Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Low-Dose Dexmedetomidine Reduces Median Effective Doses of Propofol Required for Successful Gastroscope Insertion: A Prospective Randomized Controlled Dose-Finding Trial
Authors Zhu Q ![]() , Hao PP, Cui LL
, Hao PP, Cui LL ![]() , Liu FK
, Liu FK ![]() , Xue FS
, Xue FS ![]()
Received 29 September 2025
Accepted for publication 8 January 2026
Published 12 January 2026 Volume 2026:22 571057
DOI https://doi.org/10.2147/TCRM.S571057
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Qian Zhu,1 Pei-Pei Hao,2 Ling-Li Cui,1 Fu-Kun Liu,1 Fu-Shan Xue1,3
1Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology, Maternal and Child Health Hospital of Henan Province, The Third Affiliated Hospital of Zhengzhou University, Zhengzhou, People’s Republic of China; 3Department of Anesthesiology, Shengli Clinical Medical College of Fujian Medical University, Fuzhou University Affiliated Provincial Hospital, Fujian Provincial Hospital, Fuzhou, People’s Republic of China
Correspondence: Fu-Shan Xue, Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, NO. 95 Yong-An Road, Xi-Cheng District, Beijing, 100050, People’s Republic of China, Tel +86-13911177655, Email [email protected]
Purpose: Patients undergoing painless gastrointestinal endoscopy (GIE) typically receive propofol-based sedation. However, the exact dose of propofol when combined with low-dose dexmedetomidine for this procedure remains unclear. The objective of this study was to determine and compare the median effective doses (ED50, the doses required for successful gastroscope insertion in 50% of the subjects) of propofol when used with low-dose dexmedetomidine (0.3 μg/kg) premedication versus propofol alone during painless GIE.
Patients and Methods: Adult outpatients aged 18 to 65 years scheduled for GIE were enrolled. Participants were randomized to receive either 0.9% saline (Group S) or 0.3 μg/kg of dexmedetomidine (Group D) intravenously over 5 min before induction with propofol. Using modified Dixon’s up-and-down method (MDUDM), the initial induction dose of propofol was 1.5 mg/kg, adjusted in a step size of 0.1 mg/kg. ED50 of propofol required for successful endoscope insertion was calculated by averaging the midpoints of all sequential crossovers. Using isotonic regression analysis, ED50 and ED95 (the effective doses required for successful gastroscope insertion in 95% of the subjects) were then extrapolated. All adverse events during painless GIE were recorded.
Results: Thirty patients were enrolled per group. Using MDUDM, the ED50 of propofol for successful gastroscope insertion was significantly lower in Group D (1.48 ± 0.10 mg/kg) than in Group S (1.82 ± 0.16 mg/kg; P < 0.001). The ED50 and ED95 of propofol were extrapolated to 1.80 mg/kg (83% confidence interval [CI], 1.649– 1.882) and 2.10 mg/kg (83% CI, 2.081– 2.124) for Group S, respectively, using isotonic regression analysis. These values were significantly lower in Group D, at 1.40 mg/kg (83% CI, 1.297– 1.452) and 1.70 mg/kg (83% CI, 1.667– 1.753).
Conclusion: Premedication with low-dose dexmedetomidine (0.3 μg/kg) significantly reduces the median effective doses of propofol required for successful gastroscope insertion during painless GIE.
Keywords: dexmedetomidine, propofol, effective dose, gastrointestinal endoscopy, sedation
Introduction
Gastrointestinal endoscopy (GIE) is a pivotal and extensively utilized technique for diagnosing and managing disorders of the digestive tract. Compared with sedated GIE, unsedated GIE not only causes discomfort and anxiety in patients but also is associated with an increased prevalence of adverse effects, including hypertension, tachycardia, nausea, and retching.1 Sedation can enhance patient comfort, improve lesion detection rates, and increase satisfaction of both patients and endoscopists. Nowadays, sedated GIE, also known as painless GIE, has become the preferred clinical approach.1–5
The sedation practices for GIE vary globally. Propofol has become the predominant sedative for outpatient GIE due to its rapid onset and recovery time, facilitating efficient discharge.3,4,6 Nevertheless, propofol lacks an effective antagonist and has a narrow therapeutic window.7,8 Its lack of analgesic effect when administered alone for GIE frequently necessitates higher doses, increasing the risk of hypoxemia and circulatory depression.3,4 The depth of sedation is found to be highly dose-dependent.4,8 Although higher doses generally induce deeper sedation, they concomitantly augment the risks of respiratory depression and hemodynamic suppression.
The Combination of drugs with distinct pharmacological mechanisms has been demonstrated to achieve the desired depth of anesthesia while reducing individual drug requirements and mitigating adverse effects.9,10 Recently, dexmedetomidine, a non-opioid, non-benzodiazepine sedative has emerged as a prominent agent in opioid-free anesthesia.11–13 This highly selective α2- adrenergic receptor agonist has sedative, analgesic, and anxiolytic effects.14–16 Dexmedetomidine is regarded as a safe addition to propofol due to its minimal impact on respiratory function and can attenuate physiological stress responses.16–19 Multiple studies confirm its capacity to reduce concomitant anesthetic requirements.20–22 Premedication of dexmedetomidine significantly reduces the required induction dose of propofol.20,22–28 It is noteworthy that higher doses of dexmedetomidine are associated with the occurrence of bradycardia and hypotension, while administering low-dose dexmedetomidine as an adjuvant prior to propofol induction may maximize therapeutic benefits while minimizing side effects.20,26,27,29 However, limited data exist regarding the precise dosage requirements and the magnitude of propofol reduction achievable with low-dose dexmedetomidine during GIE.
Our hypothesis was that low-dose dexmedetomidine (0.3 µg/kg) would reduce the median effective doses (ED50) of propofol required for successful gastroscope insertion. The objective of this prospective randomized controlled dose-finding trial was to quantify alterations in the ED50 of propofol when premedicated with low-dose dexmedetomidine (0.3 µg/kg administered over 5 minutes) versus propofol alone. Concurrent hemodynamic changes were documented. This investigation provides definitive data comparing the effect of low-dose dexmedetomidine (0.3 µg/kg) combined with propofol with propofol alone on the ED50 of propofol, which was previously unstudied for this specific combination.
Materials and Methods
Study Design
This prospective randomized controlled dose-finding trial was approved by the Ethics Committee of Beijing Friendship Hospital, Capital Medical University (2021-P2-395-03) and was registered with the Chinese Clinical Trial Registry (ChiCTR2200055952) on January 29, 2022. The trial was conducted at Beijing Friendship Hospital between May and August 2022, in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent.
Study Participants
Outpatients aged 18 to 65 years scheduled for GIE under sedation, with American Society of Anesthesiologists (ASA) physical status I–II, 18.0 ≤ body mass index (BMI) ≤ 30 kg/m2, and Mallampati grades I–II were enrolled. All patients fully understood the purpose and significance of this trial, voluntarily participated in this clinical trial, read and understood the informed consent form, and voluntarily sign the informed consent form.
Exclusion criteria comprised: pregnant or lactating women; inability to ambulate without assistance; bradycardia (heart rate ≤ 60 beats /min); history of severe arrhythmia or cardiac insufficiency; clinical diagnosis of cognitive impairment in medical history; body weight > 100 kg; allergies to propofol, soy, or glycerol; previous adverse reactions to dexmedetomidine; prior diagnosis of acute or chronic renal function impairment; severe liver damage leading to ascites and liver cirrhosis; use of benzodiazepines or opioids within 24 hours before GIE; uncontrolled hypertension; myocardial infarction, ischemic cardiomyopathy, or taking β-receptor blockers; history or possibility of difficult airway (eg, obstructive sleep apnea syndrome); mouth opening < 3 cm, radiation injury or tumor of the neck, instability of the cervical spine; upper airway diseases (eg, upper respiratory tract infection within two weeks).
Study Protocol
An independent researcher generated a computerized randomization sequence using SPSS for Mac version 26.0 (SPSS Inc, Chicago, IL, USA). Participants were allocated to either Group S (saline + propofol) or Group D (dexmedetomidine + propofol) in a 1:1 ratio via consecutively numbered, opaque, sealed envelopes. Anesthesiologist A was responsible for opening the envelopes for the group assignment. A 20-mL syringe, labeled identically, was prepared, containing either 10 mL of 0.9% saline or dexmedetomidine (0.3 µg/kg).
Each participant fasted for at least eight hours from fatty or fried foods, six hours from light meals, and two hours from liquids. No premedication was administered. A 22-gauge intravenous cannula was inserted into the right hand of the subject in the endoscopic suite and then connected to Lactated Ringer’s solution via a three-way stopcock. Patients were placed in a left lateral decubitus position with elevated head and slight flexion of the legs. Continuous monitoring encompassed non-invasive blood pressure (NIBP), electrocardiogram (ECG), respiratory rate (RR), and pulse oxygen saturation (SpO2). Patients held a mask over their mouth and nose to inhale 100% oxygen at a flow rate of 6 L/min. After 5 min, baseline mean arterial pressure (MAP), heart rate (HR), RR, and SpO2 were recorded. Following five deep breaths, anesthesiologist B intravenously pumped 10 mL of study solution containing 0.9% saline or 0.3 µg/kg dexmedetomidine (Jiangsu Hengrui Pharmaceutical Co Ltd., Jiangsu, China, 211222BC) over 5 min. Propofol (Fresenius Kabi Austria GmbH, 16QH2058) was then administered intravenously over 30s for induction. The anesthesiologist B, the follow-up observers, the endoscopist, and the patients all remained blinded to group assignments and syringe contents.
The initial induction dose of propofol (1.5 mg/kg) and the step size (0.1 mg/kg) followed the modified Dixon’s up-and-down method (MDUDM), based on both pilot data and previous research.30–33 Sedation depth was evaluated 60s after propofol administration using the modified observer’s assessment of alertness/sedation (MOAA/S) scale (Supplemental Table 1), targeting deep sedation (MOAA/S score ≤ 1).34,35 When MOAA/S score reached ≤ 1, an experienced endoscopist attempted gastroscope insertion. Responses were categorized as either “success (no movement)” or “failure (coughing, gagging, or body movement)”. Only first-attempt responses analyzed. In cases where the sedation level was deemed inadequate (MOAA/S score > 1) or where response was “failure”, a supplementary dose of 0.5 mg/kg of propofol was administered, repeated until the response was “success”. Subsequent patients’ induction doses were adjusted inversely: decreased by 0.1 mg/kg after “success” and increased by 0.1 mg/kg after “failure”. The MDUDM generally necessitates a minimum of six crossover points and 20–40 patients for reliable dose estimation.32,33,36,37 This trial included eight crossover points with 30 patients in each group.
During the maintenance phase of anesthesia, sedation depth was assessed every 2 min to ensure the maintenance of deep sedation from the initiation of gastroscopy through the completion of colonoscopy. For MOAA/S score > 1, coughing, gagging, or body movement, 0.5 mg/kg propofol boluses were administered. Propofol infusion was ceased upon reaching the ileocecal valve. Subsequent to this, patients were transferred to the Postanesthesia Care Unit (PACU) for observation. A Modified Aldrete score of ≥ 9 was required for PACU discharge.38 Telephone follow-ups were conducted 24 hours post-discharge.
Primary and Secondary Outcome
The primary outcome of this study was the ED50 of propofol required for successful endoscope insertion using MDUDM. Secondary outcomes encompassed the following: ED50 and ED95 (the doses required for successful endoscope insertion in 95% of patients) of propofol required for successful endoscope insertion extrapolated using isotonic regression analysis, propofol dose and patient response, procedure duration, total propofol dose, frequency of propofol supplementation, eye-opening time (interval between the final propofol bolus dose and response to the eye-opening command), recovery time (from PACU admission to discharge), MOAA/S score at the end of colonoscopy, and Aldrete score at PACU admission and discharge. The following points were used to record the variables (MAP, HR, RR, and SpO2) were recorded at the following points: T0, before propofol administration (baseline); T1, immediately after saline or dexmedetomidine administration; T2, immediately after propofol administration; T3, immediately after gastroscope insertion; T4, 2 min after gastroscope insertion; T5, at the end of gastroscopy; T6, at the beginning of colonoscopy; T7, 5 min after the beginning of colonoscopy; T8, at the end of colonoscopy; T9, at PACU admission; T10, at PACU discharge. The following parameters, including nausea and vomiting, propofol injection pain, abdominal pain (Numeric Rating Scale, NRS), intraoperative awareness, and endoscopist satisfaction, were evaluated at the point of PACU discharge. Endoscopist satisfaction was rated on a four-point scale: excellent (4), good (3), general (2), or bad (1). Patient satisfaction was evaluated 24h after PACU discharge using a four-point scale: excellent (4), good (3), tolerable (2), or intolerable (1).
All adverse events which occurred during the observed period were meticulously documented. These events included bradycardia (HR < 50 bpm), tachycardia (HR > 100 bpm), hypotension (MAP < 60 mmHg), and hypertension (an increase in MAP > 30%). These events were treated and recorded accordingly with atropine 0.25 mg, esmolol 20 mg, ephedrine 6 mg, and urapidil 10 mg, respectively. The categorization of respiratory depression was as follows: subclinical respiratory depression (90% ≤ SpO2 < 95%), hypoxia (75% ≤ SpO2 < 90% for < 60s), and severe hypoxia (SpO2 < 75% or 75% ≤ SpO2 < 90% for ≥ 60s).39 Subclinical respiratory depression was managed with a jaw-thrust maneuver. Hypoxia necessitated jaw-thrust maneuvers and an increase in oxygen flow, while severe hypoxia required mask ventilation.
Statistical Analysis
Data analysis was conducted using SPSS for Mac version 26.0 (SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk test was employed to assess the normality of data distribution. Normally distributed continuous data were reported as mean ± standard deviation (SD) and then compared between groups using Student’s t-test. Non-normally distributed continuous data were presented as median (interquartile range) with Mann–Whitney U-test for group comparisons. Categorical data were expressed as percentages and analyzed using the Chi-squared test or Fisher’s exact test, as appropriate. The changes in MAP, HR, RR, and SpO2 were analyzed using repeated-measures analysis of variance (ANOVA). P < 0.05 was considered statistically significant.
The ED50 of propofol (the dose required for successful endoscope insertion in 50% of patients) was calculated by averaging the midpoints of all crossover points from “failure” to “success” using the MDUDM.36 Subsequently, the observed responses were adjusted using the pooled-adjacent-violators algorithm (PAVA) with the “R” package (R version 4.1.3, 2022–03-10). The ED50 and ED95 of propofol and their corresponding 83% confidence intervals (CIs) were determined using isotonic regression analysis.31,33,36,40
Results
Initially, 99 patients were assessed for eligibility, and 60 patients were enrolled, with 30 in each group completing the study from May to August 2022 (Figure 1). No significant intergroup differences in demographic characteristics were observed (Table 1). The ED50 of propofol required for successful gastroscope insertion, calculated using the MDUDM, was significantly lower in Group D than in Group S (1.48 ± 0.10 mg/kg vs 1.82 ± 0.16 mg/kg, respectively; 18.7% reduction; P < 0.001; Table 2). Isotonic regression analysis confirmed significantly lower ED50 and ED95 in Group D, as indicated by non-overlapping 83% CIs (Table 2).33
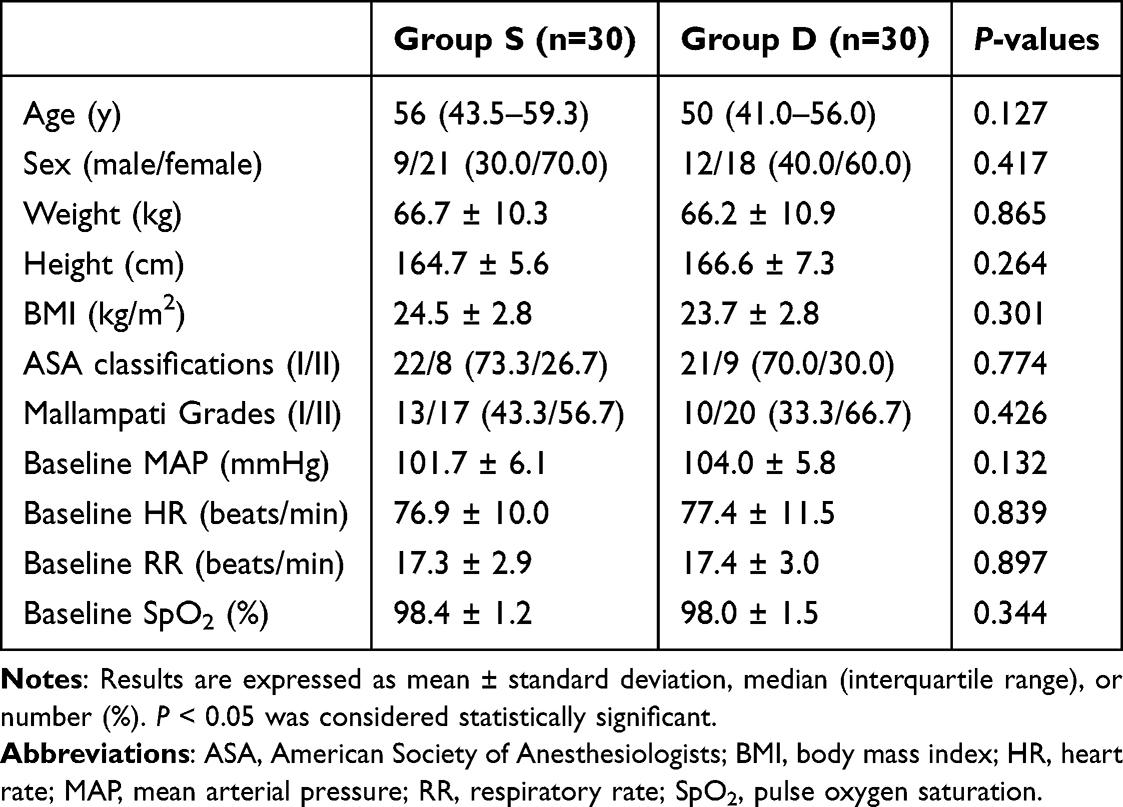 |
Table 1 Demographic Characteristics |
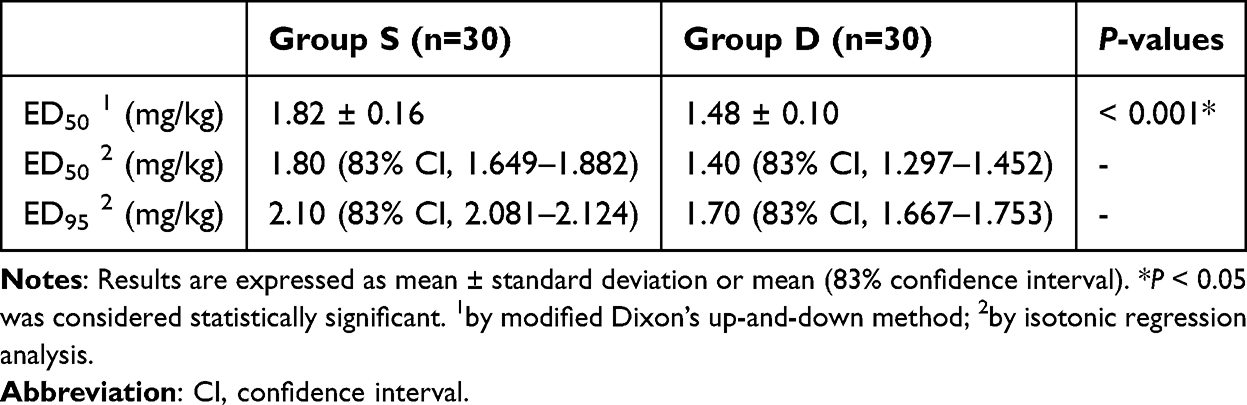 |
Table 2 ED50 and ED95 of Propofol for Successful Gastroscope Insertion |
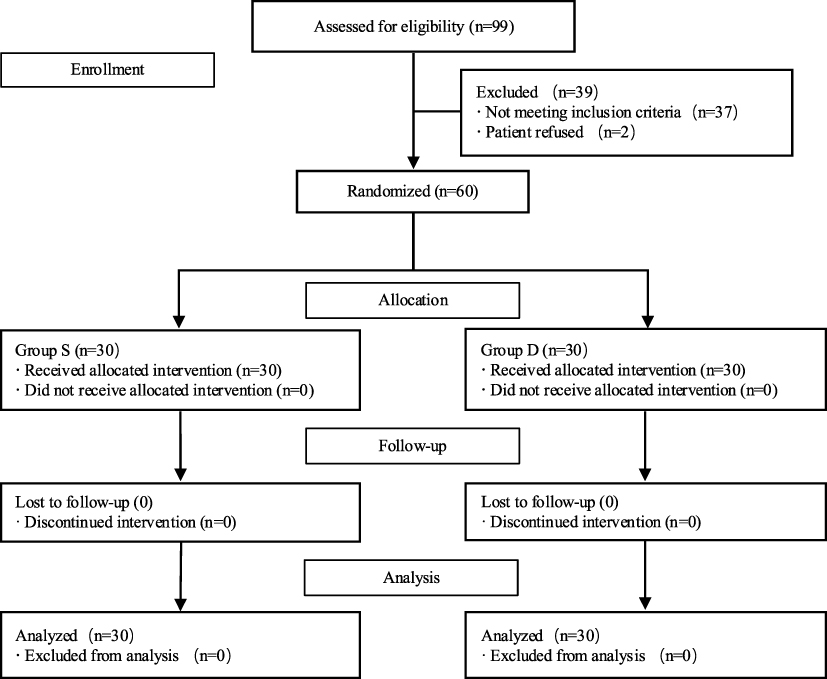 |
Figure 1 Consort flow diagram. |
Figure 2 illustrates the responses of consecutive patients to gastroscope insertion in the two groups. Group D exhibited a left-shifted dose-response curve (Figure 3). Table 3 presents observed and PAVA-adjusted response rates.
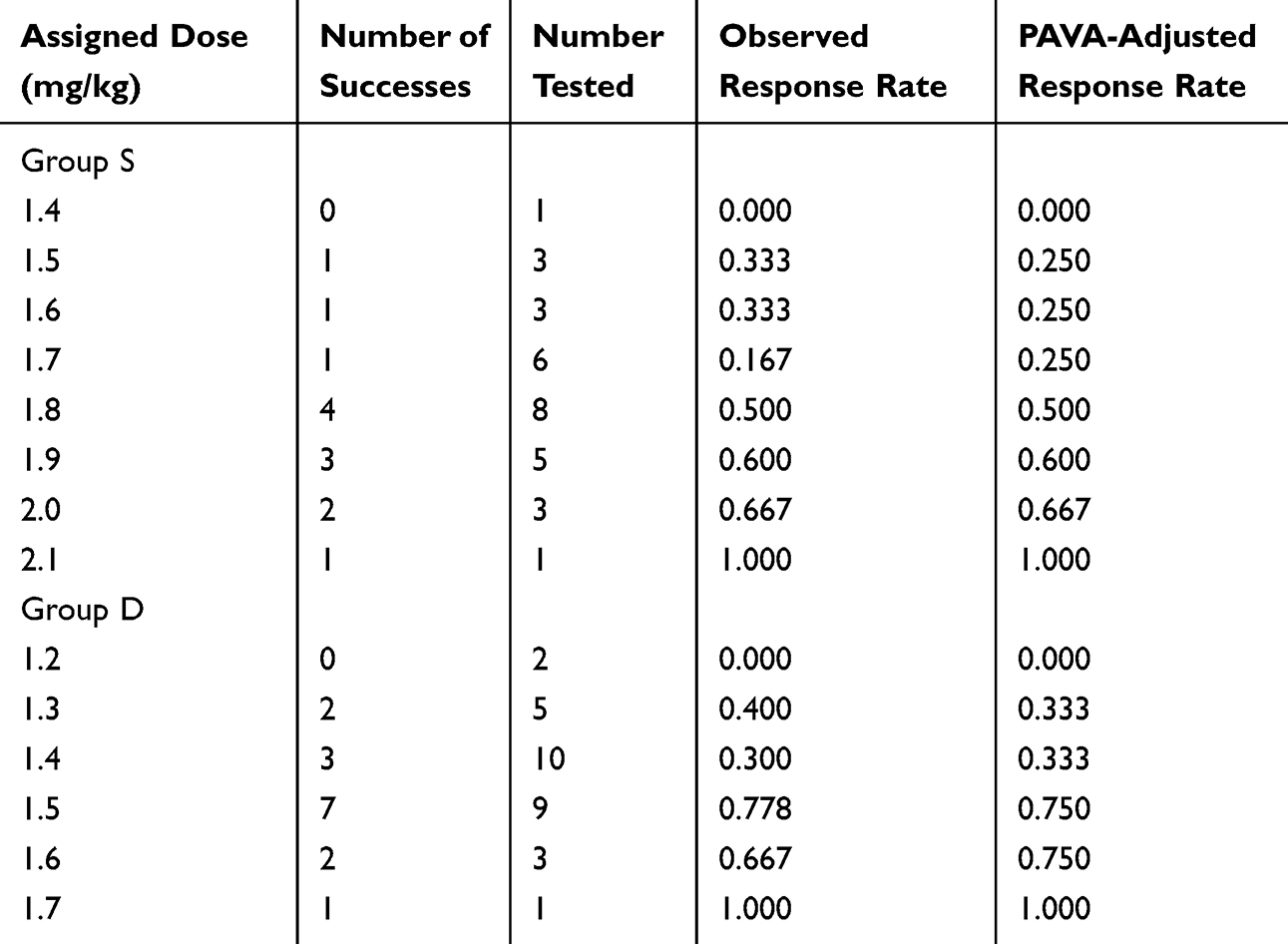 |
Table 3 Observed and Pooled-Adjacent-Violators Algorithm (PAVA)-Adjusted Response Rates |
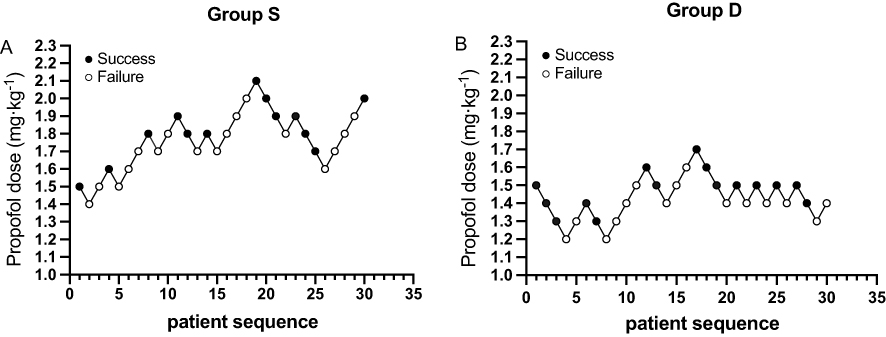 |
Figure 2 Responses of consecutive patients in Group S (A) and Group D (B) to gastroscope insertion using the modified Dixon’s up-and-down method. Note: Solid circles indicate successful insertion doses, whereas open circles indicate failed insertion doses. |
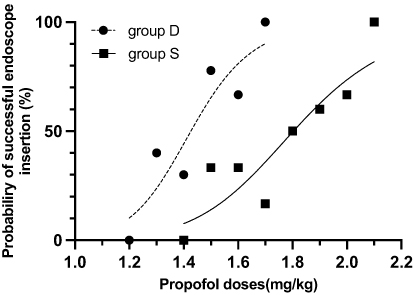 |
Figure 3 Dose-response curve of propofol for successful gastroscope insertion plotted based on isotonic regression analysis. |
Intraoperative findings and recovery outcomes are presented in Table 4. Group D required lower total propofol dose (P < 0.001), demonstrated reduced frequency of propofol supplementation (P = 0.012), and had lower Aldrete scores at PACU discharge (P = 0.010). Endoscopist satisfaction was significantly higher in Group D than in Group S (P = 0.016). Hemodynamic and respiratory changes are shown in Figure 4. Compared with Group S, Group D had significantly lower MAP at time points T8, T9, and T10 (all P < 0.05). Similarly, HR in Group D was significantly lower than that in Group S at T4, T5, and T6 (all P < 0.05). In addition, SpO2 in Group D was significantly higher than that in Group S at T4 (P < 0.05), and RR in Group D was significantly higher than that in Group S at T9 (P < 0.05).
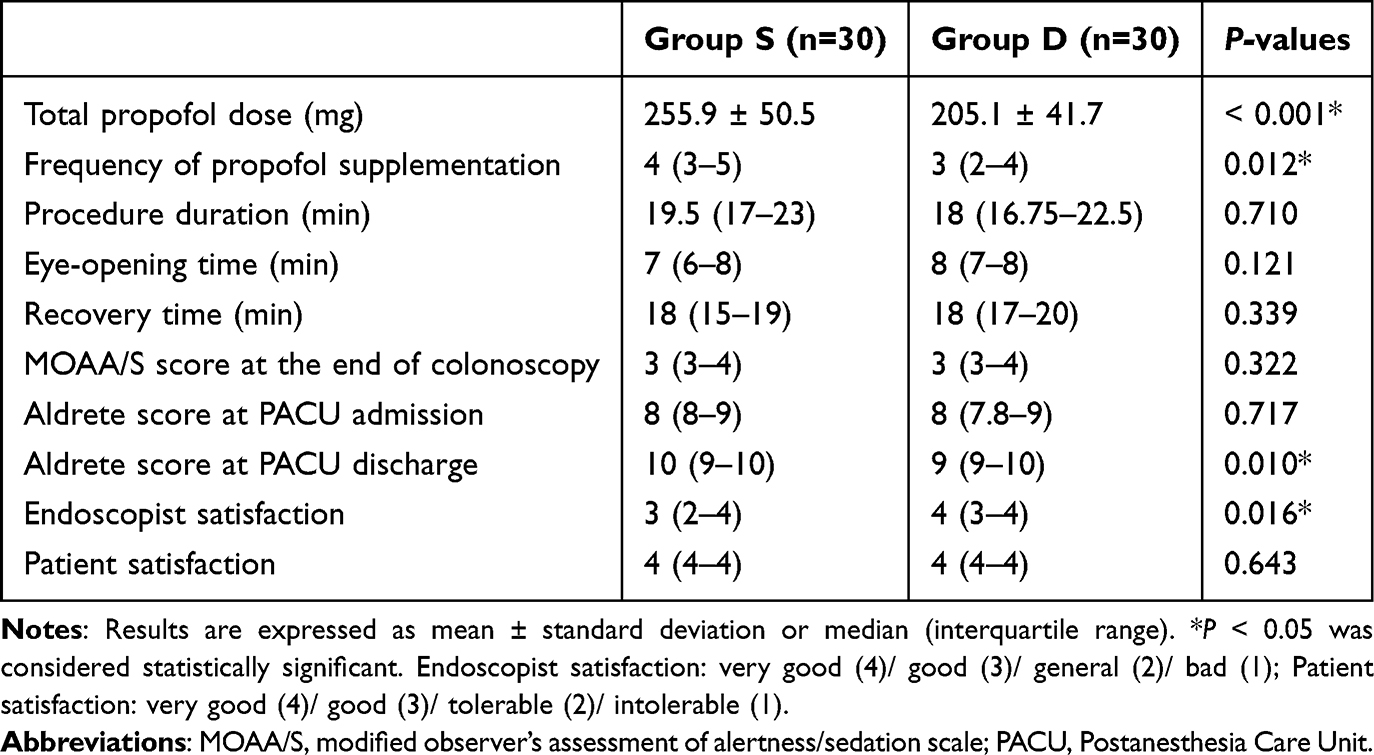 |
Table 4 Intraoperative Findings and Recovery Outcomes |
 |
Figure 4 Changes in MAP (A), HR (B), SpO2 (C), and RR (D) throughout the study period. Abbreviations: HR, heart rate; MAP, mean arterial pressure; RR, respiratory rate; SpO2, pulse oxygen saturation; T0, before propofol administration (baseline); T1, immediately after saline or dexmedetomidine administration; T2, immediately after propofol administration; T3, immediately after gastroscope insertion; T4, 2 min after gastroscope insertion; T5, at the end of gastroscopy; T6, at the beginning of colonoscopy; T7, 5 min after the beginning of colonoscopy; T8, at the end of colonoscopy; T9, at PACU admission; T10, at PACU discharge. Notes: Data are expressed as mean ± standard deviation. *P < 0.05 was considered statistically significant versus Group S. |
Adverse events are summarized in Table 5. Intraoperative subclinical oxygen desaturation was significantly lower in Group D than in Group S (16.7% vs 40.0%; P = 0.045). No patients in Group D experienced intraoperative hypoxia, compared with four patients (13.3%) in Group S (P = 0.112). One case of bradycardia occurred in Group S in a patient with a baseline HR of 61 bpm; the HR decreased to an intraoperative minimum HR of 48 bpm and resolved following atropine administration per protocol.
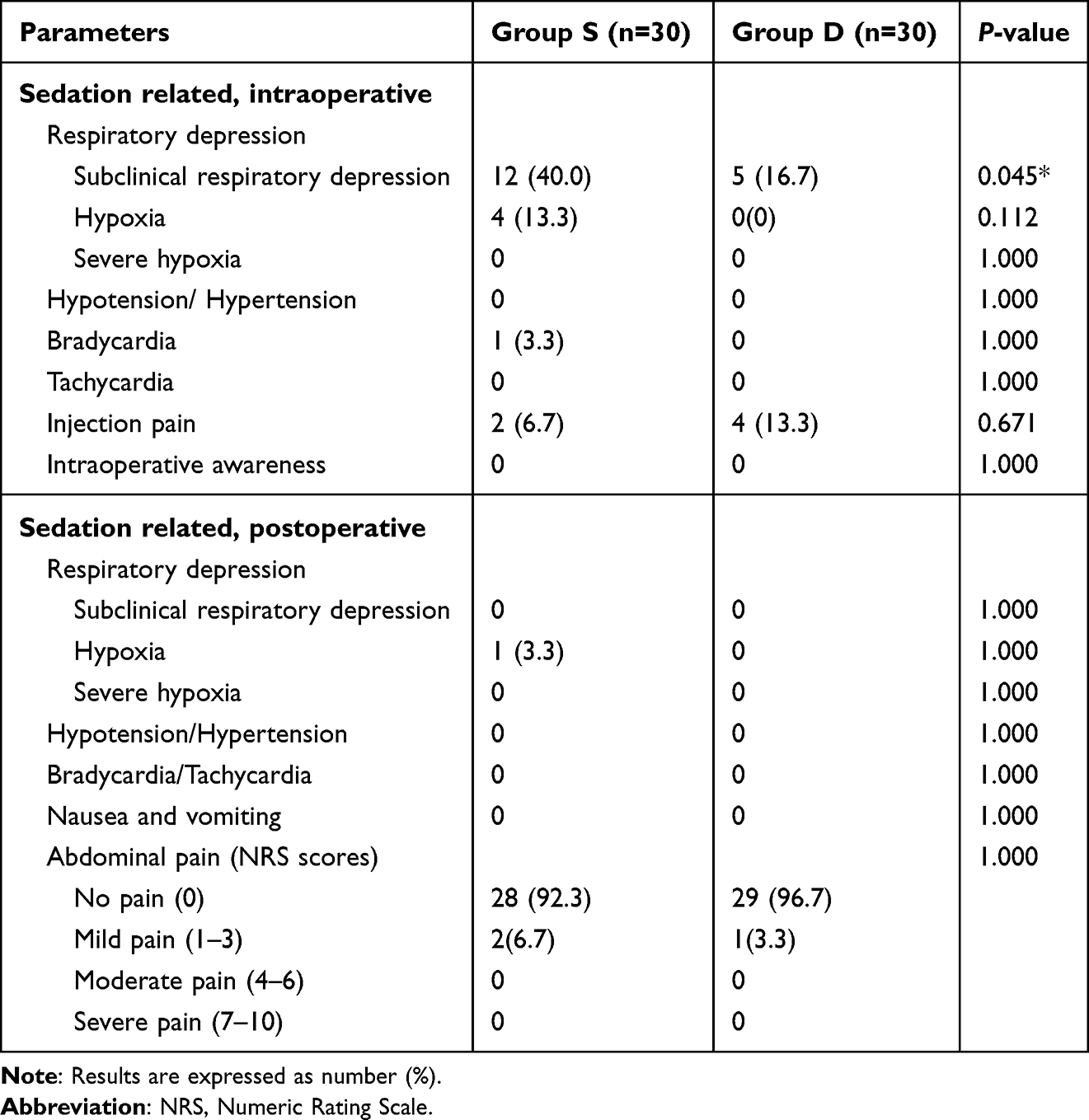 |
Table 5 Adverse Events |
Discussion
Adequate sedation during GIE optimizes patient comfort and procedural efficacy. Therefore, identifying medication regimens that ensure effective sedation while maintaining patient safety is therefore crucial. However, propofol monotherapy often yields suboptimal sedation during GIE due to its narrow therapeutic index. As a highly selective α2- adrenergic receptor agonist, dexmedetomidine has sedative, analgesic, and sympatholytic properties, and provides significant anesthetic and opioid-sparing effects by decreasing sympathetic outflow, increasing parasympathetic outflow, and influencing endogenous sleep-promoting pathways.16,20,41,42
However, dexmedetomidine administration necessitates hemodynamic consideration due to its biphasic, dose- and rate-dependent effects on blood pressure.16,43,44 Beyond its therapeutic benefits, higher loading doses increase the risk of hypotension and bradycardia. Zhao et al29 demonstrated that lower loading doses (0.5 µg/kg) reduce hemodynamic fluctuations compared to 0.75–1 µg/kg, significantly reducing the prevalence of bradycardia in particular. Kwak et al45 determined that the ED50 of dexmedetomidine for successful laryngeal mask airway insertion with propofol 2.0 mg/kg was 0.55 (95% CI, 0.44–0.66) µg/kg. Further supporting a cautious dosing approach, Edokpolo et al24 observed that low-dose dexmedetomidine (0.3 µg/kg) reduced propofol consumption without increasing the incidence of sustained bradycardia during colonoscopy. Consequently, based on this emerging favoring lower doses for stability, we selected a loading dose of 0.3 µg/kg in this study.
Our study demonstrated the efficacy of dexmedetomidine as an adjunct to propofol, with low-dose dexmedetomidine (0.3 µg/kg) significantly reducing the dose of propofol required for successful gastroscope insertion. Using the MDUDM, we observed that the ED50 of propofol for successful gastroscope insertion was 18.7% lower in Group D than in Group S (1.48 ± 0.10 mg/kg vs 1.82 ± 0.16 mg/kg; P < 0.001). Using isotonic regression analysis, we confirmed this dose-sparing effect with non-overlapping 83% CIs for both the ED50 and ED95 between the two groups.33 The ED50 and ED95 of propofol for successful gastroscope insertion in Group S were 1.80 mg/kg (83% CI, 1.649–1.882) and 2.10 mg/kg (83% CI, 2.081–2.124), respectively. In Group D, these values decreased to 1.40 mg/kg (83% CI, 1.297–1.452) and 1.70 mg/kg (83% CI, 1.667–1.753), respectively. This methodology provides statistical advantages including low bias and variance, which enable precise estimation of a response along the dose-response curve at any point (quantile).36,46–48 Group D exhibited a left-shifted dose-response curve, indicating that low-dose dexmedetomidine (0.3 µg/kg) enhanced propofol efficacy. However, the ED95 of propofol for successful gastroscope insertion are exploratory and should be interpreted with caution, serving to generate hypotheses for future research.
Previous studies across a range of procedures support our findings. Dutta et al28 reported that premedication with dexmedetomidine (1 µg/kg) in propofol total intravenous anesthesia via closed-loop control reduced the propofol induction dose by 15% and the propofol maintenance requirements by 29% in healthy subjects. Similarly, in the context of colonoscopy, Edokpolo et al24 observed that low-dose dexmedetomidine (0.3 µg/kg) significantly reduced propofol consumption compared with propofol alone (140 µg kg−1 min−1 vs 180 µg kg−1 min−1; P = 0.011). Chen et al25 demonstrated that co-administrating dexmedetomidine (0.5 or 1.0 µg/kg) reduced the EC50 of propofol via plasma target-controlled infusion by 33.4% and 44.3%, respectively, compared with the Group Control during GIE. These authors noted that these combinations of dexmedetomidine and propofol lowered HR without causing bradycardia, stabilized MAP and did not cause prolonged recovery time. Extending these benefits to surgical settings, Zheng et al26 reported that premedication with low-dose dexmedetomidine (0.5 µg/kg) can effectively reduce postoperative pain and intraoperative stress response, preserve perioperative hemodynamic stability, shorten the recovery period from anesthesia, decrease anesthetic requirements, and lower the risk of adverse events during laparoscopic cholecystectomy. In airway management, Ganesh et al20 observed that Low-dose dexmedetomidine (0.5 µg/kg) significantly reduced the EC50 of propofol for I-gel insertion with propofol target-controlled infusion compared with fentanyl, with no significant change to the hemodynamic profile. Likewise, for hysteroscopy, Zhang et al27 reported that low-dose dexmedetomidine (0.5 µg/kg) reduced the required propofol dose by approximately 45% for suppressing body movement without introducing additional adverse effects. These consistent findings across diverse clinical scenarios underscore the robustness of the dexmedetomidine-propofol synergistic interaction.
Liu et al30 reported the ED50 and ED95 of propofol required for successful endoscope insertion as 1.90 mg/kg (95% CI, 1.78–2.10) and 2.15 mg/kg (95% CI, 2.01–3.56), respectively, using probit regression analysis. Similarly, Qi et al49 determined the corresponding values to be 1.86 mg/kg (95% CI, 1.74–2.10) and 2.20 mg/kg (95% CI, 2.01–3.56), using the same method. Using isotonic regression analysis, our findings for Group S are consistent with these results, thereby validating our experimental model and baseline parameters.
Respiratory depression remains a significant clinical challenge during propofol-sedated GIE. In our study, the combination of dexmedetomidine with propofol markedly improved propofol-induced respiratory depression. Intraoperative subclinical oxygen desaturation occurred significantly less frequently in Group D than in Group S (16.7% vs 40.0%; P = 0.045). None of the patients in Group D experienced intraoperative hypoxia, compared with four in Group S (0% vs 13.3%; P = 0.112). This clinically important reduction in respiratory compromise in line with those of previous studies which also attribute it to the lower total dose of the respiratory depressant (propofol) required when dexmedetomidine is co-administered.11,27
Dexmedetomidine elicits biphasic hemodynamic effects: Low plasma concentrations cause hypotension, while high plasma concentrations cause hypertension.16,23,50 In our study, premedication with low-dose dexmedetomidine (0.3 µg/kg over 5 min) followed by propofol induction resulted in slight decreases in MAP, without inducing hypertension or hypotension. This may be attributed to the minimal changes in plasma concentration associated with a slow, controlled administration. Considerable bradycardia has been observed when dexmedetomidine is used alone for sedation, and dose-dependent bradycardia is a documented side effect of the drug.51,52 However, we did not find a statistically significant difference in the incidence of bradycardia, although a trend toward decreased HR was observed. One patient in Group S experienced bradycardia. This patient had a baseline HR of 61 bpm and an intraoperative minimum HR of 48 bpm, which was resolved with atropine. No cases of bradycardia were observed in Group D. This may result from sympathetic activation during endoscope insertion counteracting dexmedetomidine’s bradycardic effects, a procedural factor that may distinguish our study from those with less stimulus. Furthermore, this method of administration significantly enhanced endoscopist satisfaction without prolonging recovery time compared with propofol alone. This combination thus provides adequate sedation while reducing adverse events, demonstrating notable clinical utility. These findings align with those of several studies on low-dose dexmedetomidine.20,25,27 We propose that these observed effects should be attributed to the decreased propofol dose and reduced frequency of propofol supplementation, which mitigates dose-related adverse events.
However, these findings partially contradict to these of previous studies. Edokpolo et al24 observed that, compared with propofol alone, the combination of low-dose dexmedetomidine (0.3 µg/kg) and propofol caused hypotension and delayed readiness for anesthesia discharge in ambulatory colonoscopy. Zhao et al29 reported that different dexmedetomidine loading doses (0.5, 0.75, and 1 µg/kg in 10 min) significantly increased the prevalence of bradycardia compared with propofol alone. Dutta et al23 demonstrated that adding dexmedetomidine (1 µg/kg over 10 min) to propofol, delivered via a closed-loop anesthesia delivery system, was associated with an increased incidence of early postoperative sedation and hemodynamic depression. Thus, current studies have consistently confirmed the efficacy of low-dose dexmedetomidine under propofol anesthesia in gastrointestinal endoscopy (GIE). However, controversy remains regarding its side effects, which may be related to subtle variations in dexmedetomidine dosage, infusion rate, patient characteristics, and the procedure or surgery performed. Our findings suggest that a very low dose (0.3 µg/kg) infused slowly (over 5 minutes) for sequential upper and lower GIE may offer a favorable balance, minimizing hemodynamic side effects while preserving efficacy.
Several factors may influence the interpretation and generalizability of our findings. First, the administration strategy of dexmedetomidine, particularly its dosage and infusion duration, is critical. We administered a 0.3 µg/kg dose over 5 minutes, which is a lower dosage and slower infusion rate than those used in some alternative protocols; this regimen may attenuate the initial hypertensive response and subsequent bradycardia associated with dexmedetomidine use. Second, patient-related characteristics contribute to the study outcomes. Our cohort was restricted to ASA physical status I–II patients with normal organ function, who typically exhibit more stable hemodynamic reserves and predictable pharmacokinetic profiles. Notably, the sympathetic activation induced by sequential gastroscopy and colonoscopy in our study may have counterbalanced the bradycardic effects of dexmedetomidine, whereas this modulating factor is absent in studies focusing on less stimulating, single-procedure interventions. Third, the operational definition of procedural success (ie, successful gastroscope insertion with a MOAA/S score ≤1) and the use of propofol bolus injections instead of target-controlled infusion (TCI) may limit direct dose comparisons with other studies employing different methodological approaches. Collectively, these factors shape the observed trade-off between sedation efficacy and adverse events in our cohort.
The novel insights generated by this study are multifaceted and clinically relevant. First, the study provides precise estimates of the ED50 and ED95 of propofol for gastroscope insertion, both as a monotherapy and in combination with a specific low-dose dexmedetomidine regimen (0.3 µg/kg administered over 5 min), using a statistically robust isotonic regression approach. This quantification clarifies the 18.7% propofol-sparing effect of the dexmedetomidine adjuvant in the specific clinical context of sequential gastrointestinal endoscopy (GIE). Second, the research demonstrates that this low-dose, slow-infusion dexmedetomidine protocol achieves this propofol-sparing effect without translating the well-documented hemodynamic risks of dexmedetomidine into a statistically significant elevation in clinical adverse events among ASA physical status I–II patients. Third, and perhaps most clinically impactful, the study reveals that the reduction in propofol dosage directly correlates with a measurable decrease in the incidence of propofol-induced respiratory depression (specifically subclinical oxygen desaturation), thereby enhancing the safety profile of deep sedation for GIE procedures. These findings position the propofol-dexmedetomidine combination not merely as an efficacious alternative to propofol monotherapy, but as a potentially safer sedation strategy for clinical practice.
Based on the present study findings, we propose the following evidence-based recommendations for clinical practice: For ASA physical status I–II patients undergoing elective GIE under propofol sedation, premedication with a 0.3 µg/kg dexmedetomidine infusion administered over 5 minutes prior to propofol induction constitutes a clinically viable strategy. This regimen can reduce the required propofol dosage by approximately 20%, with the following anticipated benefits: (1) Mitigating the risk of dose-dependent respiratory depression and hypoxia, thereby enhancing procedural safety—an advantage that is particularly valuable in clinical settings with limited airway rescue resources; (2) Preserving hemodynamic stability, provided that the dexmedetomidine infusion is administered at a slow rate and patients are subjected to rigorous selection criteria. Clinicians should recognize that the sympathetic activation induced by the endoscopic procedure itself may confer partial protection against dexmedetomidine-associated bradycardia. This combined sedation protocol may be of particular benefit to patients with obesity or mild obstructive sleep apnea, populations in which minimizing exposure to respiratory depressants is of critical importance. Nevertheless, vigilant intraoperative monitoring for bradycardia and hypotension remains mandatory. Future clinical protocols may integrate this propofol-dexmedetomidine combination to establish a “low-propofol” sedation strategy, aiming to balance efficacy, patient safety, and faster recovery.
However, there are several limitations that warrant consideration. Firstly, sedation depth was assessed solely via the MOAA/S scale, which is a subjective measure lacking objective indicators such as bispectral index (BIS) monitoring. Although Olutoye et al53 reported no association between BIS values < 60 and loss of consciousness when determining the effective doses of propofol. The inherent lag of BIS monitoring, which results from averaging values over preceding time intervals, may limit its ability to capture rapid physiological changes during anesthesia induction. Future studies should still integrate the sedation depth scale with objective neurophysiological monitoring to comprehensively assess anesthesia depth. Secondly, enrollment was restricted to only relatively healthy patients (ASA physical status I–II) with normal hepatic and renal function. This excluded older and higher-risk individuals (ASA physical status III–IV), who may exhibit greater propofol sensitivity. Thirdly, although sequential designs enhance efficiency for dose estimation, data non-independence may bias covariate estimates (eg, age and gender). Future studies should stratify by these variables and include diverse populations to improve generalizability. As all study participants were of Chinese descent, these findings may not be generalizable to adults of all ethnicities and races undergoing outpatient gastrointestinal endoscopy (GIE). Further large-scale research is required to more precisely assess the anesthetic-sparing effect of low-dose dexmedetomidine on propofol.
Conclusion
Low-dose dexmedetomidine (0.3 µg/kg) significantly reduces the median effective doses of propofol required for successful gastroscope insertion. The combination of dexmedetomidine and propofol is safe and effective, reducing adverse events during painless GIE.
Data Sharing Statement
The data generated during the study are available from the corresponding author, Professor Fu-Shan Xue, upon reasonable request.
Acknowledgments
The authors express their gratitude to all the staff at the Gastrointestinal Endoscopy Center of Beijing Friendship Hospital and other participants who dedicated their time to the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng HR, Zhang XQ, Li LZ, et al. Multicentre prospective cohort study evaluating gastroscopy without sedation in China. Br J Anaesth. 2018;121(2):508–13. doi:10.1016/j.bja.2018.04.027
2. Committee ASoP; Early DS, Lightdale JR, Vargo JJ, et al. Guidelines for sedation and anesthesia in GI endoscopy. Gastrointest Endosc. 2018;87(2):327–337. doi:10.1016/j.gie.2017.07.018
3. Hinkelbein J, Lamperti M, Akeson J, et al. European society of anaesthesiology and European board of anaesthesiology guidelines for procedural sedation and analgesia in adults. Eur J Anaesthesiol. 2018;35(1):6–24. doi:10.1097/EJA.0000000000000683
4. Stogiannou D, Protopapas A, Protopapas A, Tziomalos K. Is propofol the optimal sedative in gastrointestinal endoscopy? Acta Gastroenterol Belg. 2018;81(4):520–524.
5. Park HJ, Kim BW, Lee JK, et al. 2021 Korean society of gastrointestinal endoscopy clinical practice guidelines for endoscopic sedation. Clin Endosc. 2022;55(2):167–182. doi:10.5946/ce.2021.282
6. Ang TL, Seet E, Goh YC, et al. Academy of medicine, Singapore clinical guideline on the use of sedation by non-anaesthesiologists during gastrointestinal endoscopy in the hospital setting. Ann Acad Med Singap. 2022;51(1):24–39. doi:10.47102/annals-acadmedsg.2021306
7. Sidhu R, Turnbull D, Newton M, et al. Deep sedation and anaesthesia in complex gastrointestinal endoscopy: a joint position statement endorsed by the British society of gastroenterology (BSG), joint advisory group (JAG) and royal college of anaesthetists (RCoA). Frontline Gastroenterol. 2019;10(2):141–147. doi:10.1136/flgastro-2018-101145
8. Sahinovic MM, Struys M, Absalom AR. Clinical pharmacokinetics and pharmacodynamics of propofol. Clin Pharmacokinet. 2018;57(12):1539–1558. doi:10.1007/s40262-018-0672-3
9. Kaye AD, Rogers BN, Carrera CY, Urman RD, Azhar S, Shekoohi S. Sedation technique considerations for nonoperating room anesthesia: a narrative review and update. Curr Opin Anaesthesiol. 2025;38(4):435–442. doi:10.1097/ACO.0000000000001541
10. Brown EN, Pavone KJ, Naranjo M. Multimodal general anesthesia: theory and practice. Anesth Analg. 2018;127(5):1246–1258. doi:10.1213/ANE.0000000000003668
11. Liu Y, Shen Y, Zhong H. Dexmedetomidine-propofol versus propofol alone for sedation in upper gastrointestinal endoscopic ultrasound: a randomized comparative study. Clin Ther. 2025;47(8):554–558. doi:10.1016/j.clinthera.2025.05.013
12. Beloeil H, Garot M, Lebuffe G, et al. Balanced opioid-free anesthesia with dexmedetomidine versus balanced anesthesia with remifentanil for major or intermediate noncardiac surgery. Anesthesiology. 2021;134(4):541–551. doi:10.1097/aln.0000000000003725
13. Feng CD, Xu Y, Chen S, et al. Opioid-free anaesthesia reduces postoperative nausea and vomiting after thoracoscopic lung resection: a randomised controlled trial. Br J Anaesth. 2024;132(2):267–276. doi:10.1016/j.bja.2023.11.008
14. Goudra B, Gouda G, Mohinder P. Recent developments in drugs for GI endoscopy sedation. Dig Dis Sci. 2020;65(10):2781–2788. doi:10.1007/s10620-020-06044-5
15. Kamibayashi T, Maze M, Weiskopf R, Weiskopf R, Todd M. Clinical uses of alpha2 -adrenergic agonists. Anesthesiology. 2000;93(5):1345–1349. doi:10.1097/00000542-200011000-00030
16. Weerink MAS, Struys M, Hannivoort LN, Barends CRM, Absalom AR, Colin P. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
17. Ding L, Zhang H, Mi W, et al. Effects of dexmedetomidine on anesthesia recovery period and postoperative cognitive function of patients after robot-assisted laparoscopic radical cystectomy. Int J Clin Exp Med. 2015;8(7):11388–11395.
18. Candiotti KA, Bergese SD, Bokesch PM, Feldman MA, Wisemandle W, Bekker AY. Monitored anesthesia care with dexmedetomidine: a prospective, randomized, double-blind, multicenter trial. Anesth Analg. 2010;110(1):47–56. doi:10.1213/ane.0b013e3181ae0856
19. Bhana N, Goa KL, McClellan KJ. Dexmedetomidine. Drugs. 2000;59(2):263–268. discussion 269-70. doi:10.2165/00003495-200059020-00012
20. Ganesh V, Luthra A, Amburu V, Naik BN, Singh A, Puri GD. Low-dose dexmedetomidine reduces median effective concentration (EC 50) of propofol more than fentanyl in unparalysed anaesthetised patients for I-gel insertion: a randomised controlled trial. Anaesth Crit Care Pain Med. 2021;40(2):100815. doi:10.1016/j.accpm.2021.100815
21. Wan L, Shao LJ, Liu Y, Wang HX, Xue FS, Tian M. Dexmedetomidine reduces sevoflurane EC(50) for supraglottic airway device insertion in spontaneously breathing morbidly obese patients. Ther Clin Risk Manag. 2019;15:627–635. doi:10.2147/tcrm.S199440
22. Le Guen M, Liu N, Tounou F, et al. Dexmedetomidine reduces propofol and remifentanil requirements during bispectral index-guided closed-loop anesthesia: a double-blind, placebo-controlled trial. Anesth Analg. 2014;118(5):946–955. doi:10.1213/ane.0000000000000185
23. Dutta A, Sethi N, Sood J, et al. The effect of dexmedetomidine on propofol requirements during anesthesia administered by bispectral index-guided closed-loop anesthesia delivery system: a randomized controlled study. Anesth Analg. 2019;129(1):84–91. doi:10.1213/ane.0000000000003470
24. Edokpolo LU, Mastriano DJ, Serafin J, Weedon JC, Siddiqui MT, Dimaculangan DP. Discharge readiness after propofol with or without dexmedetomidine for colonoscopy: a randomized controlled trial. Anesthesiology. 2019;131(2):279–286. doi:10.1097/ALN.0000000000002809
25. Chen HY, Deng F, Tang SH, Liu W, Yang H, Song JC. Effect of different doses of dexmedetomidine on the median effective concentration of propofol during gastrointestinal endoscopy: a randomized controlled trial. Br J Clin Pharmacol. 2023;89(6):1799–1808. doi:10.1111/bcp.15647
26. Zheng L, Fang T, Zhang W, et al. Beneficial effects of low-dose intravenous dexmedetomidine premedication in patient undergoing laparoscopic cholecystectomy under general anesthesia: a prospective, double-blind, randomized controlled trial. Drug Des Devel Ther. 2024;18:443–452. doi:10.2147/dddt.S452077
27. Zhang XF, Xiao F, Lou YY, Wu KW, Qian J, Zhu GW. Low-dose dexmedetomidine attenuates the dose requirement of propofol for suppression of body movement in patients undergoing operative hysteroscopy. Drug Des Devel Ther. 2025;19:1185–1193. doi:10.2147/DDDT.S503538
28. Dutta S, Karol MD, Cohen T, Jones RM, Mant T. Effect of dexmedetomidine on propofol requirements in healthy subjects. J Pharm Sci Feb. 2001;90(2):172–181. doi:10.1002/1520-6017(200102)90:2<172::aid-jps8>3.0.co;2-j
29. Zhao XN, Ran JH, Bajracharya AR, Ma MY. Effect of different doses of dexmedetomidine on median effective concentration of propofol for anesthesia induction: a randomized controlled trial. Eur Rev Med Pharmacol Sci. 2016;20(14):3134–3143.
30. Liu FK, Wan L, Shao LJZ, Zou Y, Liu SH, Xue FS. Estimation of effective dose of propofol mono-sedation for successful insertion of upper gastrointestinal endoscope in healthy, non-obese Chinese adults. J Clin Pharm Ther. 2021;46(2):484–491. doi:10.1111/jcpt.13312
31. Hao PP, Tian T, Hu B, et al. Long-term high-risk drinking does not change effective doses of propofol for successful insertion of gastroscope in Chinese male patients. BMC Anesthesiol. 2022;22(1):183. doi:10.1186/s12871-022-01725-2
32. Dixon WJ. Staircase bioassay: the up-and-down method. Neurosci Biobehav Rev. 1991;15(1):47–50. doi:10.1016/s0149-7634(05)80090-9
33. Oron AP, Souter MJ, Flournoy N. Understanding research methods: up-and-down designs for dose-finding. Anesthesiology. 2022;137(2):137–150. doi:10.1097/ALN.0000000000004282
34. Allen ML. Safety of deep sedation in the endoscopy suite. Curr Opin Anaesthesiol. 2017;30(4):501–506. doi:10.1097/aco.0000000000000479
35. Kashiwagi K, Hosoe N, Takahashi K, et al. Prospective, randomized, placebo-controlled trial evaluating the efficacy and safety of propofol sedation by anesthesiologists and gastroenterologist-led teams using computer-assisted personalized sedation during upper and lower gastrointestinal endoscopy. Dig Endosc. 2016;28(6):657–664. doi:10.1111/den.12678
36. Pace NL, Stylianou MP, Warltier DC. Advances in and limitations of up-and-down methodology: a précis of clinical use, study design, and dose estimation in anesthesia research. Anesthesiology. 2007;107(1):144–152. doi:10.1097/01.anes.0000267514.42592.2a
37. Görges M, Zhou G, Brant R, Ansermino JM. Sequential allocation trial design in anesthesia: an introduction to methods, modeling, and clinical applications. Paediatr Anaesth. 2017;27(3):240–247. doi:10.1111/pan.13088
38. Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth. 1995;7(1):89–91. doi:10.1016/0952-8180(94)00001-k
39. Lin Y, Zhang X, Li L, et al. High-flow nasal cannula oxygen therapy and hypoxia during gastroscopy with propofol sedation: a randomized multicenter clinical trial. Gastrointest Endosc. 2019;90(4):591–601. doi:10.1016/j.gie.2019.06.033
40. Payton ME, Greenstone MH, Schenker N. Overlapping confidence intervals or standard error intervals: what do they mean in terms of statistical significance? J Insect Sci. 2003;3(34):34. doi:10.1093/jis/3.1.34
41. Kang WS, Kim SY, Son JC, et al. The effect of dexmedetomidine on the adjuvant propofol requirement and intraoperative hemodynamics during remifentanil-based anesthesia. Korean J Anesthesiol. 2012;62(2):113–118. doi:10.4097/kjae.2012.62.2.113
42. Park HY, Kim JY, Cho SH, Lee D, Kwak HJ. The effect of low-dose dexmedetomidine on hemodynamics and anesthetic requirement during bis-spectral index-guided total intravenous anesthesia. J Clin Monit Comput. 2016;30(4):429–435. doi:10.1007/s10877-015-9735-2
43. Tufanogullari B, White PF, Peixoto MP, et al. Dexmedetomidine infusion during laparoscopic bariatric surgery: the effect on recovery outcome variables. Anesth Analg. 2008;106(6):1741–1748. doi:10.1213/ane.0b013e318172c47c
44. Hall JE, Uhrich TD, Barney JA, Arain SR, Ebert TJ. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg. 2000;90(3):699–705. doi:10.1097/00000539-200003000-00035
45. Kwak HJ, Min SK, Yoo JY, Park KH, Kim JY. The median effective dose of dexmedetomidine for laryngeal mask airway insertion with propofol 2.0 mg/kg. Acta Anaesthesiol Scand. 2014;58(7):815–819. doi:10.1111/aas.12338
46. Coppens M, Anssens S, Parashchanka A, et al. Determination of the median effective dose (ED50) of spinal chloroprocaine in labour analgesia. Anaesthesia. 2017;72(5):598–602. doi:10.1111/anae.13808
47. Stylianou M, Flournoy N. Dose finding using the biased coin up-and-down design and isotonic regression. Biometrics. 2002;58(1):171–177. doi:10.1111/j.0006-341x.2002.00171.x
48. Stylianou M, Proschan M, Flournoy N. Estimating the probability of toxicity at the target dose following an up-and-down design. Stat Med. 2003;22(4):535–543. doi:10.1002/sim.1351
49. Qi XR, Sun JY, An LX, Zhang K. Effect of intravenous lidocaine on the ED(50) of propofol for inserting gastroscope without body movement in adult patients: a randomized, controlled study. BMC Anesthesiol. 2022;22(1):319. doi:10.1186/s12871-022-01861-9
50. Dawes J, Myers D, Gorges M, Zhou G, Ansermino JM, Montgomery CJ. Identifying a rapid bolus dose of dexmedetomidine (ED50) with acceptable hemodynamic outcomes in children. Paediatr Anaesth. 2014;24(12):1260–1267. doi:10.1111/pan.12468
51. Carollo DS, Nossaman BD, Ramadhyani U. Dexmedetomidine: a review of clinical applications. Curr Opin Anaesthesiol. 2008;21(4):457–461. doi:10.1097/ACO.0b013e328305e3ef
52. Jalowiecki P, Rudner R, Gonciarz M, Kawecki P, Petelenz M, Dziurdzik P. Sole use of dexmedetomidine has limited utility for conscious sedation during outpatient colonoscopy. Anesthesiology. 2005;103(2):269–273. doi:10.1097/00000542-200508000-00009
53. Olutoye OA, Yu X, Govindan K, et al. The effect of obesity on the ED(95) of propofol for loss of consciousness in children and adolescents. Anesth Analg. 2012;115(1):147–153. doi:10.1213/ANE.0b013e318256858f
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.