")
Back to Journals » International Medical Case Reports Journal » Volume 9
Lyme disease caused by Borrelia burgdorferi with two homeologous 16S rRNA genes: a case report
Authors Lee SH
Received 5 November 2015
Accepted for publication 28 January 2016
Published 21 April 2016 Volume 2016:9 Pages 101—106
DOI https://doi.org/10.2147/IMCRJ.S99936
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ronald Prineas
Sin Hang Lee,1,2
1Pathology Department, Milford Hospital, Milford, CT, USA; 2Milford Molecular Diagnostics, Milford, CT, USA
Abstract: Lyme disease (LD), the most common tick-borne disease in North America, is believed to be caused exclusively by Borrelia burgdorferi sensu stricto and is usually diagnosed by clinical evaluation and serologic assays. As reported previously in a peer-reviewed article, a 13-year-old boy living in the Northeast of the USA was initially diagnosed with LD based on evaluation of his clinical presentations and on serologic test results. The patient was treated with a course of oral doxycycline for 28 days, and the symptoms resolved. A year later, the boy developed a series of unusual symptoms and did not attend school for 1 year. A LD specialist reviewed the case and found the serologic test band patterns nondiagnostic of LD. The boy was admitted to a psychiatric hospital. After discharge from the psychiatric hospital, a polymerase chain reaction test performed in a winter month when the boy was 16 years old showed a low density of B. burgdorferi sensu lato in the blood of the patient, confirmed by partial 16S rRNA (ribosomal RNA) gene sequencing. Subsequent DNA sequencing analysis presented in this report demonstrated that the spirochete isolate was a novel strain of B. burgdorferi with two homeologous 16S rRNA genes, which has never been reported in the world literature. This case report shows that direct DNA sequencing is a valuable tool for reliable molecular diagnosis of Lyme and related borrelioses, as well as for studies of the diversity of the causative agents of LD because LD patients infected by a rare or novel borrelial variant may produce an antibody pattern that can be different from the pattern characteristic of an infection caused by a typical B. burgdorferi sensu stricto strain.
Keywords: Lyme disease, Borrelia burgdorferi, homeologous 16S rRNA genes, DNA sequencing
Introduction
Lyme disease (LD) is believed to be caused exclusively by Borrelia burgdorferi sensu stricto in North America.1 Its diagnosis is primarily based on signs and symptoms, as well as a history of possible exposure to infected blacklegged ticks.2 The two-tiered serology test, namely, a positive enzyme-linked immunosorbent assay (ELISA) test followed by a positive immunoglobulin (Ig) M or IgG Western blot, is a recommended laboratory test.3 An IgM immunoblot is considered positive if two of the following three bands are present: 24 kDa (OspC), 39 kDa (BmpA), and 41 kDa (Fla). It is further recommended that an IgG immunoblot be considered positive if five of the following ten bands are present: 18 kDa, 21 kDa (OspC), 28 kDa, 30 kDa, 39 kDa (BmpA), 41 kDa (Fla), 45 kDa, 58 kDa (not GroEL), 66 kDa, and 93 kDa.4 However, in early LD, when the characteristic skin rash, erythema migrans, of the patient is <7 days old, 87% of the ELISA and 74.5% of the immunoblot tests may have a negative, equivocal, or intermediate result.5 The two-tiered serology test has been the subject of debate when it is relied upon for making the diagnosis of LD for patient management.6,7 A single-tier C6 peptide ELISA test apparently increases the detection sensitivity, but with decreased specificity.8 Recently, strains of Borrelia other than B. burgdorferi sensu stricto have been identified in some patients in the USA, with clinical manifestations of LD or symptoms and signs mimicking those observed in LD, using nucleic acid-based testing methods for identification of the causative agents.9–12 This report presents another case in which the patient’s serologic test results were questionable in the diagnosis of LD and the patient’s whole blood was positive for a novel strain of B. burgdorferi, confirmed by direct DNA sequencing. This case report also shows the need for wide implementation of the DNA sequencing technology in hospital laboratories located in LD-endemic areas for timely accurate diagnosis and appropriate treatment of LD patients, in addition to studying the diversity of the causative agents of Lyme and related borrelioses.
Case presentation
A 16-year-old boy living in the northeast state of Massachusetts (MA), USA, had flu-like symptoms in a summer at the age of 13 years and developed bilateral knee swelling in the following winter. A serology test was performed and interpreted as being positive for LD at that time. The patient was treated with a course of oral doxycycline for 28 days, and the arthritis resolved. Approximately 12 months after that treatment, the patient started to complain of periodic sweating, flushing, severe fatigue, migratory joint pains, nausea, stomach pain, insomnia, and blurry vision and had a skin rash that was described by a clinician as “typical Bartonella rash”. As the result of these symptoms, the patient did not attend school for 1 year. Finally, the patient was seen by a LD consultant who interpreted the ELISA serology test to be positive, but the Western blot test to be negative because the IgM blot was totally negative and in the IgG blot, only four bands were accepted as positive. Based on the consultant’s opinion, the patient was hospitalized for pure psychiatric disorders at a psychiatric hospital for 7 weeks. In the following winter month at the age of 16 years, a newly performed C6 peptide serology test showed that the patient had a positive C6 peptide Borrelia burgdorferi IgG/IgM Lyme Index of 3.46 (normal range: <0.91). A venous blood sample was tested by DNA sequencing for low-density spirochetemia at the Milford Hospital-affiliated molecular diagnostic laboratory (now Milford Molecular Diagnostics Laboratory). A brief history of this case with a typographic error, which stated that the consultant found five bands instead of four bands in the IgG immunoblots, was published under case 3 in Table 2 in a previous report.12 Publication of laboratory data with blinded patient identities was approved by the Milford Hospital Institutional Review Board as an ongoing research project.
The history presented in this report is the corrected version provided by the treating physician coauthor of the previous paper.12 This report records a subsequent significant laboratory finding on one of many cases previously published within a table in a peer-reviewed article,11 with the treating physician of the patient, as the coauthor. The consent from the legal guardian of the patient to publish the information on this case was obtained by the treating physician coauthor prior to publication of the previous article. The clinical history presented in this report is a replica of the history of case 3 in Table 2 of the previous article11 with a minor, but significant, correction.
Because of the unusual DNA sequence with numerous unresolved base-calling regions in the electropherogram of this case, the polymerase chain reaction (PCR) amplicons were resequenced with optimized Sanger reactions. Same-nested PCR amplification with a pair of borrelial genus-specific primers, followed by direct Sanger sequencing of the nested PCR amplicon using the M2 primer as the sequencing primer,11,12 confirmed that there were two partially homologous Borrelia burgdorferi 16S rRNA (ribosomal RNA) gene sequences in the sample isolated from the patient’s blood. Visual analysis of a 210-base DNA sequence revealed a 110-base unambiguous sequence followed by an immediately downstream 100-base ambiguous segment. The ambiguous DNA sequence is obviously caused by a shift in the reading frame (Figure 1).
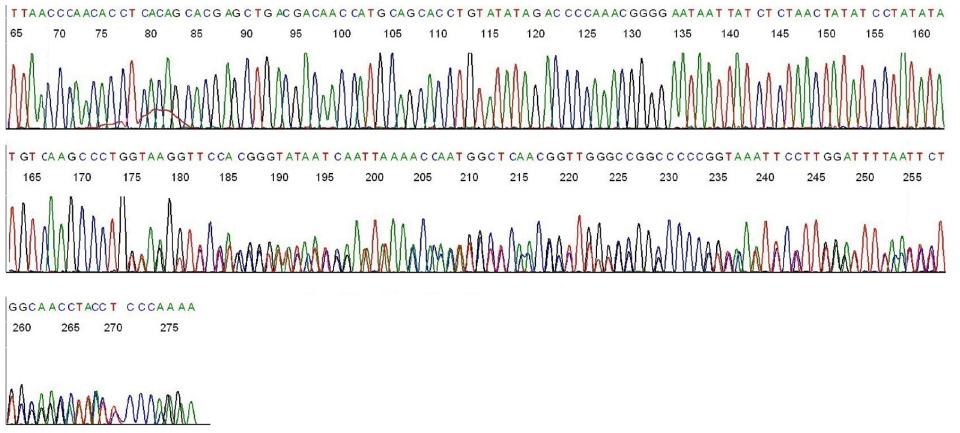 | Figure 1 Base-calling electropherogram of borrelial 16S rRNA gene sequencing, using M2 as the sequencing primer. |
Basic Local Alignment Search Tool (BLAST) algorithm showed that the first unambiguous 110 bases, namely, TTAACCCAACACCTCACAGCACGAGCTGACGACAACCATGCAGCACCTGTATATAGACCCCAAACGGGGAATAATTATCTCTAACTATATCCTATATATGTCAAGCCCTG, represent a signature sequence of the B. burgdorferi sensu lato 16S rRNA gene (GenBank sequence ID CP009656; range: 445,000–445,109). Visual analysis showed that the immediately downstream 100-base segment with numerous double peaks is a composite of two superimposed sequences, shown as follows:
- GTAAGGTTCCTCGCGTATCATCGAATTAAACCACATGCTCCACCGCTTGTGCGGGCCCCCGTCAATTCCTTTGAGTTTCACTCTTGCGAGCATACTCCCC; and
- TAAGGTTCCTAGCGTATCATCGAATTAAACCACATTCTCCACCGCTTGTGGGGGCCCCCGTCAATTCCTTTGAGTTTCACTCTTGCGAGCATACTCCCCA.
Submission of the 100-base sequence A for BLAST alignment algorithm confirmed that this is an immediately downstream continuation of a B. burgdorferi sensu lato 16S rRNA gene sequence, with ID CP009656, range: 445, 110–445,209, with a 100% ID match.
BLAST alignment algorithm of the 100-base sequence B showed no 100% ID match with any sequences cataloged in the GenBank. Due to deletion of a single “G” base at the position equivalent to 445,110 of the B. burgdorferi 16S rRNA gene sequence ID CP009656, there is a shift in the reading frame in Figure 1, caused by a sequence B superimposed on a sequence A. Based on known sequences retrieved from the National Center for Biotechnology Information database, sequence B has a maximum 97% ID match with a highly conserved 16S rRNA gene segment commonly shared by numerous spirochete species, including B. burgdorferi (ID CP009656, range: 445,111–445,210), B. turicatae (ID KP861623, range: 237–336), B. afzelii (ID CP009058, range: 447,714–447,813), B. hermsii (ID CP011060, range: 447,836–447,935), and Treponema pallidum (ID CP007548, range: 232,098–232,197). One of these examples was copied from the BLAST report returned from the GenBank and is illustrated in Figure 2.
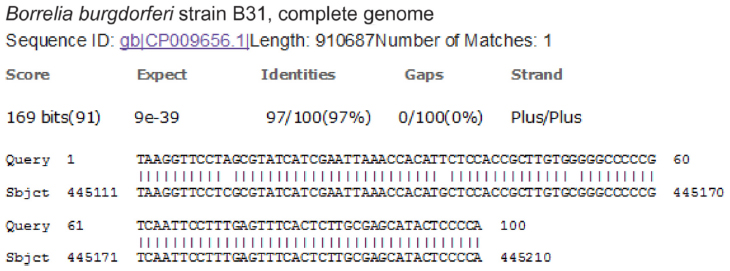 | Figure 2 BLAST alignment report showing sequence B in the search query with a maximum 97% ID match with a common spirochete 16S rRNA gene sequence cataloged in the GenBank. |
BLAST alignment analysis of the 210-base sequence composed of the 110-base unambiguous sequence and the 100-base sequence A confirmed that this 210-base sequence represents a B. burgdorferi sensu lato 16S rRNA gene region with a 100% ID match from position 445,000 to position 445,209 (GenBank sequence ID: CP009656.1).
However, alignment of the 210-base sequence composed of the 110-base unambiguous sequence and the 100-base sequence B against the sequence ID CP009656.1 showed deletion of one “G” nucleotide at reference position 445,110 and three single-base substitutions: one C→A at reference position 445,121; one G→T at position 445,146; and one C→G at position 445,161 (Figure 2). When sequencing from the homologous end of the PCR amplicon, the deletion of one “G” base and three single-base substitutions in this segment caused initial analytical difficulty due to a reading frame shift. A search of the nucleotide sequence database in the GenBank failed to find a 16S rRNA gene sequence having a 100% ID match with sequence B. Attempts to sequence from the opposite end resulted in total failures.
Based on the 110-base unambiguous 16S rRNA gene sequence, the blood sample of this patient was diagnosed as being positive for a strain of B. burgdorferi sensu lato.
PCR-based molecular diagnoses of B. burgdorferi infection are often criticized because of possible DNA cross-contamination in the laboratory. In the author’s laboratory, the positive control is a strain of B. coriaceae whose target 16S rRNA gene DNA can be amplified with the genus-specific M1/M2 primers, but its interprimer DNA sequence is different from the pathogenic borrelial species.11 Because all positive PCR products generated in this laboratory are validated with Sanger sequencing and because the sample in this case was proven to contain two partially homologous 16S rRNA gene sequences that never existed in the environment, the positive results found in this case could not have been due to laboratory DNA contamination. After the molecular diagnosis was made, the patient was referred to the infectious disease unit of a large medical center for further treatment. Clinical follow-up was not available.
Permission to publish the data included in this paper without patient identity was granted to the author by the Institutional Review Board (IRB) of Milford Hospital. A special ethical approval was not required by, and was not sought from, the IRB of Milford Hospital prior to the work included in the current report because the subsequent work revealing new information after the publication of the first article only consisted of computer and visual analysis of the DNA sequencing electropherograms generated and used to support the molecular diagnosis of infection by a B. burgdorferi sensu lato strain already reported in the first publication
Discussion
When pure cultures grown in liquid media are used as the study materials, B. burgdorferi sensu stricto is shown to have only one copy of 16S rRNA gene in the chromosome.13 Among the members of the B. burgdorferi sensu lato complex, B. afzelii and B. garinii, the two other B. burgdorferi sensu lato species found only in Europe and Asia, may contain two copies of 16S rRNA genes, which are heterogeneous.14 When there is a second 16S rRNA gene sequence found in a pure culture that does not match with a 16S rRNA gene sequence known to exist in another borrelial strain, the second copy of the two 16S rRNA genes is usually considered to be “nonfunctional” rather than as evidence of a novel strain or a mutant of Borrelia in the culture.14
Because 16S rRNA genes are highly conserved and because the sequence B as demonstrated in the current isolate with one-base deletion and three-base substitutions within a 100-base region is significantly different from a highly conserved 16S rRNA gene segment that is commonly shared by numerous spirochetes, including B. burgdorferi, B. turicatae, B. afzelii, B. hermsii, and T. pallidum, the finding of these two partially homologous 16S rRNA genes in the current case is interpreted as evidence for the presence of one isolate of B. burgdorferi with two homeologous 16S rRNA genes, rather than a mixed infection of a wild-type clone of B. burgdorferi and a novel B. burgdorferi mutant. Nonetheless, mixed borrelial infection by two species of Borreliae, ie, a B. burgdorferi sensu lato and a B. miyamotoi in one blood sample has been previously reported.12 Single-nucleotide mutations in the 16S rRNA gene of B. burgdorferi are only rarely observed, eg, in experiments in the in vitro setting when the spirochetes develop resistance to aminoglycoside and spectinomycin.15 A B. burgdorferi mutant with one base deletion and three base substitutions in a highly conserved 100-base region of the 16S rRNA gene has not been reported in the literature. Therefore, the isolate detected in the blood sample of this case is interpreted as a B. burgdorferi with two homeologous 16S rRNA genes. However, the final confirmation of such a biological entity depends on securing a pure culture of the spirochete and performance of a full chromosome sequencing if the organism can be grown in an artificial medium.
The author of this case report focuses on DNA sequencing diagnosis of Lyme borreliosis and has no access to the serology test results of this patient. According to the primary care physician of the patient, there was only one set of ELISA and Western blot tests. The IgM Western blot was consistently interpreted as negative. But the IgG Western blot was apparently questionable, initially interpreted as positive by the testing laboratory, but subsequently reinterpreted by a LD expert as negative because only four bands instead of five were accepted as positive. In real life, different interpretations by different observers of a weak band with a borderline intensity in Western blots are not uncommon. Such a questionable serologic test pattern may be consistent with a LD infection caused by a variant strain other than the “prototype” B. burgdorferi sensu stricto. A variant strain of B. burgdorferi with two homeologous 16S rRNA genes may have other biological characteristics, including a different set of epitopes, which might have contributed to the atypical immunoblot serologic test results in this case.
Because the DNA sequences of the 16S rRNA gene of all bacterial species contain their respective unique hypervariable regions, a pair of 21-base species-specific LD PCR primers has been used to amplify a unique 351 bp segment of the B. burgdorferi sensu lato 16S rRNA gene for DNA sequencing-based molecular diagnosis of LD.16 Shifting the species-specific LD primers upstream for three nucleotides on both ends of the target DNA created a pair of “genus-specific” M1/M2 primers, which can amplify a highly conserved 357 bp segment of the 16S rRNA gene of all species of the B. burgdorferi sensu lato complex and the corresponding 358 bp segment of the 16S rRNA gene of the heterogeneous relapsing fever borreliae, including B. miyamotoi.11,12 After implementation of this DNA-sequencing protocol in a molecular diagnostic laboratory, a novel Borrelia (GenBank Seq ID KM052618) was identified in an archived serum sample of a treated patient with neurologic LD.11 A strain of B. burgdorferi and a strain of B. miyamotoi were found as coinfecting organisms in a single blood sample of a LD patient by direct DNA sequencing.12 This case report adds further evidence that there is a great strain diversity in the borreliae causing Lyme and related borrelioses in the USA, which warrants further exploration.
Conclusion
DNA-sequencing technology is a highly specific tool in the molecular diagnosis of the causative agents of Lyme borreliosis. Using a pair of genus-specific PCR primers to perform same-nested PCR for amplification of the borrelial 16S rRNA gene, followed by direct Sanger sequencing of the PCR amplicon, can detect and validate a wide range of Borrelia species, including novel Borrelia strains causing Lyme and related borrelioses. Direct DNA sequencing should be implemented in hospital laboratories in LD-endemic areas for early reliable diagnosis of this infectious disease and for further studies of the diversity of the causative agents of Lyme borreliosis.
Acknowledgments
The author thanks Ms Veronica Vigliotti and Ms Jessica Vigliotti who performed all the PCR and DNA sequencing technical work for this case study. This work was presented as a poster at the meeting of the American Association for Clinical Chemistry, held at Atlanta, GA, USA, on July 29, 2015.
Disclosure
The author is currently Director of Milford Molecular Diagnostics Laboratory, Milford, CT, USA, and is specialized in developing DNA sequencing-based diagnostic tests for community hospital laboratories. This work was performed when he was employed as a pathologist at Milford Hospital. As one peer reviewer emphasized, if DNA sequencing is generally adopted by community hospital laboratories for the accurate and timely diagnosis of LD at an early stage of its infection, the author may stand to benefit financially. The author reports no other conflicts of interest in this work.
References
Feder HM Jr, Johnson BJ, O’Connell S, et al; Ad Hoc International Lyme Disease Group. A critical appraisal of “chronic Lyme disease”. N Engl J Med. 2007;357:1422–1430. | |
Centers for Disease Control and Prevention [webpage on the Internet]. Lyme Disease. Available from: http://www.cdc.gov/lyme/. Accessed February 1, 2016. | |
CDC [webpage on the Internet]. Lyme Disease. Available from: http://www.cdc.gov/lyme/healthcare/clinician_twotier.html. Accessed February 1, 2016. | |
Centers for Disease Control and Prevention [webpage on the Internet]. Recommendations for Test Performance and Interpretation from the Second National Conference on Serologic Diagnosis of Lyme Disease. Available from: http://www.cdc.gov/mmwr/preview/mmwrhtml/00038469.htm. Accessed February 1, 2016. | |
Aguero-Rosenfeld ME, Nowakowski J, McKenna DF, Carbonaro CA, Wormser GP. Serodiagnosis in early Lyme disease. J Clin Microbiol. 1993;31:3090–3095. | |
Steere AC, Taylor E, McHugh GL, Logigian EL. The overdiagnosis of Lyme disease. JAMA. 1993;269:1812–1816. | |
Stricker RB, Johnson L. Lyme wars: let’s tackle the testing. BMJ. 2007;335:1008. | |
Wormser GP, Schriefer M, Aguero-Rosenfeld ME, et al. Single-tier testing with the C6 peptide ELISA kit compared with two-tier testing for Lyme disease. Diagn Microbiol Infect Dis. 2013;75:9–15. | |
Gugliotta JL, Goethert HK, Berardi VP, Telford SR III. Meningoencephalitis from Borrelia miyamotoi in an immunocompromised patient. N Engl J Med. 2013;368:240–245. | |
Chowdri HR, Gugliotta JL, Berardi VP, et al. Borrelia miyamotoi infection presenting as human granulocytic anaplasmosis: a case report. Ann Intern Med. 2013;159:21–27. | |
Lee SH, Vigliotti JS, Vigliotti VS, Jones W, Shearer DM. Detection of borreliae in archived sera from patients with clinically suspect Lyme disease. Int J Mol Sci. 2014;15:4284–4298. | |
Lee SH, Vigliotti JS, Vigliotti VS, Jones W, Moorcroft TA, Lantsman K. DNA sequencing diagnosis of off-season spirochetemia with low bacterial density in Borrelia burgdorferi and Borrelia miyamotoi infections. Int J Mol Sci. 2014;15:11364–11386. | |
Schwartz JJ, Gazumyan A, Schwartz I. rRNA gene organization in the Lyme disease spirochete, Borrelia burgdorferi. J Bacteriol. 1992;174:3757–3765. | |
Schüler W, Bunikis I, Weber-Lehman J, et al. Complete genome sequence of Borrelia afzelii K78 and comparative genome analysis. PLoS One. 2015;10:e0120548. | |
Criswell D, Tobiason VL, Lodmell JS, Samuels DS. Mutations conferring aminoglycoside and spectinomycin resistance in Borrelia burgdorferi. Antimicrob Agents Chemother. 2006;50:445–452. | |
Lee SH, Vigliotti VS, Vigliotti JS, Jones W, Williams J, Walshon J. Early Lyme disease with spirochetemia – diagnosed by DNA sequencing. BMC Res Notes. 2010;3:273. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.