")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Magnitude of Pre-Existing Diabetes Mellitus Among Pregnant Women in Southern Ethiopia: A Cross-Sectional Study
Authors Wolka E , Deressa W , Reja A
Received 17 November 2020
Accepted for publication 24 February 2021
Published 12 March 2021 Volume 2021:14 Pages 1025—1031
DOI https://doi.org/10.2147/RMHP.S292000
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Eskinder Wolka,1 Wakgari Deressa,2 Ahmed Reja3
1School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2Department of Preventive Medicine, School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Eskinder Wolka
School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, P.O. Box: 138, Sodo, Ethiopia
Fax +251465515216
Email [email protected]
Background: The presence of maternal diabetes mellitus (DM) during pregnancy has complications for both mother and child. Pre-existing DM can result in higher risk of maternal and child mortality and morbidity. In Ethiopia, the magnitude of pre-existing DM among pregnant women is not well studied. The aim of this study was to assess the magnitude of pre-existing DM among pregnant women in Wolaita Zone, Southern Ethiopia.
Methods: A retrospective document review was carried out to determine the magnitude of pre-existing DM in three hospitals and four health centers in Wolaita Zone, Southern Ethiopia. A total of 600 pregnant mothers who attended maternity services at the study health facilities in one year period from January 1, to December 31, 2017 were included in the study. Data were collected from medical records of mothers. Chi-square and logistic regression analysis model were used to check the relationship between pre-existing DM and independent variables.
Results: A total of 600 mothers were included in the analysis. The magnitude of pre-existing DM among mothers receiving maternity care within a one year period was 2.8% (95% CI: 1.5, 4.2). The magnitudes among urban and rural residents were 3.4% and 1.4%, respectively. Pre-existing DM is significantly associated with family history of diabetes (Chi square 24.8, P-value, 0.001). Previous history of spontaneous abortion (aOR: 5.3; 95% CI: 1.6– 17.4) and fetal macrosomia (aOR: 3.9; 95% CI: 1.2– 13.1), was identified to be significantly associated with pre-existing DM. The magnitude of pre-existing DM is comparable with International Diabetes Federation Estimate to Ethiopia in the study area. Family history of DM was found to be associated with pre-existing DM. Pre-existing DM is associated with increased risk of abortion and fetal macrosomia.
Conclusion: The magnitude of pre-existing DM is comparable with previous estimates to the country. A nationwide, large-scale study is important to estimate the burden of pre-existing DM and associated risk factors among pregnant mothers at national level.
Keywords: pre-existing diabetes mellitus, Southern Ethiopia, Wolaita Zone
Introduction
Diabetes mellitus (DM) in pregnancy can happen in two ways; one is pre-existing DM and the other is gestational diabetes mellitus. Pre-existing DM refers to pregnant women who have previously been diagnosed with type I or type II DM, or other rare types of DM and extended to the period of pregnancy.1,2 Pre-existing DM can be also described as pre-gestational diabetes and it is already identified diabetes and continued through pregnancy.3
Currently, DM is considered as one of the top health problems of the world. The World Health Organization (WHO) estimated that, globally, hyperglycemia is the third highest risk factor for premature mortality, next to high blood pressure and tobacco use.4 The world estimate is that 8.8% (415 million) adults aged 20–79 were affected by DM in 2015, with little gender difference. The prevalence in Africa was estimated to be 3.2% (14.2 million) in 2015 and nearly half of these cases live in four populous countries of Africa; namely, Nigeria, Ethiopia, Democratic Republic of Congo and South Africa. The International Diabetes Federation estimated that, the adult prevalence of DM in Ethiopia in 2015 was 2.9%.5
Pregnant mothers affected by pre-existing DM can develop different complications and will have a higher risk of maternal and child mortality and morbidity.6 Both short- and long-term complications were reported among mothers with DM and infants of mothers with pre-existing DM. Acute pregnancy complications such as pre-eclampsia, infections, obstructed labour, postpartum hemorrhage, preterm births, stillbirths, birth injuries, and death in worst case scenarios, were documented in mothers with DM.7,8 In addition, the chance of an early miscarriage is higher for women with DM and the maternal mortality ratio among diabetic mothers in some countries increases up to twenty-fold when compared with non-diabetic mothers.9
Chronic complications like congenital malformation, neural tube defect and congenital heart diseases can occur among infants of mothers with pre-existing diabetes. Diabetes can also affect multiple systems, including skeletal, cardiac, central nervous, gastrointestinal, and genitourinary systems.10 In addition, the infants of mothers with pre-existing DM are at higher risk of developing type II DM and obesity in the long term.11 Kidney and eye complications, and the risk of myocardial infarction is significantly increased in women with type I DM as long-term effects.12
Appropriate diagnosis, care, and management of DM before and during pregnancy are important to minimize the risk of long- and short-term complications. Controlling blood sugar through a healthy diet, gentle exercise, and blood glucose monitoring, and in some cases insulin or oral medication, can prevent harm.13
In Ethiopia, although DM is recognized as one of the major non-communicable diseases, the magnitude of pre-existing diabetes among pregnant women is not well studied. Documenting the burden of pre-existing DM is very important to inform health policies and programs to mitigate the problem in the country.
The aim of this study was to assess the magnitude of pre-existing DM among pregnant women in Wolaita Zone, Southern Ethiopia.
Methods
Study Area and Period
The study was conducted in three hospitals and four health centers in Wolaita Zone, Southern Ethiopia. The Zone is located in the South Central part of the country, 385 km distance from the capital, Addis Ababa. The Zone has total population of about 2 million in 2017 as projected from 2007 national census. The study area in general has 12 administrative districts and three town administrations. Likewise this area share 3 Hospitals, 70 health centers and 380 health posts, among these, 12 Health Centers and all 3 hospitals provide diagnostic and management care for pregnant women with DM. The estimated number of pregnant women in the zone in 2016 was 66,646.14 Data were collected in three month period from January to March, 2018.
Study Design and Population
A retrospective document review was carried out to determine the magnitude of pre-existing DM among pregnant women. All pregnant mothers who attended maternity services in the study hospitals and health centers during the period January 1, to December 31, 2017 were included in the study.
Sampling Size and Sampling Procedure
Sample size was calculated by using single proportion formula by considering the following assumptions; confidence level of 95%, expected proportion 50% to get maximum sample size, margin of error 4%, Z - α ⁄2, Z value corresponding to a 95% level of significance = 1.96. By using the formula; n= (Z α ⁄2)2 P (1-P)/e2.
The total sample sizes used for the study were 600.
The total sample was assigned to study facilities proportionally based on case load and systematic sampling method was used to identify the assigned number from maternal medical records.
Data Collection
Data collection was carried out between January and March 2018, from maternal medical records using structured checklist. Completed documents for the intended study were included for data extraction and pre-existing diabetes was identified based on confirmed diagnoses by physicians in the registry. Data extraction was performed from selected documents in study facilities. Data were collected by nurses and midwives who have ample experience on clinical practice and data collection. Intensive training was given to data collectors and supervisors on how to extract data from medical records. Continuous supervision was in place during data collection time. The supervisors ensured data completeness and consistency on a daily basis.
Data Analysis
Data were entered and cleaned by Epi Info version 7 and analyzed using STATA version 14 software. Tables and figures were used to present the descriptive data. Chi-square and logistic regression analysis models were used to check the relationship between dependent and independent variables. Model fitness was evaluated by Hosmer-Lemeshow goodness-of-fit tests.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of College of Health Sciences, Addis Ababa University. A letter of permission was written by the Wolaita Zone health department to all study facilities. Facility administrators confirmed their willingness to provide all necessary documents and information for the study. Confidentiality and anonymity of all the information obtained from medical records and registers were maintained. In all processes of this research, the study complied with the Declaration of Helsinki.
Results
Socio-Demographic and Obstetric Characteristics
Of the 600 mothers included in the analysis, more than two-thirds (68.8%) were aged between 21 and 30 years. Nearly all (98.9%) were married and most of the women (75.7%) were urban residents. One, two and three pregnancies were documented for 36.8%, 33.0%, and 15.5% of mothers, respectively. More than half (55.8%), of the mothers had at least one live birth before index pregnancy. The distribution of women in relation to age, residence, marital status, gravidity, and parity is presented in Table 1.
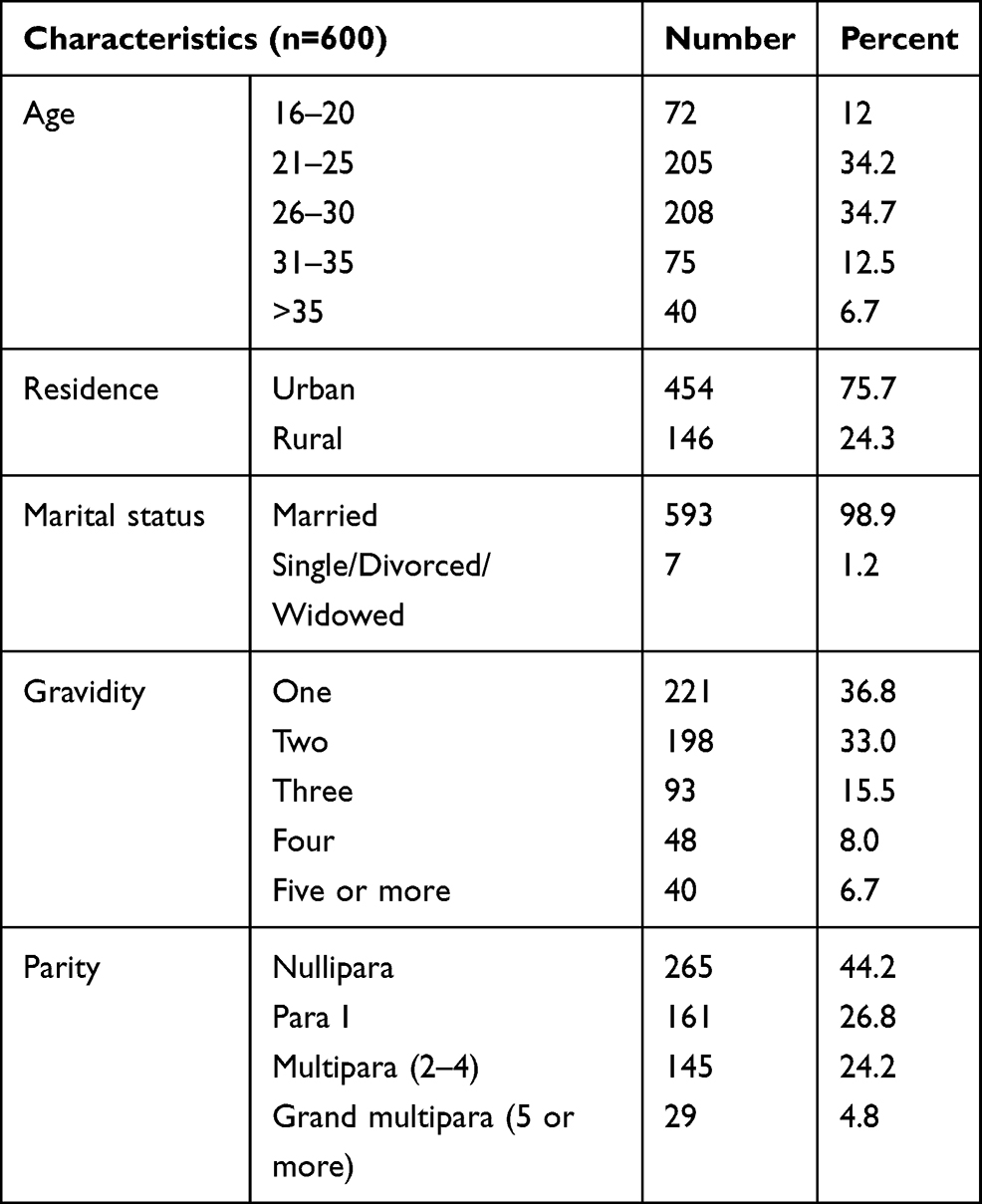 |
Table 1 Selected Socio-Demographic Characteristics of Respondents, Wolaita Zone, Southern Ethiopia, 2017 |
Maternal and Fetal Complications
Basic maternal and fetal complications were assessed in this study. The magnitude of pre-eclampsia among mothers was 5.7%. According to medical records, 2.7% and 5% of mothers had still births and preterm deliveries, respectively. Macrosomia was documented in 7.2% of mothers and caesarean section rate was 10.5%. Abortion complications were recorded in 10% of mothers and 3 cases of early neonatal death occurred (Table 2).
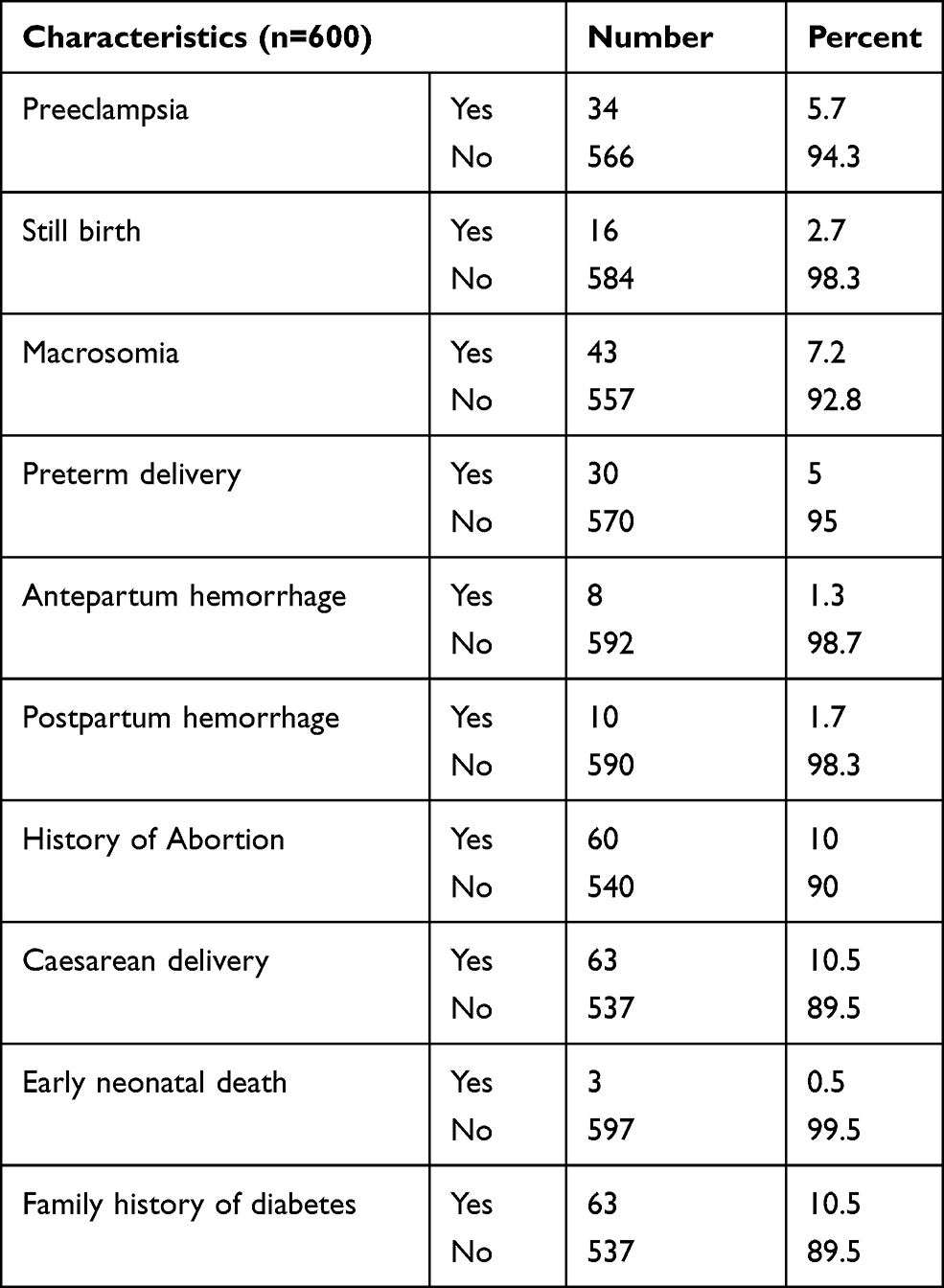 |
Table 2 Selected Obstetric Characteristics of Respondents, Wolaita Zone, Southern Ethiopia, 2017 |
Magnitude of Pre-Existing Diabetes Mellitus
The magnitude of pre-existing diabetes among mothers receiving maternity care within a one year period from January 1, 2017 to December 31, 2017 in study area was 2.8% (95% CI: 1.5, 4.2). The magnitude among urban and rural residents were 3.4% and 1.4%, respectively. Of 17 cases of pre-existing diabetes, 12 cases were type II DM and the remaining 5 cases were type I DM. No cases of pre-existing DM were documented for mothers aged less than 20and the highest proportion (8.0%) was identified for mothers aged more than 35 years (Figure 1).
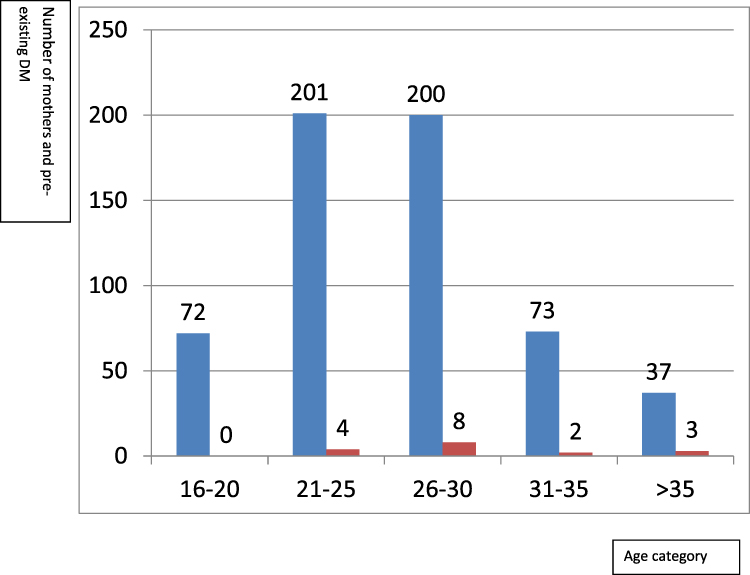 |
Figure 1 Number of pre-existing diabetes mellitus cases according to age category, Wolaita Zone, Southern Ethiopia, 2017. Notes: Blue – total number of mothers. Red – number of DM. |
The highest proportion of pre-existing DM was documented for mothers with 3 or more pregnancies and none for women in their first pregnancy (Figure 2).
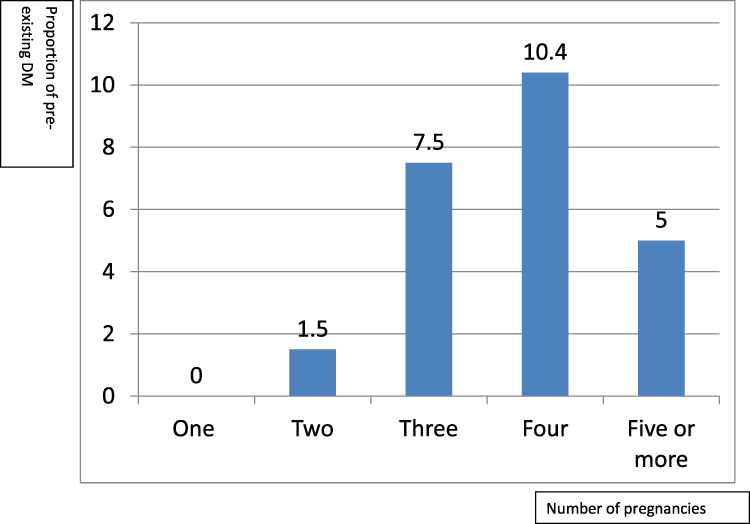 |
Figure 2 Proportion of pre-existing diabetes mellitus cases according to number of pregnancies, Wolaita Zone, Southern Ethiopia, 2017. Note: Blue – proportion of pre-existing diabetes per number of pregnancy. |
The mean age (standard deviation) of mothers with pre-existing DM was 31.8 (±5.1) and for those without diabetes was 26.7 (±5.0). Diabetic mothers were significantly older (P- value, 0.001) than non-diabetic mothers.
The results showed that a higher proportion of mothers with DM had pre-eclampsia than non-diabetic mothers (23.5% versus 4.8%). Based on the study, 29.4% of mothers with diabetes had a caesarean section delivery and for non-diabetic mothers it was 9.9%.
Factors Associated with Pre-Existing Diabetes Mellitus
Pre-existing DM is significantly associated with family history of diabetes (Chi square 24.8, P-value, 0.001). Binary logistic regression model was used to assess the relationship between some variables and pre-existing DM. In a multivariate logistic regression model, previous history of spontaneous abortion (aOR: 5.3; 95% CI: 1.6–17.4) and fetal macrosomia (aOR: 3.9; 95% CI: 1.2–13.1), were identified to be significantly associated with pre-existing diabetes.
Discussion
The study assessed the magnitude of pre-existing DM among mothers receiving maternity care in 3 hospitals and 4 health centers between January 1 and December 31, 2017, in Wolaita Zone, Southern Ethiopia. A total of 600 mothers were included in the analysis; nearly all, (98.9%), were married and three quarters of the women (75.7%), were urban residents. From these findings we can see that the majority of maternity service users in the study facilities were urban dwellers. More than half (55.8%) of the mothers included in our study had at least one live birth before index pregnancy and the number of multigravida women included in the study was higher than the number of primigravida women.
The magnitude of pre-existing DM among mothers receiving maternity care during a one year period in study area was 2.8% (95% CI; 1.5–4.2). The magnitudes among urban and rural residents were 3.4% and 1.4%, respectively. The majority (70.5%) of pre-existing DM were type II DM and the remaining 5 caseswere type I DM. This figure is comparable with the adult diabetes prevalence estimate of the World Diabetes Federation for Ethiopia.5 The magnitude is lower than the finding of a facility-based retrospective cohort study conducted in Saudi Arabia.15
In this study, some demographic characteristics of women with pre-existing DM were compared with non-diabetic mothers. The findings suggested that diabetic mothers were significantly older than non-diabetic women and this was documented by evidence from other studies.16
The result showed that a higher proportion of mothers with DM had pre-eclampsia than non-diabetic mothers. It was reported that a pregnancy associated with diabetes is commonly complicated with pregnancy-induced hypertension and preeclampsia.7,17
Caesarean section delivery increased three-fold among mothers with DM. The reason behind the tendency towards delivery by caesarean section can be linked to a higher rate of macrosomia occuring among diabetic mothers. This finding is supported by other studies that reported women with pre-existing DM are more likely to be delivered by caesarean section.16,18
Our study revealed that there is association between family history of diabetes and pre-existing DM among pregnant mothers. The International Diabetes Federation report indicated that some factors which play a significant role in pre-existing diabetes generally include obesity, unhealthy diets, physical inactivity, family history of DM, and maternal age.5
Persistent high blood sugar level in mothers can have influence on fetal growth and weight and having a big baby is also related to maternal diabetes.19 In our study, fetal macrosomia is 4.9 times more likely to occur among diabetic mothers. Macrosomia can result in obstetric complications like caesarean delivery, birth asphyxia, or perinatal mortality.20
Based on the results, abortion is more common among mothers with DM when compared with non-diabetic mothers. It is supposed that hyperglycemia could cause damage to the developing yolk sac, an increased production and liberation of free oxygen radicals and genotoxic effect might occur and this may result in damage to the fetus and miscarriages.21
This study was limited to assess the magnitude of pre-existing DM among mothers who received care in health facilities and it did not address those mothers who had not visited the studied health facilities during the study period.
Conclusions
The results of this study showed that 2.8% of women receiving maternity cares in the study area have pre-existing DM, and that diabetic women were significantly older. Family history of diabetes is found to be associated with pre-existing diabetes. Pre-existing DM is associated with increased risk of abortion and fetal macrosomia. A higher proportion of mothers with DM had pre-eclampsia and caesarean delivery. Special attention should be given to pregnant mothers with pre-existing DM during antenatal care to control and manage hyperglycemia effectively. A nationwide large-scale study is important to estimate the burden of pre-existing DM among pregnant mothers at a national level and its effect on maternal and birth outcomes.
Data Sharing Statement
Data is available up on request from corresponding author.
Ethical Approval
Ethical approval was obtained from the Institutional Review Board of College of Health Sciences, Addis Ababa University. Letter of permission was written by Wolaita Zone health department to all study facilities. Facility administrators confirmed their willingness to provide all necessary documents and information for the study. Confidentiality of all the information obtained from medical records and registers was maintained.
Acknowledgments
The authors acknowledge Addis Ababa University, Wolaita Sodo University, Wolaita Zone Health Department, officials of study facilities, data collectors and supervisors for their contribution for the success of this study.
Disclosure
The authors declare that there is no conflict of interests.
References
1. International Diabetes Federation. Diabetes Report. Brussels, Belgium; 2009.
2. Alberti K, Zimmet P, Shaw J. A consensus of type 2 diabetes prevention. Diabet Med. 2007;24:451–463. doi:10.1111/j.1464-5491.2007.02157.x
3. Gabbe SG, Graves CR. Management of diabetes mellitus complicating pregnancy. Obstet Gynecol. 2003;102(4):857–868. doi:10.1016/j.obstetgynecol.2003.07.001
4. World Health Organization. Global health risks: mortality and burden of disease attributable to selected major risks. Geneva, Switzerland: WHO; 2009.
5. International Diabetes Federation. Diabetes Atlas. Brussels, Belgium; 2015.
6. Jensen DM, Damm P, Moelsted PL, et al. Outcomes in type 1 diabetic pregnancies. Diabetes Care. 2004;27(12):2819–2823. doi:10.2337/diacare.27.12.2819
7. Moore T, Smith C. Diabetes mellitus and pregnancy. Medscape drugs, diseases and procedures reference; 2012.
8. Macintosh MC, Fleming MK, Bailey JA, et al. Perinatal mortality and congenital anomalies in babies of women with type 1 or type 2 diabetes in England, Wales, and Northern Ireland, population based study. BMJ. 2006;333:177. doi:10.1136/bmj.38856.692986.AE
9. Pekka J, Leinonen MD, Vilho K, et al. Maternal mortality in type 1 diabetes. Diabetes Care. 2001;24(8):101–1502.
10. Correa A, Gilboa SM, Besser ML, et al. Diabetes mellitus and birth defects. Am J Obstet Gynecol. 2008;199(3):277e1–9. doi:10.1016/j.ajog.2008.06.028
11. Dabelea D, Knowler WC, Pettitt DJ. Effect of diabetes in pregnancy on offspring: follow-up research in the Pima Indians. J Maternal Fetal Med. 2000;9(1):83–88. doi:10.1002/(SICI)1520-6661(200001/02)9:1<83::AID-MFM17>3.0.CO;2-O
12. Sheth BP. Does pregnancy accelerate the rate of progression of diabetic retinopathy?. Current Diabetes Rep. 2002;2(4):227–330. doi:10.1007/s11892-002-0022-5
13. Hod M. Pregnancy outcome of diabetic women 15 years after the St. Vincent declaration: success or failure?. Endocrinol Nutr. 2005;52(10):271–274. doi:10.1016/S1575-0922(05)71067-6
14. Wolaita Zone Health Department. Annual report; 2016
15. Wahabi HA, Esmaeil SA, Fayed A, et al. Pre-existing diabetes mellitus and adverse pregnancy outcomes. BMC Res Notes. 2012;5:496. doi:10.1186/1756-0500-5-496
16. El Mallah KO, Narchi H, Kulaylat NA, et al. Gestational and pre-gestational diabetes: comparison of maternal and fetal characteristics and outcome. Int J Gynaecol Obstet. 1997;58:203–209. doi:10.1016/S0020-7292(97)00084-2
17. Lapolla A, Dalfra MG, Di CG, et al. A multicenter Italian study on pregnancy outcome in women with diabetes. Nutr Metab Cardiovasc Dis. 2008;18:291–297. doi:10.1016/j.numecd.2006.12.001
18. Barakat MN, Youssef RM, Al-Lawati JA. Pregnancy outcomes of diabetic women: charting Oman’s progress towards the goals of the Saint Vincent Declaration. Ann Saudi Med. 2010;30:265–270. doi:10.4103/0256-4947.65253
19. Rackham O, Paize F, Weindling AM. Cause of death in infants of women with pregestational diabetes mellitus and the relationship with glycemic control. Postgrad Med. 2009;121:26–32. doi:10.3810/pgm.2009.07.2026
20. Ojule JD, Fiebai PO, Okongwu C. Perinatal outcome of macrosomic births in Port Harcourt. Niger J Med. 2010;19:436–440. doi:10.4314/njm.v19i4.61971
21. Reece EA, Homko C. Why do diabetic women deliver malformed infants?. Clin Obstet Gynecol. 2000;43:32–45. doi:10.1097/00003081-200003000-00004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.