")
Back to Journals » Vascular Health and Risk Management » Volume 18
Magnitudes of Risk Factors of Venous Thromboembolism and Quality of Anticoagulant Therapy in Ethiopia: A Systematic Review
Received 3 November 2021
Accepted for publication 30 March 2022
Published 11 April 2022 Volume 2022:18 Pages 245—252
DOI https://doi.org/10.2147/VHRM.S347667
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Takashi Kajiya
Bekalu Kebede, Tirsit Ketsela
Clinical Pharmacy Unit, Pharmacy Department, Health Science College, Debre Markos University, Debre Markos, Ethiopia
Correspondence: Bekalu Kebede, Department of Pharmacy, College of Health Sciences, Debre Markos University, P.O. Box 269, Debre Markos, Ethiopia, Tel +251 921286140, Email [email protected]
Background: Venous thromboembolism is one of the major public health problems in the world. Though several studies were conducted to estimate common risk factors of venous thromboembolism and quality of anticoagulant therapy in Ethiopia, it is difficult to estimate the overall burdens of risk factors and quality of anticoagulant use because of the lack of a nationwide study.
Objective: To assess magnitudes of risk factors of venous thromboembolism and quality of anticoagulant therapy in Ethiopia.
Materials and Methods: Electronic searching using PubMed, EMBASE, Science Direct, Cochrane Database, Scopus, Hinari, Sci-Hub, African Journals Online Library, and Free-text Web Searches using Google Scholar was conducted from September, 15 to October 27, 2021. Each of the original studies was identified by Mesh terms and Boolean search technique using full title, various keywords and was assessed using the Joanna Briggs Institute Critical Appraisal Checklist. The data were extracted using a format prepared in Microsoft Excel and exported to STATA 14.0 for the outcome analyses.
Results: The database search delivered a total of 2118 studies. After articles were removed by duplications, titles, reading the abstract, and assessed for eligibility criteria, 12 articles were found suitable for the systematic review. Prolonged immobilization (41.30%) was the most commonly observed risk factor of venous thrombosis followed by acute infection (40.25%). The proportion of therapeutic range (INR = 2– 3), sub-therapeutic range (INR < 2), and supra-therapeutic range (INR > 3) were 32.15%, 47.58%, and 17.62%, respectively. One hundred and thirty-eight patients (11.4%) have developed minor or major bleeding complications.
Conclusion: Prolonged immobilization and acute infection were the main risk factors for venous thromboembolism. The quality of anticoagulant therapy in Ethiopia was poor and bleeding complications were high. A strong effort is needed to improve the quality of anticoagulation and close monitoring of patients’ international normalized ratio is required to improve treatment outcomes.
Keywords: anticoagulant, risk assessment, thrombosis, risk factors, venous thromboembolism, Ethiopia
Introduction
Venous thromboembolic diseases (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a leading cause of morbidity and mortality in the world.1,2 It is a serious condition with an incidence of 10% to 30% of people dying within 1 month of diagnosis and one-half of them have long-term complications.3–5 It is also associated with significant cardiac and pulmonary complications such as hypoxemias, increased pulmonary vascular resistance (pulmonary hypertension) leading to right heart failure, and bleeding.6–9
Including Ethiopia, VTE is common in developing countries.10–12 Mortality rate is high, hospitalizations are frequent and associated with worse outcomes with high use healthcare cost.11 Moreover, in developing countries priority, is given to acute disorders, child and maternal health care, and control of communicable diseases; with little emphasis on non-communicable diseases.2,4 Advanced age, malignancy, trauma, post-surgery, obesity, chronic disease, pregnancy, oral contraceptive, long-term immobilization, and HIV infection are the most common risk factors for VTE reported from different studies.6,9,10
Anticoagulation therapies remain the mainstay of VTE treatment, DVT and PE are treated similarly.11 International clinical practice guidelines such as American college chest physicians’ treatment guidelines recommended that injectable anticoagulation should overlap with warfarin therapy for at least 5 days and until an international normalized ratio (INR) ≥2 for at least 24 hours.12 This guideline also emphasizes that unfractionated heparin (UFH) should be weight-based dosing, subcutaneously (initial dose 333 units/kg followed by 250 units/kg twice daily) and intravenous dose (80–100 units/kg loading dose; followed by 18–20 units/kg/hour initial infusion rate). The dose of warfarin should be periodically adjusted to achieve and maintain an INR between 2 and 3 with a duration of treatment of 3 months or longer. These guideline-based treatment approaches were significantly associated with lower death, stroke/coronary heart diseases (CHD), and acute kidney injury (AKI).13 However, these important principles are not evident in resource-limited countries for several reasons, including insufficient laboratory setup, lack of appropriate medications, cost of medications, and discontinuity of care.14 Suboptimum quality of anticoagulation management increases the risk of VTE recurrence, prolonged hospitalization, long-term complication, and increased risk of bleeding.12,15,16
Though several studies were conducted to estimate the magnitude of risk factors of VTE and the quality of anticoagulant therapy in Ethiopia.2,8,11 There is no nationwide study on this area, which is an important research gap. A systematic review is key to improving the accuracy of estimates through the use of more data sets. Thus, this study was aimed to determine the overall magnitude of risk factors of VTE and the quality of anticoagulant therapy in Ethiopia.
Materials and Methods
Search Strategy
An electronic search for studies was done by two (BKS and TK) of the authors from September, 15 to October 27, 2021. PubMed, EMBASE, Science Direct, Cochrane Database, Scopus, Hinari, Sci-Hub, African Journals Online Library, and Free-text Web Searches using Google Scholar were searched for articles. First, articles were searched by using the full titles (“Magnitudes of Venous thromboembolism Risk Factors and quality of anticoagulant therapy in Ethiopia”) and then keywords (Burden, Anticoagulant, Risk assessment, thrombosis, Risk Factors, venous thromboembolism, Deep vein thrombosis, pulmonary embolism, Ethiopia).
Specific names of anti-coagulants, which are available in Ethiopia, including Warfarin, Heparin, and enoxaparin also used as search terms. These keywords were used separately and in combination using Mesh terms and Boolean operators “OR” or NOT “AND”. In addition, we searched from the reference lists of all the included studies (snowball technique) to identify any other studies that may have been missed by our search strategy. All searches were limited to articles written in the English language.
Study Selection Criteria
All available studies and data were incorporated based on the following predefined eligibility criteria.
Inclusion Criteria
- Study setting and period: all studies conducted in Ethiopia from 2000 to October 27, 2021
- Study design: all facility-based observational studies
- Study population: age ≥18 years old with a diagnosis of VTE
- Article types: The published and unpublished studies reporting the risk factors of VTE and/or quality of anticoagulant in terms of INR or Proportion of time spent in the therapeutic range (TTR)
- Language: All searches were limited to articles written in the English language.
Exclusion Criteria
We excluded studies limited to the use of anticoagulant prophylaxis. Furthermore, reviews and systematic review articles, case reports, case series, and articles which were only available in abstract form were excluded. If multiple publications were reported from a similar study, only the most recent or most complete publication for each data set for a specific outcome was selected.
Data Extraction
Essential data were extracted from eligible studies using Microsoft Excel spreadsheet format independently by two (BK and WY) of the authors for data quality and methodological validity. A standard extraction format adapted from the Joanna Briggs Institute (JBI) data extraction form was used to extract data.17 The following information was identified for data extraction: The last name of the first author and year of publication, the region of the study conducted, study design and period, sex of patients, total sample size, risk factors of VTE, number of INR measured, and INR range. Any inconsistencies in the data extraction process were decided through discussion involving all authors.
Article Quality Assessment
The quality assessment of tools was accompanied by two reviewers independently according to the Critical Appraisal Checklist recommended by the Joanna Briggs Institute (JBI).17 Moreover, the disagreements were resolved by consensus and decided by taking the average score of the two reviewers. The JBI checklist was composed of ten questions, the scores ranged from zero to ten. The studies which obtained more than 60% were considered as good quality studies. None of them had poor quality status and all of them were included in the present inquiry.
Data analysis: The data were extracted using a format prepared in Microsoft Excel 2010 and exported to STATA 14.0 (STATA, College Station, TX, USA) for the outcome analyses. Frequency and percentages were computed using descriptive statics for the magnitude of risk factors for VTE. The quality of anticoagulation control (expressed as TTR). TTR was calculated using Rosendaal’s method, which used linear interpolation to assign an INR value to each day between successive observed INR values. This was defined as the proportion of INRs within the therapeutic range of 2.0–3.0 (it was calculated as the number of INRs within the therapeutic range divided by the total number of INR measurements).18
Those individuals with TTR ≥65% were declared as good quality of anticoagulation therapy.19 Accordingly, patients with an INR score of <2, 2–3, and >5 were classified under subtherapeutic, therapeutic, and supratherapeutic range categories, respectively. Prevalence of bleeding complication, defined as the percentage of patients who had bleeding adverse effect out of the total number of study participants. Meta-analysis was not conducted because of the large variability in methodology and geographical region. Since the number of studies from regions was small, they were combined and a percentage of risk factors were generated.
Result
Characteristics of Studies Included in the Analysis
In total, 2, 118 articles were identified. After articles were removed by duplications, titles, and reading the abstract, 103 studies were assessed for eligibility criteria. Consequently, 91 articles were excluded due to different reasons because they were irrelevant. Finally, a total of 12 studies met the inclusion criteria and were included in the final analysis (Figure 1). Of a total of 2182 study participants, 1277 (58.52%) of them were females. The articles were published between 2013 and 2021. Of selected studies, two articles were unpublished (accepted manuscript) which were obtained from Addis Ababa and Gondar University repositories. Most of the studies (9/12, 75%) were cross-sectional studies, others were longitudinal or retrospective observational studies. More than one-third of the studies were conducted in Addis Ababa city (n = 6) followed by Amhara region (n = 3), Oromia region (n = 1), Tigray region (n = 1), Harar regional state (n = 1) and 1 study was multicenter conducted at Addis Ababa, and Oromia regional state (Supplementary Table S1).
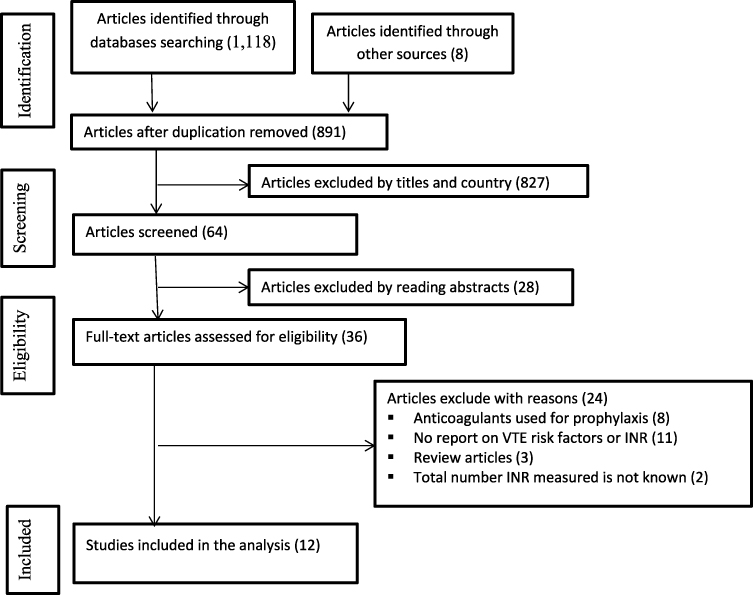 |
Figure 1 Flow diagram of literature search and study selection. |
The Magnitude of Risk Factors for Thromboembolism in Ethiopia
In this systematic review, various factors contribute to thrombotic events among patients in Ethiopia. Prolonged immobilization (41.30%) and acute infection (40.25%) were the most frequently seen VTE risk factors in Ethiopia. Furthermore, history of major bleeding or blood transfusion (26.44), lung disease (non-infectious) (21.48%), and prior history of surgery (21.91%) were also common risk factors for the development of thrombotic events (Table 1).
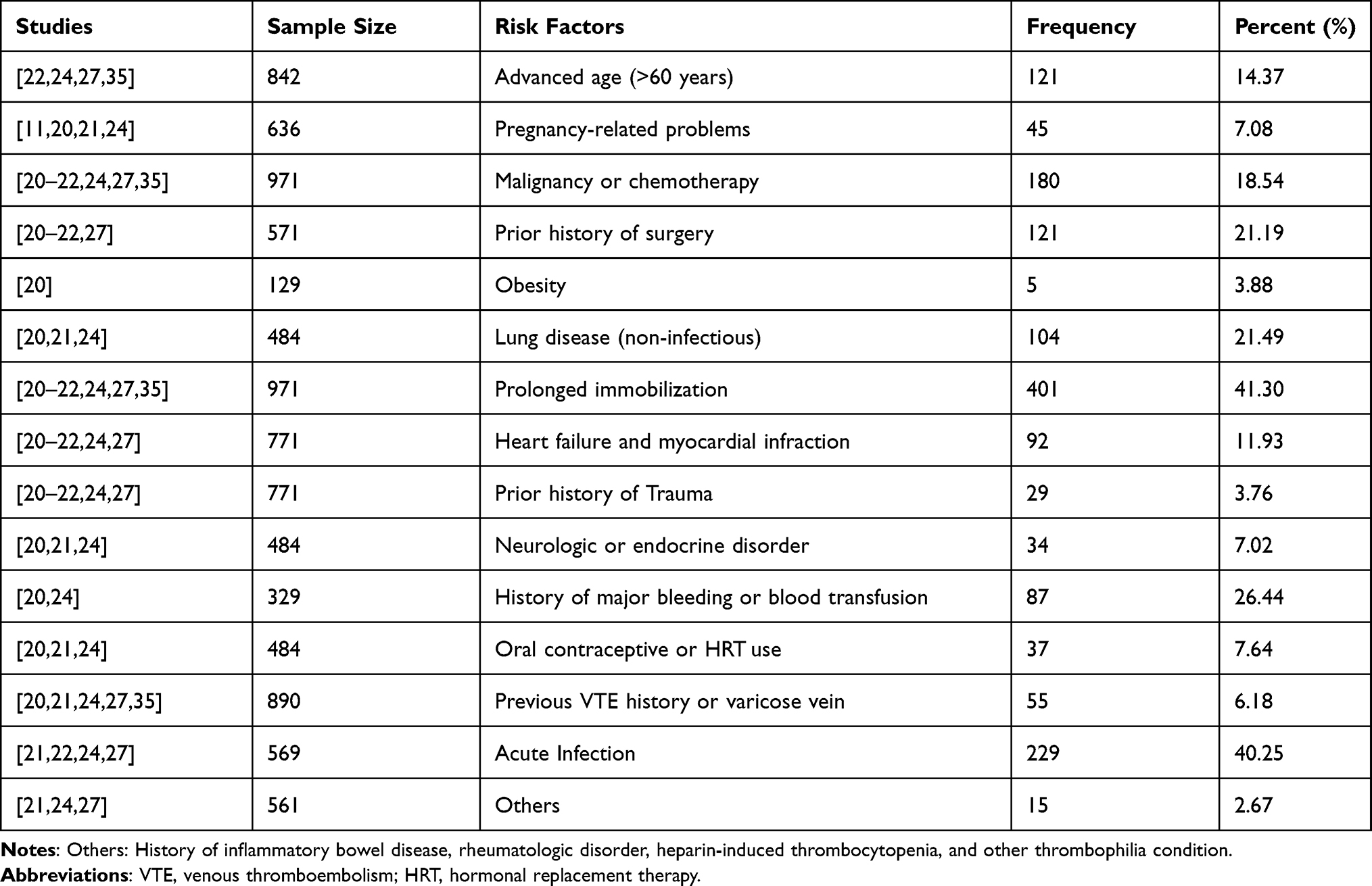 |
Table 1 Magnitude of Risk Factors for Thromboembolism in Ethiopia |
Quality of Anticoagulant Therapy and Incident of Bleeding
A total of 4086 INRs values were recorded from 1211 participants in six studies.23,25,26,28–30 One-third (1330/4086, 32.15%) of study subjects achieved the proportion of INRs within the therapeutic range (INR = 2–3), while nearly half of participants (47.58%) were on the sub-therapeutic range (INR <2), and 17.62% of their time in the supra-therapeutic range (INR >3). From the total, the study participants 11.40% (138/1211) of patients had the bleeding event, which required regular INR determination and dose adjustment (Table 2).
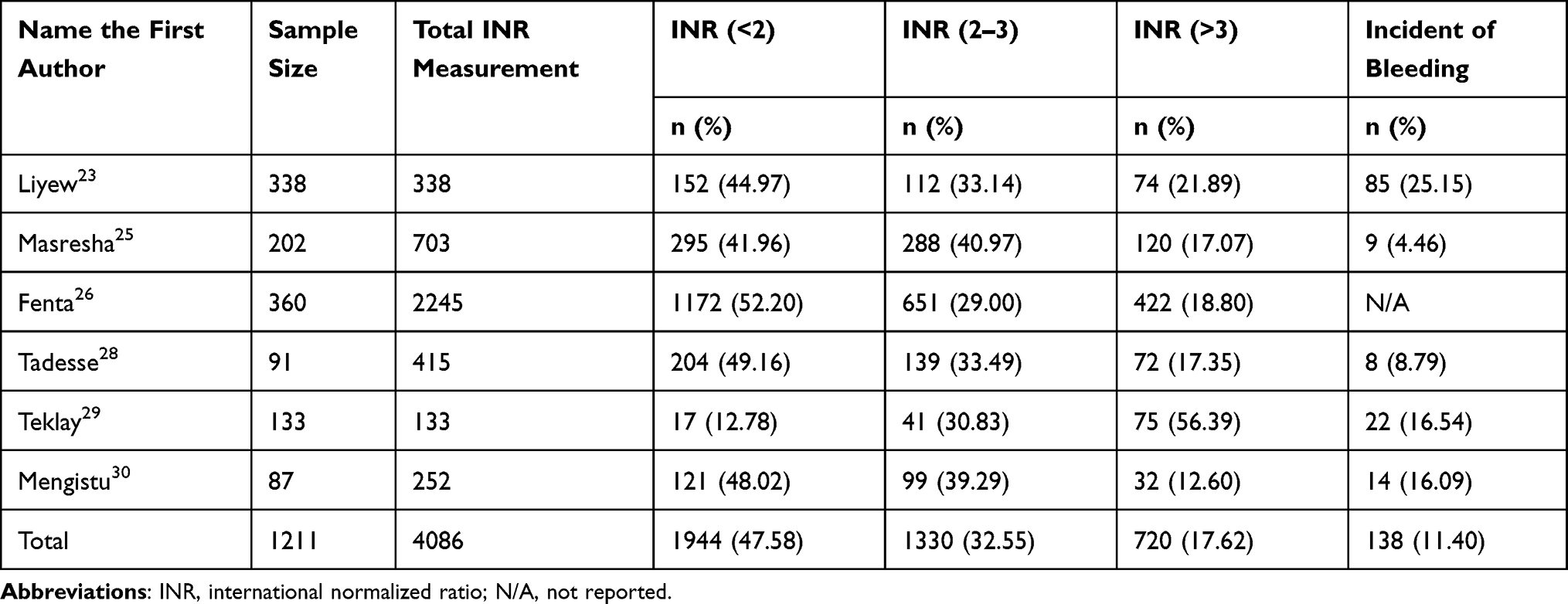 |
Table 2 Quality of Anticoagulant Therapy and Incident of Bleeding in Ethiopia |
Discussion
Risk stratification of VTE patients may assist clinicians and clinical pharmacists in determining the best treatment and the appropriate setting for the initial therapy.4,12 The results of this study indicate that the most commonly noted risk factor for the study population was prolonged immobilization (41.30%). The result was in line with a study done in China.31 A similar study conducted in France showed that prolonged immobilization was the most powerful risk factor of VTE.32 This might be because immobility increases the possibility of a prethrombotic state when the duration is >24 hours, it will be a risk factor if the duration exceeds 3 days. We should pay more attention to the risk of VTE in patients with bed rest. A study conducted in Cameroon explained that the main risk factors of VTE were obesity (44.9%), hypertension (37.2%), and immobility (20.5%).33 On the other hand, a study conducted in India showed malignancy (31.0%) and surgery (30. %) were the major contributors’ risk factors for VTE.34 The different lifestyles, diets, use of VTE prophylaxis during surgery, and disease predominance in these different populations can be a cause of the difference in frequencies of the different risk factors of VTE observed.
Acute infection and the associated systemic inflammation may increase the risk of VTE. Our study revealed that acute infections were the second leading (40.25%) risk factor for VTE. The result was close similarly with studies conducted in Norway (37.8%) and China (45.0%).36,37 A massive localized or generalized inflammatory response with the release of proteases, cytokines, and hormones from multiple tissue and circulatory cells caused extensive damage to the vascular endothelium which played an important role in the pathophysiology of intravascular coagulation.31,38 History of major bleeding or blood transfusion is also another important risk factor in this study. A study conducted in the USA showed that blood transfusion in non-cancer patients is associated with a 3-fold higher risk of being diagnosed with acute VTE.39 This might be explained by major bleeding red blood cell transfusion is a common event. Transfused blood disrupts the balance of coagulation factors and modulates inflammation cascade, which may be associated with the development of VTE.40
In this study, the mean time spent in the therapeutic range was 32.55%. The finding was close similar to study done in Botswana (30.8%), Kenya (39%), and South Africa (32.58%).2,11,19 However, lower than reports from London (57.0%), Netherlands (73%), United State of America (83.0%), Italy (60%), and Spain (66.8%).15,18,41–43 The reason behind this difference may be that their standard of care is much better than the current setting. Prolonged duration of INR monitoring, longer appointment date due to patient load, absence of a standard protocol for anticoagulant therapy, and lack of anticoagulation clinic in Ethiopia might be a potential reason for the poor quality of anticoagulant therapy.
In the current study, out of total INR measured two-thirds of the time (65.2%) was out of the therapeutic range. They spent the majority of their time (47.58%) in the sub-therapeutic range the percentage of sub-therapeutic and supra-therapeutics range in this study was higher than a study in Canada (35% and 11%, respectively).43 Supra-therapeutics range was also higher than the results previously reported (11,-14%).44 This might increase the risk of over anticoagulation and thus expose the patients to a high risk of bleeding complications as supported by different studies.18,19
In this study prevalence of bleeding was found to be 11.40%, which is near to a study carried out in the Worcester VTE study (12%), a study in Kenya (16.9%), and South Africa (14%).3,32,45 However, it was higher than the study done in Japan (2.3%) and Italy, which was 4.2% among patients who received conventional anticoagulant therapy 4.2% and 1.8% in those receiving direct oral anticoagulants.46,47 Different researches show different risk factors such as drugs used, age, concurrent drug use, dose, and duration of treatment were associated with bleeding complications.19,31,41 The risk of bleeding should be an issue of utmost importance. Therefore, these trends should be guided by valid treatment guidelines to improve clinical outcomes and minimize unwanted complications due to anticoagulant drug overdose.
The limitations of the current review include that there may be data not accessible by our search and therefore important measurement on INR value might have been missed. In addition, most of the studies done in Ethiopia did not consider types of anticoagulants, dose, and duration of treatment. Due to these, we did not systematically capture data on these key parameters which might have been useful for creating better prediction on the quality of anticoagulant therapy. Finally, most of the studies were conducted at Addis Ababa, Ethiopia, with different methodologies, and different Clinical and Laboratory Standard guidelines; these may have an impact on the generalizability of the study findings to the entire country. However, this review provides useful information about the burden of risk factors that contributed to the development of VTE. Besides, the review provides insight into the problems on the quality of anticoagulants at the national level to help policymakers to design cost-effective plans and treatment strategies to compact VTE burden and improve treatment outcomes.
Conclusions
Venous thromboembolism is a major public health problem in Ethiopia with diverse clinical risk factors. Prolonged immobilization was the most common risk factor noted for VTE followed by acute infection. The quality of anticoagulant therapy among patients in Ethiopia is poor; two-thirds of INR values were not in the therapeutic range. Importantly, there is a high prevalence of bleeding adverse effects among patients in anticoagulant therapy, possibly due to high event of supra-therapeutic INR range.
Clinicians should always be conscious that patients who have any of the risk factors may develop VTE at any time. Poor TTR reported in this study calls for efforts to improve the level of anticoagulation control among patients on anticoagulants in Ethiopia. Institution-based validated protocol and anti-coagulation clinic would be required to scale-up INR control. In addition, frequent monitoring of INR value is vital to predicting treatment outcomes of patients who received anticoagulants.
Abbreviations
DMCSH, Debre Markos Comprehensive Specialized Hospital; DVT, deep Vein thrombosis; ICU, intensive care unit; INR, international normalized ratio; LMWH, low molecular weight heparin; NCD, non-communicable diseases; PE, pulmonary embolism; UFH, unfractionated heparin; VTE, venous thromboembolism.
Data Sharing Statement
All relevant data are within the manuscript and its Supplementary material.
Author Contributions
Both authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Hodkinson K, Mahlangu J. Deep-vein thrombosis in the era of high HIV and tuberculosis prevalence: a prospective review of its diagnosis and treatment in a quaternary center. South Afr Med J. 2017;107(10). doi:10.7196/SAMJ.2017.v107i10.12443
2. Pastakia SD, Crisp WI, Schellhase EM, Manji I, Ouma MN, Akwanalo C. Implementation of a pharmacist-managed anticoagulation clinic in Eldoret, Kenya. South Med Rev. 2010;3(2):e32.
3. Spencer FA, Emery C, Joffe SW, et al. Incidence rates, clinical profile, and outcomes of patients with venous thromboembolism. The Worcester VTE study. J Thromb Thrombolysis. 2009;28(4):401–409. doi:10.1007/s11239-009-0378-3
4. Cushman M, Tsai AW, White RH, et al. Deep vein thrombosis and pulmonary embolism in two cohorts: the longitudinal investigation of thromboembolism etiology. Am J Med. 2004;117(1):19–25. doi:10.1016/j.amjmed.2004.01.018
5. Nutescu E, Crivera C, Schein J, Bookhart B. Incidence of hospital readmission in patients diagnosed with DVT and PE: clinical burden of recurrent events. Int J Clin Pract. 2015;69(3):321–327. doi:10.1111/ijcp.12519
6. Baser O, Liu X, Phatak H, et al. Venous thromboembolism prophylaxis and clinical consequences in medically ill patients. Am J Ther. 2013;20(2):132–142. doi:10.1097/MJT.0b013e31826910dd
7. Shiferaw F, Letebo M, Misganaw A, et al. Non-communicable Diseases in Ethiopia: disease burden, gaps in health care delivery and strategic directions. Ethiop J Health Dev. 2018;32(3):1–12.
8. Tefera YG, Abegaz TM, Abebe TB, Mekuria AB. The changing trend of cardiovascular disease and its clinical characteristics in Ethiopia: a hospital-based observational study. Vasc Health Risk Manag. 2017;13:143. doi:10.2147/VHRM.S131259
9. Fischer CR, Wang E, Steinmetz L, et al. Prevalence of risk factors for hospital-acquired venous thromboembolism in neurosurgery and orthopedic spine surgery patients. Int j Spine Surg. 2020;14(1):79–86. doi:10.14444/7011
10. Beckman MG, Hooper WC, Critchley SE, Ortel TL. Venous thromboembolism: a public health concern. Am J Prev Med. 2010;38(4):495–501. doi:10.1016/j.amepre.2009.12.017
11. Tiryaki F, Nutescu EA, Hennenfent JA, et al. Anticoagulation therapy for hospitalized patients: patterns of use, compliance with national guidelines, and performance on quality measures. Am J Health Syst Phar. 2011;68(13):1239–1244. doi:10.2146/ajhp100543
12. Bates SM, Jaeschke R, Stevens SM, et al. Diagnosis of DVT: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2012;141(2):351–419. doi:10.1378/chest.11-2299
13. Durand WM, Goodman AD, Johnson JP, Daniels AH. Assessment of 30-day mortality and complication rates associated with extended deep vein thrombosis prophylaxis following hip fracture surgery. Injury. 2018;49(6):1141–1148. doi:10.1016/j.injury.2018.03.019
14. Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: A Pathophysiologic Approach.
15. Gallagher AM, de Vries F, Plumb JM, Haß B, Clemens A, van Staa T-P. Quality of INR control and outcomes following venous thromboembolism. Clin Appl Thromb/Hemost. 2012;18(4):370–378. doi:10.1177/1076029611426139
16. Liu S, Singer A, McAlister FA, et al. Quality of warfarin management in primary care: determining the stability of international normalized ratios using a nationally representative prospective cohort. Can Fam Physician. 2019;65(6):416–425.
17. Peters M, Godfrey C, McInerney P, Soares C, Khalil H, Parker D. The Joanna Briggs Institute reviewers’ manual 2015: a methodology for JBI scoping reviews; 2015.
18. Boon GJ, Rein NV, Bogaard HJ, et al. Quality of initial anticoagulant treatment and risk of CTEPH after acute pulmonary embolism. PLoS One. 2020;15(4):e0232354.
19. Mwita JC, Francis JM, Oyekunle AA, Gaenamong M, Goepamang M, Magafu MG. Quality of anticoagulation with warfarin at a tertiary hospital in Botswana. Clin Appl Thromb/Hemost. 2018;24(4):596–601. doi:10.1177/1076029617747413
20. Mulatu A, Melaku T, Chelkeba L. Deep venous thrombosis recurrence and its predictors at selected tertiary hospitals in Ethiopia: a Prospective Cohort Study. Clin Appl Thromb/Hemost. 2020;26:1–14. doi:10.1177/1076029620941077
21. Tadesse TA, Kedir HM, Fentie AM, Abiye AA. Venous thromboembolism risk and thromboprophylaxis assessment in surgical patients based on caprini risk assessment model. Risk Manag Healthc Policy. 2020;13:2545. doi:10.2147/RMHP.S272852
22. Haile L, Hawaz Y, Assefa G. Risk factors of deep venous thrombosis in duplex and color Doppler ultrasound at Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia. East Cent Afr J Surg. 2013;18(2):61–69.
23. Liyew Z, Bekele N, Tsegaye T. Evaluation of anticoagulation outcome among patients taking Warfarin: a single-center experience, Northwest Ethiopia; 2021: 1–15.
24. Ahmed F, Hussen S, Assefa T. Venous thromboembolism risk, prophylaxis and outcome in hospitalized patients to medical wards of university teaching hospital. J Clin Exp Cardiolog. 2019;10(621):2–7. doi:10.4172/2155-9880.1000620
25. Masresha N, Muche EA, Atnafu A, Abdela O. Evaluation of warfarin anticoagulation at university of Gondar comprehensive specialized hospital, North-West Ethiopia. J Blood Med. 2021;12:189. doi:10.2147/JBM.S282948
26. Fenta TG, Assefa T, Alemayehu B. Quality of anticoagulation management with warfarin among outpatients in a tertiary hospital in Addis Ababa, Ethiopia: a retrospective cross-sectional study. BMC Health Serv Res. 2017;17(1):1–7. doi:10.1186/s12913-017-2330-0
27. Ayalew MB, Horsa BA, Zeleke MT. Appropriateness of pharmacologic prophylaxis against deep vein thrombosis in medical wards of an Ethiopian referral hospital. Int J Vasc Med. 2018;2018:1–7. doi:10.1155/2018/8176898
28. Tadesse F, Engidawork E. Drug-related problems and potential contributing factors in the management of deep vein thrombosis. BMC Hematol. 2016;16(1):1–8. doi:10.1186/s12878-015-0037-1
29. Teklay G, Shiferaw N, Legesse B, Bekele ML. Drug-drug interactions and risk of bleeding among inpatients on warfarin therapy: a prospective observational study. Thromb J. 2014;12(1):1–8. doi:10.1186/1477-9560-12-20
30. Mengistu G, Lemma B, Molla M. Utilization patterns of anticoagulants at the medical ward of hiwot fana Specialized university hospital, Harar, Ethiopia. J Basic Clin Pharm. 2017;8(4):235–238.
31. Wang H, Ye J, Wang L, Jin W. Risk characteristics of venous thromboembolism in Chinese patients. Clin Appl Thromb/Hemost. 2016;22(5):490–494. doi:10.1177/1076029615569272
32. Obayo A, Ngunga M, Shah J, Sokwala A, Barasa A. Bleeding complications in patients on new oral anticoagulants for venous thromboembolism in Kenya; 2021: 2–16.
33. Kamdem F, Ngahane BHM, Hamadou B, et al. Epidemiology, clinical presentations and in-hospital mortality of venous thromboembolism at the Douala General Hospital: a cross-sectional study in Cameroon, Sub-Saharan Africa. World J Cardiovasc Dis. 2018;8(02):123–128. doi:10.4236/wjcd.2018.82012
34. Lee AD, Stephen E, Agarwal S, Premkumar P. Venous thrombo-embolism in India. Eur J Vasc Endovasc Surg. 2009;37(4):482–485. doi:10.1016/j.ejvs.2008.11.031
35. Negash N. Practice of venous thromboembolism prophylaxis in hospitalized patients at Tikur Anbessa specialized hospital according to the existing guideline; 2019: 1–29.
36. Grimnes G, Isaksen T, Tichelaar YV, Brækkan SK, Hansen JB. Acute infection as a trigger for incident venous thromboembolism: results from a population‐based case‐crossover study. Res Pract Thromb Hemost. 2018;2(1):85–92. doi:10.1002/rth2.12065
37. Zhou H, Hu Y, Li X, et al. Assessment of the risk of venous thromboembolism in medical inpatients using the Padua prediction score and Caprini risk assessment model. J Atheroscler Thromb. 2018;43653:2–14.
38. Yu Y, Shen Y, Li J, Liu J, Liu S, Song H. Viral infection-related venous thromboembolism: potential mechanism and therapeutic targets. Ann Palliat Med. 2020;9(3):1257–1263. doi:10.21037/apm.2020.04.05
39. Rogers MA, Levine DA, Blumberg N, Flanders SA, Chopra V, Langa KM. Triggers of hospitalization for venous thromboembolism. Circulation. 2012;125(17):2092–2099. doi:10.1161/CIRCULATIONAHA.111.084467
40. White RH. Identifying risk factors for venous thromboembolism. Circulation. 2012;125:2051–2053. doi:10.1161/CIRCULATIONAHA.112.102814
41. Manzoor BS, Cheng WH, Lee JC, Uppuluri EM, Nutescu EA. Quality of pharmacist-managed anticoagulation therapy in long-term ambulatory settings: a systematic review. Ann Pharmacother. 2017;51(12):1122–1137. doi:10.1177/1060028017721241
42. Van Dongen CJ, Prandoni P, Frulla M, Marchiori A, Prins MH, Hutten BA. Relation between quality of anticoagulant treatment and the development of the postthrombotic syndrome. J Thromb Haemost. 2005;3(5):939–942. doi:10.1111/j.1538-7836.2005.01333.x
43. Roca RA, Guerrero CA, de Paz VM, et al. Quality control of oral anticoagulant therapy in Primary Care in Madrid City, Spain: CHRONOS-TAO study. Med Clín. 2015;145(5):192–197.
44. Aspinall SL, Zhao X, Handler SM, et al. The quality of warfarin prescribing and monitoring in Veterans Affairs nursing homes. J Am Geriatr Soc. 2010;58(8):1475–1480. doi:10.1111/j.1532-5415.2010.02967.x
45. Sonuga B. Profile and anticoagulation outcomes of patients on warfarin therapy in an urban hospital in Cape Town: a review of records of patients attending Victoria Hospital, Cape Town, South Africa (Master’s thesis, University of Cape Town. MMED Fam Med. 2015;5:4–32.
46. Nakamura M, Miyata T, Ozeki Y, et al. Current venous thromboembolism management and outcomes in Japan. Circ J. 2014;78(3):708–717.
47. Margaglione M, Antonucci E, D’Andrea G, et al. Anticoagulation in Italian patients with venous thromboembolism and thrombophilic alterations: findings from START2 register study. Blood Transfus. 2020;18(6):486–489. doi:10.2450/2020.0091-20
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.