")
Back to Journals » Journal of Blood Medicine » Volume 12
Management of Adult Patients with Immune Thrombocytopenia (ITP): A Review on Current Guidance and Experience from Clinical Practice
Authors Song F, Al-Samkari H
Received 18 March 2021
Accepted for publication 12 July 2021
Published 26 July 2021 Volume 2021:12 Pages 653—664
DOI https://doi.org/10.2147/JBM.S259101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Fei Song,1,2 Hanny Al-Samkari2,3
1Department of Medicine, Massachusetts General Hospital, Boston, MA, USA; 2Harvard Medical School, Boston, MA, USA; 3Division of Hematology, Massachusetts General Hospital, Boston, MA, USA
Correspondence: Hanny Al-Samkari
Division of Hematology, Massachusetts General Hospital, Suite 118, Room 112, Zero Emerson Place, Boston, MA, 02114, USA
Tel +617-643-6214
Fax +617-643-8840
Email [email protected]
Abstract: Immune thrombocytopenia (ITP) is an autoimmune process resulting in increased destruction and inadequate production of platelets that can result in bleeding, fatigue, and reduced health-related quality of life. While treatment is not required for many patients with ITP, the occurrence of bleeding manifestations, severe thrombocytopenia, and requirement for invasive procedures are among the reasons necessitating initiation of therapy. Corticosteroids, intravenous immunoglobulin, and anti-RhD immune globulin are typical first-line and rescue treatments, but these agents typically do not result in a durable remission in adult patients. Most patients requiring treatment therefore require subsequent line therapies, such as thrombopoietin receptor agonists (TPO-RAs), rituximab, fostamatinib, splenectomy, or a number of other immunosuppressive agents. In this focused review, we discuss management of adult ITP in the acute and chronic settings.
Keywords: platelets, immune thrombocytopenia, ITP, treatment, corticosteroids, IVIG, splenectomy, thrombopoietin receptor agonist, rituximab, fostamatinib
Introduction
Immune thrombocytopenia (ITP) results from autoimmune destruction of platelets in the reticuloendothelial system due to platelet autoantibodies and other immune mechanisms, resulting in increased platelet turnover as well as inadequate platelet production.1–5 Primary ITP is defined as an isolated thrombocytopenia <100 × 109/L in the absence of other causes or disorders that may be associated with thrombocytopenia, as distinguished from secondary ITP, which is associated with other conditions such as infections, drug effects, rheumatological diseases, or lymphoproliferative disorders.6,7 The incidence of ITP in the US population is approximately 6.1 per 100,000 persons per year, or 13.7 per 100,000 persons per year in those 65 years or greater, and results in significant economic burden.8 Clinical presentation can vary between asymptomatic to severe bleeding complications, and prior to 2010, fatal bleeding rates were estimated at 1.62–3.89 cases per 100 patient-years and predicted 5-year mortality rates varied from 2.2% for persons <40 years up to 47.8% for those aged >60 years.9 Although many laboratory studies can support diagnosis or guide treatment selection, ultimately diagnosis is clinical, after ruling out other etiologies of thrombocytopenia.7,10,11
Given the wide variation in presentation, not all patients require treatment immediately after diagnosis. The American Society of Hematology (ASH) Immune Thrombocytopenia Clinical Guideline provides a grading system for severity of ITP, defining severe ITP as clinical bleeding requiring treatment.7 Of note, the degree of thrombocytopenia is not reliably indicative of bleeding risk when platelets are above 10 × 109/L.12–15 Factors thought to increase risks of bleeding include reduced platelet count, female sex, and exposure to NSAIDs.16 There is also concern of increased frequency of intracranial hemorrhage in elderly patients aged ≥70 years when platelets are less than 20–30 × 109/L, so clinicians should also consider age when deciding on a threshold for treatment.17 The goal of treatment of ITP is to reduce bleeding risks by raising platelet counts. Treatment must be individualized, accounting for an individual patient’s risks of bleeding given their history of bleeding, trauma risks, and the risk of adverse events from therapeutics.
In this focused review article, we will discuss the treatment of adult ITP, incorporating the most recent evidence as well as expert opinion.
Treatment of ITP
Response Criteria
The International Working Group (IWG) defines complete response (CR) to ITP treatment as a platelet count ≥100 x 109/L and absence of bleeding and response (R) as platelet count ≥ 30 x 109/L and >2 fold increase in platelet count from baseline and absence of bleeding, both measured on 2 occasions greater than 7 days apart.6 No response (NR), per the IWG definition, is characterized by a platelet count <30 x 109/L or a less than 2-fold increase in platelet count from baseline, or the presence of bleeding.6
First-Line/Rescue Treatments
Corticosteroids
The standard first-line treatment and most common rescue therapy in newly diagnosed ITP are corticosteroids, often with prednisone (0.5–2 mg/kg daily for a 4–8 week tapering course) or high-dose dexamethasone (40 mg daily for 4 days for 1–4 cycles).7,10,18 Corticosteroids have been shown to decrease capillary permeability, reduce platelet autoantibody production, increase platelet production, increase myeloid-derived suppressor cells, and change T cell subsets to decrease platelet destruction.19–24
Overall, the choice of corticosteroid agent should be made in consideration of adverse event risk and the need for a rapid response. In a meta-analysis comparing prednisone with dexamethasone in previously untreated adult primary ITP, one to three courses of high dose dexamethasone, compared with prednisone 1 mg/kg for 4 weeks with taper, showed a platelet count response (79% vs 58%) at 14 days, but there was no difference in overall platelet response at 6 months (54% vs 53%) or rates of sustained response.25 High-dose dexamethasone may be more likely to precipitate acute psychotic complications in the elderly or those with a history of psychiatric disease, however, and this should be considered upon agent selection.
Intravenous Immunoglobulin (IVIG) and Intravenous Anti-RhD Immune Globulin
Intravenous immunoglobulin (IVIG) is another common first-line or rescue therapy often employed when a patient presents with significant bleeding. It can be administered when a more rapid increase in platelet count is required, and also be added to corticosteroid therapy or when corticosteroids are contraindicated.7 IVIG is recommended to be given at a dose of 1 g/kg daily for 1–2 days (high-dose) or 0.4 g/kg daily for up to 5 days (low-dose).10 IVIG has many complex mechanisms of action in decreasing inflammatory processes by multiple pathways, including inhibition of the IgG Fc receptor, which is crucial to link the adaptive and innate immune systems, inhibiting phagocytosis and suppression and/or elimination of platelet autoantibodies.26–30
In one meta-analysis, effect rate, time of cessation of bleeding, and rate of development of chronic ITP was not statistically different between high-dose and low-dose IVIG for acute ITP and low-dose IVIG was associated with decreased risk of side effects.31 In a case-control study by Zhou et al., there was no difference in therapeutic response in groups receiving IVIG doses between 0.2–0.4 g/kg/day, which suggests that ITP patients could be treated more cost-effectively by lower conventional dosages of IVIG.32
Intravenous anti-RhD immune globulin (administered at a dose of 50 mcg/kg to 75 mcg/kg daily)33,34 is an alternative to IVIG for non-splenectomized, Rh (+) patients. It is thought to saturate macrophage Fc receptors with anti-D coated RBCs to prevent destruction of autoantibody-coated platelets.35 In one study, IVIG and IV anti-RhD immune globulin treatments of patients with ITP yielded no statistical difference in cumulative response and remission rates.36 Anti-RhD immune globulin induces a controlled hemolysis, with a majority of patients experiencing a decrease in hemoglobin concentration of 0.5–2.0 g/dL 3–7 days after infusion, with recovery to baseline within 3 weeks of administration.37 Rarely, this hemolysis can degenerate into life-threatening disseminated intravascular coagulation.
Second/Subsequent Line Therapies
An estimated 68% of adult patients develop persistent ITP despite first-line treatments including corticosteroids and IVIG.38 There are no randomized controlled trials directly comparing the different second-line therapy options, so the results of placebo-controlled trials of second-line therapy are examined. The choice of second-line therapy is primarily based on patient values and priorities as well as available resources.
Based on the available data, the most recent American Society of Hematology ITP clinical guidelines conditionally recommend TPO-RA rather than rituximab and rituximab is recommended over splenectomy, though choice of treatment should be individualized, e.g. depending on patient goals of avoidance of surgery, achieving durable response, or avoidance of long-term medications.39
Splenectomy
Splenectomy is an effective treatment as the spleen is a site of platelet destruction as well as a site of antibody production. Splenectomy has been shown to help 74% of patients achieve sustained CR lasting more than 6 months40 and 64% after a minimum of 5 years.41 Previous studies have shown that mortality was 1.0% (48 of 4955 patients) with laparotomy and 0.2% (3 of 1301 patients) with laparoscopy.42 Splenectomy also increases infection risk as well, with reports of sepsis in 2.1% of splenectomized patients43 as well as a 2-4-fold risk of venous thromboembolism.44,45 Given risks of the surgery and potential for spontaneous remission of ITP within the first year, splenectomy as a treatment option should be deferred until the patient is confirmed to have chronic ITP (ITP lasting for more than 12 months), when the rate of spontaneous remission is much lower.
Rituximab
Rituximab is a monoclonal anti-CD20 antibody that decreases anti-platelet antibody production by B cells and has been an off-label treatment for ITP for many years. Overall response rates of 40–70% were seen in patients given four weekly doses of 375 mg/m2 of rituximab, though remission is rarely sustained, decreasing to only 21% at 5 years.46–49 Despite the relapse rate, patients treated with rituximab had a longer duration of response compared with placebo (median 8.2 months vs 1.8 months).50 Studies examining different dosages of rituximab, including a lower dose of 100 mg/week for four weeks51 and a dose of 1000 mg on days 1 and 15 did not show significant differences in response rate or infection risks.52,53 Rituximab has also been studied in combination with other therapies such as high-dose dexamethasone in newly diagnosed ITP, with an initial strong overall response though sustained response after 12 months of follow up decreased to 61.5%, with an 11.1% incidence of adverse effects.54 In a meta-analysis of randomized controlled trials, rituximab plus standard of care was shown to have a higher complete response rate (46.8% vs 32.5%) by 6 months than standard of care alone.48 Infection is an important safety concern of rituximab: in a large ITP patient registry, the incidence of infection was 23.8% after 34 months, with 8.5% being severe (grade III to IV) infections.46 Some clinicians use anti-infective prophylaxis for patients undergoing rituximab treatment, though evidence to support its use is lacking.55 Given the ongoing COVID-19 pandemic, clinicians also must take into consideration the B-cell depletion effect of rituximab, which may impair vaccine response for at least 6 months after administration.56
Thrombopoietin Receptor Agonists
Thrombopoietin receptor agonists (TPO-RA) mimic endogenous TPO function to increase megakaryocyte maturation and platelet production.57 In a large systematic review, treatment failure was seen in 21% of TPO-RA treated patients compared with 47% of control patients, with a lower risk of significant bleeding and all-cause mortality.58 There are currently three TPO-RAs approved for treatment of ITP: romiplostim, eltrombopag, avatrombopag, described below and summarized in Table 1.59 Thrombosis is the major potential adverse event of concern with TPO-RA use and though clinical trials have not found an increased thrombotic risk of TPO-RA agents compared with placebo, uncontrolled observational data suggest an increase in thrombotic risk on the order of 2-3-fold.60
 |
Table 1 Phase III Trials of TPO-RAs in ITP |
Romiplostim is a peptide TPO-RA approved by the US FDA for ITP following the failure of a first-line treatment and is administered subcutaneously on a weekly schedule, starting at 1 mcg/kg, increased weekly to a maximum dose of 10 mcg/kg until platelet count is consistently 50–200 × 109/L.61 In two parallel phase III trials, durable platelet response was achieved in 38–56% of patients with overall platelet response rate of 79–88% in patients given romiplostim, with platelet counts to ≥50 × 109/L for 13.8 weeks, compared with 0.8 weeks in the placebo group.62 In another open-label study, comparing romiplostim to the medical standard of care in patients without history of splenectomy, patients who received romiplostim were 2.3 times as likely to have a platelet response as those who received the standard of care (71–92% patients who received romiplostim had a platelet response, compared with 51% in the standard of care group).63 Though romiplostim does not have the ease of administration as oral TPO-RAs, a recent study has found that self-administration of romiplostim by patients did not increase adverse events compared with administration by healthcare professionals.64,65
Eltrombopag is a small molecule TPO-RA approved by the US FDA for ITP following the failure of a first-line treatment and is initiated orally at a dose of 50 mg daily in adults (or 25 mg daily in patients of East Asian descent), titrated to a maximum dose of 75 mg daily to reach a goal platelet count of 50–200 x 109/L.66 Multiple studies have found eltrombopag significantly increases platelet response (59–79%) with less bleeding (statistically significant OR 0.49) and reduced use of concomitant ITP treatment.67,68 Ethnic differences in eltrombopag were noted in patients of East Asian descent, with about 60% responding to a 12.5 mg or 25 mg daily dose.69,70 Commonly reported adverse effects of eltrombopag include hepatotoxicity (11%), headache (2.9%), diarrhea, and upper respiratory tract infection.68–71 A disadvantage of eltrombopag is the dietary restrictions (avoidance of dietary fat and divalent cations, such as calcium and magnesium in food) for a 4–6 hour window around taking the medication to prevent dietary and medication interference with adequate absorption.72,73 Given the half-life of 26–35 hours,74 one method proposed to address this is alternative intermittent dosing of eltrombopag less frequently than once daily, which has been shown to be effective in observational data.75
Avatrombopag is small molecule oral TPO receptor agonist approved for chronic ITP in adults as well as patients with liver disease scheduled to undergo a procedure. In ITP, it is initiated at a dose of 20 mg daily76 titrated to a maximum dose of 40 mg daily to achieve a goal platelet count of 50–200 x 109/L. Unlike eltrombopag, avatrombopag does not require strict dietary restrictions for a 4–6 hour window around when it is taken. Also, it does not have a known signal for hepatotoxicity, nor does it require dose adjustment for the race of the patient. In a phase II double-blind randomized controlled trial in patients with persistent and chronic ITP who failed or relapsed after prior therapy, 75% of patients receiving avatrombopag had an overall response, with the drug overall well-tolerated (common adverse events included fatigue and headache).77 In a phase III study, avatrombopag was superior to placebo in mean cumulative number of weeks with platelet count ≥50 x 109/L during a 6-month treatment period with higher rates of reduced concomitant ITP medication use and durable response compared with placebo. In a post hoc analysis of the 2018 phase III study, avatrombopag was shown to have higher rates of platelet response and complete response in the first 6 months and a reduction in chronic corticosteroid use.78,79 In addition to treatment of ITP, avatrombopag has also been studied extensively in patients with liver disease and has shown to be efficacious in the peri-procedural setting in patients with thrombocytopenia of chronic liver disease.80–83
A fourth TPO-RA, lusutrombopag, is also a small molecule oral TPO-RA, approved for thrombocytopenia due to chronic liver disease prior to an invasive procedure.84 Its effect in ITP has not yet been well studied. A phase II study of lusutrombopag in ITP was recently terminated early due to results suggesting a higher dose was necessary to elicit an efficacy effect.
Thus far, there have not been any head-to-head randomized controlled trials completed comparing TPO-RAs. The relative potency of these agents is a topic of interest.85 In a single center retrospective comparison of romiplostim and eltrombopag, there was no significant difference in platelet responses or tolerability.86 One meta-analysis of nine randomized placebo-controlled trials showed no significant difference in overall response rate, bleeding incidence, incidence of adverse events, or durable response.87 In a systematic review of 18 retrospective studies, the response rate after switching from one TPO-RA agent to another due to lack of efficacy, adverse events, or patient preference was 77.5%.74
There have been no formal guidelines regarding the discontinuation or tapering of TPO-RAs.88 In a single-center observational study of patients who discontinued TPO-RAs, the 2-year treatment-free remission rate was 66.4% with 46% cumulative incidence of loss of complete response, but there was no clear predictive factor for sustained response.89 In a meta-analysis, the incidence of remission after TPO-RA discontinuation ranged from 5–36%.58 Tapering of TPO-RAs is dependent on multiple factors, including platelet count at or above the lower limit of normal, lack of a major bleeding history, low trauma risk, and taking into account antiplatelet or anticoagulant agents the patient is taking.90 In an expert consensus panel, the duration of ITP, duration on TPO-RA, and timing of platelet response did not affect the panel’s recommendations regarding discontinuation.90 A recent phase II study of sustained remission off treatment after discontinuation from TPO-RAs found that 25% of responders were able to maintain the response during 6 months after tapering from eltrombopag.91 This study also reviewed biomarkers including TPO levels, which did not have a significant association with response or with sustained remission, and IL-10, IL-4, and TNF-α, each of which had negative predictive response. Other studies have found that TPO levels can predict response to TPO-RAs.92 More research is needed to identify predictive factors that might be able to guide the tapering of TPO-RAs.
Fostamatinib
Fostamatinib is a spleen tyrosine kinase inhibitor which inhibits the inflammatory response and clearance of auto-antibody coated platelets by the reticuloendothelial system.93 It was approved for ITP after the failure of other therapies at an initial dose of 100 mg twice daily, with uptitration to 150 mg twice daily for an inadequate response. Two phase III randomized placebo-controlled trials of fostamatinib in patients with persistent/chronic ITP showed an overall response in 43% of patients on fostamatinib with a median time to response of 15 days.94 In the follow-up, open-label extension study, responses appeared durable, with 44% of patients achieving an overall response for a median of >28 months.95 In this study, most adverse events were mild to moderate, with the most common events including diarrhea, hypertension, nausea, epistaxis, and transaminase elevation.95
Therapies Currently Under Investigation
There is ongoing research involving Bruton’s tyrosine kinase inhibitors in the potential treatment of immune-related diseases.96 Rilzabrutinib is an oral, reversible small molecule selective BTK inhibitor that has shown preclinical efficacy in rapidly inhibiting antibody mediated innate immune response as well as antibody production, exhibiting potential for ITP treatment.96 Rilzabrutinib was also shown to be safe and well tolerated in a phase I trial, with favorable pharmacokinetics that could result in fast onset of effect.97
Bortezomib is a proteasome inhibitor that was shown in a preclinical study to improve thrombocytopenia in ITP by inducing apoptosis in long-lived plasma cells which were thought to play a role in corticosteroid resistant ITP.98 Bortezomib has been shown to have success in treatment of relapsing ITP in a case report,99 though further clinical trials are needed.
Salvage Therapies
Other treatments of ITP include immunosuppressants (azathioprine, cyclophosphamide, cyclosporine, mycophenolate mofetil, vinca alkaloids), dapsone and danazol. These agents are typically used after failure of multiple standard second/subsequent-line treatment options. A brief summary of these therapies can be found in Table 2. 11 The management of patients with refractory ITP is discussed in more detail elsewhere.100–102
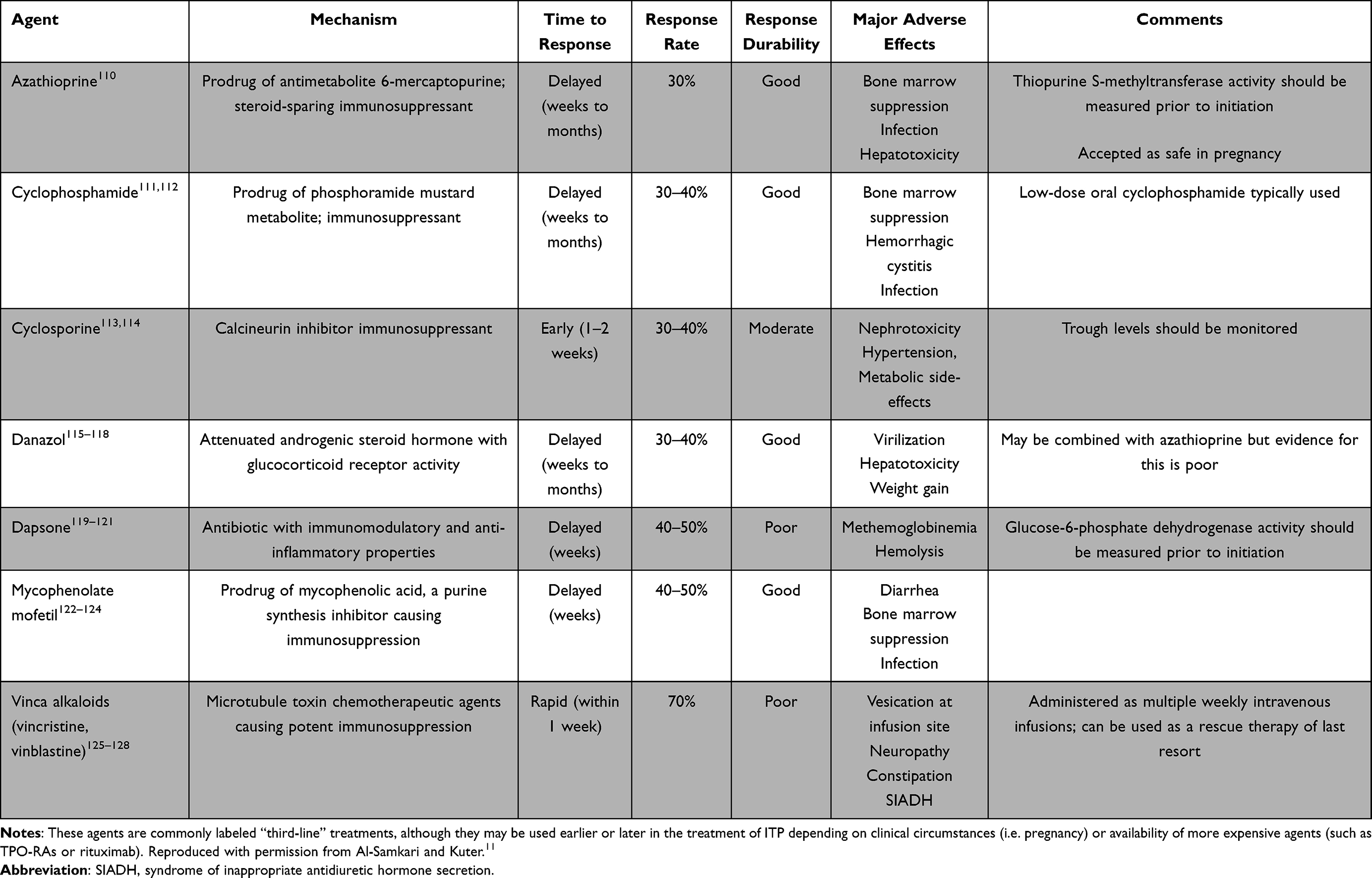 |
Table 2 Other Agents for Use in the Subsequent Treatment Setting in ITP |
Special Considerations in ITP Management
Bleeding Emergencies in ITP
Management of bleeding emergencies in ITP is an important topic which requires further study. In the Updated International Consensus Report, Provan et al. provides a review of recommendations for treatment of life-threatening hemorrhage due to ITP.88 Recommendations incorporate general supportive care with a combination of treatments, including IV corticosteroids, IVIG, and platelet transfusions in order to increase platelet count rapidly, and in the absence of significant response, the early addition of a TPO-RA should also be considered.88 Ultimately, aggressive management to provide for a rise in the platelet count which often incorporates the use of multiple agents simultaneously without waiting for a single agent to be effective is appropriate. When TPO-RAs are used, they may be dosed more aggressively (e.g. romiplostim 5–10 mcg/kg to start). This is done with recognition of a potential thrombocytosis risk but with the understanding that the risk of ongoing severe thrombocytopenia and worsened bleeding is greater and requires urgent mitigation.
ITP in Pregnancy
Pregnancy complications in the setting of ITP include maternal hemorrhage, fetal loss, low birth weight, and may be treated to maintain a platelet level in the mother (≥30 × 109/L until close to term), with the goal then adjusted based on delivery procedures.10,103,104 Recommended treatments include corticosteroids or IVIG, or a combination.105 In the event that both modalities fail, TPO-RAs can be considered as a salvage therapy in severe cases, on the basis of limited observational data. One multicenter observational study of 15 pregnant women showed a response rate of 77% to TPO-RA (romiplostim or eltrombopag) though mostly in combination with concomitant ITP therapy.106 And while this study showed no thromboembolic events and aside from one case of neonatal thrombosis, no other fetal complications,106 more information is needed about other therapies in pregnancy. The management of pregnant patients is discussed in more detail in a review by Gernsheimer et al.107
Conclusions and Future Directions
Modern treatment of ITP in adults involves a number of tried and true first-line therapies, primarily corticosteroids and IVIG, as well as newer therapies in the TPO-RAs and fostamatinib. Though there are many more options for the management of ITP at present than in even the relatively recent past, there remains unmet need in this disease. Thankfully, additional therapies are under development for ITP, including inhibitors of the Bruton tyrosine kinase (e.g. rilzabrutinib), complement inhibitory therapies (e.g. sutimlimab), neonatal Fc receptor antagonists (e.g. rozanolixizumab, efgartigimod), and others. Management of chronic ITP may involve cycling through multiple drug therapies, consideration of splenectomy, and in some patients, reaching for salvage therapies or clinical trials of novel agents. Lastly, bleeding emergencies in ITP require prompt, aggressive management, typically with multiple agents.
Acknowledgments
H. Al-Samkari is the recipient of the Harvard KL2/Catalyst Medical Research Investigator Training Award and the American Society of Hematology Scholar Award.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Dr Hanny Al-Samkari reports consultancy for Agios, Dova, Rigel, Argenx, Sobi, Novartis, and Moderna and research funding from Agios, Dova, Amgen. The authors report no other conflicts of interest in this work.
References
1. Harrington WJ, Minnich V, Hollingsworth JW, et al. Demonstration of a thrombocytopenic factor in the blood of patients with thrombocytopenic purpura. J Lab Clin Med. 1951;38(1):1–10.
2. Shulman NR, Marder VJ, Weinrach RS. Similarities between known antiplatelet antibodies and the factor responsible for thrombocytopenia in idiopathic purpura. Physiologic, serologic and isotopic studies. Ann N Y Acad Sci. 2006;124(2):499–542. doi:10.1111/j.1749-6632.1965.tb18984.x
3. Ballem PJ, Segal GM, Stratton JR, et al. Mechanisms of thrombocytopenia in chronic autoimmune thrombocytopenic purpura. Evidence of both impaired platelet production and increased platelet clearance. J Clin Invest. 1987;80(1):33–40. doi:10.1172/JCI113060
4. Al-Samkari H, Rosovsky RP, Karp Leaf RS, et al. A modern reassessment of glycoprotein-specific direct platelet autoantibody testing in immune thrombocytopenia. Blood Adv. 2020;4(1):9–18. doi:10.1182/bloodadvances.2019000868
5. Cheloff AZ, Kuter DJ, Al-Samkari H. Serum complement levels in immune thrombocytopenia: characterization and relation to clinical features. Res Pract Thromb Haemost. 2020;4(5):807–812. doi:10.1002/rth2.12388
6. Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386–2393. doi:10.1182/blood-2008-07-162503
7. Neunert C, Lim W, Crowther M, et al. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood. 2011;117(16):4190–4207. doi:10.1182/blood-2010-08-302984
8. Weycker D, Hanau A, Hatfield M, et al. Primary immune thrombocytopenia in US clinical practice: incidence and healthcare burden in first 12 months following diagnosis. J Med Econ. 2020;23(2):184–192. doi:10.1080/13696998.2019.1669329
9. Cohen YC, Djulbegovic B, Shamai-Lubovitz O, et al. The bleeding risk and natural history of idiopathic thrombocytopenic purpura in patients with persistent low platelet counts. Arch Intern Med. 2000;160(11):1630–1638. doi:10.1001/archinte.160.11.1630
10. Provan D, Stasi R, Newland AC, et al. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010;115(2):168–186. doi:10.1182/blood-2009-06-225565
11. Al-Samkari H, Kuter DJ. Immune thrombocytopenia in adults: modern approaches to diagnosis and treatment. Semin Thromb Hemost. 2020;46(3):275–288. doi:10.1055/s-0039-1700512
12. Slichter SJ, Harker LA. Thrombocytopenia: mechanisms and management of defects in platelet production. Clin Haematol. 1978;7(3):523–539. doi:10.1016/S0308-2261(21)00047-3
13. Slichter SJ, Kaufman RM, Assmann SF, et al. Dose of prophylactic platelet transfusions and prevention of hemorrhage. N Engl J Med. 2010;362(7):600–613. doi:10.1056/NEJMoa0904084
14. Lacey JV, Penner JA. Management of idiopathic thrombocytopenic purpura in the adult. Semin Thromb Hemost. 2008;3(3):160–174. doi:10.1055/s-0028-1086135
15. Harker LA, Slichter SJ. The bleeding time as a screening test for evaluation of platelet function. N Engl J Med. 1972;287(4):155–159. doi:10.1056/NEJM197207272870401
16. Piel-Julian ML, Mahevas M, Germain J, et al. Risk factors for bleeding, including platelet count threshold, in newly diagnosed immune thrombocytopenia adults. J Thromb Haemost. 2018;16(9):1830–1842. doi:10.1111/jth.14227
17. Hato T, Shimada N, Kurata Y, et al. Risk factors for skin, mucosal, and organ bleeding in adults with primary ITP: a nationwide study in Japan. Blood Adv. 2020;4(8):1648–1655. doi:10.1182/bloodadvances.2020001446
18. McVerry BA. Management of idiopathic thrombocytopenic purpura in adults. Br J Haematol. 1985;59(2):203–208. doi:10.1111/j.1365-2141.1985.tb02985.x
19. Shulman NR, Weinrach RS, Libre EP, et al. The role of the reticuloendothelial system in the pathogenesis of idiopathic thrombocytopenic purpura. Trans Assoc Am Physicians. 1965;78:374–390.
20. Gernsheimer T, Stratton J, Ballem PJ, et al. Mechanisms of response to treatment in autoimmune thrombocytopenic purpura. N Engl J Med. 1989;320(15):974–980. doi:10.1056/NEJM198904133201505
21. Pang SJ, Lazarus AH. Mechanisms of platelet recovery in ITP associated with therapy. Ann Hematol. 2010;89(Suppl 1):31–35. doi:10.1007/s00277-010-0916-2
22. Li J, Wang Z, Hu S, et al. Correction of abnormal T cell subsets by high-dose dexamethasone in patients with chronic idiopathic thrombocytopenic purpura. Immunol Lett. 2013;154(1–2):42–48. doi:10.1016/j.imlet.2013.08.006
23. Hou Y, Feng Q, Xu M, et al. High-dose dexamethasone corrects impaired myeloid-derived suppressor cell function via Ets1 in immune thrombocytopenia. Blood. 2016;127(12):1587–1597. doi:10.1182/blood-2015-10-674531
24. Kitchens CS. Amelioration of endothelial abnormalities by prednisone in experimental thrombocytopenia in the rabbit. J Clin Invest. 1977;60(5):1129–1134. doi:10.1172/JCI108864
25. Mithoowani S, Gregory-Miller K, Goy J, et al. High-dose dexamethasone compared with prednisone for previously untreated primary immune thrombocytopenia: a systematic review and meta-analysis. Lancet Haematol. 2016;3(10):e489–e96. doi:10.1016/S2352-3026(16)30109-0
26. Hansen RJ, Balthasar JP. Mechanisms of IVIG action in immune thrombocytopenic purpura. Clin Lab. 2004;50(3–4):133–140.
27. Crow AR, Lazarus AH. The mechanisms of action of intravenous immunoglobulin and polyclonal anti-d immunoglobulin in the amelioration of immune thrombocytopenic purpura: what do we really know? Transfus Med Rev. 2008;22(2):103–116. doi:10.1016/j.tmrv.2007.12.001
28. Nimmerjahn F, Ravetch JV. Anti-inflammatory actions of intravenous immunoglobulin. Annu Rev Immunol. 2008;26:513–533. doi:10.1146/annurev.immunol.26.021607.090232
29. Brückner C, Lehmann C, Dudziak D, et al. Sweet SIGNs: IgG glycosylation leads the way in IVIG-mediated resolution of inflammation. Int Immunol. 2017;29(11):499–509. doi:10.1093/intimm/dxx053
30. Schwab I, Nimmerjahn F. Intravenous immunoglobulin therapy: how does IgG modulate the immune system? Nat Rev Immunol. 2013;13(3):176–189. doi:10.1038/nri3401
31. Qin YH, Zhou TB, Su LN, et al. The efficacy of different dose intravenous immunoglobulin in treating acute idiopathic thrombocytopenic purpura: a meta-analysis of 13 randomized controlled trials. Blood Coagul Fibrinolysis. 2010;21(8):713–721. doi:10.1097/MBC.0b013e3283401490
32. Zhou Z, Qiao Z, Li H, et al. Different dosages of intravenous immunoglobulin (IVIg) in treating immune thrombocytopenia with long-term follow-up of three years: results of a prospective study including 167 cases. Autoimmunity. 2016;49(1):50–57. doi:10.3109/08916934.2015.1104671
33. Newman GC, Novoa MV, Fodero EM, et al. A dose of 75 microg/kg/d of i.v. anti-D increases the platelet count more rapidly and for a longer period of time than 50 microg/kg/d in adults with immune thrombocytopenic purpura. Br J Haematol. 2001;112(4):1076–1078. doi:10.1046/j.1365-2141.2001.02627.x
34. Tarantino MD, Young G, Bertolone SJ, et al. Single dose of anti-D immune globulin at 75 microg/kg is as effective as intravenous immune globulin at rapidly raising the platelet count in newly diagnosed immune thrombocytopenic purpura in children. J Pediatr. 2006;148(4):489–494. doi:10.1016/j.jpeds.2005.11.019
35. Ware RE, Zimmerman SA. Anti-D: mechanisms of action. Semin Hematol. 1998;35(1Suppl 1):14–22.
36. Rodeghiero F, Schiavotto C, Castaman G, et al. A follow-up study of 49 adult patients with idiopathic thrombocytopenic purpura treated with high-dose immunoglobulins and anti-D immunoglobulins. Haematologica. 1992;77(3):248–252.
37. Scaradavou A, Woo B, Woloski BM, et al. Intravenous anti-D treatment of immune thrombocytopenic purpura: experience in 272 patients. Blood. 1997;89(8):2689–2700. doi:10.1182/blood.V89.8.2689
38. Moulis G, Germain J, Comont T, et al. Newly diagnosed immune thrombocytopenia adults: clinical epidemiology, exposure to treatments, and evolution. Results of the CARMEN multicenter prospective cohort. Am J Hematol. 2017;92(6):493–500. doi:10.1002/ajh.24702
39. Neunert C, Terrell DR, Arnold DM, et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23):3829–3866. doi:10.1182/bloodadvances.2019000966
40. Stasi R, Stipa E, Masi M, et al. Long-term observation of 208 adults with chronic idiopathic thrombocytopenic purpura. Am J Med. 1995;98(5):436–442. doi:10.1016/s0002-9343(99)80342-8
41. Rodeghiero F. A critical appraisal of the evidence for the role of splenectomy in adults and children with ITP. Br J Haematol. 2018;181(2):183–195. doi:10.1111/bjh.15090
42. Kojouri K, Vesely SK, Terrell DR, et al. Splenectomy for adult patients with idiopathic thrombocytopenic purpura: a systematic review to assess long-term platelet count responses, prediction of response, and surgical complications. Blood. 2004;104(9):2623–2634. doi:10.1182/blood-2004-03-1168
43. Bisharat N, Omari H, Lavi I, et al. Risk of infection and death among post-splenectomy patients. J Infect. 2001;43(3):182–186. doi:10.1053/jinf.2001.0904
44. Boyle S, White RH, Brunson A, et al. Splenectomy and the incidence of venous thromboembolism and sepsis in patients with immune thrombocytopenia. Blood. 2013;121(23):4782–4790. doi:10.1182/blood-2012-12-467068
45. Ruggeri M, Tosetto A, Palandri F, et al. Thrombotic risk in patients with primary immune thrombocytopenia is only mildly increased and explained by personal and treatment-related risk factors. J Thromb Haemost. 2014;12(8):1266–1273. doi:10.1111/jth.12636
46. Deshayes S, Khellaf M, Zarour A, et al. Long-term safety and efficacy of rituximab in 248 adults with immune thrombocytopenia: results at 5 years from the French prospective registry ITP-ritux. Am J Hematol. 2019;94(12):1314–1324. doi:10.1002/ajh.25632
47. Ghanima W, Khelif A, Waage A, et al. Rituximab as second-line treatment for adult immune thrombocytopenia (the RITP trial): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2015;385(9978):1653–1661. doi:10.1016/S0140-6736(14)61495-1
48. Chugh S, Darvish-Kazem S, Lim W, et al. Rituximab plus standard of care for treatment of primary immune thrombocytopenia: a systematic review and meta-analysis. Lancet Haematol. 2015;2(2):e75–e81. doi:10.1016/S2352-3026(15)00003-4
49. Arnold DM, Dentali F, Crowther MA, et al. Systematic review: efficacy and safety of rituximab for adults with idiopathic thrombocytopenic purpura. Ann Intern Med. 2007;146(1):25–33. doi:10.7326/0003-4819-146-1-200701020-00006
50. Tjønnfjord E, Holme PA, Darne B, et al. Long-term outcomes of patients treated with rituximab as second-line treatment for adult immune thrombocytopenia - follow-up of the RITP study. Br J Haematol. 2020;191(3):460–465. doi:10.1111/bjh.16672
51. Zaja F, Vianelli N, Volpetti S, et al. Low-dose rituximab in adult patients with primary immune thrombocytopenia. Eur J Haematol. 2010;85(4):329–334. doi:10.1111/j.1600-0609.2010.01486.x
52. Mahevas M, Ebbo M, Audia S, et al. Efficacy and safety of rituximab given at 1000 mg on days 1 and 15 compared to the standard regimen to treat adult immune thrombocytopenia. Am J Hematol. 2013;88(10):858–861. doi:10.1002/ajh.23518
53. Tran H, Brighton T, Grigg A, et al. A multi-centre, single-arm, open-label study evaluating the safety and efficacy of fixed dose rituximab in patients with refractory, relapsed or chronic idiopathic thrombocytopenic purpura (R-ITP1000 study). Br J Haematol. 2014;167(2):243–251. doi:10.1111/bjh.13029
54. Zhou H, Liu L, Shu X, et al. Clinical efficacy and safety of high-dose dexamethasone plus low-dose rituximab as first-line therapy in newly diagnosed primary immune thrombocytopenia. Indian J Hematol Blood Transfus. 2019;35(3):507–512. doi:10.1007/s12288-018-1061-7
55. Raso S, Napolitano M, Arrigo G, et al. Antimicrobial prophylaxis in patients with immune thrombocytopenia treated with rituximab: a retrospective multicenter analysis. Ann Hematol. 2021;100:653–659. doi:10.1007/s00277-021-04438-7
56. Nazi I, Kelton JG, Larché M, et al. The effect of rituximab on vaccine responses in patients with immune thrombocytopenia. Blood. 2013;122(11):1946–1953. doi:10.1182/blood-2013-04-494096
57. Kuter DJ. The biology of thrombopoietin and thrombopoietin receptor agonists. Int J Hematol. 2013;98(1):10–23. doi:10.1007/s12185-013-1382-0
58. Birocchi S, Podda GM, Manzoni M, et al. Thrombopoietin receptor agonists for the treatment of primary immune thrombocytopenia: a meta-analysis and systematic review. Platelets. 2020;32:1–11. doi:10.1080/09537104.2020.1745168.
59. Al-Samkari H, Kuter DJ. Optimal use of thrombopoietin receptor agonists in immune thrombocytopenia. Ther Adv Hematol. 2019;10:2040620719841735. doi:10.1177/2040620719841735
60. Al-Samkari H, Van Cott EM, Kuter DJ. Platelet aggregation response in immune thrombocytopenia patients treated with romiplostim. Ann Hematol. 2019;98(3):581–588. doi:10.1007/s00277-018-3556-6
61. Amgen Inc. Nplate (Romiplostim) [Prescribing Information]. Thousand Oaks, CA: Amgen; 2017.
62. Kuter DJ, Bussel JB, Lyons RM, et al. Efficacy of romiplostim in patients with chronic immune thrombocytopenic purpura: a double-blind randomised controlled trial. Lancet. 2008;371(9610):395–403. doi:10.1016/S0140-6736(08)60203-2
63. Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889–1899. doi:10.1056/NEJMoa1002625
64. Kuter DJ, Arnold DM, Rodeghiero F, et al. Safety and efficacy of self-administered romiplostim in patients with immune thrombocytopenia: results of an integrated database of five clinical trials. Am J Hematol. 2020;95(6):643–651. doi:10.1002/ajh.25776
65. Al-Samkari H, Grace RF, Kuter DJ. The role of romiplostim for pediatric patients with immune thrombocytopenia. Ther Adv Hematol. 2020;11:2040620720912992. doi:10.1177/2040620720912992
66. GlaxoSmithKline. Promacta (Eltrombopag) [Prescribing Information]. Research Triangle Park, NC.: GlaxoSmithKline; 2017.
67. Bussel JB, Kuter DJ, Pullarkat V, et al. Safety and efficacy of long-term treatment with romiplostim in thrombocytopenic patients with chronic ITP. Blood. 2009;113(10):2161–2171. doi:10.1182/blood-2008-04-150078
68. Cheng G, Saleh MN, Marcher C, et al. Eltrombopag for management of chronic immune thrombocytopenia (RAISE): a 6-month, randomised, phase 3 study. Lancet. 2011;377(9763):393–402. doi:10.1016/S0140-6736(10)60959-2
69. Tomiyama Y, Miyakawa Y, Okamoto S, et al. A lower starting dose of eltrombopag is efficacious in Japanese patients with previously treated chronic immune thrombocytopenia. J Thromb Haemost. 2012;10(5):799–806. doi:10.1111/j.1538-7836.2012.04695.x
70. Yang R, Hou M, Li J, et al. Effect of eltrombopag on platelet response and safety results in Chinese adults with chronic ITP-primary result of a phase III study. Blood. 2014;124(21):1464. doi:10.1182/blood.V124.21.1464.1464
71. Elgebaly AS, Ashal GE, Elfil M, et al. Tolerability and efficacy of eltrombopag in chronic immune thrombocytopenia: meta-analysis of randomized controlled trials. Clin Appl Thromb Hemost. 2017;23(8):928–937. doi:10.1177/1076029616663849
72. Williams DD, Peng B, Bailey CK, et al. Effects of food and antacids on the pharmacokinetics of eltrombopag in healthy adult subjects: two single-dose, open-label, randomized-sequence, crossover studies. Clin Ther. 2009;31(4):764–776. doi:10.1016/j.clinthera.2009.04.010
73. Wire MB, Bruce J, Gauvin J, et al. A randomized, open-label, 5-period, balanced crossover study to evaluate the relative bioavailability of eltrombopag powder for oral suspension (PfOS) and tablet formulations and the effect of a high-calcium meal on eltrombopag pharmacokinetics when administered with or 2 hours before or after PfOS. Clin Ther. 2012;34(3):699–709. doi:10.1016/j.clinthera.2012.01.011
74. González-Porras JR, Godeau B, Carpenedo M. Switching thrombopoietin receptor agonist treatments in patients with primary immune thrombocytopenia. Ther Adv Hematol. 2019;10:2040620719837906. doi:10.1177/2040620719837906
75. Al-Samkari H, Kuter DJ. An alternative intermittent eltrombopag dosing protocol for the treatment of chronic immune thrombocytopenia. Br J Clin Pharmacol. 2018;84(11):2673–2677. doi:10.1111/bcp.13717
76. AkaRx. DOPTELET (Avatrombopag) [Prescribing Information]. Durham, NC: AkaRx; 2020.
77. Bussel JB, Kuter DJ, Aledort LM, et al. A randomized trial of avatrombopag, an investigational thrombopoietin-receptor agonist, in persistent and chronic immune thrombocytopenia. Blood. 2014;123(25):3887–3894. doi:10.1182/blood-2013-07-514398
78. Al-Samkari H, Nagalla S. Efficacy and safety evaluation of avatrombopag in immune thrombocytopenia: analyses of a phase III study and long-term extension. Platelets. 2021;1–8. doi:10.1080/09537104.2021.1881952
79. Jurczak W, Chojnowski K, Mayer J, et al. Phase 3 randomised study of avatrombopag, a novel thrombopoietin receptor agonist for the treatment of chronic immune thrombocytopenia. Br J Haematol. 2018;183(3):479–490. doi:10.1111/bjh.15573
80. Cheloff AZ, Al-Samkari H. Avatrombopag for the treatment of immune thrombocytopenia and thrombocytopenia of chronic liver disease. J Blood Med. 2019;10:313–321. doi:10.2147/jbm.S191790
81. Terrault N, Chen YC, Izumi N, et al. Avatrombopag before procedures reduces need for platelet transfusion in patients with chronic liver disease and thrombocytopenia. Gastroenterology. 2018;155(3):705–718. doi:10.1053/j.gastro.2018.05.025
82. Virk ZM, Kuter DJ, Al-Samkari H. An evaluation of avatrombopag for the treatment of thrombocytopenia. Expert Opin Pharmacother. 2021;22(3):273–280. doi:10.1080/14656566.2020.1841748
83. Al-Samkari H. Avatrombopag maleate for the treatment of periprocedural thrombocytopenia in patients with chronic liver disease. Drugs Today. 2018;54(11):647–655. doi:10.1358/dot.2018.54.11.2899441
84. Thrombopoietin Receptor Agonists. LiverTox: Clinical and Research Information on Drug-Induced Liver Injury. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
85. Al-Samkari H, Kuter DJ. Relative potency of the thrombopoietin receptor agonists eltrombopag, avatrombopag and romiplostim in a patient with chronic immune thrombocytopenia. Br J Haematol. 2018;183(2):168. doi:10.1111/bjh.15432
86. Arnall JR, DiSogra KY, Downing L, et al. Comparative utilization and efficacy of thrombopoietin receptor agonists in relapsed/refractory immune thrombocytopenia. Am J Ther. 2021;Publish Ahead of Print. doi:10.1097/mjt.0000000000001335
87. Zhang J, Liang Y, Ai Y, et al. Eltrombopag versus romiplostim in treatment of adult patients with immune thrombocytopenia: a systematic review incorporating an indirect-comparison meta-analysis. PLoS One. 2018;13(6):e0198504. doi:10.1371/journal.pone.0198504
88. Provan D, Arnold DM, Bussel JB, et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019;3(22):3780–3817. doi:10.1182/bloodadvances.2019000812
89. Iino M, Sakamoto Y, Sato T. Treatment-free remission after thrombopoietin receptor agonist discontinuation in patients with newly diagnosed immune thrombocytopenia: an observational retrospective analysis in real-world clinical practice. Int J Hematol. 2020;112(2):159–168. doi:10.1007/s12185-020-02893-y
90. Cuker A, Despotovic JM, Grace RF, et al. Tapering thrombopoietin receptor agonists in primary immune thrombocytopenia: expert consensus based on the RAND/UCLA modified delphi panel method. Res Pract Thromb Haemost. 2021;5(1):69–80. doi:10.1002/rth2.12457
91. Lucchini E, Palandri F, Volpetti S, et al. Eltrombopag second-line therapy in adult patients with primary immune thrombocytopenia in an attempt to achieve sustained remission off-treatment: results of a phase II, multicentre, prospective study. Br J Haematol. 2021;193:386–396. doi:10.1111/bjh.17334
92. Al-Samkari H, Kuter DJ. Thrombopoietin level predicts response to treatment with eltrombopag and romiplostim in immune thrombocytopenia. Am J Hematol. 2018;93(12):1501–1508. doi:10.1002/ajh.25275
93. Markham A. Fostamatinib: first global approval. Drugs. 2018;78(9):959–963. doi:10.1007/s40265-018-0927-1
94. Bussel J, Arnold DM, Grossbard E, et al. Fostamatinib for the treatment of adult persistent and chronic immune thrombocytopenia: results of two phase 3, randomized, placebo-controlled trials. Am J Hematol. 2018;93(7):921–930. doi:10.1002/ajh.25125
95. Bussel JB, Arnold DM, Boxer MA, et al. Long-term fostamatinib treatment of adults with immune thrombocytopenia during the phase 3 clinical trial program. Am J Hematol. 2019;94(5):546–553. doi:10.1002/ajh.25444
96. Langrish CL, Bradshaw JM, Francesco MR, et al. Preclinical efficacy and anti-inflammatory mechanisms of action of the bruton tyrosine kinase inhibitor rilzabrutinib for immune-mediated disease. J Immunol. 2021;206(7):1454–1468. doi:10.4049/jimmunol.2001130
97. Smith PF, Krishnarajah J, Nunn PA, et al. A phase I trial of PRN1008, a novel reversible covalent inhibitor of Bruton’s tyrosine kinase, in healthy volunteers. Br J Clin Pharmacol. 2017;83(11):2367–2376. doi:10.1111/bcp.13351
98. Li G, Wang S, Li N, et al. Proteasome inhibition with bortezomib induces apoptosis of long-lived plasma cells in steroid-resistant or relapsed immune thrombocytopaenia. Thromb Haemost. 2018;118(10):1752–1764. doi:10.1055/s-0038-1669921
99. Beckman JD, Rollins-Raval MA, Raval JS, et al. Bortezomib for refractory immune-mediated thrombocytopenia purpura. Am J Ther. 2018;25(2):e270–e272. doi:10.1097/mjt.0000000000000517
100. Cuker A, Neunert CE. How I treat refractory immune thrombocytopenia. Blood. 2016;128(12):1547–1554. doi:10.1182/blood-2016-03-603365
101. Miltiadous O, Hou M, Bussel JB. Identifying and treating refractory ITP: difficulty in diagnosis and role of combination treatment. Blood. 2020;135(7):472–490. doi:10.1182/blood.2019003599
102. Mahévas M, Gerfaud-Valentin M, Moulis G, et al. Characteristics, outcome, and response to therapy of multirefractory chronic immune thrombocytopenia. Blood. 2016;128(12):1625–1630. doi:10.1182/blood-2016-03-704734
103. Webert KE, Mittal R, Sigouin C, et al. A retrospective 11-year analysis of obstetric patients with idiopathic thrombocytopenic purpura. Blood. 2003;102(13):4306–4311. doi:10.1182/blood-2002-10-3317
104. Al-Jama FE, Rahman J, Al-Suleiman SA, et al. Outcome of pregnancy in women with idiopathic thrombocytopenic purpura. Aust N Z J Obstet Gynaecol. 1998;38(4):410–413. doi:10.1111/j.1479-828X.1998.tb03099.x
105. Nicolescu A, Vladareanu AM, Voican I, et al. Therapeutic options for Immune Thrombocytopenia (ITP) during pregnancy. Maedica. 2013;8(2):182–188.
106. Michel M, Ruggeri M, Gonzalez-Lopez TJ, et al. Use of thrombopoietin receptor agonists for immune thrombocytopenia in pregnancy: results from a multicenter study. Blood. 2020;136(26):3056–3061. doi:10.1182/blood.2020007594
107. Gernsheimer T, James AH, Stasi R. How I treat thrombocytopenia in pregnancy. Blood. 2013;121(1):38–47. doi:10.1182/blood-2012-08-448944
108. Bussel JB, Provan D, Shamsi T, et al. Effect of eltrombopag on platelet counts and bleeding during treatment of chronic idiopathic thrombocytopenic purpura: a randomised, double-blind, placebo-controlled trial. Lancet. 2009;373(9664):641–648. doi:10.1016/S0140-6736(09)60402-5
109. Shirasugi Y, Ando K, Miyazaki K, et al. Romiplostim for the treatment of chronic immune thrombocytopenia in adult Japanese patients: a double-blind, randomized Phase III clinical trial. Int J Hematol. 2011;94(1):71–80. doi:10.1007/s12185-011-0886-8
110. Quiquandon I, Fenaux P, Caulier MT, et al. Re-evaluation of the role of azathioprine in the treatment of adult chronic idiopathic thrombocytopenic purpura: a report on 53 cases. Br J Haematol. 1990;74(2):223–228. doi:10.1111/j.1365-2141.1990.tb02569.x
111. Verlin M, Laros RK, Penner JA. Treatment of refractory thrombocytopenic purpura with cyclophosphamine. Am J Hematol. 1976;1(1):97–104. doi:10.1002/ajh.2830010111
112. Pizzuto J, Ambriz R. Therapeutic experience on 934 adults with idiopathic thrombocytopenic purpura: multicentric trial of the cooperative Latin American group on hemostasis and thrombosis. Blood. 1984;64(6):1179–1183. doi:10.1182/blood.V64.6.1179.1179
113. Choudhary DR, Naithani R, Mahapatra M, et al. Efficacy of cyclosporine as a single agent therapy in chronic idiopathic thrombocytopenic purpura. Haematologica. 2008;93(10):
114. Kappers-Klunne MC, Van’t Veer MB. Cyclosporin A for the treatment of patients with chronic idiopathic thrombocytopenic purpura refractory to corticosteroids or splenectomy. Br J Haematol. 2001;114(1):121–125. doi:10.1046/j.1365-2141.2001.02893.x
115. Fenaux P, Quiquandon I, Huart JJ, et al. The role of danazol in the treatment of refractory idiopathic thrombocytopenic purpura. A report of 22 cases. Nouv Rev Fr Hematol. 1990;32(2):143–146.
116. Li HQ, Zhang L, Zhao H, et al. Chronic idiopathic thrombocytopenic purpura in adult Chinese patients: a retrospective single-centered analysis of 1791 cases. Chin Med J (Engl). 2005;118(1):34–37.
117. Liu W, Gu X, Fu R, et al. The effect of danazol in primary immune thrombocytopenia: an analysis of a large cohort from a single center in China. Clin Appl Thromb Hemost. 2016;22(8):727–733. doi:10.1177/1076029615622002
118. Maloisel F, Andres E, Zimmer J, et al. Danazol therapy in patients with chronic idiopathic thrombocytopenic purpura: long-term results. Am J Med. 2004;116(9):590–594. doi:10.1016/j.amjmed.2003.12.024
119. Damodar S, Viswabandya A, George B, et al. Dapsone for chronic idiopathic thrombocytopenic purpura in children and adults--a report on 90 patients. Eur J Haematol. 2005;75(4):328–331. doi:10.1111/j.1600-0609.2005.00545.x
120. Godeau B, Durand JM, Roudot-Thoraval F, et al. Dapsone for chronic autoimmune thrombocytopenic purpura: a report of 66 cases. Br J Haematol. 1997;97(2):336–339. doi:10.1046/j.1365-2141.1997.412687.x
121. Zaja F, Marin L, Chiozzotto M, et al. Dapsone salvage therapy for adult patients with immune thrombocytopenia relapsed or refractory to steroid and rituximab. Am J Hematol. 2012;87(3):321–323. doi:10.1002/ajh.22266
122. Hou M, Peng J, Shi Y, et al. Mycophenolate mofetil (MMF) for the treatment of steroid-resistant idiopathic thrombocytopenic purpura. Eur J Haematol. 2003;70(6):353–357. doi:10.1034/j.1600-0609.2003.00076.x
123. Taylor A, Neave L, Solanki S, et al. Mycophenolate mofetil therapy for severe immune thrombocytopenia. Br J Haematol. 2015;171(4):625–630. doi:10.1111/bjh.13622
124. Zhang WG, Ji L, Cao XM, et al. Mycophenolate mofetil as a treatment for refractory idiopathic thrombocytopenic purpura. Acta Pharmacol Sin. 2005;26(5):598–602. doi:10.1111/j.1745-7254.2005.00088.x
125. Ahn YS, Harrington WJ, Mylvaganam R, et al. Slow infusion of vinca alkaloids in the treatment of idiopathic thrombocytopenic purpura. Ann Intern Med. 1984;100(2):192–196. doi:10.7326/0003-4819-100-2-192
126. Facon T, Caulier MT, Wattel E, et al. A randomized trial comparing vinblastine in slow infusion and by bolus i.v. injection in idiopathic thrombocytopenic purpura: a report on 42 patients. Br J Haematol. 1994;86(3):678–680. doi:10.1111/j.1365-2141.1994.tb04810.x
127. Fenaux P, Quiquandon I, Caulier MT, et al. Slow infusions of vinblastine in the treatment of adult idiopathic thrombocytopenic purpura: a report on 43 cases. Blut. 1990;60(4):238–241. doi:10.1007/BF01728791
128. Park YH, Yi HG, Lee MH, et al. Clinical efficacy and tolerability of vincristine in splenectomized patients with refractory or relapsed immune thrombocytopenia: a retrospective single-center study. Int J Hematol. 2016;103(2):180–188. doi:10.1007/s12185-015-1903-0
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.