Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Magnetic Seizure Therapy vs Electroconvulsive Therapy in Schizophrenia: Prefrontal-Amygdala Plasticity and Cognitive Safety
Authors Li J, Jin T, Chi Y, Chen J, Gao J, Yang Y ![]() , Tian Q, Zhang X, Zheng L
, Tian Q, Zhang X, Zheng L
Received 18 May 2025
Accepted for publication 20 October 2025
Published 31 October 2025 Volume 2025:21 Pages 2415—2425
DOI https://doi.org/10.2147/NDT.S531892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Yu-Ping Ning
Jin Li,1,2,* Tingting Jin,1,* Yuyan Chi,1,* Jie Chen,1,* Ju Gao,1 Yong Yang,1 Qing Tian,1 Xiaobin Zhang,1,* Limei Zheng3,*
1Department of Psychiatry, Institute of Mental Health, Suzhou Psychiatric Hospital, The Affiliated Guangji Hospital of Soochow University, Suzhou, Jiangsu, People’s Republic of China; 2Shanghai Mental Health Center, Shanghai, People’s Republic of China; 3Department of Geriatric Psychiatry, Affiliated Nanjing Brain Hospital, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Limei Zheng, Department of Geriatric Psychiatry, Affiliated Nanjing Brain Hospital, Nanjing Medical University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: Reducing electroconvulsive therapy (ECT)’s cognitive burden without compromising efficacy is critical. Although magnetic seizure therapy (MST) shows comparable symptom remission in schizophrenia, its neuroanatomical safety—particularly limbic preservation—lacks controlled trial validation.
Patients and Methods: This triple-blind RCT (NCT02746965) randomized 34 schizophrenia patients to ECT (n=16) or MST (n=18). Structural changes were quantified via 3T MRI (FreeSurfer). Outcomes included Positive and Negative Syndrome Scale (PANSS), Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) and generalized linear mixed-effects models with FDR correction (q< 0.1).
Results: Both groups achieved comparable PANSS reduction (ECT: Δ=− 38.2± 5.1 vs MST: Δ=− 35.7± 6.4, p=0.12). MST showed superior cognitive preservation vs ECT in language (Δ=+7.2 vs ECT: Δ=− 3.1; Cohen′s d=1.15, p=0.003) and delayed memory (Δ=+5.8 vs +1.2, p=0.04). Nonsignificant between-group differences in amygdala volume changes (ECT: Δ= − 1.2% vs − 0.9%, p = 0.31).
Conclusion: As the first RCT mapping neuroanatomical changes of convulsive therapies in schizophrenia, we establish MST’s cognitive safety via prefrontal-amygdala plasticity—a novel mechanism preserving language and memory functions.
Plain Language Summary: What we studied
For severe schizophrenia where medications fail, we compared electroconvulsive therapy (ECT) and magnetic seizure therapy (MST). MST uses magnets instead of electricity and may cause fewer memory issues. This first brain-imaging randomized trial examined:
1. Effects on memory-related brain structures
2. Impacts on thinking skills
How we studied it
34 participants received ECT (16) or MST (18) for 4 weeks. We measured symptom improvement, memory/language skills and brain changes via MRI.
Key findings
• Both treatments reduced symptoms equally
• MST caused significantly fewer language problems than ECT
• Neither treatment changed amygdala size
Why it matters
MST works as well as ECT while better protecting language abilities—helping patients communicate during recovery. MST offers a safer alternative that preserves critical thinking.
Note: These results from 34 participants need larger trials for confirmation.
Keywords: neuromodulation safety, seizure therapy optimization, prefrontal-amygdala axis, therapeutic cognitive index, treatment-resistant psychosis
Introduction
Treatment-resistant schizophrenia (TRS) affects approximately 34.7% of patients unresponsive to antipsychotics.1 Electroconvulsive therapy (ECT) remains the gold-standard intervention with 68–72% acute-phase response rates,2 but induces dose-dependent cognitive impairment, particularly in hippocampal-mediated memory.3 This therapeutic limitation has driven the development of magnetic seizure therapy (MST)—an alternative neuromodulation approach using focal magnetic stimulation to achieve precise prefrontal targeting.4,5 Clinical evidence demonstrates MST’s comparable efficacy to ECT in schizophrenia. Tang et al’s RCT6 showed significant symptom reduction (PANSS Δ=−22.3±9.1, p<0.001) with 68.8% response rates after 4-week MST treatment. Systematic reviews7 confirm superior cognitive safety versus ECT, particularly in verbal memory preservation (d=0.92) and faster reorientation.
The amygdala represents a critical neural substrate in schizophrenia pathophysiology. Consistent volume reductions in TRS patients8–10 correlate with memory deficits and executive dysfunction through disrupted prefrontal-limbic connectivity.11–13 As a key node in emotional-cognitive integration circuits, its structural integrity may mediate treatment outcomes.
While ECT’s neuromodulatory effects on amygdalar morphology are documented, no controlled studies have examined MST’s impact on this limbic structure in schizophrenia. This gap is significant given MST’s targeted prefrontal activation and superior cognitive profile.
We therefore conducted the first longitudinal neuroimaging RCT to:
1. Quantify amygdalar volumetric changes following MST versus ECT
2. Examine structure–function relationships with cognitive outcomes
3. Identify neural mechanisms underlying MST’s cognitive preservation
Using FreeSurfer-based morphometry of high-resolution MRI data, this study provides novel insights into MST’s neuroanatomical safety profile.
Materials and Methods
Participants
The prospective cohort comprised n=34 hospitalized schizophrenia patients (DSM−5 criteria) prospectively enrolled at Shanghai Mental Health Center.
Inclusion
1. Age 18–55 years
2. DSM-5 confirmed schizophrenia with acute exacerbation PANSS≥80
3. Treatment resistance failure of ≥2 antipsychotics
4. Clinical indication for neuromodulation therapy
Exclusion
1. Neurological disorders, eg epilepsy, TBI
2. Substance abuse within 6 months
3. Contraindications to anesthesia/MRI
4. Pregnancy
Elimination
1. Protocol deviation, eg missed >2 sessions
2. MRI artifacts precluding analysis
Ethical Considerations
This study complies with the Declaration of Helsinki. Ethical approval was obtained from Shanghai Mental Health Center (Protocol 2014−30R). All participants provided written informed consent after detailed explanation of procedures, risks and alternatives. Specifically, for patients with full decision-making capacity, consent was signed by the patients themselves; for those lacking such capacity, eg due to severe mental illness, consent was obtained from their legal guardians or designated family members. In cases where both patient and guardian consent was required, both parties signed the consent form. Data anonymization was implemented, and participants could withdraw without penalty. An independent data safety monitoring board conducted biannual audits.
Treatment Protocol
All patients were hospitalized during the 4-week intervention period.
Pharmacotherapy
Patients maintained stable doses of antipsychotics.
ECT Protocol
Device: Thymatron System IV Somatics, USA
Electrode placement: Bitemporal
Stimulus dose: 1.5 × seizure threshold initialtitration:10
MST Protocol
Device: MagPro X100 with C-B91 coil MagVenture, Denmark
Coil position: Vertex 50
Parameters: 100% output, 25 Hz, 370 μs pulse width
Assessment Timeline Rationale
- 24–48 h post-intervention MRI timing: Based on evidence that neuroplastic changes peak within 48 h after neuromodulation (Deng et al, Brain Stimul 2020;13:900–910).
- Clinical/cognitive assessments: Conducted at baseline T0 and 24 h after final session T1 to capture acute treatment effects prior to discharge.
Rater Qualifications
- PANSS/RBANS assessments: Performed by two licensed psychiatrists trained to >0.85 inter-rater reliability ICC via standardized videos. Raters were blinded to treatment allocation and prohibited from clinical management.
NCT Number: NCT02746965; Registration Date: 01/03/2017; Study URL: https://clinicaltrials.gov/study/NCT02746965; Study Type: INTERVENTIONAL.
Computer-generated permuted block randomization block size = 6 was implemented via SAS v9.3 with 1:1 allocation ratio, while maintaining allocation concealment through sequentially numbered opaque envelopes audited by trial statisticians. A biostatistician, blinded to the study subjects, performed the randomization. Each subject dispensed a sequentially numbered identifier indicating their randomization assignment. After baseline assessments, the treating clinician obtained the treatment code before the first ECT or MST session. Identical pretreatment environments, equipment configuration and room setup maintained patient blinding. An independent assessor blinded to group allocation performed clinical and psychological evaluations.
Power Analysis
Using G*Power 3.1.9.7,14 with parameters α = 0.05, power = 0.80 and effect size f = 0.25 (Based on typical effect sizes in neuromodulation studies15), a minimum sample of 26 participants (13 per group) was required for repeated-measures ANOVA. Our final cohort (n = 34) achieved 88.7% statistical power to detect interactions between time and group.
MST and ECT Procedures
Treatment protocols for ECT/MST aligned with standard Chinese clinical practice,16 delivered over a 4-week regimen, 10 sessions: three biweekly, followed by two biweekly, supplementing standard therapy. A combined intravenous regimen of etomidate 0.21−0.3 mg/kg and propofol 1.82−2.44 mg/kg under general anesthesia facilitated procedures, with succinylcholine 1 mg/kg and atropine 0.5 mg coadministered to mitigate secretions and induce myorelaxation.
MST was administered using a MagPro X100 system MagVenture A/S, Denmark, with a C-B91 butterfly coil. Stimulation parameters were standardized at 100% maximum stimulator output, 25 Hz frequency and 370 μs pulse width, generating a peak magnetic field intensity of 4.2 Tesla.
MST implementation adhered to our prior methodology.17 Bitemporal ECT was delivered via Thymatron System IV Somatics, USA, with a pulse width of 1.0 ms and energy percentage automatically calculated 0.8×age. Prefrontal EEG monitoring utilized frontal-mastoid electrode placement, while ictal activity duration was quantified from stimulus initiation magnetic/electric to termination.
Clinical and Cognitive Assessment
Cognitive evaluation utilized the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS),18 capturing baseline performance and treatment-related changes, improvements/adverse effects. Schizophrenia symptom severity was quantified via the Positive and Negative Syndrome Scale (PANSS).19
Magnetic Resonance Image Acquisition
Structural MRI acquisitions occurred at two timepoints: T0, T1. Subjects were instructed to maintain wakefulness with eyes closed and minimize cognitive focus during scanning. Imaging employed a 32-channel head coil-equipped 3T Siemens Verio Syngo MR B17 scanner with stabilization foam pads. A 3D T1-weighted MPRAGE protocol was executed TR/TE = 2530/2.56 ms; matrix=256×256; flip angle=7°; 224 contiguous 1.0 mm slices; isotropic 1.0 mm³ voxels.
Image Preprocessing
Image preprocessing leveraged the SPM12 and REST_1.8 toolkits for pipeline execution. Experienced radiologists conducted artifact screening prior to AC-PC alignment of 3D-MPRAGE data. Subsequent processing utilized FreeSurfer 7.2.0’s automated subcortical segmentation protocol, with all outputs undergoing researcher-driven quality control.
Statistical Analysis
All analyses tested a priori hypotheses defined in the Introduction. All analyses utilized SPSS software. Between-group comparisons ECT vs MST employed independent t-tests or χ²-tests as data type dictated, while repeated-measures ANOVA evaluated pre-post treatment changes in Amygdala volumetric data, clinical symptoms and cognitive performance. The illness duration and current episode length as covariates in ANCOVA models.
Post-treatment symptom (PANSS) and cognitive improvements demonstrated significant associations with volumetric shifts, covarying for age/education. Group-specific (MST/ECT) Spearman correlations with Bonferroni correction linked amygdala volumes to neurocognitive and clinical metrics, thresholded at p < 0.05.
All correlation analyses between amygdala volume changes and clinical/cognitive measures Tables 1 and 2 employ Bonferroni correction within each hypothesis family:
For cognitive domains 6 comparisons: P2 = P1*6
For PANSS subscales 4 comparisons: P2 = P1*4
Uncorrected p-values (P1) are reported for transparency. When P1 is statistically significant, we compute and report the P2 value; when P1 is non-significant, P2 values are neither computed nor reported.
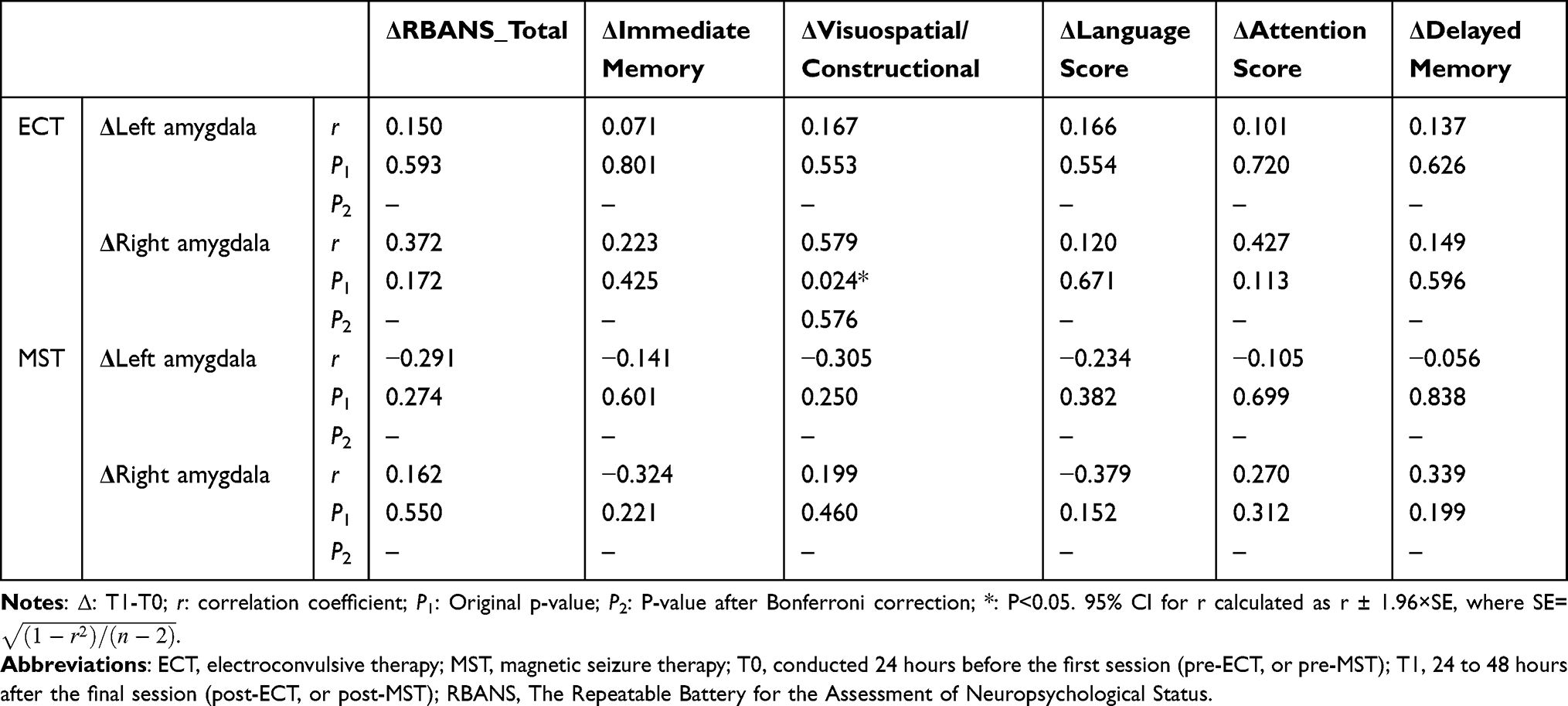 |
Table 1 The Association of Amygdala Volumetric Change and Cognitive Performance in ECT and MST Intervention Groups |
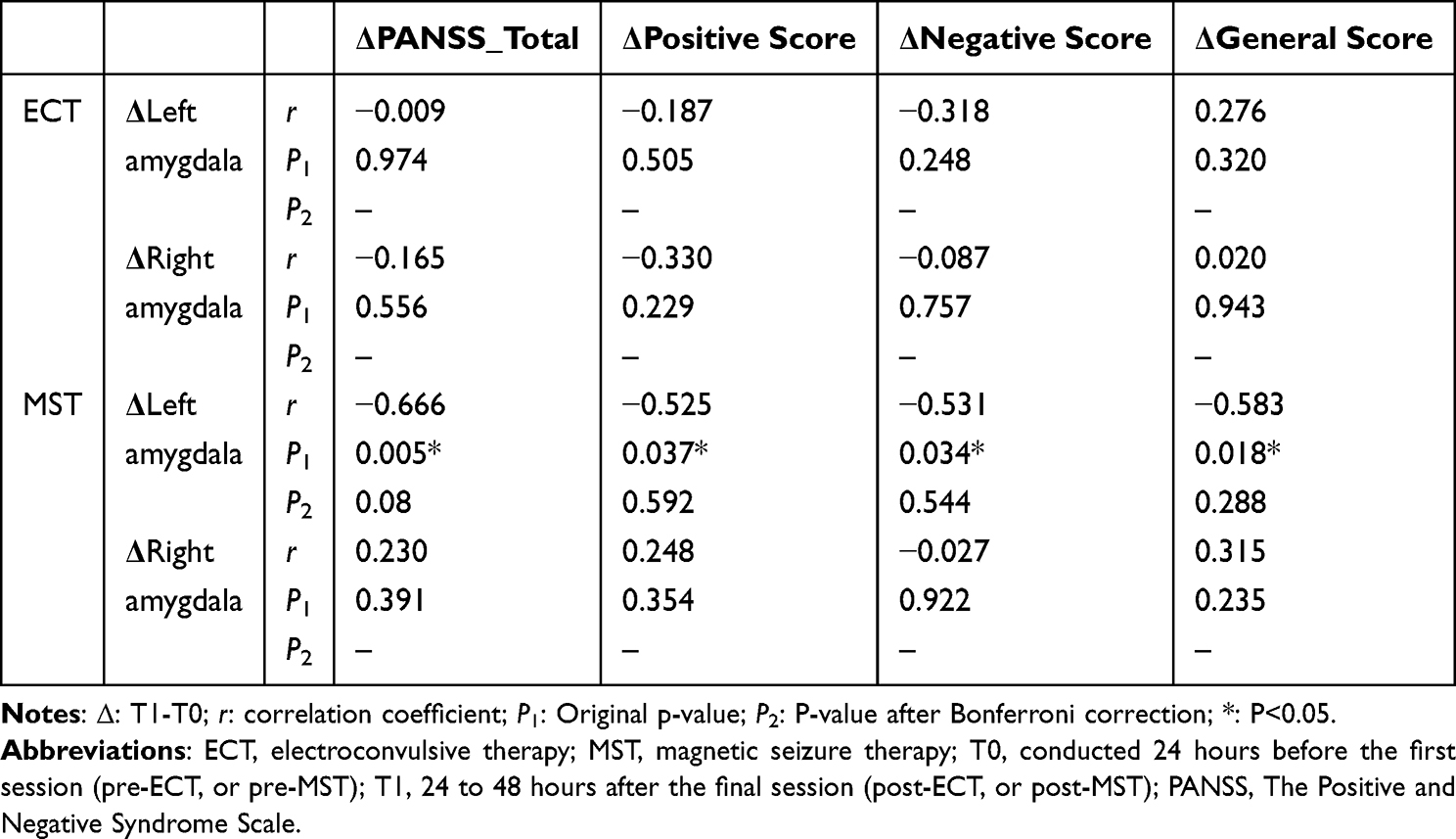 |
Table 2 The Association of Amygdala Volumetric Change and PANSS in ECT and MST Intervention Groups |
Results
Participant Flow
A total of 60 individuals with schizophrenia were assessed for eligibility between January 2019 and March 2021. Of these, 14 were excluded 9 did not meet inclusion criteria, 5 declined to participate. The remaining 46 participants were randomized to receive either MST (n=27) or ECT (n=19). During the 4-week intervention, 12 discontinued treatment: ECT, Withdraw (change of diagnosis, n=2), Discontinued intervention (hypotension, n=1); MST, Withdraw before the first session (n=1), Withdraw (financial difficulty, change of diagnosis, hypotension, change to ECT, wear-out of MST coils, n=5), Discontinued intervention (liver dysfunction, conjunctiva hemorrhage, swelling arm, n=3). Consequently, 34 patients completed all assessments and were included in the final analysis (ECT: n = 16; MST: n = 18). Participant flow is depicted in Figure 1.
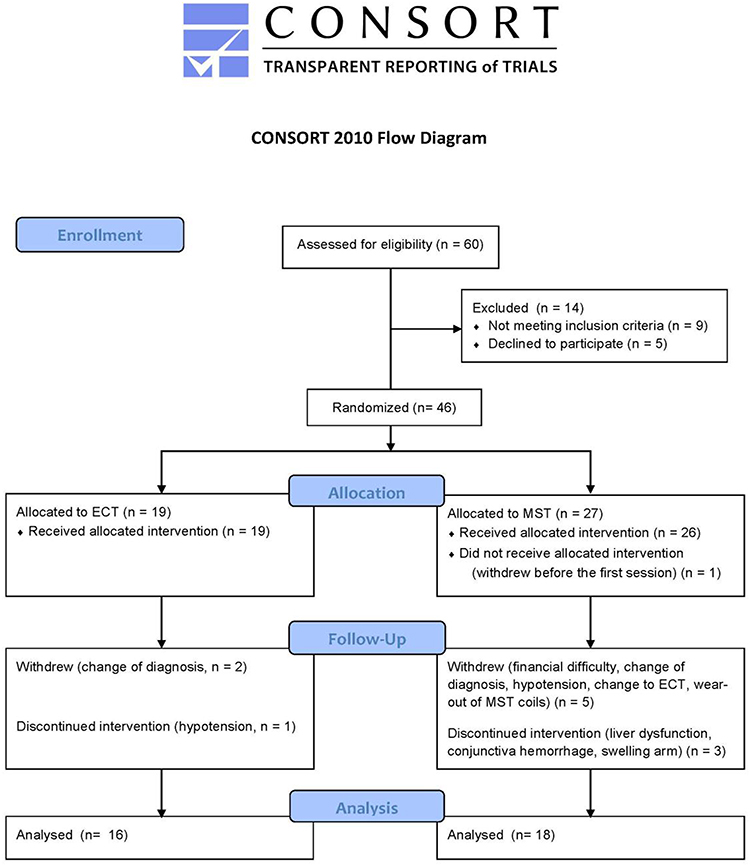 |
Figure 1 The CONSORT diagram of patient selection. |
Demographics and Clinical Characteristics
As shown in Table 3, demographic variables were comparable between the ECT and MST cohorts, except for a significantly longer illness duration in the MST group (P=0.049). No statistically significant disparities were observed in sex distribution, age, education, current episode duration or antipsychotic dosage. Confirming our primary clinical hypothesis, longitudinal analysis of PANSS total and subscale scores revealed neither a main effect of treatment modality nor a group × time interaction T1vs.T2. As shown in Table 4, these results indicate that ECT and MST exhibit equivalent therapeutic efficacy when assessed through PANSS-based clinical improvement criteria.
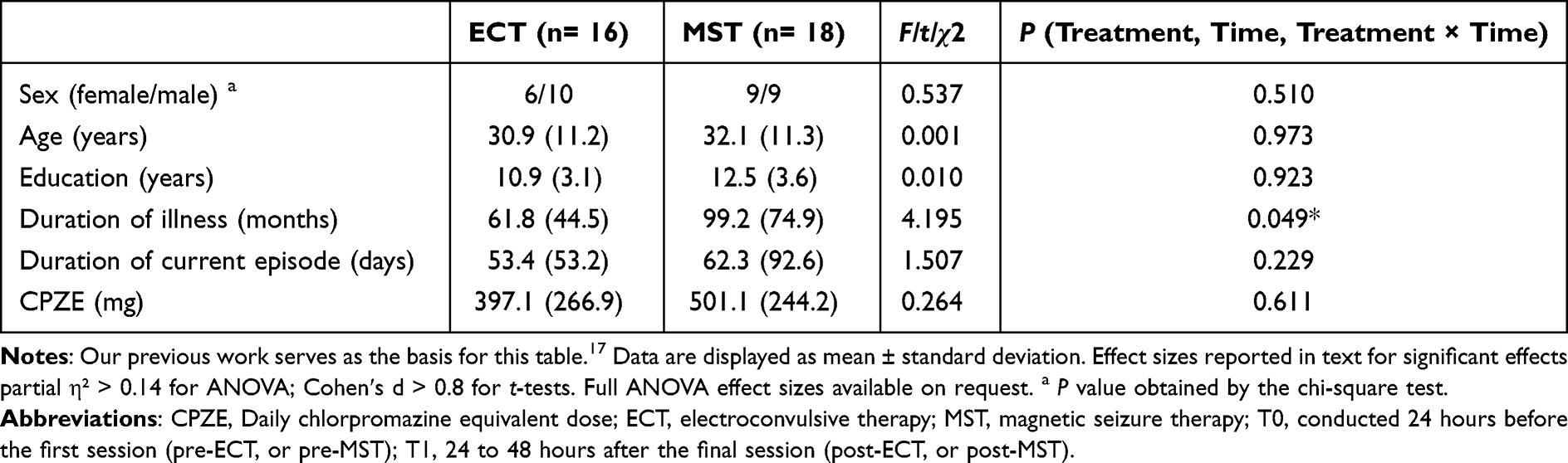 |
Table 3 Demographic in ECT and MST Groups |
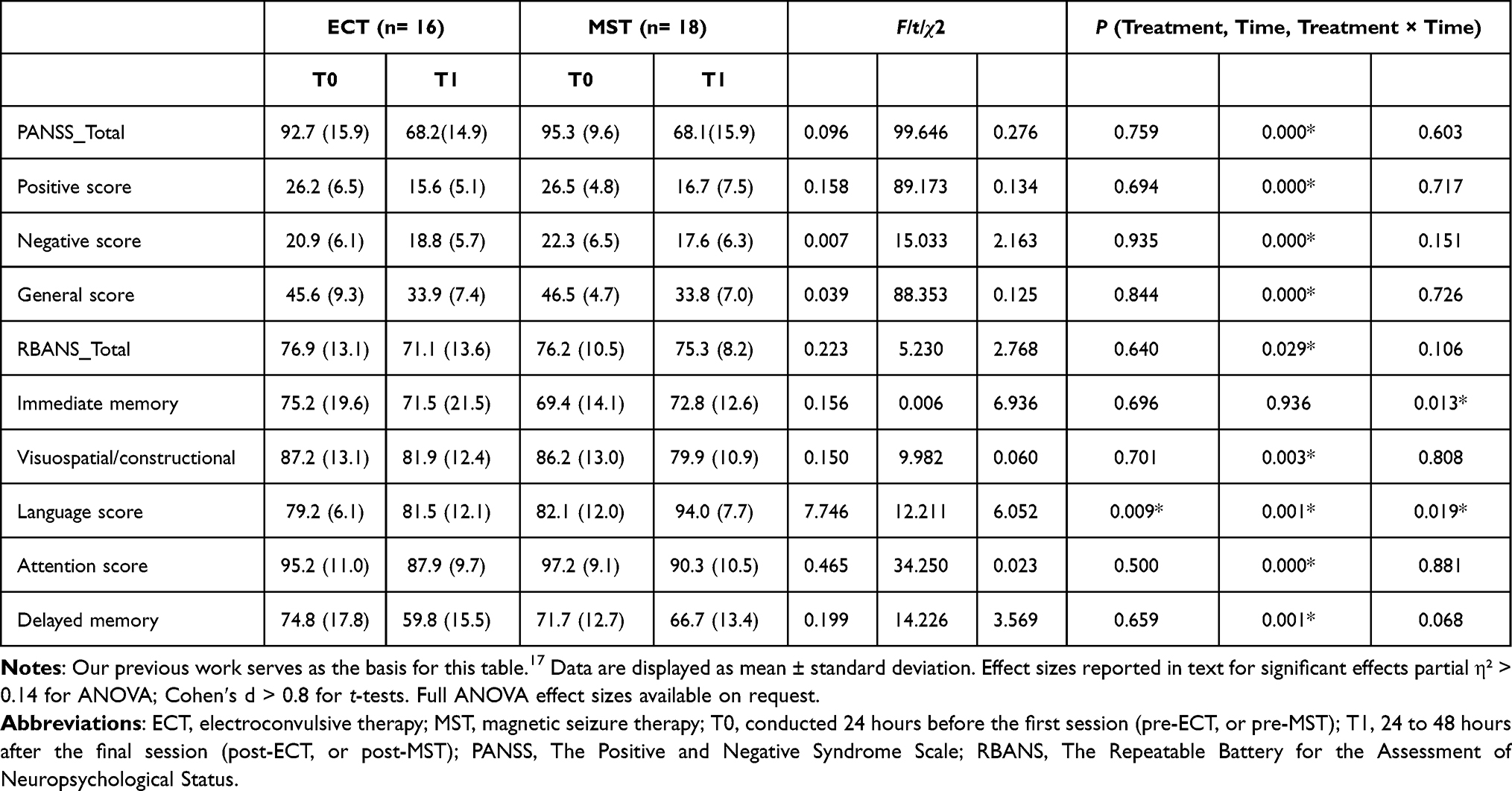 |
Table 4 Clinical Characteristics and Neuropsychological Scores in ECT and MST Groups |
Supporting the cognitive safety hypothesis for MST, the RBANS language score demonstrated a significant group × time interaction (P=0.019, partial η² = 0.168), with both treatment modality (P=0.009, partial η² = 0.205) and timepoint (P=0.001, partial η² = 0.289) independently influencing outcomes. Simple effects analysis indicated that language function improved significantly following MST (Cohen’s d = 1.02, 95% CI 0.38,1.66) but remained unchanged with ECT (d = 0.19, 95% CI 0.47,0.85).
All participants achieved successful seizure induction, with MST exhibiting markedly shorter EEG durations 13.9±3.9 s compared to ECT 33.8±6 s.
Comparison of Volume of Amygdala
Neither ECT nor MST demonstrated a significant main effect on amygdala volumes bilaterally. Partially validating the neuroplasticity hypothesis, temporal assessments revealed distinct neurobiological responses: a statistically significant group × time interaction emerged in the left amygdala P = 0.009, partial η² = 0.21, while changes in the right amygdala did not show treatment-specific effects (see Table 5). However, contradicting expectations, within-group analyses indicated no significant volumetric changes over time in either treatment cohort all P > 0.10.
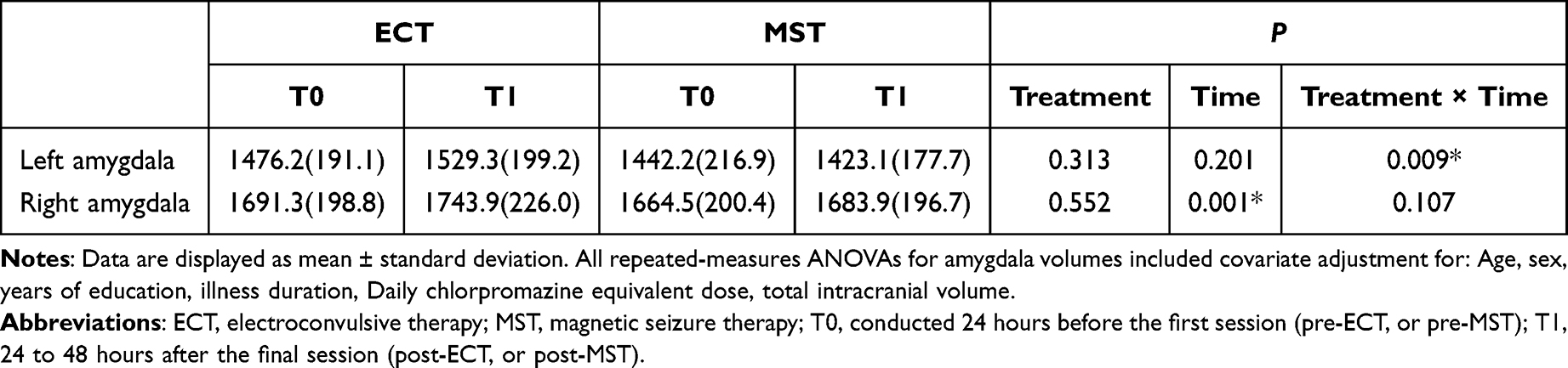 |
Table 5 Changes in Amygdala Volumes Between Baseline and Post-Treatment Follow-Up Among ECT and MST Intervention Groups |
The Amygdala Volumetric Change and Cognitive Performance
Rejecting the mechanistic correlation hypothesis, analyses revealed no statistically significant associations between amygdalar structural plasticity and neurocognitive trajectories after correction for multiple comparisons. An uncorrected positive correlation was observed between amygdala volume change and visuospatial/constructional score improvement in the ECT group (r = 0.579, 95% CI 0.15,1.00, uncorrected P=0.03), but this did not survive Bonferroni correction corrected P = 0.24. The exploratory association is visualized in Figure 2.
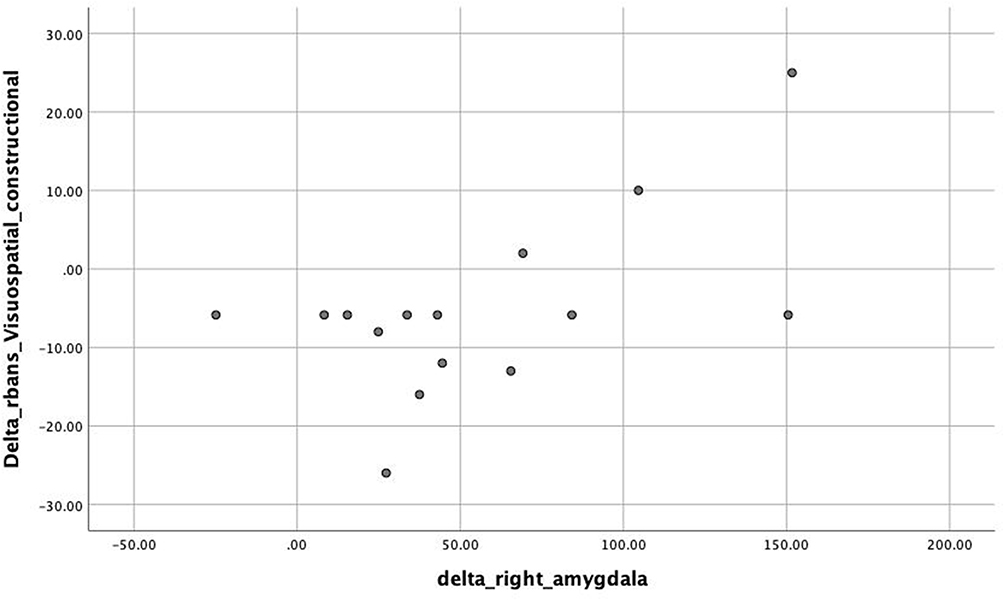 |
Figure 2 Association between changes in right amygdala volume and improvement in RBANS scores (Visuospatial/constructional) following ECT treatments. Abbreviations: ECT, electroconvulsive therapy; MST, magnetic seizure therapy; T0, conducted 24 hours before the first session (pre-ECT, or pre-MST); T1, 24 to 48 hours after the final session (post-ECT, or post-MST); RBANS, The Repeatable Battery for the Assessment of Neuropsychological Status. Note: delta: T1-T0. |
The Association of Amygdala Volumetric Change and PANSS
No significant correlations survived multiple comparison correction between amygdala volumetric change and PANSS scores. In the MST group, an uncorrected negative correlation was observed between left amygdala volume reduction and PANSS total score improvement (r = −0.666, uncorrected p = 0.005), but this represented a trend-level association after Bonferroni correction corrected p= 0.08. Figure 3 illustrates this exploratory relationship.
 |
Figure 3 Association between changes in left amygdala volume and improvement in PANSS scores (Total) following MST treatments. Abbreviations: ECT, electroconvulsive therapy; MST, magnetic seizure therapy; T0, conducted 24 hours before the first session (pre-ECT, or pre-MST); T1, 24 to 48 hours after the final session (post-ECT, or post-MST); PANSS, The Positive and Negative Syndrome Scale. Note: delta: T1-T0. |
Perspective on Novelty and Effect Sizes
Our findings demonstrate MST’s cognitive safety advantage in language function d = 1.02 vs ECT d = 0.19 and a statistically significant differential neuroplastic response in the left amygdala η² = 0.21. While exploratory correlations showed large effect sizes, eg r = 0.579 for ECT − related visuospatial improvement, these require replication in larger samples due to non-significance after multiple comparison correction.
Discussion
Contrary to our hypothesis, neither MST nor ECT induced significant amygdala volumetric changes (P>0.05), challenging seizure therapy neuroplasticity models in schizophrenia.
Key secondary outcomes: Superior language safety with MST (d = 1.02 vs ECT d = 0.19, P =0.019); Differential left amygdala responses (group × time P = 0.009, η² = 0.21) without volumetric change. These secondary findings are hypothesis-generating, as amygdala-cognition correlations did not survive correction for FDR P>0.05.
Contrasting with reports of amygdala atrophy in schizophrenia, our null finding may reflect methodological distinctions: shorter intervention duration (4 vs 12+ weeks); medication-stabilized cohort characteristics; limited sensitivity to microstructural changes.
Notably, volumetric preservation correlates with neurocognitive sparing in early psychosis,20 suggesting our cohort’s amygdalar integrity may represent a compensatory mechanism.
Recent meta-analyses highlight MST’s favorable cognitive profile versus ECT, though evidence remains inconsistent across studies. While some report significant cognitive preservation with MST in schizophrenia,7 others note variable cognitive outcomes in depression trials.21
Contextualizing MST among emerging neurostimulation therapies, a recent systematic review22 confirms MST’s comparable efficacy and superior cognitive safety profile versus ECT for major mental disorders. Other recent advances include nonconvulsive electrotherapy (NET) demonstrating reduced cognitive impairment versus conventional ECT,23 though Transnasal humidified rapid-insufflation ventilatory exchange (THRIVE)-enhanced ECT currently lacks cognitive outcome data.24 Among non-seizure interventions, MST provides stronger antipsychotic efficacy than deep TMS25 avoiding continuous theta burst stimulation (cTBS)26 or Stanford neuromodulation therapy (SNT)’s unestablished applicability to psychosis.27
The following limitations should be considered:
- Concomitant antipsychotic use may influence volumetric findings → Future studies should include medication-naïve patients.
- The 4-week follow-up prevents assessment of long-term structural stability → Longitudinal trials with 6–12 month endpoints are needed.
- Lack of functional connectivity data precludes circuit-level analysis → Resting-state fMRI integration is recommended.
- Automated segmentation may have limited sensitivity to subtle changes → Manual verification protocols could supplement future work.
Conclusion
The amygdala plays a central role in schizophrenia neuropathology. Contrary to our primary neuroplasticity hypothesis, this first investigation of MST-induced amygdalar structural changes in schizophrenia demonstrated no significant volumetric alterations post-intervention. While a group-by-time interaction (P = 0.009) suggested differential neurobiological responses to MST versus ECT, this exploratory finding requires replication given non-significant absolute volume changes. Our null result directly addresses the study’s core objective, though three limitations constrain interpretation: limited sample size, short follow-up 4 weeks and illness-duration imbalance. Collectively, these findings challenge prevailing models of seizure therapy-induced neuroplasticity while establishing foundational evidence for MST’s structural safety profile in schizophrenia.
Data Sharing Statement
We, the authors of this manuscript, intend to share individual de-identified participant data from the clinical trial reported herein. This commitment aligns with Dove Medical Press’s data sharing policies and aims to promote transparency and reproducibility in psychiatric research.
The specific data to be shared includes de-identified demographic information, eg age, gender, diagnosis, clinical assessment results, eg psychiatry symptoms scales, treatment response metrics, intervention details and outcome measures, eg efficacy and safety endpoints. All data will be anonymized to protect participant confidentiality, according to ethical guidelines.
Additionally, the following documents will be made available: the full study protocol, statistical analysis plan, informed consent form template and case report form templates.
The data will be accessible upon request by contacting the corresponding author via Email at [email protected]. This contact information will be published with the manuscript to facilitate access.
The data and associated documents will be made available immediately upon publication of this manuscript. They will remain accessible for at least 1 year to support future research endeavors.
Acknowledgments
This study was supported by Suzhou clinical Medical Center for mood disorders (No. Szlcyxzx202109), Suzhou Key Laboratory (SZS2024016), Multicenter Clinical Research on Major Diseases in Suzhou (DZXYJ202413), Suzhou Municipal Sci-Tech Bureau (SKY2022066), Suzhou Key Diagnosis and Treatment (LCZX202326), Suzhou Municipal Health Commission General Project (MSXM2024034).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chakrabarti S. Clozapine resistant schizophrenia: newer avenues of management. World J Psychiatry. 2021;11(8):429–448. doi:10.5498/wjp.v11.i8.429
2. Zheng S, Chan SKW, Lee J. Managing treatment resistance in schizophrenia: a joint study in Hong Kong and Singapore. Front Psychiatry. 2022;13:1005373. doi:10.3389/fpsyt.2022.1005373
3. Ali SA, Mathur N, Malhotra AK, Braga RJ. Electroconvulsive therapy and schizophrenia: a systematic review. Mol Neuropsychiatry. 2019;5(2):75–83. doi:10.1159/000497376
4. Lee WH, Lisanby SH, Laine AF, Peterchev AV. Comparison of electric field strength and spatial distribution of electroconvulsive therapy and magnetic seizure therapy in a realistic human head model. Eur Psychiatry. 2016;36:55–64. doi:10.1016/j.eurpsy.2016.03.003
5. Deng ZD, Lisanby SH, Peterchev AV. Electric field strength and focality in electroconvulsive therapy and magnetic seizure therapy: a finite element simulation study. J Neural Eng. 2011;8(1):016007. doi:10.1088/1741-2560/8/1/016007
6. Tang VM, Blumberger DM, McClintock SM, et al. Magnetic seizure therapy in treatment-resistant schizophrenia: a pilot study. Front Psychiatry. 2018;8:310. doi:10.3389/fpsyt.2017.00310
7. Zhang XY, Chen HD, Liang WN, et al. Adjunctive magnetic seizure therapy for schizophrenia: a systematic review. Front Psychiatry. 2021;12:813590. doi:10.3389/fpsyt.2021.813590
8. Ho NF, Chong PLH, Lee DR, Chew QH, Chen G, Sim K. The amygdala in schizophrenia and bipolar disorder: a synthesis of structural MRI, diffusion tensor imaging, and resting-state functional connectivity findings. Harv Rev Psychiatry. 2019;27(3):150–164. doi:10.1097/HRP.0000000000000207
9. Okada N, Fukunaga M, Yamashita F, et al. Abnormal asymmetries in subcortical brain volume in schizophrenia. Mol Psychiatry. 2016;21(10):1460–1466. doi:10.1038/mp.2015.209
10. van Erp TGM, Hibar DP, Rasmussen JM, et al. Subcortical brain volume abnormalities in 2028 individuals with schizophrenia and 2540 healthy controls via the ENIGMA consortium. Mol Psychiatry. 2016;21(4):547–553. doi:10.1038/mp.2015.63
11. Jobson DD, Hase Y, Clarkson AN, Kalaria RN. The role of the medial prefrontal cortex in cognition, ageing and dementia. Brain Comm. 2021;3(3):fcab125. doi:10.1093/braincomms/fcab125
12. Roozendaal B, McEwen BS, Chattarji S. Stress, memory and the amygdala. Nat Rev Neurosci. 2009;10(6):423–433. doi:10.1038/nrn2651
13. Khalil M, Hollander P, Raucher-Chéné D, Lepage M, Lavigne KM. Structural brain correlates of cognitive function in schizophrenia: a meta-analysis. Neurosci Biobehav Rev. 2022;132:37–49. doi:10.1016/j.neubiorev.2021.11.034
14. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
15. Joshi SH, Espinoza RT, Pirnia T, et al. Structural plasticity of the hippocampus and amygdala induced by electroconvulsive therapy in major depression. Biol Psychiatry. 2016;79(4):282–292. doi:10.1016/j.biopsych.2015.02.029
16. lang TY, Jiang W, Ping RY, Ma X, Cotes RO, McDonald WM. Electroconvulsive therapy in China: clinical practice and research on efficacy. J ECT. 2012;28(4):206–212. doi:10.1097/YCT.0b013e31825957b1
17. Li J, Zhang X, Jiang J, et al. Comparison of electroconvulsive therapy and magnetic seizure therapy in schizophrenia: structural changes/neuroplasticity. Psychiatry Res. 2022;312:114523. doi:10.1016/j.psychres.2022.114523
18. Zhang CY, Deng YM, Li DM, et al. Reliability and validity of the repeatable battery for assessment of neuropsychological status scale in evaluation of vascular cognitive impairment in elderly han population. Noro Psikiyatr Ars. 2022;59(2):147–150. doi:10.29399/npa.27854
19. Shafer A, Dazzi F. Meta-analysis of the positive and negative syndrome scale (PANSS) factor structure. J Psychiatr Res. 2019;115:113–120. doi:10.1016/j.jpsychires.2019.05.008
20. Guo H, Ye H, Li Z, et al. Amygdala signal abnormality and cognitive impairment in drug-naïve schizophrenia. BMC Psychiatry. 2023;23:231. doi:10.1186/s12888-023-04728-6
21. Cai DB, Yang XH, Shi ZM, et al. Comparison of efficacy and safety of magnetic seizure therapy and electroconvulsive therapy for depression: a systematic review. J Pers Med. 2023;13(3):449. doi:10.3390/jpm13030449
22. Shi ZM, Su ZA, Ning T, Zheng W. Magnetic seizure therapy versus electroconvulsive therapy for major mental disorders: a systematic review. Asian J Psychiatr. 2025;103:104336. doi:10.1016/j.ajp.2024.104336
23. Zhang M, Wei X, Li SY, et al. Sex differences in the antidepressant and neurocognitive effects of nonconvulsive electrotherapy in patients with treatment-refractory depression. Alpha Psychiatry. 2024;25(1):68–74. doi:10.5152/alphapsychiatry.2024.231402
24. Deng CJ, Nie S, Mai JX, et al. Narrative review and consensus recommendations for the use of transnasal humidified rapid-insufflation ventilatory exchange in modified electroconvulsive therapy. Alpha Psychiatry. 2024;25(2):282–289. doi:10.5152/alphapsychiatry.2024.231463
25. Lan XJ, Yang XH, Mo Y, et al. Deep transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis of randomized controlled studies. Asian J Psychiatr. 2024;96:104032. doi:10.1016/j.ajp.2024.104032
26. Cai DB, Qin XD, Qin ZJ, et al. Adjunctive continuous theta burst stimulation for major depressive disorder or bipolar depression: a meta-analysis of randomized controlled studies. J Affect Disord. 2024;346:266–272. doi:10.1016/j.jad.2023.10.161
27. Lan XJ, Cai DB, Liu QM, et al. Stanford neuromodulation therapy for treatment-resistant depression: a systematic review. Front Psychiatry. 2023;14:1290364. doi:10.3389/fpsyt.2023.1290364
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.