Back to Journals » Infection and Drug Resistance » Volume 19
Lymphocyte-Predominant Ascites as a Clue to Peritoneal Tuberculosis: Two Case Reports and a Literature Review
Authors Sun W, Lai K ![]() , Huang C, Ye Y, Chen Y, Xu S
, Huang C, Ye Y, Chen Y, Xu S
Received 9 March 2026
Accepted for publication 4 June 2026
Published 8 June 2026 Volume 2026:19 606594
DOI https://doi.org/10.2147/IDR.S606594
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Wan Sun,1,* Keyuan Lai,2,* Chunxia Huang,2 Yuanyang Ye,2 Yuan Chen,2 Shaoqiang Xu2
1Department of Respiratory Medicine, General Hospital of Southern Theater Command, Guangzhou, People’s Republic of China; 2Department of Clinical Laboratory, Guangdong Sanjiu Brain Hospital, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shaoqiang Xu, Email [email protected]
Background: Peritoneal tuberculosis (PTB) is difficult to diagnose because its clinical and imaging features are nonspecific and may mimic peritoneal malignancy or other intra-abdominal diseases. In addition, microbiological and molecular tests of ascitic fluid may be negative in paucibacillary disease.
Case Presentation: We report two patients with PTB whose initial diagnostic evaluation was inconclusive. Both presented with abdominal distension and imaging findings suspicious for alternative diagnoses. In Case 1, acid-fast bacilli (AFB) staining and Mycobacterium tuberculosis (M. tuberculosis) nucleic acid amplification test (NAAT) of ascitic fluid were negative; targeted next-generation sequencing (tNGS) was not performed. Ascitic fluid cytology showed a nucleated cell count of 7900 × 106/L, with 76% lymphocytes, mesothelial cells less than 1%, and no malignant cells. The patient improved after empiric treatment, and the diagnosis was later confirmed by positive ascitic fluid culture for M. tuberculosis. In Case 2, AFB staining and tNGS performed on pleural and ascitic fluid samples did not detect M. tuberculosis or other pathogens. Ascitic fluid cytology showed a nucleated cell count of 6,726 × 106/L, with 82% lymphocytes, mesothelial cells less than 1%, and no atypical cells. PTB was ultimately confirmed by laparoscopic biopsy with histopathology and positive tissue AFB staining.
Conclusion: In the appropriate clinical setting, lymphocyte-predominant ascitic fluid with a low mesothelial cell proportion may provide a useful supportive clue to PTB when initial tests are negative or nondiagnostic. However, these cytological findings are nonspecific and should be interpreted together with clinical, microbiological, and histopathological findings.
Keywords: peritoneal tuberculosis, ascites, cytology, lymphocyte predominance, mesothelial cells
Introduction
Peritoneal tuberculosis (PTB) is an important form of abdominal and extrapulmonary tuberculosis, but its diagnosis remains challenging because the clinical presentation and imaging findings are often nonspecific and may overlap with peritoneal carcinomatosis, cirrhotic ascites, bacterial peritonitis, and inflammatory bowel disease.1–5 The burden of PTB may be greater in patients with cirrhosis, diabetes, chronic kidney disease, those receiving peritoneal dialysis, or those living with HIV.6–9 Delayed recognition of PTB may worsen outcomes and complicate subsequent diagnostic and therapeutic decision-making,2 as well as result in unnecessary empiric treatment, which is relevant to antimicrobial stewardship.
Microbiological confirmation of PTB from ascitic fluid is often difficult because these specimens are typically paucibacillary. Acid-fast bacilli (AFB) staining has low sensitivity, and NAAT may also yield negative results in this setting.10,11 Although targeted next-generation sequencing (tNGS) has expanded diagnostic options in infectious diseases and tuberculosis, its performance in low-burden serous specimens remains variable, and ascites-specific data are still limited, with some available evidence derived from pleural rather than peritoneal effusions.12,13 Therefore, a negative molecular result should not be considered sufficient to exclude PTB. In such situations, routine ascitic fluid cytology, while nonspecific, may still serve as a practical and accessible supportive clue to prompt further tuberculosis-directed evaluation rather than replace microbiological or histopathological confirmation.
Routine ascitic fluid examination remains widely available and inexpensive. In tuberculous serositis, the host immune response may be reflected by lymphocyte-predominant ascitic fluid with few mesothelial cells.14–18 However, lymphocyte-rich ascites may also be seen in lymphoma, peritoneal carcinomatosis, and some chronic inflammatory or fungal conditions; therefore, these cytological findings should be interpreted cautiously in the full clinical context rather than in isolation. In this report, we describe two cases of PTB in which initial diagnostic testing was inconclusive, whereas ascitic fluid cytology raised suspicion for tuberculous serositis and supported further diagnostic evaluation. These cases suggest that conventional cytology may still have value as a practical supportive clue when PTB is under consideration.
Case 1
A 38-year-old man presented with a several-month history of unexplained abdominal distension. Physical examination showed mild abdominal distension and shifting dullness, suggesting a small volume of intra-abdominal ascites. The remainder of the abdominal and systemic examination was unremarkable. He had no fever, night sweats, cough, or sputum production.
Laboratory testing showed elevated inflammatory markers, including a C-reactive protein level of 53.7 mg/L and a serum amyloid A level of 113.2 mg/L. Tumor markers were within normal limits except for a mildly elevated Cancer antigen 125 (CA-125) level of 36.2 U/mL. Abdominal computed tomography (CT) showed thickening of the greater omentum, extensive thickening in areas of peritoneal adhesion and along the omental surface, superficial nodular changes, a small amount of pelvic fluid, and localized peritoneal thickening, suggesting peritoneal inflammation. Acute appendicitis with regional reactive lymphadenopathy was also considered on imaging (Figure 1).
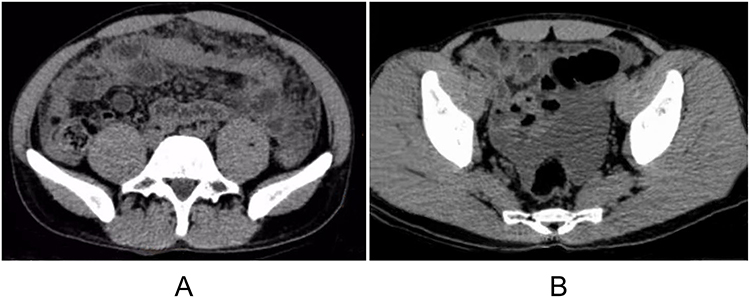 |
Figure 1 Thoracoabdominal radiological features. (A) Thickening of the greater omentum. (B) Fluid accumulation within the pelvic cavity. |
Diagnostic paracentesis yielded yellow, turbid ascitic fluid. Ascitic fluid analysis showed a markedly elevated adenosine deaminase (ADA) level of 91 U/L. AFB staining and Mycobacterium tuberculosis (M. tuberculosis) NAAT were negative (Figure 2). NAAT was performed as the initial rapid and more affordable molecular test, whereas NGS was not pursued because of financial constraints. Cytological examination showed a nucleated cell count of 7,900 ×106/L, with lymphocytes accounting for 76% of nucleated cells, mesothelial cells accounting for less than 1%, and no malignant cells. Although nonspecific, these findings supported consideration of PTB in the appropriate clinical context.
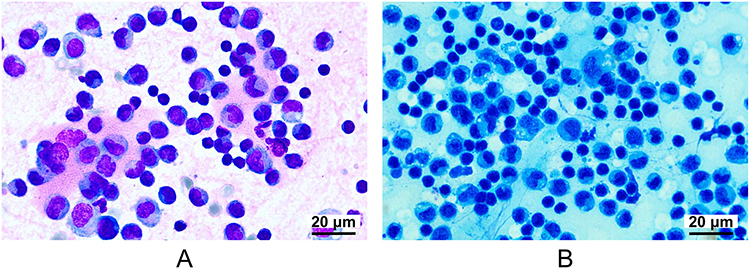 |
Figure 2 Cytological smear of the ascitic fluid. (A) The Wright-Giemsa stain shows abundant mature lymphocytes diffusely distributed across the field. These cells are characterized by scant cytoplasm and dense nuclei, with a notable absence of malignant cells and neutrophils (original magnification ×100). (B) The AFB stain reveals a blue microscopic background with no red-stained AFB identified (original magnification ×100). |
Based on the overall clinical findings, empiric treatment was initiated with isoniazid (0.3 g once daily), rifampicin (0.45 g once daily), pyrazinamide (1.5 g once daily), and ethambutol (0.75 g once daily). Symptomatic treatment included spironolactone, furosemide, and intermittent therapeutic paracentesis. After 2 weeks, the patient’s abdominal distension improved, and follow-up ultrasonography showed a marked reduction in ascites. After 5 weeks, ascitic fluid culture grew M. tuberculosis, confirming the diagnosis of PTB.
Case 2
A 61-year-old man presented with 3 weeks of progressive abdominal distension, accompanied by anorexia, exertional dyspnea, and an unintentional weight loss of approximately 5 kg. Physical examination showed abdominal distension with shifting dullness and decreased breath sounds bilaterally. External CT and positron emission tomography demonstrated massive bilateral pleural effusions, marked abdominopelvic fluid accumulation, and extensive heterogeneous thickening of the hepatic capsule, peritoneum, and greater omentum with increased metabolic activity. Based on the clinical and imaging findings, malignant ascites was initially considered, although PTB remained in the differential diagnosis.
Further investigations were inconclusive. Ascitic fluid CA-125 was mildly elevated at 114.71 U/mL, whereas the remaining tumor markers were within normal limits. The T-SPOT.TB assay was positive, but the overall diagnostic picture remained discordant. Ascitic fluid ADA was low at 5 U/L. In addition, AFB staining was negative, and tNGS did not detect M. tuberculosis or other pathogens in the serous fluid samples. These discordant findings complicated the initial diagnostic evaluation (Table 1).
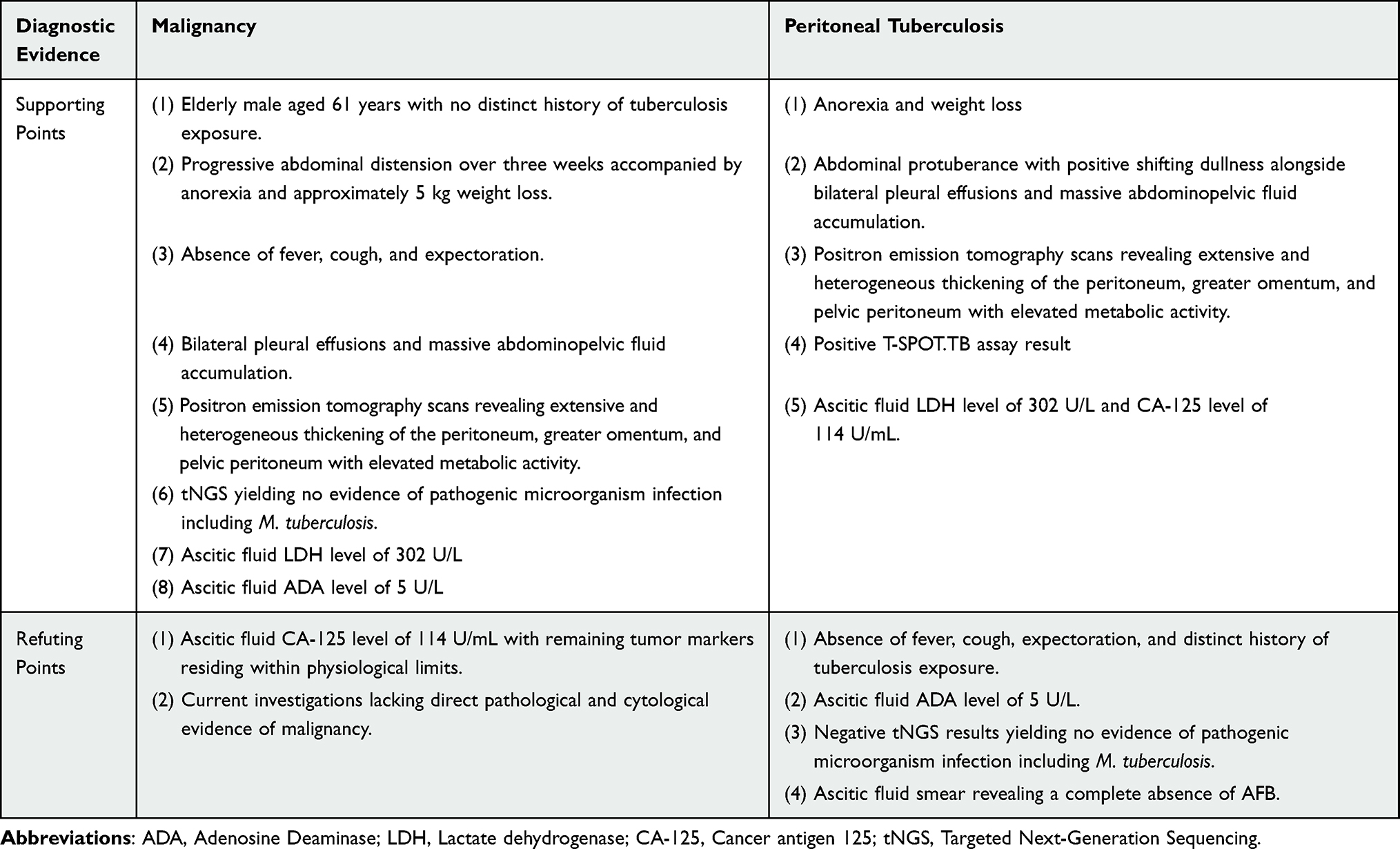 |
Table 1 Summary of Clinical Evidence for the Differential Diagnoses of Case 2 |
Cytological examination of the ascitic fluid showed a nucleated cell count of 6,726 ×106/L, with lymphocytes accounting for 82% of nucleated cells, mesothelial cells less than 1%, and no atypical or malignant cells. Pleural fluid cytology showed a similar inflammatory pattern, with lymphocyte predominance (70%) and mesothelial cells accounting for 8% (Figure 3). Although nonspecific, these findings supported consideration of PTB in the clinical context and made peritoneal malignancy less likely.
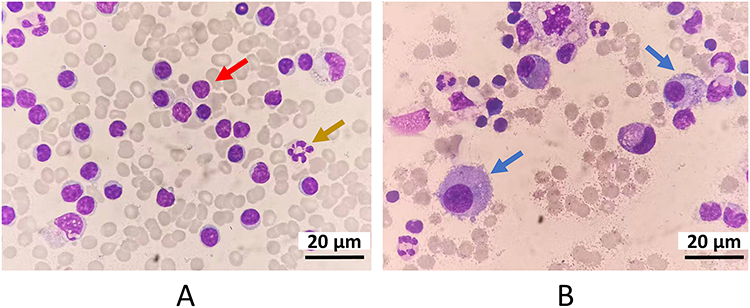 |
Figure 3 Cytomorphological features of the pleural and ascitic fluids. (A) Red arrows identify lymphocytes and green arrows highlight neutrophils. The image utilizes a Wright-Giemsa stain at an original magnification of ×100. (B) Pleural fluid cytology shows 70% lymphocytes and 8% mesothelial cells. Blue arrows specifically denote mesothelial cells. The image utilizes a Wright-Giemsa stain at an original magnification of ×100. |
Because the diagnosis remained uncertain, exploratory laparoscopy was performed. Intraoperatively, the intestines and greater omentum were densely studded with small gray-white nodules (Figure 4A). Histopathological examination of the peritoneal biopsy showed collagenized fibrous connective tissue with marked inflammatory cell infiltration and multifocal necrosis, without neoplastic cells (Figure 4B). Tissue AFB staining was positive (Figure 4C and D), and the diagnosis of PTB was established.
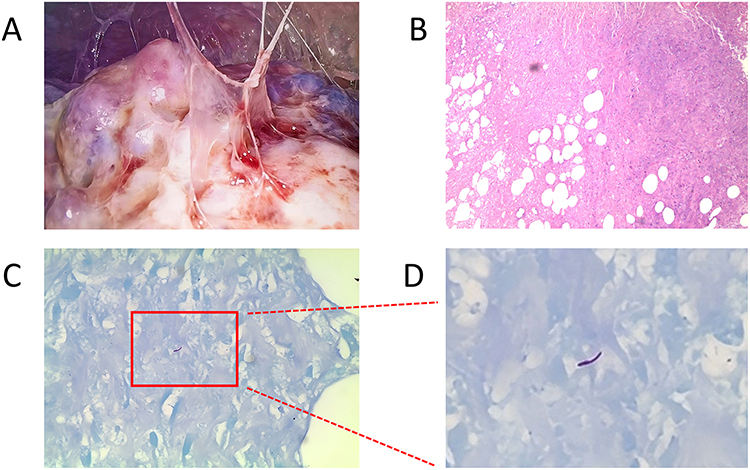 |
Figure 4 Laparoscopic manifestations of the peritoneum alongside histopathological and AFB staining results of the peritoneal biopsy. (A) Laparoscopic visualization reveals extensive thickening of the greater omentum and peritoneum with surfaces densely studded with numerous grayish white nodules. (B) Collagenized fibrous connective tissue accompanied by massive inflammatory cell infiltration. The section utilizes a hematoxylin and eosin stain at an original magnification of ×100. (C) Clear visualization of AFB exhibiting positive staining. The section utilizes an AFB stain at an original magnification of ×100. (D) Magnified view of the positive region in panel C (original magnification, ×300). |
Antituberculosis treatment was started with isoniazid 300 mg once daily, rifampicin 600 mg once daily, pyrazinamide 1500 mg once daily, ethambutol 750 mg once daily, and levofloxacin 500 mg once daily. Supportive management included ultrasound-guided pleural and abdominal drainage, furosemide, intravenous albumin, and enteral nutritional support. Despite these interventions, the patient developed chills, high fever, hypotension, and progressive oliguria. Laboratory testing showed marked inflammatory worsening, with C-reactive protein rising to 210 mg/L and procalcitonin to 25 ng/mL. He was transferred to the intensive care unit for advanced supportive care, but his condition progressed to sepsis with multiorgan failure, and he died during hospitalization.
Cytological Processing and Interpretation of Serous Fluids
Pleural and ascitic fluid specimens first underwent routine gross examination, including assessment of color and clarity. Total nucleated cell counts were then performed. For cytological evaluation, fluid samples were processed by cytocentrifugation at 800 rpm for 10 min, and the resulting smears were stained with Wright-Giemsa stain for 15 min. Differential cell classification was subsequently performed, and cytomorphological features were described based on microscopic examination. For reproducibility, all cytological slides were independently reviewed by two experienced laboratory physicians.
Discussion
PTB is an important form of extrapulmonary tuberculosis, but its diagnosis remains challenging because the clinical and radiologic findings are often nonspecific and may overlap with those of peritoneal carcinomatosis, cirrhotic ascites, bacterial peritonitis, and inflammatory bowel disease.19–22 Our two cases illustrate this difficulty. In Case 1, abdominal distension was the main manifestation without systemic symptoms of tuberculosis. In Case 2, progressive abdominal distension, pleural effusions, anorexia, and weight loss initially raised strong concern for malignancy. Imaging was likewise nondiagnostic in both patients, showing peritoneal and omental thickening but not establishing the etiology.3,21
Microbiological and molecular testing also had important limitations. Direct detection methods in serous effusions are known to have suboptimal sensitivity, particularly in paucibacillary specimens.10,13 In Case 1, ascitic fluid AFB staining and M. tuberculosis NAAT were negative. Because PTB was already strongly suspected clinically, NAAT was prioritized as the initial rapid and more affordable molecular test; NGS was not pursued thereafter because of the patient’s financial constraints. In Case 2, ascitic ADA was low, AFB staining was negative, and tNGS performed on pleural and ascitic fluid samples did not detect M. tuberculosis. Published evidence supports this limitation. PTB is typically paucibacillary, and molecular testing of ascitic fluid therefore has limited sensitivity.23 Available PTB-specific molecular data mainly concern Xpert/NAAT rather than mNGS or tNGS: reported ascitic-fluid Xpert sensitivities range from 28.6% to 70.6%, and a review citing pooled data reported a sensitivity of 59% and a specificity of 97.9%, corresponding to an estimated false-negative rate of 41%.24,25 Even for peritoneal tissue, Xpert sensitivity was only 60.7% in one study.26 Robust ascites-specific false-negative estimates for tNGS/mNGS are currently unavailable because direct studies in tuberculous ascites are scarce. Therefore, evidence from ascitic-fluid Xpert studies and broader sequencing studies of extrapulmonary tuberculosis and serous-fluid specimens was cited only as indirect contextual support. In a smear-negative extrapulmonary tuberculosis cohort, mNGS sensitivity was 56.1%, and a recent nanopore study reported 76.9% sensitivity in a small abdominal-effusion subgroup, supporting cautious interpretation of negative sequencing results in serous specimens.27,28
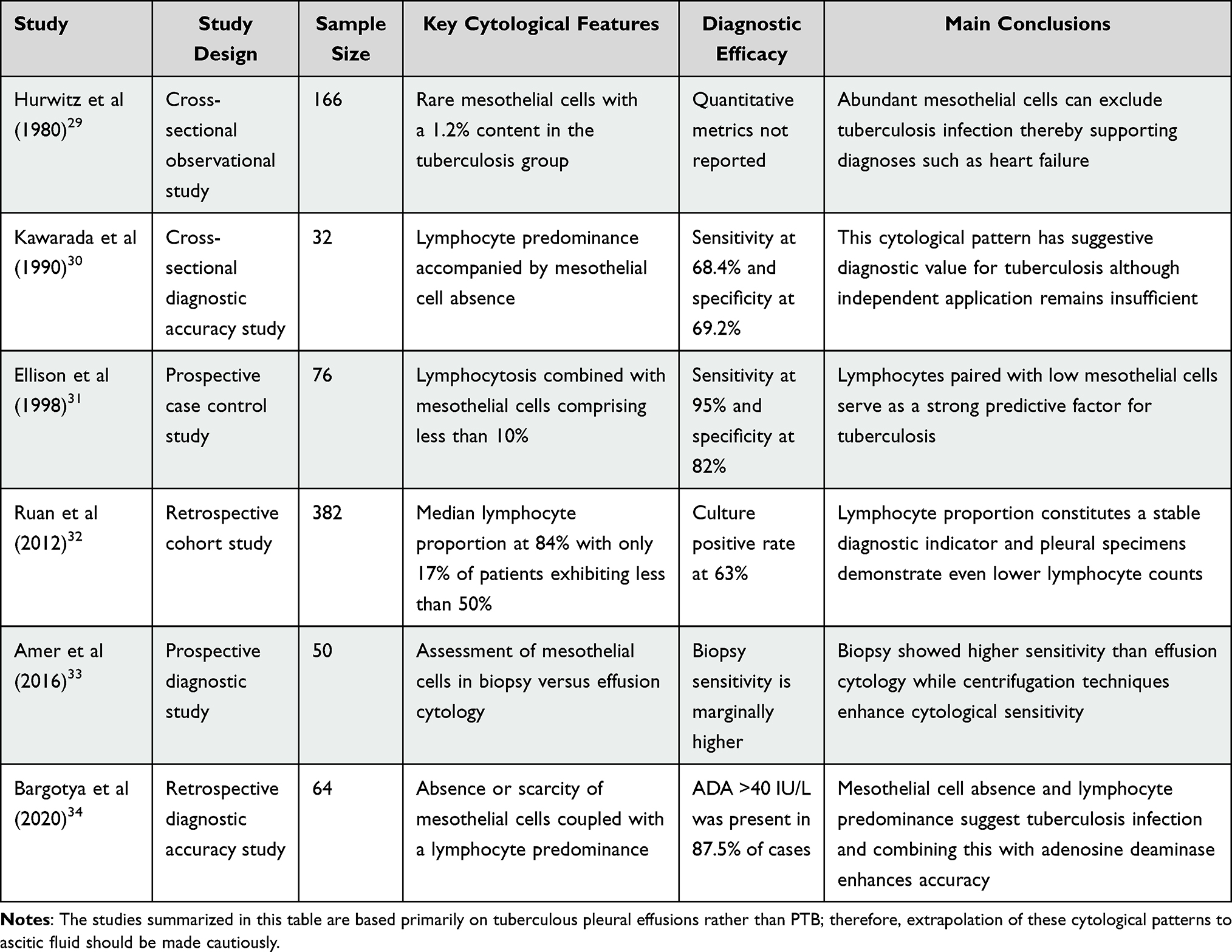 |
Table 2 Summary of Published Studies Describing the Cytological Features of Tuberculous Pleural Effusions |
In this setting, routine cytological examination provided an additional clue. Case 1 showed a nucleated cell count of 7,900 ×106/L, with 76% lymphocytes, mesothelial cells less than 1%, and no malignant cells. Case 2 showed a nucleated cell count of 6,726 ×106/L, with 82% lymphocytes, mesothelial cells less than 1%, and no atypical cells in ascitic fluid; the pleural fluid also showed lymphocyte predominance. Although nonspecific, these findings supported consideration of PTB in the appropriate clinical context. Importantly, the absence of malignant cells on cytology does not exclude peritoneal malignancy. Previous studies have reported that tuberculous serous effusions are often characterized by lymphocyte predominance and a low proportion of mesothelial cells (Table 2).29–34 In practical terms, such effusions generally have lymphocytes accounting for more than 50% of nucleated cells, often reaching 80–90% in tuberculous pleural effusions, whereas mesothelial cells are typically sparse, often less than 10% and frequently less than 5% or even absent.29–34 However, most available data derive from pleural rather than PTB, so extrapolation to ascitic fluid should be made cautiously. Ascites-specific differential cell proportion data remain limited, although one series of PTB described 91.9% of ascitic fluid samples as lymphocyte-rich.35 In addition, cytology alone is insufficient to establish the diagnosis. These cytomorphologic findings should therefore be regarded as supportive rather than definitive. The biological basis for this pattern is plausible. Tuberculous serositis is associated with a predominantly cell-mediated immune response, with lymphocyte recruitment at the serosal surface and granulomatous inflammation in involved tissue.36–39 Chronic inflammatory injury may also reduce the mesothelial cell component in effusion specimens.40,41 Even so, this pattern likely reflects the host inflammatory response rather than pathogen burden itself.
This study is limited by its retrospective, descriptive design, the inclusion of only two cases, and the lack of a validated cytological cutoff for PTB. Routine ascitic fluid cytology should not replace microbiological or histopathological confirmation, and robust evidence for its diagnostic performance in PTB remains lacking.23 However, because it is inexpensive and widely available, a lymphocyte-predominant, mesothelial-poor effusion may still provide a practical supportive clue when NGS is unavailable or molecular results are negative or nondiagnostic.23,25 This may be particularly relevant in patients at risk of poor outcomes, as older age, ascites, rapid weight loss, and renal or hepatic dysfunction, including elevated serum creatinine or ALT, have been associated with adverse prognosis in PTB.42 Case 2 had several of these concerning features, including older age, marked ascites, and recent weight loss; thus, although earlier diagnosis might have improved his chance of survival, it would not necessarily have guaranteed a favorable outcome.42,43 Larger prospective studies are needed to clarify the diagnostic value of these cytological findings. Overall, PTB remains challenging to diagnose, and these cytological findings should be interpreted as supportive rather than diagnostic in the appropriate clinical context. Taken together, our cases suggest that routine ascitic fluid cytology may still serve as a useful adjunct in the stepwise evaluation of suspected PTB.
Data Sharing Statement
The original contributions presented in the study are included in the article material. Further inquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This retrospective case report was approved by the Ethics Committee of General Hospital of Southern Theater Command (No. NZLLKZ2025062). Written informed consent for publication of the clinical details and accompanying imaging materials of Patient 1 was obtained from the patient directly. For Patient 2, who is deceased, written informed consent for publication of their clinical details and accompanying imaging materials was obtained from their legally authorized next of kin. Prior to signing the consent forms, both the patient and the next of kin were provided with and reviewed the complete manuscript to ensure full understanding and agreement to the publication of the case details.
Funding
The authors declare that no financial support was received for the research, authorship, and/or publication of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jha DK, Pathiyil MM, Sharma V. Evidence-based approach to diagnosis and management of abdominal tuberculosis. Indian J Gastroenterol. 2023;42(1):17–8. doi:10.1007/s12664-023-01343-x
2. Adegbite BR, Elegbede-Adegbite NOM, Edoa JR, et al. Clinical features, treatment outcomes and mortality risk of tuberculosis sepsis in HIV-negative patients: a systematic review and meta-analysis of case reports. Infection. 2023;51(3):609–621. doi:10.1007/s15010-022-01950-4
3. Jha DK, Gupta P, Neelam PB, et al. Clinical and radiological parameters to discriminate tuberculous peritonitis and peritoneal carcinomatosis. Diagnostics. 2023;13(20):3206. doi:10.3390/diagnostics13203206
4. Muñoz-Muñoz M, Enciso-Hurtado AA, Morado-López AN, et al. Peritoneal tuberculosis with an atypical presentation: surgical case report. Int J Surg Case Rep. 2024;123:110299. doi:10.1016/j.ijscr.2024.110299
5. Yu J, Chang Y, Liang C, et al. Study on the association network of tuberculosis lesions in adult extrapulmonary tuberculosis in China: a large-scale multicenter observational study. Can J Infect Dis Med Microbiol. 2025;2025:4944872. doi:10.1155/cjid/4944872
6. Ling CW, Sud K, Castelino RL, et al. Systematic review on treatment and outcomes of tuberculous peritonitis in patients on peritoneal dialysis. Kidney Int Rep. 2023;9(2):277–286. doi:10.1016/j.ekir.2023.11.012
7. Jha DK, Kakadiya R, Sharma A, et al. Assessment and management for latent tuberculosis before advanced therapies for immune-mediated inflammatory diseases: a comprehensive review. Autoimmun Rev. 2025;24(3):103758. doi:10.1016/j.autrev.2025.103758
8. Sester M, Altet-Gomez N, Andersen SB, et al. Diagnostic accuracy and predictive value of the QuantiFERON-TB Gold Plus assay for tuberculosis in immunocompromised individuals: a prospective TBnet study. Lancet Reg Health Eur. 2025;57:101416. doi:10.1016/j.lanepe.2025.101416
9. Cox H, Salaam-Dreyer Z, Goig GA, et al. Potential contribution of HIV during first-line tuberculosis treatment to subsequent rifampicin-monoresistant tuberculosis and acquired tuberculosis drug resistance in South Africa: a retrospective molecular epidemiology study. Lancet Microbe. 2021;2(11):e584–e593. doi:10.1016/S2666-5247(21)00144-0
10. Cohen LA, Light RW. Tuberculous pleural effusion. Turk Thorac J. 2015;16(1):1–9. doi:10.5152/ttd.2014.001
11. Gao S, Wang C, Yu X, et al. Xpert MTB/RIF Ultra enhanced tuberculous pleurisy diagnosis for patients with unexplained exudative pleural effusion who underwent a pleural biopsy via thoracoscopy: a prospective cohort study. Int J Infect Dis. 2021;106:370–375. doi:10.1016/j.ijid.2021.04.011
12. Dookie N, Khan A, Padayatchi N, et al. Application of next generation sequencing for diagnosis and clinical management of drug-resistant tuberculosis: updates on recent developments in the field. Front Microbiol. 2022;13:775030. doi:10.3389/fmicb.2022.775030
13. Mor P, Dahiya B, Parshad S, et al. Recent updates in diagnosis of abdominal tuberculosis with emphasis on nucleic acid amplification tests. Expert Rev Gastroenterol Hepatol. 2022;16(1):33–49. doi:10.1080/17474124.2022.2021068
14. Patel KP, Korbitz PM, Gallagher JP, et al. Ascitic calprotectin and lactoferrin for detection of spontaneous bacterial peritonitis: a systematic review and meta-analysis. Transl Gastroenterol Hepatol. 2022;7:37. doi:10.21037/tgh-20-323
15. Osman HA, Aly SS, Salah-Eldin EM, et al. Diagnostic validity of flow cytometry vs manual counting of polymorphonuclear leukocytes in spontaneous bacterial peritonitis. J Clin Lab Anal. 2018;32(5):e22395. doi:10.1002/jcla.22395
16. Lovey A, Verma S, Kaipilyawar V, et al. Early alveolar macrophage response and IL-1R-dependent T cell priming determine transmissibility of Mycobacterium tuberculosis strains. Nat Commun. 2022;13(1):884. doi:10.1038/s41467-022-28506-2
17. Hamada Y, Cirillo DM, Matteelli A, et al. Tests for tuberculosis infection: landscape analysis. Eur Respir J. 2021;58(5):2100167. doi:10.1183/13993003.00167-2021
18. Sutherland JS, Garba D, Fombah AE, et al. Highly accurate diagnosis of pleural tuberculosis by immunological analysis of the pleural effusion. PLoS One. 2012;7(1):e30324. doi:10.1371/journal.pone.0030324
19. Baykan AH, Sayiner HS, Aydin E, et al. Extrapulmonary tuberculosis: an old but resurgent problem. Insights Imaging. 2022;13(1):39. doi:10.1186/s13244-022-01172-0
20. Zebarjadi Bagherpour J, Bagherian Lemraski S, Haghbin Toutounchi A, et al. Peritoneal tuberculosis pretending an acute abdomen: a case report and literature review. Int J Surg Case Rep. 2023;109:108507. doi:10.1016/j.ijscr.2023.108507
21. Uygur-Bayramicli O, Dabak G, Dabak R. A clinical dilemma: abdominal tuberculosis. World J Gastroenterol. 2003;9(5):1098–1101. doi:10.3748/wjg.v9.i5.1098
22. Chen H, Wu M, Chang W, et al. Abdominal tuberculosis in southeastern Taiwan: 20 years of experience. J Formos Med Assoc. 2009;108(3):195–201. doi:10.1016/S0929-6646(09)60052-8
23. Koff A, Azar MM. Diagnosing peritoneal tuberculosis. BMJ Case Rep. 2020;13(2):e233131. doi:10.1136/bcr-2019-233131
24. Ahmad R, Changeez M, Khan JS, et al. Diagnostic accuracy of peritoneal fluid GeneXpert in the diagnosis of intestinal tuberculosis, keeping histopathology as the gold standard. Cureus. 2018;10(10):e3451. doi:10.7759/cureus.3451
25. Rufai SB, Singh S, Singh A, et al. Performance of Xpert MTB/RIF on ascitic fluid samples for detection of abdominal tuberculosis. J Lab Physicians. 2017;9(1):47–52. doi:10.4103/0974-2727.187927
26. Dahale AS, Puri AS, Kumar A, et al. Tissue Xpert MTB/RIF assay in peritoneal tuberculosis: to be (done) or not to be (done). Cureus. 2019;11(6):e5009. doi:10.7759/cureus.5009
27. Sun W, Lu Z, Yan L. Clinical efficacy of metagenomic next-generation sequencing for rapid detection of Mycobacterium tuberculosis in smear-negative extrapulmonary specimens in a high tuberculosis burden area. Int J Infect Dis. 2021;103:91–96. doi:10.1016/j.ijid.2020.11.165
28. Chen Y, Ling Y, Xu X, et al. Diagnostic utility of nanopore sequencing for tuberculous serous effusions. Infect Drug Resist. 2025;18:3661–3670. doi:10.2147/IDR.S524986
29. Hurwitz S, Leiman G, Shapiro C. Mesothelial cells in pleural fluid: TB or not TB? S Afr Med J. 1980;57(23):937–939.
30. Kawarada Y, Nagata N, Takayama K, et al. The significance of pleural fluid cytology in the differential diagnosis of pleurisy showing lymphocyte-predominant pleural effusion. Kekkaku. 1990;65(9):575–579.
31. Ellison E, Lapuerta P, Martin SE. Cytologic features of mycobacterial pleuritis: logistic regression and statistical analysis of a blinded, case-controlled study. Diagn Cytopathol. 1998;19(3):173–176. doi:10.1002/(SICI)1097-0339(199809)19:3<173::AID-DC3>3.0.CO;2-E
32. Ruan SY, Chuang YC, Wang JY, et al. Revisiting tuberculous pleurisy: pleural fluid characteristics and diagnostic yield of mycobacterial culture in an endemic area. Thorax. 2012;67(9):822–827. doi:10.1136/thoraxjnl-2011-201363
33. Amer S, Hefnawy AE, Wahab NA, et al. Evaluation of different laboratory methods for rapid diagnosis of tuberculous pleurisy. Int J Mycobacteriol. 2016;5(4):437–445. doi:10.1016/j.ijmyco.2016.07.001
34. Bargotya M, Kachhap P, Kumar L, et al. Importance of absence of mesothelial cells and other useful parameters in the diagnosis of tubercular pleural effusion: our experience in a tertiary care hospital. Int J Biol Med Res. 2020;11(2):7046–7050.
35. Maheshwari A, Gupta S, Rai S, et al. Clinical and laboratory characteristics of patients with peritoneal tuberculosis mimicking advanced ovarian cancer. South Asian J Cancer. 2021;10(2):102–106. doi:10.1055/s-0041-1736030
36. Jiang F, Han Y, Liu Y, et al. A comprehensive approach to developing a multi-epitope vaccine against Mycobacterium tuberculosis: from in silico design to in vitro immunization evaluation. Front Immunol. 2023;14:1280299. doi:10.3389/fimmu.2023.1280299
37. Van Dis E, Fox DM, Morrison HM, et al. IFN-gamma-independent control of M. tuberculosis requires CD4 T cell-derived GM-CSF and activation of HIF-1alpha. PLoS Pathog. 2022;18(7):e1010721. doi:10.1371/journal.ppat.1010721
38. Novita BD, Tjahjono Y, Wijaya S, et al. Characterization of chemokine and cytokine expression pattern in tuberculous lymphadenitis patient. Front Immunol. 2022;13:983269. doi:10.3389/fimmu.2022.983269
39. Pullagurla A, Rapolu B, Ahmad S, et al. Immune profiles of MCP-1 with Mtb antigens and recombinant cytokines stimulation in tuberculosis. Cytokine. 2024;179:156622. doi:10.1016/j.cyto.2024.156622
40. Jhilta A, Jadhav K, Sharma R, et al. Host-directed therapy with inhalable lovastatin microspheres for matrix metalloproteinase inhibition in tuberculosis. ACS Appl Bio Mater. 2025;8(2):1533–1546. doi:10.1021/acsabm.4c01723
41. Zang X, Zhang J, Jiang Y, et al. Serine protease Rv2569c facilitates transmission of Mycobacterium tuberculosis via disrupting the epithelial barrier by cleaving E-cadherin. PLoS Pathog. 2024;20(5):e1012214. doi:10.1371/journal.ppat.1012214
42. Tanoglu A, Erdem H, Friedland JS, et al. Clinicopathological profile of peritoneal tuberculosis and a new scoring model for predicting mortality: an international ID-IRI study. Eur J Clin Microbiol Infect Dis. 2023;42(8):981–992. doi:10.1007/s10096-023-04630-9
43. Chow KM, Chow VCY, Hung LCT, et al. Tuberculous peritonitis-associated mortality is high among patients waiting for the results of mycobacterial cultures of ascitic fluid samples. Clin Infect Dis. 2002;35(4):409–413. doi:10.1086/341898
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.