")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Magnitude and Determinants of Syphilis and HIV Co-Infection Among Female Sex Workers in Ethiopia: Evidence from Respondent Driven Samples, 2019–2020
Authors Barba A , Bati F , Tura JB, Addis B , Abrahim S
Received 29 July 2022
Accepted for publication 8 October 2022
Published 31 October 2022 Volume 2022:14 Pages 473—485
DOI https://doi.org/10.2147/HIV.S384213
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Ammar Barba,1 Fayiso Bati,2 Jaleta Bulti Tura,2 Beza Addis,1 Saro Abrahim2
1Director General Office, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 2Tuberculosis and HIV/AIDS Research Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia
Correspondence: Ammar Barba, Director General Office, Ethiopian Public Health Institute, Addis Ababa, Ethiopia, Tel +251 925 229 205, Email [email protected]
Background: Female sex workers (FSWs) play an important role in transmitting Human Immunodeficiency Virus (HIV) and syphilis from high-risk groups to the general population. Syphilis and HIV infections are generally more prevalent among FSWs. However, in Ethiopia, up-to-date evidence about Syphilis–HIV co-infections among FSWs was lacking.
Objective: To determine the magnitude and determinants of Syphilis–HIV co-infection among FSWs in Ethiopia, 2019– 2020.
Methods: A cross-sectional HIV and other sexually transmitted infections Bio-Behavioral Survey (HSBS) was conducted using respondent-driven sampling (RDS) among 6,085 FSWs in Ethiopia from August 2019 to January 2020. Data was collected, merged with laboratory data, and analyzed in R software using the RDS package. The odds ratio was calculated at 95% CI to measure associations between the dependent and independent variables. Variables that yield p< 0.25 in univariate analysis were included in multivariate analysis. In multivariate analysis, variables with p< 0.05 were declared as statistically significant. Results were presented in frequency tables and charts.
Results: The prevalence of Syphilis–HIV co-infection among FSWs was 2.9% [95% CI=2.6– 3.2]. Age of the FSWs (15– 19 years old (AOR=0.03; 95% CI=0.01– 0.12)), non-formal educational level (AOR=3.18; 95% CI=1.78– 5.68), monthly income < 2,500 ETB (AOR=3.05; 95% CI=1.45– 6.42), major depression (AOR=1.85; 95% CI=1.18– 2.89), forced first sex experience (AOR=1.71; 95% CI=1.2– 2.44), condom breakage (AOR=1.62; 95% CI=1.14– 2.30), Hepatitis B seropositivity (AOR=2.32; 95% CI=1.10– 4.90), and Hepatitis C seropositivity (AOR=5.37; 95% CI=1.70– 16.93) were strongly associated with Syphilis–HIV co-infection among FSWs in Ethiopia.
Conclusion: The prevalence of Syphilis–HIV co-infection among FSWs in Ethiopia was high. To ward off Syphilis–HIV co-infection among FSWs, a special FSWs-targeted HIV and Syphilis/STIs prevention program and treatment approach needs to be devised. An outreach approach to address the sexual and reproductive health needs of FSWs has to be part of the strategy.
Keywords: female sex workers, syphilis–HIV co-infection, Ethiopia
Introduction
Human Immunodeficiency Virus (HIV) and syphilis are sexually transmitted infections (STIs) and share modes of transmission. Syphilis is a systemic disease caused by a bacterium called T. pallidum.1 Syphilis infection has been associated with a several-fold increased risk of acquiring and transmitting HIV in key populations.2 Syphilis–HIV co-infection was associated with higher virologic failure.3 Persons with HIV infection who have early syphilis might be at increased risk for neurologic complications and might have higher rates of inadequate serologic response with recommended regimens.4 Moreover, Syphilis–HIV co-infection had a negative impact on immune recovery and antiretroviral effectiveness.3 As a result of these, identifying factors associated with Syphilis–HIV co-infection is essential to formulate integrated clinical management approach, prevention and control strategies for HIV and STIs.
Female sex workers (FSWs) play an important role in transmitting HIV and syphilis from high-risk groups to the general population.4 HIV and T. pallidum, with epidemiological similarities co-infect the same host, and infections are generally more prevalent among FSWs.5 Moreover, FSWs bear a high burden of STIs. In Brazil, the prevalence of Syphilis–HIV co-infection among FSWs was 1.09%. The prevalence of STIs was 5.3% for HIV and 8.5% for active syphilis.6 The prevalence of Syphilis–HIV co-infection among FSWs in Rwanda was 27.4%. The prevalence was increasing with age and decreased with the level of education. The study also revealed that Syphilis–HIV co-infection had a positive association with age 25 years and older, having had a genital sore in the last 12 months, and having had an HBsAg-positive test.5 According to a study conducted in Kigali, Rwanda, the prevalence of serologic syphilis was 43% in HIV-positive and 19% in HIV-negative FSWs.7
In Russia, weighted HIV prevalence was 3.1% and for syphilis it was 13.9%. Factors associated with HIV–STIs co-infection were having never been tested for HIV and having a low level of knowledge regarding HIV transmission, showed 2-fold and 5-fold increases, respectively, compared with the control group.8
Over the last two decades, Ethiopia has been one of the hardest hit countries by the HIV epidemic in Africa. The HIV epidemic remains one of the major public health challenges in Ethiopia, causing significant morbidity and mortality since the mid-1980s. The Ethiopian adult (15–49 years of age) HIV prevalence was 0.93% in 2019.9 The HIV epidemic in Ethiopia was characterized as mixed and heterogeneous, with wide regional variations and concentrations in urban areas, including some distinct hotspot areas driven by key and priority populations.10 The national HIV incidence rate in the adult population is estimated at 0.03% in females, with an estimated 15,000 (9,000 females and 6,000 males) new infections, the majority (67%) of these occurring in the age group below 30 years.11 A study conducted among FSWs in Dessie showed that the seroprevalence of Syphilis-HIV co-infection was 4.4%. According to the study, older age was identified as an associated factor of increased Syphilis-HIV co-infection. In the same study, marital status, sharing of sharp materials, breakage of condom, number of customers per week, genital discharge and pain had significant associations with increased STIs acquisition including Syphilis-HIV co-infection. Old age FSWs were more likely to be affected by Syphilis-HIV co-infection.12 According to another study conducted in Hawassa, the overall seroprevalence of syphilis in HIV-infected participants was 7.3%.13
In general, there is limited information on key populations in Ethiopia. The available information indicated that certain segments of the population are more affected than others due to their high level of exposure to risky sexual behaviors and limited access to health services. It is a well-known fact that, since the HIV epidemic started, FSWs have been highly exposed to HIV. This is due to their high levels of exposure to risky behaviors, their increased ability to transmit HIV when co-infected with other STIs, and their having sex with different sub-populations. Sex workers have often been described as a “core group”, namely, a small group in which the infection is endemic and from whom it spreads to the general population.14 The most at risk populations (MARPs) survey conducted in 2013 in Ethiopia showed that the aggregate estimate of HIV prevalence among FSWs in big cities and transport corridors was found to be 23.0%, with a 95% CI of 19.0–28.0.10
In summary, data and literature related to the status of the Syphilis–HIV co-infection in Ethiopia strongly indicates the need for further surveys and studies aimed at identifying and estimating the level of Syphilis–HIV co-infection and sexual behaviors of key groups and vulnerable populations who are most at risk for Syphilis–HIV co-infection and who may be fueling the epidemic. The information is essential to inform the HIV program managers, policymakers, and the design of effective strategies for the prevention and control of Syphilis–HIV co-infection among FSWs in Ethiopia.
Methods and Materials
Study Design
To determine the magnitude and determinants of Syphilis and HIV co-infection among Female Sex Workers in Ethiopia, data was extracted from the national HIV and other STIs Bio-Behavioral Survey (NHSBS), a cross-sectional study conducted using Respondent-driven sampling (RDS) technique among 6,085 FSWs in 16 regional capitals and major towns of Ethiopia from August 2019 to January 2020.
Study Area
Ethiopia is located in the Horn of Africa, with a total surface area of 1,127,127 km² bordering six African countries: Eritrea to the North, Djibouti to the East, Sudan republic and southern Sudan to the West, Somali to the Southeast, and Kenya to the South.15 Ethiopia has an administrative division that consists of nine regional capitals, two city administrations, and other major towns. The survey was conducted in regional capitals and towns of Ethiopia. The survey included Addis Ababa, Dire Dawa, Bahir Dar, Harar, Gambella, Hawassa, and Logia/Semera from regional capitals and city administrations. Among major towns in Ethiopia, Adama, Arba Minch, Kombolja/Desse, Dilla, Gondar, Jimma, Mizan, Nekemte, and Shashemene were included in the survey.
Study Population
The study populations were female sex workers in regional capitals and towns of Ethiopia.
Study Variables
The dependent variable was Syphilis–HIV co-infection, a dichotomous variable coded as “1” when the FSW’s test results became positive for both Syphilis and HIV infections and “0” when either or both of the test results became negative.
The independent variables were the demographic, socio-economic, and behavioral characteristics of the FSWs.
Inclusion Criteria
Female sex workers aged 15 years old or older, who had worked as a FSW in the selected study site for at least 30 days, and had at least four paying partners in the last 30 days prior to the survey were included in the study as participants.
Sampling Procedures and Data Collection
Training was given to the study team, which included coordinators, interviewers, blood sample collectors, coupon managers, and receptionists on survey sampling methods, procedures, data collection tools, and overall study site management.
For each study site, the initial respondents of the survey (referred to as “seeds”) were determined based on the result of formative assessment. The “seeds” were selected based on the type of sex worker, age category, and geographic location of the site. These included those FSWs who were bar- and/or hotel-based, red light houses, local drinking houses, street-based, and hidden (cell phone-based). As a result, 5 seeds for each site with less than 450 sample sizes, 6–8 seeds for each site with between 450 and 900 sample sizes, and 12 for 1,250 sample sizes were recruited. An FSW with a known social network was given three coupons so that she can invite other FSWs in her network. The coupon was active from the day the coupon was given to the potential recruit and expired after 2 weeks or when the study was completed. Anonymously, fingerprint-based codes using biometric fingerprint scanners were used to ensure that all participants participated only once. The fingerprint information was never linked to the questionnaire, as was used only for avoiding multiple enrollments.
Each participant who was invited to participate in the study brought a coupon that identified who referred her, by number. Each new participant was given three coupons and asked to recruit three additional FSWs from their contacts. The same process continued until the desired sample size was achieved and the RDS equilibrium condition was reached. Progress towards attaining the equilibrium was monitored by using key parameters like current HIV status, type of sex work, current age, educational status, and average price per sex act.
Each participant was asked to return in 2 weeks for her second visit, where she was given compensation for successful recruitment and to assess those who received coupons and had not yet showed up. Compensation was also given for each participant she successfully recruited and also for transportation.
Data were collected using a standardized NHSBS questionnaire.
Ethical Clearance
This study complies with the Declaration of Helsinki and was performed according to approval from the Scientific and Ethical Review Office (SERO) of the Ethiopian Public Health Institute (EPHI). The study was approved during Institutional Review Board Meeting Number 027 with Protocol Number EPHI-IRB-108-2018, and Reference number EPHI-6.13/5A. As it was difficult to obtain surrogates of FSWs 15–18 years of age, they were approved by the SERO to provide informed consent on their own behalf. Participants were provided with an information sheet describing the objectives and procedures of the survey. Informed consent was obtained from each respondent to participate in the study including for interviews, blood sample collection, and for handling of the bio-specimen. A team member administering the consent, after having read aloud the informed consent in local language to the participant, signed his/her own name on the consent form and gave one copy to the participant and the remaining copy was archived in the participant’s folder.
An approved waiver of the requirement of written informed consent was used to minimize the risk of a confidentiality breach; the survey did not collect any personal identifying information from the participants. Participation in the survey was on a voluntarily basis. Moreover, participation in the survey did not pose any risk to the participants.
All the data obtained, including test results and any contact numbers, were kept confidential. The data was not linked to personal identifiers and were kept in a locked cabinet and computers were protected by passwords with access only to survey staff.
Laboratory Procedures
Blood Specimen Handling
Whole blood was used for rapid HIV, Hepatitis-B, and Syphilis testing. After collecting each study participant’s whole blood of 5 mL using an EDTA tube, HIV, HBsAg, HCV, and Syphilis testing were done soon after sample collection. After centrifuging the whole blood, the plasma was separated and liquidated into two 1.8 mL preprinted labeled Nunc® tubes for viral load quantification and quality control testing.
For each participant, the plasma was separated and stored using two Nunc® tubes (1.8 mL) at −20℃ in a nearby health laboratory until been collected by the survey team. Subsequently, plasma samples were transported to EPHI on a weekly basis enclosed with sample transport forms, by the laboratory personnel recruited as sample collectors. Plasma specimens were transported by using triple-packaged Iceboxes (with Ice packs, less than 0℃). Until testing, the plasma specimens were stored at −80℃ at the EPHI National HIV Reference Laboratory. After viral load testing, the remaining plasma samples were stored for future further testing.
HIV Testing
After collecting blood samples from survey participants, HIV testing was done using a national rapid tests algorithm, and results were returned during the second study visit. Participants who opted to receive their results earlier were referred to a local VCT delivering facility which had been contacted before the survey started. Results were communicated using nurse counselors according to the Ethiopian national guidelines for voluntary counseling and testing of HIV. New HIV-positive participants were linked to ART-providing centers.
Syphilis Testing
Syphilis was screened using the Chembio Dual Path Platform (DPP) Syphilis Screen and Confirm Assay, according to manufacturer principles and procedures from the kit insert. Training was given to lab personnel on how to conduct syphilis testing and interpret the results against control lines, based on the manufacturer’s job aid.
Hepatitis-B and Hepatitis-C Testing
Hepatitis B surface antigen (HBsAg) and Hepatitis C were screened by using rapid test kits. Training was given to lab personnel on how to use the test kits and interpret results, based on the manufacturer’s job aid. QC panels consisting of a positive and negative control specimen were done in parallel with the testing procedure to ensure test kits were performing correctly.
Data Analysis
Female sex worker’s data was collected electronically using a tablet in the ODK database and was exported to an MS-EXCEL sheet, merged with lab data and converted to RDS format for analysis in R software using the RDS package. The data was further exported to SPSS V21 for statistical analysis. Descriptive statistics were computed using frequency distribution, percentages, and proportions.
In the analysis of factors associated with Syphilis–HIV co-infection, variables that yield p<0.25 in Bivariable binary logistic regression were included in multivariable binary logistic regressions. Multicollinearity was checked using the variance inflation factor at a cut-off value of 5. The model fitness was tested by Hosmer and Lemeshow’s goodness of fit χ2 test. The model was defined to be reasonably well fit, at p>0.05. The direction and strength of statistical association were measured by odds ratio with the corresponding 95% confidence interval (CI). Finally, in multivariable analysis, variables with a p-value of <0.05 were declared as statistically significant. Results are presented in frequency tables and charts.
Results
Demographic, Socio-Economic, and Behavioral Characteristics of Respondents
A total of 6,085 FSWs, from 16 towns in Ethiopia, were included in the study. The majority of the respondents (1,101; 18.1%) were from Addis Ababa. In total, 1,980 (32.5%) respondents were in the age group of 20–24 years. About half (48.4%) of the respondents were never married (Table 1).
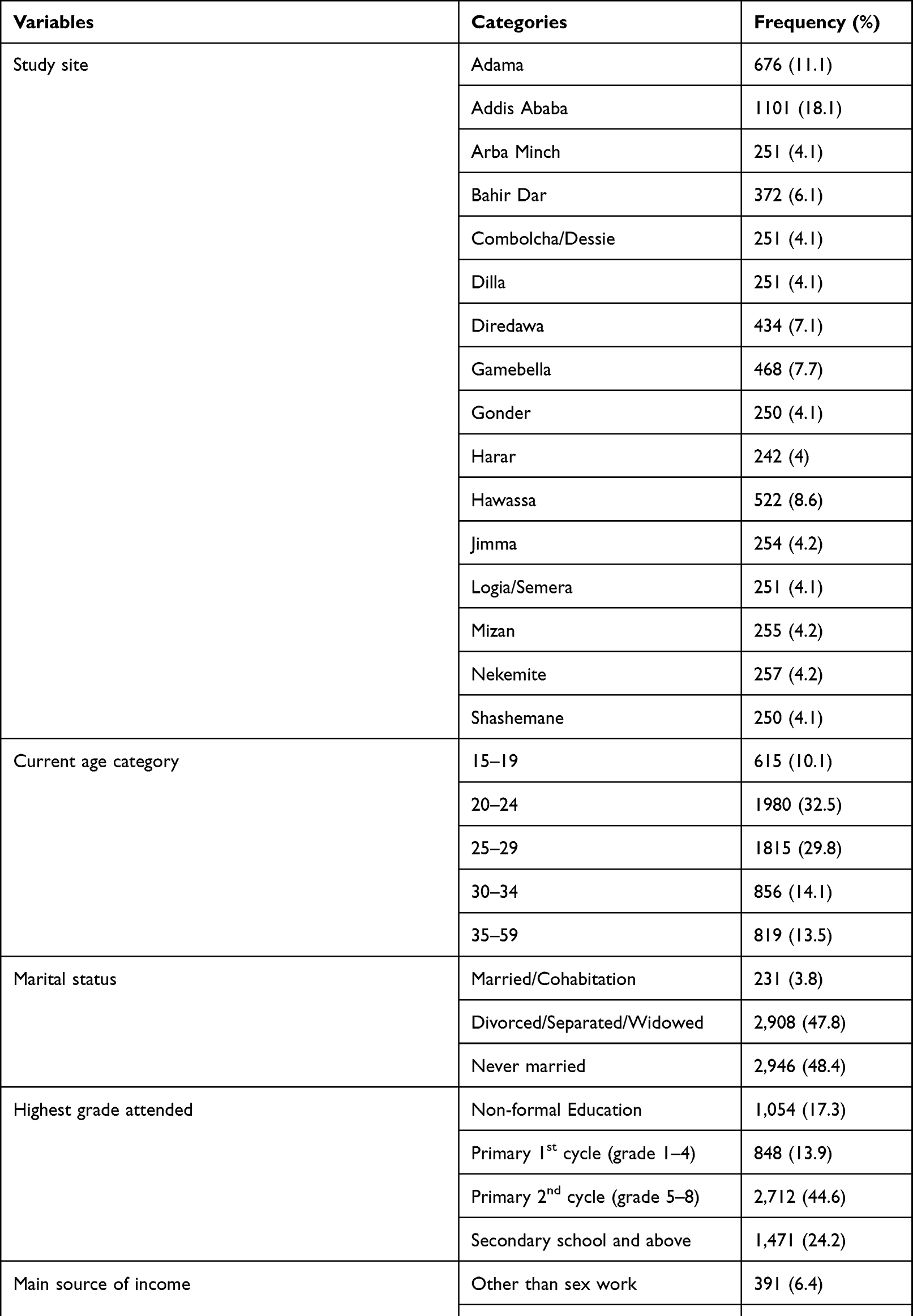 |
Table 1 Descriptive Statistics for the Demographic and Socio-Economic Characteristics of the Respondents, 2019–2020 |
Age at first selling of sex was <20 years in 2,328 (38.3%) participants; and 1,513 (24.9%) participants changed location of selling sex in the past 6 months. Among all the participants, 1,436 (23.6%), 696 (11.4%), and 1,645 (27%) had 31–60, 61–90, and more than 90 clients in the past 6 months, respectively. In the last 30 days, the number of sexual partners without consistent condom use and condom breakage were 966 (15.9%) and 1,825 (30%), respectively.
The majority of the respondents (4,449; 73.1%) had no sufficient HIV comprehensive knowledge. Out of 6,085 respondents, 639 (10.5%) were never tested or had never received a test result for HIV, 1,140 (18.7%) were positive for HIV (565 new positives and 575 known positives), 157 (2.6%) were reactive for Hepatitis B, 339 (5.6%) were reactive for syphilis, and 161 (2.6%) were syphilis/HIV co-infected.
Magnitude of Syphilis–HIV Co-Infection Among FSWs in Ethiopia
The overall weighted prevalence of Syphilis–HIV co-infection among FSWs was 2.9% (95% CI=2.6–3.2). The weighted prevalence of Syphilis–HIV co-infection was highest (8.2%; 95% CI=6.4–10.2) in Jimma town, followed by Dilla town (6.2%; 95% CI=4.7–8.2). Weighted prevalence of Syphilis–HIV co-infection by study towns is shown in Figure 1.
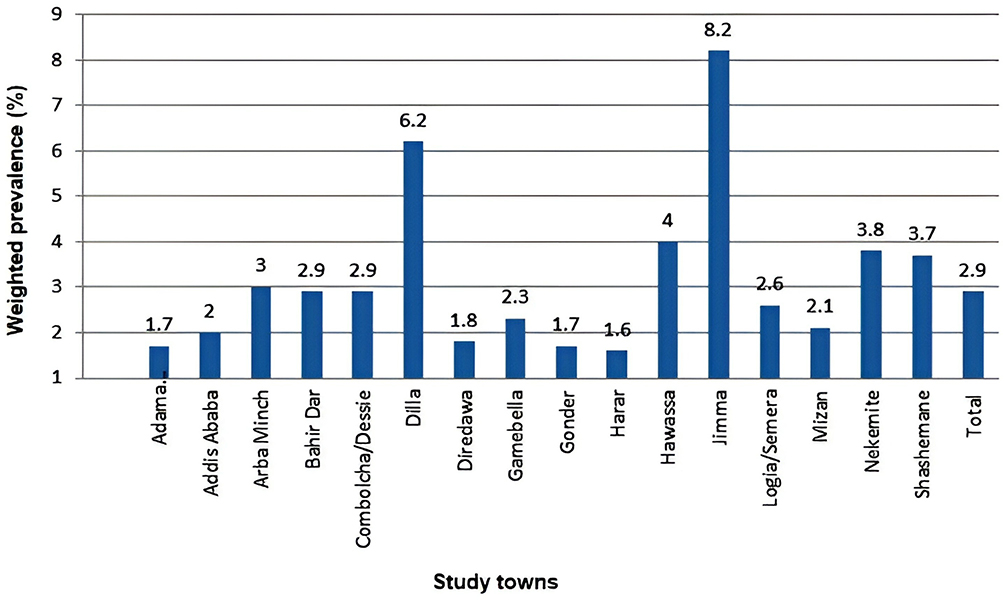 |
Figure 1 Weighted prevalence of Syphilis-HIV co-infection by study towns. The survey was conducted using respondent-driven sampling (RDS) among 6,085 FSWs in Ethiopia from August 2019 to January 2020. |
The prevalence of Syphilis–HIV co-infection among the FSWs varies depending on the participants’ demographic and socio-economic characteristics (Table 2). Moreover, the prevalence of Syphilis–HIV co-infection among the participants has shown disparities by behavioral characteristics (Table 3).
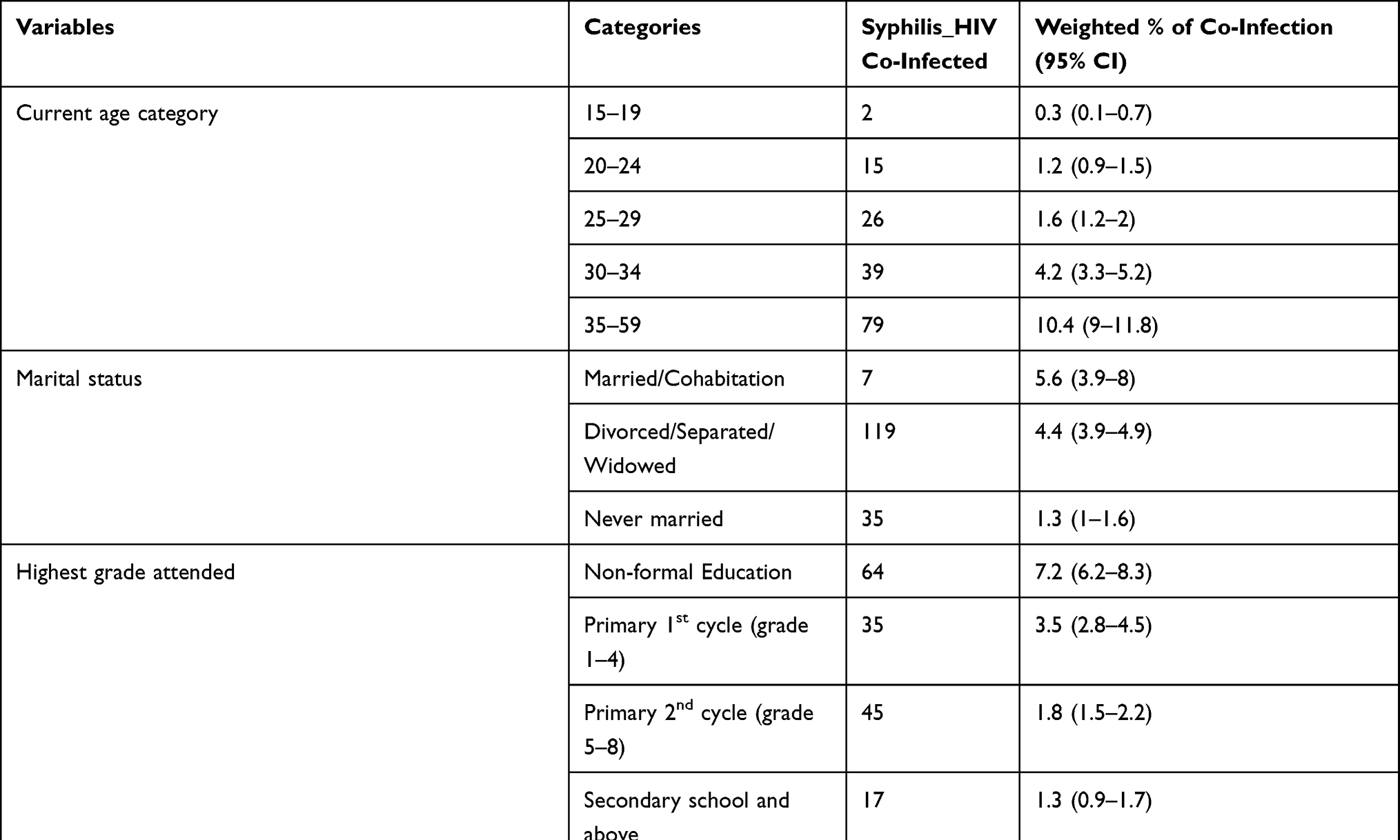 |
Table 2 Prevalence of Syphilis–HIV Co-Infection Among Ethiopian FSWs, by Demographic and Socio-Economic Characteristics, 2019–2020 |
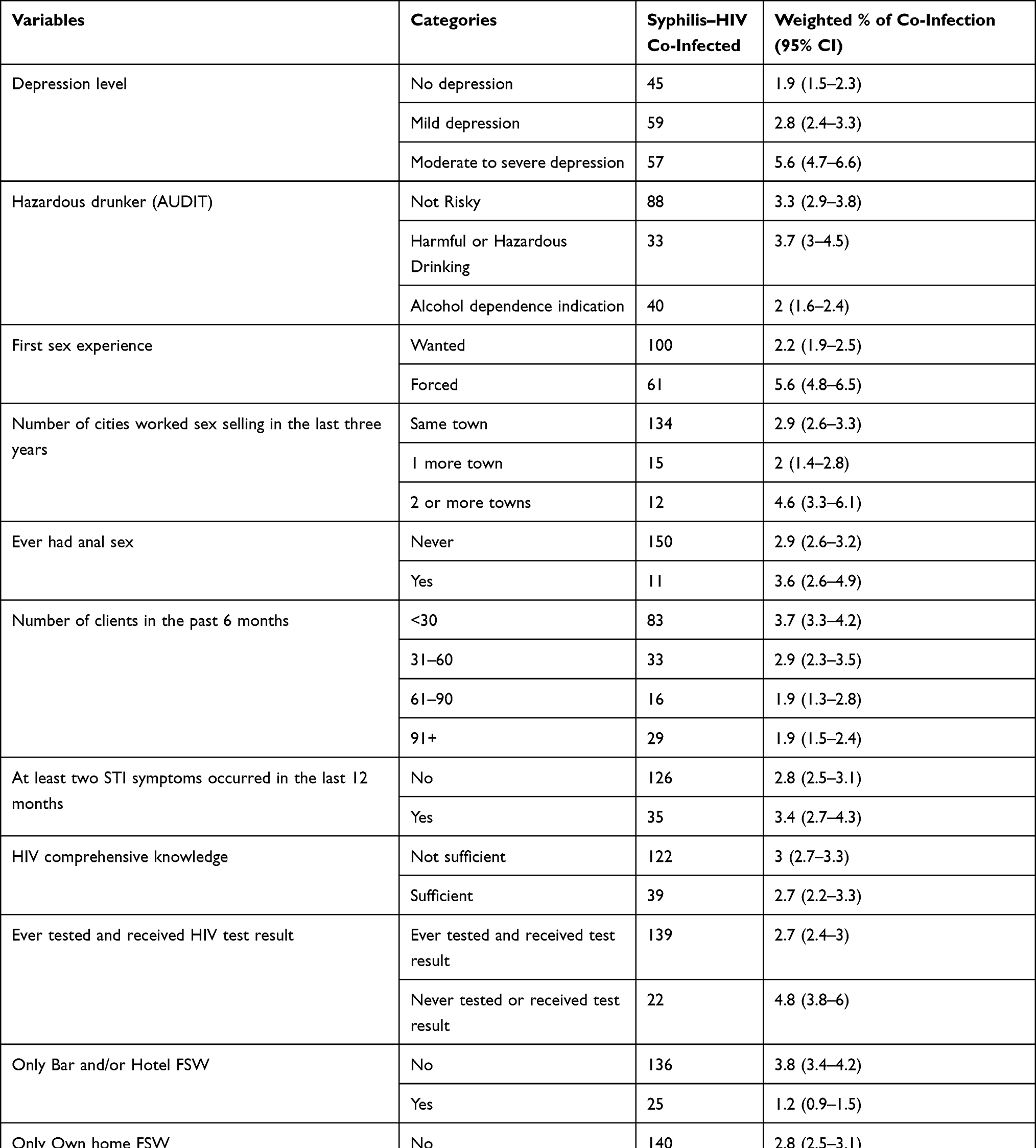 |
Table 3 Weighted Prevalence of Syphilis–HIV Co-Infection Among FSWs, by Behavioral Characteristics, 2019–2020 |
Determinants of Syphilis–HIV Co-Infection Among FSWs in Ethiopia
In univariate analysis, marital status, years lived in the current city, number of sexual partners without condom use in the last 30 days, increasing age, poor educational status, low income, major depression, forced first sex experience, condom breakage, Hepatitis B seroreactivity, and Hepatitis C seroreactivity were significantly associated with Syphilis–HIV co-infection among the FSWs.
In multivariate analysis, eight variables had shown a statistically significant association with Syphilis–HIV co-infection, but other variables (marital status, years lived in the current city, and the number of sexual partners without condom use in the last 30 days) did not show an association.
The odds of Syphilis–HIV co-infection among the age category of 15–19 years were 97% (AOR=0.03; 95% CI=0.01–0.12) less likely, compared to the age category of 35–59 years. The odds of Syphilis–HIV co-infection were 3.18-times (95% CI=1.78–5.68) higher among FSWs who attended only non-formal education. It was about 3-times (AOR=3.05; 95% CI=1.45–6.42) higher among FSWs who had an average monthly income <2,500 ETB and 1.85-times (95% CI=1.18–2.89) higher among FSWs who had major depression. The odds of Syphilis–HIV co-infection among FSWs who had forced first sex experience were 1.71-times (AOR=1.71; 95% CI=1.20–2.44, p=0.003) higher compared to FSWs who had wanted their first sex experience. The odds of Syphilis–HIV co-infection were 1.62-times (95% CI=1.14–2.30) higher among FSWs who had experience of condom breakage in the last 30 days compared to FSWs who had not experienced condom breakage in the last 30 days. The odds of Syphilis–HIV co-infection were 2.32-times (95% CI=1.10–4.90) higher among FSWs who had been reactive for Hepatitis B and 5.37-times (95% CI=1.70–16.93) higher among FSWs who had been reactive for Hepatitis C (Table 4).
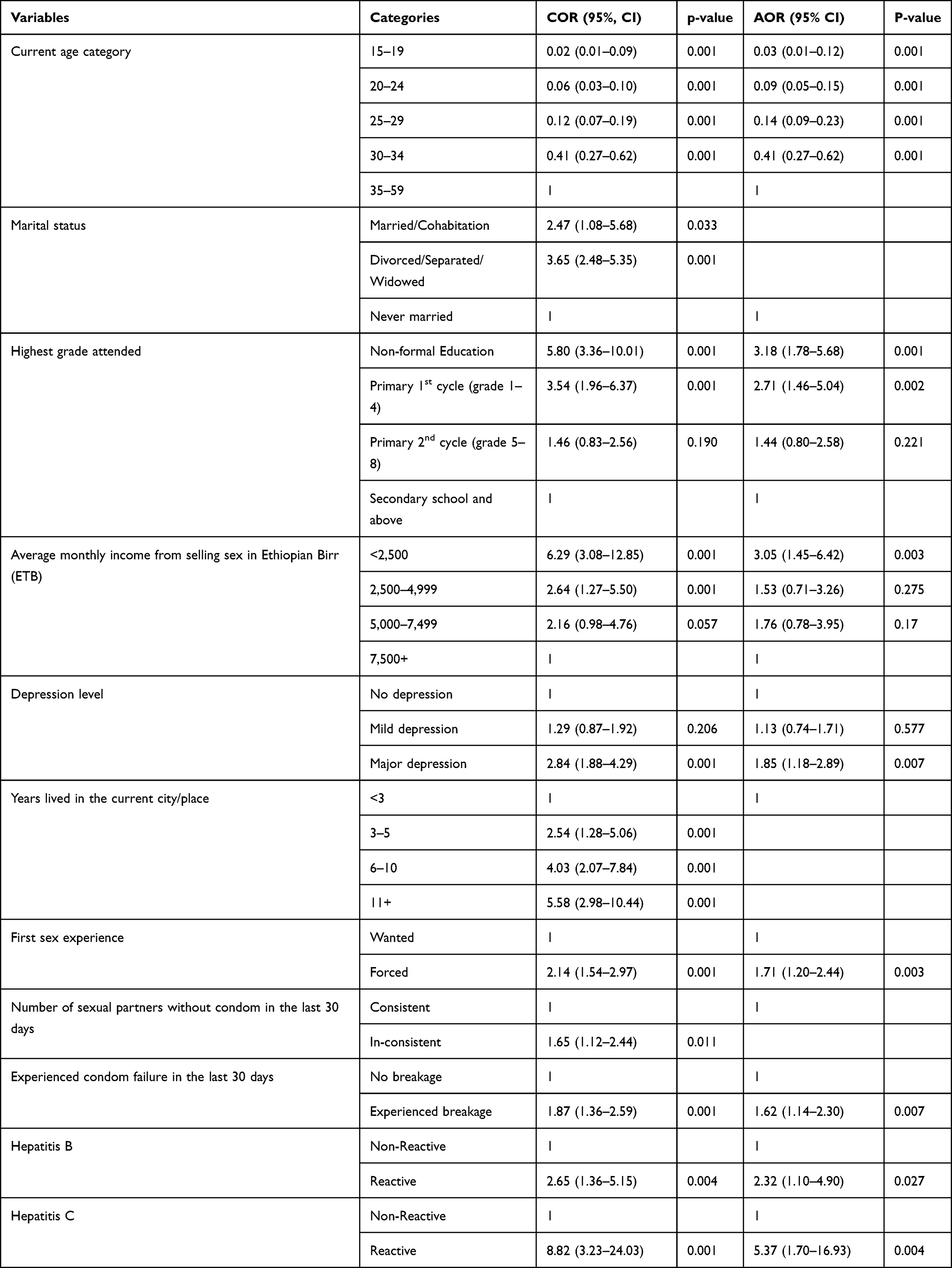 |
Table 4 Determinants of Syphilis–HIV Co-Infection Among FSWs in Ethiopia, 2019–2020 |
Discussion
Our study has shown up-to-date evidence about Syphilis–HIV co-infection among FSWs in Ethiopia. The study also revealed factors associated with Syphilis–HIV co-infection among the FSWs. According to our study findings, the prevalence of Syphilis–HIV co-infection among FSWs in Ethiopia was 2.9%. This finding was lower than the prevalence study reports from Rwanda (27.4%)5 and Mexico (23%).16 On the other hand, the result of our study was higher than the findings from a study in Brazil (1.09%).6 These discrepancies might be due to the differences between laboratory procedures, sample size, study period, socio-economic, and demographic characteristics of the FSWs. Moreover, our study also showed a Syphilis–HIV co-infection prevalence of 2.9% in Kombolcha/Dessie town; which was in line with a previous prevalence study result in Dessie (4.4%).12 The prevalence of Syphilis–HIV co-infection was highest (8.2%) in Jimma town, followed by Dilla town (6.2%). Although a published report on this related to the study area was not found, such a high prevalence of Syphilis–HIV co-infection might be due to cultural practices like polygamy, which is allowed in some religions like Muslim, which accounts for the majority of the population in these towns. Additionally, it might be related to low rates of condom use and high rates of extramarital sex by men.11 However, the current study result indicates a need for further studies in these towns to discover reasons behind the high prevalence of the Syphilis–HIV co-infection.
According to our study, the odds of Syphilis–HIV co-infection among FSWs in the age category of 15–19 years were 97% less likely, compared to FSWs in the age category of 35–59 years. Moreover, the odds of Syphilis–HIV co-infection among FSWs in the age category of 30–34 years were 59% less likely compared to FSWs in the age category of 35–59 years. The odds of Syphilis–HIV co-infection were 3.18-times higher among FSWs who attended only non-formal education and 2.71-times higher among FSWs who attended only the primary first cycle, compared to FSWs who completed secondary school and above. These findings were in line with a finding from an African cohort study where a lower education level was significantly associated with Syphilis–HIV co-infection17 and a study from Rwanda where the prevalence of Syphilis–HIV co-infection was increasing with the increasing age and decreasing with increasing level of education5 and a study in Nepal where HIV and syphilis were strongly associated with old age and low level of education.18 Similarly, a study from Dessie has revealed that the prevalence of Syphilis–HIV co-infection was increasing with the increasing age of the FSWs.12 In line with the findings of our study, a study report of the Republic of Congo showed that the age groups greater than 40 years were positively associated with behaviors at high risk of HIV (16.67%) and syphilis (6.25%) infections.19
Our study revealed the odds of Syphilis–HIV co-infection was about 3-times higher among FSWs with an average monthly income of <2,500 ETB compared to FSWs who earned an average monthly income of >7,500 ETB. This finding was corroborated by a study in China where the highest prevalence of syphilis (13.8%) was observed among socio-economically disadvantaged FSWs20 and due to the fact that syphilis was strongly correlated with HIV18 as rates of HIV diagnosis were high after women had STI.21 However, a study conducted in Togo showed there was no relation between HIV status and syphilis infection.22
In our study, the odds of Syphilis–HIV co-infection was 1.62-times higher among FSWs who had experienced condom breakage in the last 30 days compared to FSWs who had not experienced condom breakage in the last 30 days. This finding was in line with the findings from a study conducted in Dessei town which showed condom breakage was associated with an increasing prevalence of STI.12
Findings from a study conducted in Papua New Guinea showed that experiences of physical violence was associated with HIV infection among FSWs23 and 40% of FSWs experienced recent physical or sexual violence.24 The fact that syphilis was strongly correlated with HIV18 was in favor of findings from our study which shows the odds of Syphilis–HIV co-infection among FSWs who had a forced first sex experience was 1.71-times higher compared to FSWs who had wanted their first sex experience.
Our study findings showed that the odds of Syphilis–HIV co-infection were 2.32-times higher among FSWs who had been reactive for Hepatitis B compared to FSWs who had been non-reactive for Hepatitis B. This is in line with a study conducted in Rwanda where the odds of syphilis–HIV co-infection were 3-imes higher among those with a HBsAg-positive test.5
Our study covered a large scope of the study area. However, this study targeted only regional capitals and major towns of Ethiopia. Even in the selected cities, the presence of hard-to-reach sex worker groups like home-based sex workers may have not been fully represented. Lack of detailed city maps for all regional capitals and lack of street names had challenged the mapping of our study and presentation of the results.
Health program managers, health professionals, and other stakeholders may use the result of this study as a baseline during health intervention planning and implementation to maximize the sexual and reproductive health needs of FSWs. Moreover, given the high prevalence of Syphilis–HIV co-infection, the findings of this study provide general information for physicians and other clinical practitioners to modify their clinical practice and patient care in an integrated manner to maximize patient care and efficient use of resources.
Conclusion
Based on our findings, we conclude that the prevalence of Syphilis–HIV co-infection among FSWs in Ethiopia was high. To ward off Syphilis–HIV co-infection among FSWs, a special FSWs-targeted HIV and Syphilis/STIs prevention program and treatment approach needs to be devised. An outreach approach to address the sexual and reproductive health needs of FSWs has to be part of the strategy. We suggest that the government and other stakeholders need to focus on interventions that improve FSWs’ educational status, financial capacity, and healthy lifestyles.
Acknowledgments
The authors are grateful to the Ethiopian Public Health Institute (EPHI) for financial, material, and technical support. The Tuberculosis and HIV Research Directorate at the EPHI is especially acknowledged for its crucial administrative and technical support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Workowski KA, Bachmann LH, Chan PA, et al. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021;70:1–187.
2. Gong H, Hu K, Lyu W, et al. Risk factors for the co-infection with HIV, hepatitis B and C virus in syphilis patients. Acta Derm Venereol. 2020;100(17):adv00296. doi:10.2340/00015555-3657
3. Fan L, Yu A, Zhang D, Wang Z, Ma P. Consequences of HIV/syphilis co-infection on HIV viral load and immune response to antiretroviral therapy. IDR. 2021;14:2851–2862. doi:10.2147/IDR.S320648
4. Xie T, Wang G, Sun Q. Prevalence and predictors of syphilis in female sex workers in Eastern China: findings from six consecutive cross-sectional surveys. J Multidiscip Healthc. 2021;14:853–860. doi:10.2147/JMDH.S305492
5. Mutagoma M, Nyirazinyoye L, Sebuhoro D, Riedel DJ, Ntaganira J. Syphilis and HIV prevalence and associated factors to their co-infection, hepatitis B and hepatitis C viruses prevalence among female sex workers in Rwanda. BMC Infect Dis. 2017;17:525. doi:10.1186/s12879-017-2625-0
6. Ferreira-Júnior O, Guimarães MDC, Damacena GN, et al. Prevalence estimates of HIV, syphilis, hepatitis B and C among female sex workers (FSW) in Brazil, 2016. Medicine. 2018;97:S3–S8. doi:10.1097/MD.0000000000009218
7. Ingabire R, Parker R, Nyombayire J, et al. Female sex workers in Kigali, Rwanda: a key population at risk of HIV, sexually transmitted infections, and unplanned pregnancy. Int J STD AIDS. 2019;30(6):557–568. doi:10.1177/0956462418817050
8. Bernier A, Rumyantseva T, Reques L, et al. HIV and other sexually transmitted infections among female sex workers in Moscow (Russia): prevalence and associated risk factors. Sex Transm Infect. 2020;96:601–607. doi:10.1136/sextrans-2019-054299
9. Federal HIV/AIDS Prevention and Control Office (FHAPCO). HIV/AIDS National Strategic Plan for Ethiopia 2021 - 2025: Addis Ababa: FHAPCO; 2020. https://Cover frtnt.jpg (hapco.gov.et)
){kind=link}
10. Federal HIV/AIDS Prevention and Control Office (FHAPCO). Synthesis of the HIV Epidemics and Response in Ethiopia. Addis Ababa: FHAPCO; 2019.
11. Ethiopian Public Health Institute (EPHI). Ethiopia Population-based HIV Impact Assessment (EPHIA) 2017-2018: Final Report. Addis Ababa: EPHI; August 2020.
12. Metaferia Y, Ali A, Eshetu S, Gebretsadik D. Seroprevalence and associated factors of human immunodeficiency virus, Treponema pallidum, hepatitis B virus, and hepatitis C virus among female sex workers in Dessie City, Northeast Ethiopia. Biomed Res Int. 2021;2021:6650333. doi:10.1155/2021/6650333
13. Shimelis T, Lemma K, Ambachew H, Tadesse E. Syphilis among people with HIV infection in southern Ethiopia: sero-prevalence and risk factors. BMC Infect Dis. 2015;15(189). doi:10.1186/s12879-015-0919-7
14. Federal HIV/AIDS Prevention and Control Office (FHAPCO). Ethiopian Strategic Plan for the Multisectoral HIV/AIDS response, 2009-2014. Addis Ababa: FHAPCO; December 2009.
15. The Federal Democratic Republic of Ethiopia, Central Statistics Agency (CSA). The 2007 Population and Housing Census of Ethiopia. Addis Ababa, Ethiopia: CSA; July 2007.
16. Patterson TL, Strathdee SA, Semple SJ, et al. Prevalence of HIV/STIs and correlates with municipal characteristics among female sex workers in 13 Mexican cities. Salud Publica Mex. 2019;61:116–124. doi:10.21149/8863
17. Gilbert L, Dear N, Esber A, et al. Prevalence and risk factors associated with HIV and syphilis co-infection in the African cohort study: a cross-sectional study. BMC Infect Dis. 2021;21(1123). doi:10.1186/s12879-021-06668-6
18. Kakchapati S, Singh DR, Rawal BB, Lim A. Sexual risk behaviors, HIV, and syphilis among female sex workers in Nepal. HIV. 2017;9:9–18. doi:10.2147/HIV.S123928
19. Niama FR, Loukabou Bongolo NC, Mayengue PI, et al. A study on HIV, syphilis, and hepatitis B and C virus infections among female sex workers in the Republic of Congo. Arch Public Health. 2017;75:21. doi:10.1186/s13690-017-0189-5
20. Guo Y, Xu X, Fu G, et al. Risk behaviours and prevalences of HIV and sexually transmitted infections among female sex workers in various venues in Changzhou, China. Int J STD AIDS. 2017;28(11):1135–1142. doi:10.1177/0956462416689763
21. Newman DR, Rahman MM, Brantley A, Peterman TA. Rates of new human immunodeficiency virus (HIV) diagnoses after reported sexually transmitted infection in women in Louisiana, 2000–2015: implications for HIV prevention. Clin Infect Dis. 2019. doi:10.1093/cid/ciz303
22. Ekouevi DK, Bitty-Anderson AM, Gbeasor-Komlanvi FA, et al. Low prevalence of syphilis infection among key populations in Togo in 2017: a national cross-sectional survey. Arch Public Health. 2019;77(39). doi:10.1186/s13690-019-0365-x
23. Kelly-Hanku A, Weikum D, Badman SG, et al. Factors associated with HIV and syphilis infection among female sex workers in three cities in Papua New Guinea: findings from Kauntim mi tu, a biobehavioral survey. Sex Health. 2020;17(4):311–320. doi:10.1071/SH19218
24. Hendrickson ZM, Leddy AM, Galai N, et al. Work-related mobility and experiences of gender-based violence among female sex workers in Iringa, Tanzania: a cross-sectional analysis of baseline data from Project Shikamana. BMJ Open. 2018;8:e022621. doi:10.1136/bmjopen-2018-022621
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.