")
Back to Journals » Research and Reports in Urology » Volume 14
Male Sexual Health Implications of the 2022 Global Monkeypox Outbreak
Authors White J, Rivero MJ , Mohamed AI , Thomas J, Muthigi A, Rahman F, Ory J, Petrella F, Ramasamy R
Received 17 August 2022
Accepted for publication 16 November 2022
Published 21 November 2022 Volume 2022:14 Pages 415—421
DOI https://doi.org/10.2147/RRU.S381191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Panagiotis J Vlachostergios
Joshua White,1 Marco-Jose Rivero,1 Arslan I Mohamed,2 Jamie Thomas,3 Akhil Muthigi,1 Farah Rahman,1 Jesse Ory,4 Francis Petrella,5 Ranjith Ramasamy1
1Urology, University of Miami Miller School of Medicine, Miami, FL, USA; 2Undergraduate Medical Education, City University of New York, New York, NY, USA; 3Undergraduate Medical Education, Nova Southeastern University Kiran Patel College of Osteopathic Medicine, Fort Lauderdale, FL, USA; 4Urology, Dalhousie University, Halifax, Nova Scotia, Canada; 5Urology, McGill University, Montreal, Quebec, Canada
Correspondence: Joshua White; Ranjith Ramasamy, Email [email protected]; [email protected]
Abstract: The 2022 global monkeypox (MPX) outbreak is the largest in history to occur outside of endemic African regions. Disease spread during this outbreak has been primarily through human-to-human transmission, with sexual contact being of particular concern. Clinical presentations have commonly featured genital, perianal, and oral lesions associated with sexual activity among men who have sex with men (MSM), who compose the vast majority of MPX cases. This review discusses the epidemiology, clinical features, and evaluation of MPX with regards to men’s sexual health. Comparisons were made between MPX and its relative from the Orthopoxvirus genus, smallpox, in order to make informed inferences on the potential effects of MPX on men’s sexual health. This review also discusses the role of men’s health specialists and urologists in addressing the current outbreak.
Keywords: monkeypox, infertility, sexual health, transmission, men’s health
Introduction
In July 2022, the World Health Organization sounded its highest alarm level for monkeypox (MPX), declaring a public health emergency of international concern.1 MPX is a viral zoonotic infection for which, prior to 2020, fewer than 100 cases within the United States had been reported.2,3 The first positive test in the current outbreak was identified on May 18, 2022.4 The disease spread from the United Kingdom to the United States with alarming speed to where, in August 2022, the United States had the most cases in the world with more than 6600.1 As of late September 2022, the current case count is more than 25,000 in the United States and more than 68,000 globally.5 Relatively little is known about the optimal clinical approach to MPX, as only a few thousand cases have been reported across the literature in the past five decades.6,7 Moreover, there is a lack of literature guiding the diagnosis and treatment of MPX as it pertains to men’s sexual health. Much of what we can anticipate and learn is from other similar conditions, such as smallpox.
Recently, a case report has been published highlighting the first documented case of a soft tissue abscess infected with MPX.8 This suggests that the virus has the capacity to infect and replicate in deep tissue. Understanding the spectrum of disease requires providers to consider MPX in a broader range of clinical presentations. Viral involvement of male reproductive organs has been demonstrated in contemporary literature. For example, the West Nile virus and the severe acute respiratory syndrome coronavirus have both been associated with orchitis.9 Mumps is caused by a single-stranded Paramyxoviridae virus, with orchitis being the most common extra-salivary gland inflammatory manifestation. Up to 30% of men who developed mumps in the post-puberty period experience infertility or subfertility.10 In a set of recent paradigm-shifting publications, it has been found that the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19, invades both penile and testicular tissue.11,12 COVID-19 infection has also been associated with the development of erectile dysfunction.12 While these are vastly different conditions, it is an important reminder of the potential for gonadal involvement in viral diseases. In this review, we appraise the most contemporary data on MPX, draw parallels with comparable viral illnesses, and discuss potential ramifications on male sexual health.
Monkeypox Virus Background
MPX virus is a double-stranded DNA virus that is endemic to several Western and Central African countries. It was first reported in 1970 in the Democratic Republic of Congo.13 As a member of the Orthopoxvirus genus, MPX virus is a close cousin of smallpox virus, one of the deadliest infectious pathogens in documented history.14 Smallpox is also a success story in the implementation of effective vaccination policies; on May 8, 1980, the World Health Assembly declared the world free of smallpox.15 Although the recent COVID-19 pandemic remains fresh in public memory, the history of smallpox will likely play a role in informing the public health response to MPX.
There are several important similarities between MPX and smallpox that allow up to 85% cross reactive immunity against MPX in those who had received the smallpox vaccine.6,7 Clinical trials are currently underway to determine the prevalence of MPX amongst those who have received the smallpox vaccine.16 The clinical presentation is quite similar to smallpox as well, although MPX has lower morbidity and lower mortality and often presents with lymphadenopathy. The current outbreak has demonstrated, however, that many patients present with atypical features, such as a rash limited to the genital, and perianal areas presenting at varying stages of development.6,17
The typical course of MPX involves a febrile prodrome with classic flu-like symptoms (eg, fevers, chills, myalgias) followed by the development of deep, well-circumscribed lesions that progress from macules, to papules, to vesicles, ultimately developing into a scab (Figure 1).7,18,41 The rash generally starts in the mouth and spreads to the extremities, and lesions can be quite itchy, particularly as they form scabs. Lesions are assumed to be contagious for up to 4 weeks from when they first appear and, following transmission, have a 1–2 week incubation period.6,7 Oftentimes, these lesions are misdiagnosed as chickenpox, shingles or herpes, particularly in non-endemic areas of the world. Failure to diagnose MPX and prevent further transmission has likely contributed to rapid propagation of the virus. Furthermore, reports of asymptomatic patients infected with MPX raise concern that such patients may transmit the condition to others even in the absence of characteristic lesions.19
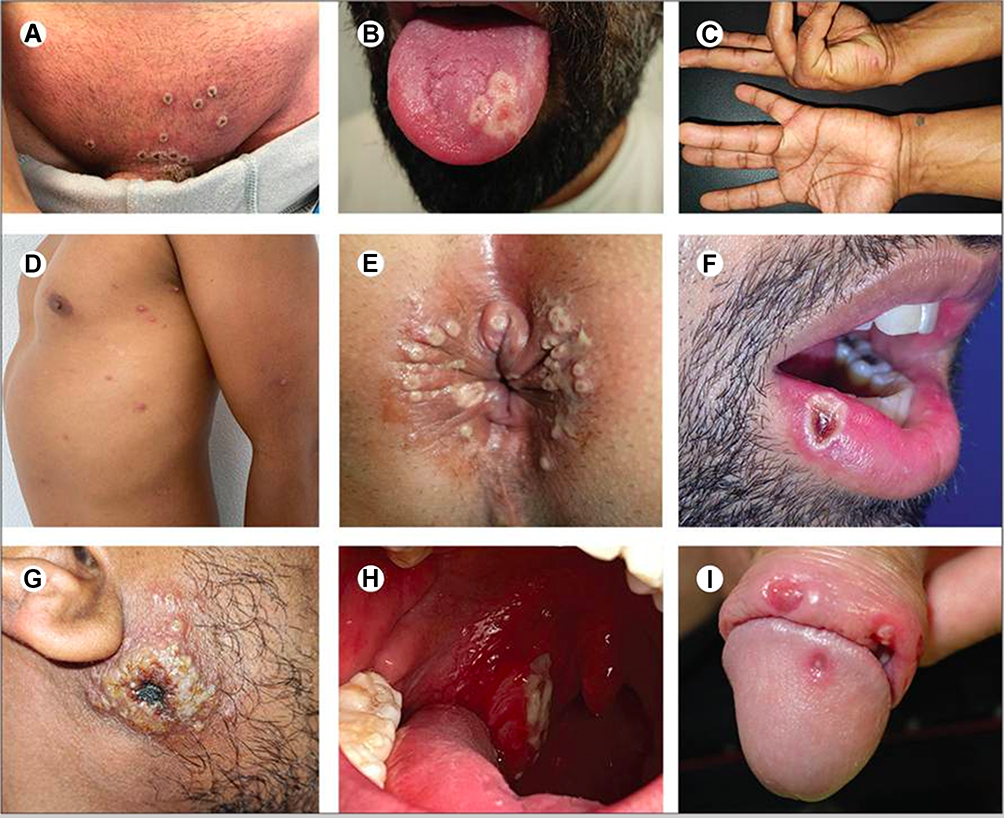 |
Figure 1 Clinical presentations of monkeypox (A) Pustules in the genital and pubic region, in which the initial umbilication has progressed to necrotic crust with central depression. (B) Three semiconfluent pustular lesions with a depressed centre located on the left side of the tongue dorsum. (C) Pearly acral vesicles embedded in the thick stratum corneum of the palmar skin, shotty on palpation. (D) Scattered papules, pustules, and umbilicated pustules surrounded by an erythematous halo on the lateral aspect of the chest and left arm. (E) Pustules circumferentially distributed on the anal margin and perianal skin. (F) A pustular lesion with a crusted centre on the semimucosa of the lower lip, close to the right oral commissure. (G) Primary inoculation site with a large, crusted lesion on the right cheek. (H) The right palatine tonsil is reddened and enlarged and has a fibrin-covered ulcer. (I) The penile glans and foreskin have lesions of varying sizes and stages of evolution, with oedema surrounding the larger ulcer. Notes: Reproduced from Tarín-Vicente EJ, Alemany A, Agud-Dios M et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: a prospective observational cohort study. Lancet. 2022;400(10353):661–669. Open Access.41 |
In the current outbreak, there has been an increased involvement of the characteristic rash in the genital and perianal areas, which understandably has been confused with other infections such as herpes simplex, syphilis, and molluscum contagiosum.6 Indeed, a recent literature review found both anal and genital lesions (ulcers and vesicles) present in over 30% of MPX cases. It is important to note that anogenital lesions were very uncommon findings in previous MPX outbreaks.20 As such, underdiagnosis may have contributed to the increased transmission that is being observed globally. There is a broad spectrum of disease ranging from mild to potentially fatal.7 As such, an increased level of suspicion for MPX should be maintained when evaluating genital and perianal lesions.
Monkeypox Viral Transmission
Transmission of MPX has traditionally been from animals, including small mammals and nonhuman primates, to humans via scratches, bites, or other exposure to animal fluids. The current outbreak was initially thought to be primarily via human-to-human transmission through direct skin-to-skin contact as well and indirect contact with contaminated bedding or clothing, or large respiratory droplets.6,20–22 Further evidence suggests that transmission is indeed primarily from direct and/or prolonged skin-to-skin contact. The true transmissibility due to large respiratory droplets is unclear, but is most likely limited.20 What is unique about the current outbreak, is that for unexplained reasons, the vast majority of cases have been in men who have sex with men (MSM).21 Interestingly, there is a case report of MPX relapse with temporal association between sexual intercourse and development of inguinal lymphadenopathy and skin lesions positive for viral DNA.23 Condomless sex or sex with multiple partners were reported in 84% of cases in a large case series in Spain.24 It is not currently known whether this relates to spread via cutaneous lesions in the genital area, or if the virus spreads through seminal or other bodily fluids. It should be noted, however, that a broad range of virus families have been shown to actively replicate within the male reproductive tract.25,26
Concomitant human immunodeficiency virus infection and resultant immunosuppression has been a proposed mechanism for an increased risk of MPX transmission, but does not explain the majority of the cases.7,17,27 There are recent case reports that have identified MPX virus in semen, blood and urine weeks after resolution of the initial infection.17,27 These cases involved anal and genital lesions associated with corresponding sexual behaviour. While these findings do suggest that sexual intercourse plays a role in viral transmission, no definitive conclusions can be drawn based on these limited case reports. Whether or not MPX can be transmitted sexually is an area requiring further investigation.
Cause for the Current Outbreak
One of the true success stories in the history of vaccination has been the eradication of smallpox in the early 1980s. Smallpox vaccination programs have been inactive for several decades, meaning there are large numbers of the global population that are not immunized against smallpox.6,28 Given that smallpox vaccination provides up to 85% cross-protection against MPX infection, the decline of smallpox vaccination programs is a potential factor contributing to the current global outbreak.29,30 There is no evidence currently to suggest that novel virus strains are responsible for the current outbreak.6,7 Human-to-human transmission is the suggested cause of the current outbreak, which is puzzling as this route was underrepresented in previous outbreaks in Central and Western Africa.17
Unfortunately, we do not currently understand why there has been such a dramatic uptick in cases, whether there is sexual transmission, or why there seems to be a disproportionate number of MSM patients who have contracted MPX. These are important questions that require dedicated clinical research in order to educate ourselves, our patients, and the global community on how to most effectively approach the outbreak.
Potential Impact on Male Sexual Health
The impact of MPX infection on male sexual health, including fertility, erectile function, and hypogonadism is unknown. We can draw some inferences from smallpox, though smallpox was eradicated in the early 1980s; well before the era of evidence-based medicine. There are reports of smallpox being a major etiological factor in patients with nonobstructive azoospermia.31 Pathological specimens in such patients demonstrate severe seminiferous tubule atrophy, tubular hyalinization, and even arrest of spermatogenesis at various stages.32 MPX virus has been isolated from seminal cultures, and viral seeding in the reproductive tract has been shown to occur in the setting of viremia.17 This is in part related to the presence of inflammation, which compromises the integrity of the blood-testis barrier. The testes are a sanctuary from an immunological standpoint, which suggests that the virus may be able to occupy the reproductive tract without needing to replicate systemically. The clinical significance of this remains a question.
Impact of Outbreak for Urologists
Urologists are among several healthcare providers that may be at the forefront of diagnosing MPX, particularly given the increased prevalence of genital lesions associated with the current outbreak. It is critically important that urologists and any healthcare provider who may encounter genital and perianal lesions in clinical practice keep MPX high on the differential. Further research is needed to clarify whether MPX can be sexually transmitted through genital fluids, or if transmission is limited to direct/indirect contact with lesions and respiratory droplets.
When clinical suspicion for MPX exists, clinicians should perform a thorough social history, including travel and sexual history. Identifying close contacts and reporting cases to public health may help reduce viral transmission. A thorough physical exam, including genital exam, should be performed to evaluate the clinical progression of these lesions, as bacterial superinfection resulting in profound pitting scars is a concerning long-term sequela.7 Clinicians in France recently found two MPX cases with lesions exclusively on the genitals, which further argues for thorough physical exams in the MSM population.33
Public health authorities in the United Kingdom have recommended abstinence from sexual intercourse for up to 8 weeks after recovery.23 This seems to be a reasonable approach until there is more information to guide sexual health counselling specific to MPX. It is important to emphasize to patients that we have only begun to scratch the surface in understanding this disease. We know very little about the viral kinetics of MPX infection in humans. Nevertheless, there are prioritized vaccination programs for patients at increased risk of developing MPX, eg, MSM, which have been implemented in efforts to contain the outbreak.34,35
In the current outbreak, genital lesions are a common presenting symptom that clinicians will encounter. Perirectal lesions, proctitis, and ocular involvement have also been documented (Figure 2).18,36–38 Though, it is also important to remember the nonspecific presentation of rash, fever, and/or lymphadenopathy.
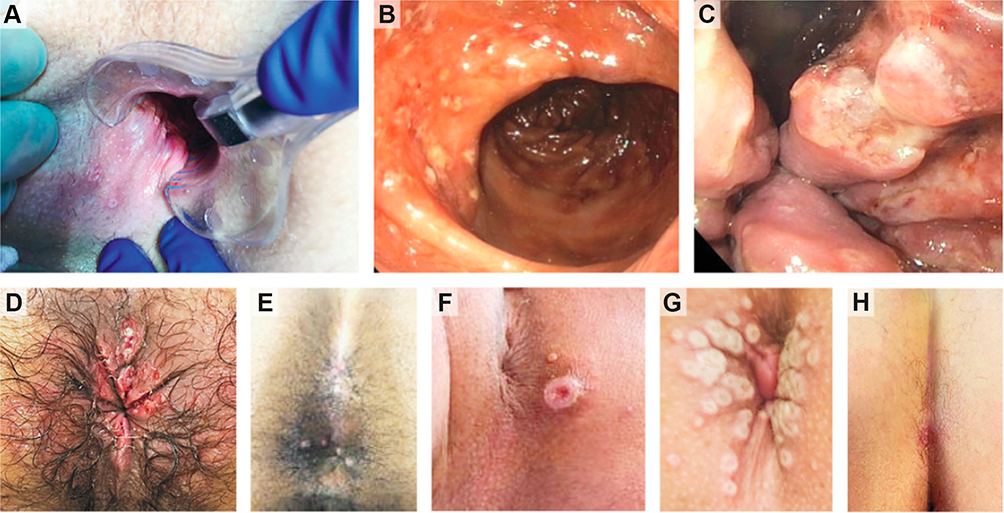 |
Figure 2 Anorectal and perianal monkeypox lesions (A–C) anal, perianal and rectal lesions (D) perianal ulcers (E) anal lesions (F) umbilicated perianal lesion (G) umbilicated perianal lesion (H) perianal ulcer. Notes: From N Engl J Med. Thornhill JP, Barkati S, Walmsley S et al. Monkeypox Virus Infection in Humans across 16 Countries - April-June 2022. 387(8):679–691. Copyright © (2022). Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society.18 |
At the time of writing this review, a vaccine has yet to be created specifically against MPX. However, the two vaccines currently recommended for MPX include JYNNEOS and ACAM2000, which are both vaccinia virus-based vaccines originally designed to protect against smallpox.34,35,39 JYNNEOS, a Modified Vaccinia Ankara vaccine, is a two-dose vaccine administered twenty-eight days apart, believed to reach maximal immune protection two weeks following the second dose. Its efficacy has been inferred from studies using animal models.34,39 ACAM2000, a live Vaccinia virus vaccine, is a single-dose vaccine. It is believed to reach maximal protection four weeks following administration and, as a direct derivative of the Dryvax vaccine used against smallpox, has effectiveness in preventing orthopoxviruses including MPX.35,40 Both vaccines are authorized for patients above the age of 18 with one of the following risk criteria: close contact or sexual activity with someone diagnosed with MPX; sexual activity in an area with known MPX; or work in a high-risk setting such as laboratory, healthcare, and public health. JYNNEOS is recommended for immunocompromised patients as ACAM2000 has the potential for uncontrolled systemic replication, which could lead to serious adverse effects in this population. A JYNNEOS booster is recommended every 2 years for patients who have received either vaccine and are at ongoing risk for exposure to MPX, as the ACAM2000 booster has been found to increase the risk of myopericarditis.39
Finally, there is an important social aspect of care that must be addressed. There has been an unacceptable stigma directed towards gay, bisexual, and other MSM, similar to the stigma experienced by these groups during the early days of HIV.6 Clinicians must be strong patient advocates, providing healthcare that is supportive and free of judgment. Although MSM are disproportionately affected and may benefit from routine sexual health counselling, clinicians should emphasize to patients that infectious pathogens have no preferences in terms of race, gender, or sexual orientation.
Conclusion
There is a need for up-to-date, consistent, and longitudinal research into the men’s sexual implications associated with MPX infection. Most cases in the current outbreak have been identified in MSM, meriting sexual health preventive measures in this patient population. Otherwise, we do not yet have the data to guide clinical management effectively. While smallpox provides a starting point for understanding the current MPX outbreak, we advocate for a deliberate effort in elucidating the virology of MPX in order to better understand the full extent of the clinical implications. Currently there is a worldwide shortage of vaccines, which may further exacerbate patient anxiety. Clinicians should counsel at-risk patients on the safety and efficacy of the vaccinations currently available. Advocacy for safe sexual practices to help limit the spread of the virus remains paramount, as well as a knowledge and recognition of the disease. Long-term follow-up will be required to better understand the clinical effects of MPX on male sexual and reproductive health.
Funding
Funding for this project was supported by the National Institute of Health Grant R01 DK 130991 to Dr. Ranjith Ramasamy at the University of Miami.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reuters T. U.S. declares monkeypox a public health emergency CBC news. CBC; 2022. Available from: https://www.cbc.ca/news/health/us-declare-monkeypox-public-health-emergency-1.6541279.
2. Centers for Disease Control and Prevention (CDC). Multistate outbreak of monkeypox--Illinois, Indiana, and Wisconsin, 2003. MMWR Morb Mortal Wkly Rep. 2003;52(23):537–540.
3. Reed KD, Melski JW, Graham MB, et al. The detection of monkeypox in humans in the Western Hemisphere. N Engl J Med. 2004;350(4):342–350. doi:10.1056/NEJMoa032299
4. Key Questions About the Current U.S. Monkeypox Outbreak. KFF; 2022. Available from: https://www.kff.org/other/issue-brief/key-questions-about-The-current-u-s-monkeypox-outbreak/.
5. CDC. Monkeypox in the U.S. Centers for disease control and prevention; 2022. Available from: https://www.cdc.gov/poxvirus/monkeypox/response/2022/index.html.
6. Titanji BK, Tegomoh B, Nematollahi S, Konomos M, Kulkarni PA. Monkeypox: a contemporary review for healthcare professionals. Open Forum Infect Dis. 2022;9(7):ofac310. doi:10.1093/ofid/ofac310
7. Beer EM, Rao VB. A systematic review of the epidemiology of human monkeypox outbreaks and implications for outbreak strategy. PLoS Negl Trop Dis. 2019;13(10):e0007791. doi:10.1371/journal.pntd.0007791
8. Davido B, D’Anglejan E, Baudoin R, et al. Monkeypox outbreak 2022: an unusual case of peritonsillar abscess in a person previously vaccinated against smallpox. J Travel Med. 2022;29(6):taac082. doi:10.1093/jtm/taac082
9. Payne K, Kenny P, Scovell JM, Khodamoradi K, Ramasamy R. Twenty-first century viral pandemics: a literature review of sexual transmission and fertility implications in men. Sex Med Rev. 2020;8(4):518–530. doi:10.1016/j.sxmr.2020.06.003
10. Wu H, Wang F, Tang D, Han D. Mumps orchitis: clinical aspects and mechanisms. Front Immunol. 2021;12:582946. doi:10.3389/fimmu.2021.582946
11. Achua JK, Chu KY, Ibrahim E, et al. Histopathology and ultrastructural findings of fatal COVID-19 infections on testis. World J Mens Health. 2021;39(1):65–74. doi:10.5534/wjmh.200170
12. Kresch E, Achua J, Saltzman R, et al. COVID-19 endothelial dysfunction can cause erectile dysfunction: histopathological, Immunohistochemical, and ultrastructural study of the human penis. World J Mens Health. 2021;39(3):466–469. doi:10.5534/wjmh.210055
13. Multi-country monkeypox outbreak in non-endemic countries. Available from: https://www.who.int/emergencies/disease-outbreak-news/item/2022-DON385.
14. Fenner F, Henderson DA, Arita I, Jezek Z, Ladnyi ID. Smallpox and Its Eradication. World Health Organization; 1988. Available from: https://apps.who.int/iris/handle/10665/39485.
15. Strassburg MA. The global eradication of smallpox. Am J Infect Control. 1982;10(2):53–59. doi:10.1016/0196-6553(82)90003-7
16. CDC. Monkeypox technical reports. Centers for disease control and prevention; 2022. https://www.cdc.gov/poxvirus/monkeypox/cases-data/technical-report/report-1.html.
17. Antinori A, Mazzotta V, Vita S, et al. Epidemiological, clinical and virological characteristics of four cases of monkeypox support transmission through sexual contact, Italy, May 2022. Euro Surveill. 2022;27:22. doi:10.2807/1560-7917.ES.2022.27.22.2200421
18. Thornhill JP, Barkati S, Walmsley S, et al. Monkeypox virus infection in humans across 16 countries - April-June 2022. N Engl J Med. 2022;387(8):679–691. doi:10.1056/NEJMoa2207323
19. Abbasi J. Reports of asymptomatic monkeypox suggest that, at the very least, some infections Go unnoticed. JAMA. 2022;328(11):1023–1025. doi:10.1001/jama.2022.15426
20. Bragazzi NL, Kong JD, Mahroum N, et al. Epidemiological trends and clinical features of the ongoing monkeypox epidemic: a preliminary pooled data analysis and literature review. J Med Virol. 2022. doi:10.1002/jmv.27931
21. Rimoin AW, Mulembakani PM, Johnston SC, et al. Major increase in human monkeypox incidence 30 years after smallpox vaccination campaigns cease in the Democratic Republic of Congo. Proc Natl Acad Sci U S A. 2010;107(37):16262–16267. doi:10.1073/pnas.1005769107
22. Jezek Z, Grab B, Szczeniowski MV, Paluku KM, Mutombo M. Human monkeypox: secondary attack rates. Bull World Health Organ. 1988;66(4):465–470.
23. Adler H, Gould S, Hine P, et al. Clinical features and management of human monkeypox: a retrospective observational study in the UK. Lancet Infect Dis. 2022;22(8):1153–1162. doi:10.1016/S1473-3099(22)00228-6
24. Iñigo Martínez J, Gil Montalbán E, Jiménez Bueno S, et al. Monkeypox outbreak predominantly affecting men who have sex with men, Madrid, Spain, 26 April to 16 June 2022. Euro Surveill. 2022;27(27). doi:10.2807/1560-7917.ES.2022.27.27.2200471
25. Salam AP, Horby PW. The breadth of viruses in human semen. Emerg Infect Dis. 2017;23(11):1922–1924. doi:10.3201/eid2311.171049
26. Dejucq N, Jégou B. Viruses in the mammalian male genital tract and their effects on the reproductive system. Microbiol Mol Biol Rev. 2001;65(2):208–231. doi:10.1128/MMBR.65.2.208-231.2001
27. Noe S, Zange S, Seilmaier M, et al. Clinical and virological features of first human monkeypox cases in Germany. Infection. 2022. doi:10.1007/s15010-022-01874-z
28. Lofaro J; Reporter Ctvn ca D, Contact F. Montreal public health shifting vaccination plan as monkeypox cases grow to 126. Montreal; 2022. Available from: https://montreal.ctvnews.ca/montreal-public-health-shifting-vaccination-plan-as-monkeypox-cases-grow-to-126-1.5946380.
29. Petersen E, Kantele A, Koopmans M, et al. Human monkeypox: epidemiologic and clinical characteristics, diagnosis, and prevention. Infect Dis Clin North Am. 2019;33(4):1027–1043. doi:10.1016/j.idc.2019.03.001
30. Nalca A, Rimoin AW, Bavari S, Whitehouse CA, Whitehouse CA. Reemergence of monkeypox: prevalence, diagnostics, and countermeasures. Clin Infect Dis. 2005;41(12):1765–1771. doi:10.1086/498155
31. Shchelkunov SN. An increasing danger of zoonotic orthopoxvirus infections. PLoS Pathog. 2013;9(12):e1003756. doi:10.1371/journal.ppat.1003756
32. Shchelkunov SN, Marennikova SS, Moyer RW, eds. Orthopoxviruses Pathogenic for Humans. Springer; 2005.
33. Davido B, D’anglejan E, Jourdan J, Robinault A, Davido G. Monkeypox 2022 outbreak: cases with exclusive genital lesions. J Travel Med. 2022;29(6):taac077. doi:10.1093/jtm/taac077
34. CDC. Jynneos Vaccine. Centers for disease control and prevention; 2022. Available from: https://www.cdc.gov/poxvirus/monkeypox/vaccines/jynneos.html.
35. CDC. ACAM2000 Vaccine. Centers for disease control and prevention; 2022. Available from: https://www.cdc.gov/poxvirus/monkeypox/vaccines/acam2000.html.
36. Lucar J, Roberts A, Saardi KM, Yee R, Siegel MO, Palmore TN. Monkeypox virus-associated severe proctitis treated with oral tecovirimat: a report of two cases. Ann Intern Med. 2022;175:1626–1627. doi:10.7326/L22-0300
37. Gedela K, Da Silva Fontoura D, Salam A, et al. Infectious proctitis due to human monkeypox. Clin Infect Dis. 2022:ciac713. doi:10.1093/cid/ciac713
38. Mazzotta V, Mondi A, Carletti F, et al. Ocular involvement in monkeypox: description of an unusual presentation during the current outbreak. J Infect. 2022;S0163–4453(22):474. doi:10.1016/j.jinf.2022.08.011
39. Rao AK, Petersen BW, Whitehill F, et al. Use of JYNNEOS (smallpox and monkeypox vaccine, live, nonreplicating) for preexposure vaccination of persons at risk for occupational exposure to orthopoxviruses: recommendations of the advisory committee on immunization practices - United States, 2022. MMWR Morb Mortal Wkly Rep. 2022;71(22):734–742. doi:10.15585/mmwr.mm7122e1
40. Mullendore NF, Lawner BJ, Malone JD. Monkeypox Attack. In: Ciottone’s Disaster Medicine. Elsevier; 2016:774–776. doi:10.1016/B978-0-323-28665-7.00149-7
41. Tarín-Vicente EJ, Alemany A, Agud-Dios M, et al. Clinical presentation and virological assessment of confirmed human monkeypox virus cases in Spain: a prospective observational cohort study. Lancet. 2022;400(10353):661–669. doi:10.1016/S0140-6736(22)01436-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.