")
Back to Journals » International Medical Case Reports Journal » Volume 15
Management of Chronic Ulcer Mimicking Oral Squamous Cell Carcinoma in Down Syndrome Child with Motoric Disorders
Authors Shafuria A , Dwiarie TA, Hidayat W
Received 29 June 2022
Accepted for publication 12 August 2022
Published 19 August 2022 Volume 2022:15 Pages 419—424
DOI https://doi.org/10.2147/IMCRJ.S379798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Amira Shafuria,1 Theodora Adhisty Dwiarie,1 Wahyu Hidayat2
1Oral Medicine Residency Program, Faculty of Dentistry, Padjadjaran University, Bandung, Indonesia; 2Oral Medicine Department, Faculty of Dentistry, Padjadjaran University, Bandung, Indonesia
Correspondence: Amira Shafuria, Email [email protected]
Introduction: Down syndrome is a congenital genetic disorder caused by an error in cell division, resulting in the presence of an additional third chromosome 21. Down syndrome is one of the leading causes of intellectual disability. Millions of these patients face various health issues. This study aimed to provide information about the challenges in the management of chronic ulcer mimicking OSCC in Down Syndrome child with motoric disorders.
Case: A 12-year-old boy with Down Syndrome and motoric disorders was referred to Oral Medicine Department. In the extraoral examination, the patient had a dysmorphic face and dry lips. Lymph node examination could not be assessed because the patient wore a cervical collar. The intraoral examination showed an irregular ulcer with 1× 0.7 cm in diameter, indurated margin, and white-yellowish base at the right lateral border of the tongue. The 55 teeth were sharp and caused an occlusion trauma to the right lateral border of the tongue. The patient was diagnosed with a chronic traumatic ulcer mimicking OSCC based on clinical examination. The medication given to the patient were sodium chloride 0.9%, povidone-iodine mouthwash 1%, and petroleum jelly.
Conclusion: Children with Down syndrome often suffer from orofacial abnormalities which can affect their oral health and their family’s quality of life. Dental and oral care for Down Syndrome children with motoric disorders required some challenges and collaboration with their parents, families, and caregivers.
Keywords: down syndrome, chronic ulcer, oral squamous cell carcinoma, motoric disorders
Introduction
Down syndrome is a congenital genetic disorder caused by an error in cell division, resulting in the presence of an additional third chromosome 21. Three genetic variations can cause Down Syndrome. In 95% of cases, Down Syndrome is caused by an extra chromosome 21 in all cells (trisomy 21). This condition gives them 47 chromosomes instead of the normal 46. The incidence of trisomy is influenced by maternal age and differs in the population (between 1 in 319 and 1 in 1000 live births).1–3
Down syndrome is one of the leading causes of intellectual disability. Millions of these patients face various health issues including learning and memory, cancers, leukemia, congenital heart disease, Alzheimer’s disease, and Hirschprung disease.3 Multidisciplinary treatment depends on the level and type of disability. It involves a team of clinician specialists in neurology, ophthalmology, orthopedics, audiology, cardiology, physical and occupational therapy, speech-language therapy, nutrition, and mental health.1
People with Down Syndrome are more prone to suffer from orofacial conditions such as dental anomalies, malocclusion, periodontal disease, xerostomia, a compromised buffer capacity of saliva, and soft tissue disturbances such as inverted lips and protruding tongues.2,4,5 They have dysfunctional chewing and swallowing, a higher probability of being mouth breathers, and they are also susceptible to demineralization and dental caries.6 Uncooperative behavior during dental care, poor oral health, and susceptibility to periodontal disease make people with Down Syndrome at an increased risk for poor oral health. Parents reported difficulty across almost all oral care variables, including oral care in the home, oral care at the dentist, and access to oral care. Those behaviors and sensitivities made care challenging.7
Case Presentation
A 12-year-old boy with Down Syndrome and motoric disorders was referred from the Pediatric Department to the Oral Medicine Department of RS Hasan Sadikin Bandung. The patient was diagnosed with Down Syndrome and myeloradiculopathy. The patient’s mother said that the patient was admitted to the hospital because of weakness in both patient’s hands and feet. The patient had a history of falling down about one year ago. The patient’s mother also had a difficulty in cleaning the patient’s oral cavity regularly.
In the extraoral examination, the patient had a dysmorphic face. The patient also had a cracking and desquamative condition of the vermillion border of the lips. Lymph node examination could not be assessed because the patient wore a cervical collar. The intraoral examination showed an irregular ulcer with 1×0.7 cm in diameter, indurated margin, and white-yellowish base at the right lateral border of the tongue. There was dentinal caries on 63 tooth and also the tooth remnants on 55, 62, 74, and 85 teeth. The upper and lower tooth remnants were suggested to be extracted by pediatric dentist. The space of the extracted teeth will be maintained using a space maintainer. The 55 tooth was sharp and caused an occlusion trauma to the right lateral border of the tongue [Figure 1].
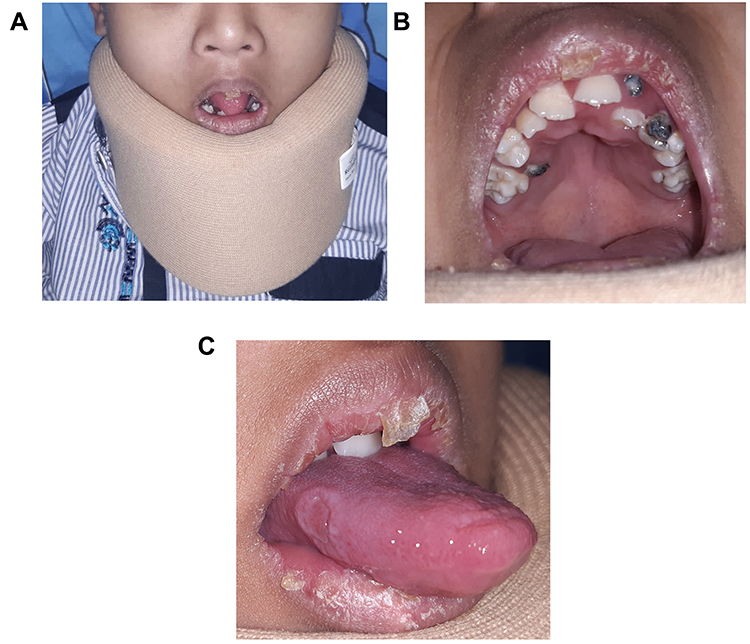 |
Figure 1 Clinical manifestations in the first visit. |
Laboratory examination showed a decrease in sodium value (130 mEq/L) and an increase in lymphocyte value (46%). The MRI examination was performed in the Radiology Department to determine the presence of abnormalities in the cervical spine. The results of the MRI examination showed a dislocation of the patient’s cervical spine. The patient’s mother provided informed consent to publish the patient’s case details and any accompanying images [Figure 2].
 |
Figure 2 The results of the MRI examination showed a dislocation of the patient’s cervical spine. |
Based on the history review, the clinical examination, and appropriate investigation, the patient was diagnosed with a chronic traumatic ulcer mimicking OSCC, exfoliative cheilitis, reversible pulpitis of 63 teeth, and radix gangrene on 55, 62, 74, and 85 teeth. The diagnosis of the chronic ulcer was based on clinical examination. There was an indurated margin in the traumatic lesion, which mimicked Oral Squamous Cell Carcinoma clinically. The patient has been hospitalized for 4 days and was given paracetamol 120 mg/5 mL oral suspension and amoxicillin 125 mg/5 mL oral suspension from the Pediatric Department. The patient also was given sodium chloride 0.9% solution, povidone-iodine mouthwash 1%, and petroleum jelly from the Oral Medicine Department. The patient’s mother was instructed to clean the patient’s oral cavity using gauze soaked in sodium chloride 0.9% solution, compress the ulcer using povidone-iodine mouthwashes 1% three times a day as an antiseptic and anti-inflammatory agent to the oral ulcer, and apply petroleum jelly to moisturize the patient’s lips. The patient was also suggested to extract the 55, 62, 74, and 85 teeth.
In the second visit (3 days follow-up), oral lesions already showed improvement [Figure 3]. In the third visit (1-week follow-up), the size of the oral ulcer at the lateral border of the tongue was getting smaller and the lesion of the lips had some improvement [Figure 4].
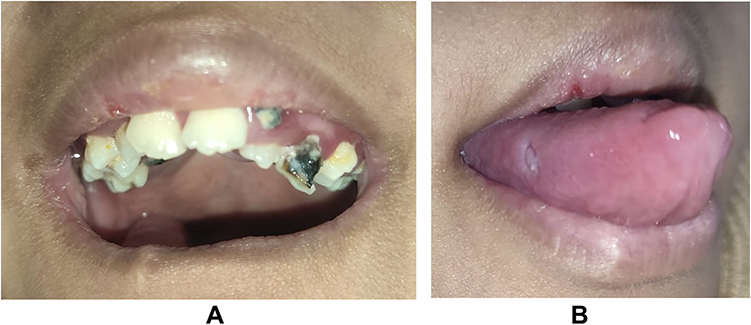 |
Figure 3 The oral lesions already showed improvement (3 days follow-up). |
 |
Figure 4 The size of the oral ulcer at the lateral border of the tongue was getting smaller and showed some improvement in the third visit (1-week follow-up). |
In the fourth visit (10 days follow-up), the size of the oral ulcer at the lateral border of the tongue already had significant improvement. Two days after the fourth visit, the patient underwent neurosurgery. The patient was observed in the Pediatric Intensive Care Unit postoperatively. After two weeks of observation in the Pediatric Intensive Care Unit, the experienced respiratory failure and was declared dead [Figure 5].
 |
Figure 5 In the fourth visit (10 days follow-up), the size of the oral ulcer at the lateral border of the tongue already had a significant improvement. |
Discussion
In this case, the patient was diagnosed with chronic ulcer mimicking Oral Squamous Cell Carcinoma (OSCC). The patient suffered from a traumatic ulcer on the lateral border of the tongue caused by an occlusal trauma from 55 teeth. The most common cause of single ulcers on the oral mucosa is trauma. The diagnosis is based on the history and physical findings. Squamous cell carcinoma is always in the differential diagnosis for a nonhealing ulcer. All ulcers present for two to four weeks should be biopsied to rule out squamous cell carcinoma or other pathology.8
The medication given by the Oral Medicine Department was sodium chloride 0.9% solution, povidone-iodine mouthwash 1%, and petroleum jelly. The patient’s mother was instructed to clean the patient’s oral cavity using gauze soaked in sodium chloride 0.9% solution three times a day, compress the ulcer using povidone-iodine mouthwashes 1% three times a day, and apply the petroleum jelly to the patient’s lips.
Kurniawati et al studied the effectiveness of oral rinsing with sodium chloride and sterile water in preventing and reducing the damage in oral mucous membranes. The experiment showed that oral rinsing with sodium chloride is more effective in reducing damage to the oral mucous membrane.9 Huynh et al also described that rinsing with sodium chloride solution promotes migration. This is an essential process during wound healing in the human gingival fibroblast. Rinsing the mouth with a salt solution is the most preferable method for oral wound care.10
Kanagalingam et al observed the anti-inflammatory properties of povidone-iodine on host cytokine generation induced by pathogens. TNF-α has several roles as a regulator of inflammation. Povidone-iodine has potent anti-inflammatory, anti-edematous, antiseptic, and hemostyptic effects. These effects of povidone-iodine can benefit patients suffering from oral mucositis. Several studies described the usage of povidone-iodine in treating the symptoms. These studies demonstrating reduced incidence, severity, time to onset, and duration of oral mucositis.11,12
Individuals with Down syndrome have some orofacial abnormalities which can impact their oral health and their family’s quality of life. Early professional treatment and daily care at home can reduce their severity and allow people with Down syndrome to enjoy the benefits of a healthy mouth.13 In their recent study, AlJameel et al examined the Oral Health-Related Quality of Life (OHRQoL) for children with Down Syndrome and their families from parents’ perspectives. The results indicated that oral health issues can cause negative impacts on their quality of life at different levels. These children need to receive appropriate care promptly. Poor oral health status often results in pain, emotional, and social issues.4
Children with Down Syndrome have learning disabilities but exhibit a wide range of behaviour in the dental setting. It includes compliance, cooperation, phobia, mild to moderate anxiety, and complete lack of cooperation. Motor functions are usually delayed in younger persons with Down Syndrome. Therefore, good oral hygiene may need to be the responsibility of the primary caregiver until the individual can develop the necessary coordination to become self-sufficient.1
According to Stein et al, parents reported difficulty across almost all oral care variables. One-third of parent respondents reported that toothbrushing was difficult and that brushing occurred 4 or fewer days a week. Over half of the respondents reported it was difficult to have a dental professional clean their child’s teeth. That those behaviours and sensitivities made care challenging.7 Peinado et al compared the dental characteristics and the oral health-care needs of patients with Cerebral Paralysis and Down Syndrome. Dental prophylaxis was the most prevalent treatment in patients with Down Syndrome and the most frequent habit was oral breathing.6 Martinez et al also described that the children with Cerebral Palsy and those with Down Syndrome presented a large number of anomalies in dental development, such as delayed eruption and the presence of wear and abrasions. Both studies concluded that patients with Cerebral Palsy and Down Syndrome require early dental care in order to prevent and limit the severity of the pathologies.6,14
Patients with disabilities have some oral health problems due to poor oral hygiene which caused by a limited cooperation by the patient to daily oral hygiene procedures, the difficulty during mastication and to cariogenic diet. Regular dental check-ups are important to achieve and maintain a high standard of oral health. It is useful to anticipate the first dental examination in children with special health care needs at 1 year of age and scheduling regular dental recalls at least on a four/six-month basis. Improving dentists’ willingness is also important to treat people with special health-care needs. This could be attained by providing lectures and hands-on education in dental therapy in persons with special health-care needs and also coordination of the professional team through an integrated education.15
In this case report, the patient was diagnosed with Down Syndrome with motoric disorders. This condition causes the weakness of both patient’s hands and feet. The patient could not move his upper and lower extremities. There were some difficulties to treat and maintain the patient’s oral health status. This condition becomes a challenge in the management of chronic ulcer mimicking OSCC in Down Syndrome child with motoric disorders. Therefore, the health providers, family, and caregivers should be involved to maintain a high standard of oral health in children with special health-care needs.
Conclusion
Children with Down syndrome often suffer from orofacial abnormalities which can affect their oral health and their family’s quality of life. In this case report, the therapy given to the patient were sodium chloride 0.9%, povidone-iodine mouthwash 1%, petroleum jelly, and also extraction of the tooth remnants. Dental and oral care for Down Syndrome children with motoric disorders required some challenges and collaboration with their parents, families, and caregivers.
Acknowledgment
We would like to thank the patient and his family who participated kindly in this study. This study was approved by Oral Medicine Department, Faculty of Dentistry, Padjadjaran University.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Aldossary DMS. Down syndrome: a review for the dental professionals. IOSR J Dent Med Sci. 2017;16(07):61–66. doi:10.9790/0853-1607016166
2. Contaldo M, Santoro R, Romano A, et al. Oral manifestations in children and young adults with down syndrome: a systematic review of the literature. Appl Sci. 2021;11(12):5408. doi:10.3390/app11125408
3. Asim A, Kumar A, Muthuswamy S, Jain S, Agarwal S. Down syndrome: an insight of the disease. J Biomed Sci. 2015;22(1):1–9. doi:10.1186/s12929-015-0138-y
4. Aljameel AH, Alkawari H. Oral health-related quality of life (Ohrqol) of children with down syndrome and their families: a cross-sectional study. Children. 2021;8(11):954. doi:10.3390/children8110954
5. Ghaith B, Al Halabi M, Kowash M. Dental implications of Down Syndrome (DS): review of the oral and dental characteristics. JSM Dent. 2017;5(2):1087.
6. Rodríguez Peinado N, Mourelle Martínez MR, Diéguez Pérez M, De Nova García MJ. A study of the dental treatment needs of special patients: cerebral paralysis and down syndrome. Eur J Paediatr Dent. 2018;19(3):233–238. doi:10.23804/ejpd.2018.19.03.12
7. Stein Duker LI, Richter M, Lane CJ, Polido JC, Cermak SA. Oral care experiences and challenges for children with down syndrome: reports from caregivers. Pediatr Dent. 2020;42(6):430–435.
8. Glick M. Burket’s Oral Medicine Diagnosis & Treatment.
9. Kurniawati D. Oral hygiene normal saline vs air steril: mengurangi kerusakan membran mukosa oral. J Ilm Kesehat. 2018;6(2):68–72. doi:10.35952/jik.v6i2.95
10. Huynh NC, Everts V, Leethanakul C, Pavasant P. Rinsing with saline promotes human gingival fibroblast wound healing in vitro. PloS One. 2016;1–13. doi:10.1371/journal.pone.0159843
11. Amtha R, Kanagalingam J. Povidone-iodine in dental and oral health: a narrative review. J Int Oral Heal. 2020;12(5):407–412. doi:10.4103/jioh.jioh_89_20
12. Kanagalingam J, Feliciano R, Hah JH, Labib H, Le TA, Lin JC. Practical use of povidone-iodine antiseptic in the maintenance of oral health and in the prevention and treatment of common oropharyngeal infections. Int J Clin Pract. 2015;69(11):1247–1256. doi:10.1111/ijcp.12707
13. National Institute of Dental and Craniofacial Research. Practical Oral Care for People with Down Syndrome. National Institute of Dental and Craniofacial Research; 2009.
14. Diéguez-Pérez M, de Nova-García MJ, Mourelle-Martínez MR, Bartolomé-Villar B. Oral health in children with physical (Cerebral Palsy) and intellectual (Down Syndrome) disabilities: systematic review I. J Clin Exp Dent. 2016;8(3):e337–43. doi:10.4317/jced.52922
15. Vozza I. Preventive strategies in oral health for special needs patients. Ann Stomatol. 2015;96–99. doi:10.11138/ads/2015.6.3.096
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.