Back to Journals » Clinical Ophthalmology » Volume 17
Magnitude of Maladaptive Coping Strategy and Its Associated Factors Among Adult Glaucoma Patients Attending Tertiary Eye Care Center in Ethiopia
Authors Birhan GS ![]() , Belete GT
, Belete GT ![]() , Eticha BL
, Eticha BL ![]() , Ayele FA
, Ayele FA
Received 25 November 2022
Accepted for publication 24 February 2023
Published 3 March 2023 Volume 2023:17 Pages 711—723
DOI https://doi.org/10.2147/OPTH.S398990
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Getenet Shumet Birhan,1 Gizachew Tilahun Belete,1 Biruk Lelisa Eticha,1 Fisseha Admassu Ayele2
1Department of Optometry, School of Medicine, University of Gondar, Comprehensive Specialized Hospital, Gondar, Ethiopia; 2Department of Ophthalmology, School of Medicine, University of Gondar, Comprehensive Specialized Hospital, Gondar, Ethiopia
Correspondence: Biruk Lelisa Eticha, POB: 196, Tel +251921950568, Fax +251-58-114 1240, Email [email protected]
Introduction: Coping strategy is the mechanism by which patients adjust to the condition they face. It can be adaptive or maladaptive. A maladaptive coping strategy is a harmful and ineffective way of dealing with stress or anxiety. It is common among patients with chronic illnesses. Despite Ethiopia having a greater glaucoma prevalence, there was no evidence of patients with glaucoma using maladaptive coping mechanisms.
Objective: The main goal of this study was to evaluate the magnitude of maladaptive coping strategy use and the factors that associate with it among adult glaucoma patients enrolled in the Tertiary Eye Care and Training Center at the University of Gondar in Northwest Ethiopia in 2022.
Methods and Materials: At the University of Gondar, Tertiary Eye Care and Training Center, a facility-based cross-sectional study was carried out on a sample of 423 glaucoma patients chosen by a systematic random sampling technique from May 15 to June 30, 2022. Optometrists conducted an interview with the study subject and reviewed the medical record, and administered a pretested, structured questionnaire of the brief cope inventory assessment. In the multivariable logistic regression, binary logistic regression was performed to identify the related factors, and significance was taken into account when the p-value was less than 0.05 at the 95% confidence interval.
Results: The study found that among study participants 50.1% (95% CI: 45.1– 54.5%) had a maladaptive coping strategy. Female sex (AOR=2.031, 95% CI:1.185– 3.480), chronic medical illness (AOR=1.760, 95% CI:1.036– 2.989), bilateral glaucoma (AOR=2.321, 95% CI: 1.328– 4.055), receiving both drug and surgery treatment (AOR=1.895, 95% CI: 1.002– 3.585), severe visual impairment (AOR=2.758, 95% CI:1.110– 6.852), absolute glaucoma (AOR=2.543, 95% CI:1.048– 6.169), duration of diagnosis > 12 months (AOR=3.886, 95% CI: 2.295– 6.580) were significantly associated with a maladaptive coping strategy.
Conclusion and Recommendation: Half of the participants had a maladaptive coping strategy. It is better to set and plan strategies that enable the integration of coping strategy care into the current treatment of patients with glaucoma to encourage positive coping strategies instead of maladaptive ones.
Keywords: adult, Ethiopia, Gondar, maladaptive coping strategy
Introduction
The term “coping strategy” refers to cognitive and behavioral attempts to address particular external or internal demands (and conflicts between them) that are regarded as exhausting or surpassing one’s resources.1 From the perspective of a person with a handicap, coping is the way individuals manage their unique constraints.2
Maladaptive coping strategies (MCS) and adaptive coping techniques may generally be distinguished from one another.3,4 An ineffective, harmful manner of trying to cope with stress or anxiety is known as a maladaptive coping strategy.5 It is common among patients with chronic illnesses or chronic stressors, including glaucoma.6,7
The chronic, progressive, and irreversible eye condition known as glaucoma is characterized by optic neuropathy and visual field loss.8 Worldwide, it is among the leading cause of irreversible blindness and significant visual impairment.9 Due to its chronic nature, associated vision loss, and lifelong treatment, which compels the patient to deal with difficulties every day, it has an impact on the quality of life of patients.10,11
Utilizing coping strategies like finding solace in religious activities and beliefs benefits the person. However, using maladaptive coping strategies like using drugs and alcohol may be characterized as unhealthy and lead to poor health outcomes for patients.12
Recently, MCS was adopted by nearly 50% of the study participants among glaucoma patients.13 Venting, self-distraction and denial make up a larger portion of the MCS subscales in glaucoma patients, but eye care professionals frequently overlook them in favor of the patient’s ophthalmic care.5,14,15
According to an Australian study, the prevalence of MCS among glaucoma patients was 63%.15 While the other study in Australia found that the prevalence of MCS was 50%.13
MCS is strongly linked to mental health problems among glaucoma patients and is connected with glaucoma progression, poorer health outcomes, and a lower quality of life.5,8
Some research has been done on risk factors connected to the prevalence of MCS in glaucoma patients. It is asserted that the severity of a person’s visual impairment and female sex are predictors of this.2
Other chronic conditions have seen success with intervention (educational and self-care interventions) that target MCS like denial.16 Similar to this, the study’s findings indicate that glaucoma patients might benefit from positive coping strategy encouragement or discouragement of MCS, which can be given as part of their regular care by adequately qualified counselors or doctors.5,8 As a result, the holistic therapy of glaucoma patients is preferable.2,5
There is little research on the scope and contributing variables of MCS among glaucoma patients despite the higher prevalence of glaucoma and prevalent mental illnesses among glaucoma patients in Ethiopia.17–19 Additionally, studies conducted in Africa and other regions of the world indicate that the magnitude of MCS is substancially high among glaucoma patients, and that there are significant differences between the reported magnitude of MCS among glaucoma patients in Africa and other regions of the world.
In light of the fact that there are currently no studies being done in the subject region, this study intends to evaluate the magnitude of MCS and the associated factors among adult glaucoma patients.
Methods and Materials
Study Design
The institution-based cross-sectional study design was used.
Study Area and Period
From May 15 to June 30, 2022, the study was carried out at the University of Gondar’s Tertiary Eye Care and Training Center (UoGCSH-TECTC). It is situated in the Amhara National Regional state’s Central Gondar administrative zone, which is roughly 750 kilometers northwest of Addis Abeba (the capital city of Ethiopia).
The UoGCSH-TECTC provides various treatments to around 31,200 patients annually in both the outpatient and inpatient departments, as shown by the registration logbook of the facility.20 It offers laser services, surgical procedures, medicinal therapy, and refraction with optical correction.
The center comprises two main configurations, including optometry and ophthalmology, which offer complete eye care services and has been serving as a hub for research and training as a higher education institution. The optometry setup has major units including refraction, outpatient department, dispensing, pediatric, low vision, binocular vision, diagnostic, minor operation, and community eye health, while the ophthalmology clinic includes glaucoma, retina, oculoplasty, pediatric, anterior segment, emergency, and major and minor operation clinics.
For follow-up cases, the eye care center sees glaucoma patients on Monday, Wednesday, and Friday, but five days a week for new cases. The service includes everything, including routine follow-up and early diagnosis.
Source and Study Population
All adult glaucoma patients with glaucoma follow-up who have attended UoGCSH-TECTC for at least the last 3 months and those who avail themselves during the data collection period.
Inclusion and Exclusion Criteria
Inclusion Criteria
All adult glaucoma patients with glaucoma follow-up who have attended UoGCSH-TECTC for at least the last 3 months.
Exclusion Criteria
Participants who were unable to answer included those with speech and hearing impairments, a history of psychosocial issues, or who were now using long-term psychiatric drugs that would impair their capacity to respond.
Sample Size Determination
To calculate the sample size, a single population proportion formula is utilized by considering 50% as the hypothesized proportion of MCS among adult glaucoma patients since previous pieces of evidence on the magnitude of MCS among glaucoma patients in Ethiopia were not found. Because no consistently significant associated factors were discovered, only the objective one’s sample size was determined.

Where:
n –sample size.
Z – Value of z statistic at 95% confidence level = 1.96.
P – 50% (0.50), Then, q=1-P =0.50.
d – Maximum allowable error 5% = 0.05, therefore the sample size is 384.
The ultimate sample size was 423 (384 + 38.4) after adding 10% to account for the non-response rate.
Sampling Technique and Procedures
To choose the study participants, a method of systematic random sampling was adopted. The attending patients are served by the glaucoma clinic on Monday, Wednesday, and Friday. According to the statistics that are currently available, the center typically saw 150 glaucoma follow-up patients per week, or roughly 50 per day, and 900 per month and two weeks. The sampling fraction was 2 which is 900/423 and the first patient was selected using the lottery method from 1–2 and the other participants were selected by adding the sampling fraction from the first selected person. Among these patients, 24 patients were selected per day and 15 patients were selected on the last day of data collection. When there were fewer than 24 patients present at the clinic, all of them were included in the study according to the inclusion criteria.
Variables of the Study
Dependent Variable
Maladaptive coping strategy.
Independent Variables
Socio-demographic factors: Age, sex, level of education, religion, marital status, average monthly family income, and health insurance.
Glaucoma-related factors: Type of glaucoma, stage of glaucoma, laterality of glaucoma, duration of diagnosis, frequency of follow up.
Treatment-related factors: Type of treatment, take medication for other ocular disease, and side effects of drugs.
Systemic chronic comorbidities: Diabetes mellitus, hypertension, tuberculosis.
Visual-related factor: CURRENT visual acuity.
Operational Definition
Maladaptive coping strategy users: Individuals were deemed to have a maladaptive coping strategy if they had a score of the overall mean or higher on the brief Coping Orientation to Problem Experienced (brief COPE) inventory questionnaire.2,21
Adult: A person who is 18 years old or above.22
Psychosocial disorder: Individuals with a mental health condition having difficulty functioning in social situations and may have problems effectively communicating with others, which presents barriers to their equality with others.23
Data Collection Procedures (Tool, Personnel)
An Amharic version of a pretested, structured questionnaire with questions about socio-demographic characteristics, MCS in glaucoma patients, and related factors was used to collect data and the English version of the questionnaire was available as a Supplementary Material. Three trained optometrists conducted face-to-face interviews to gauge MCS and examined patients’ medical records using a checklist to identify clinical variables. The study was overseen by one MSc optometrist and one principal investigator.
One of the most often employed validated coping measures is the Brief COPE inventory instrument which was uploaded as a supplementary material as part of the data collection tool of this study. The Brief COPE inventory instrument was created by Professor Charles Carver at the University of Miami. It is a 28-item questionnaire with 14 different scales for chronic disease stress (2 questions per category). Active coping, planning, positive reframing, acceptance, humor, religion, emotional support, and instrumental assistance are among the eight adaptive coping mechanism subscales. Additionally, it includes six unhealthy coping mechanisms, including self-distraction, denial, venting, substance abuse, behavioral disengagement, and self-blame.24 Due to the fact that this study solely focused on the MCS, it only utilized the tool’s maladaptive component. Each item was measured on a 4-point Likert scale ranging from 1 (I do not do this at all) to 4 (I do this a lot). Higher scores indicated greater usage of that coping strategy, which was determined by adding the results of each sub-scale separately. This scale was validated using a pre-test at Felege Hiwot referral hospital. The items’ reliability was checked by calculating Cronbach’s alpha value (0.78).
Data Quality Control
To ensure consistency, questions were first translated into the regional language Amharic and then back into English version by experts in languages.
A pretest was done on 5% (22) of the sample size at the Felege Hiwot referral hospital. Before doing the actual data collection, the pre-test was completed and the appropriate adjustments were made. Before data collection was started, training was given to the data collectors on how to interview for half a day. There was daily oversight and discussion throughout the data collection process. Prior to analysis, the lead investigator checked 5% of the obtained data for accuracy, completeness, and clarity. He also cleaned up and double-checked the data.
Data Processing and Analysis
The information was entered into Kobo Collect version 2021.2.4, and then it was exported, validated, cleaned, and analyzed using Statistical Package for Social Science (SPSS) version 26. The researcher used the same statistical program to conduct the analysis. Calculated descriptive statistics include proportions, frequencies, ratios, and summary statistics.
To identify factors associated with MCS, binary logistic regression was used. Multivariable logistic regression was used for analysis on all variables having a p-value of less than 0.2. In the multivariable logistic regression analysis, factors with p-values less than 0.05 were deemed statistically significant. The Hosmer and Lemeshow model fitness test was used to determine the model’s fitness, and the result was 0.894. The strength of the association was demonstrated using an adjusted odds ratio (AOR) with a 95% confidence interval (CI).
Ethical Considerations
The University of Gondar’s College of Medicine and Health Sciences’ School of Medicine Ethical Review Committee accepted and granted approval for the study and the verbal informed consent for the study. Each participant in the study verbally consented after being fully informed about the study’s objectives. All study participants were also made fully aware of their unrestricted ability to decline or withdraw from the study at any point during data collection. This investigation was conducted in accordance with the Helsinki Declaration.
Results
Socio-Demographic and Economic Characteristics of Study Participants
A total of 415 participants completed the study with a response rate of 98.1%. The median age of the participants was 56 years with an interquartile range of 18. Of the total participants 305 (73.5%) were females, 313 (75.4%) were married, 120 (28.9%) were unable to read and write, 135 (32.53%) were farmers and 234 (56.4%) were urban residents. The median family monthly income of the respondents was 2000 Ethiopian birr (ETB) with interquartile range of 3000 ETB (Table 1).
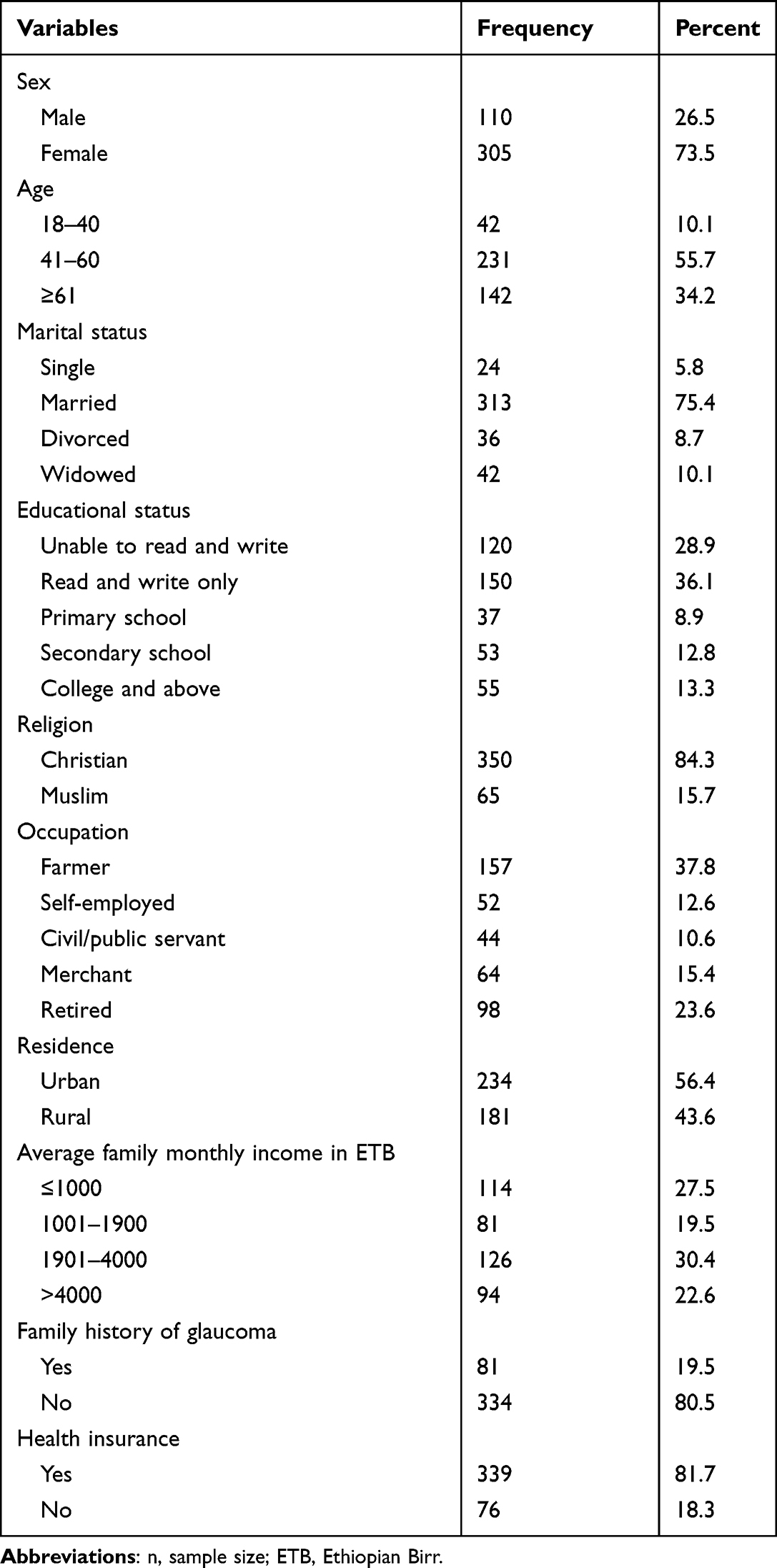 |
Table 1 Socio-Demographic and Economic Characteristics of Adult Glaucoma Patients Attending Tertiary Eye Care Center in Ethiopia (n=415) |
Ocular Clinical Characteristics of Study Participants
Regarding the ocular clinical characteristics, the most prevalent type of glaucoma was primary open-angle glaucoma (236; 56.9%). The majority of participants had moderate glaucoma (173; 41.7%), moderate visual impairment (198; 47.7%), a diagnosis of more than twelve months (290; 69.9%), bilateral glaucoma (316; 76.1%), and 348 (83.9%) were only on drug treatment (Table 2).
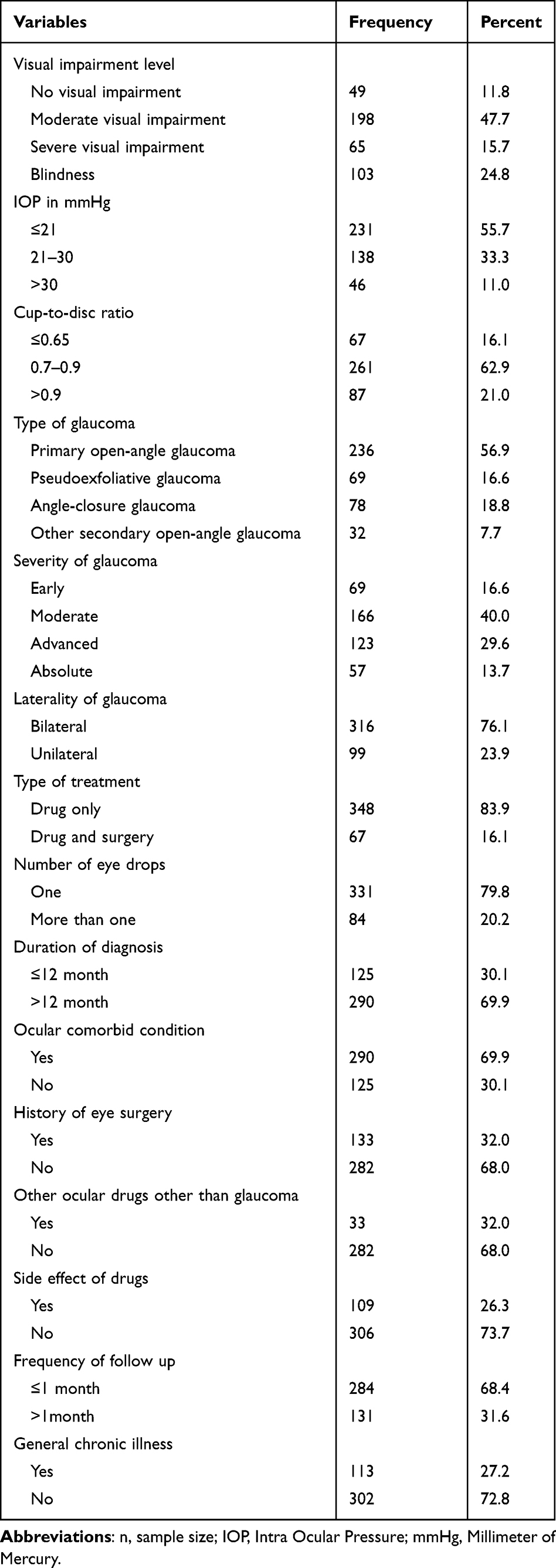 |
Table 2 Clinical Characteristics of Adult Glaucoma Patients Attending Tertiary Eye Care Center in Ethiopia (n=415) |
The Magnitude of Maladaptive Coping Strategy
Two hundred-eight adult glaucoma patients scored ≥24 on brief COPE questions from a total of 48. This makes the prevalence of maladaptive coping strategy among adult glaucoma patients 50.1% (95% CI: 45.1–54.5) (Figure 1).
 |
Figure 1 Magnitude of maladaptive coping strategy among adult glaucoma patients attending tertiary eye care center in Ethiopia. (n=415). |
Subscales Encountered by Study Participants
Among the six maladaptive coping strategy subscales encountered by adult glaucoma patients self-blame (54.0%) was the most common subscale followed by venting (52.3%) and the least common subscale was substance use (19.0%) (Figure 2).
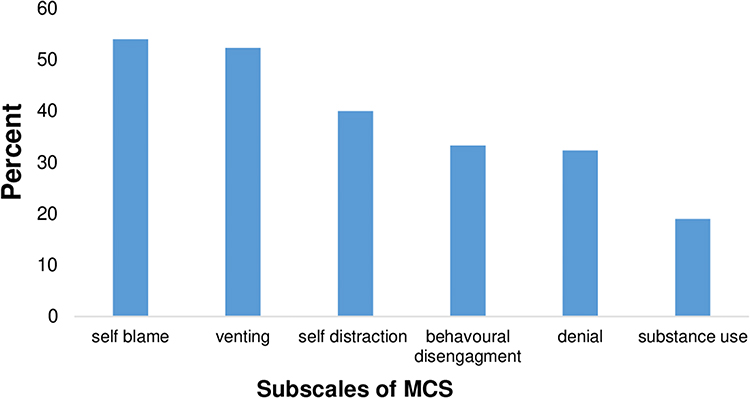 |
Figure 2 Subscales of MCS among adult glaucoma patients attending at tertiary eye care center in Ethiopia. (n=415). |
Factors Associated with a Maladaptive Coping Strategy
All variables were entered into the bivariable logistic regression model separately. Age, educational status, average monthly family income, health insurance, side effects of drugs, and taking other ocular prescriptions had a p-value of greater than 0.2 and were not fitted to multivariable logistic regression. Finally, the association was determined using the enter method in multivariable logistic regression. The level of significance was determined using a p-value of 0.05 at 95% CI, and the following variables were discovered to have a significant association with MCS:
The likelihood of using MCS was about twofold higher among women as compared to men (AOR=1.978, 95% CI: 1.150–3.401). Participants reporting chronic medical illness were nearly two times more likely to use MCS compared with participants without chronic medical illness (AOR=1.713 95% CI:1.007–2.914).
Study participants with a duration of diagnosis greater than twelve months were nearly four times more likely to have MCS compared with participants with a diagnosis duration of less than 12 months (AOR=3.886, 95% CI: 2.295–6.580). Similarly, study participants who were on drug and surgery treatment were two times more likely to use maladaptive coping strategy compared with those participants who were on drug treatment (AOR = 1.895, 95% CI: 1.002–3.585).
This study shows that patients with severe visual impairment were nearly three times more likely to have MCS compared with those who had no visual impairment (AOR= 2.758, 95% CI:1.110–6.852). Similarly, study participants with absolute glaucoma were 2.543 (AOR=2.543, 95% CI: 1.048–6.169) times more likely to use MCS compared with those who had mild glaucoma.
Moreover, the odds of using MCS was 2.3 times higher in bilateral glaucoma patients as compared to patients who had unilateral glaucoma (AOR=2.321, 95% CI: 1.328–4.055) (Table 3).
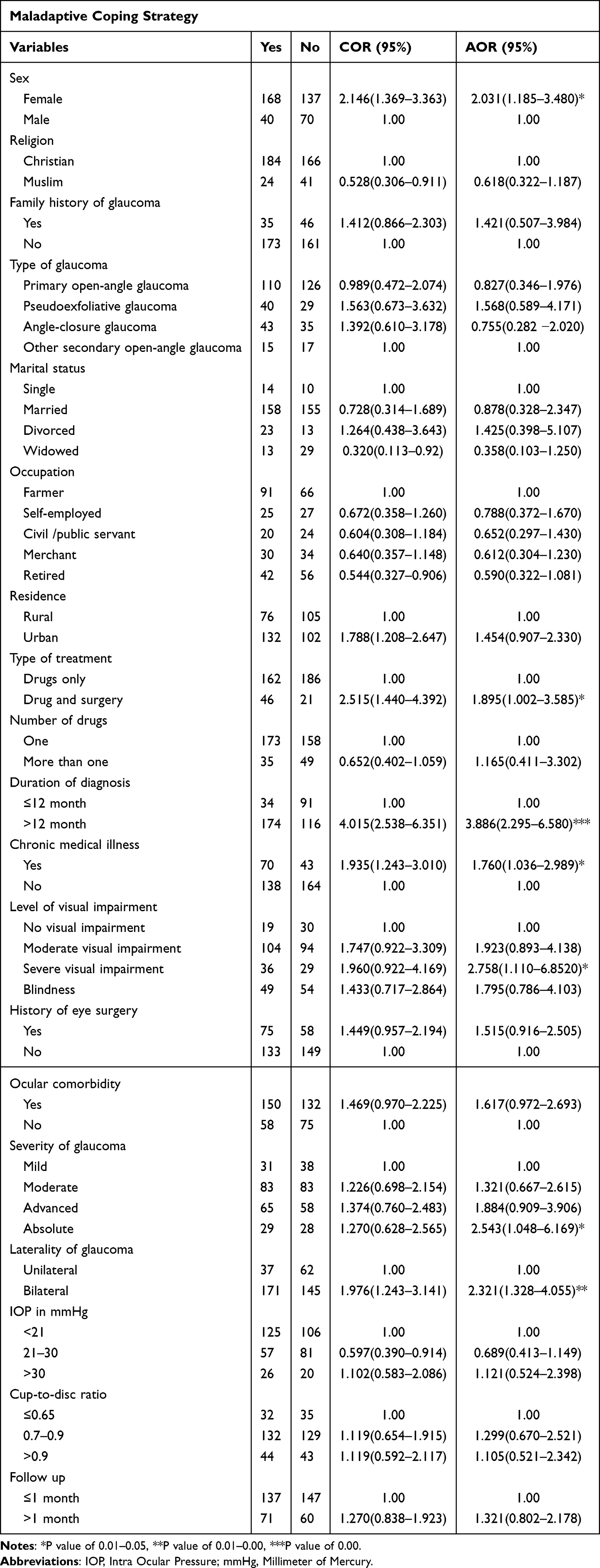 |
Table 3 Factors Associated with Maladaptive Coping Strategy Among Adult Glaucoma Patients Attending at Tertiary Eye Care Center in Ethiopia (n=415) |
Discussion
This study has assessed the magnitude of MCS and its associated factors among adult glaucoma patients attending Tertiary Eye Care Center in Ethiopia.
In this study, the magnitude of the MCS was 50.1% (95% CI: 45.1–54.5). This result was consistent with a study conducted in Australia (50%).13 This might be due to similarities in the ocular clinical characteristics of the study participants. For instance, the majority of patients in both studies had moderate visual impairment, had been diagnosed for more than a year, had bilateral glaucoma, and many of them were on one topical drug treatment.
However, the result of this study was lower than studies conducted in Australia (63%)15 and India (75%).2 This discrepancy might be caused by the difference in sample size, which was larger in the current study. The mentioned studies were qualitative, while the current study is quantitative. There were also population characteristic differences. Additionally, there was a difference in the coping strategy instrument employed; the current study used the brief COPE inventory tool, whereas the Indian study used the Proactive Coping Inventory.
In this study, women were about two times more likely to experience MCS as compared to men. This finding was consistent with studies done in China,25 India,2 USA.26 The reasons might be the impact of family role, social role, sexist stressors, exposure to domestic and social violence, and women’s relative poverty, which are all contributing to the use of MCS.27 On the other hand, this result was not supported by a study done in India.2 The Proactive Coping Inventory was the coping strategy tool used in the Indian study, which may account for the discrepancy, along with the smaller sample size in the current study.
The present study found that participants with chronic medical illnesses were two times more likely to have MCS as compared with participants without chronic medical illness. This may be due to the fact that patients with chronic illnesses may develop thoughts of passing away or becoming permanently disabled, worry about their drugs and potential side effects, experience anxiety about lifestyle interruptions, worry about losing their jobs, and worry about financial difficulty.
This result was supported by studies done in Poland28 and the USA.29 On the other hand, this result was inconsistent with a study done in India.2 A smaller sample size than what was used in the current study may be the cause.
Study participants with a duration of diagnosis greater than twelve months were nearly four times more likely to have MCS compared with those with those with a duration of diagnosis less than or equal to twelve months. This could be as a result of the patients’ decreased likelihood of becoming economically active with extended diagnostic periods.30 The other possible reason might be that with a longer duration, there is disease progression, a higher cost of medication, and more side effects from drugs.
Having both medical and surgical therapy is significantly associated with MCS. This might be contributed by surgical therapy related to outcome expectations and complication-related fear.31
Participants with severe visual impairment were nearly three times more likely to have MCS compared with those participants with no visual impairment. This result agrees with a study done in India.2 This may be because when visual acuity declines, daily tasks may become more difficult, impacting social and economic standing, increasing dependency, raising the risk of falls, and deteriorating emotional health, leading to the employment of MCS.32
Study participants with bilateral glaucoma were more than two times more likely to have MCS compared with those with unilateral glaucoma. This may be because individuals with bilateral glaucoma have a lower quality of life, less mobility, have stopped driving, and have a greater fear of falling than those with unilateral glaucoma.33,34
The likelihood of MCS among subjects with advanced and absolute glaucoma was two- and threefold higher, respectively, as compared to subjects with early glaucoma. This may be because, as glaucoma advances, there will be a lower quality of life brought on by functional loss (visual acuity and visual field), treatment inconveniences, therapeutic side effects, and associated costs, all of which may encourage MCS.35
Limitation of the Study
This study has some limitations. First off all, because the study was cross-sectional, there was no evaluation of MCS over time, and the association between the dependent and independent variables was not shown to be causal. Second, the patient’s response and the potential for recall bias influenced the results. Finally, the questionnaire’s design led to social desirability bias.
Conclusion
Maladaptive coping strategy have been found in half (50.1%) of adult glaucoma patients. Female sex, chronic medical illness, a longer duration of diagnosis, drug and surgery treatment, bilateral glaucoma, advanced and absolute glaucoma stages, and severe visual impairment had a statistically significant association with MCS among adult patients with glaucoma. It is better to set and plan strategies that enable the integration of coping strategy care into the current treatment of patients with glaucoma to encourage positive coping strategies instead of maladaptive ones.
Acknowledgment
All the respected bodies were acknowledged (Gondar University, the department of optometry, all the participants, and Dovepress).
Disclosure
The authors report no conflicts of interest in this work. Before conducting the study, ethical clearance was obtained from University of Gondar, College of Medicine and Health Sciences ethical review committee. Oral consent from each participant was obtained after explaining the purpose of the study and they also have the full right to discontinue or refuse to participate in the study. The research was conducted according to the World Medical Association Declaration of Helsinki.
References
1. Group WB. World Development Report 2016: Digital Dividends. World Bank Publications; 2016.
2. Rai P, Rohatgi J, Dhaliwal U. Coping strategy in persons with low vision or blindness–an exploratory study. Indian J Ophthalmol. 2019;67(5):669. doi:10.4103/ijo.IJO_1655_18
3. Nyman SR, Dibb B, Victor CR, Gosney MA. Emotional well-being and adjustment to vision loss in later life: a meta-synthesis of qualitative studies. Disabil Rehabil. 2012;34(12):971–981. doi:10.3109/09638288.2011.626487
4. Hodge S, Barr W, Bowen L, Leeven M, Knox P. Exploring the role of an emotional support and counselling service for people with visual impairments. Br J Vis Impair. 2013;31(1):5–19. doi:10.1177/0264619612465168
5. Eni EN, Edet BE, Ibanga AA, Duke RE. Cross-sectional study on the coping strategies among glaucoma patients attending a secondary eye clinic in Calabar, Nigeria. Clin Ophthalmol. 2020;14:1307. doi:10.2147/OPTH.S242443
6. Wahl H-W. The psychological challenge of late-life vision impairment: concepts, findings, and practical implications. J Ophthalmol. 2013;2013. doi:10.1155/2013/278135
7. Glen FC, Crabb DP. Living with glaucoma: a qualitative study of functional implications and patients’ coping behaviours. BMC Ophthalmol. 2015;15(1):1–15. doi:10.1186/s12886-015-0119-7
8. Chen J, Lin Z-N, Tao Y-T, et al. Influences of personality characteristics and coping modes on anxiety in primary glaucoma patients. Int J Ophthalmol. 2019;12(7):1163. doi:10.18240/ijo.2019.07.18
9. Hommer A. A review of preserved and preservative-free prostaglandin analogues for the treatment of open-angle glaucoma and ocular hypertension. Drugs Today. 2010;46(6):409–416. doi:10.1358/dot.2010.46.6.1482107
10. Lin S, Mihailovic A, West SK, et al. Predicting visual disability in glaucoma with combinations of vision measures. Transl Vis Sci Technol. 2018;7(2):22. doi:10.1167/tvst.7.2.22
11. Hirneiss C, Vogel M, Kampik A, Neubauer A, Kernt M. Measurement of glaucoma-specific functionality with the GQL-15 and correlation with parameters of visual function. Ophthalmologe. 2011;108(10):939–946.
12. Koenig HG. Religion, spirituality, and health: the research and clinical implications. Int Sch Res Notices. 2012;2012:33.
13. Knight LSWLS, Ridge B, Staffieri SE, Craig JE, Senthil MP, Souzeau E. Quality of life in adults with childhood glaucoma: an interview study. Ophthalmol Glaucoma. 2022;5(3):325–336. doi:10.1016/j.ogla.2021.09.007
14. Freeman EE, Lesk MR, Harasymowycz P, et al. Maladaptive coping strategies and glaucoma progression. Medicine. 2016;95(35):e4761. doi:10.1097/MD.0000000000004761
15. Knight LS, Ridge B, Staffieri SE, Craig JE, Senthil MP, Souzeau E. The caregiver experience in childhood glaucoma: an interview study. Ophthalmol Glaucoma. 2022;531–543. doi:10.1016/j.ogla.2022.02.005
16. Carrico AW, Antoni MH, Durán RE, et al. Reductions in depressed mood and denial coping during cognitive behavioral stress management with HIV-positive gay men treated with HAART. Ann Behav Med. 2006;31(2):155–164. doi:10.1207/s15324796abm3102_7
17. Tilahun MM, Yibekal BT, Kerebih H, Ayele FA, Tesfaye M. Prevalence of common mental disorders and associated factors among adults with glaucoma attending University of Gondar comprehensive specialized hospital tertiary eye care and training center, Northwest, Ethiopia 2020. PLoS One. 2021;16(5):e0252064. doi:10.1371/journal.pone.0252064
18. Yibekal BT, Adimassu NF, Ayele FA. Pseudoexfoliation syndrome and associated factors among adults at Gondar University comprehensive specialized hospital tertiary eye care and training center: a cross-sectional study. Clin Optom. 2021;13:249. doi:10.2147/OPTO.S321716
19. Wubet GM, Assefa AA. Glaucoma and its predictors among adult patients attending ophthalmic outpatient department: a hospital-based study, North West Ethiopia. BMC Ophthalmol. 2021;21(1):1–9. doi:10.1186/s12886-021-02168-y
20. Tegegn MT, Belete GT, Ferede AT, Assaye AK. Proportion and associated factors of low vision among adult patients attending at University of Gondar tertiary eye care and training center, Gondar Town, Ethiopia. J Ophthalmol. 2020;2020:1–7. doi:10.1155/2020/7042905
21. Alosaimi FD, Alawad HS, Alamri AK, et al. Stress and coping among consultant physicians working in Saudi Arabia. Ann Saudi Med. 2018;38(3):214–224. doi:10.5144/0256-4947.2018.214
22. Petry NM. A comparison of young, middle-aged, and older adult treatment-seeking pathological gamblers. Gerontologist. 2002;42(1):92–99. doi:10.1093/geront/42.1.92
23. Craig A, Perry KN. Guide for Health Profes Sionals on the Psychosocial Care of People with a Spinal Cord Injury. New South Wales: State Spinal Cord Injury Service; 2008.
24. Carver C. Brief COPE inventory [Database record]. PsycTESTS. 1997;10:1.
25. Daughtry D, Paulk DL. Gender differences in depression-related coping patterns. Consult Clin Psychol J. 2006;3(2):47–59.
26. Howerton A, Van Gundy K. Sex differences in coping styles and implications for depressed mood. Int J Stress Manag. 2009;16(4):333. doi:10.1037/a0016843
27. Matud MP. Gender differences in stress and coping styles. Pers Individ Dif. 2004;37(7):1401–1415. doi:10.1016/j.paid.2004.01.010
28. Kalka D. Quality of life and proactive coping with stress in a group of middle adulthood women with type 2 diabetes. Pol Psychol Bull. 2016;47(3):327–337. doi:10.1515/ppb-2016-0039
29. Blixen C, Levin JB, Cassidy KA, Perzynski AT, Sajatovic M. Coping strategies used by poorly adherent patients for self-managing bipolar disorder. Patient Prefer Adherence. 2016;10:1327. doi:10.2147/PPA.S110199
30. Rijken M, Spreeuwenberg P, Schippers J, Groenewegen PP. The importance of illness duration, age at diagnosis and the year of diagnosis for labour participation chances of people with chronic illness: results of a nationwide panel-study in the Netherlands. BMC Public Health. 2013;13(1):1–13. doi:10.1186/1471-2458-13-803
31. Nijkamp M, Kenens C, Dijker A, Ruiter R, Hiddema F, Nuijts R. Determinants of surgery related anxiety in cataract patients. Br J Ophthalmol. 2004;88(10):1310–1314. doi:10.1136/bjo.2003.037788
32. Yibekal BT, Alemu DS, Anbesse DH, Alemayehu AM, Alimaw YA. Vision-related quality of life among adult patients with visual impairment at University of Gondar, Northwest Ethiopia. J Ophthalmol. 2020;2020. doi:10.1155/2020/9056097
33. Freeman EE, Muñoz B, West SK, Jampel HD, Friedman DS. Glaucoma and quality of life: the salisbury eye evaluation. Ophthalmology. 2008;115(2):233–238. doi:10.1016/j.ophtha.2007.04.050
34. Chan EW, Chiang PP, Wong TY, et al. Impact of glaucoma severity and laterality on vision-specific functioning: the Singapore Malay eye study. Invest Ophthalmol Vis Sci. 2013;54(2):1169–1175. doi:10.1167/iovs.12-10258
35. Quaranta L, Riva I, Gerardi C, Oddone F, Floriano I, Konstas AG. Quality of life in glaucoma: a review of the literature. Adv Ther. 2016;33(6):959–981. doi:10.1007/s12325-016-0333-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Peripheral Cytopenia and Its Associated Factors in Type 2 Diabetes Mellitus Patients, Northwest Ethiopia
Aynalem M, Getu F, Adane T
Journal of Blood Medicine 2022, 13:373-383
Published Date: 4 July 2022
Determinants of Asthma Attack Among Adult Asthmatic Patients Attending at Public Hospitals of West Shoa Zone, Oromia Regional State, Ethiopia, 2021: Case–Control Study
Megersa S, Chala G, Fikremariam K
Journal of Asthma and Allergy 2022, 15:1143-1154
Published Date: 24 August 2022
Evaluation of Seven Different Brands of Metformin Hydrochloride Tablets Available in the Market in Gondar City, Ethiopia
Flatie Alemu A, Tegegne AA, Getaw NS
Drug, Healthcare and Patient Safety 2024, 16:19-28
Published Date: 1 February 2024