Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Lung Function and Health Status in Individuals with Severe Alpha-1-Antitrypsin Deficiency at the Age of 42
Authors Schramm GR ![]() , Mostafavi B, Piitulainen E, Wollmer P, Tanash HA
, Mostafavi B, Piitulainen E, Wollmer P, Tanash HA
Received 4 September 2021
Accepted for publication 14 November 2021
Published 23 December 2021 Volume 2021:16 Pages 3477—3485
DOI https://doi.org/10.2147/COPD.S335683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Georg Rüdiger Schramm,1 Behrouz Mostafavi,1 Eeva Piitulainen,1 Per Wollmer,2 Hanan A Tanash1
1Department of Respiratory Medicine and Allergology, Skåne University Hospital, Lund University, Malmö, Sweden; 2Department of Medical Imaging and Physiology, Skåne University Hospital, Lund University, Malmö, Sweden
Correspondence: Georg Rüdiger Schramm
Department of Respiratory Medicine and Allergology, Skåne University Hospital, Jan Waldenströms Gata 24, Malmö, S – 205 02, Sweden
Tel +46 40 33 25 85
Fax +46 40 33 74 90
Email [email protected]
Background: Severe hereditary alpha-1-antitrypsin deficiency (AATD) is a known risk factor for the early development of pulmonary emphysema and COPD, especially in smokers. By the Swedish national screening programme carried out from 1972 to 1974, a cohort of individuals with severe (PiZZ) AATD was identified and has been followed up regularly. The aim of this study was to investigate health status, quality of life and lung function in this cohort at the age of 42 years compared with an age-matched control group randomly selected from the population registry.
Methods: All study participants answered a questionnaire on smoking habits, symptoms, occupation, exposure to airway irritants and quality of life using Saint George’s Respiratory Questionnaire (SGRQ). They underwent complete pulmonary function tests (PFT) and forced oscillation technique (FOT) for the measurement of airway resistance and reactance. Blood samples were taken for allergies and IgG-subclasses as an indicator of increased risk of airway infections.
Results: The residual volume (RV), total lung capacity (TLC) and RV/TLC ratio were significantly higher in the PiZZ ever-smokers compared to the PiMM ever-smokers and PiZZ never-smokers (p < 0.05). The resistance in the upper, small and total airways was significantly lower in PiZZ subjects compared to PiMM subjects (p < 0.05). A greater proportion of PiZZ never-smokers had an FEV1/VC ratio < 0.7 than PiMM never-smokers (p = 0.043). PiZZ subjects with occupational exposure to airway irritants showed a significantly lower FEV1, VC and higher RV/TLC ratio than PiMM individuals with exposure (p < 0.05).
Conclusion: At the age of 42, ever-smoking PiZZ individuals have signs of COPD, and also PiZZ never-smokers have early, physiological signs of emphysema.
Keywords: alpha-1-antitrypsin deficiency, COPD, lung function, quality of life
Introduction
Severe alpha-1-antitrypsin (AAT) deficiency (PiZZ) is a relatively rare genetic disorder characterised by reduced serum levels of AAT. This genetic defect results in the polymerisation of the AAT molecules in the hepatocytes leading to the accumulation of the Z protein within the hepatocytes and a decreased release into the circulation. In individuals with normal AAT alleles (PiMM), circulating AAT is distributed to the lungs to serve a protective function against elastases, particularly neutrophil elastase (NE), that destroys the protein elastin in the lung parenchyma.1 Individuals with severe AATD (PiZZ) have an increased risk of early development of pulmonary emphysema because of an imbalance between NE and AAT in the lung parenchyma.2
AAT deficiency is caused by a single gene mutation, but there is a great variation in the development of emphysema in individuals with AAT deficiency. Smoking is the most important risk factor for the development of emphysema. However, never-smokers also have an increased risk of developing emphysema, which suggests that there are other risk factors than smoking that affect the variation and manifestation of lung disease in these patients.
Despite the extensive and growing research on AAT deficiency since its discovery in 1963 by Laurell and Eriksson, its natural course is still not well known.
By the Swedish national AAT screening of all 200,000 new-born children over the period from 1972 to 1974, a cohort of 127 PiZZ and 2 PiZnull individuals was identified. The aims of the screening programme were to estimate the prevalence of AATD in the Swedish population, to study the natural course of AATD in relation to external influences such as smoking and exposure to airway irritants, and to gain information on the negative effects of smoking. The prevalence of severe AATD in Sweden was estimated to be 1/1600.3
The cohort has been followed up regularly concerning lung function and health status. Since the age of 30, an age-matched control group, randomly selected from the population registry, has been followed up in order to compare the results between the AAT-deficient individuals and the Swedish general population.4,5 Our results have shown that ever-smoking PiZZ individuals develop signs of COPD already before the age of 40, while PiZZ never-smokers have normal lung function.6
Our aim was to study smoking habits, symptoms, lung function, quality of life, presence of allergy and other diseases in the cohort at the age of 42 years compared to the age-matched control group, randomly selected from the population registry.
Methods
This was a prospective, national, case–control study comparing individuals with severe AATD (PiZZ), identified by neonatal screening, with an age-matched control group randomly selected from the population registry.
The Study Population
All AAT-deficient individuals in the cohort were invited to this follow-up study at the age of 42 years. The same 300 age-matched control subjects, who had been randomly selected from the Swedish population registry, as in the 30-, 34- and 38-year follow-up studies, were invited as a control group.4–6 The check-up of the cohort was performed either at the Department of Respiratory Medicine in Malmö, Sweden, or at the participants’ local hospital. The control subjects visited the Department of Respiratory Medicine, Malmö.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Regional Ethical Review Board of Lund, Sweden. All study participants gave their signed, informed consent.
Questionnaire
A questionnaire was sent to all study participants by regular mail. The following questions were included in the questionnaire: smoking history (yes/no, duration of smoking and number of cigarettes per day), symptoms of coughing with sputum production at least 3 months over 2 consecutive years (ie, chronic bronchitis), wheezing, self-estimated exertion capacity and health status on the VAS (Visual Analogue Scale) of 100 millimetres (0 = no dyspnoea/good general health status and 100 = severe breathlessness/poor general health status), current and former occupation, exposure to airway irritants (yes/no, type and duration of exposure), other diseases, history of pneumonia and (only the AAT-subjects) whether the knowledge received about AATD influenced the decision to stop/not to start smoking. A smoker was defined as any individual who had smoked more than 20 packs of cigarettes during his/her life. Ever-smokers were defined as former smokers or current smokers.
For the estimation of dyspnoea, we also used the Medical Research Council (MRC) scale: score 1 [=breathlessness with strenuous exercise] to 5 [=too breathless to leave home]. The cut-off for significant dyspnoea was MRC ≥3, which is equal to ≥2 on the modified MRC (mMRC) scale that is used in the GOLD criteria for COPD. For the evaluation of quality of life, the study participants answered the Saint George’s Respiratory Questionnaire (SGRQ) [Score 0–100 where high scores indicate poorer quality of life].7
Pulmonary Function Tests
The study participants underwent complete pulmonary function tests (PFT) including dynamic spirometry before and 15 minutes after bronchodilation with terbutaline 1.5 µg, total lung capacity (TLC), residual volume (RV), functional residual capacity (FRC) and CO diffusing capacity (DLCO) (Intramedic Masterscreen®, Sollentuna, Sweden). They also underwent forced oscillation technique (FOT) test, using the impulse oscillometry system (IOS) for the measurement of resistance and reactance.8 Pulmonary function tests were performed either at Skåne University Hospital in Malmö, Sweden, or at the participants’ local hospital.
The results of pulmonary function tests are expressed as percent of the reference values stipulated by the European Community for Steel and Coal. The ratios of forced expiratory volume in one second/vital capacity (FEV1/VC ratios) are presented as absolute values. Post-bronchodilator values are reported except for the FEV1 for which both pre- and post-bronchodilator values are reported.9
Allergy and IgG Sub-Classes
The presence of allergy was analysed by the serological test Phadiatop and total IgE at the Laboratory of Clinical Immunology at Skåne University Hospital, Malmö. The Phadiatop test included specific IgE antibodies of the most common inhaled allergens (dog, cat, horse, dust mite, grass, birch, mugwort, and mould). The results are both qualitative and quantitative. A value for the total IgE of 129 kU/L or higher was considered pathological.10 Measurement of fractional exhaled nitric oxide (FENO) was performed by using NIOX VERO®. To avoid false-low values, the FENO was measured before the pulmonary function tests. A value over 25 ppb was considered as an elevated value.11,12
The serum IgG sub-classes (IgG1, IgG2, IgG3 and IgG4) were analysed by nephelometry (Immage 800®) which is used for the quantitative measurement of antigen–antibody complexes using a laser. The following cut-off values were considered as IgG sub-class deficiency: IgG1 <2.8g/L, IgG2 <1.15g/L, IgG3 <0.24g/L and IgG4 <0.052g/L.13,14
Statistical Analyses
The Statistical Package for the Social Sciences (SPSS), version 25, was used for the statistical analyses. Continuous variables were analysed with the non-parametric Mann–Whitney U-test due to high skewness. Categorical variables are given as frequencies and percentages. The Pearson Chi-square (χ2) test was used to compare categorical variables. A p-value <0.05 was considered as significant.
Results
The Study Population
Prior to the present check-up, seven of the 129 PiZZ subjects had died, five in early childhood and two in adulthood.15 Of the 300 control individuals, five had died after their identification.
Ninety-nine (81%) of the 122 PiZZ individuals and 90 (31%) of the 295 control subjects (PiMM) answered the questionnaire. None of the PiZZ subjects had been treated with AAT replacement therapy. The number of participants, their age and smoking habits are presented in Table 1. The proportion of men was lower in the control group than among the PiZZ subjects. The proportion of smokers and the total tobacco consumption was lower among the individuals with AAT deficiency than among the controls, but the differences did not quite attain statistical significance. None of the AAT-deficient individuals was a current smoker.
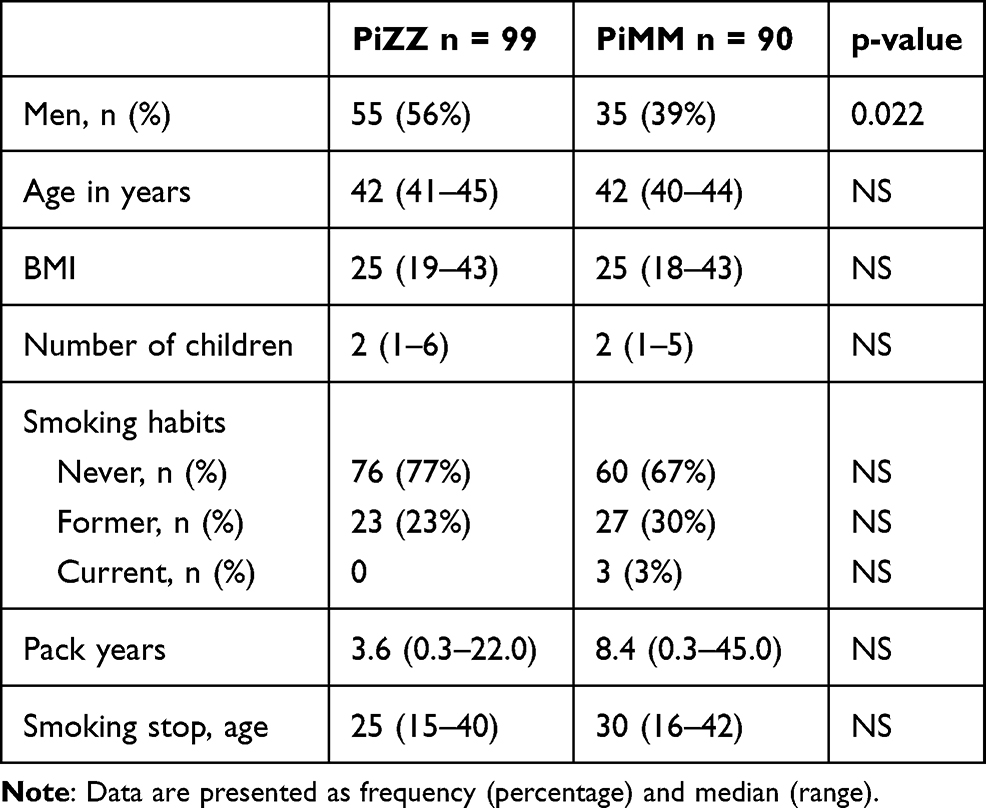 |
Table 1 Demographic Data of Study Population |
Of the 99 PiZZ individuals, 47 (47%) answered the question about the influence of their knowledge of their AATD diagnosis on their smoking habits. Thirty-three of them (70%) stated a positive influence of the early diagnosis of AATD on their lifestyle. Seventeen (94%) of the 18 never-smokers did not start smoking due to their knowledge of AATD and 9 (60%) of the 15 ever-smokers stopped smoking due to this knowledge.
Respiratory Symptoms, Diagnoses and Quality of Life
The presence of respiratory symptoms, diagnoses and quality of life are presented in Table 2. The ever-smoking study participants as a whole had significantly worse general health on the VAS than the never-smoking subjects. Among the ever-smokers as a whole, the proportion of subjects with an MRC score of ≥3 was also significantly higher than among the never-smokers. One (1%) of the PiZZ never-smokers, but none of the never-smoking control subjects had an MRC score of ≥3. Furthermore, the ever-smokers as a whole had a significantly higher, ie, poorer, SGRQ symptom score, impact score and total score than the never-smokers (Table 2).
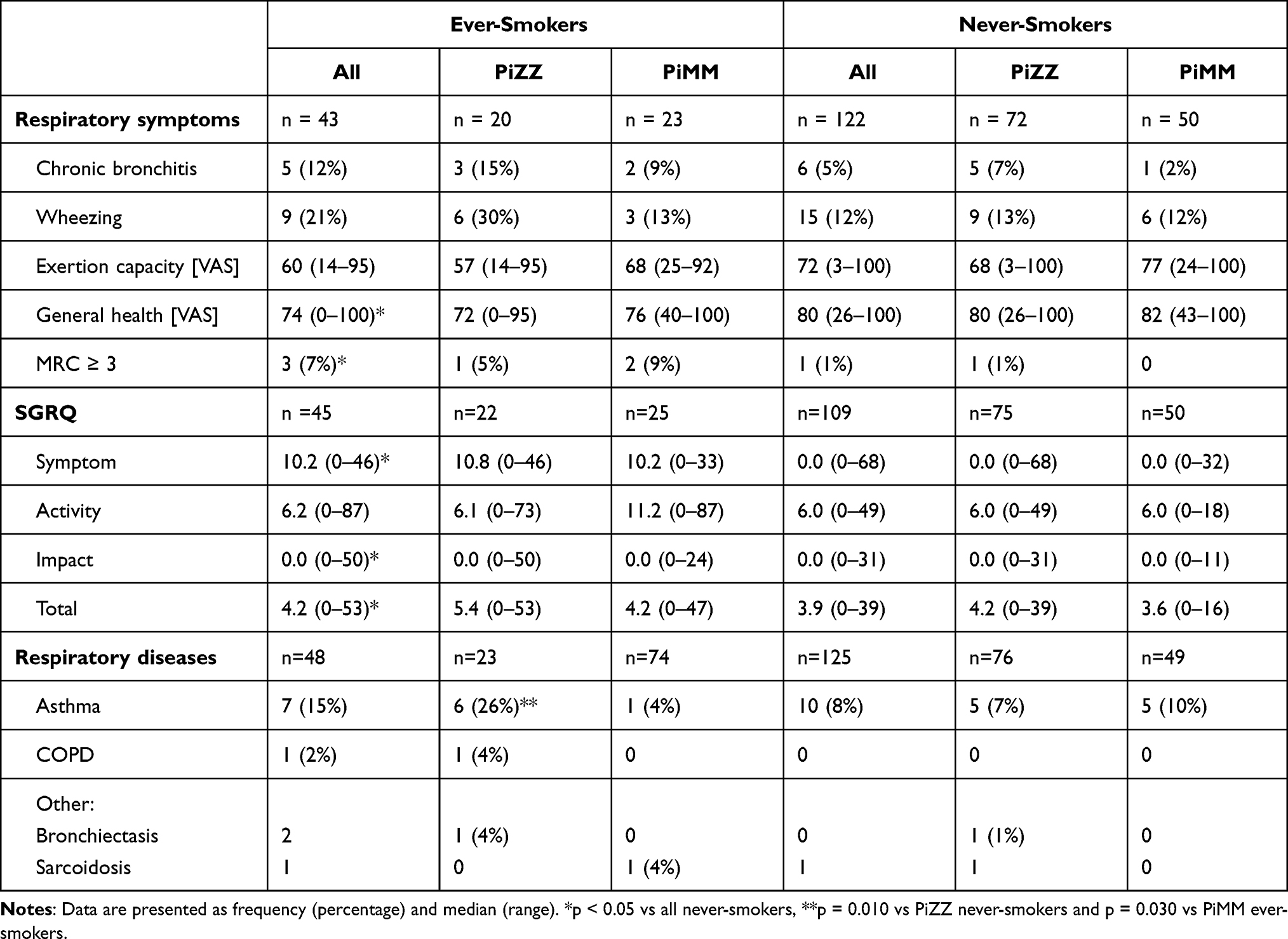 |
Table 2 Respiratory Symptoms, Diagnoses, Health Status and the Results of the Saint George’s Respiratory Questionnaire (SGRQ) in Individuals with Severe Alpha-1-Antitrypsin Deficiency and the Controls Stratified by Smoking Habits |
Asthma was reported by 11 PiZZ subjects (11%) and by 6 PiMM (8%), p = 0.480. Asthma was more common among the PiZZ ever-smokers than among the PiZZ never-smokers and PiMM ever-smokers (Table 2).
Allergic diseases other than asthma (allergic rhinitis, conjunctivitis, eczema, and urticaria) were reported by 10 PiZZ (10%) and 7 (8%) PiMM subjects (p = 0.577). Two of the 80 (3%) PiZZ and 7 (10%) of the 74 PiMM subjects had an elevated IgE-value (p = 0.066). No significant differences were found in other diagnoses of respiratory diseases between the Pi and smoking sub-groups.
The IgG sub-classes were analysed in 84 PiZZ and 74 PiMM individuals. Two (2%) of the PiZZ and 1 (1%) of the PiMM subjects had an IgG1 below the lower reference level (p = 0.636). All other IgG sub-classes were within the normal range. None of the study population had a diagnosis of IgG sub-class deficiency.
Pulmonary Function Tests
The results of pulmonary function tests, diffusion capacity, resistance and reactance in the Pi sub-groups are shown in Table 3. The PiZZ individuals had a significantly higher median RV, FRC and RV/TLC ratio than the PiMM subjects. A significantly higher proportion of the PiZZ subjects than of the PiMM subjects had an FEV1/VC ratio <0.7. The PiZZ subjects had significantly lower median R5Hz, R20Hz and R5Hz-R20Hz when compared with the PiMM subjects (Table 3).
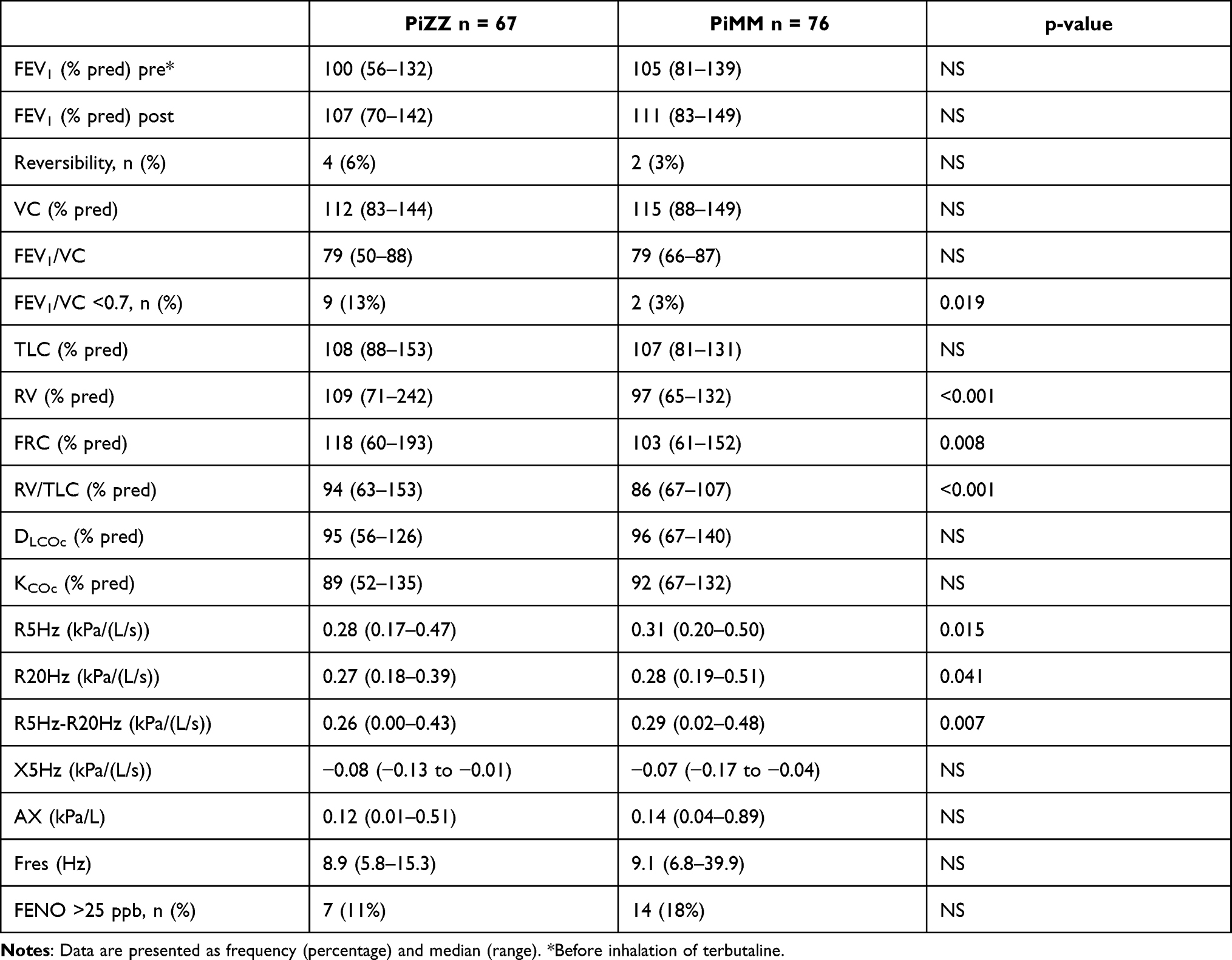 |
Table 3 Results of Lung Function Tests in 67 PiZZ and 76 PiMM Subjects |
Sixty-two PiZZ (63%) and 75 PiMM subjects (83%) underwent assessment of fractionated exhaled nitric oxide (FENO). To avoid false low values, the three PiMM current smokers were excluded from the statistical analyses. The difference in the proportion of subjects with an elevated FENO value, ie, >25 ppb, was not significant.
The results of the pulmonary function tests in the smoking sub-groups are shown in Table 4. The ever-smoking PiZZ subjects had a significantly higher TLC, RV, FRC and TLC/RV ratio than the PiMM ever-smokers. Compared to the PiZZ never-smokers, the PiZZ ever-smokers had significantly higher VC, TLC, RV and FRC. The median FEV1/VC ratio was significantly lower in the PiZZ ever-smokers compared to the PiZZ never-smokers. The proportion of subjects with an FEV1/VC ratio <0.7 was significantly higher among the PiZZ ever-smokers than among the PiZZ never-smokers. Four never-smoking PiZZ (8%) subjects, but none of the never-smoking control subjects had an FEV1/VC ratio <0.7.
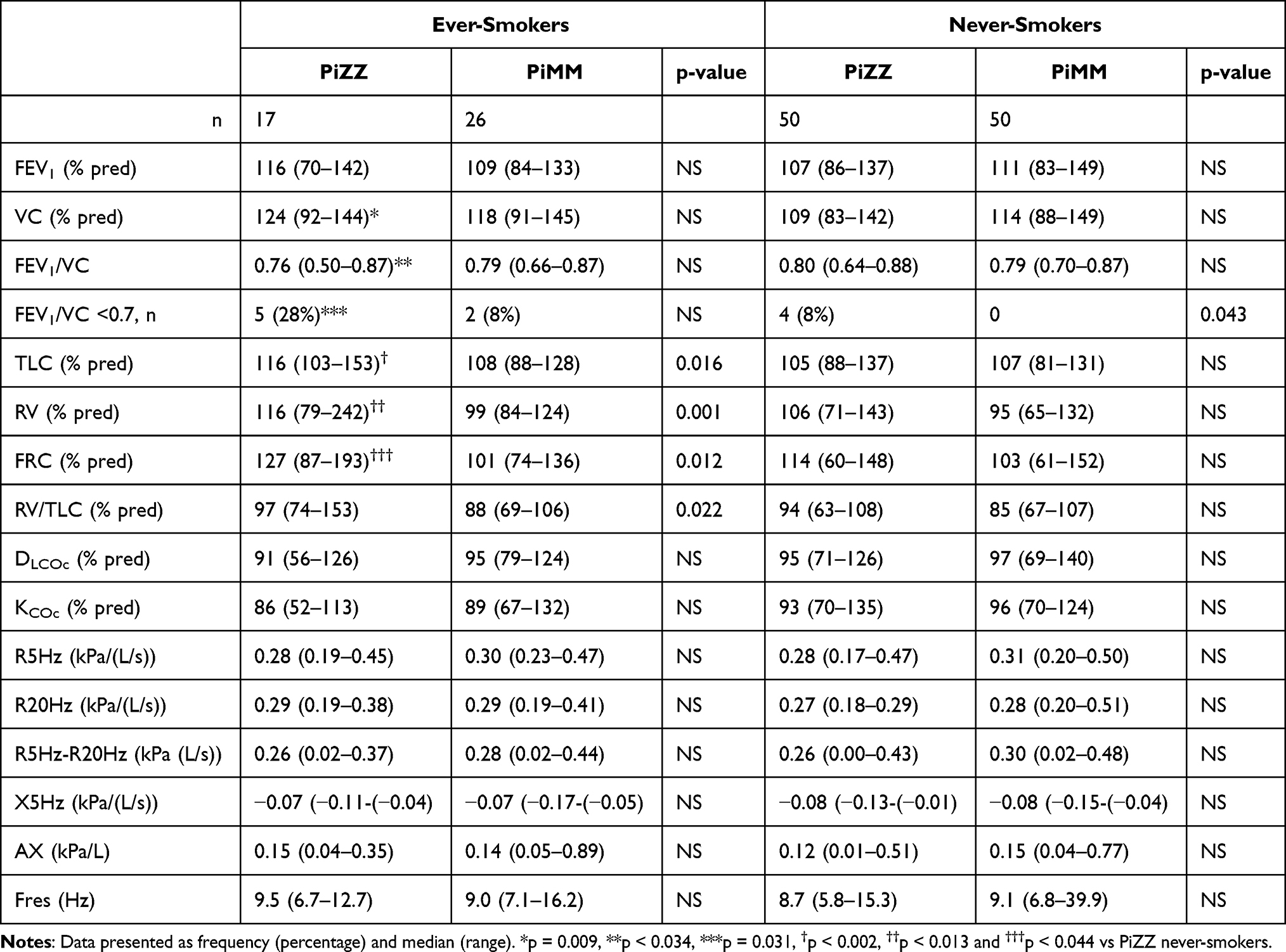 |
Table 4 Results of Lung Function Tests in 67 PiZZ and 76 PiMM Subjects Stratified by Smoking Habits |
Occupational Exposure to Airway Irritants
Ninety-three PiZZ (93%) and 67 PIMM subjects (74%) reported their occupation and whether they had been exposed to airway irritants. Thirty-nine (42%) of the PiZZ and 21 (31%) of the PiMM subjects reported an occupational exposure to airway irritants (p = 0.090). In order to avoid the effect of smoking on symptoms and pulmonary function tests, the ever-smokers were excluded from the analyses of the effect of occupational exposure on lung function and symptoms. The results are shown in Table 5. The median exposure time to airway irritants was lower for the PiZZ individuals than for the controls, but the difference was not statistically significant.
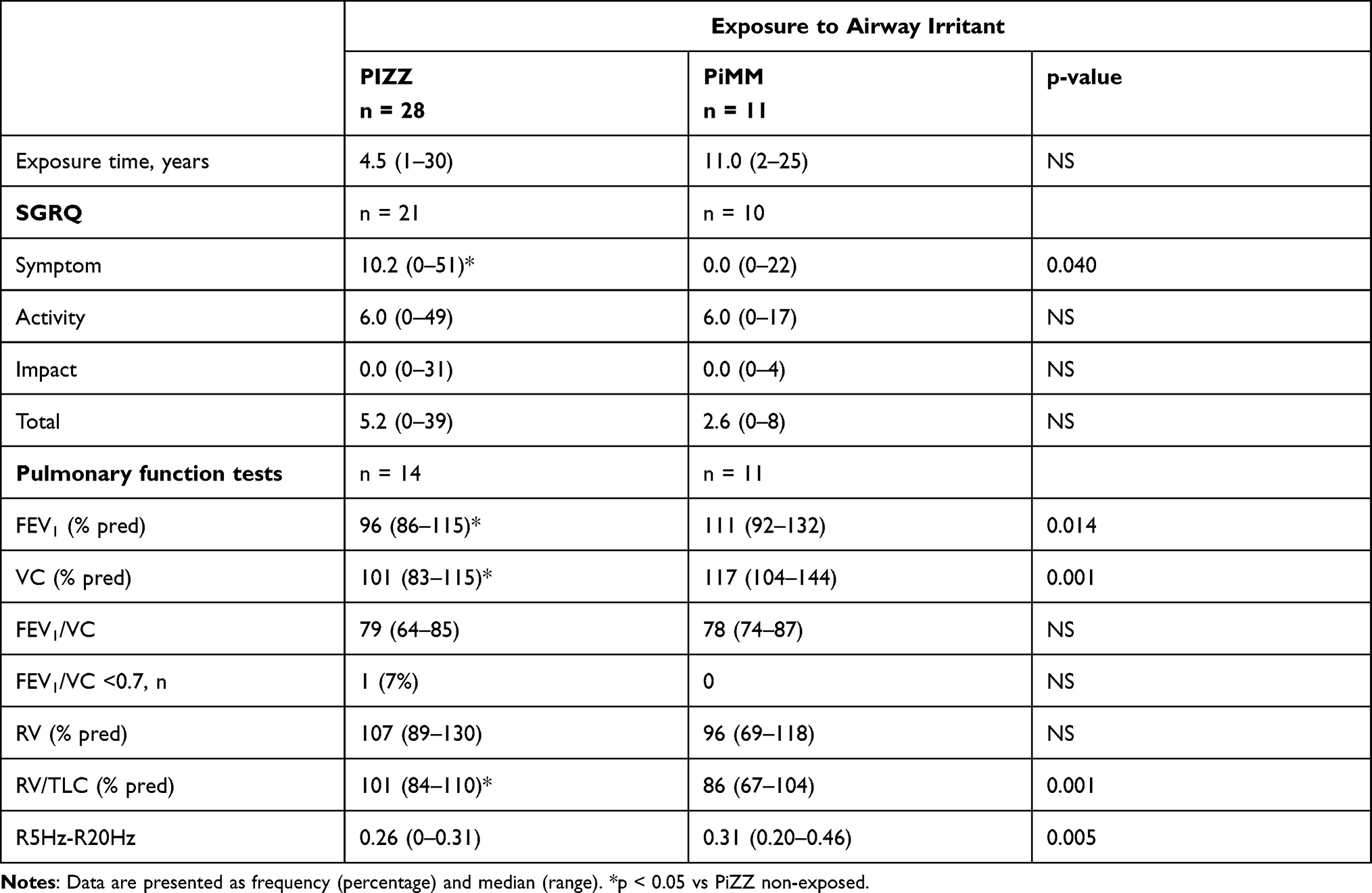 |
Table 5 Results of Quality of Life as Registered in the Saint George’s Respiratory Questionnaire (SGRQ) and Lung Function Tests in Never-Smokers with Occupational Exposure to Airway Irritants |
The following occupations with exposure were reported: dust in the timber industry, passive smoking in pubs, welder smoke, farming and “other”. The never-smoking PiZZ individuals with occupational exposure to airway irritants had a significantly higher SGRQ symptom score, lower FEV1 and VC and a significantly higher RV/TLC ratio compared to the PiMM individuals with occupational exposure (Table 5).
The forty never-smoking PiZZ subjects without exposure to airway irritants had a median (range) SGRQ symptom score of 0.0 (0–68), p = 0.037, vs that of the exposed PiZZ subjects. The PiZZ individuals without occupational exposure had a median (range) % for predicted FEV1 of 109 (87–130) (p = 0.004 vs PiZZ exposed), VC 112 (90–142) (p = 0.004 vs PiZZ exposed) and a median (range) RV/TLC ratio 92 (63–108) (p = 0.006 vs PiZZ exposed).
Other Diseases
There were no significant differences in the occurrence of the following reported diseases between the PiZZ individuals and the controls: depression 6 (6%) PiZZ vs 5 (6%) PiMM and cardiovascular disease (hypertension and congestive heart failure) 2 (2%) PiZZ vs 2 (2%) PiMM. The diagnosis of inflammatory bowel disease (Crohn’s disease, ulcerative colitis/proctitis, and irritable bowel syndrome) was found in four (4%) PiZZ individuals compared with one (1%) of the controls. Rheumatic disease was found in 4 (4%) of the PiZZ subjects compared with 2 (2%) of the controls (fibromyalgia, Bechterew’s disease, and myalgia). Two (2%) PiZZ individuals reported dermatological diseases (rosacea and alopecia), and a further two (2%) PiZZ subjects had neurological disorders (tension headache and epilepsy). One (1%) PiZZ and 4 (4%) PiMM subjects reported endocrinological disease (hypothyreosis and diabetes type II).
Discussion
Our study confirms that, at the age of 42 years, ever-smoking PiZZ individuals, identified by neonatal screening, have significantly higher TLC, RV, FRC and TLC/RV ratio than the PiMM ever-smokers, indicating airway hyperinflation. Also, some never-smoking PiZZ individuals have early physiological signs of emphysema at the age of 42 years. To our knowledge, this is the only study of the natural history of severe AATD in a cohort of individuals identified at birth and followed up regularly.
At the present check-up, a greater proportion of the PiZZ subjects had airflow obstruction with an FEV1/VC ratio <0.7, which is the GOLD spirometric criterion for the diagnosis of COPD, than at the previous check-up at the age of 38 (13% vs 8%). Among the controls, the corresponding figures were 3% vs 1%, respectively.6 Furthermore, we found that eight percent of the PiZZ never-smokers, but none of the PiMM never-smokers had airflow obstruction. At the age of 38, only five percent of the PiZZ never-smokers had airflow obstruction.6 Our previously published register-based study has shown that in PiZZ never-smokers, lung function deteriorates after the age of 50.16 The results of the present check-up indicate that in never-smoking PiZZ individuals the development of COPD may start already before the age of 50.
At the present check-up, forced oscillation technique (FOT) showed that the resistance was significantly lower both at 5Hz, which is often considered reflecting the whole bronchial tree, and between 5 and 20Hz, which is considered representing the small airways. At the age of 38, the PiZZ subjects had significantly lower resistance only at 5 and 20Hz, ie, in the small airways.6 A putative explanation is that emphysema leads to hyperinflation and dilated small airways. In the absence of significant bronchial disease, resistance may then be lower than expected. Usually, the resistance is increased in COPD patients with normal AAT levels. The future follow-up of the cohort will elucidate whether the lower resistance persists in the PiZZ subjects.
A significantly higher proportion of the PiZZ ever-smokers than PiZZ never-smokers reported a diagnosis of asthma. This may be related to the fact that the AAT-deficient individuals in the cohort in general are checked up more often than the controls due to the diagnosis of AATD, which may lead to the diagnosis of asthma. Another possible reason is that individuals with respiratory symptoms at a young age are more often classified as asthmatics rather than as having COPD. Asthma and airway hyper-reactivity have previously been reported in AAT-deficient subjects, especially in young adults, prior to a diagnosis of COPD.17 It is also possible that lack of defence against neutrophil elastase makes their airways susceptible to inflammation. However, we did not find any increased prevalence of allergy nor eosinophil inflammation by using the Phadiatop test, total IgE and FENO in the PiZZ subjects. The fact that many PiZZ subjects have a diagnosis of asthma shows the importance of early identification of AATD for a correct diagnosis.
Occupational exposure to airway irritants is a possible risk factor for the development of pulmonary diseases.18 Among the subjects who reported occupational exposure to airway irritants, we found poorer lung function in the PiZZ subjects than in the controls. They also registered more symptoms in the SGRQ than the controls. Furthermore, they had poorer results in some PFT parameters and symptoms than the non-exposed PiZZ subjects. Thus, already at the age of 42, occupational exposure to airway irritants may have an effect on lung function and symptoms in PiZZ individuals. These results also confirm the importance of early advice to AAT-deficient individuals concerning their choice of occupation. Our group has previously reported, by analysing results of the Swedish AAT deficiency register, that occupational exposure to airway irritants is a risk factor for respiratory symptoms and decreased lung function in severe AAT deficiency.16,19
Respiratory infections causing exacerbations of COPD have a negative effect on the prognosis of COPD.20 IgG sub-class deficiency is a possible risk factor for exacerbations caused by airway infections in PiZZ individuals.13,21 We did not find any differences in the levels of IgG sub-classes between the PiZZ and the control subjects. It is possible that the number of study participants was too low to show differences in IgG sub-classes because of their low prevalence in the Swedish population.
Similar to our previous findings from the age of 30 onwards, the ever-smokers, independent of AAT level, have more respiratory symptoms as assessed by quality of life than the never-smokers.4,5,22 Thus, in all individuals, including those with normal AAT levels, smoking has a negative effect on quality of life and respiratory symptoms at an early age, before any signs of COPD occur in pulmonary function tests.
Strengths
This cohort of individuals with severe AAT deficiency is the only existing, population-based, epidemiological study on the natural course of severe AAT deficiency. After identification at birth, the cohort has been followed up regularly, which makes it possible to study the natural course of this disorder. To our knowledge, no other cohort of individuals with severe AAT deficiency, which has been identified by a national neonatal screening, has been followed up into adulthood. In the Oregon State Public Health Laboratory, 107,000 new-born children were screened between 1971 and 74, and 21 PiZZ individuals were identified. The latest follow-up of these was published at the age of 15.23 Between 1984 and 85, Kempen et al screened about 10,000 new-borns in Limburg, Belgium, and identified 6 PiZZ individuals.24 No long-term follow-up has been published on these six PiZZ subjects.
Another strength of our study is the fact that since the age of 30, the results are compared with the same control group that was randomly selected from the population registry. The Swedish system with an individual personal identification number makes it possible both to know the vital status and to facilitate contact with all the AAT-deficient subjects and controls at each follow-up.
Limitations
Our study also has some limitations, one being that some AAT-deficient subjects and also some control subjects did not participate in the check-up, which leads to a weaker statistical power. Several study parameters showed a high level of skewness. The most common reasons for non-attendance were shortage of time, long distance to travel and no interest/fear of knowledge about one’s health.
Conclusion
Ever-smoking PiZZ individuals have developed COPD at the age of 42 years. Also, some PiZZ never-smokers have early physiological signs of emphysema.
Acknowledgments
The authors thank Åsa Wallander and Anna Brandt for technical and secretarial support.
The authors would like to thank all Swedish colleagues for reporting data. We are also most grateful to Dr Tomas Sveger, who has initiated this screening study, for his support.
Funding
The authors were supported by unrestricted grants from the Swedish Heart-Lung Foundation, the Skåne University Hospital and the Swedish Society of Medicine.
Disclosure
Professor Per Wollmer reports grants from Swedish Heart and Lung Foundation, during the conduct of the study; personal fees from Chiesi Pharma, outside the submitted work. The authors report no other conflicts of interest. The authors alone are responsible for the drafting as well as the content of this study.
References
1. Laurell CB, Eriksson S. The electrophoretic α1-globulin pattern of serum in α1-antitrypsin deficiency. Scand J Clin Lab Invest. 1963;15:132–140.
2. Strnad P, McElvaney NG, Lomas DA, Longo DL. Alpha1-antitrypsin deficiency. N Engl J Med. 2020;382(15):1443–1455. doi:10.1056/NEJMra1910234
3. Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med. 1976;294:1316–1321.
4. Bernspang E, Wollmer P, Sveger T, Piitulainen E. Lung function in 30-year-old alpha-1-antitrypsin-deficient individuals. Respir Med. 2009;103(6):861–865. doi:10.1016/j.rmed.2008.12.021
5. Piitulainen E, Montero LC, Nystedt-Düzakin M, et al. Lung function and CT densitometry in subjects with alpha-1-antitrypsin deficiency and healthy controls at 35 years of age. COPD. 2015;12(2):162–167. doi:10.3109/15412555.2014.922068
6. Mostafavi B, Diaz S, Piitulainen E, et al. Lung function and CT lung densitometry in 37- to 39-year-old individuals with alpha-1-antitrypsin deficiency. Int J Chron Obstruct Pulmon Dis. 2018;13:3689–3698. doi:10.2147/COPD.S167497
7. Ferrer M, Villasante C, Alonso J, et al. Interpretation of quality of life scores from the St George’s respiratory questionnaire. Eur Respir J. 2002;19(3):405–413. doi:10.1183/09031936.02.00213202
8. Oostveen E, MacLeod D, Lorino H, et al. The forced oscillation technique in clinical practice: methodology, recommendations and future developments. Eur Respir J. 2003;22(6):1026–1041. doi:10.1183/09031936.03.00089403
9. Quanjer P, Tammeling GJ, Cotes J, et al. Lung volumes and forced ventilatory flows. Report working party standardization of lung function tests, European Community for Steel and Coal. Official statement of the European Respiratory Society. Eur Respir J Suppl. 1993;16:5–40. doi:10.1183/09041950.005s1693
10. Yman L. Standardization of in vitro methods. Allergy. 2001;56(Suppl s67):70–74. doi:10.1111/j.1398-9995.2001.00921.x
11. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184:602–615. doi:10.1164/rccm.9120-11ST
12. Taylor DR, Pijnenburg MW, Smith AD, et al. Exhaled nitric oxide measurements: clinical application and interpretation. Thorax. 2006;61(9):817–827. doi:10.1136/thx.2005.056093
13. Kim J-H, Park S, Hwang YI, et al. Immunoglobulin G subclass deficiencies in adult patients with chronic airway diseases. J Korean Med Sci. 2016;31(10):1560–1565. doi:10.3346/jkms.2016.31.10.1560
14. Schauer U, Stemberg F, Rieger CHL, et al. IgG subclass concentrations in certified reference material 470 and reference values for children and adults determined with the binding site reagents. Clin Chem. 2003;49(11):1924–1929. doi:10.1373/clinchem.2003.022350
15. Mostafavi B, Piitulainen E, Tanash HA. Survival in the Swedish cohort with alpha-1-antitrypsin deficiency, up to the age of 43–45 years. Int J Chron Obstruct Pulmon Dis. 2019;14:525–530. doi:10.2147/COPD.S183205
16. Piitulainen E, Tornling G, Eriksson S. Effect of age and occupational exposure to airway irritants on lung function in non-smoking individuals with alpha 1-antitrypsin deficiency (PiZZ). Thorax. 1997;52(3):244–248. doi:10.1136/thx.52.3.244
17. Eden E, Mitchell D, Mehlman B, et al. Atopy, asthma, and emphysema in patients with severe α−1-antitrypsin deficiency. Am J Respir Crit Care Med. 1997;156(1):68–74. doi:10.1164/ajrccm.156.1.9508014
18. Reid PA, Reid PT. Occupational lung disease. J R Coll Physicians Edinb. 2013;43(1):44–48. doi:10.4997/JRCPE.2013.111
19. Piitulainen E, Tornling G, Eriksson S. Environmental correlates of impaired lung function in non-smokers with severe alpha 1-antitrypsin deficiency (PiZZ). Thorax. 1998;53(11):939–943. doi:10.1136/thx.53.11.939
20. Santos S, Marín A, Serra-Batlles J, et al. Treatment of patients with COPD and recurrent exacerbations: the role of infection and inflammation. Int J Chron Obstruct Pulmon Dis. 2016;11:515–525. doi:10.2147/COPD.S98333
21. Morell A. Clinical relevance of IgG subclass deficiencies. Ann Biol Clin. 1994;52:49–52.
22. Piitulainen E, Mostafavi B, Tanash HA. Health status and lung function in the Swedish alpha 1-antitrypsin deficient cohort, identified by neonatal screening, at the age of 37–40 years. Int J Chron Obstruct Pulmon Dis. 2017;12:495–500. doi:10.2147/COPD.S120241
23. Wall M, Moe E, Eisenberg J, et al. Long-term follow-up of a cohort of children with alpha-1-antitrypsin deficiency. J Pediatr. 1990;116(2):248–251. doi:10.1016/S0022-3476(05)82882-3
24. Kimpen J, Bosmans E, Raus J. Neonatal screening for alpha-1-antitrypsin deficiency. Eur J Pediatr. 1988;148(1):86–88. doi:10.1007/BF00441823
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.