")
Back to Journals » International Journal of Women's Health » Volume 12
Magnitude and Determinants of the Late Request for Safe Abortion Care Among Women Seeking Abortion Care at a Tertiary Referral Hospital in Ethiopia: A Cross-Sectional Study
Authors Kebede K , Gashawbeza B, Gebremedhin S , Tolu LB
Received 5 October 2020
Accepted for publication 8 December 2020
Published 7 January 2021 Volume 2020:12 Pages 1223—1231
DOI https://doi.org/10.2147/IJWH.S285282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Lemi Belay Tolu,1 Kidus Kebede,1 Biruck Gashawbeza,1 Samson Gebremedhin2
1Saint Paul New Millennium Medical College, Addis Ababa, Ethiopia; 2School of Public Health, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Lemi Belay Tolu Email [email protected]
Background: Second-trimester abortions disproportionately contribute to the increased medical cost, maternal morbidity, and mortality compared to the first trimester. Therefore, the aim of the current study was to determine the magnitude and determinants of late presentation for safe abortion care at a tertiary hospital in Ethiopia.
Methods: We conducted a cross-sectional study among pregnant women who requested safe abortion care from January 2019 to April 2020. Participants were selected using systematic sampling and data were collected using the interviewer-administered questionnaire. P-value adjusted odds ratios (AOR) with their 95% confidence interval (CI) were used to determine the association between variables.
Results: The prevalence of second-trimester abortion was 53.4%. Young age, ≤ 19 years (AOR= 6.37, 95% CI=1.84– 22.06), decision ambivalence (AOR=5.64, 95% CI=1.71– 18.61), delay to suspect pregnancy (AOR= 8.56, 95% CI=2.11– 34.57), delay to diagnose pregnancy (AOR=3.83, 95% CI=1.51– 9.75), lack of awareness on pregnancy signs and symptoms (AOR=4.22, 95% CI=1.59– 11.23), delay to get the service (AOR =4.43, 95% CI=1.43– 13.67), and lack of information where to get the abortion service (AOR=3.90, 95% CI=1.53– 9.96) were significantly associated with presentation in second trimester.
Conclusion: More than half of women who request safe abortion at Saint Paul’s Hospital Millennium Medical College do so in the second trimester. Young age, delay in diagnosis of pregnancy, delayed decision, and lack of information where to get service were contributing factors. Therefore, comprehensive adolescent sexuality education, increasing access to contraception, and safe abortion service including self-care interventions are very imperative to avert late gestation abortion and its consequences.
Keywords: late gestation abortion, safe abortion, Saint Paul Millennium Medical College
Introduction
An estimated 56 million induced abortions occur each year globally, and 22,800 women die from complications of unsafe abortion contributing to 8% of maternal deaths worldwide.1,2 The medical cost, morbidity, and mortality and, for some women, social or emotional challenges are higher in second-trimester abortion than in the first.3–5 In Ethiopia, an estimated 620,300 induced abortions were performed per year making the annual abortion rate 28 per 1000 women aged 15–49.6 Unsafe abortion accounts for 8.6% of maternal death in Ethiopia and many more suffer from injuries or illness related to unsafe procedures.2,7,8
Worldwide, 10 to 15% of the abortions performed annually are second-trimester abortion.9 The prevalence of induced second-trimester abortion according to an institution-based cross-sectional study in the Amhara region of Ethiopia was 19%.10 The frequently mentioned reasons for the delayed request are irregular menstrual cycle, late recognition of pregnancy, difficulty locating a provider, relying on financial assistance to pay for the procedure, a previous failed attempt to terminate the pregnancy, and emotional factors such as exclusion from abortion-related decisions, discouragement from family and fear of abortion.10–19
In Ethiopia, the liberalization of the abortion law in 2005 and the establishment of technical guidelines have served as essential step in determining the practice of safe abortion services.7,20 However, eradication of morbidity from unsafe abortion has not yet been achieved.8 Access to second-trimester abortions is severely limited and only 9–10% of all facilities have a provider who can perform this service.7 Saint Paul Hospital Millennium Medical College (SPHMMC) is one of the tertiary hospitals in Ethiopia which provide abortion service, and request for late abortion is frequently encountered at Michu clinic of SPHMMC. However, the evidence on the contributing factors and reasons why women delay seeking an abortion and their relative magnitude are limited. Understanding the complex factors and reasons why women delay seeking an abortion until the late second trimester, help to reduce the prevalence of second-trimester abortion and the associated mortality and morbidity. Therefore, the current study aims to determine the magnitude and factors associated with the late request for safe abortion care among women seeking abortion care at the SPHMMC. The late request means in the current study second-trimester abortion which is defined as abortion at or after the gestational age of 13 completed weeks up to 28 weeks of gestation. The evidence generated can help to frame policy guidelines and contextual interventions. Furthermore, this study will serve as a baseline to conduct a national survey on the related research areas.
Methods
Study Design, Area, and Period
We conducted a prospective hospital-based cross-sectional study at Michu clinic, SPHMMC in Addis Ababa, the capital city of Ethiopia. SPHMMC is one of the teaching and tertiary referral hospitals directly under the federal ministry of health. According to the statistics office report, the hospital gives service to 200,000 people annually. It gives service under different clinical disciplines which include Obstetrics and Gynecology. Michu clinic is under the Department of Obstetrics and Gynecology department which provides abortion and family planning-related services. Around 1500 women receive abortion care in the hospital annually.
The data were collected from January 2019 to April 2020. The study population were all pregnant women requesting a safe abortion service during the study period at Michu Clinic. We included all pregnant women who requested a safe abortion service and gave written informed consent. We excluded those women who seek abortion service for indications of fetal demise, fetal anomaly, and life-threatening maternal medical disorders. Besides, those who presented after the gestational age of viability (≥28 weeks) and those who are seriously ill and unable to communicate during the data collection period were excluded.
Sample Size and Sampling Procedure
The sample size was calculated using the single population proportion formula taking a P value of 0.192 from the study done in the Amhara region which shows the prevalence of second-trimester abortion as 19.2%.10 Using the power of 80%, adding a marginal error of 5%, and a contingency rate, the estimated sample size was 246. We used systematic sampling to recruit eligible study participants. Considering 420 data collection days in the study period to recruit 246 participants we recruited every 2nd client prospectively. In cases when the 2nd patient is not eligible the patient immediately before or after the patient will be enrolled.
Data Collection Procedures
The data were collected at the time of client presentation to Michu clinic by interviewer-administered structured questionnaires. The questionnaire was prepared in English, translated to Amharic which is a local language, and then translated back to English to check for consistency. Pretesting of the questionnaire was conducted on ten women and appropriate modification was applied. Data collectors were trained at Michu Clinic for 02 consecutive days by the principal investigator in pre-tested checklists. The operational manual for the study was prepared to assure a uniform standard for carrying out the study with good quality control. All data were collected and stored anonymously. All filled questionnaires were checked daily for completeness, accuracy, and consistency by the principal investigator. Supervision was carried out by the principal investigator throughout the data collection.
Timing for seeking abortion care was the dependent variable and categorized as second trimester (≥13 weeks of gestation and < 28 weeks) and early (< 13 weeks of gestation). The independent variables were socio-demographic characteristics (age, marital status, educational status, place of residency, monthly income, religion), reproductive characteristics (gravidity, parity, abortion history, menstrual nature, gestational age, whether the pregnancy was a result of sexual assault or not), logistic factors (financial, transportation and information problems, service availability around vicinity), interpersonal and intrapersonal factors (partner or family conflict, social or religious stigma, decision ambivalence), level of awareness on reproductive health (pregnancy window period, pregnancy signs and symptoms, contraception use, alternative options for unplanned and unwanted pregnancies, abortion care centers, early and safe pregnancy duration for induced abortion, abortion complications)
Data Management and Analysis
After data were collected, each questionnaire was given code and checked visually for completeness. The data were entered Epi-info version 3.5.1 and transported to SPSS version 20 software packages for analysis. Further, data cleaning was performed to check for outliers, missed values, and any inconsistencies before the data analysis. For any missed values and inconsistency, the principal investigator cross-checked the patient medical record using the codes and made necessary corrections. Data were analyzed using SPSS 20.0 version. Socio-demographic and reproductive characteristics of the participants and their level of awareness on reproductive health were described using descriptive statistics. Bivariable and Multivariable logistic regression was used to identify independent factors associated with the late request for safe abortion. Bivariate analysis was carried out first to observe the crude association between independent and outcome variables. The variables with P value < 0.2 in bivariate analysis, were considered as candidate variables for the multivariable model. Finally, statistically significant variables that fit the final regression model were identified using the odds ratio with a 95% confidence interval and P value < 0.05.
Ethical Consideration
The current study was conducted following the Declaration of Helsinki. Ethical clearance was obtained from the Institutional Review Board (IRB) of SPHMMC including informed written consent for participants under the age of 18 years. Permission to conduct the study was taken from the hospital administration. Informed consent was obtained from each study participants after the objectives of the study were explained. To ensure the confidentiality of participants, we did not collect or store any identifying information about participants. All the datasets used and/or analyzed during the current study are included in the manuscript.
Results
Out of 246 women who were enrolled in the study population 238 women completed the interview administered questionnaire. Eight patients declined to complete the whole interview, hence excluded from analysis. Therefore, data analysis was made based on 238 cases that had completed the interview. The response rate was 96.7%.
Socio-Demographic Characteristics
One hundred three (43.3%) of participants were in the age range of 20–24 years and the mean age was 23.5 ± 4.9. Two-third of the respondents 175 (73.5%) were single, 161 (67.6%) lived in Addis Ababa, and 162 (68.1%) were Orthodox Christian in religion. Private employment including housemaid account for fifty percent of the participant’s occupation, and 96 (40.3%) are having a monthly income of <26.3 dollars. Only 37 (15%) of the respondents have attended college and two-third have the educational level of primary and secondary school, respectively (Table 1).
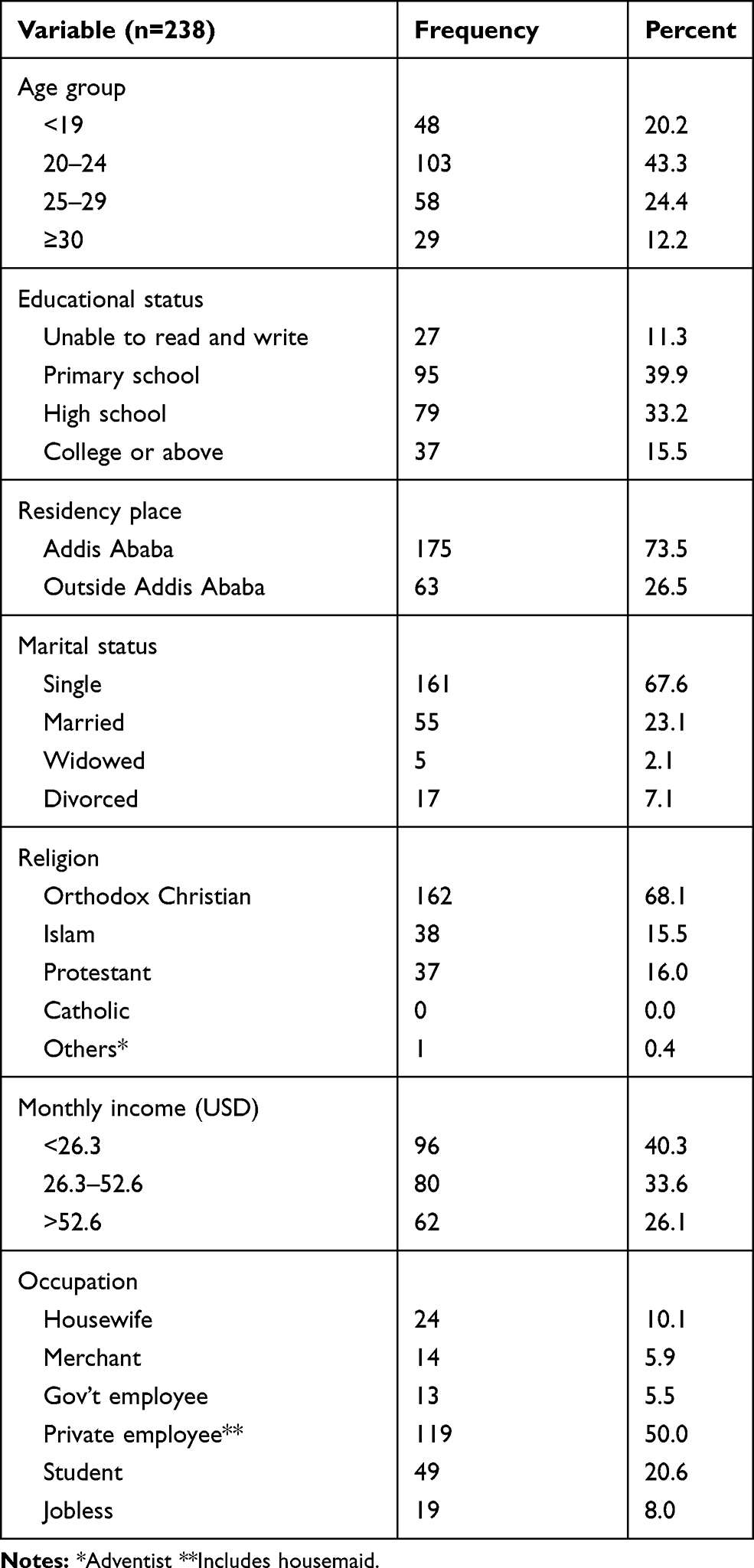 |
Table 1 Socio-Demographic Characteristics of Women |
Reproductive Characteristics and Prevalence of Induced Second-Trimester Abortion
Seventy-four (31.1%) of the respondents had an irregular menstrual cycle before their current pregnancy. One hundred forty-eight (62.2%) of the participants were pregnant for the first time, while thirty (12.6%) of the clients had a history of prior induced abortion. During the study period, a total of 238 women requested abortion service from which 127 (53.4%) of the respondents presented in the second trimester. From those second-trimester clients, 91 (38.2%) of them presented in the late second trimester between 21 and 28 weeks of gestational age (Table 2).
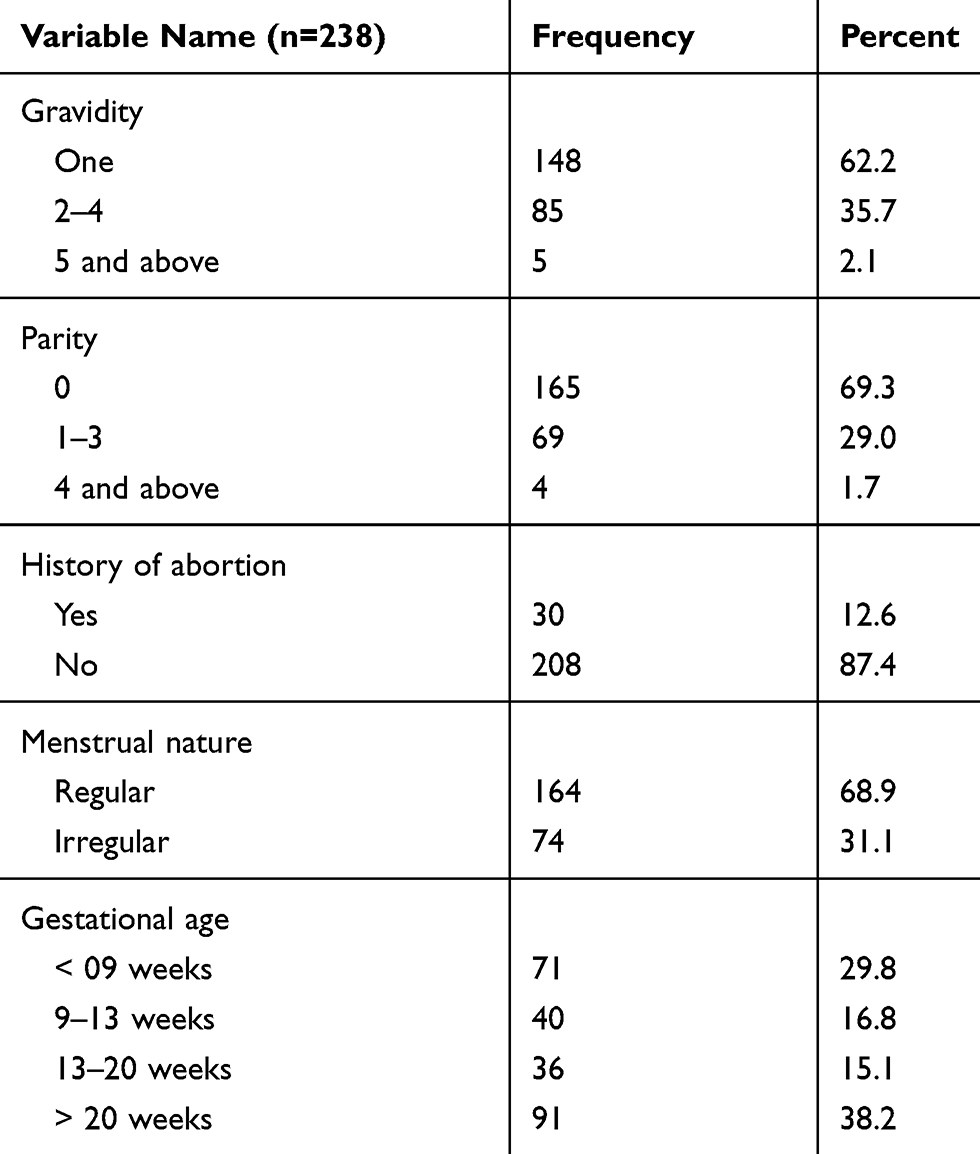 |
Table 2 Reproductive Characteristics of Women Seeking Abortion Service at Michu Clinic |
Level of Awareness on Some Reproductive Health Factors
Eight three (34.9%) of the participants know two and above pregnancy signs and symptoms, while 37 (15.5%) of the participants did not mention even one contraception method they know. Near to half, 124 (52.1%) of the respondents mentioned two or more health institutions that provide abortion service. Only 24 (10%) of the participants know the pregnancy window period in the menstrual cycle, and 124 (52.1%) of them know the safest time for induced abortion (Table 3).
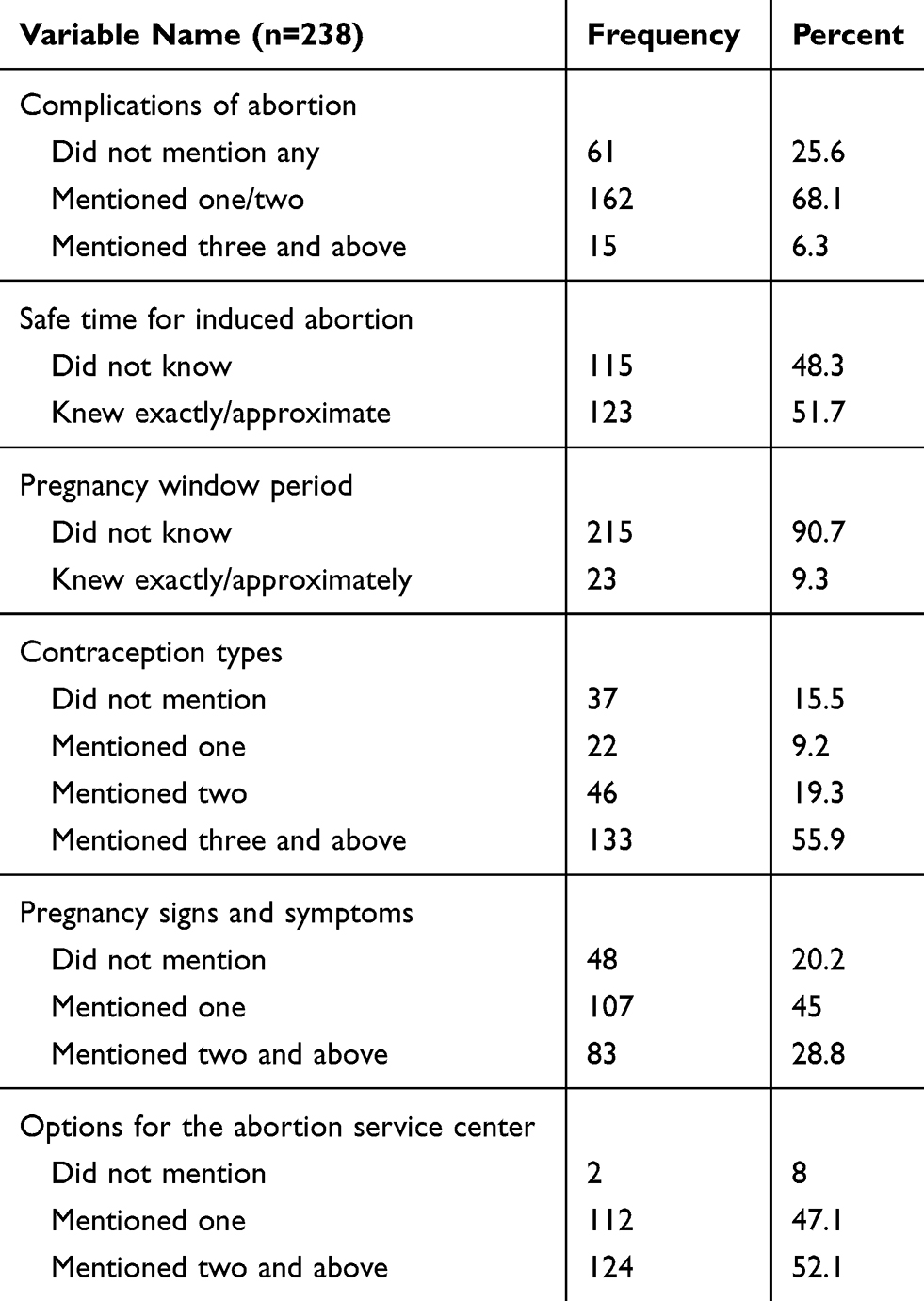 |
Table 3 Level of Awareness on Some Reproductive Health Factors |
Associated Factors of Induced Second-Trimester Abortion
Age, educational status, place of residency, knowledge on pregnancy signs and symptoms, awareness on pregnancy window period, delay after the decision for abortion made, religious stigma, social stigma, decision ambivalence, sexual assault, financial problem, transportation problem, lack of information where to get the service, delay to suspect pregnancy, delay to diagnose pregnancy, and family conflict were found to be associated with second-trimester abortion in the bivariable analysis. Those variables were entered once into a stepwise multivariable logistic regression model to control confounders. Finally, the model retains only those factors with significant associations with P-value < 0.05 level. Age younger than 20 (AOR= 6.37, CI 1.84–22.06), decision ambivalence (AOR=5.64, CI 1.71 −18.61), greater than one month delay from last menstrual period (LNMP) to suspect pregnancy (AOR= 8.56, CI 2.12–34.58), greater than one month delay to diagnose pregnancy (AOR= 3.84, CI 1.51 −9.76), limited knowledge on pregnancy signs and symptoms (AOR= 4.22, CI 1.59 −11.23), more than 1-month delay to get the abortion service (AOR =4.43, CI 1.43 −13.67), and lack of information were to get the service (AOR =3.907, CI 1.532–9.965) were variables associated with a presentation in second-trimester for termination of pregnancy (Table 4).
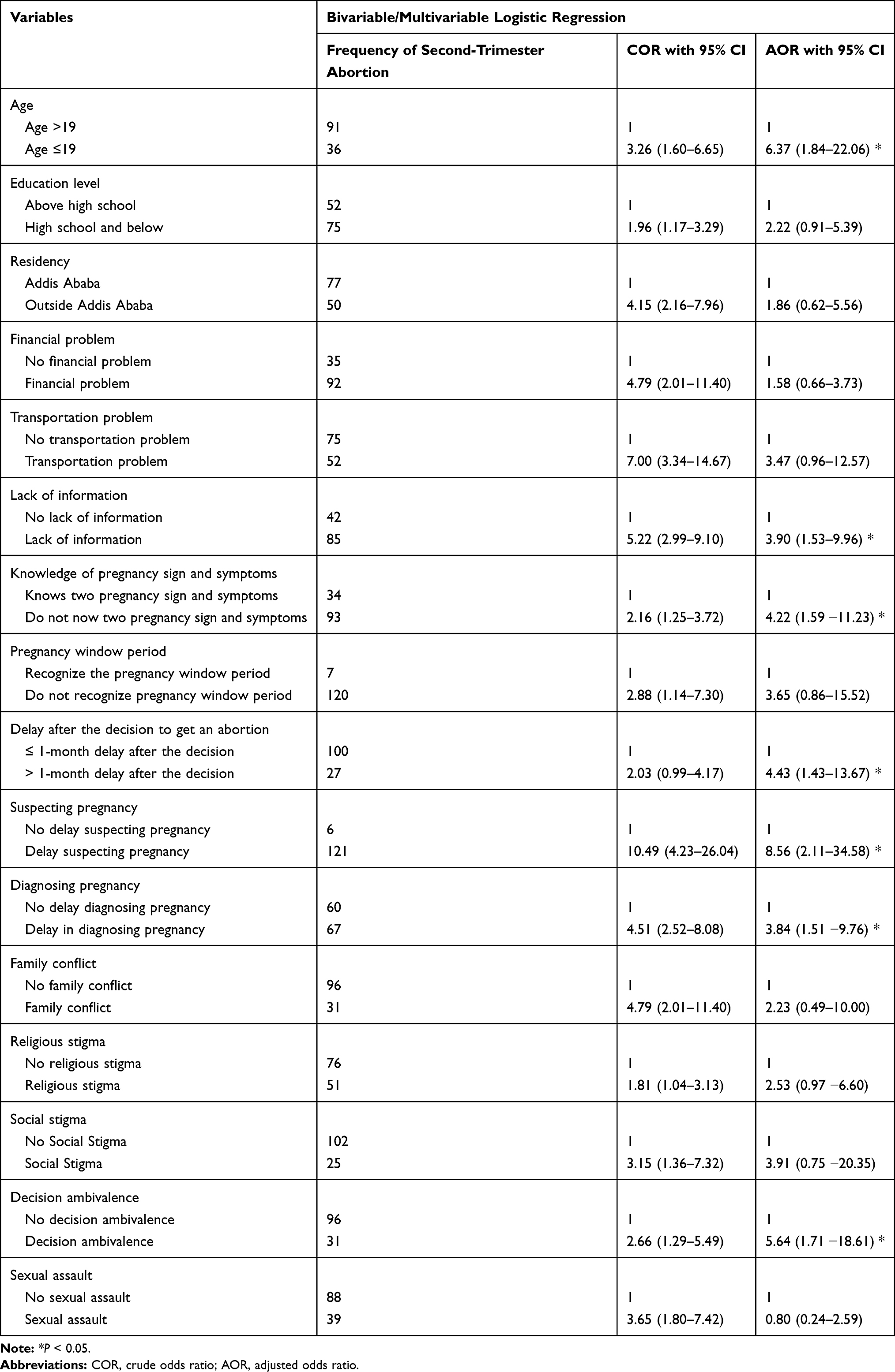 |
Table 4 The Bivariable and Multivariable Logistic Regression Results on Factors Associated with Induced Second-Trimester Abortion |
Discussion
The current study is undertaken at SPHMMC to determine the demand for second-trimester abortion and explore the reasons why women delay seeking an abortion. The prevalence of induced second-trimester abortion in our study is found to be 53.4%. This finding is greater than the 10–15% of the globally reported prevalence and studies done in Mexico and Maharashtra (Aurangabad and Jalna districts) which reported prevalence of the second-trimester abortion as 8.10%, and 23% respectively.1,17,19 It is also not in line with the study done in the Amhara region and Jimma town, Ethiopia that reported the prevalence of 19.2% and 12% respectively.10,11 Both first and second-trimester abortion is provided for free in government hospitals in Ethiopia. The possible explanation for this significant proportion of second-trimester abortion in the current study might be the limited access to second-trimester abortion services forcing many women to visit referral hospitals. Moreover, SPHMMC is one of the biggest tertiary hospitals in Ethiopia and patients get referred from every corner of the country. Michu clinic of SPHMMC is also the most well-organized family planning and abortion clinic in the country where service is provided by resident physicians and expert subspecialists. Most private institutions, health centers, and non-governmental organizations are not providing abortion care beyond 12 weeks of gestation except on rare occasions like private hospitals staffed by specialists (obstetrician/gynecologist).
Across countries with different cultures and development, factors related to presenting late at or after 13 weeks gestation appear similar and disproportionately affect the poor, uneducated, and underserved women. For example, in Cambodia, Ethiopia, and Kenya 17%, 38%, and 41% of all women needing post-abortion care present at or after 13 weeks of gestation respectively.21–23 A cross-sectional study conducted in Jimma town of Ethiopia reported that age 19 years or younger, having education of primary school level or below, residence outside Jimma zone, and nulliparity were associated uneducated with presenting for second-trimester abortion.11 The current study also showed that young is associated with late presentation for abortion service. The current study also showed that more than one-month delay getting the service after the decision to have an abortion was significantly associated with late presentation. This might be happening because of a lack of information where to get service, lack of easy access or absence of youth-friendly health service, and lack of economic freedom of young girls and women facing the transportation and other logistic problems.
Although there is substantial progress on the proportion of abortion care provided in the public sector in Ethiopia, access-related problems still are among factors contributing to delayed presentation for abortion. A study done in the Amhara region of Ethiopia showed that access-related problems contribute significantly to late presentation for safe abortion.10
Delays in suspecting and testing for pregnancy cumulatively caused 58% of second-trimester patients to miss the opportunity to have a first-trimester abortion in a case-control study in the US.13 Our study also highlighted those women who did not know the signs and symptoms of pregnancy were almost four times more likely to miss the opportunity to have an abortion in the first trimester than their counterparts. Lack of information, delays in suspecting, and testing for pregnancy were also associated with the second-trimester presentation for termination of pregnancy. Spending much time collecting money and lack of information in locating service for pregnancy tests might explain the delay to diagnose pregnancy early.
In current study, a large proportion of the respondents had limited awareness of the pregnancy window period of the menstrual cycle, contraceptive options, pregnancy signs and symptoms, and the safe time of pregnancy for induced abortion. Similarly, in a cross-sectional study conducted among female students in secondary schools in Mekelle town, Ethiopia, 12% of the students were not aware of any methods of contraception and 15% of the sexually active students had never used contraception.24 This may be due to a lack of information and poor utilization of sexual and reproductive health services. Another cross-sectional study done in Southwest Oromia, Ethiopia, reported that lack of information and poor perceptions about sexual and reproductive health, feeling of shame, fear of being seen by others, restrictive cultural norms, lack of privacy, confidentiality, and unavailability of services were deterring the use of sexual and reproductive health services.25 Thus, improving open parent-child communication and appropriate peer-to-peer communication in schools on sexual and reproductive health, school-based service delivery, youth centers, and outreach/community volunteers’ approach may help to create awareness on reproductive health issues.
The strengths of the study include the prospective primary data collection at a single contact per patient with less participant’s loss from the study. Besides, the relatively long duration of data collection over one year and four months could help capture variability over time and increase the representativeness of samples that possibly predict the outcome variable. The study also has its limitations. The sample size calculation did not consider the number of variables included and might not be adequate. As any cross-sectional study, it could not explain the cause and effect relationship. Besides, being a single and tertiary referral hospital-based study; the current study might have suffered from the possibility of selection bias and overestimation of late abortion care requests. Furthermore, the profile of those patients may be different from patients in other hospitals. These factors limit the generalizability of current findings especially regarding the magnitude of second-trimester abortion. However, the current study explored and provided good input for a further multidimensional and multicenter study on magnitude and determinants of late request for an abortion.
Conclusions and Recommendations
The current study revealed a high prevalence of second-trimester abortion at SPHMMC compared to previous studies conducted both locally and globally. This finding indicates the necessity of expanding second-trimester abortion service into primary health care units by task sharing and shifting mechanisms. Young age, lack of knowledge of sign and symptoms of pregnancy, failure to suspect and delay in diagnosis of pregnancy, decision ambivalence, and delay in decision making, lack of information where to get service, and delay in getting service after decision were factors significantly associated with induced abortion in the second trimester. Consequently, we recommend public health interventions such as comprehensive adolescent sexuality education to improve adolescent girl’s and women’s knowledge about pregnancy and earlier recognition of pregnancy, reproductive physiology, and reproductive health. Moreover, it is very imperative to increase access to adolescent and women-friendly contraceptive counseling and first-trimester abortion service. The WHO recommends that individuals can self-manage their abortions in early pregnancy until 12 weeks. This is very important to prevent facility visits, increase client privacy and autonomy resulting in increased access to early abortion and reduction of second-trimester abortion. Because of the sensitive nature of abortion, a qualitative study may be needed to further dig out the underlying reasons why women make late decisions to terminate their pregnancy in the second-trimester period. Furthermore, the national and regional survey needs to be conducted to determine the prevalence of second-trimester abortion and contributing factors at the country and continent level for setting contextual policy directions and framing evidence-based interventions.
Abbreviations
AOR, Adjusted Odd Ratio; CI, Confidence Interval; IRB, Institutional Review Board; LNMP, Last Normal Menstrual Period; OR, Odds Ratio; OBGYN, Obstetrics, and Gynecology; SPHMMC, Saint Paul’s Hospital Millennium Medical College; SPSS, Statistical Package for Social Science; US, United States; WHO, World Health Organization.
Acknowledgments
We would like to thank the institutional review board of SPHMMC for the ethical clearance and the hospital administration for permission to conduct the study. Furthermore, we would like to thank all study participants and data collectors for their contribution to the success of this work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Sedgh G, Bearak J, Singh S. Abortion incidence between 1990 and 2014: global, regional, and sub regional levels and trends. Lancet. 2016;388(10041):258–267. doi:10.1016/S0140-6736(16)30380-4
2. Unsafe abortion: global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008 [Internet]. Avenue Appia; 2011 [cited January 18, 2019]. Available from: http://who.int/reproductivehealth/publications/unsafe_abortion/978924150118/en/.
3. Andersson IM, Gemzeil-Danielsson K. Experiences, feelings and thoughts of women undergoing second trimester medical termination of pregnancy. PLoS One. 2014;9(12):e115957. doi:10.1371/journal.pone.0115957
4. Bartlett LA, Zane SB, Berg CJ. Risk factors for legal induced abortion-related mortality in the United States. Obstet Gynecol. 2004;104(3):635. doi:10.1097/01.AOG.0000137733.29798.4e
5. Lince-Deroche N, Sinanovic E, Devjee J, Blanchard K. The costs and cost-effectiveness of providing second-trimester medical and surgical safe abortion services in Western Cape Province, South Africa. PLoS One. 2018;13(6):e0197485. doi:10.1371/journal.pone.0197485
6. Moor AM, Fetters T, DibabaWado Y, et al. The estimated incidence of induced abortion in Ethiopia, 2014: changes in the provision of services since 2008. Int Perspect Sex Reprod Health. 2016;42(3):111–120. doi:10.1363/42e1816
7. Facts on Unintended Pregnancy and Abortion in Ethiopia, 2010 [Internet]. Guttmacher Institute; 2010 [cited February 17. 2019]. Available from: [email protected].
8. Yirgu Gebrehiwot TF, Gebreselassie H, Moore A, et al. Changes in morbidity and abortion care in Ethiopia after legal reform: national results from 2008 and 2014. Int Perspect Sex Reprod Health. 2016;42(3):121–130. doi:10.1363/42e1916
9. Facts on Induced Abortion Worldwide [Internet]. World Health Organization; 2012 [cited January 16, 2019]. Available from: [email protected].
10. Mulat A, Bayu H, Mellie H, Alemu A. Induced second trimester abortion and associated factors in Amhara Region Referral Hospitals. Biomed Res Int. 2015;2015(256534):6. doi:10.1155/2015/256534
11. Bonnen K, Tuijje DN, Rasch V. Determinants of first and second trimester induced abortion: results from a cross-sectional study taken place 7 years after abortion law revisions in Ethiopia. BMC Pregnancy Childbirth. 2014;14:416. doi:10.1186/s12884-014-0416-9
12. Foster G, Jackson RAJ, Cosbya K, Weitza TA, Darney PD, Drey EA. Predictors of delay in each step leading to an abortion Contraception. 2008;77:289–293. doi:10.1016/j.contraception.2007.10.010
13. Drey EA, Foster DG, Jackson RA, Lee SJ, Cardenas LH, Darney,PD. Factors in abortion delay into the 2nd trimester. Obstet Gynecol. 2006;107:128–135. doi:10.1097/01.AOG.0000189095.32382.d0
14. Jones RK, Jerman J. Characteristics and circumstances of US women, who obtain very early and second-trimester abortions. PLoS One. 2017;12(1):e0169969. doi:10.1371/journal.pone.0169969
15. Kiley JW, Yee LM, Niemi CM, Feinglass JM, Simon,MA. delays in a request for pregnancy termination: comparison of patients in the first and second trimesters. Contraception. 2010;81:446–451. doi:10.1016/j.contraception.2009.12.021
16. Mentula MJ, Niinimäki M, Suhonen S, Hemminki E, Gissler M, Heikinheimo O. Young age and termination of pregnancy during the second trimester are risk factors for repeat second-trimester abortion. Am J Obstet Gynecol. 2010;203(107):1–7. doi:10.1016/j.ajog.2010.03.004
17. Saavedra-Avendano B, Schiavon R, Sanhueza P, Rios-Polanco R, Garcia-Martinez L. Who presents past the gestational age limit for first-trimester abortion in the public sector in Mexico City? PLoS One. 2018;13(2):e0192547. doi:10.1371/journal.pone.0192547
18. Waddington A, Reid R. Determinants of late presentation for induced abortion care. J Obstet Gynecol. 2015;37(1):40–45.
19. Zavier AJ, Jejeebhoy S, Kalyanwala S. Factors associated with second trimester abortion in rural Maharashtra and Rajasthan, India. Glob Public Health. 2012;8:897–908. doi:10.1080/17441692.2011.651734
20. Bridgman‐Packer D, Kidanemariam S. The implementation of safe abortion services in Ethiopia. Int J Gynecol Obstet. 2018;143(Suppl. 4):19–24. doi:10.1002/ijgo.12673
21. Fetters T, Vonthanak S, Picardo T, Rathavy T. Abortion-related complications in Cambodia. BJOG. 2008;115(8):957–968. doi:10.1111/j.1471-0528.2008.01765.x
22. Gebreselassie H, Fetters T, Singh S, et al. Caring for women with abortion complications in Ethiopia: national estimates and future implications. Int Perspect Sex Reprod Health. 2010;36(1):6–15. doi:10.1363/3600610
23. Incidence and complications of unsafe abortion in Kenya: key findings of a national study [Internet]. Ministry of Health Kenya, Ipas Kenya, & Guttmacher Institute; 2013 [cited January 16, 2019]. Available from: http://guttmacher.org/sites/default/files/reports_pdf/abortion-in-kenya.pdf. Accessed:January 5, 2019.
24. Adama Melaku YB, Kinsman J, Redal HL. Sexual and reproductive health communication and awareness of contraceptive methods among secondary school female students, northern Ethiopia: a cross-sectional study. BMC Public Health 2014;14:252. doi:10.1186/1471-2458-14-252
25. Zewdie Birhanu KT, Jebel MG. Sexual and reproductive health services use, perceptions, and barriers among young people in Southwest Oromia, Ethiopia. Ethiop J Health Sci. 2017;28(1):37. doi:10.4314/ejhs.v28i1.6
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.