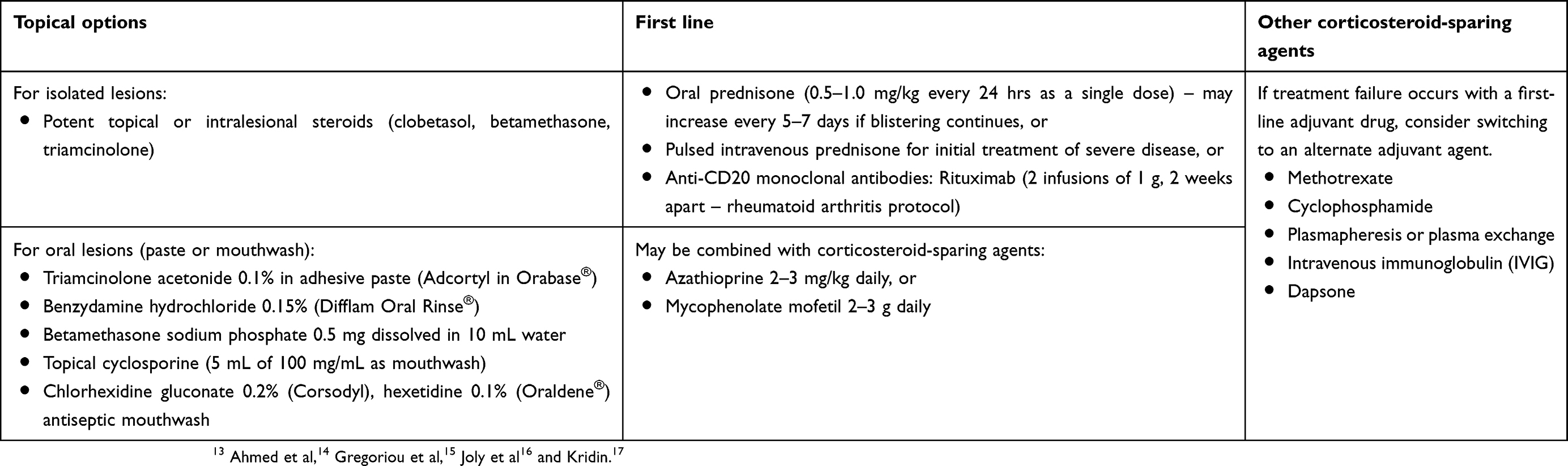 |
Table 2 Pharmacological treatment for pemphigus |
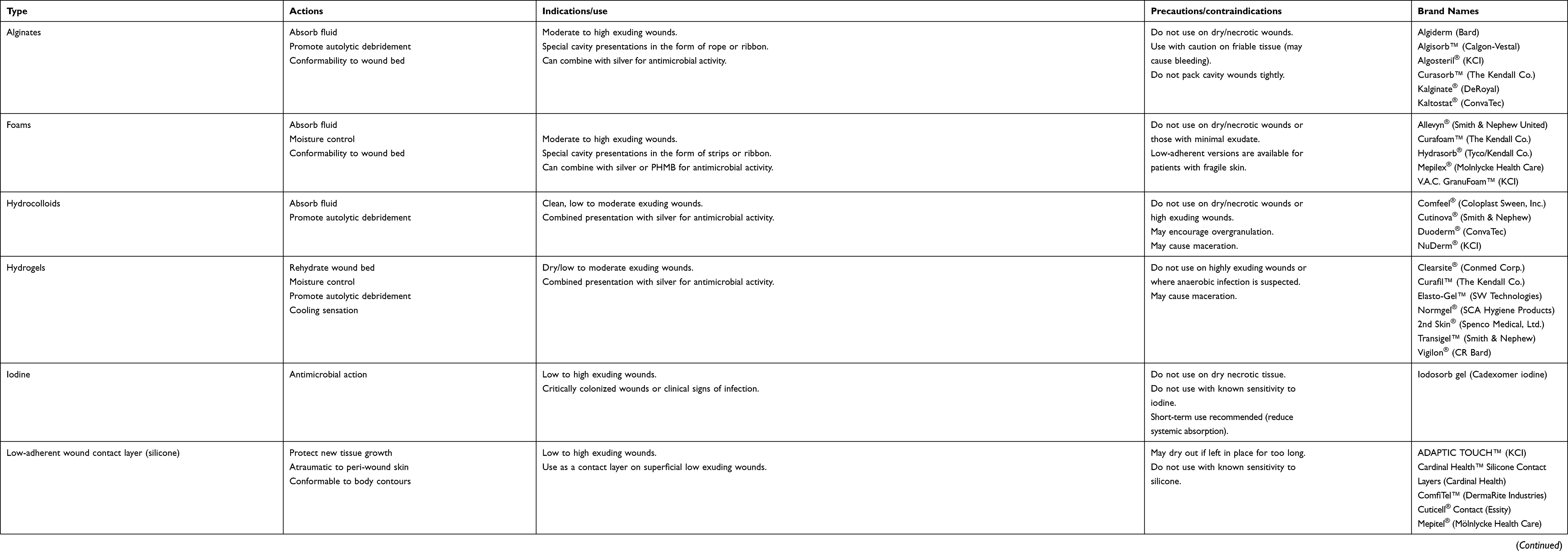 |
Table 3 Properties of dressing materials and topical agents |
Pharmacological treatment
The approach to the treatment of PV and PF is similar. Treatment is aimed at achieving a rapid and sustained remission with the resolution of cutaneous lesions and elimination of circulating antibody, with the eventual goal of maintenance with low-dose therapy, or ideally tapering off all treatment.1 Without treatment, PV does not spontaneously remit. The mortality of PV was 75% on average before the introduction of corticosteroids (CS) in the early 1950.12 The management approach of PV may be considered in 2 general phases: remission induction and remission maintenance. It is important to note that relapse rates can be high initially (up to 47% if treatment is stopped after 1 year). If PV is localized in distribution and mild in severity, therapy with potent topical corticosteroids can be attempted. In moderate to severe cases, systemic corticosteroids with adjuvant immunosuppressants are the primary therapy (Table 2).13–17 Clinical response may be observed within days of starting treatment, although cessation of new blister formation may take a few weeks,18,19 with complete healing occurring at 6–8 weeks.20 Rituximab can also be considered as first-line therapy.16 Patients requiring long-term use of corticosteroids and/or cytotoxic drugs must be monitored carefully for adverse effects. Sun avoidance and sun-protection measures (eg, using sunscreens, wearing barrier clothing) should be recommended. Following successful therapy, cutaneous manifestations of pemphigus tend to resolve in lighter skin phototypes, whereas post-inflammatory pigmentary changes often occur in patients with darker skin phototypes.
Oral mucosal lesions are usually painful during active disease. Patients should maintain oral hygiene (toothbrushing and antiseptic mouthwashes) and avoid spicy, sharp, very hot, or abrasive foods.21 Topical anesthetics such as topical lidocaine 2% gel or solution can be applied to reduce pain.7 Medium or high potency topical corticosteroids have shown to improve oral symptoms of pemphigus in some patients.21,22 In one case report, topical trichloroacetic acid (TCA) 33% seemed promising for the treatment of persistent, old, and refractory oral PV lesions in a patient who is otherwise in clinical remission.23
PV and PF are associated with considerable morbidity and mortality.2 Mortality has considerably decreased to 1.6–12% since the regular use of corticosteroids and adjuvant immunosuppressants was introduced but is approximately 2-3-fold higher in patients with pemphigus than in the general population.2 The most frequently reported causes of death in patients with pemphigus include septicemia, respiratory tract infections, and cardiovascular disease.2,24
Wound management
The four main goals of wound care are (1) prevention of infection, (2) maintenance of a moist environment, (3) protection of the wound, and (4) minimizing scar formation.25 small blisters should be left intact, to prevent secondary infection. However, large blisters should be punctured and aspirated with a large (18-gauge) sterile needle, to keep the blister roof in place for wound protection. Gentle cleansing is an early priority and can be accomplished by normal saline or antibacterial soap/antiseptic twice a day. Allow it to dry well. Next, a bland emollient ointment, such as 50% white soft paraffin +50% liquid paraffin, is applied directly to the wound bed, or apply the ointment to a dressing. If a wound is wet, the dressing should absorb excess exudate. If a wound is dry, the dressing should provide moisture to the wound bed.26
Pemphigus is characterized by superficial wounds, where the damage is generally limited to the epidermis and dressing is comparable to dressing surgical wounds except that extra attention should be paid to early closure and prevention of fluid losses through evaporation. This can be accomplished by using moisture retentive dressings, either occlusive or semiocclusive, help promote reepithelialization and help restore the skin barrier. Non-adherent gauze, transparent film, hydrocolloid, and hydrogel dressings may be used directly on the wounds. When selecting a dressing, one should take into account not only wound characteristics, but also specific dressing features such as absorptive capacity, hydrating quality, adhesive quality, and comfortability. Various types of wound dressing are highlighted in (Table 3).10,27–30 All dressing products used for pemphigus patients must be non-adherent.
Films are thin, elastic dressing made of see-through transparent material (generally composed of polyurethane), available in a wide variety of shapes and sizes to conform to different wounds. They are excellent for erosions and superficial ulcers.28 Films provide a barrier to shield from bacterial invasion.10 They are waterproof but provide one-way exit passage for gas (CO2) and excess moisture. Films are non-absorbant and are only suitable for delicate and minimally exudative, superficial wounds. It is not recommended to use films in high-exudate wounds. To avoid potential tearing or damage to the newly-formed epidermis, films should be non-adherent to the wound area, especially in patients with fragile skin, including the elderly or patients with cutaneous atrophy.10
Hydrogel dressings are made of polyethylene and up to 97% water. They are available in two main forms, sheets (traditional form) and amorphous form. They are useful for dry wounds as they provide a moist environment. Hydrogels also have a marked cooling and soothing effect on the skin, which is valuable in burns and painful wounds. Most hydrogels are nonadhesive, thus requiring a secondary dressing.26 Xeroform gauze or a film can be placed over the hydrogel sheet to stabilize it and to prevent it from drying out.31 Hydrogels should not be used on infected or heavily draining wounds since they are not absorptive.26
Hydrocolloid dressings are available in two forms: sheets and a hydrocolloid gel. Both are composed, for the most part, of carboxymethyl cellulose, gelatin, and pectins. The sheet hydrocolloid dressing has an external semipermeable layer and an internal layer of hydrophilic carboxymethyl cellulose molecules suspended in a hydrophobic mass of gelatin and pectins.10 Hydrocolloid dressings are a cost-effective and convenient option because they can be worn for several days before changing. In addition to having some absorptive properties, they seem particularly useful in causing painless debridement. However, hydrocolloids may cause contact dermatitis. Many hydrocolloids contain adhesives which could damage fragile skin in pemphigus. Hydrocolloid dressings may also produce a malodorous yellow gel on the inner side of the dressing referred to as “gel and smell.” Patients should be informed to expect this as it may be confused with infection.10
Polymeric membrane dressings (PMDs) are multifunctional dressings composed of a hydrophilic polyurethane membrane matrix with a continuous semipermeable polyurethane film backing, which comes in different thicknesses based on wound exudate.10 PMDs have been used successfully in superficial abrasions without overdrying.32,33 PMDs contain ingredients that work synergistically to cleanse wounds and expedite healing continuously.34
When the disease becomes severe with extensive skin involvement, patients are typically admitted to the burn unit. Therefore, supportive care resembles that performed for severe thermal burns TEN. It aims at minimizing potential complications, which may ultimately lead to patient mortality. For instance, it aims to avoid hypovolemia, electrolyte imbalance, renal insufficiency, and sepsis
Approach to infected or colonized lesions
Superimposed infections are often a significant cause of morbidity and mortality in pemphigus, either secondary to the breakdown of the skin barrier or immune suppression related to treatment. Bacterial skin colonization and infection may render pemphigus refractory to treatment by preventing or delaying wound healing.35 The most frequently reported cause of death in pemphigus is septicemia which is usually secondary to cutaneous Staphylococcus aureus infection.36 Prevention of infections is a crucial factor in the overall clinical outcome. An ideal dressing should decrease the microbial burden without causing cytotoxic damage. Patients should be encouraged not to “pop” or drain blisters since this could provide a route for infection. Patients should also be informed about the warning signs of infection to facilitate prompt diagnosis and early treatment.
Infected wounds clinically present with erythema, warmth, edema, and pain or local tenderness. Purulence, increased wound drainage and new or worsening malodor can occur. Systemic signs such as fever and leukocytosis are indicators of progression to bacteremia or septicemia. In such cases, systemic antibiotics are warranted.37
Culture and sensitivity should be considered to determine the most appropriate antibiotic for an infected wound. Superficial swab cultures are of limited utility because wounds, like skin, are covered with transient bacteria rendering the isolation and accurate identification of the pathogenic bacteria impossible. Quantitative swab cultures can help to identify the pathogenic microorganism.10 It is known that a quantitative culture of 1×106 organism/gram of tissue confirms the diagnosis of infection.38
The presence of bacteria in a wound can be grouped into three distinct situations (a) contamination: the presence of bacteria on the surface without multiplication, and the absence of clinical disease. (b) colonization: the bacteria multiply, but without signs and symptoms of infection, and (c) infection: the proliferation of bacteria associated with local host reaction, delayed healing and tissue damage.39,40
In critically colonized wounds, bacteria may delay wound healing without apparent signs of infection. Mild topical antiseptics frequently used to cleanse wounds include Dakins solution (bleach and water), eusol solution (bleach, boric acid, and water), and acetic acid (one tablespoon white vinegar in a cup of water). These solutions cannot be used for a prolonged period of time due to their ability to cause cytotoxicity (each dressing change for no more than 10 min).
Topical antimicrobials are useful when the sensitivity of the organism is determined. Both Mupirocin and retapamulin are effective against gram-positive organisms.41,42 Topical metronidazole provides good anaerobic coverage. These agents can be applied directly to the wound bed with appropriate covering dressings.
Iodine - and silver-based dressings are commonly used as antimicrobial dressings in the management of wounds that are at risk of infection. These dressings have been formulated to be noncytotoxic.10 Cadexomer iodine (eg, Iodosorb) is a slow-release antimicrobial and has shown to be bactericidal against all gram-positive and gram-negative bacteria as well as fungi, and it provides a moist wound environment.43 A recent meta-analysis reported that cadexomer iodine dressings might be associated with better healing compared with standard of care.44
Silver is an antimicrobial agent with broad-spectrum bactericidal activity. Silver-based dressings are available in different forms such as foams, hydrofibers, and hydrocolloids.26 An international consensus on the appropriate use of silver dressings recommends that silver dressings be used for infected wounds or wounds that are at high risk of infection for an initial period of 2-week, after which the wound should be reevaluated to decide if a silver dressing remains appropriate or if a more aggressive intervention is warranted.10,45 It is important to note that silver ions—not silver atoms—produce the antimicrobial effect. Thus, silver dressings require moist wound environments to release their active antimicrobial agent.46,47 Newer silver dressings aim to decrease the cytotoxicity seen in older silver dressings. PMD with silver is one such example. A marked improvement in wound healing and patient comfort were observed in a patient with PV after application of silver-containing hydrofiber dressings (SHD) such as Aquacel-Ag®.48 Acticoat® is another silver biologic dressing containing a 15 nm bactericidal coat of nano-crystallized ions of silver in a cluster structure.49 In one study, Acticoat® shown complete healing in 13 cases of pemphigus wounds.49
Nutrition is a crucial aspect of care, due to the loss of protein and other essential components in the serous sanguineous drainage. Patients should avoid excessive skin manipulation and minimize activities that may traumatize the skin and mucous membranes during active phases of the disease.10 These include contact sports and eating or drinking food that may irritate the oral cavity (spicy, acidic, hard and crunchy foods).
Summary
Pemphigus presents with superficial wounds (erosions) in the skin and oral mucosa. Systemic corticosteroids are typically used for treatment initiation, however, due to the need for prolonged treatment and high morbidity of long corticosteroid courses, the early introduction of corticosteroid-sparing immunosuppressive agents is a key principle of treatment. Measures aimed at managing cutaneous wounds are additional important aspects of the management of pemphigus. There is more to wound care than just dressing. Wound care has to do with creating an optimal wound microenvironment and addressing the needs of the patient. Dressing selection is best guided by both the wound characteristics and dressing special features. The ideal dressing material should provide a moist environment to the wound while shielding it from bacterial invasion. In patients with pemphigus, wounds are superficial, and dressings such as films, hydrogels, and PMDs would be appropriate choices.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bystryn J-C, Rudolph JL. Pemphigus. Lancet. 2005;366(9479):61–73. doi:10.1016/S0140-6736(05)66829-8
2. Kasperkiewicz M, Ellebrecht CT, Takahashi H, et al. Pemphigus. Nat Rev Dis Primers. 2017;3:17026. doi:10.1038/nrdp.2017.26
3. Bolognia J, Jorizzo JL, Schaffer JV. Dermatology.
4. Joly P, Litrowski N. Pemphigus group (vulgaris, vegetans, foliaceus, herpetiformis, brasiliensis). Clin Dermatol. 2011;29(4):432–436. doi:10.1016/j.clindermatol.2011.01.013
5. Brenner S, Wohl Y. A survey of sex differences in 249 pemphigus patients and possible explanations. SKINmed. 2007;6(4):163–165. doi:10.1111/skm.2007.6.issue-4
6. Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, Wolff K. Fitzpatrick’s dermatology in general medicine. In: McGraw-Hill’s Access Medicine Clinical Library.
7. Harman K, Brown D, Exton L, et al. British Association of Dermatologists’ guidelines for the management of pemphigus vulgaris 2017. Br J Dermatol. 2017;177(5):1170–1201. doi:10.1111/bjd.15930
8. Reis VM, Toledo RP, Lopez A, Diaz LA, Martins JE; Research CGoFS. UVB-induced acantholysis in endemic Pemphigus foliaceus (Fogo selvagem) and Pemphigus vulgaris. J Am Acad Dermatol. 2000;42(4):571–576.
9. James KA, Culton DA, Diaz LA. Diagnosis and clinical features of pemphigus foliaceus. Dermatol Clin. 2011;29(3):405–412. doi:10.1016/j.det.2011.03.012
10. Dabiri G, Damstetter E, Phillips T. Choosing a wound dressing based on common wound characteristics. Adv Wound Care. 2016;5(1):32–41. doi:10.1089/wound.2014.0586
11. Hertl M. Pathogenesis, Clinical Manifestations, and Diagnosis of Pemphigus. UpToDate, Post TW (Ed), UpToDate. Waltham (MA): UpToDate Inc. Available from: https://www.uptodate.com.
12. Bystryn J-C, Steinman NM. The adjuvant therapy of pemphigus: an update. Arch Dermatol. 1996;132(2):203–212.
13. Murrell DF, Peña S, Joly P, et al. Diagnosis and Management of Pemphigus: recommendations by an International Panel of Experts. J Am Acad Dermatol. 2018. doi:10.1016/j.jaad.2018.02.021
14. Ahmed AR, Spigelman Z, Cavacini LA, Posner MR. Treatment of pemphigus vulgaris with rituximab and intravenous immune globulin. N Engl J Med. 2006;355(17):1772–1779. doi:10.1056/NEJMoa062930
15. Gregoriou S, Efthymiou O, Stefanaki C, Rigopoulos D. Management of pemphigus vulgaris: challenges and solutions. Clin Cosmet Investig Dermatol. 2015;8:521. doi:10.2147/CCID
16. Joly P, Maho-Vaillant M, Prost-Squarcioni C, et al. First-line rituximab combined with short-term prednisone versus prednisone alone for the treatment of pemphigus (Ritux 3): a prospective, multicentre, parallel-group, open-label randomised trial. Lancet. 2017;389(10083):2031–2040. doi:10.1016/S0140-6736(17)30070-3
17. Kridin K. Emerging treatment options for the management of pemphigus vulgaris. Ther Clin Risk Manag. 2018;14:757. doi:10.2147/TCRM.S142471
18. Lapidoth M, David M, Ben-Amitai D, Katzenelson V, Lustig S, Sandbank M. The efficacy of combined treatment with prednisone and cyclosporine in patients with pemphigus: preliminary study. J Am Acad Dermatol. 1994;30(5):752–757. doi:10.1016/s0190-9622(08)81506-x
19. Ratnam K, Phay K, Tan C. Pemphigus therapy with oral prednisolone regimens a 5-year study. Int J Dermatol. 1990;29(5):363–367.
20. Lever WF, White H. Treatment of pemphigus with corticosteroids: results obtained in 46 patients over a period of 11 years. Arch Dermatol. 1963;87(1):12–26. doi:10.1001/archderm.1963.01590130018006
21. Harman K, Albert S, Black M. Guidelines for the management of pemphigus vulgaris. Br J Dermatol. 2003;149(5):926–937. doi:10.1111/j.1365-2133.2003.05665.x
22. Knudson RM, Kalaaji AN, Bruce AJ. The management of mucous membrane pemphigoid and pemphigus. Dermatol Ther. 2010;23(3):268–280. doi:10.1111/j.1529-8019.2010.01323.x
23. Mahmoudi H, Balighi K, Tavakolpour S, Daneshpazhooh M, Chams-Davatchi C. Trichloroacetic acid as a treatment for persistent oral mucosal lesions in pemphigus vulgaris. J Am Acad Dermatol. 2019;80(3):e51–e52. doi:10.1016/j.jaad.2018.08.039
24. Hsu D, Brieva J, Sinha A, Langan S, Silverberg JI. Comorbidities and inpatient mortality for pemphigus in the USA. Br J Dermatol. 2016;174(6):1290–1298. doi:10.1111/bjd.14463
25. Falanga V. Occlusive wound dressings: why, when, which? Arch Dermatol. 1988;124(6):872–877.
26. Han S-K. Interactive wound dressings. In: Innovations and Advances in Wound Healing. Berlin: Springer; 2016:39–61.
27. Armstrong DG. Basic Principles of Wound Management. UpToDate, Post TW (Ed), UpToDate. Waltham (MA): UpToDate Inc. 2019. Available from:. https://www.uptodate.com.
28. Powers JG, Morton LM, Phillips TJ. Dressings for chronic wounds. Dermatol Ther. 2013;26(3):197–206. doi:10.1111/dth.12055
29. Broussard KC, Powers JG. Wound dressings: selecting the most appropriate type. Am J Clin Dermatol. 2013;14(6):449–459. doi:10.1007/s40257-013-0046-4
30. Borda LJ, Macquhae FE, Kirsner RS. Wound dressings: a comprehensive review. Curr Dermatol Rep. 2016;5(4):287–297. doi:10.1007/s13671-016-0162-5
31. de la Feld SF, Sami N. Local treatments and supportive care. In: Sami N, editor. Autoimmune Bullous Diseases: approach and management. Berlin: Springer; 2016:243–262.
32. Blackman JD, Senseng D, Quinn L, Mazzone T. Clinical evaluation of a semipermeable polymeric membrane dressing for the treatment of chronic diabetic foot ulcers. Diabetes Care. 1994;17(4):322–325. doi:10.2337/diacare.17.4.322
33. Kim YJ, Lee SW, Hong SH, Lee HK, Kim EK. The effects of PolyMem (R) on the wound healing. J Korean Soc Plast Reconstr Surg. 1999;26(6):1165–1172.
34. Benskin LL. PolyMem® Wic® Silver® Rope: a multifunctional dressing for decreasing pain, swelling, and inflammation. Adv Wound Care. 2012;1(1):44–47. doi:10.1089/wound.2011.0285
35. Lehman JS, Murrell DF, Camilleri MJ, Kalaaji AN. Infection and infection prevention in patients treated with immunosuppressive medications for autoimmune bullous disorders. Dermatol Clin. 2011;29(4):591–598. doi:10.1016/j.det.2011.06.021
36. Ahmed AR, Moy R. Death in pemphigus. J Am Acad Dermatol. 1982;7(2):221–228. doi:10.1016/s0190-9622(82)70111-2
37. Schultz GS, Sibbald RG, Falanga V, et al. Wound bed preparation: a systematic approach to wound management. Wound Repair Regen. 2003;11:S1–S28.
38. Robson MC. Wound infection: a failure of wound healing caused by an imbalance of bacteria. Surg Clin North Am. 1997;77(3):637–650.
39. Bowler P, Duerden B, Armstrong DG. Wound microbiology and associated approaches to wound management. Clin Microbiol Rev. 2001;14(2):244–269. doi:10.1128/CMR.14.2.244-269.2001
40. Krasner D, Kane D. Chronic Wound Care: A Clinical Source Book for Healthcare Professionals. Wayne (PA): Health Management Publications; 1997.
41. Lundberg CV, Frimodt-Møller N. Efficacy of topical and systemic antibiotic treatment of meticillin-resistant Staphylococcus aureus in a murine superficial skin wound infection model. Int J Antimicrob Agents. 2013;42(3):272–275. doi:10.1016/j.ijantimicag.2013.05.008
42. O’Donnell JA, Gelone SP, Safdar A, editors. Topical antibacterials. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Elsevier; 2015:452–462.e452.
43. Lipsky BA, Hoey C. Topical antimicrobial therapy for treating chronic wounds. Clin Infect Dis. 2009;49(10):1541–1549. doi:10.1086/644732
44. O’Meara S, Richardson R, Lipsky BA. Topical and systemic antimicrobial therapy for venous leg ulcers. JAMA. 2014;311(24):2534–2535. doi:10.1001/jama.2014.4574
45. Leaper D. Appropriate use of silver dressings in wounds: international consensus document. Int Wound J. 2012;9(5):461–464. doi:10.1111/j.1742-481X.2012.01091.x
46. Fonder MA, Lazarus GS, Cowan DA, Aronson-Cook B, Kohli AR, Mamelak AJ. Treating the chronic wound: A practical approach to the care of nonhealing wounds and wound care dressings. J Am Acad Dermatol. 2008;58(2):185–206. doi:10.1016/j.jaad.2007.08.048
47. Lansdown AB. Silver. I: its antibacterial properties and mechanism of action. J Wound Care. 2002;11(4):125–130. doi:10.12968/jowc.2002.11.4.26389
48. Wu CS, Hsu HY, Hu SCS, Chiu HH, Chen GS. Silver‐containing Hydrofiber Dressing is an Effective Adjunct in the Treatment of Pemphigus Vulgaris. Kaohsiung J Med Sci. 2009;25(11):622–627. doi:10.1016/S1607-551X(09)70567-4
49. Masjedi H, Malekzad F, Marashian SM, Younespour S. The healing effect of nano-silver dressings in pemphigus vulgaris. Wounds. 2015;2(2).
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.