Back to Journals » Clinical Ophthalmology » Volume 20
Macular and Functional Outcomes After Secondary IOL Implantation Using the Yamane Technique in Aphakia, IOL Subluxation, and IOL Dislocation
Authors Visioli G ![]() , Albanese GM
, Albanese GM ![]() , Magherini S, Cappiello D, Baratta C, Armentano M, Lucchino L
, Magherini S, Cappiello D, Baratta C, Armentano M, Lucchino L ![]() , Iannetti L, Gharbiya M
, Iannetti L, Gharbiya M
Received 10 December 2025
Accepted for publication 23 February 2026
Published 24 February 2026 Volume 2026:20 587908
DOI https://doi.org/10.2147/OPTH.S587908
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Giacomo Visioli,1,2,* Giuseppe Maria Albanese,1,3,* Silvia Magherini,1 Daniele Cappiello,1 Carmen Baratta,1 Marta Armentano,1 Luca Lucchino,1 Ludovico Iannetti,4 Magda Gharbiya1,4
1Department of Sense Organs - Sapienza University of Rome, Rome, Italy; 2Ophthalmology Unit, San Giovanni Addolorata Hospital, Rome, Italy; 3Pediatric Ophthalmology Department, Rothschild Foundation Hospital, Paris, France; 4Vitreoretinal Surgery Unit, Policlinico Umberto I University Hospital, Rome, Italy
*These authors contributed equally to this work
Correspondence: Giacomo Visioli, Department of Sense Organs - Sapienza University of Rome, Viale del Policlinico 155, Rome, 00161, Italy, Tel +39 0649975389, Email [email protected]
Purpose: To assess whether preoperative lens status—aphakia, intraocular lens (IOL) subluxation, or complete IOL dislocation—influences retinal and functional outcomes after secondary IOL implantation using the Yamane technique.
Methods: This retrospective study included 59 eyes undergoing the Yamane technique: 13 aphakic, 25 with subluxated IOLs, and 21 with dislocated IOLs. All patients completed a 12-month follow-up with spectral-domain OCT at 1, 3, and 12 months. The primary endpoint was cystoid macular edema (CME) or epiretinal membrane (ERM). Secondary endpoints were best-corrected visual acuity (BCVA), subjective refractive astigmatism (SRAST), and endothelial cell density (ECD). A quantile regression model was used to identify predictors of visual improvement.
Results: At 3 months, CME was observed in 19 eyes (32.2%). After excluding eyes with pre-existing macular changes, incident postoperative CME occurred in 6 eyes (10.2%). At 12 months, CME was present in 8 eyes (13.6%). Postoperative ERM developed in 5 eyes (8.5%). BCVA improved significantly in all three groups (p < 0.001), and SRAST remained stable (p = 0.819). ECD decreased significantly in subluxated and dislocated eyes but not in aphakic eyes. Baseline BCVA was the only independent predictor of visual improvement at 12 months.
Conclusion: Retinal and functional outcomes after Yamane fixation were comparable across aphakia, IOL subluxation, and IOL dislocation. Although a transient peak in CME prevalence was observed at 3 months, the incidence of new postoperative CME was limited and mainly associated with IOL explantation. Visual recovery was primarily determined by preoperative visual acuity.
Plain Language Summary: When the natural support of an intraocular lens (IOL) is lost, a secondary procedure may be required to reposition or replace the lens. The Yamane technique allows sutureless fixation of an IOL. We evaluated how this technique performs in three different clinical situations: aphakia (no lens), partial IOL subluxation, and complete IOL dislocation.
We assessed the occurrence of retinal complications such as cystoid macular edema (macular swelling) and epiretinal membrane, as well as changes in vision, astigmatism, and corneal endothelial cell density over 12 months.
Macular swelling was observed in approximately one third of eyes at 3 months; however, new postoperative cases occurred in about 10% of patients, and the prevalence decreased by the final follow-up. Vision improved significantly in all three groups, and outcomes were comparable across aphakia, IOL subluxation, and IOL dislocation. Visual recovery was primarily determined by preoperative visual acuity.
Our findings indicate that the Yamane technique provides consistent anatomical and functional outcomes across different types of lens instability.
Keywords: Yamane technique, secondary intraocular lens implantation, aphakia, IOL subluxation, IOL dislocation, cystoid macular edema, epiretinal membrane, endothelial cell density, visual outcomes, scleral fixation
Introduction
Aphakia, subluxated intraocular lenses (IOLs), and complete IOL dislocation are common indications for secondary IOL implantation and remain surgically challenging. Among the available options, the sutureless intrascleral fixation technique described by Yamane has gained widespread adoption due to its minimally invasive design and avoidance of suture-related complications.1–3
Several studies have reported favorable outcomes with the Yamane technique, including good visual recovery and refractive stability.4–6 However, most series have combined heterogeneous indications—aphakia, subluxation, and dislocation—into a single cohort, without stratifying outcomes by preoperative lens status. This limits the ability to determine whether different baseline conditions influence postoperative vision, macular complications, or endothelial changes.
Recent investigations illustrate this variability. Sahin Vural et al reported significant BCVA improvements in predominantly aphakic eyes but noted frequent need for adjunctive procedures.7 Fanelli et al found higher rates of corneal edema and cystoid macular edema (CME) in anatomically complex eyes undergoing combined Yamane implantation and vitrectomy.8 Guerin et al reported comparable visual recovery but less predictable refractive outcomes versus iris-claw IOLs.9
Macular complications remain of particular interest: Ishikawa et al described a higher incidence of CME after Yamane fixation compared with sutured scleral fixation.6,10 Whether such differences reflect the surgical technique, the need for IOL explantation, or preoperative lens status is not yet clear. Most available evidence on sutureless scleral-fixated IOL implantation involves concomitant pars plana vitrectomy (PPV), a setting associated with increased postoperative inflammatory response and dynamic macular changes, including transient CME, particularly in complex secondary IOL cases.11–13 Comparative analyses and long-term series suggest that macular complications, including CME and retinal detachment, vary primarily according to surgical approach, case complexity, and adjunctive procedures rather than fixation technique alone.14
To date, no study has comprehensively compared anatomical and functional outcomes after Yamane fixation across aphakia, IOL subluxation, and dislocation. The influence of preoperative status on endothelial cell density, refractive stability, and macular changes also remains insufficiently defined. The aim of this study is to determine whether preoperative lens status affects the incidence of postoperative CME and epiretinal membrane (ERM) after Yamane secondary IOL implantation. Secondary objectives include assessing differences in best-corrected visual acuity (BCVA), subjective refractive astigmatism (SRAST), and endothelial cell density (ECD) among the three groups.
Materials and Methods
This retrospective study included patients who underwent secondary intraocular lens (IOL) implantation using the Yamane technique at the Vitreoretinal Surgery Unit of the Ophthalmology Clinic, Policlinico Umberto I, Sapienza University of Rome, between May 2021 and February 2024. The study adhered to the tenets of the Declaration of Helsinki.
In our cohort we included patients > 18 years of age, with aphakia, subluxated IOL, or dislocated IOL who undergo secondary implantation surgery using the Yamane technique. Only patients with a complete 12-month follow-up were included, as all cases were monitored through this fixed interval. Inclusion required spectral-domain OCT imaging at 1, 3, and 12 months, and available ECD measurements at both baseline and 12 months.
Patients were excluded in the presence of glaucoma or intraocular pressure greater than 21 mmHg at baseline, a cup-to-disc ratio greater than 0.5 on OCT, active intraocular uveitis or previous history of uveitis, corneal pathologies affecting surgical outcomes, retinal condition such as age-related macular degeneration, vascular occlusion, inherited dystrophies, or retinal detachment. Diabetic patients were excluded to minimise potential confounding effects on macular changes.
Clinical data were collected at baseline and at 1, 3, and 12 months postoperatively. Parameters included age, sex, the preoperative status of the lens, categorized into aphakia (Group 1), subluxated IOL (Group 2), and complete IOL dislocation (Group 3)—time elapsed since previous surgery, history of pars plana vitrectomy, (BCVA), subjective astigmatism variation (SA), endothelial cell count (measured only at baseline and 12 months), and axial length (AXL). Biometric measurements were obtained using the IOLMaster 500 (Carl Zeiss Meditec, Dublin, CA, USA). IOL power was calculated using the SRK/T formula. The target refraction was determined individually based on patient preference. Manufacturer-recommended IOL constants were used. OCT scans (Spectralis OCT, Heidelberg, Germany) were reviewed to detect postoperative CME or ERM. Data regarding any intraoperative IOL explantation or retinal membrane peeling were also recorded. ECD, polymegathism, and pleomorphism were evaluated using the Perseus endothelial microscope (CSO, Florence, Italy). BCVA was measured using the standardised 70-letter ETDRS chart (Chart “R”, Precision Vision, La Salle, IL, USA) at a 4-meter distance.
Surgical Technique
The procedure was performed under local or, when necessary, general anesthesia by experienced surgeons (MG and LI). A 3-piece IOL PU6AS KOWA (Kowa Co LTD) was used for implantation. A complete pars plana vitrectomy was performed to clear the vitreous cavity. In all cases requiring IOL explantation, the dislocated one-piece IOL was removed via pars plana vitrectomy using an intraocular Pacman segmentation technique.15 The surgeons created 2 mm-long scleral tunnels parallel to the limbus and positioned 180 degrees apart: the scleral tunnels were created 2.50 mm from the limbus using a PRC-300131 30 Gauge × 13 mm ultra-thin-walled needle (TSK STERiJECT, TSK Laboratory, Japan) The leading haptic of the 3-piece IOL was inserted into the lumen of one of the needles and then externalised. A second needle was used to create the opposite sclerotomy, and the trailing haptic was threaded into this needle and externalised thereafter. The externalised haptics were cauterized with a low-temperature cautery device, creating small flanges at the ends. These flanges prevent the haptics from slipping back into the sclera. The flanged haptics were gently pushed back into the scleral tunnels, securing the IOL in place. A peripheral iridotomy was performed to prevent iris capture. The anterior chamber is checked for stability.1,16
After surgery, patients received topical antibiotics (4 times a day for 10 days) as well as dexamethasone eye drops (4 times a day for 10 days and then tapered every week). After 10 days, they also received topical non-steroidal anti-inflammatory drugs (NSAIDs) eye drops for the following 3 months.17
Statistical Analysis
All statistical analyses and figure generation were performed using Stata version 18.0 (StataCorp LLC, College Station, TX, USA). Data distribution was assessed using the Shapiro–Wilk test. Continuous variables are presented as mean ± standard deviation or median with interquartile range (IQR), as appropriate, while categorical variables are reported as absolute values and percentages. For comparisons among the three groups, one-way ANOVA or the Kruskal–Wallis test was used according to data distribution. Post hoc pairwise comparisons were performed only when global significance was detected. Categorical variables were compared using the chi-square or Fisher exact test. A p-value <0.05 was considered statistically significant.
Changes over time in continuous outcomes, including BCVA, SRAST, and spherical equivalent, were evaluated using a linear panel regression model. This approach accounted for repeated measures within individuals at different time points (baseline, 1, 3, and 12 months) and allowed estimation of time-dependent effects while adjusting for intra-subject correlation. Marginal effects derived from the panel model are displayed in Figures 1 and 2, representing model-predicted means and 95% confidence intervals across time points and lens status subgroups.
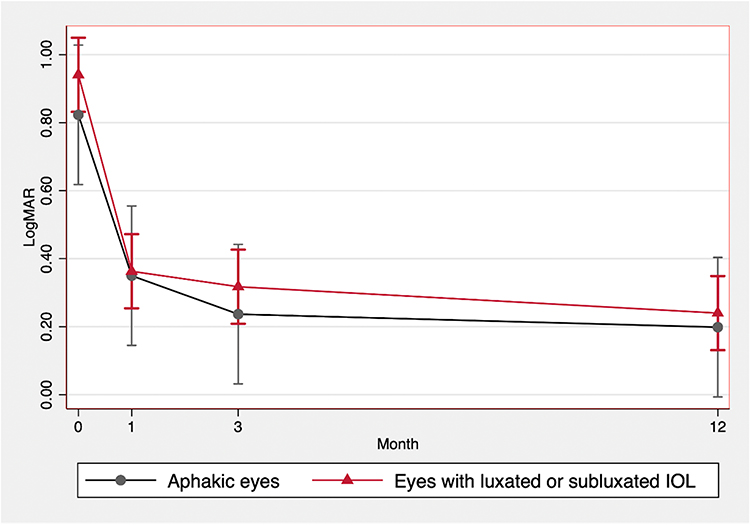 |
Figure 1 Marginal effects of time on best-corrected visual acuity (BCVA) following Yamane surgery, estimated using panel regression analysis. BCVA is reported in logMAR at baseline and at 1, 3, and 12 months of follow-up. Results are stratified by preoperative status: aphakic eyes and eyes with luxated or subluxated intraocular lens (IOL). Error bars indicate 95% confidence intervals. |
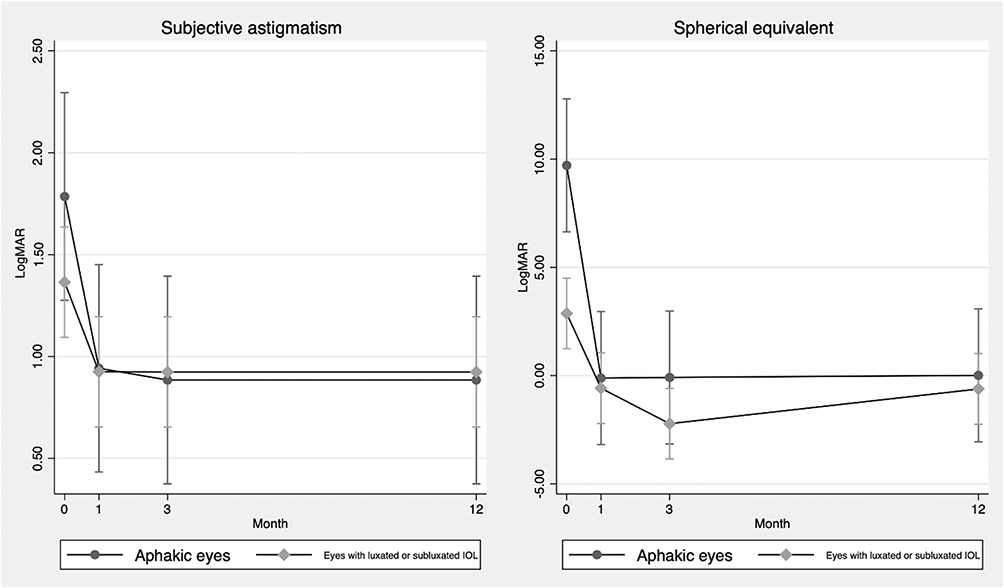 |
Figure 2 Marginal effects of time on subjective astigmatism (left panel) and spherical equivalent (right panel) following Yamane surgery, estimated using panel regression analysis. Results are stratified by preoperative status: aphakic eyes and eyes with luxated or subluxated intraocular lens (IOL). Error bars indicate 95% confidence intervals. |
Macular complications (CME and ERM) were analyzed as categorical variables. Incidence and point prevalence were reported at each predefined time point, and between-group comparisons were performed using appropriate categorical tests. Finally, a quantile regression model was used to identify preoperative factors associated with visual acuity improvement at 12 months.
Results
A total of 59 eyes from 59 patients were included. Thirteen eyes were aphakic (Group 1), 25 had subluxated IOLs (Group 2), and 21 had complete IOL dislocation (Group 3). Baseline characteristics are summarized in Table 1.
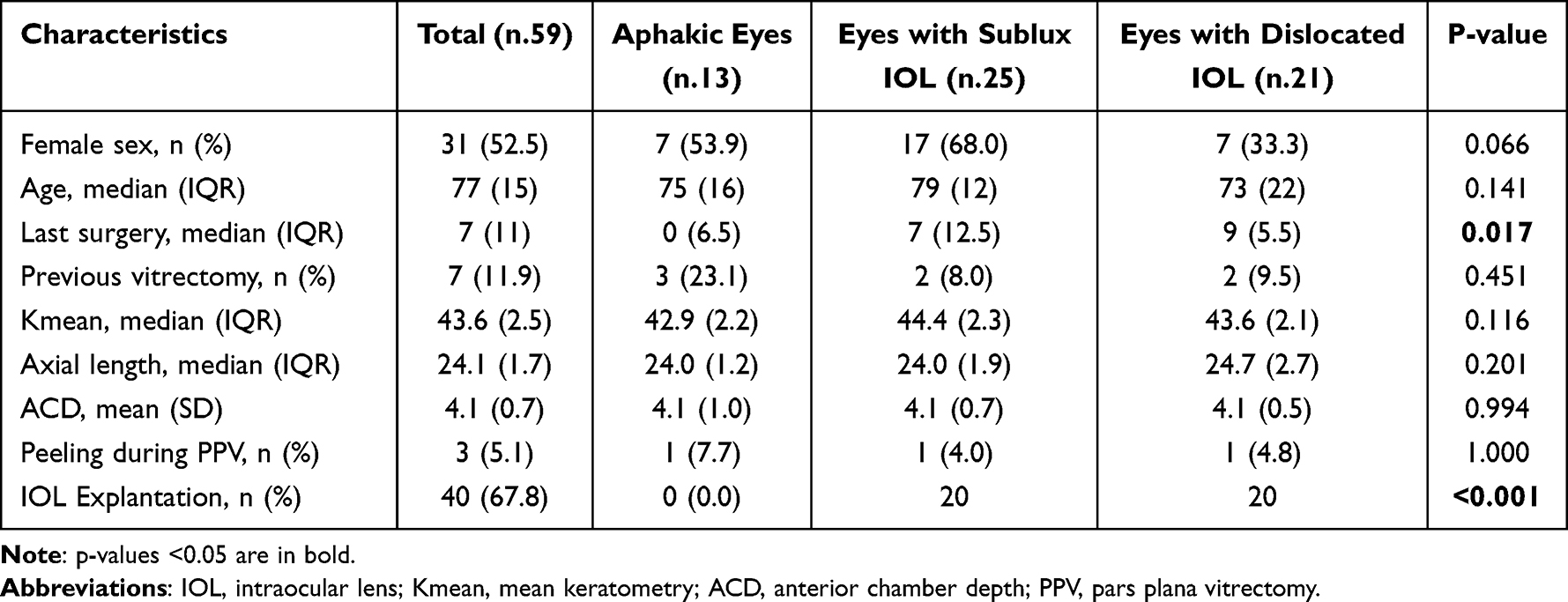 |
Table 1 Baseline Characteristics of Included Eyes Stratified by Preoperative Intraocular Lens (IOL) Status Before Yamane Surgery |
No significant differences were observed among groups in age, sex, preoperative BCVA, keratometry, axial length, anterior chamber depth, or previous vitrectomy. The time elapsed since the last intraocular surgery differed significantly, being shorter in aphakic eyes (median 0 years, IQR 6.5) compared to Group 2 (7 years, IQR 12.5) and Group 3 (9 years, IQR 5.5) (p = 0.017). IOL explantation was performed in 20 eyes in both Groups 2 and 3 (p < 0.001). Postoperative intraocular pressure remained stable or decreased, with no between-group differences.
CME prevalence varied over time. It was detected in 7 eyes (11.9%) at month 1, increased to 19 eyes (32.2%) at month 3, and decreased to 8 eyes (13.6%) at month 12 (Table 2). Three cases were present preoperatively; one resolved during follow-up, while two persisted at month 12. After excluding eyes with pre-existing CME, incident postoperative CME occurred in 6 eyes (10.2%). No significant differences in CME prevalence were found among the three groups at any time point.
 |
Table 2 Functional and Anatomical Outcomes Before and After Yamane Surgery Stratified by Preoperative Intraocular Lens (IOL) Status |
CME was more frequently observed in eyes requiring IOL explantation, accounting for 6 of 7 cases at month 1, 13 of 19 at month 3, and 6 of 8 at month 12. Most cases were mild and responded to topical nonsteroidal anti-inflammatory therapy.
The epiretinal membrane was observed in 5 eyes (8.5%) and did not require surgical treatment. The distribution of ERM cases across groups was substantially comparable (p = 0.180). Preoperatively, ERM was identified in 10 patients, all of whom underwent intraoperative macular peeling during the Yamane procedure. The 5 postoperative ERM cases occurred in eyes without pre-existing membrane at baseline.
At the 12-month follow-up, BCVA significantly improved in all groups (Table 2). Median final visual acuity was 0.2 logMAR in Groups 1 and 2, and 0.1 logMAR in Group 3 (p < 0.001). Changes over time in visual acuity are illustrated in Figure 1, showing consistent improvement across all groups.
SRAST assessed by comparing manifest refraction at baseline and 12 months, showed improvement in 24 patients, stability in 23, and worsening in 12 (Table 3). The proportion of cases with refractive worsening, stability, or improvement did not significantly differ between groups (p = 0.819). Figure 2 shows the estimated marginal effects of lens status on astigmatic and spherical outcomes over time.
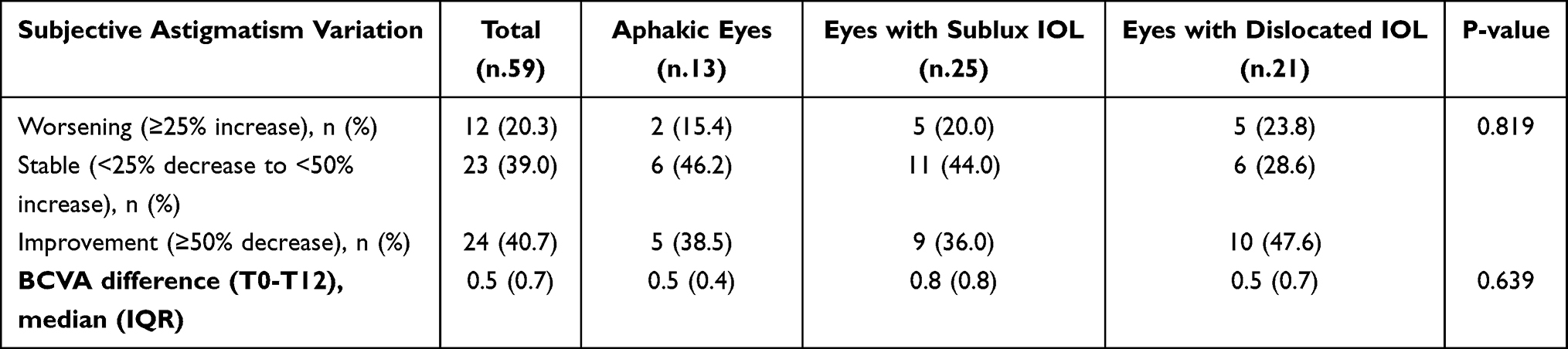 |
Table 3 Variation in Subjective Astigmatism and Best-Corrected Visual Acuity (BCVA) After Yamane Surgery Stratified by Preoperative Intraocular Lens (IOL) Status |
ECD significantly decreased at 12 months in the subluxated and dislocated IOL groups (p = 0.001 and p < 0.001, respectively), but not in the aphakic group (p = 0.220). Only two eyes experienced transient postoperative corneal edema.
Predictors of BCVA Improvement
A quantile regression model (median regression) was applied to identify preoperative predictors of visual acuity improvement at 12 months, defined as the change in logMAR BCVA from baseline. The pseudo R2 of the model was 0.5986. Independent variables included lens status (coded as subluxated/dislocated vs aphakia), baseline BCVA, age, intraocular pressure, axial length, corneal astigmatism, and endothelial cell count.
Among all predictors, only baseline BCVA was significantly associated with visual improvement (β = 0.95, p < 0.001). None of the other covariates were retained as relevant predictors: lens status (β = –0.008, p = 0.874), age (β = 0.0018, p = 0.649), intraocular pressure (β = 0.0023, p = 0.668), corneal astigmatism (β = –0.0006, p = 0.430), axial length (β = –0.0058, p = 0.745), and endothelial cell count (β = 0.0004, p = 0.660). The model intercept was –0.18 (p = 0.771).
Discussion
This study primarily evaluated macular complications following secondary IOL implantation with the Yamane technique, with specific focus on the incidence and temporal profile of CME and ERM across different preoperative lens conditions. At 12 months, CME was present in 13.6% of eyes, while the incidence of newly developed postoperative CME, after excluding pre-existing cases, was 10.2%. These values are comparable to the 13.0% rate reported at 3 months by Ishikawa et al following Yamane fixation.6 However, the temporal pattern observed in our cohort warrants clarification. CME prevalence increased to 32.2% at 3 months before declining to 13.6% at the final follow-up. Importantly, the 3-month figure represents point prevalence and includes both persistent and newly developed cases rather than cumulative incidence. This transient peak may reflect postoperative inflammatory changes and surgical manipulation, particularly in eyes requiring IOL explantation or presenting with greater vitreoretinal complexity.18 The subsequent reduction in prevalence during follow-up supports a largely self-limited or treatment-responsive course.19
Across all timepoints, CME was more frequently observed in eyes requiring IOL explantation, supporting the hypothesis that the extent of intraoperative manipulation may contribute to postoperative macular inflammation. Explantation entails additional vitreoretinal handling and, in some cases, prolonged surgical time, which may increase inflammatory stress. Comparative studies and long-term series further indicate that macular complications vary primarily according to surgical approach, case complexity, and adjunctive procedures—such as IOL explantation or retinal intervention—rather than fixation technique alone.20,21 In the series by Ishikawa et al, details regarding IOL explantation were not specified, and it is unclear whether dislocated lenses were repositioned or removed. Differences in baseline surgical approaches across studies, including the use of alternative technical variants such as posterior approaches, may partly account for variability in reported CME rates.22,23 In addition, approximately one-sixth of the eyes in our cohort underwent concurrent epiretinal membrane treatment, which may have further increased susceptibility to postoperative macular changes.24 In contrast, Ishikawa et al excluded ERM cases, potentially selecting a less complex population.6 Finally, their follow-up was limited to 3 months. In our cohort, CME prevalence peaked at 3 months and subsequently declined, indicating a dynamic course. This temporal pattern suggests that short-term follow-up may not fully characterize the evolution of postoperative macular changes after Yamane fixation.
As confirmed by the recent systematic review and meta-analysis by Nagino et al, the incidence of cystoid macular edema appears lower with the flanged intrascleral fixation technique described by Yamane compared to other sutureless scleral fixation techniques, such as the scleral tunnel and glued method.3 This is consistent with our findings, which showed a limited number of CME cases (10.2% incidence), mostly transient and predominantly observed in eyes undergoing IOL explantation. This reinforces the evidence supporting the favorable safety profile of the Yamane technique with respect to macular complications. In addition, Nagino et al hypothesized that the shorter surgical time associated with the Yamane approach may contribute to a reduced inflammatory burden, potentially explaining the lower CME rate compared to more invasive fixation methods. In a large multisurgeon real-world cohort, Redden et al reported CME as a safety endpoint after intrascleral haptic fixation, providing a broader benchmark for complication rates in this setting. Differences in cohort composition, baseline comorbidities, and the timing and definition of CME assessment may contribute to variability between studies.25
ERM developed in 5 eyes (8.5%), despite systematic intraoperative peeling in the 10 eyes where ERM was identified at baseline. This incidence is consistent with the rate reported by Sahin Vural et al (6.7%) and the isolated cases noted by Fanelli et al in complex combined procedures.7,8 Although ERM is not frequently emphasized in the Yamane literature, its development in secondary IOL cases may be influenced by surgical complexity and vitreoretinal manipulation. In our cohort, only three eyes underwent concurrent ERM peeling during PPV, and this potential confounding factor has been acknowledged in the interpretation of postoperative macular changes. ERM formation after vitreoretinal surgery has been associated with postoperative inflammatory remodeling rather than with the fixation technique itself.24,26
Postoperative BCVA improved significantly in all groups, with final values of 0.2 logMAR in aphakic and subluxated eyes, and 0.1 logMAR in dislocated IOLs. These results align with the original series by Yamane and others, who reported BCVA improvements ranging from 0.17 to 0.09 logMAR depending on the follow-up interval.1,16,27 Similar findings have been described in more recent studies: Sahin Vural et al reported a BCVA gain from 0.94 to 0.37 logMAR in a predominantly aphakic cohort, despite frequent adjunctive procedures.7 Likewise, Nagino et al reported that the flanged technique yielded the best postoperative visual outcomes among sutureless fixation methods, with a mean BCVA of 0.16 logMAR.3
The refractive profile remained stable across groups, with no significant variation in SRAST. Although prediction error was not directly assessed, these findings are in line with those reported by Schranz et al, who noted that IOL tilt has a limited effect on refractive outcomes, and with Guerin et al, who observed lower predictability in Yamane cases compared to iris-claw IOLs, particularly regarding postoperative hyperopia and refractive error.9,28
Endothelial cell loss was observed mainly in eyes undergoing IOL explantation, whereas aphakic eyes showed no significant reduction. This suggests that endothelial damage is more likely related to surgical manipulation than to the fixation method itself. This interpretation is supported by previous studies and meta-analyses showing similar ECD outcomes between sutureless and sutured scleral fixation techniques.29–32 Our findings are also consistent with previous reports of transient corneal edema in 10–20% of Yamane cases, with generally good long-term tolerance.8,33
Baseline BCVA was associated with visual improvement at 12 months. Given the limited sample size and number of events, even if lens status and other ocular variables did not show significant associations, this finding should be interpreted as an association within this cohort rather than as a definitive predictive model.
Among the limitations of this study are its retrospective design, the relatively small sample size, and the absence of a control group, which limit direct comparisons with alternative fixation techniques. The relatively low number of CME and ERM events further limits statistical power for subgroup comparisons and increases the risk of type II error; therefore, absence of significant differences should not be interpreted as evidence of equivalence between preoperative lens status groups. The 12-month follow-up does not allow assessment of delayed complications such as late IOL dislocation or long-term endothelial cell loss. The study population was heterogeneous, including eyes with different underlying etiologies such as zonular weakness, trauma, or long axial length, which were not stratified in the analysis and may have contributed to variability in anatomical and functional outcomes. In addition, concurrent procedures, including IOL explantation or ERM peeling, may represent relevant confounding factors, as surgical manipulation and inflammatory burden could independently influence the incidence and temporal profile of postoperative CME. Surgical duration was not recorded, and objective measurements of IOL position (eg, AS-OCT measurements), were not collected. Functional outcomes beyond BCVA, such as contrast sensitivity or patient-reported measures, were also not evaluated. Finally, differences in vitreous management strategies may affect postoperative inflammatory response and macular outcomes.
Conclusions
The Yamane technique provided consistent anatomical and functional outcomes across aphakia, IOL subluxation, and IOL dislocation in this selected cohort. Lens status itself was not associated with significant differences in macular complication rates or visual recovery. Although CME prevalence peaked at 3 months, the incidence of newly developed postoperative CME was limited, and most cases followed a non-progressive course. Macular changes were more frequently observed in eyes requiring IOL explantation, suggesting that surgical complexity rather than preoperative lens status may be a relevant determinant of postoperative inflammation. Visual improvement was mainly driven by baseline visual acuity. As eyes with significant pre-existing macular pathology were excluded, these findings regarding macular safety should be interpreted within a selected surgical population and may not be fully generalizable to all real-world Yamane cases. Further prospective studies with standardized surgical variables, longer follow-up, and objective optical measurements are warranted to better define long-term safety and refine patient selection.
Data Sharing Statement
The data presented in this study are available on reasonable request from the corresponding author. The data are not publicly available due to informed consent restrictions that aim to protect the privacy of research participants.
Ethics Approval
The project has been reviewed and approved by the committee of Policlinico Umberto I University Hospital (approval number 354/2020). Written informed consent was obtained from each patient.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yamane S, Sato S, Maruyama-Inoue M, et al. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmology. 2017;124(8):1136–10. doi:10.1016/J.OPHTHA.2017.03.036
2. Boz AAE, Atum M, Özmen S, et al. Comparison of three different intraocular lens implantation techniques in the absence of capsular support: sutured scleral, haptic flanged intrascleral, and four flanged intrascleral fixations. Int Ophthalmol. 2023;43(12):5045–5053. doi:10.1007/S10792-023-02907-8
3. Nagino K, Inomata T, Ohta T, et al. Postoperative complications of intrascleral intraocular lens fixation: a systematic review and meta-analysis. Surv Ophthalmol. 2025;70(3):489–498. doi:10.1016/J.SURVOPHTHAL.2024.12.001
4. Price FW, Wellemeyer M. Transscleral fixation of posterior chamber intraocular lenses. J Cataract Refract Surg. 1995;21(5):567–573. doi:10.1016/S0886-3350(13)80219-2
5. Hoffman RS, Fine IH, Packer M, et al. Scleral fixation using suture retrieval through a scleral tunnel. J Cataract Refract Surg. 2006;32(8):1259–1263. doi:10.1016/J.JCRS.2006.02.065
6. Ishikawa H, Uchida K, Terasaki H, et al. Cystoid macular oedema after flanged intraocular lens scleral fixation using the Yamane technique: a multicentre cohort study. Sci Rep. 2025;15(1). doi:10.1038/S41598-025-85370-Y
7. Sahin Vural G, Guven YZ, Karahan E, et al. Long term outcomes of Yamane technique in various indications *. Eur J Ophthalmol. 2023;33(6):2210–2216. doi:10.1177/11206721231167198
8. Faneli A, Amaral DC, Guedes J, et al. Long term outcomes of Yamane technique combined with pars plana vitrectomy in various indications: a retrospective study. Invest Ophthalmol Vis Sci. 2024;65:4020.
9. Guerin PL, Guerin GM, Pastore MR, et al. Long-term functional outcome between Yamane technique and retropupillary iris-claw technique in a large study cohort. J Cataract Refract Surg. 2024;50(6):605–610. doi:10.1097/J.JCRS.0000000000001421
10. Sun H, Wang C, Wu H. Recent advances and current challenges in suture and sutureless scleral fixation techniques for intraocular lens: a comprehensive review. Eye Vision. 2024;11(1):1–26. doi:10.1186/S40662-024-00414-0
11. Słoka A, Chorągiewicz T, Urbańska K, et al. Anatomical and functional outcomes of sutureless scleral-fixated carlevale intraocular lens implantation: a retrospective study. J Clin Med. 2025;14(20):7309. doi:10.3390/jcm14207309
12. Strathmann J, Dalbah S, Kiefer T, et al. Implantation of sutureless scleral-fixated carlevale intraocular lens (IOL) in patients with insufficient capsular bag support: a retrospective analysis of 100 cases at a single center. J Clin Med. 2025;14(12):4378. doi:10.3390/jcm14124378
13. Shelke K, Rishi E, Rishi P. Surgical outcomes and complications of sutureless needle-guided intrascleral intraocular lens fixation combined with vitrectomy. Indian J Ophthalmol. 2021;69(9):2317–2320. doi:10.4103/ijo.IJO_1636_20
14. Hauser D, Ben-David D, Masarwa D, et al. Cystoid macular edema after four-point scleral fixation of intraocular lens. Retina. 2021;41(10):2035–2040. doi:10.1097/IAE.0000000000003142
15. Bao X, Chen S, Wang Y, et al. Comparison of pacman cutting technique and trisection cutting technique for hydrophobic acrylic intraocular lens removal. Indian J Ophthalmol. 2024;72(9):1359. doi:10.4103/IJO.IJO_39_24
16. Yamane S, Inoue M, Arakawa A, et al. Sutureless 27-gauge needle-guided intrascleral intraocular lens implantation with lamellar scleral dissection. Ophthalmology. 2014;121(1):61–66. doi:10.1016/j.ophtha.2013.08.043
17. Albanese GM, Visioli G, Iannetti L, et al. Does choroidal thickness predict persistent subretinal fluid after rhegmatogenous retinal detachment repair? A retrospective study with fellow eye comparison. Acta Ophthalmol. 2023;101(4):413–421. doi:10.1111/aos.15298
18. Debellemaniere G, Rampat R, Gatinel D. Intraocular lens exchange and pars plana vitrectomy for missed refractive target and myodesopsia. JCRS Online Case Rep. 2025;13. doi:10.1097/j.jcro.0000000000000164
19. Khaksar P, John V, Mackin A, et al. Incidence of cystoid macular edema after the Yamane technique for secondary intraocular lens fixation. Invest Ophthalmol Vis Sci. 2025;66:2224.
20. Icoz M, Erkan E. Comparison of two different intraocular lenses used in the modified Yamane technique. J Cataract Refract Surg. 2025;51(9):784–789. doi:10.1097/j.jcrs.0000000000001701
21. Märker DA, Radeck V, Barth T, et al. Long-term outcome and complications of IOL-exchange. Clin Ophthalmol. 2023;17:3243–3248. doi:10.2147/OPTH.S436963
22. Iannetti L, Baratta C, Figliola F, et al. A modified Yamane technique with a posterior approach in a case report of intraocular lens dislocation. Int J Surg Case Rep. 2025;131:111369. doi:10.1016/j.ijscr.2025.111369
23. Tang Y, Yao S, Chu Y, et al. Vitreous management in Yamane’s technique for crystalline lens dislocation: anterior vitrectomy or PPV? BMC Ophthalmol. 2023;23(1):1–9. doi:10.1186/S12886-023-03204-9/FIGURES/4
24. Gharbiya M, Visioli G, Iannetti L, et al. Comparison between scleral buckling and vitrectomy in the onset of cystoid macular edema and epiretinal membrane after rhegmatogenous retinal detachment repair. Retina. 2022;42(7):1268–1276. doi:10.1097/IAE.0000000000003475
25. Redden LD, Hoang D, Rangu N, et al. Refractive, visual, and safety outcomes of three surgical techniques for aphakia correction. J Cataract Refract Surg. 2025;51(11):995–1003. doi:10.1097/j.jcrs.0000000000001723
26. Fung AT, Galvin J, Tran T. Epiretinal membrane: a review. Clin Exp Ophthalmol. 2021;49(3):289–308. doi:10.1111/CEO.13914
27. Błagun N, Krix-Jachym K, Rękas M. Comparison of safety and efficacy of four-point scleral intraocular lens fixation and the Yamane technique. Ophthalmology and Therapy. 2024;13(7):1955–1966. doi:10.1007/S40123-024-00962-7
28. Schranz M, Reumüller A, Kostolna K, et al. Refractive outcome and lens power calculation after intrascleral intraocular lens fixation: a comparison of three-piece and one-piece intrascleral fixation technique. Eye Vision. 2023;10(1). doi:10.1186/S40662-023-00341-6
29. Cui Y, Li Q, Shi X, et al. A comparative study of transscleral sutured intraocular lens fixation and sutureless flanged intraocular lens fixation. BMC Ophthalmol. 2023;23(1). doi:10.1186/S12886-023-02782-Y
30. Do JR, Park SJ, Mukai R, et al. A 1-year prospective comparative study of sutureless flanged intraocular lens fixation and conventional sutured scleral fixation in intraocular lens dislocation. Ophthalmologica. 2021;244(1):68–75. doi:10.1159/000507713
31. Kim MJ, Le Han G, Chung TY, et al. Comparison of clinical outcomes among conventional scleral fixation, retropupillary iris-claw intraocular lens implantation, and intrascleral fixation. Korean J Ophthalmol. 2022;36(5):413–422. doi:10.3341/KJO.2022.0042
32. Zhang C, Palka C, Zhu D, et al. Clinical outcomes in scleral fixation secondary intraocular lens with Yamane versus suture techniques: a systematic review and meta-analysis. J Clin Med. 2024;13(11):3071. doi:10.3390/JCM13113071
33. Yalcinbayir O, Avci R, Ucan Gunduz G, et al. Comparison of two techniques in posterior lens dislocations: scleral suture fixation vs. modified Yamane intrascleral lens fixation. J Fr Ophtalmol. 2022;45(1):13–19. doi:10.1016/J.JFO.2021.09.009
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Surgical Outcomes of Lens Removal with or Without Intraocular Lens Implantation in Marfan Syndrome: A Retrospective Cohort Study
Bin Helayel H, Magliyah MS, Alnutaifi R, Badawi AH
Clinical Ophthalmology 2025, 19:4245-4255
Published Date: 17 November 2025
Combined versus Sequential Surgery in Lamellar Macular Holes: A Multicenter Observational Study
López Arbués S, Gómez Rivera S, Tamayo Rodríguez I, Arredondo Montero J, Sellés-Navarro I, Montoliu Antón A, Bilbao-Malavé V, González-Zamora J, García-Layana A, Aliseda Pérez de Madrid D
Clinical Ophthalmology 2026, 20:593498
Published Date: 28 April 2026