Back to Journals » Journal of Inflammation Research » Volume 13
Lymphatic Flow: A Potential Target in Sepsis-Associated Acute Lung Injury
Authors Wu C, Li H ![]() , Zhang P
, Zhang P ![]() , Tian C, Luo J
, Tian C, Luo J ![]() , Zhang W, Bhandari S, Jin S
, Zhang W, Bhandari S, Jin S ![]() , Hao Y
, Hao Y ![]()
Received 27 September 2020
Accepted for publication 10 November 2020
Published 23 November 2020 Volume 2020:13 Pages 961—968
DOI https://doi.org/10.2147/JIR.S284090
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Chenghua Wu,1,* Hui Li,1,2,* Puhong Zhang,1 Chao Tian,1 Jun Luo,1 Wenyan Zhang,1 Suwas Bhandari,1 Shengwei Jin,1 Yu Hao1
1Department of Anaesthesia and Critical Care, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 2Key Laboratory of Anaesthesiology of Zhejiang Province, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shengwei Jin; Yu Hao Email [email protected]; [email protected]
Abstract: Sepsis is life-threatening organ dysfunction caused by an imbalance in the body’s response to infection and acute lung injury (ALI) related to sepsis is a common complication. The rapid morbidity and high mortality associated with sepsis is a significant clinical problem facing critical care medicine. Inflammation plays a vital role in the occurrence of sepsis. Notably, the body produces different immune cells and pro-inflammatory factors to clear pathogens. However, excessive inflammation can damage multiple tissues and organs when it fails to resolve in time. Additionally, lymphatic vessels could effectively transfer inflammatory cells and factors away from tissues and into blood circulation, thereby reducing damage, and promoting the resolution of inflammation. Therefore, any dysfunction and/or destruction of the lymphatic system may result in lymphedema followed by inflammatory storms and eventual sepsis. Consequently, the present study aimed to review and highlight the role of lymphatic vessels in related body tissues and organs during sepsis and other associated diseases.
Keywords: sepsis, acute lung injury, lymphatic flow
Introduction
Sepsis-3, which was published in 2016, defines sepsis as life-threatening organ dysfunction caused by a dysregulated host response to infection.1–3 On the other hand, septic shock refers to a subset of sepsis in which underlying circulatory and cellular metabolism abnormalities are profound enough to substantially increase mortality.1–3 It is also considered to have a higher mortality rate than sepsis although both conditions are significant clinical problems in critical care medicine. According to recent reports, there were approximately 48.9 million new cases of sepsis worldwide in 2017 alone (95% uncertainty interval [UI] 38.9–62.9), out of which 11 million (10.1–12.0) resulted in death. This accounted for about 19.7% of all the deaths worldwide (18.2–21.4).4 The data also showed that patients with sepsis often developed new adverse sequelae after treatment, including long-term disability and worsening chronic health conditions,5 which required them to be re-hospitalized.6,7 Therefore, it is critical for new and effective therapeutic targets for sepsis to be developed.
Lymphatic vessels are dynamically structured and closely related to the surrounding microenvironment. They are also a passive conduit for transporting liquids and proteins. The vessels are widely found in the dermis of the skin and the mucous membranes covering major organs, including the respiratory tract, gut, kidney, heart and lungs.8 In addition, Louveau et al showed that lymphatic vessels are present in the meninges and were able to effectively remove β-amyloid.9 Lymphatic vessels are tubular structures composed of a single layer of oak-leaf-shaped Lymphatic Endothelial Cells (LECs) and some surrounding parietal cells.10
The most superficially placed lymphatic vessels starting from the blind lymphatic capillaries absorb the interstitial fluid exuded from blood. However, they all converge from the afferent lymphatic vessel to the lymph node, hence, transporting the interstitial fluid to the collecting lymphatic vessels through the efferent lymphatics.11,12 This eventually flows into blood circulation through the lymphatic vein.11 Moreover, several neutrophils, macrophages, T cells and B cells capable of identifying and eliminating foreign antigens are present in the lymph nodes.13,14 As such, lymphatic vessels play an essential role in immune surveillance including the recruitment of white blood cells and macrophages with the subsequent formation of adaptive immunity after resolving inflammation. Interestingly, the flow of interstitial fluid occurs primarily through the collecting lymphatic vessels, while the initial lymphatic vessel is responsible for the absorption of interstitial fluid.15 This can be better explained by the distinct anatomies of the two lymphatic vessels. Moreover, absorption is made possible due to the smooth muscle cells and pericytes found around the collecting lymphatic vessels, although they are not absent in the initial lymphatic vessels.15
Most lymphatic networks are formed during the embryonic period, although they are dynamically impacted later at adulthood, in cases of wound healing, tumor formation and lymphogenesis after organ transplantation.9,10 Additionally, lymphatic capillaries consist of a single layer of LECs lacking in solid support cells and tissues including pericytes and smooth muscle cells. This lack of support cells and tissues therefore makes them susceptible to physical and medical injuries resulting to dysfunction in lymphatics followed by lymphedema.16,17 Thus, this study sought to review and highlight the role of lymphatic vessels in related body tissues and organs during sepsis and other related diseases.
Lymphatic Flow
In most vertebrates, the primary function of lymphatic vessels is to collect the excess protein-rich fluid exuding from blood vessels and transporting it back to blood circulation.18,19 Nevertheless, studies show that lymphatic vessels are multifunctional structures that respond positively to the tissue microenvironment of the tissue. In addition, the vessels have essential immune monitoring functions as they deliver various antigens and activated antigen-presenting cells to the lymph nodes and output immune effector cells as well as and humoral immune factors into blood circulation.20,21 Therefore, they can significantly regulate specific biological processes, such as tumors and inflammation.
Lymphatic flow is widely described in cancer and is considered to be a detrimental factor in tumor control. However, surrounding lymphatic network(s) can be affected due to the carcinogenic deposits in lymph nodes.22 In mouse models, overexpression of the Vascular Endothelial Growth Factor C (VEGFC) and other pro-lymphangiogenic factors can result in the rapid growth of the lymphatic vessels around tumors, thereby promoting metastasis.22 Currently, researchers are keen to ascertain the role of meningeal lymphatic vessels in regulating tumor metastasis following the discovery of meningeal lymphatic vessels in 2015. Additionally, Hu et al showed that destruction of the meningeal lymphatic vessels reduces the spread of tumor cells to deep-lying cervical lymph nodes.23 Therefore, targeting the lymphatic drainage function (inhibiting lymphangiogenesis near tumor cells) is one of the potential strategies for the treatment of cancer. Moreover, Alitalo et al showed that lymphatics plays a crucial role in regulating the resolution of inflammation,24 leading to increased research in chronic inflammation including Rheumatoid Arthritis (RA) and periodontitis. It was previously observed that K/B×N mice (a typical RA model mouse) demonstrated a marked decrease in lymphatic flow.25 However, Zhou et al reported increased lymphangiogenesis maintaining adequate lymphatic flow in the initial stages of RA although it was only a compensatory phenomenon that did not change the final outcome,26 where lymphatic flow markedly decreased. With advances made in technology, visualization and quantification of lymphatic function using Near-infrared (NIR) imaging provides a unique opportunity to examine the role of lymphatic flow in various human diseases.27–29 For instance, Bell et al investigated the function of lymphatic draining in the hands of RA patients and healthy volunteers through NIR imaging. The results showed that lymphatic drainage in the hands of RA patients was reduced compared to that of healthy volunteers.30 Interesting research on chronic inflammation including periodontitis also exists. For example, Hua Wang and colleagues demonstrated that there was impaired lymphatic flow in mice and patients with periodontitis.31 In addition, promoting lymphatic flow by enhancing lymphangiogenesis can effectively reduce alveolar bone damage and alleviate periodontitis. Given the advances in technology, there is currently a keen focus on the relationship between lymphatic flow and chronic inflammation. However, literature on lymphatic flow in acute inflammation, such as sepsis is currently scarce.
Sepsis is primarily caused by infection. When bacteria or other pathogens invade the body, innate cells recognize the pathogens through a series of Pattern Recognition Receptors (PRR) that identify Pathogen-Associated Molecular Patterns (PAMPs) and Damage-Associated Molecular Patterns (DAMP). Afterwards, activated Nuclear Factor kappa-B (NF-κB) enters the nucleus and subsequently activates target genes, including those encoding cytokines, which are essential for inducing inflammation (Figure 1). Some Pro-inflammatory cytokines are involved in the pathogenesis of sepsis, including the Tumor Necrosis Factor (TNF), Interleukin-1β (IL-1β), Interleukin-12 (IL-12) and Interleukin-18 (IL-18).32,33 In addition, it was reported that blocking or eliminating these cytokines had some protective effects in animal models with acute fulminant infections.33 Additionally, persistent inflammation leads to redness, pain, fever and possible multiple organ failure. Moreover, failure of adequately resolve inflammation can influence the formation of adaptive immunity, eventually leading to chronic inflammation such as obesity and RA.34
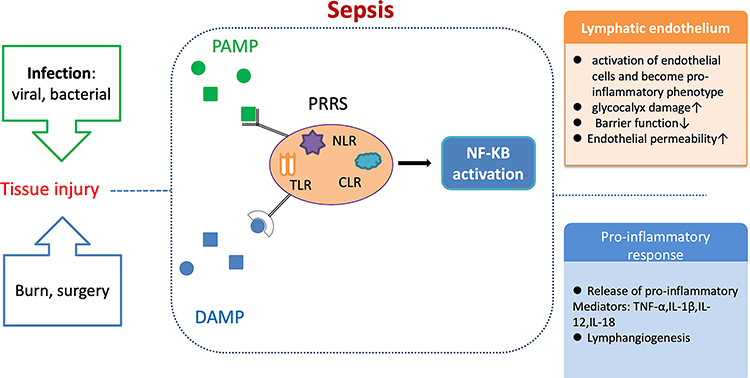 |
Figure 1 A series of immune and inflammatory reactions are triggered after the body is invaded by foreign pathogens. After infection or injury, the invading pathogen encounters the host innate immune system. The innate cells “sense” pathogens by recognizing PAMP and DAMP through the amount of PRRS, including TLR, NLR and CLR. The NF-ΚB pathway is then activated and this transports pro-inflammatory factors through the lymphatic vessels to the site of inflammation. During sepsis, endothelial homeostasis is impaired in both blood and lymphatic vessels. In addition, the endothelial barrier is destroyed and permeability is increased. |
Over the years, our research group has been dedicated to understanding the pathogenesis of sepsis. As a result, it was shown that one of the fundamental causes of sepsis is the inability to resolve inflammation since promoting the resolution of inflammation in mice with sepsis effectively reduced mortality.35,36 Additionally, lymphatic vessels could effectively transfer inflammatory cells and factors away from tissues and into blood circulation, thereby reducing damage, and promoting the resolution of inflammation. Furthermore, existing research on rat mesentery suggests that Lipopolysaccharide (LPS) modulate neutrophil recruitment and macrophage polarization on lymphatic vessel, thereby impairing lymphatic function.37 Therefore, it is clear that inflammation is closely related to the function of the lymphatic system.
Interestingly, the morphology of the lymphatic vessels also changes during this process. Lymphatic vessels are usually button-shaped after birth although they have a zipper-shaped morphology during the embryonic stage. However, during inflammation, they return to the zipper-shaped form.38 It is worth mentioning that the button-shaped lymphatic vessels drain into the lymphatic system faster than the zipper-shaped ones.39 Moreover, experimental results on transgenic mice overexpressing VEGFC revealed increased lymphatic vessel density, and this improved tissue edema in UV irradiation or lipopolysaccharide models.38 This therefore leads to the question on whether the inflammatory storm during sepsis is caused by disorders in lymphatic flow.
Nonetheless, the role of lymphatic vessels on the onset of sepsis remains largely unclear. However, it is known that the most severely damaged organs in sepsis patients are usually the lungs, kidneys and the heart.39 Moreover, patients with sepsis sometimes develop the Acute Respiratory Distress Syndrome (ARDS), acute kidney injury and other complications. Previous research established that mice with impaired lymphatics had more pulmonary edema compared to the control mice.40 Furthermore, it was reported that impaired lymphatics could lead to decreased blood oxygen saturation and reduced lung function.40 Therefore, more focus should be put on impaired lymphatic flow as it is closely related to the pathogenesis of sepsis.
Sepsis-Related Organ Damage
Sepsis and ALI Model
Bacterial LPS (endotoxin) is a toxic component on the outer membrane of the cell wall of gram-negative bacteria and can induce inflammation.41 Also, nearly 20% of previous studies on ALI confirmed the relationship between endotoxins and inflammation using the model.42 This is because the model is highly reproducible in establishing relative neutrophilic alveolitis and damage caused to the alveolar-capillary membrane. Additionally, the model makes it easy to assess the degree of pulmonary inflammation, and evaluate both the early and resolution phases of ALI.43
LPS is the major Gram-negative PAMP and can stimulate inflammation by binding to cells that express the Toll-like receptor 4 (TLR4).44 Nonetheless, it also binds to the LPS Binding Protein (LBP) which is recognized by CD14 (membrane-anchored co-receptor), thus creating a channel for LPS to bind to the extracellular portion of TLR4,45 as shown in Figure 1. Notably, the dosage used for each species is often different during the establishment of the LPS-induced ALI model. For instance, in the C57BL/6 mice, the dosage ranged from 1mg/kg to 6mg/kg for 6h to 96h and administered through intra-tracheal route.42,46,47 However, in Sprague-Dawley rats, the dosage ranged from 5mg/kg to 20mg/kg and was administered through the tail vein for at least 6h.48–50
Apart from the most reported LPS models, there is also an ALI model induced by Cecal Ligation and Puncture (CLP). Given that several cases of human sepsis and lung injury follow intraperitoneal infection, animal models on sepsis and acute lung injury after peritonitis have been established and this includes the CLP model.51 The obvious difference between the two models is that the effect of the CLP model generally occurs within a few days while that of the LPS model is immediate. For example, in the LPS model, leukopenia and lung injury occurred within 24–30 hours and 18–72 hours, respectively, after surgery.52
All in all, the LPS-induced and CLP-induced ALI models are the most common models of sepsis. Nonetheless, several animal models of sepsis have been developed for the study of ALI, since the condition is a significant cause of death in ARDS.53
ALI and Lymphatic Flow
ALI is a common disease and ARDS is its most severe manifestation. ARDS is a clinical syndrome in critically ill patients and is associated with acute respiratory failure, hypoxemia and bilateral pulmonary infiltrates consistent with edema. Although our understanding of the pathophysiological changes associated with ALI/ARDS has improved, it is still difficult to effectively control the disease since the mortality rate is still high at ~40%.54 However, the pathogenesis of ALI/ARDS can best be understood by focusing on lung endothelial injury and alveolar epithelial injury.
First, pulmonary vascular injury is the leading cause of ALI/ARDS since changes in vascular permeability caused by lung vessels and significant endothelial injury lead to pulmonary edema, considerably rich in protein.55,56 Moreover, there are diverse mechanisms for pulmonary vascular endothelial injury, but the most reported one is neutrophil-dependent lung injury.57,58 In the setting of lung injury, neutrophils accumulate and activate in the pulmonary microvasculature, releasing various harmful mediators such as proteases, reactive oxygen species, proinflammatory cytokines, and procoagulant molecules. These result to changes in pulmonary vascular permeability and subsequent loss of endothelial barrier function.52
Other studies also exist on the synergistic role of platelets and neutrophils in causing pulmonary vascular endothelial injury.59 Notably, pulmonary vascular injury is a prerequisite for the development of protein-rich pulmonary edema in ALI/ARDS. However, in the absence of a certain degree of lung epithelial injury, lung endothelial injury is usually not sufficient to cause ARDS.60 Additionally, experimental studies on animal models showed that when the lung endothelium was moderately injured, the alveolar epithelium was not damaged.61 Interestingly, the mechanism of alveolar epithelial damage was shown to be similar to that of pulmonary vascular endothelial damage, where a large number of neutrophils were aggregated and activated.60,61
In general, injury to the pulmonary vascular endothelium and the alveolar epithelium causes pulmonary edema and leukocyte infiltration, leading to poor gaseous exchange and in severe cases, progression to ALI/ARDS. During this stage, there is usually a large amount of edema fluid and inflammatory cells in the patient’s alveoli that cannot be eliminated on time, leading to disorder in the resolution of inflammation and eventual progression to sepsis (Figure 2). Normally, pulmonary edema fluid and inflammatory cells can be eliminated through blood vessels. However, due to the damage of alveolar epithelium and vascular endothelium in ALI/ARDS, a large amount of edema fluid and inflammatory cells penetrate into the interstitial tissue instead of being eliminated through blood circulation. Therefore, a new way of eliminating edema fluid and inflammatory cells is needed and lymphatic vessels may play an important role in this process.
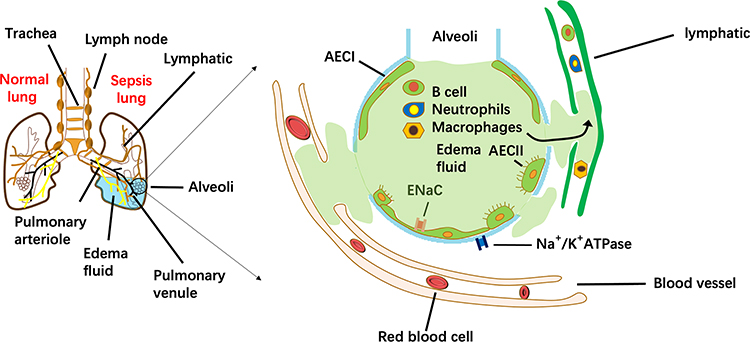 |
Figure 2 How to remove the edema fluid and inflammatory cells in the alveoli during sepsis. Compared to the normal lung, a large amount of pulmonary edema fluid and inflammatory cells (B cell, Neutrophils, Macrophages) accumulate in the alveoli of the sepsis lung. They are mainly discharged through ENaC and Na+/K+ ATPase into the interstitial space and blood circulation. However, increasing evidence has shown that lymphatic vessels play a vital role in draining alveolar fluid and inflammatory cells. During sepsis, destruction of the structure of lymphatic vessels leads to flow dysfunction, causing pulmonary edema and disorder in the resolution of inflammation. |
Over the past two decades, both pre-clinical and clinical studies have shown that there are always changes in pulmonary lymphatics in nearly all lung diseases.62 The changes include increased lymphangiogenesis in pneumonia, growth as well as the remodeling of lymphatic vessels in idiopathic pulmonary fibrosis and regression of lymphatic vessels in asthma.63 Additionally, pulmonary lymphatic vessels are widely spread throughout the pleura, mainly around the perivascular connective tissue, primarily at the venules and arterioles as well as the terminal and respiratory bronchioles.64 However, little information currently exists on lymphatic flow in ALI/ARDS and other related lung diseases. Moreover, the role of the lymphatic vessels in the occurrence of diseases is still unknown.
Nevertheless, Reed et al found that pulmonary collecting lymphatics have valves but lack Smooth Muscle Cells (SMCs),40 which is different from the characteristics of normal collective lymphatic vessels. They also found that the drainage of pulmonary collecting lymphatics primarily relies on respiration-associated pressure changes in the chest wall rather than vessel contraction.65 Moreover, most studies showed that the ability of alveolar epithelium to clear edema fluid is significantly impaired during ALI/ARDS.66,67 Therefore, drainage of pulmonary lymphatics for the prevention of pulmonary edema, as proposed by Reed et al, might improve gaseous exchange.40
It is therefore important to understand the function of lymphatic vessels in ALI/ARDS. In addition, it is possible that maintaining normal lymphatic flow might be a potential for the treatment of ALI/ARDS patients. A study by Hu et al showed that VEGFC-overexpressing mice had more dendritic cells transported to the deep cervical lymph nodes compared to the control group, and this process relied on the CCL21 and CCR7.23 Therefore, this leads to a second question on whether there is a relationship between the dysfunction in resolution of lung inflammation and lymphatic vessels. Arokiasamy et al found that lymphatic vessels also have an endothelial glycocalyx structure that functions in a similar manner to the endothelial glycocalyx in blood vessels.68 Notably, the structure is destroyed during inflammation, damaging the lymphatic barrier in the process.
Therefore, it can be suggested that the drainage capacity of lymphatics is hampered in ALI/ARDS due to the structural destruction of lymphatic vessels. Thus, many inflammatory cells in the lungs cannot be adequately drained into the lymph nodes, resulting to impairment in the resolution of inflammation resolution (Figure 2). Consequently, maintaining sufficient lymphatic flow in patients with ALI/ARDS may be a useful strategy.
Conclusion and Future Perspectives
Sepsis is an acute and critical illness with rapid onset and high mortality, that affects hundreds of thousands of people worldwide. Although there is currently a series of treatment options for sepsis, none of them completely clears the condition. Notably, some patients get re-hospitalized, even after adequate treatment, while a few people suffer from severe adverse reactions. Therefore, it is urgent to find new and useful therapeutic targets for the management of sepsis. Previous research from our study group using the LPS-induced sepsis model revealed a large number of inflammatory cells and inflammatory factors, as well as a dysfunction in the resolution of inflammation, resulting in a high mortality rate.
Moreover, lymphatic endothelial cells can secrete specific chemokines to promote the elimination of inflammatory cells, thereby accelerating the resolution of inflammation. It is worth noting that both chronic inflammation (RA and/or periodontitis) and LPS-induced acute inflammation result to a dysfunction in lymphatic flow. Additionally, the glycocalyx structure of the lymphatic endothelium is also damaged in acute inflammation. Consequently, it is significant to evaluate the changes in lymphatic function and structure during sepsis. Notably, a number of reports exist on the general molecular mechanisms that regulate lymphatic development and function. Therefore, more studies are needed to establish the crosslink between lymphatics in relative tissues and other organs systems, causing multiple organ dysfunction syndromes, particularly in sepsis.
Furthermore, maintaining normal lymphatic flow or promoting lymphangiogenesis during sepsis may be a potential therapeutic strategy. Generally, lymphangiogenesis can be promoted by increasing the expression of critical factors that regulate the development and maturation of lymphatic vessels, such as VEGFC and Vascular Endothelial Growth Factor Receptor 3 (VEGFR3). In addition, Specialized Pro-resolving Mediators (SPMs) are endogenous lipid mediators that play an essential role in resolving inflammation and are produced by arachidonic acid and omega-3 unsaturated fatty acids. It was previously reported that aspirin-triggered Resolvin D3 could promote lymphangiogenesis during acid-induced acute lung injury.69 Moreover, the formation of lymphatic vessels facilitates lymphatic flow, promoting the elimination of inflammatory cells and pulmonary edema fluid. Previous studies from our research group also showed that SPMs could reduce mortality in rats with sepsis and promote the elimination of pulmonary edema fluid as well as inflammatory cells.36,69 Therefore, more studies are needed to establish the therapeutic efficacy of SPMs in promoting the repair and the generation of lymphatics, which will eventually accelerate the resolution of inflammation during sepsis.
Acknowledgments
We hereby confirm that all figures are original. We thank Jian-guang Wang, Panhan Fu and Hongxia Mei for their support and advice.
Funding
This work was funded by the Natural Science Foundation of Zhejiang Province (No. LQ20H150003, No. LY19H150002), Key research and development project of Zhejiang province (No. 2019C03011), and the Wenzhou Science and Technology Bureau Project (No. Y20190087, No. Y20190118).
Disclosure
All authors report no potential conflicts of interest with regard to this work.
References
1. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:762–774. doi:10.1001/jama.2016.0288
2. Shankar-Hari M, Phillips GS, Levy ML, et al. Developing a new definition and assessing new clinical criteria for septic shock: for the third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:775–787.
3. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315:801–810. doi:10.1001/jama.2016.0287
4. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395:200–211. doi:10.1016/S0140-6736(19)32989-7
5. Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304:1787–1794. doi:10.1001/jama.2010.1553
6. Shah FA, Pike F, Alvarez K, et al. Bidirectional relationship between cognitive function and pneumonia. Am J Respir Crit Care Med. 2013;188:586–592. doi:10.1164/rccm.201212-2154OC
7. Yende S, Linde-Zwirble W, Mayr F, Weissfeld LA, Reis S, Angus DC. Risk of cardiovascular events in survivors of severe sepsis. Am J Respir Crit Care Med. 2014;189:1065–1074.
8. Petrova TV, Koh GY. Organ-specific lymphatic vasculature: from development to pathophysiology. J Exp Med. 2018;215:35–49. doi:10.1084/jem.20171868
9. Louveau A, Smirnov I, Keyes TJ, et al. Structural and functional features of central nervous system lymphatic vessels. Nature. 2015;523:337–341. doi:10.1038/nature14432
10. Pawlak JB, Bálint L, Lim L, et al. Lymphatic mimicry in maternal endothelial cells promotes placental spiral artery remodeling. J Clin Invest. 2019;129:4912–4921. doi:10.1172/JCI120446
11. Levick JR, Michel CC. Microvascular fluid exchange and the revised Starling principle. Cardiovasc Res. 2010;87:198–210. doi:10.1093/cvr/cvq062
12. Schulte-Merker S, Sabine A, Petrova TV. Lymphatic vascular morphogenesis in development, physiology, and disease. J Cell Biol. 2011;193(4):607–618. doi:10.1083/jcb.201012094
13. Förster R, Davalos-Misslitz AC, Rot A. CCR7 and its ligands: balancing immunity and tolerance. Nat Rev Immunol. 2008;8:362–371. doi:10.1038/nri2297
14. Johnson LA, Jackson DG. Cell traffic and the lymphatic endothelium. Ann N Y Acad Sci. 2008;1131:119–133. doi:10.1196/annals.1413.011
15. Petrova TV, Koh GY. Biological functions of lymphatic vessels. Science. 2020;369:eaax4063. doi:10.1126/science.aax4063
16. Mortimer PS, Rockson SG. New developments in clinical aspects of lymphatic disease. J Clin Invest. 2014;124:915–921. doi:10.1172/JCI71608
17. Aspelund A, Robciuc MR, Karaman S, Makinen T, Alitalo K. Lymphatic system in cardiovascular medicine. Circ Res. 2016;118:515–530. doi:10.1161/CIRCRESAHA.115.306544
18. Jeltsch M, Tammela T, Alitalo K, Wilting J. Genesis and pathogenesis of lymphatic vessels. Cell Tissue Res. 2003;314:69–84. doi:10.1007/s00441-003-0777-2
19. Oliver G, Alitalo K. The lymphatic vasculature: recent progress and paradigms. Annu Rev Cell Dev Biol. 2005;21:457–483. doi:10.1146/annurev.cellbio.21.012704.132338
20. Huggenberger R, Siddiqui SS, Brander D, et al. An important role of lymphatic vessel activation in limiting acute inflammation. Blood. 2011;117:4667–4678. doi:10.1182/blood-2010-10-316356
21. Kim J, Park DY, Bae H, et al. Impaired angiopoietin/Tie2 signaling compromises Schlemm’s canal integrity and induces glaucoma. J Clin Invest. 2017;127:3877–3896. doi:10.1172/JCI94668
22. Skobe M, Hawighorst T, Jackson DG, et al. Induction of tumor lymphangiogenesis by VEGF-C promotes breast cancer metastasis. Nat Med. 2001;7:192–198. doi:10.1038/84643
23. Hu X, Deng Q, Ma L, et al. Meningeal lymphatic vessels regulate brain tumor drainage and immunity. Cell Res. 2020;30:229–243.
24. Karpanen T, Alitalo K. Molecular biology and pathology of lymphangiogenesis. Annu Rev Pathol. 2008;3:367–397. doi:10.1146/annurev.pathmechdis.3.121806.151515
25. Zhou Q, Wood R, Schwarz EM, Wang YJ, Xing L. Near-infrared lymphatic imaging demonstrates the dynamics of lymph flow and lymphangiogenesis during the acute versus chronic phases of arthritis in mice. Arthritis Rheum. 2010;62:1881–1889.
26. Li J, Zhou Q, Wood RW, et al. CD23(+)/CD21(hi) B-cell translocation and ipsilateral lymph node collapse is associated with asymmetric arthritic flare in TNF-Tg mice. Arthritis Res Ther. 2011;13:R138. doi:10.1186/ar3452
27. Proulx ST, Luciani P, Dieterich LC, Karaman S, Leroux JC, Detmar M. Expansion of the lymphatic vasculature in cancer and inflammation: new opportunities for in vivo imaging and drug delivery. J Control Release. 2013;172:550–557. doi:10.1016/j.jconrel.2013.04.027
28. Mumprecht V, Detmar M. In vivo imaging of lymph node lymphangiogenesis by immuno-positron emission tomography. Methods Mol Biol. 2013;961:129–140.
29. Sevick-Muraca EM, Kwon S, Rasmussen JC. Emerging lymphatic imaging technologies for mouse and man. J Clin Invest. 2014;124:905–914. doi:10.1172/JCI71612
30. Bell RD, Rahimi H, Kenney HM, et al. Altered lymphatic vessel anatomy and markedly diminished lymph clearance in the rheumatoid hand with active arthritis. Arthritis Rheumatol. 2020;72:1447–1455. doi:10.1002/art.41311
31. Wang H, Chen Y, Li W, et al. Effect of VEGFC on lymph flow and inflammation-induced alveolar bone loss. J Pathol. 2020;251:323–335. doi:10.1002/path.5456
32. Kumar S, Ingle H, Prasad DV, Kumar H. Recognition of bacterial infection by innate immune sensors. Crit Rev Microbiol. 2013;39:229–246. doi:10.3109/1040841X.2012.706249
33. Wiersinga WJ, Leopold SJ, Cranendonk DR, van der Poll T. Host innate immune responses to sepsis. Virulence. 2014;5:36–44.
34. Fullerton JN, Gilroy DW. Resolution of inflammation: a new therapeutic frontier. Nat Rev Drug Discov. 2016;15:551–567.
35. Zhang JL, Zhuo XJ, Lin J, et al. Maresin1 stimulates alveolar fluid clearance through the alveolar epithelial sodium channel Na,K-ATPase via the ALX/PI3K/Nedd4-2 pathway. Lab Invest. 2017;97:543–554.
36. Zhang PH, Han J, Cao F, et al. PCTR1 improves pulmonary edema fluid clearance through activating the sodium channel and lymphatic drainage in lipopolysaccharide-induced ARDS. J Cell Physiol. 2020.
37. Chakraborty S, Zawieja SD, Wang W, et al. Lipopolysaccharide modulates neutrophil recruitment and macrophage polarization on lymphatic vessels and impairs lymphatic function in rat mesentery. Am J Physiol Heart Circ Physiol. 2015;309:H2042–2057. doi:10.1152/ajpheart.00467.2015
38. Kim KE, Koh YJ, Jeon BH, et al. Role of CD11b+ macrophages in intraperitoneal lipopolysaccharide-induced aberrant lymphangiogenesis and lymphatic function in the diaphragm. Am J Pathol. 2009;175:1733–1745. doi:10.2353/ajpath.2009.090133
39. Singh S, Evans TW. Organ dysfunction during sepsis. Intensive Care Med. 2006;32:349–360. doi:10.1007/s00134-005-0038-9
40. Reed HO, Wang L, Sonett J, et al. Lymphatic impairment leads to pulmonary tertiary lymphoid organ formation and alveolar damage. J Clin Invest. 2019;129:2514–2526. doi:10.1172/JCI125044
41. Bayston KF, Cohen J. Bacterial endotoxin and current concepts in the diagnosis and treatment of endotoxaemia. J Med Microbiol. 1990;31:73–83. doi:10.1099/00222615-31-2-73
42. Voiriot G, Contou D, Tran Van Nhieu J, et al. Middle age exacerbates acute respiratory distress syndrome in a double hit murine model. Exp Gerontol. 2017;96:146–154. doi:10.1016/j.exger.2017.06.022
43. D’Alessio FR. Mouse models of acute lung injury and ARDS. Methods Mol Biol. 2018;1809:341–350.
44. Dickson K, Lehmann C. Inflammatory response to different toxins in experimental sepsis models. Int J Mol Sci. 2019;20:4341. doi:10.3390/ijms20184341
45. Janssens S, Beyaert R. Role of Toll-like receptors in pathogen recognition. Clin Microbiol Rev. 2003;16:637–646. doi:10.1128/CMR.16.4.637-646.2003
46. Oliveira SDS, Castellon M, Chen J, et al. Inflammation-induced caveolin-1 and BMPRII depletion promotes endothelial dysfunction and TGF-β-driven pulmonary vascular remodeling. Am J Physiol Lung Cell Mol Physiol. 2017;312:L760–l771. doi:10.1152/ajplung.00484.2016
47. Voiriot G, Razazi K, Amsellem V, et al. Interleukin-6 displays lung anti-inflammatory properties and exerts protective hemodynamic effects in a double-hit murine acute lung injury. Respir Res. 2017;18:64. doi:10.1186/s12931-017-0553-6
48. Wang Q, Zheng X, Cheng Y, et al. Resolvin D1 stimulates alveolar fluid clearance through alveolar epithelial sodium channel, Na,K-ATPase via ALX/cAMP/PI3K pathway in lipopolysaccharide-induced acute lung injury. J Immunol. 2014;192:3765–3777. doi:10.4049/jimmunol.1302421
49. Qi W, Li H, Cai XH, et al. Lipoxin A4 activates alveolar epithelial sodium channel gamma via the microRNA-21/PTEN/AKT pathway in lipopolysaccharide-induced inflammatory lung injury. Lab Invest. 2015;95:1258–1268. doi:10.1038/labinvest.2015.109
50. Zhuo XJ, Hao Y, Cao F, et al. Protectin DX increases alveolar fluid clearance in rats with lipopolysaccharide-induced acute lung injury. Exp Mol Med. 2018;50:49. doi:10.1038/s12276-018-0075-4
51. Brun-Buisson C, Doyon F, Carlet J, et al. Incidence, risk factors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study in intensive care units. French ICU Group for Severe Sepsis. JAMA. 1995;274:968–974. doi:10.1001/jama.1995.03530120060042
52. Cai S, Zemans RL, Young SK, Worthen GS, Jeyaseelan S. Myeloid differentiation protein-2-dependent and -independent neutrophil accumulation during Escherichia coli pneumonia. Am J Respir Cell Mol Biol. 2009;40:701–709. doi:10.1165/rcmb.2008-0152OC
53. Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am J Respir Crit Care Med. 1995;151:293–301. doi:10.1164/ajrccm.151.2.7842182
54. Matthay MA, Zemans RL, Zimmerman GA, et al. Acute respiratory distress syndrome. Nat Rev Dis Primers. 2019;5:18.
55. Staub NC. Pulmonary edema. Physiol Rev. 1974;54:678–811. doi:10.1152/physrev.1974.54.3.678
56. Staub NC. Pulmonary edema due to increased microvascular permeability. Annu Rev Med. 1981;32:291–312. doi:10.1146/annurev.me.32.020181.001451
57. Flick MR, Perel A, Staub NC. Leukocytes are required for increased lung microvascular permeability after microembolization in sheep. Circ Res. 1981;48:344–351. doi:10.1161/01.RES.48.3.344
58. Matthay MA, Zimmerman GA. Acute lung injury and the acute respiratory distress syndrome: four decades of inquiry into pathogenesis and rational management. Am J Respir Cell Mol Biol. 2005;33:319–327. doi:10.1165/rcmb.F305
59. Looney MR, Nguyen JX, Hu Y, Van Ziffle JA, Lowell CA, Matthay MA. Platelet depletion and aspirin treatment protect mice in a two-event model of transfusion-related acute lung injury. J Clin Invest. 2009;119:3450–3461.
60. Wiener-Kronish JP, Albertine KH, Matthay MA. Differential responses of the endothelial and epithelial barriers of the lung in sheep to Escherichia coli endotoxin. J Clin Invest. 1991;88:864–875. doi:10.1172/JCI115388
61. Martin TR, Pistorese BP, Chi EY, Goodman RB, Matthay MA. Effects of leukotriene B4 in the human lung. Recruitment of neutrophils into the alveolar spaces without a change in protein permeability. J Clin Invest. 1989;84:1609–1619. doi:10.1172/JCI114338
62. Stump B, Cui Y, Kidambi P, Lamattina AM, El-Chemaly S. Lymphatic changes in respiratory diseases: more than just remodeling of the lung? Am J Respir Cell Mol Biol. 2017;57:272–279. doi:10.1165/rcmb.2016-0290TR
63. Hong YK, Shin JW, Detmar M. Development of the lymphatic vascular system: a mystery unravels. Dev Dyn. 2004;231:462–473. doi:10.1002/dvdy.20179
64. Schraufnagel DE. Lung lymphatic anatomy and correlates. Pathophysiology. 2010;17:337–343. doi:10.1016/j.pathophys.2009.10.008
65. Outtz Reed H, Wang L, Kahn ML, Hancock WW. Donor-host Lymphatic Anastomosis After Murine Lung Transplantation. Transplantation. 2020;104:511–515. doi:10.1097/TP.0000000000003041
66. Matthay MA, Folkesson HG, Clerici C. Lung epithelial fluid transport and the resolution of pulmonary edema. Physiol Rev. 2002;82:569–600. doi:10.1152/physrev.00003.2002
67. Folkesson HG, Matthay MA. Alveolar epithelial ion and fluid transport: recent progress. Am J Respir Cell Mol Biol. 2006;35:10–19. doi:10.1165/rcmb.2006-0080SF
68. Arokiasamy S, King R, Boulaghrasse H, et al. Heparanase-dependent remodeling of initial lymphatic glycocalyx regulates tissue-fluid drainage during acute inflammation in vivo. Front Immunol. 2019;10:2316. doi:10.3389/fimmu.2019.02316
69. Colby JK, Abdulnour RE, Sham HP, et al. Resolvin D3 and aspirin-triggered resolvin D3 are protective for injured epithelia. Am J Pathol. 2016;186:1801–1813. doi:10.1016/j.ajpath.2016.03.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.