Back to Journals » Clinical Ophthalmology » Volume 16
Low-Level Light Therapy in Association with Intense Pulsed Light for Meibomian Gland Dysfunction
Authors Marques JH ![]() , Marta A
, Marta A ![]() , Baptista PM
, Baptista PM ![]() , Almeida D
, Almeida D ![]() , José D
, José D ![]() , Sousa PJM
, Sousa PJM ![]() , Barbosa I
, Barbosa I ![]()
Received 30 July 2022
Accepted for publication 5 October 2022
Published 6 December 2022 Volume 2022:16 Pages 4003—4010
DOI https://doi.org/10.2147/OPTH.S384360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
João Heitor Marques,1 Ana Marta,1,2 Pedro Manuel Baptista,1,2 Daniel Almeida,1 Diana José,1 Paulo JM Sousa,1 Irene Barbosa1,2
1Ophthalmology Department, Centro Hospitalar Universitário do Porto, Porto, Portugal; 2Instituto de Ciências Biomédicas Abel Salazar, Universidade do Porto, Porto, Portugal
Correspondence: João Heitor Marques, Centro Hospitalar Universitário do Porto, Largo Prof. Abel Salazar, Porto, Portugal, Email [email protected]
Purpose: To study the clinical benefit of low-level light therapy when associated with intense pulsed light for the treatment of meibomian gland dysfunction.
Methods: An observational study. Two groups of patients that were treated with IPL were considered: group 1 (31 subjects, 62 eyes), intense pulsed light followed by low-level light therapy and group 2 (31 subjects, 62 eyes) intense pulsed light alone. In both groups, treatments were performed in 3 sessions and subjects were evaluated at baseline and 3 weeks after the last treatment session. Values are shown as mean difference ± standard deviation.
Results: We observed a significant improvement in OSDI-12 score and lipid layer thickness, in both groups (− 22.7± 17.5, p< 0.001 in group 1 and − 23.6± 23.8, p< 0.001 in group 2 for OSDI and +18.6 ± 37.0, p< 0.001 in group 1 and +19.9 ± 26.4, p< 0.001 in group 2 for lipid layer thickness). Despite no differences between groups at baseline (p=0.469), only group 1 had a significant improvement in Schirmer test (+1.6± 4.8, p=0.009 in group 1 and +1.7± 6.9, p=0.057 in group 2). No significant side effects were noted. No patient in any group felt subjectively “worse” after the treatment.
Conclusion: Intense pulsed light seems effective and safe for the treatment of meibomian gland dysfunction, improving symptoms and the tear film lipid layer. This study shows no strong evidence of the benefit of low-level light therapy, but it shows weak evidence that it may further improve aqueous tear production.
Keywords: dry eye syndromes, meibomian gland dysfunction, phototherapy, intense pulsed light therapy, low-level light therapy
Introduction
Meibomian gland dysfunction (MGD) is currently considered a crucial factor in dry eye disease.1 The prevalence of MGD ranges from 3.5% to 60%,2 it leads to patient-reported symptoms3 and it objectively and subjectively impairs visual function and life quality4,5 because of tear film instability and inflammation.
The treatment of MGD underwent a revolution in the past years: in addition to classical self-administered options such as warm compresses, lid massage and several types of ocular lubricants, new in-office targeted therapies are now available. Intense pulsed light (IPL) is broad spectrum high-power light pulsed that, in controlled trials, has been shown to improve tear film quality and symptoms.6–8 It may be more effective than eyelid hygiene in improving meibomian gland structure and reducing inflammation.9 The proposed mechanisms for its effectiveness are ablation of superficial blood vessels in the eyelids, leading to a reduced supply of inflammatory agents; reduction of bacterial and parasitic growth; meibum liquefaction, and collagen remodeling.10
Low-level light therapy (LLLT) is a different type of photomodulation, where low-power monochromatic red light is applied for a longer period, promoting tissue repair, antioxidation and reducing inflammation.11 LLLT has been more recently studied in combination with IPL in the treatment of MGD.12–14 Conversely, there is neither a published controlled study using LLLT alone nor a study comparing IPL plus LLLT with IPL alone. Therefore, the benefit of adding LLLT to IPL therapy remains unknown.
Our purpose was to evaluate the safety and effectiveness of LLLT when associated with IPL for the treatment of MGD.
Materials and Methods
Study Design
A prospective observational study was performed. The researcher collecting the data was masked to the subject’s group and subjects were unaware of the treatment allocation. The treatment was performed always by the same experienced unmasked clinician, but who was not involved in data collection.
Participants and Protocol
Subjects with clinical diagnosis of MGD according to The International Workshop on Meibomian Gland Dysfunction15 and aged over 18 years were considered for treatment in the Ophthalmology Department of Centro Hospitalar Universitário do Porto. Atrophy of meibomian glands on any of the lower eyelids (loss area of the meibomian glands through infrared meibography over 40%, measured automatically with IDRA® Ocular Surface Analyzer (SBM Sistemi, Italy) in the inferior eyelid led to exclusion from the treatment. Other contra-indications were: (1) ocular trauma, intraocular surgery, or intraocular inflammatory disease in the past six months; (2) contact lens wear in the past six months; (3) previous eyelid or lacrimal surgery; (4) skin cancer anywhere or pigment lesions on the periorbital skin; (5) pregnancy or nursing; and (6) inability to comply with the treatment or with the follow-up regimen.
Two groups of patients that were treated with IPL were considered:
- Group 1: Patients that underwent IPL+LLLT, 31 subjects, 62 eyes. Each treatment session started with 5 IPL (Eye-Light® with Optimal Power Energy®, Espansione Marketing S.p.A., Bologna, Italy) pulses applied inferiorly (4 pulses) and laterally (1 pulse) to each eye followed The application of a cooling gel was not necessary with the Optimal Power Energy® technology. Treatment was followed by bilateral application of LLLT (My Mask®, Espansione Marketing S.p.A., Bologna, Italy) for 15 minutes, independently of the skin pigmentation. The treatments were performed in 3 sessions 1 week apart, as recommended by the manufacturer.
- Group 2: Patients that underwent IPL alone, 31 subjects, 62 eyes. Each treatment session consisted of 5 IPL (E>Eye, E-SWIN, Paris, France) pulses applied inferiorly (4 pulses) and laterally (1 pulse) to each eye, over a layer of gel applied to the skin for optimized cooling and light conduction. The treatments were performed in 3 sessions, at day 0, day 15 and day 45, as recommended by the manufacturer.
Before IPL treatment, protective shields were placed over the eyes and the skin was cleaned in the areas to be treated. Hyperpigmented skin lesions were covered with a protective adhesive. Regardless of the group, the level of energy delivered was automatically set for each patient according to the degree of skin pigmentation (subjectively evaluated with skin Fitzpatrick scale) and each manufacture recommendation. The light pulses were applied perpendicularly to the skin to minimize reflexion. The clinician that applied the treatment was subject to the use of protective goggles. Between treatment sessions and during 15 days after the last treatment session, subjects were encouraged to apply sunscreen daily and avoid direct sun exposure.
There were no restrictions regarding the use of regular artificial tears, but no changes were allowed on every patient during the study and no drops could be used during the day of the study visit until after the examination. Moreover, mechanical gland expression, warm compresses, antibiotic, or anti-inflammatory treatments were not used during the study period. All subjects included for analysis completed all treatment sessions.
Outcomes
Subjects underwent the following evaluation both at baseline and 3 weeks after the last treatment session: (1) A validated dry-eye related questionnaire (OSDI 12); (2) automated ocular surface analysis as described previously16 (IDRA® Ocular Surface Analyzer SBM Sistemi, Italy) that reported non-invasive break-up time (NIBUT), eye blink quality (EB, score calculated automatically by the device using blinking frequency and completeness), lipid layer thickness (LLT), loss area of the meibomian glands (LAMG) in the inferior eyelid and tear meniscus height (TMH); (3) tear osmolarity (OSM, measured with TearLab® Osmolarity System, Tearlab, San Diego, CA, USA); (4) Schirmer test type 1 and (5) slip lamp evaluation with fluorescein and the presence of corneal staining (CFS) were noted.
Due to the presence of mucinous filaments in the corneal surface at baseline visit, the automatic measurement of LLT was not feasible in 17 eyes (3 in group 1 and 14 in group 2). Therefore, these eyes were excluded from the analysis that considered LLT. There were no other missing values.
At the post-treatment evaluation, each patient answered a subjective end report as feeling “better”, “the same” or “worse”.
Statistical Analysis
The estimated sample size (30 subjects per group) was calculated with G*Power software (ver. 3.1.9.7; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany. Using the mean change in lipid layer thickness after IPL treatment found in two previous studies,12,17 for a power of 90%, a significance level of 1%.
Regarding the ocular surface outcomes, both eyes were included for analysis and each eye was considered the statistical unit. For demographic data, subjects were considered the statistical unit.
Analysis was performed using IBM SPSS version 26.0.0.0. Chi-square and McNemar tests were used in categorical variables. t-tests were used in continuous variables after confirmation of the variables’ normal distribution (Shapiro–Wilk test) and equal variance (Levene´s test). Statistical significance was set as a p-value inferior to 0.01 to minimize type I statistical errors. Values are shown as mean ± standard deviation.
Results
Comparison of baseline demographic and clinical data between groups is shown in Table 1. An analysis of the outcomes before and after treatment is shown in Table 2 (quantitative analysis) and Table 3 (qualitative analysis).
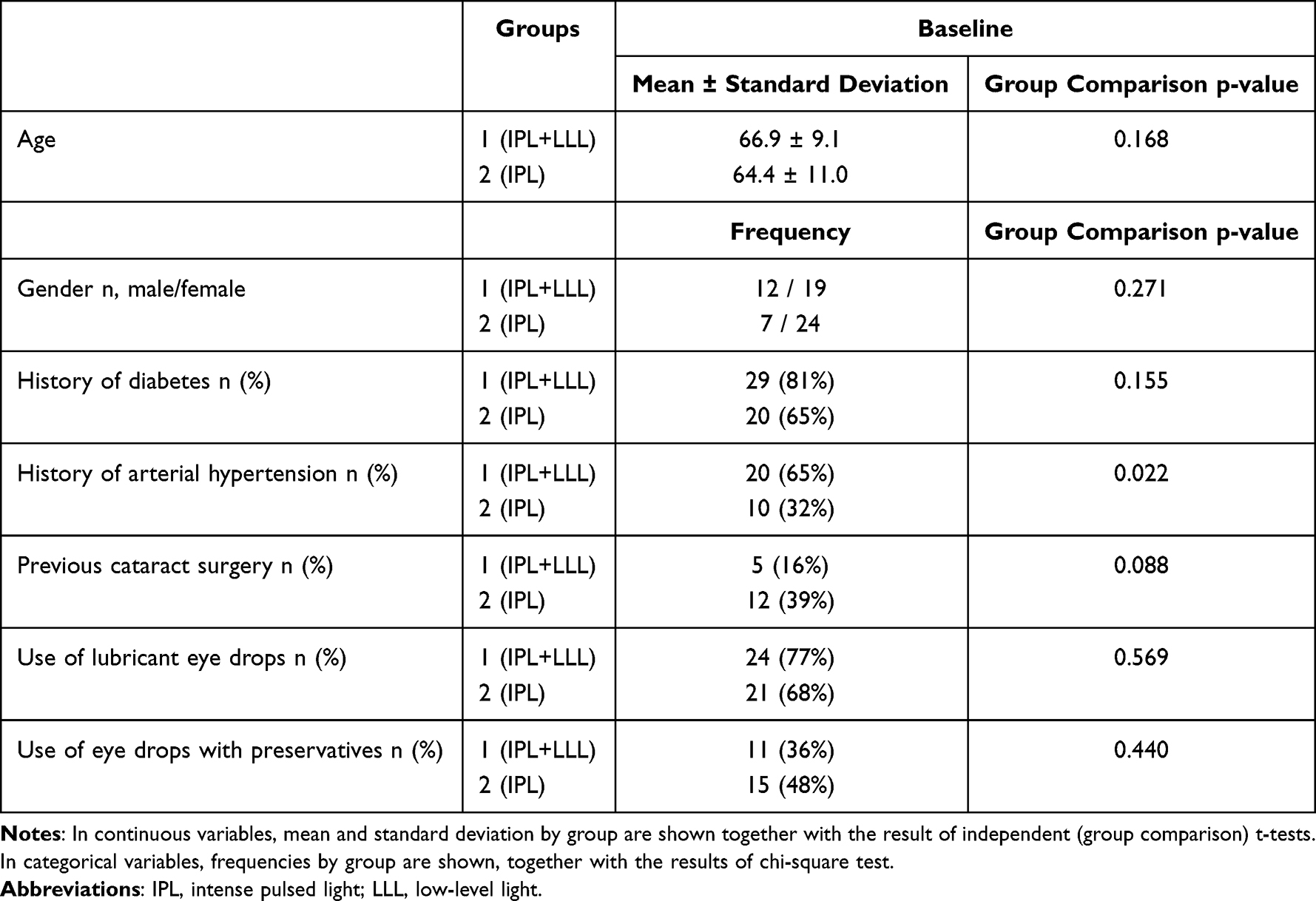 |
Table 1 Demographic and Medical History Comparison Between Groups (31 Subjects in Each Group) |
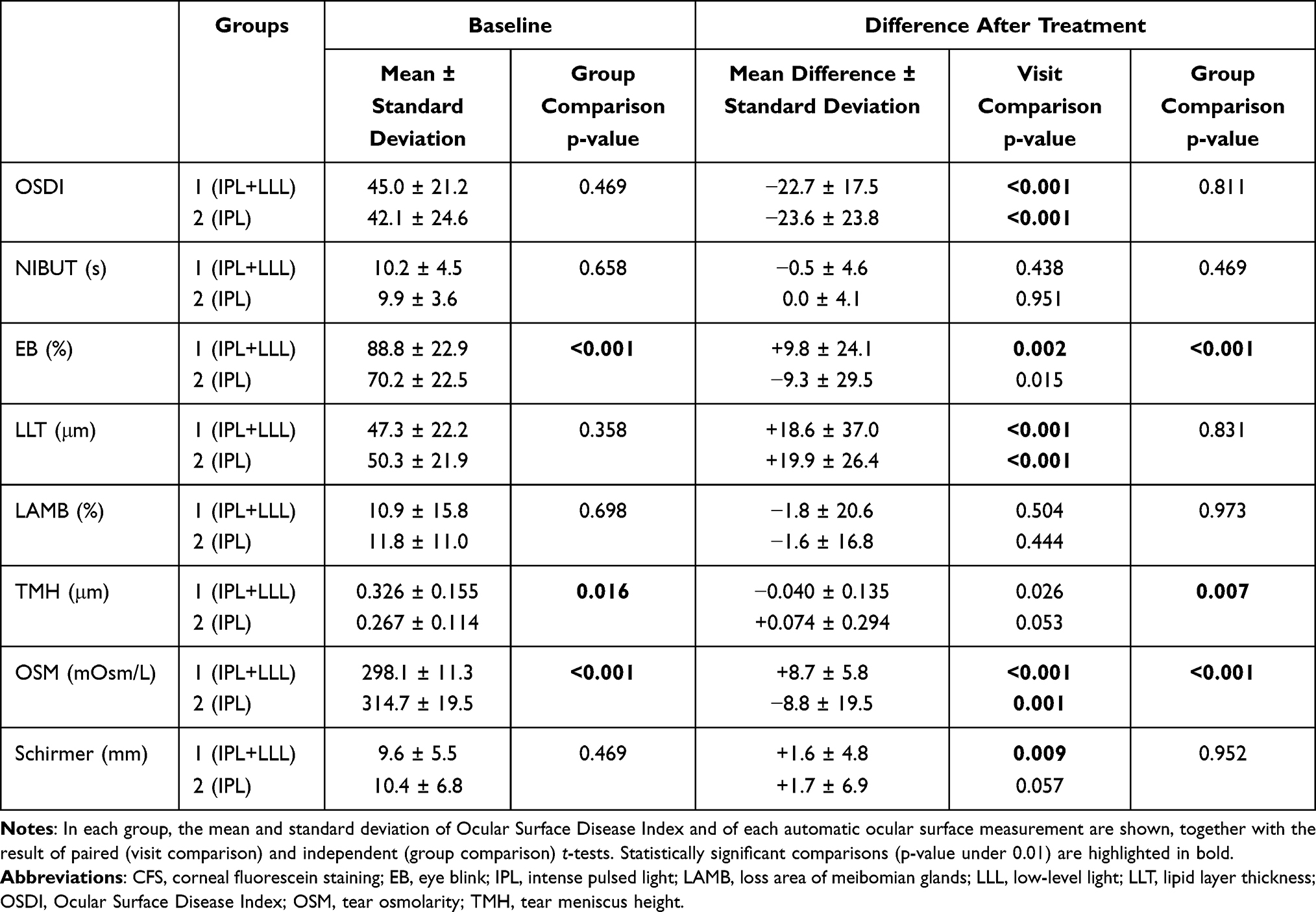 |
Table 2 Quantitative Analysis of 62 Eyes in Each Group |
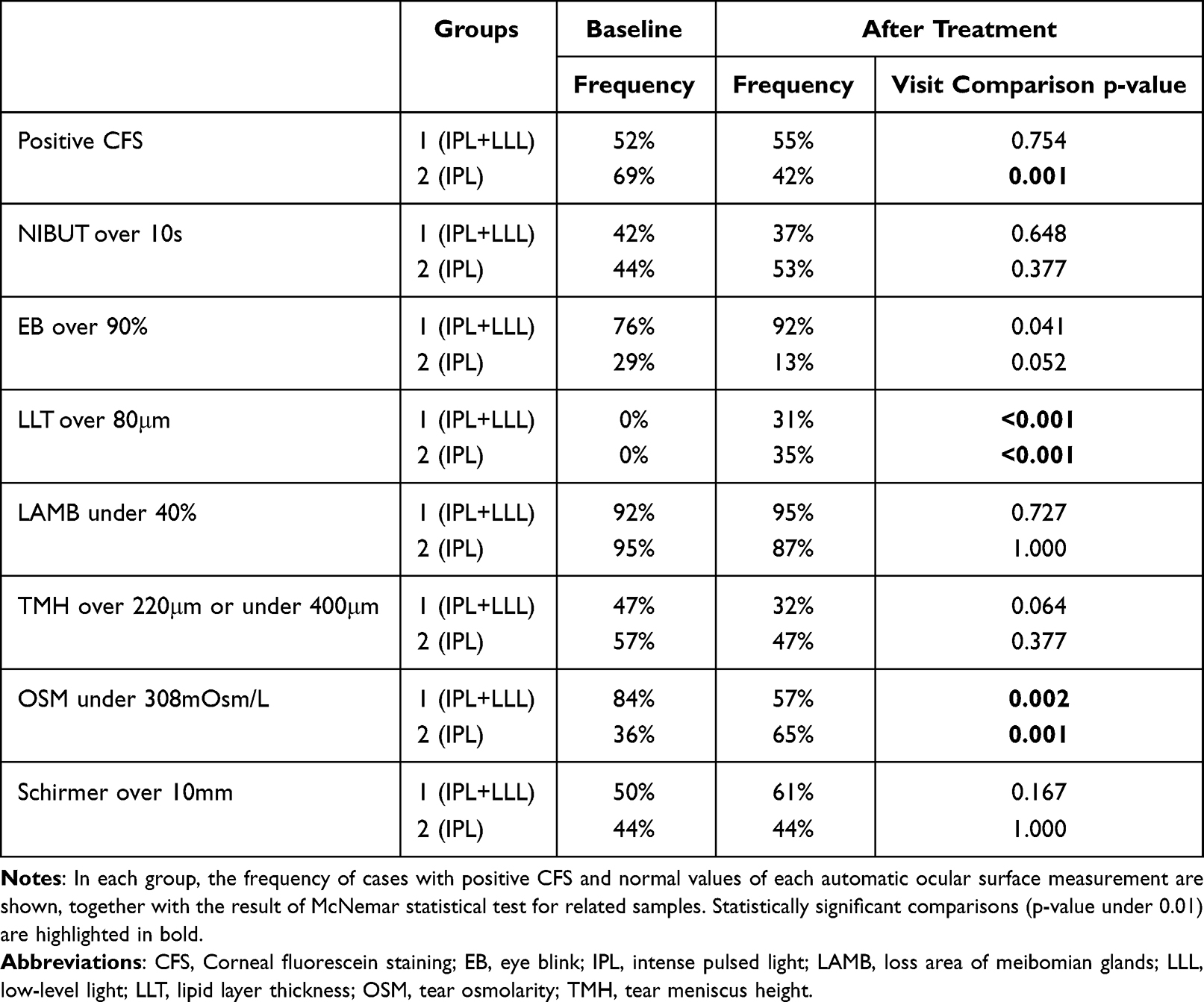 |
Table 3 Qualitative Analysis of 62 Eyes in Each Group |
Moreover, in group 1 (IPL+LLLT), 4/32 eyes (13%) with CSF at baseline exhibited its resolution with treatment. In group 2 (IPL), this frequency was 21/43 (49%, p=0.002). Furthermore, 6/30 (20%) eyes in group 1 (IPL+LLLT) and 4/19 (21%) eyes in group 2 (IPL) that had no CSF at baseline developed it by the time of the post-treatment visit.
Concerning the subjective end report, in group 1, 25/31 patients (81%) reported feeling “better” and 6/31 patients (19%) stated feeling “the same” after treatment. In group 2, these frequencies were 30/31 patients (97%) and 1/31 patients (3%), respectively (p=0.005). No patient in any group felt “worse” after the treatment.
Regarding the safety analysis, no adverse effects were noted in any group (no conjunctivitis, blistering, edema, skin pigmentation changes or loss of eyelashes).
Analyzing all eyes (124 eyes), there were no differences in the magnitude of changes in OSDI, LLT, EB or OSM (outcomes with significant changes) regarding the use of lubricant eye drops (p>0.189), use of antihypertensive eye drops (p>0.061), use of eye drops with preservatives (p>0.188) or previous cataract surgery (p>0.014).
Discussion
Our results, regarding both IPL alone and IPL plus LLLT, corroborate previous studies that showed the objective and subjective efficacy of IPL in the treatment of patients with dry eye disease and MGD.6–9,18–21 Conversely, a 2020 Cochrane meta-analysis, that included 3 of these previous studies, found uncertain evidence of effectiveness and safety of IPL as a treatment for MGD.22 In the current trial, regardless of the treatment arm, we observed a reduction in OSDI and an increase in LLT. Figure 1 shows a case study.
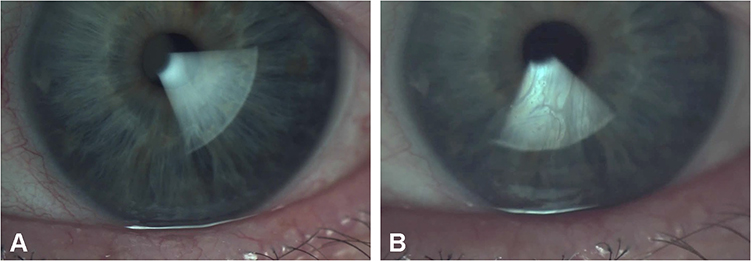 |
Figure 1 Light photography of the anterior segment of the eye together with tear interferometry to access lipid layer thickness before (A) and after (B) intense pulsed light treatment. In addition to the change in the interferometric pattern, it is also noticeable a reduction in the caliber of the eyelid margin telangiectasia. |
The reduction in OSDI may be accompanied by a placebo effect from inclusion in the study but may also be associated with less eyelid inflammation and better tear film quality after treatment. The anti-inflammatory properties of IPL are thought to be one of its main benefits in tear film homeostasis.23 In fact, Choi et al found a significant decrease in inflammatory cytokines (IL-4, IL-6, IL-10, IL-17A, and TNF-a) tear concentration after IPL treatment.21 The reduction in OSDI score was very similar between both groups (similar improvement in symptoms). Interestingly, considering the other patient reported outcome, a higher number of subjects reported to feel “better” after the treatment in the IPL group, when compared to the IPL+LLLT group. We hypothesize that the extra treatment time and warm sensation during and after the treatment with LLLT will lead some patients to undervalue the benefit.
We postulate that the increase in LLT is a consequence of the improved outflow of meibum from the glands and their enhanced function and morphology, as it has been already described.9 In both groups, LLT increased equally and on average 39% from baseline to the post-treatment visit and 30% of cases reached normal values. Still, the other 70% of cases did not reach the normal value of LLT at 1 month, a result that should be interpreted carefully. An improvement in patients with MGD may be clinically significant even if normal values (calculated for a healthy population) are not met. Moreover, it has been showed that LLT may further improve up to 6 months after the treatment.12 Other studies have evaluated the lipid layer after IPL treatment: Most studies observed improvement in a qualitative evaluation, making it difficult to compare with our study.6,17,24 Performed a quantitative evaluation that showed the same magnitude of improvement that our study, regardless of the treatment modality.
Regarding comparative studies using IPL, there is a single published one that showed few clinically significant differences between two distinct devices.25 Regarding LLLT, there is no published article exploring this treatment alone in humans. There are three previous single arm studies using IPL combined with LLLT,12–14 showing improvement in symptoms and objective measures, similar to the effect of IPL alone. However, proper comparisons with other studies using IPL alone were not possible given the variable methodologies used. Therefore, there has been no discrimination in the effect of LLLT. The current study is the first to compare the clinical efficacy and safety of IPL combined with LLLT to IPL alone.
Our study groups were relatively well-balanced regarding demographic data and most baseline ocular surface parameters. Yet, there were baseline differences between groups in EB, THM and OSM, that limit proper longitudinal comparison of these outcomes between groups. Still, regarding the Schirmer test, significance was reached in the IPL plus LLLT group and not in the IPL alone group. Low energy delivery during a longer period induces biomodulation without tissue coagulation or destruction. As previously suggested in a pre-clinical study,26 LLLT alone may have an effect on the lacrimal gland, increasing tear volume and reducing neutrophil infiltration. As Marta et al highlighted,12 LLLT, but not IPL, is applied directly to the superior lid (and over the lacrimal gland) which may justify the differences regarding aqueous tear production after treatment. We found no other significant differences between groups in the changes after treatment. However, other studies found an improvement in tear break-up time after IPL that relates to the augmentation of lipid layer and consequent stabilization of the tear film.6,7,17,24,27 The non-improvement in both groups of our study sample may be related to the fact that baseline NIBUT was close to normal and higher than those previous studies.
A significant reduction in CFS after treatment was seen in the IPL group and not in the IPL+LLLT group. There was however no difference between groups in the number of eyes that developed de novo CFS, suggesting it was not a safety issue. This finding may be a consequence of non-significant but uneven distribution of diabetic patients between groups, with higher frequency in the IPL+LLLT group. Diabetic patients show increased corneal epithelial fragility, delayed healing, and persistent defects.28,29 Anyhow, further research is needed regarding the effect of IPL and LLLT in the corneal epithelium.
The results of this study support no clear superiority in efficacy or safety when comparing both treatment modalities. In clinical practice, it should also be taken into consideration the extra burden caused by LLLT namely the increased treatment time, and some discomfort caused by the application of heat. Our methodology did not consider these two outcomes.
A possible limitation of this study is the use of different IPL devices in each group and different treatment intervals. Currently there is no approved device to perform LLLT separately. We used the commercially available devices to perform each treatment and the session intervals recommended by each manufacturer. The observational design of the study impaired true randomization of the subjects or experimentation with the use LLLT alone. Another limitation is the short follow-up. Other studies with longer follow-up periods observed an effect up to 3–6 months after similar treatment protocols.8,12,14,19 It remains unclear if LLLT will affect the results in the long term.
IPL seems to have advantages in patients which are refractory or uncompliant to classic therapies, but formal indications are not yet established. Future studies should also determine the stage of MGD and other patient’s characteristics that predict the best cost-effectiveness for this treatment.
Conclusion
In summary, our results suggest that IPL is effective and safe in the short term for the treatment of MGD. Combining LLLT to IPL may additionally improve lacrimal gland function and tear production, but further studies must confirm this finding.
Abbreviations
CFS, corneal staining; EB, eye blink quality; IPL, intense pulsed light; LLT, lipid layer thickness; LAMG, loss area of the meibomian glands; LLLT, low-level light therapy; MGD, meibomian gland dysfunction; NIBUT, non-invasive break-up time; TMH, tear meniscus height; OSM, tear osmolarity.
Data Sharing Statement
Raw data that supports the results of this study is available by request at the first author.
Ethics and Patient Consent
The study was approved by our institutional review board and ethics committee - Departamento de Ensino Formação e Investigação, Centro Hospitalar Universitário do Porto, ID 2021-037 (029-DEFI-030-CE) and it was conducted accordingly to the principles of the Declaration of Helsinki for the protection of human subjects in medical research. Written informed consent was obtained from all subjects.
Acknowledgments
The authors would like to thank the Head of the Ophthalmology Department of Centro Hospitalar Universitário do Porto, Prof. Dr. Pedro Menéres, for the support granted for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was obtained for this study.
Disclosure
The authors declare that they have no conflict of interests.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II definition and classification report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Schaumberg DA, Nichols JJ, Papas EB, Tong L, Uchino M, Nichols KK. The international workshop on meibomian gland dysfunction: report of the subcommittee on the epidemiology of, and associated risk factors for, MGD. Invest Ophthalmol Vis Sci. 2011;52(4):1994–2005. doi:10.1167/iovs.10-6997e
3. Bron AJ, Tiffany JM. The contribution of meibomian disease to dry eye. Ocul Surf. 2004;2(2):149–164. doi:10.1016/S1542-0124(12)70150-7
4. Miljanović B, Dana R, Sullivan DA, Schaumberg DA. Impact of dry eye syndrome on vision-related quality of life. Am J Ophthalmol. 2007;143(3):409–415.e2. doi:10.1016/j.ajo.2006.11.060
5. Denoyer A, Rabut G, Baudouin C. Tear film aberration dynamics and vision-related quality of life in patients with dry eye disease. Ophthalmology. 2012;119(9):1811–1818. doi:10.1016/j.ophtha.2012.03.004
6. Craig JP, Chen YH, Turnbull PRK. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2015;56(3):1965–1970. doi:10.1167/iovs.14-15764
7. Piyacomn Y, Kasetsuwan N, Reinprayoon U, Satitpitakul V, Tesapirat L. Efficacy and safety of intense pulsed light in patients with meibomian gland dysfunction-a randomized, double-masked, sham-controlled clinical trial. Cornea. 2020;39(3):325–332. doi:10.1097/ICO.0000000000002204
8. Xue AL, Wang MTM, Ormonde SE, Craig JP. Randomised double-masked placebo-controlled trial of the cumulative treatment efficacy profile of intense pulsed light therapy for meibomian gland dysfunction: intense pulsed light therapy for meibomian gland dysfunction. Ocul Surf. 2020;18(2):286–297. doi:10.1016/j.jtos.2020.01.003
9. Yin Y, Liu N, Gong L, Song N. Changes in the meibomian gland after exposure to intense pulsed light in Meibomian Gland Dysfunction (MGD) patients. Curr Eye Res. 2018;43(3):308–313. doi:10.1080/02713683.2017.1406525
10. Vora GK, Gupta PK. Intense pulsed light therapy for the treatment of evaporative dry eye disease. Curr Opin Ophthalmol. 2015;26(4):314–318. doi:10.1097/ICU.0000000000000166
11. Rojas JC, Gonzalez-Lima F. Low-level light therapy of the eye and brain. Eye Brain. 2011;3:49. doi:10.2147/eb.s21391
12. Marta A, Baptista PM, Marques JH, et al. Intense pulsed plus low-level light therapy in meibomian gland dysfunction. Clin Ophthalmol. 2021;15:2803–2811. doi:10.2147/OPTH.S318885
13. Stonecipher K, Abell TG, Chotiner B, Chotiner E, Potvin R. Combined low level light therapy and intense pulsed light therapy for the treatment of meibomian gland dysfunction. Clin Ophthalmol. 2019;13:993–999. doi:10.2147/OPTH.S213664
14. Pérez-Silguero MA, Pérez-Silguero D, Rivero-Santana A, Bernal-Blasco MI, Encinas-Pisa P. Combined intense pulsed light and low-level light therapy for the treatment of dry eye: a retrospective before–after study with one-year follow-up. Clin Ophthalmol. 2021;15:2133–2140. doi:10.2147/OPTH.S307020
15. Tomlinson A, Bron AJ, Korb DR, et al. The international workshop on meibomian gland dysfunction: report of the diagnosis subcommittee. Invest Ophthalmol Vis Sci. 2011;52(4):2006–2049. doi:10.1167/iovs.10-6997f
16. Vigo L, Pellegrini M, Bernabei F, Carones F, Scorcia V, Giannaccare G. Diagnostic performance of a novel noninvasive workup in the setting of dry eye disease. J Ophthalmol. 2020;2020:1–6. doi:10.1155/2020/5804123
17. Arita R, Fukuoka S, Morishige N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul Surf. 2019;17(1):104–110. doi:10.1016/J.JTOS.2018.11.004
18. Arita R, Mizoguchi T, Fukuoka S, Morishige N. Multicenter study of intense pulsed light therapy for patients with refractory meibomian gland dysfunction. Cornea. 2018;37(12):1566–1571. doi:10.1097/ICO.0000000000001687
19. Rong B, Tang Y, Liu R, et al. Long-term effects of intense pulsed light combined with meibomian gland expression in the treatment of meibomian gland dysfunction. Photomed Laser Surg. 2018;36(10):562–567. doi:10.1089/pho.2018.4499
20. Liu R, Rong B, Tu P, et al. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating meibomian gland dysfunction. Am J Ophthalmol. 2017;183:81–90. doi:10.1016/j.ajo.2017.08.021
21. Choi M, Han SJ, Ji YW, et al. Meibum expressibility improvement as a therapeutic target of intense pulsed light treatment in meibomian gland dysfunction and its association with tear inflammatory cytokines. Sci Rep. 2019;9(1):1–8. doi:10.1038/s41598-019-44000-0
22. Cote S, Zhang AC, Ahmadzai V, et al. Intense pulsed light (IPL) therapy for the treatment of meibomian gland dysfunction. Cochrane Database Syst Rev. 2020;2020:3. doi:10.1002/14651858.CD013559
23. Vergés C, Salgado-Borges J, March de Ribot F, Ribas V. Current developments of intensive pulsed light treatment for dry eye disease and meibomian gland dysfunction. Expert Rev Ophthalmol. 2021:1–9. doi:10.1080/17469899.2021.1954504
24. Yan X, Hong J, Jin X, et al. The efficacy of intense pulsed light combined with meibomian gland expression for the treatment of dry eye disease due to meibomian gland dysfunction: a multicenter, randomized controlled trial. Eye Contact Lens. 2021;47(1):45–53. doi:10.1097/ICL.0000000000000711
25. Wu Y, Li J, Hu M, et al. Comparison of two intense pulsed light patterns for treating patients with meibomian gland dysfunction. Int Ophthalmol. 2020;40(7):1695–1705. doi:10.1007/s10792-020-01337-0
26. Goo H, Kim H, Ahn J-C, Cho KJ. Effects of low-level light therapy at 740 nm on dry eye disease in vivo. Med Lasers; Eng Basic Res Clin Appl. 2019;8(2):50–58. doi:10.25289/ML.2019.8.2.50
27. Chen Y, Li J, Wu Y, Lin X, Deng X, Yun-e Z. Comparative evaluation in intense pulsed light therapy combined with or without meibomian gland expression for the treatment of meibomian gland dysfunction. Curr Eye Res. 2021;46(8):1125–1131. doi:10.1080/02713683.2020.1867750
28. Chen WL, Lin CT, Ko PS, et al. In vivo confocal microscopic findings of corneal wound healing after corneal epithelial debridement in diabetic vitrectomy. Ophthalmology. 2009;116(6):1038–1047. doi:10.1016/j.ophtha.2009.01.002
29. Ljubimov AV. Diabetic complications in the cornea. Vision Res. 2017;139:138–152. doi:10.1016/j.visres.2017.03.002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pulsed Light Therapy in the Management of Dry Eye Disease: Current Perspectives
Barbosa Ribeiro B, Marta A, Ponces Ramalhão J, Marques JH, Barbosa I
Clinical Ophthalmology 2022, 16:3883-3893
Published Date: 24 November 2022