")
Back to Journals » Clinical Interventions in Aging » Volume 18
Management of Agitation in Behaviours That Challenge in Dementia Care: Multidisciplinary Perspectives on Non-Pharmacological Strategies
Authors James IA , Reichelt K, Shirley L, Moniz-Cook E
Received 30 November 2022
Accepted for publication 19 January 2023
Published 18 February 2023 Volume 2023:18 Pages 219—230
DOI https://doi.org/10.2147/CIA.S399697
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Ian Andrew James,1,* Katharina Reichelt,2,* Louisa Shirley,3 Esme Moniz-Cook4
1Innovations Group, Cumbria Northumberland Tyne & Wear NHS Trust, Newcastle upon Tyne, UK; 2Older People’s Services, Cumbria Northumberland Tyne & Wear NHS Trust, Newcastle upon Tyne, UK; 3Clinical and Health Psychology, University of Manchester, Manchester, UK; 4Faculty of Health Sciences, University of Hull, Hull, UK
*These authors contributed equally to this work
Correspondence: Ian Andrew James, Innovations Team, Campus for Ageing and Vitality, Westgate Road, Newcastle-Upon-Tyne, NE4 6BE, UK, Tel +44 7375635573, Email [email protected]
Objective: NICE guidelines recommend non-pharmacological interventions as the first-line approach for the management of behaviours that challenge. Recent work, however, highlights dissatisfaction with the lack of detailed guidance in the national guidelines regarding non-drug interventions. This study examines the views of practitioners regarding non-pharmacological treatments. It further explores perspectives on non-pharmacological strategies used in the management of agitation occurring within episodes of behaviours that challenge.
Methods: Forty-two experienced practitioners attended a workshop where behaviours that challenge were described as occurring in three phases of agitation, using a framework adapted from the Positive Behaviour Support framework (pre-agitation, triggering and escalating, high level). The participants were asked to populate a template derived from the adapted framework. The completed templates recorded the clinical strategies the participants found useful to (i) prevent the occurrence of agitation, (ii) de-escalate distress and (iii) deal with perceived high levels of agitation.
Results: The Positive Behaviour Support conceptual framework was perceived by participants as helpful in organising their clinical work. A number of interventions were suggested as preventative strategies: music therapy, doll therapy, physical activity and generic person-centred communication skills to enhance wellbeing. In contrast, de-escalation strategies identified by the participants focused on reducing emotional distress. The approaches for dealing with continued high levels of agitation involved a number of “control and restraint” techniques as well as medication.
Conclusion: The template allowed specialist multidisciplinary professionals to identify skills for the management of distress and agitated behaviour linked to the respective phase of arousal. The template has scope to guide practitioners to identify the detail needed for the management of behaviours that challenge. The findings have the potential to influence the contents of forthcoming guidelines on alternatives to psychotropics in dementia care.
Keywords: dementia, behaviour, distress, micro-skills, strategies, Positive Behaviour Support, PBS
Introduction
Existing guidelines recommend non-pharmacological intervention as the first-line approach for the management of behaviours that challenge,1,2 but a number of studies note that the quality of the non-drug recommendations in such guidelines require improvement.3,4 Dyer and colleagues’ summary of the findings of fifteen systematic reviews5 concluded that non-pharmacological approaches had similar effect sizes to pharmacological approaches, but with a lower risk of adverse events. Importantly, the reviewers acknowledged that the best effect-sizes were observed for atypical antipsychotics (marginally better than the best non-drug interventions); however, the side-effect profiles for antipsychotics were highly problematic. Individualised formulation-led interventions are, to date, the best evidenced alternative to both antipsychotics and other psychotropic drugs.6,7 These individualised approaches are sometimes known as functional-analysis-based interventions,5,8 involving a structured biopsychosocial method of gathering information to detect the unmet need and potential cause(s) of behaviour. They are usually developed with the support of a psychologist, and are appreciated by staff working in care homes.9
“Behaviours that challenge” (BtC) is a broad term covering wide ranging behaviours such as depression, apathy, aggression, repetitive questioning, psychosis, sleep problems, wandering, and socially inappropriate behaviours.10 Various other names have been given to this group of emotions and actions, including: challenging behaviour, behavioural and psychological symptoms of dementia, behaviours of concern, distressed behaviours, etc. Currently, the precise terminology is subject to debate amongst professionals, people with dementia and families.11–14
For the remainder of this article, however, the authors will refer to the behaviour of interest as “agitation”. A number of researchers have suggested that agitation is an important sub-syndrome of BtC,15,16 with features such as depression and apathy sitting outside the grouping. In clinical practice, agitation is a general term that includes a range of actions – such as physical aggressive behaviour (hitting, grabbing, kicking, pushing), physically non-aggressive behaviour (pacing, restlessness), verbal aggressive behaviour (swearing, threats) and verbal non-aggressive behaviour (requests for attention, complaining, negativism, ceaseless talking, groaning).16 The current study examined the specific management of situations involving high degrees of emotional arousal on the part of people living with dementia by focusing on agitation within BtC.
When assessing the impact of agitation in more detail, it is evident that it is associated with substantial costs, both personal and financial. Studies calculate the financial impact as 44% of the total health and social care annual costs for people with dementia in care homes in the UK, and 29% of the total costs for those living at home.17,18 The costs associated with agitation across Europe and in the US are also high, with the total incremental cost reported as $4.3 billion.19,20
On reviewing management of agitation, Livingston et al21 concluded that person-centred care and supervised communication skills training were effective, but only for those living in care homes. Subsequent empirical work suggested that the delivery of person-centred care and communication training required intensive input from experienced and qualified staff. Indeed, when the training programmes were delivered by graduate psychologists significant effects were not obtained.22 The mechanisms through which “good” carer communication skills lead to reductions in agitation are currently a major focus of investigation.23–25 Understanding the mechanisms is particularly relevant because there is a risk of undermining the dignity in a person living with dementia through poor quality interactions by care providers.26
An area of interest in relation to improving communication skills is mapping carers’ verbal and non-verbal communication skills onto people’s levels of emotional arousal during episodes of agitation.27,28 A promising approach that has scope to manage heightened arousal and agitation in dementia is the Positive Behavioural Support (PBS) Arousal framework,29 which is widely applied in intellectual disability services. It has been used for the management of frontotemporal dementia presentations30,31 and its “Arousal Graph” has been adapted for dementia care practice.7 James and colleagues7 employed the graph on an inpatient unit and showed that it can be used clinically to investigate the change-mechanisms underpinning the successful management of agitation. The PBS arousal graph represents behaviours in terms of four phases of a bell-shaped curve: pre-agitation; escalation; heightened agitation; and calming. These distinctive phases provide a template for targeting non-pharmacological interventions for agitation as follows: agitation prevention, de-escalation, risk management, and calming.
The present study aims to detail the skills and strategies suggested by specialist multidisciplinary professionals working in dementia care, using a template derived from the PBS Arousal Graph. More specifically, the study seeks to investigate management strategies in terms of their micro-skills,32 where micro-skills are defined as ‘the communication and interactions skills employed by caregivers when providing good dementia care including the use of calm language and behaviour, along with other communication techniques”.33 Hence, the study attempts to investigate the fine grain communication and interaction skills associated with the over-arching management of agitation and emotional distress. It is worth noting that the micro-skills can be contrasted with the “macro-features” of care, which are the structural aspects such as care plans, formulations and “named” therapies. The macro-features have often received greater attention than the micro-skills,5 but both aspects work together in the delivery of quality care (eg, it is the structured frameworks that guide the delivery of the micro-skills).
Materials and Methods
Professionals working with people with dementia with specialist interest in behaviours that challenge were invited to a one-day workshop. They were recruited via email from a network of experienced practitioners working in services providing care for people with dementia, and from key professional organisations in the UK (eg, Royal Colleges of Psychiatry, GPs, Nursing, Occupational Therapy, and third sector representatives).
Forty-two professionals attended and consented to this study. They were psychologists (26.2%), the voluntary sector/charities (14.3%), social workers (11.9%), nurses (9.5%), psychiatrists (9.5%), occupational therapists (9.5%), and other professionals (19%), ie, Specialist General Practitioners (n = 3), speech and language therapists (n = 3), and pharmacists (n = 2).
Data Collection
On the day of the workshop participants were seated on seven tables of six people each. At the start of the session, the participants were introduced to the concept of the PBS “Arousal” graph. The use of the graph in the learning difficulty specialty was discussed, as well as its adaptation.7 No information on management strategies or interventions was provided. Participants were then asked to engage in group discussions on each table regarding the management of agitation, prior to completing a questionnaire. The questionnaire was split into the three phases (preventative strategies; de-escalation strategies; strategies to deal with high levels of agitation and emotion). The calming phase was not a focus of the current study, due to the fact that there is a great deal of overlap between the preventative and calming phases. For each of the three phases, participants were invited to describe their preferred non-pharmacological management strategies. Each participant was asked to respond as an individual, although their responses were informed by both the presentation and the group discussions that occurred on their respective tables.
The following instructions were given regarding the completion of the questionnaire:
We’d like your advice about actions and responses you’d use to manage “Behaviours that Challenge”. We’d like you to provide answers in terms of three phases - strategies to: (i) prevent agitation occurring, (ii) de-escalate behaviours once triggered; (iii) deal with highly agitated or emotional behaviours.
The three phases are explained in more detail below:
(i) Prevention – In this phase the aim is to use non-drug approaches to prevent agitation arising.
(ii) De-escalation – In this phase the aim is to respond to early warning signals to stop or reduce the escalation of agitation.
(iii) Dealing with highly emotional and/or agitated behaviours – In this phase the aim is to respond to behaviours in which a great deal of emotion is being expressed (eg, aggression, anxiety, etc.).
The participants were given 60 minutes to complete the task individually following the group discussions. Facilitators were available during the workshop to answer any queries from the participants. A debriefing about the use of the template was undertaken following the completion of the questionnaire to determine the participants’ perceptions of the PBS framework.
Data Analysis: Frequency counts of words were used where appropriate, because many participants responded with lists of words and phrases rather than descriptive sentences (eg, training, assess pain, good communication, use of formulations, etc.). Where required, analyses of sentences were carried out using Braun and Clarke’s34 approach to thematic analysis, which involves coding and theme development. Two researchers read and re‐read the data, noting any initial analytic observations. They then undertook a process of systematic data coding, identifying key features of the sentences. The first coder produced a list of themes, with detailed criteria for the different themes. The list was used by the second coder on ten sentences and consensus was obtained via discussion in terms of theme and the descriptive criterion. Then, the second coder analysed all the sentences, with the same themes being identified in 89% sentences. For those sentences where the coders did not agree, they worked together to reach consensus.
Ethics
The project was approved by the University of Hull Ethics Committee. The participants consented for their anonymized responses to be published.
Results
From the 42 people who attended the workshop, thirty-two questionnaires were submitted. One group of participants mistakenly completed their forms in pairs, and four participants did not submit a questionnaire. The debriefing, following the submission of the data, suggested that the participants found the PBS template useful in helping them to consider the different management strategies relating to agitation. However, no formal evaluation on the usefulness of the template was undertaken, which is a limitation of the study. The participants’ responses to the questionnaires are presented in three tables. Table 1 shows the participants’ recommendations for the preventative phase; Table 2 shows strategies to deal with behavioural escalation. Table 3 outlines recommendations for the management of behavioural displays of high levels of emotion (agitation and anxiety).
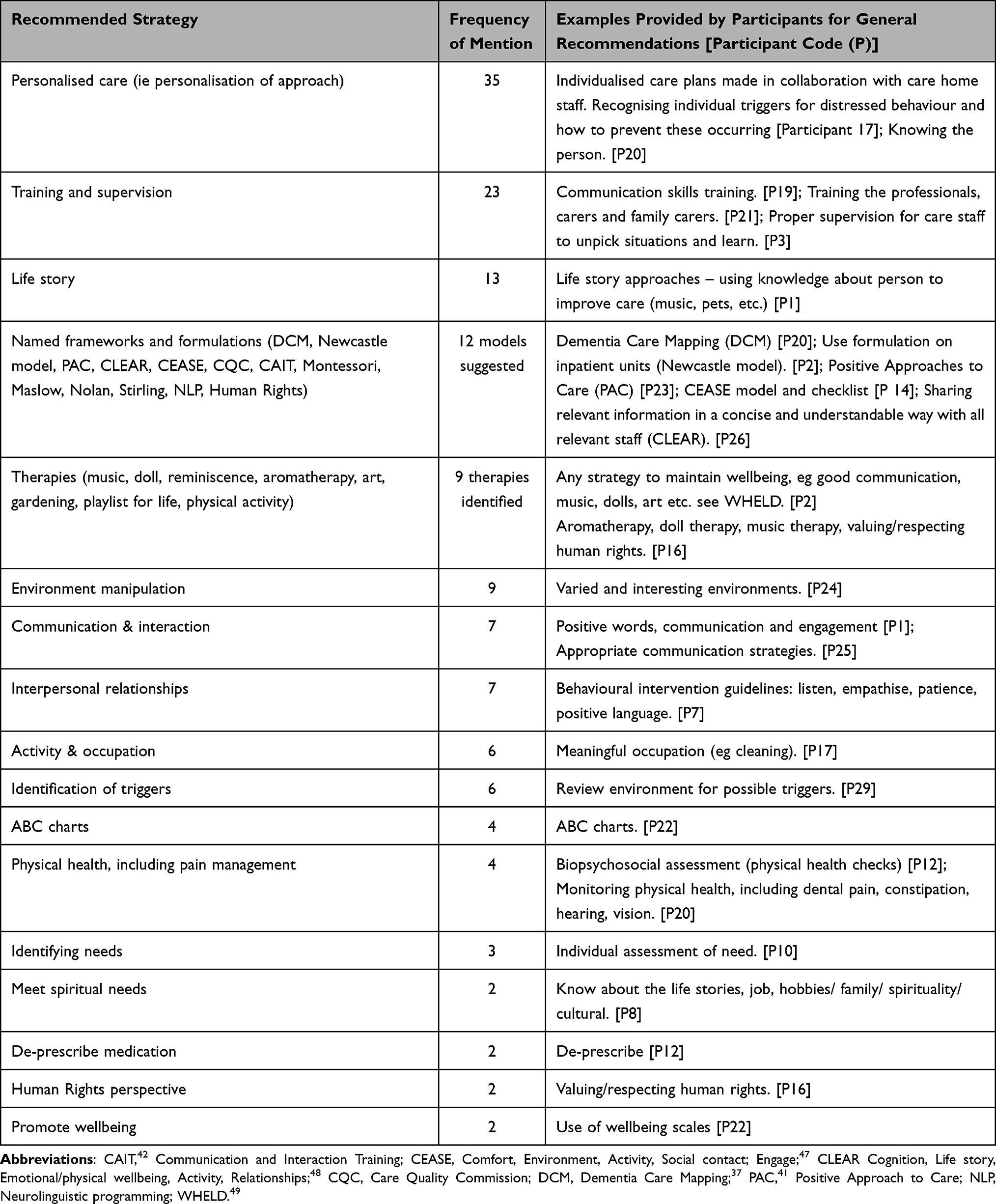 |
Table 1 Preventative Phase Strategies |
 |
Table 2 De-Escalation Strategies |
Preventative Strategies
Table 1 shows the types of strategies that were recommended, the number of times each strategy was mentioned by the participants, and examples of the participants’ statements.
Despite the term “person-centred” only being mentioned once, the terms “person” and “personalisation” featured many times within the section on “prevention”. It was clear that prevention was thought to require bespoke strategies:
Life story across all – but to bring this much more alive in terms of what this means for the person’s personal routines and preferences and to maintain wellbeing, e.g. to know their personality preferences/choices are they more likely to need quiet, space (introverted), or do they enjoy mixing – some higher depth of info and more about a person’s values and beliefs as well. [Participant (P) 24]
The term “training” was mentioned 23 times, but this begged the question of “training in what?”. From the data it was evident that the greatest areas identified for training and supervision were communication, improving relationships and use of bespoke activities. Participants recommended training of staff, families, and the use of “train the trainer” models. There were calls for the training to be relevant, practical and experiential, with the employment of coaching techniques, as illustrated:
Reflections/experiential training, with good level of knowledge about dementia. Family carer sessions – group and individual to help with solving problems. [P10].
There was a recommendation for online training programs, which is highly relevant in the context of COVID-19. One of the participants noted that it was important to establish a positive relationship between the trainers and the carers prior to the training commencing:
Build relationships with staff - develop trust before training and problem solving. [P3]
The term “formulation” was not used by any participant but a number of different conceptual frameworks were mentioned. Dementia Care Mapping was identified by four participants, and the Newcastle Model and Positive Approach to Care (PAC) by three respondents each; all the remaining frameworks were mentioned once or twice.
The use of specific therapies was recommended, with music, dolls, reminiscence and pet therapies being most commonly identified. The role of the environment in preventing the triggering of agitation was also perceived to be important. One participant recommended following the Royal College of Psychiatrists’ MSNAP guidance:
Environmental checklist to ensure facilities are designed to best practice, consider whether any of the MSNAP standards are relevant. [P10]
In contrast to the macro features outlined above, a number of participants suggested the use of micro-skills. For example, good communication was recognised as a means of maintaining wellbeing in people living with dementia, and preventing the occurrence of agitation. Participant 25 recommended coaching in the use of communication and de-escalation skills:
Need better access to communication strategies training and de-escalation strategies. [P25]
The role of physical health problems, especially pain management, was recognised as a potential trigger for agitation. Hence, physical health checks were seen as important preventative strategies. In an attempt to reduce potential problems arising, a number of participants mentioned the importance of recognising patterns of behaviours via the use of ABC charts, and other methods for understanding and identifying triggers. Other preventative strategies identified were to ensure people’s needs were being met, particularly in relation to pain, over-medicating and meeting people’s spiritual needs.
De-Escalation Phase Strategies
Table 2 shows the types of strategies that were recommended for “de-escalating” agitation; the number of times they were mentioned by the participants; participants’ quotes.
 |
Table 3 Strategies for Managing Risk |
In this section, participants provided more specific examples and focused responses such as PAC, BANGS and VERA, which are organised protocols developed specifically for improving carer interactions with people living with dementia. The recommendation of specified frameworks regarding “de-escalation” may reflect the perceived need for more precise strategies. The most frequently mentioned strategy was to provide practical and bespoke training. The participants highlighted the importance of good communication as part of the de-escalation plan. The CAIT and PAC programs were mentioned on a number of occasions, which is relevant because these are training packages that specifically teach de-escalation strategies.35
The other major response in this section was to promote effective environments. This feature related to the physical layout:
Check environment and biology. [P7].
and the culture of the environment:
More considerate to what’s required in a supportive environment, with details that are bespoke to the individual. [P24].
Management of High Levels of Emotional Behaviour
Table 3 shows the types of strategies recommended for managing highly emotional behaviours; the number of times each recommendation was mentioned by the participants; participants’ quotes.
In the responses to this phase, there was a greater emphasis on the use of “management of risk” protocols in order to keep the various stakeholders safe. Recommendations relating to control and restraint, forced care, and more formalised PMVA techniques featured strongly. Training programmes associated with these activities were also highly recommended. There was also support for training the carers at the preventative stage of the behaviours to identify the triggers, in order to reduce the likelihood of more problematic behaviours arising. There was an emphasis on organisational responses, including the use of guidance from regulatory bodies such as the Care Quality Commission (CQC) in the UK to ensure the appropriate governance was being followed.
One of the participants thought the strategies to be used in this phase should be similar to the previous phases, although with more emphasis on risk management, leading to more systematic interventions:
I don’t think there’s anything specifically about maintaining safety in itself – aside from the same things that apply in the other categories (Prevention and de-escalation categories above). Perhaps some greater focus on risks management options for more input and support for MDT assess/review. [P24]
A number of participants mentioned the importance of changing environments to reduce stress, but also looking at ways of creating environments which are safe for the residents and workers:
Can the person go anywhere else; should anything be moved from the environment. [P20]
The appropriate use of medication was also recommended. The specific use of “when required” medications was mentioned, which is consistent with national guidelines. Finally, it was felt by some participants that specialist teams may have a role in dealing with risky episodes of agitation. A helpful summary of many of the features highlighted in this section was provided by participant 13, who said:
Identify regular triggers, ensure people/staff are mindful of these. Identify what works in order to calm the situation before further escalation and offer training in identifying need and life history. [P13]
Discussion
The debriefing following the completion of the questionnaire suggested that the participants had a positive perception of the PBS framework. They found it helpful to breakdown the analyses of agitation into discrete phases because this helped to guide the use of more specific management strategies. It was also commented by the participants that in the past the value of preventative strategies in the management of agitation may have been overly promoted due to the methodological limitations of some of the major trials.1 This bias may be due to the fact that it is easier to design studies examining the impact of standardised therapies (aromatherapy, music therapy, etc.) compared to projects assessing the impact of de-escalation and restraint strategies.
In relation to the questionnaire data, the findings from this multi-disciplinary group show the participants recommended a mix of macro-features and micro-skills for the management of agitation across all phases. The discussion will first focus on “macro-features”, which are typically clinical pathways, care plans, formulations and “named” therapies. As such, macro-features are the structured conceptualisations or frameworks that guide the interventions and the micro-skills. Then, we will consider the micro-skills (process/interpersonal aspects).
Participants recommended the use of highly personalised forms of care in order to prevent and de-escalate agitation, and to manage risky behaviours. The use of “life story” work, and person-centred documentation (“This is me”) was favoured by a number of participants. The type of information that is required for this documentation is termed “biopsychosocial”, with information about the person’s physical and mental health, premorbid-personality, social routines and preferences being collected. One of the first widely used biopsychosocial models in the UK was Kitwood’s equation of care,36 which states that a person’s experience of dementia is determined by the interaction of their neurological impairment + physical health status + biography + malignant social psychology. Kitwood paid particular attention to the notion of “malignant social psychology”, which is a measure of whether someone with dementia is experiencing a loss of their “personhood” (ie, becoming stigmatised, infantilised, objectified or ignored, etc.). Kitwood developed a tool for assessing wellbeing and personhood called Dementia Care Mapping (DCM37); this is an important measure, which was reflected in its use being strongly recommended by the participants in the current study. The Newcastle model was also referenced frequently by participants. The Newcastle model has been employed successfully in the FITS (Focused Intervention Training and Support) randomised control trial.38 This was also the most widely used formulation nationally in a recent review of “Behaviours that challenge” formulation models,39 which identified 30 different frameworks used in the UK.
In terms of obtaining details about the behaviours themselves, participants suggested using monitoring tools such as ABC (antecedents-behaviour-consequences) charts as ways of identifying potential triggers. Such tools are crucial because they provide therapists with systematic information about the behaviour, particularly if the clinician has not been able to witness the behaviour in person. Via the use of such charts carers are also able to identify recurring patterns which may offer a point of intervention, eg, by changes to the environment or by the administering of health-related medications to deal with issues such as pain or delirium. Of note, the participants stressed the relevance of having appropriate physical and social environments in both maintaining wellbeing and dealing with risky behaviours.
The participants supported the use of training, supervision and coaching. It was made clear that they wanted relevant training, providing knowledge, support and skills for all carers across settings. Surr and Gates40 recently completed an extensive review of training in dementia care. In their education and training study “What Works?” they developed dementia training quality standards, informing the design and delivery of training in different settings.40
Three of the training programmes mentioned by participants provide extensive guidance on styles of communicating and interacting with people living with dementia.
DCM,37 as noted above, is based on the work of Kitwood and his colleagues at Bradford University. It is an evidence-based monitoring tool that assesses the features associated with both ill-being and wellbeing within a setting. As part of the program guidance is given about how to improve the wellbeing and reduce ill-being of people living with dementia.
PAC, the Positive Approaches to Care program41 was developed by the American occupational therapist Teepa Snow. It is a comprehensive training package that has an emphasis on care delivery and styles of interaction.
CAIT, Communication and Interaction Training,23,42 is a programme developed for the management of agitation. It emphasises the importance of carer micro-skills in the day-to-day communication skills of carers. It is the only framework mentioned that incorporates the Positive Behavioural Support arousal graph as part of its training programme.
These training frameworks are relevant because the workshop participants highlighted the need to employ effective carer communication and good interpersonal skills across all three phases of agitation. These interpersonal aspects are the features referred to as micro-skills. Thompson and colleagues discuss the use of micro-skills in relation to agitation.32 In their article, they highlight the role of micro-skills in delivering person-centred care, and also how the skills can be used as de-escalation strategies. Via a case study, Thompson describes how carers employ effective body language, appropriate physical contact, and banter to de-escalate a potentially violent situation on an inpatient unit. The workshop participants in the present study acknowledged the importance of such subtle skills, suggesting it was important for the carers to maintain “good relationships” with people living with dementia.
In terms of the phases, while there was overlap between the three phases, in the de-escalation stage some highly specific techniques were suggested to reduce levels of emotion (eg, BANGS, Therapeutic lies). Therapeutic lying is a controversial topic, and is acceptable only when certain criteria are met.43 However, it sometimes may be required in order to de-escalate scenarios when the person living with dementia’s incorrect perception of the situation should not be challenged. In such situations, it may be preferable to “go-along” with the person’s incorrect assumption (eg, her deceased partner is still alive). In contrast, BANGS, developed by a family carer,44 is a set of instructions for avoiding confrontation and reducing the degree of emotionality in a potentially difficult exchange. For example, in a situation where a carer is being accused of stealing the person’s purse, the carer can avoid getting into a confrontation by: “Breathing to centre themselves, Agree with the person’s accusation, Never argue, Go with the flow (look for the purse), Say Sorry”.42
In the third phase (dealing with high levels of agitation), participants were concerned with maintaining safety in the presence of risk. The participants suggested that carers are taught techniques involving control and restraint, forced care and the “Prevention and Management of Violence and Aggression” (PMVA). Crooks and colleagues45 recently provided a useful paper, containing a case study, which discusses the use of PMVA for people displaying agitation. The article provides an example of a care plan, and also discusses some of the legal frameworks concerning this level of management.
The current project highlights the complex and dynamic nature of managing agitation. It is suggested that the distinction between macro-features and micro-skills is helpful. Indeed, macro-features usefully specify the types of structural interventions that are valuable in the field – use of biopsychosocial models, specific therapies, DCM and other training programmes. However, it is also important to understand the crucial role played by the processes and mechanics of how these features are delivered through micro-skills. The micro-skills are also crucial independently of the macro-structures, because they represent the moment-to-moment exchanges between the carers and people living with dementia which can help manage behaviour. Thompson et al’s article32 highlights the role of banter, good body language, etc. in relation to both preventative and de-escalation strategies. They also make the point that carers are often unable to recognise and articulate these skills. This lack of “dementia care literacy” is detrimental within the field. Indeed, it is suggested that if carers were able to develop a conscious awareness of their skills, this would allow them to pass on their competencies to others, having better dialogues with management, and boosting their self-esteem.35
The concept of micro-skills provides a framework in which we can recognise, describe and therefore teach others this important set of skills that is integral to the delivery of good dementia care.
A limitation of the study is that participants were provided with highly structured response sheets, which mirrored the PBS arousal framework. Hence, there is the danger of a confirmation bias, with responses being limited to concepts that fulfilled the researchers’ preconceived ideas. However, the questionnaire was a product of a series of interviews and surveys from a larger programme of work conducted previously on the management of behaviours that challenge,46 and the arousal graph had been shown to be useful in this context. Hence, the current study was specifically designed to examine how participants populated the different phases of the arousal framework. Another potential caution is that participants were asked in very general terms to describe strategies and so they may have generated more macro-features than micro skills.
Conclusions
The Positive Behaviour Support framework was found to be helpful in linking non-drug interventions to arousal levels in agitated behaviours. This is the first empirical study in the area of dementia to make such links. The framework identified three phases requiring interventions – the preventative phase; trigger and escalation; and the high agitation and risky phase.
The study also examined the notion of macro-features and micro-skills. Macro-features are the structural elements of the interventions (formulations, specific types of therapy, care plan, measures, charts, etc.). In contrast, the micro-skills are the communication skills used in the moment-to-moment interactions with people living with dementia (use of humour, banter, good pacing, non-verbals, etc.). It is evident that both of these features are required, relevant, and inter-related. For example, it is argued that the micro-skills are frequently the means by which the goals of the macro-features are delivered (ie, what a camera would capture during the delivery of a therapy, technique, formulation or care plan).
Overall, this study has provided precise advice regarding the micro and macro skills required in the management of distress and agitation in dementia care. A clear template has been presented to enable clinicians to better structure their interventions in line with the level of arousal being displayed by people living with dementia. The findings from this project are thought to be sufficiently important to be included in the forthcoming British Psychological Society’s guidance regarding the non-pharmacological management of behaviours that challenge.46
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rabins PV, Blacker D, Rovner BW., et al.; APA Work Group on Alzheimer’s Disease and other Dementia. American Psychiatric Association practice guideline for the treatment of patients with Alzheimer’s disease and other dementias. Am J Psychiatry. 2007;164(12 Suppl):5–56.
2. NICE. Dementia: assessment, management and support for people living with dementia and their carer. 2018; NG97. Available from: www.nice.org.uk/guidance/ng97.
3. Ma H, Lu X, Zhou A, et al. Clinical practice guidelines for the management of behavioral and psychological symptoms of dementia: a systematic review with AGREE II. Front Neurol. 2022;13:799723. doi:10.3389/fneur.2022.799723
4. Gray K, Moniz-Cook E, Reichelt FK, James IA, James IA. Professional perspectives on applying the NICE and British Psychological Society Guidelines for the management of Behaviours that Challenge in dementia care: an e-survey. Br J Clin Psychol. 2021;61(1):112–131. doi:10.1111/bjc.12316
5. Dyer S, Harrison S, Laver K, Whitehead C, Crotty M. An overview of systematic reviews of pharmacological and non-pharmacological interventions for the treatment of behavioral and psychological symptoms of dementia. Int Psychogeriatr. 2018;30(3):295–309. doi:10.1017/S1041610217002344
6. Holle D, Halek M, Holle B, Pinkert C. Individualized formulation-led interventions for analyzing and managing challenging behavior of people with dementia – an integrative review. Aging Ment Health. 2016;21:1229–1247. doi:10.1080/13607863.2016.1247429
7. James I, Gray K, Moniz-Cook E, Lee K, Reichelt K, Richardson J. Behavioural and psychological symptoms of dementia: a new framework for holistic understanding and nonpharmacological management. Br J Psychiatry Advan. 2021. doi:10.1192/bja.2021.12
8. Moniz-Cook ED, Swift K, James I, Malouf R, De Vugt M, Verhey F. Functional analysis-based interventions for challenging behaviour in dementia. Cochrane Database Sys Rev. 2012;2:CD006929.
9. McKenna M, Brown LJ, Berry K. Formulation‐led care in care homes: staff perspectives on this psychological approach to managing behaviour in dementia care. Int J Older People Nurs. 2022;17:e12465. doi:10.1111/opn.12465
10. James IA, Jackman L. Understanding Behaviour in Dementia That Challenges: A Guide to Assessment and Treatment.
11. Wolverson E, Birtles H, Moniz-Cook E, James IA, Brooker D, Duffy F. Naming and framing the Behavioural and Psychological Symptoms of Dementia (BPSD) paradigm: professional stakeholder perspectives. OBM Geriatrics. 2019;3(4):19. doi:10.21926/obm.geriatr.1904080
12. Cunningham C, Macfarlane S, Brodaty H. Language paradigms when behaviour changes with dementia: banBPSD. Int J Geriatr Psychiatr. 2019;34(8):1109–1113. doi:10.1002/gps.5122
13. Wolverson E, Dunn R, Moniz‐Cook E, Gove D, Diaz‐Ponce A. The language of behaviour changes in dementia: a mixed methods survey exploring the perspectives of people with dementia. J Ad Nurs. 2021;77(4):992–2001.
14. Wolverson E, Moniz-Cook E, Dunn R, Dunning R. Family carer perspectives on the language of behaviour change in dementia: an online mixed methods survey. Age Ageing. 2022;51(3):afac047. doi:10.1093/ageing/afac047
15. Cohen-Mansfield J. Conceptualization of agitation: results based on the Cohen-Mansfield Agitation Inventory and the Agitation Behavior Mapping Instrument. Int Psychogeriatr. 1997;8(S3):309–315. doi:10.1017/S1041610297003530
16. Cohen-Mansfield J, Marx MS, Rosenthal AS. A description of agitation in a nursing home. J Gerontol. 1989;44:M77–M84. doi:10.1093/geronj/44.3.M77
17. Panca M, Livingston G, Barber J, et al. Healthcare resource utilisation and costs of agitation in people with dementia living in care homes in England - The Managing Agitation and Raising QUality of LifE in dementia (MARQUE) study. PLoS One. 2019;14:e0211953. doi:10.1371/journal.pone.0211953
18. Gola AB, Morris S, Candy B, et al. Healthcare utilization and monetary costs associated with agitation in UK care home residents with advanced dementia: a prospective cohort study. Int Psychogeriatr. 2020;32(3):359–370. doi:10.1017/S1041610219002059
19. Costa N, Wübker A, De Mauléon A, et al. Costs of care of agitation associated with dementia in 8 European countries: results from the RightTimePlaceCare study. J American Med Assoc. 2018;19(1):95–e1.
20. Cloutier M, Gauthier-Loiselle M, Gagnon-Sanschagri P, et al. Institutionalization risk and costs associated with agitation in Alzheimer’s disease. Alzheimer's & Disease:Trans Res Clin Interven. 2019;5:851–861. doi:10.1016/j.trci.2019.10.004
21. Livingston G, Kelly L, Lewis-Holmes E, et al. Non-pharmacological interventions for agitation in dementia: systematic review of randomised controlled trials. The Br J Psychiatry. 2014;205(6):436–442. doi:10.1192/bjp.bp.113.141119
22. Livingston G, Barber J, Marston L, et al. Clinical and cost-effectiveness of the managing agitation and raising quality of life (MARQUE) intervention for agitation in people with dementia in care homes: a single-blind, cluster-randomised controlled trial. Lancet Psychiatry. 2019;6(4):293–304. doi:10.1016/S2215-0366(19)30045-8
23. James IA. The use of CBT in dementia care: a rationale for Communication and Interaction Therapy (CAIT) and therapeutic lies. Cogn Behav Therapist. 2015;8. doi:10.1017/S1754470X15000185
24. O’Brien R, Goldberg SE, Pilnick A, et al. The VOICE study – a before and after study of a dementia communication skills training course. PLoS One. 2018;13(6):e0198567. doi:10.1371/journal.pone.0198567
25. Harwood RH, O’Brien R, Goldberg SE, et al. A staff training intervention to improve communication between people living with dementia and health-care professionals in hospital: the VOICE mixed-methods development and evaluation study. Health Serv Deliv Res. 2018;6:41. doi:10.3310/hsdr06410
26. Torossian MR. (2021) The dignity of older individuals with Alzheimer’s disease and related dementias: a scoping review. Dementia. 2021;20(8):2891–2915. doi:10.1177/14713012211021722
27. James IA, Hope A. Relevance of emotions and beliefs in the treatment of behaviors that challenge in dementia patients. Neurodegener Dis Manag. 2013;3(6):575–588. doi:10.2217/nmt.13.60
28. Kverno KS, Black BS, Nolan M, Rabins PV. Research on treating neuropsychiatric symptoms of advanced dementia with non-pharmacological strategies, 1998–2008: a systematic literature review. Int Psychogeriatr. 2009;21(5):825–843. doi:10.1017/S1041610209990196
29. Hallett N, Dickens GL. De-escalation of aggressive behaviour in healthcare settings: concept analysis. Int J Nurs Studies. 2017;75:10–20. doi:10.1016/j.ijnurstu.2017.07.003
30. O’Connor CMC, Mioshi E, Kaizik C, Fisher A, Hornberger M, Piguet O. Positive behaviour support in frontotemporal dementia: a pilot study. Neuropsychol Rehab. 2021;31(4):507–530. doi:10.1080/09602011.2019.1707099
31. Fisher AC, Cheung SC, O’Connor CMC, Piguet O. The Acceptability and usefulness of Positive Behaviour Support education for family carers of people with frontotemporal dementia: a pilot study. J Geriatr Psychiatry and Neurol. 2022;37(12). doi:10.1177/08919887221090214
32. Thompson D, Shirley L, Gray K, James IA. New perspectives on the management of behavioural & emotional expressions of need: the micro-skills involved in de-escalating agitation. J Dement Care. 2022;30(2):22–23.
33. Vasse E, Vernooij M, Spijker A, Olde Rikkert M, Koopmans R. A systematic review of communication strategies for people with dementia in residential and nursing homes. Int Psychogeriatr. 2010;22(2):189–200. doi:10.1017/S1041610209990615
34. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
35. James I, Randall C, Reichelt K. Thirty-six ways to de-escalate ‘behaviour that challenge’: helping carers know what they already know by improving ‘dementia care literacy’. J Dement Care. 2022;30(5):29–33.
36. Kitwood T. Dementia Reconsidered: The Person Comes First. Buckingham: Open University Press; 1997.
37. Bradford Dementia Group. Dementia Care Mapping 8 User’s Manual. The DCM Method, University of Bradford; 2005.
38. Fossey J, Ballard C, Juczak E, et al. Effect of enhanced psychosocial care on antipsychotic use in nursing home residents with severe dementia: a cluster randomised trial. Br Med J. 2006;332:756–758. doi:10.1136/bmj.38782.575868.7C
39. James I, Mahesh M, Duffy F, Reichelt K, Moniz-Cook E. UK clinicians’ views on the use of formulations for the management of BPSD: a multidisciplinary survey. Ageing Ment Health. 2020;25(12):2347–2354. doi:10.1080/13607863.2020.1830944
40. Surr C, Gates C. What works in delivering dementia education or training to hospital staff? A synthesis of the evidence. Int J Nurs Studies. 2017;75:172–188. doi:10.1016/j.ijnurstu.2017.08.002
41. Ehlman M, Nimkar S, Nolan B, Thomas P, Caballero C, Snow T. Health worker’s knowledge and perceptions of dementia in skilled nursing homes: a pilot implementation of Teepa Snow’s positive approach to care certification course. J Contin Educ Health Profess. 2018;38(3):190–197. doi:10.1097/CEH.0000000000000216
42. James IA, Gibbons L. Communication Skills for Effective Dementia Care. London: Jessica Kingsley; 2019.
43. Culley H, Barber R, Hope A, James IA. Therapeutic lying in dementia care. Nurs Standard. 2013;28(1):35–39. doi:10.7748/ns2013.09.28.1.35.e7749
44. McCaulay S (2015). B is for Breathe in BANGS. Available from http://myalzheimersstory.com/2015/06/18/b-is-for-breathe-in-bangs.
45. Crooks M, Smith K, Bell L, James IA. Restraints and restrictive interventions during essential personal care in elderly people living with dementia in care homes. Neuropsychiatr Dis J. 2021;15(2):26–38. doi:10.9734/indj/2021/v15i230150
46. James IA, Moniz-Cook E, Duffy F. Editorial of Special Edition on Behaviours that Challenge. Psychol Older People. 2019;148:3–5. doi:10.53841/bpsfpop.2019.1.148.3
47. Edgar F. Mnemonic techniques: how to CEASE stress and distress. J Dement Care. 2017;25(5):32–34.
48. Duffy F. CLEAR Dementia Care © A Model to Assess and Address Unmet Need. Jessica Kingsley Publishers; 2019.
49. Ballard C, Orrell M, Moniz-Cook E, et al. Improving mental health and reducing antipsychotic use in people with dementia in care homes: the WHELD research programme including two RCTs. Programme Grants Appl Res. 2020;8(6). doi:10.3310/pgfar08060
50. Blackhall A, Hawkes D, Hingley D, Wood S. VERA framework: communication with people who have dementia. Nurs Standard. 2021;26(100):35–39. doi:10.7748/ns.26.10.35.s49
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.