Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Macrocytosis among patients with heroin use disorder
Authors Ng MH, Chen VCH, Ting H, Lin TY, Chang SH, Gossop M ![]()
Received 9 April 2019
Accepted for publication 19 July 2019
Published 12 August 2019 Volume 2019:15 Pages 2293—2298
DOI https://doi.org/10.2147/NDT.S211649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Mei-Hing Ng,1,2 Vincent Chin-Hung Chen,3,4 Hua Ting,1,5 Tsang-Yaw Lin,2 Sheng-Huang Chang,2 Michael Gossop6
1Institute of Medicine, Chung Shan Medical University, Taichung, Taiwan; 2Tsaotun Psychiatric Center, Ministry of Health and Welfare, Nan-Tou County, Taiwan; 3Department of Psychiatry, Chang Gung Medical Foundation, Chiayi Chang Gung Memorial Hospital, Chiayi County, Taiwan; 4Department of Psychiatry, School of Medicine, Chang Gung University, Taoyuan City, Taiwan; 5Department of Physical Medicine and Rehabilitation, Chung-Shan Medical, University Hospital, Chung-Shan Medical University, Taichung, Taiwan; 6National Addiction Center, Institute of Psychiatry, King’s College London, London, UK
Purpose: Few empirical studies have investigated hematological parameters among people with a heroin use disorder. This study explores the prevalence of macrocytosis and associated factors among patients with heroin use disorder who were entering methadone maintenance treatment (MMT) in Taiwan.
Patients and methods: In this cross-sectional study, hematological parameters were measured and the prevalence of macrocytosis was assessed in a sample of 958 patients with a heroin use disorder entering the MMT program at Tsaotun Psychiatric Center in Taiwan. The demographic characteristics, heroin-related issues, other substance use history, and other clinical variables were analyzed. Univariate analysis was used to assess the association of all variables. Multivariable logistic regression was used to identify the relationship between the significant factors and macrocytosis.
Results: The study found that nearly one-fifth (19.5%) of the participants had macrocytosis. Older age, longer duration of heroin use, and more days of alcohol use within the previous month were associated with macrocytosis.
Conclusion: We found that concurrent use of alcohol was an important factor related to macrocytosis among people with a heroin use disorder. The prevalence of macrocytosis indicated that alcohol use is common among this population. It is suggested that policies and practices regarding alcohol use should be addressed within methadone maintenance programs.
Keywords: addiction, opioid dependence, substitution treatment, megalocytes
Introduction
Globally, it is estimated that 13.5 million people take opioids, including 9.2 million who use heroin.1 The World Health Organization estimated that 0.7% of the global burden of disease in 2004 was due to opioid and cocaine use, with the social cost of illicit substance use being in the region of 2% of the GDP in those countries which have measured it.2 About 30% of the countries reported the availability of opioid agonist pharmacotherapy for the maintenance treatment of opioid dependence in 2008.3 In Taiwan, methadone maintenance therapy (MMT) was commenced in 2006. Hematological parameters of patients with heroin use disorder were investigated while the subject was attending the MMT program in Taiwan. Enlarged erythrocytes were noticed clinically in this population. However, very few previous studies4–6 focus on the macrocytosis of the heroin users, which is important because of possible cardiac and hemodynamic complications may be of significance for clinical practice.5
Macrocytosis is the condition of having erythrocytes which (on average) are too large. This has usually been defined as the mean corpuscular volume (MCV), a measure of the average volume of a red blood corpuscle, greater than 95 to 100 femtoliters (fL). In the general population, prevalence estimates range from 1.7% to 3.6%.5 An independent association has been found between macrocytosis and the metabolic syndrome7 and suggested that MCV might be a metabolic marker. Studies of alcohol abusers have reported similar hematological findings and this has been defined as “alcoholic macrocytosis”.8,9 Excessive ethanol consumption may affect the peripheral blood cells and bone marrow. Poor nutrition intake of alcohol abusers causes vitamin B12 and folate deficiency, and this may lead to secondary megaloblastosis.10
In a previous study,5 the term “heroin macrocytosis” (heroin macrocytic anemia) was established and linked to the increased red blood cell distribution width (RDW) in chronic heroin abusers. Another study6 reported that the mu opioid receptors of erythrocytes and the rheological parameters were changed among opioid-dependent patients. However, the findings of the studies were limited by small sample sizes. The appearance of heroin macrocytosis has not been well documented. No other research studies have investigated the association between heroin use and macrocytosis.
The present study investigates changes in the hematological properties of erythrocytes (ie, macrocytosis) among patients with heroin use disorder receiving methadone maintenance therapy and also identifies associated factors. The study hypothesized that macrocytosis would be present among the population with heroin use disorder and that it would be correlated with heroin use.
Materials and methods
Participants and procedures
The sample comprised 958 heroin-dependent patients. They were recruited from an MMT program at the Tsaotun Psychiatric Center in central Taiwan, between January 2007 and October 2013. All subjects had the diagnostic interview with a senior psychiatrist and the heroin dependence diagnosis was confirmed according to DSM-IV-TR. Those individuals who were illiterate or had the diagnosis of intellectual disability were excluded. At admission to the MMT program, all participants completed self-report questionnaires with the assistance of a trained psychiatric nurse, which were designed to assess demographic data, medical history, psychosocial information, criminal history, and substances use history.
Measures
We assessed the heroin-related behaviors of the participants at the beginning of the MMT program. Information included the onset age of heroin use, multiple substance use (including amphetamine, club drugs, alcohol, marijuana use, but not including tobacco use) and any alcohol use in the last 6 months, any infection of hepatitis B (HBV) or C virus (HCV), and human immunodeficiency virus. We assessed the frequency and quantity of heroin used per day in the last 30 days before the subject entered the program to determine the amount of heroin used. In Taiwan, a traditional measuring unit usually relates to the weight of heroin: half Qian. One Qian is approximately equal to 3.75 g and half Qian is about 1.875 g. The dosage of heroin used per day then was calculated by dividing the total amount used by number of days. The participants’ blood samples were taken at their entry to the MMT program and tests were carried out at the Division of Laboratory Medicine in Tsaotun Psychiatric Center, using Beckman Coulter Hematology Analyzer LH 750. The hematological parameters were red blood cell count (RBC), hemoglobin (Hb), hematocrit (Hct), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), white blood cell count (WBC), and platelet count. We also measured the liver function by using glutamate oxaloacetate transaminase (GOT) and glutamate pyruvate transaminase (GPT). The definition of macrocytosis, MCV>95 fL was used.11
Data analyses
The study carried out a descriptive analysis for the demographic characteristics, heroin-related issues, substance use history, and other clinical variables. We used means, standard deviations, and proportions to present the data when relevant. The association of all variables was assessed by an independent t-test and Chi-square test. We entered all significant factors into a multivariable logistic regression analysis model to determine their association with heroin use and macrocytosis. Adjustment was made for the potential effects of other variables, including age, sex, alcohol use, multiple substance use, and hypothyroidism. We conducted the analyses by using SPSS 15.0 for Windows and the differences were considered significant if p<0.05.
Ethics
The study was reviewed and approved by the Institutional Review Board of the Tsaotun Psychiatric Center and was conducted in accordance with the Declaration of Helsinki. All individuals provided written informed consent before participation. They were informed of their right to discontinue participation at any time and legal prosecution will not result from participation in the study. Their treatment rights will not be influenced and assurance of confidentiality.
Results
Demographic data of participants
The demographic data of the participants (n=958) are shown in Table 1. Their mean age was 36.58±7.69 years. The mean duration of heroin use was 10.65±5.89 years. The majority were male (n=873, 91.1%). About half of our participants (n=467, 48.7%) were multiple substance users, and a quarter (n=248, 25.9%) were using alcohol. As high as 90% of them were infected by HCV. Most of them had the hematological parameters, thyroxin, and GPT level within normal range. Among all of our participants, nearly one-fifth (n=187, 19.5%) had MCV greater than 95 fL, ie, macrocytosis.
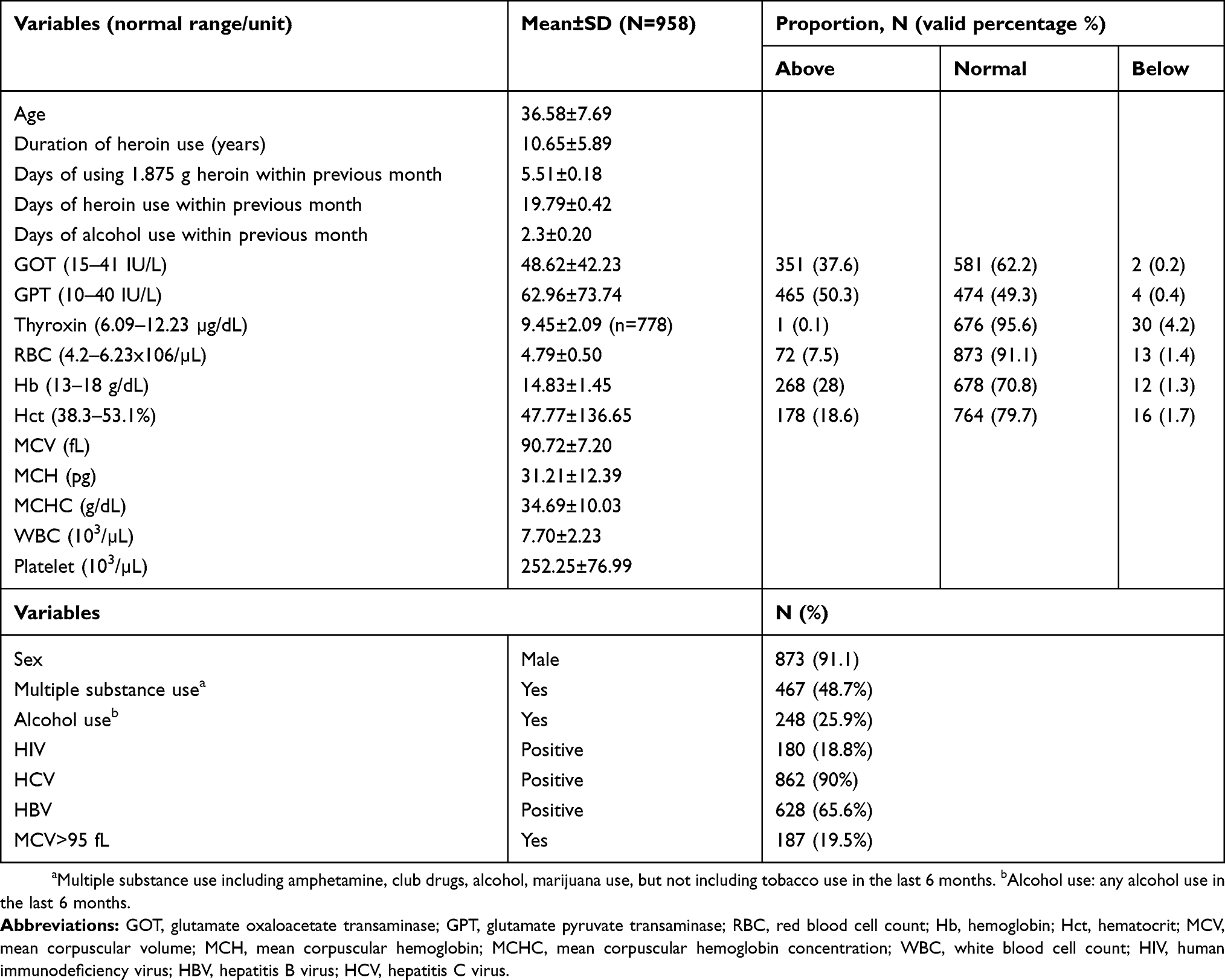 |
Table 1 Demographic characteristics of the sample |
Macrocytosis and associated factors
In univariate analysis (Table 2), age (p<0.0001), duration of heroin use (p=0.003), and more days of alcohol use within the previous month (p<0.0001) were found to be associated with macrocytosis. Of those with macrocytosis, 97.3% were male (p=0.001) and 38% of them were current alcohol users (p<0.0001) compared to 89.6% male and 23% current alcohol users among those without macrocytosis. No statistically significant difference was found between these two groups of individuals with regard to multiple substance use, HIV, and HCV infection.
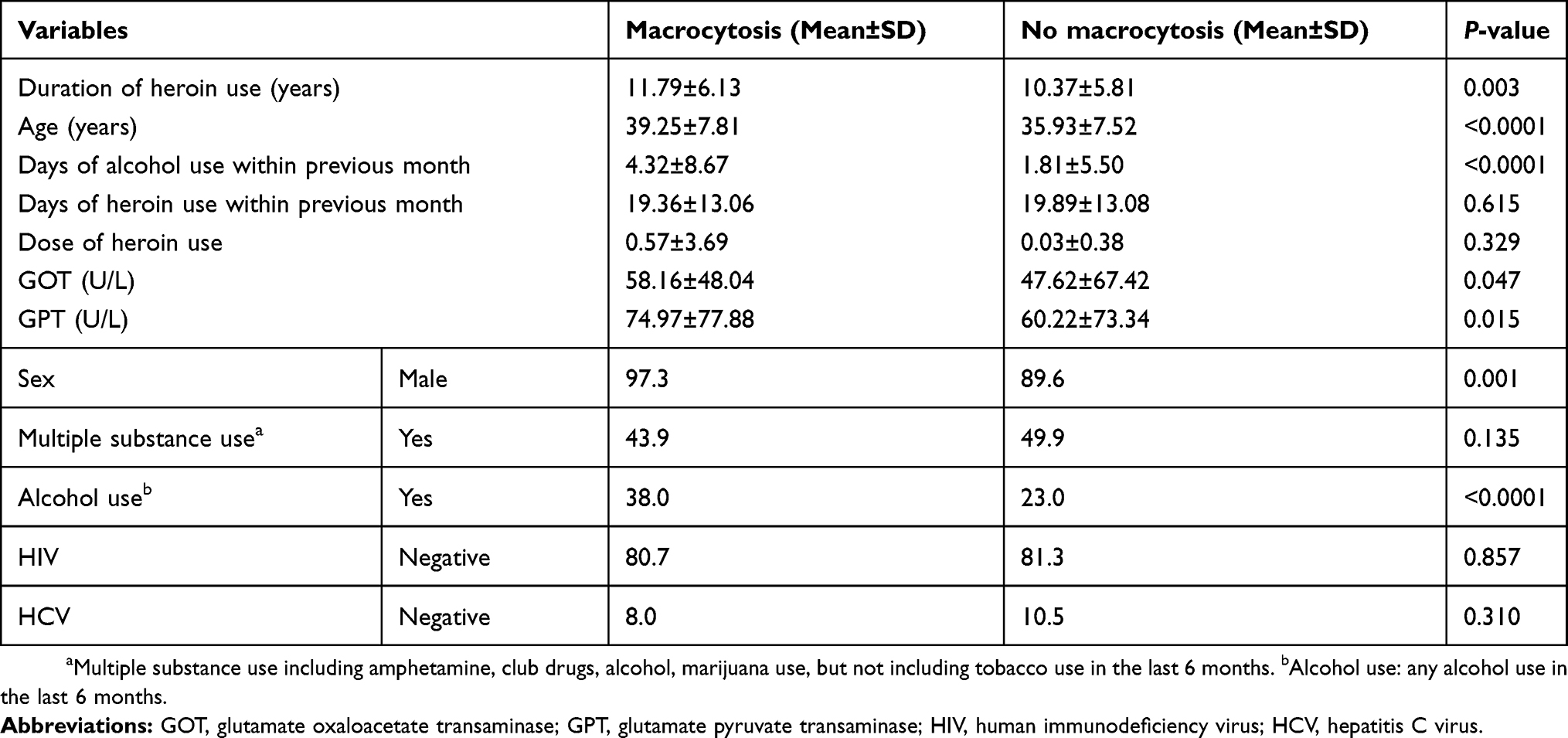 |
Table 2 The difference between the macrocytosis group and without macrocytosis among MMT patients |
Multivariable logistic regression analysis was performed to identify the variables significantly associated with macrocytosis after adjustment (Table 3). Independent associations were found for male gender (AOR 4.21; 95% CI, 1.30–13.70), age (AOR 1.05; 95% CI, 1.03–1.08), and more days of alcohol use within the previous month (AOR 1.03; 95% CI, 1.00–1.06). Duration of heroin use and liver function was not significantly associated with macrocytosis.
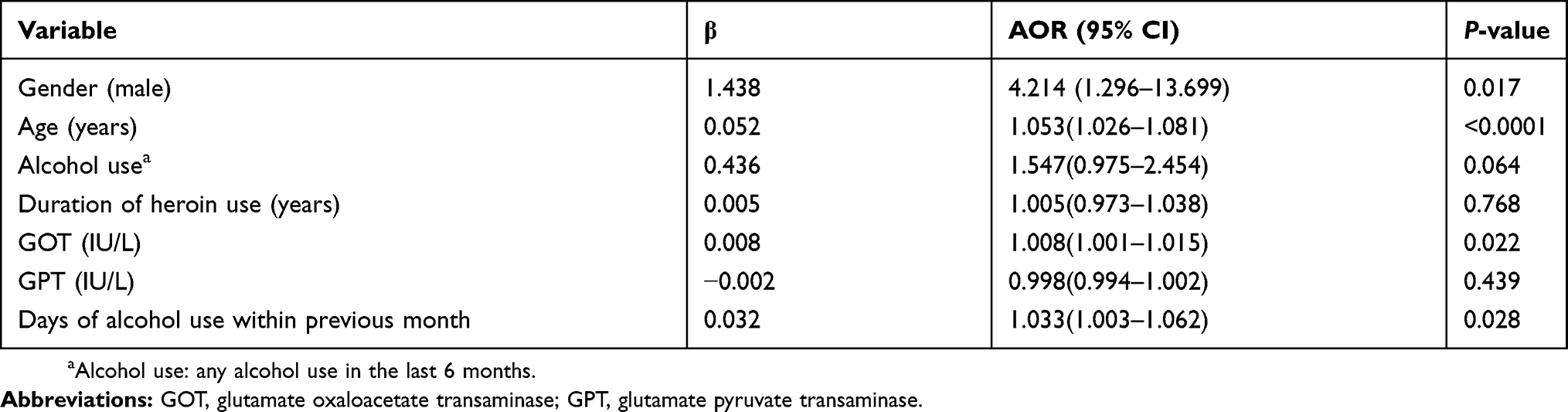 |
Table 3 Factors associated with macrocytosis. (Multivariable logistic regression analysis) |
Discussion
Prevalence of macrocytosis
This is the first study that focuses on the association between heroin use and macrocytosis. Nearly one-fifth of dependent heroin users in our sample had macrocytosis. About half of them were multiple substance users and a quarter were using alcohol. Older age, longer duration of heroin use, and more days of alcohol use within the previous month were associated with macrocytosis. The factors that were found to be independently associated with macrocytosis among the participants were male gender, older age, and more days of alcohol use in the previous month.
No previous data were available regarding the prevalence of macrocytosis in this population. The present study found that 19.5% of the participants had macrocytosis, which is 5 to 10 times higher than that of the general population.10 This is close to the prevalence of macrocytosis among alcohol abusers (26%).12 With regard to the hematology, one possible reason for the macrocytosis among heroin users might be because the erythrocytes from the chronic opioid users have high opioid receptor levels and have high deformability.6 Many of the patients who enrolled in the MMT program have lifestyle problems with eating too little, smoking, and drinking too much.13
Comorbidity of alcohol
In the present study, 25.9% of the participants were still consuming alcohol and 38% of the drinkers had macrocytosis at admission to the MMT program. The comorbidity of heroin use disorder and alcohol use was high. A previous systematic review found that alcohol consumption often does not change when patients are on MMT.14 In the UK National Treatment Outcome Research Study (NTORS), Gossop et al15 found that heavy drinking was relatively common among the heroin users. Approximately a quarter of the NTORS sample was drinking heavily at treatment intake, and the same proportion continued to drink heavily throughout the 5-year follow-up. Among the drug misusers who have drinking problem, their typical daily amounts of alcohol were between 10 and 19 units.16 This suggests that greater attention should be paid to the problem of alcohol use among the heroin users from both the perspectives of treatment and of preventive medicine. The finding of macrocytosis may remind us to look more closely at the underlying problematic alcohol use of patients and to provide them a more precisely tailored intervention in MMT programs. Interventions to tackle alcohol use, and especially excessive drinking should be established within MMT programs. Examples might include providing additional health education on alcohol to the MMT patients with problematic alcohol use and asking them to have an alcohol breath test before they receive their daily methadone dose in order to reduce problematic alcohol use and further harmful effects from alcohol.
Association of the heroin use factors and macrocytosis
The factors that were found to be related to macrocytosis among the heroin use disorder population included male gender, age, and more days of alcohol use within the previous month. There was considerable variation in the duration of heroin use among the heroin use disorder individuals with macrocytosis. Our results do not support the hypothesis of “heroin macrocytosis” that was proposed. However, the findings do indicate that alcohol macrocytosis is an important feature of this population.
Macrocytosis was associated with older age. This is consistent with the findings of previous studies that showed macrocytosis to be more common in older adults,17,18 with prevalence figures for macrocytosis reported at 8.4% for the adults aged ≥45. Our finding that men were more likely to have macrocytosis is also consistent with other studies of older adults.18 This might be explained by poor nutritional intake or increased losses of vitamin B12 in the elderly.19 Deficiency of vitamin B12 increases with age.20 However, no previous research data were available regarding age and macrocytosis among the population of heroin use disorder.
Most (90%) of the participants had hepatitis C viral infection. This was consistent with previous findings.21 Hepatitis B virus and hepatitis C virus may induce severe bone marrow aplasia. Chronic liver diseases including viral hepatitis cause portal hypertension and splenomegaly, and may lead to secondary hemolysis and macrocytosis.22 In addition, the treatment of chronic hepatitis C with a combination of interferon and ribavirin may also cause macrocytosis.23 Despite the high HCV infection prevalence among our participants, there was no significant difference between the groups with and without macrocytosis (p=0.31).
Limitations
The current study has some limitations. Reporting bias exists, and in particular, the dose or duration of heroin, multiple substance use, and alcohol use might be under-reported. Also, the samples were not randomly selected but were enrolled from a single psychiatric center in central Taiwan. Accordingly, the findings may not generalize to different settings. The heroin use disorder patients included in the study may be a highly selected group. They may have greater severity of dependence and differ from the broader range of the heroin use population. These samples may not represent all heroin users in the country, even though we have large community-based samples. Our study did not include information on red cell distribution width (RDW), nutritional status, serum level of folic acid and thiamine, the amount of drinking, and the status of HCV treatment which might have given us more information. Further research using a cohort design and which collects the details of nutrient profile and alcohol use among the patients with heroin use disorder may help to differentiate the megaloblastic effect of heroin from that of alcohol. On the other hand, the study does have certain strengths, not least because of its inclusion of a relatively large sample.
Conclusion
We found that nearly one-fifth of the patients with heroin use disorder had macrocytosis, and a quarter were also using alcohol. Macrocytosis among the patients with heroin use disorder was independently associated with male gender, older age, and more days of alcohol use in the previous month. Our study suggested that greater attention should be paid to the issue of alcohol use and related macrocytosis problems among the patients with heroin use disorder.
Acknowledgment
We acknowledge Professor Michael Gossop for English language editing and review.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Management of Substance Abuse: opiates: facts and Figures; 2011. Available from: https://www.who.int/substance_abuse/facts/en/.
2. World Health Organization. The Global Burden of Disease: 2004 Update; 2008. Available from: http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/.
3. World Health Organization. Opioid Agonist Pharmacotherapy for the Maintenance Treatment of Opioid Dependence; 2012. Available from: http://www.who.int/gho/substance_abuse/treatment/pharmacotherapy/en/.
4. Galante A, De Luca A, Pietroiusti A, et al. Effects of opiates on blood rheology. J Toxicol Clin Toxicol. 1994;32:411–417.
5. Savov Y, Antonova N, Zvetkova E, Gluhcheva Y, Ivanov I, Sainova I. Whole blood viscosity and erythrocyte hematometric indices in chronic heroin addicts. Clin Hemorheol Microcirc. 2006;35:129–133.
6. Zeiger AR, Patkar AA, Fitzgerald R, Lundy A, Ballas SK, Weinstein SP. Changes in mu opioid receptors and rheological properties of erythrocytes among opioid abusers. Addict Biol. 2002;7:207–217. doi:10.1080/135562102200120433
7. Harrington JM, Buckley CM, O’Shea S, Perry IJ, Cahill MR. Macrocytosis: a metabolic marker? Blood. 2013;122:4663. doi:10.1182/blood-2012-12-471029
8. Seppa K, Sillanaukee P, Saarni M. Blood count and hematologic morphology in nonanemic macrocytosis: differences between alcohol abuse and pernicious anemia. Alcohol. 1993;10:343–347. doi:10.1016/0741-8329(93)90018-J
9. Niemela O, Parkkila S. Alcoholic macrocytosis – is there a role for acetalaldehyde and adducts? Addict Biol. 2004;9:3–10. doi:10.1080/13556210410001674031
10. Aslinia F, Mazza JJ, Yale SH. Megaloblastic anemia and other causes of macrocytosis. Clin Med Res. 2006;4:236–241.
11. Ebdon C, Batty P, Smith G. Haematopoiesis and red blood cells. Surgery (Oxford). 2013;31:200–205. doi:10.1016/j.mpsur.2013.02.005
12. Kaferle J, Strzoda CE. Evaluation of macrocytosis. Am Fam Physician. 2009;79:203–208.
13. Best D, Lehmann P, Gossop M, Harris J, Noble A, Strang J. Eating too little, smoking and drinking too much: wider lifestyle problems among methadone maintenance patients. Addict Res. 1998;6:489–498. doi:10.3109/16066359809004367
14. Srivastava A, Kahan M, Ross S. The effect of methadone maintenance treatment on alcohol consumption: a systematic review. J Subst Abuse Treat. 2008;34:215–223. doi:10.1016/j.jsat.2007.04.001
15. Gossop M, Browne N, Stewart D, Marsden J. Alcohol use outcomes and heavy drinking at 4–5 years among a treatment sample of drug misusers. J Subst Abuse Treat. 2003;25:135–143. doi:10.1016/S0740-5472(03)00129-6
16. Gossop M, Marsden J, Stewart D, Rolfe A. Patterns of drinking and drinking outcomes among drug misusers: one year follow-up results. J Subst Abuse Treat. 2000;19:45–50. doi:10.1016/S0740-5472(99)00097-5
17. Mahmoud MY, Lugon M, Anderson CC. Unexplained macrocytosis in elderly patients. Age Ageing. 1996;25(4):310–312. doi:10.1093/ageing/25.4.310
18. McNamee T, Hyland T, Harrington J, et al. Haematinic deficiency and macrocytosis in middle-aged and older adults. PLoS One. 2013;8(11):e77743. doi:10.1371/journal.pone.0077743
19. Wahlin A, Bäckman L, Hultdin J, Adolfsson R, Nilsson LG. Reference values for serum levels of vitamin B12 and folic acid in a population-based sample of adults between 35 and 80 years of age. Public Health Nutr. 2002;5:505–511. doi:10.1079/PHNPHN200167
20. Hin H, Clarke R, Sherliker P, et al. Clinical relevance of low serum vitamin B12 concentrations in older people: the banbury B12 study. Age Ageing. 2006;35:416–422. doi:10.1093/ageing/afl033
21. Ng MH, Chou JY, Chang TJ, et al. High prevalence but low awareness of hepatitis C virus infection among heroin users who received methadone maintenance therapy in Taiwan. Addict Behav. 2013;38:2089–2093. doi:10.1016/j.addbeh.2013.01.010
22. Gonzalez-Casas R, Jones EA, Moreno-Otero R. Spectrum of anemia associated with chronic liver disease. World J Gastroenterol. 2009;15:4653. doi:10.3748/wjg.15.919
23. Bugdaci MS, Sokmen M, Toptas T. Additive effect of folic acid deficiency on pegylated interferon’s bone marrow toxicity. Eur J Gastroenterol Hepatol. 2011;23:1079–1080. doi:10.1097/MEG.0b013e32834be999
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.