Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Low Aggregate Index of Systemic Inflammation Values Correlate with Favorable Prognosis and High Abundance of Parabacteroides in Hepatocellular Carcinoma
Authors Sun W, Zhou F, Shi C, Xu C, Wang Z, Guo X ![]()
Received 3 May 2025
Accepted for publication 23 October 2025
Published 6 November 2025 Volume 2025:12 Pages 2491—2500
DOI https://doi.org/10.2147/JHC.S538192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Wenju Sun,1,* Fengqin Zhou,2,* Chengyu Shi,3 Congcong Xu,4 Zhihai Wang,4 Xufeng Guo5
1Department II of Radiotherapy, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, Qingdao, Shandong, People’s Republic of China; 2Department of Infectious Diseases, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Hepatobiliary Surgery I, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, Qingdao, Shandong, People’s Republic of China; 4Department of Oncology, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, Qingdao, Shandong, People’s Republic of China; 5Department of Oncology, Renmin Hospital of Wuhan University, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhihai Wang, Department of Oncology, Qingdao Central Hospital, University of Health and Rehabilitation Sciences, No. 127, Siliu South Road, Sifang District, Qingdao, Shandong, 266000, People’s Republic of China, Email [email protected] Xufeng Guo, Department of Oncology, Renmin Hospital of Wuhan University, No. 99 Ziyang Road, Wuhan, Hubei, 430000, People’s Republic of China, Email [email protected]
Purpose: Systemic inflammatory response is reported to occupy a crucial role in the progression of hepatocellular carcinoma (HCC). The prognostic significance of SII and PNI in HCC has been explored, but the prognostic significance of aggregate index of systemic inflammation (AISI) in HCC is still unknown. This study was designed to determine the prognostic significance of AISI in HCC and explain the potential underlying mechanisms via gut microbiota and fecal metabolomic profiling.
Patients and Methods: A cohort of 109 cases of HCC individuals during January 2023 to August 2024 was included into this clinical research, and the clinical information and fresh fecal samples were collected. The fecal samples were collected for 16S rRNA sequence and metabolomics analysis.
Results: Survival analysis revealed that HCC patients in low AISI group tend to experience relatively longer survival time compared with those in high AISI group. Then, we employed ROC analysis to measure the predictive performance of AISI for the survival outcome, and ROC curve showed that levels of AISI had good predictive performance for the survival status with an AUC of 0.771 (95%CI: 0.671– 0.871). 16S rRNA sequencing results revealed that levels of Parabacteroides were up-regulated in the low AISI group, and levels of Fusicatenibacter were up-regulated in the high AISI group. Metabolic analysis demonstrated that cavipetin A, pemptoporphyrin, and 8-Oxo-dGMP with high VIP value were the most distinct fecal metabolites.
Conclusion: AISI is a potential prognostic biomarker in individuals with HCC. A low level of AISI was correlated with high abundance of Parabacteroides and some metabolites, indicating that AISI might affect the prognosis of HCC individuals via the regulations of gut microbes and metabolites.
Keywords: hepatocellular carcinoma, gut microbes, parabacteroides, aggregate index of systemic inflammation, metabolites
Introduction
Hepatocellular carcinoma (HCC) is the most common type in liver cancer, ranking the third most common cause of cancer-related deaths all over the world.1 From the global perspective, the 5-year survival rate of HCC individuals is less than 20%.2 In China, cirrhosis derived from the infection of hepatitis B virus is the most important risk factor for HCC, but nonalcoholic fatty liver disease (NFLD) has arisen as the second cause in recent years.3 Currently, surgical resection is still the first selection for liver cancer individuals in the early phase. However, HCC patients with late TNM stage and postoperative recurrence are not surgical candidates, and systemic anti-tumor therapies, such as immunotherapy and targeted therapy might be their last hope.4 While these therapies are not only limited by relatively low response rates but also by a tendency for drug resistance. A comprehensive understanding of the pathological mechanism is vital for designing more effective treatment strategies.5
Recent studies have pointed out that chronic inflammation occupies a significant role in the initiation and progression of HCC.6,7 Chronic inflammation initiates a vicious cycle between HCC and chronic liver diseases, such as NFLD and chronic hepatitis.8 Cancer-related inflammation has been the research hotpot in the field of cancer, and some systemic inflammatory response indexes, such as GRIm score,9 CRP,10 and the systemic immune-inflammation index (SII),11 are proven to be the prognostic biomarker for HCC population. SII was calculated as platelets×neutrophils/lymphocytes, and monocytes are reported to play crucial role in repairing necrotic liver lesions,12 thus should be added into the inflammatory response index. The four indexes derived from blood routine provide a comprehensive reflection of the systemic inflammation in the whole body, which is called aggregate index of systemic inflammation (AISI). Both SII and AISI are accessible and cost-effective markers of systemic inflammation, and AISI incorporates monocyte levels, which is a more comprehensive measure.
The systemic inflammation index, AISI, was based on four immune cells from blood routine, which is very feasible and convenient in the clinical practice. Wang et al13 concluded that high levels of AISI were closely associated with worse prognosis of esophageal cancer and could be served as a reliable biomarker to guide the clinical prognostic assessment of patients with esophageal cancer. However, whether AISI could be used as a prognostic biomarker among HCC population is still unknown. In this study, we first explored the clinical significance and prognostic value of AISI in a Chinese HCC cohort. Then, we investigated the correlation between levels of AISI and gut microbes via 16S rRNA sequencing. Finally, we determined the significant fecal metabolites between the low AISI and high AISI groups via metabolomics.
Materials and Methods
HCC Cohort
This was a prospective clinical study of HCC patients seen at the Wuhan Union hospital from January 2023 to August 2024. The confirmed diagnosis of HCC was based on histopathologic examination. Exclusion criteria were listed as the followings: (1) patients were diagnosed with cholangiocarcinoma; (2) HCC individuals lost for follow-up; (3) HCC patients were complicated by acute infection or hematological diseases. Therefore, a total of 109 cases of HCC were recruited into our cohort. The overall survival time was defined as the total period from diagnosis of HCC to the endpoint or the last follow-up time. AISI was calculated as platelets×monocytes×neutrophils/lymphocytes. The 33rd percentile AISI was used as the cut-off to divide the patients into low AISI group (n=36) and high AISI group (n=73). The fresh fecal samples of HCC individuals were collected within 24 hour on admission, and then stored in -80°C refrigerator for further analysis. This clinical research was adherent to the Helsinki Declaration, and was approved by the Ethics Committee of the Tongji Medical College of Huazhong University of Science and Technology (Approval number: 2023-S117). Moreover, the written informed consent was obtained from all the included HCC individuals.
16S rRNA Sequencing
PF Mag-Bind Stool DNA Kit (Omega Bio-tek, Georgia, US) was used for the extraction of the total microbial genomic DNA. The V3–V4 region of the microbial 16S rRNA gene was amplified, and then determined using MiSeq platform (Illumina, San Diego, California, USA). The statistical analysis and drawing were finished with the aid of the Majorbio Cloud (https://cloud.majorbio.com). Chao index and ACE index were measured to judge the alpha diversity between the AISI and high AISI groups. The compositions of gut bacterium between the low and high AISI groups were analyzed via bar plots. The significant microbes between the low and high AISI groups were determined by the linear discriminant analysis effect size (LEfSe) analysis.
Metabolomics
Metabolome profiling was finished on liquid chromatography-mass spectrometry (LC-MS) using ultra-high performance liquid chromatography (UHPLC) system. The raw metabolomic data were first pre-treated and then analyzed by the progenesis QI software (Waters Corporation, Milford, USA). The statistical analysis and drawing were finished with the aid of the Majorbio Cloud (https://cloud.majorbio.com). Principal component analysis (PCA) was used to visualize the metabolic changes between low AISI group and high AISI group. Generally, fecal metabolites between the low and high AISI groups were considered significant if variable importance in the projection (VIP) >1 along with P<0.05. Moreover, significant metabolites between the low AISI group and high AISI group were further selected for the enrichment analysis.
Statistical Analysis
Continuous data were represented with mean±standard deviation and compared using student t test or non-parametric test where applicable. Categorical indexes were displayed as numbers and compared with X2 test. The prognostic significant of AISI was assessed by the Kaplan–Meier curve, and discrepancies between the low and high AISI groups were determined by the Log rank test. Receiver operating characteristic (ROC) analysis was selected for the quantification of the predictive performance of AISI. The two-sided level of P-value less than 0.05 was regarded as statistically significant. Analyses were performed using IBM SPSS Statistics for Windows (version 19.0) and Graphpad prism (version 5.0).
Results
Clinical Features of 109 HCC Individuals
Based on the three inclusion criterion, a total of 109 HCC patients were selected into our analysis. The average age of the 109 HCC patients was 57.94 years, and the majority of them (85.32%) were male sufferers. The detailed features of the 109 HCC patients were listed in Table S1. The majority of HCC patients (79.82%) exhibited high levels of serum AFP, 66.97% complicated with liver cirrhosis, 37.61% suffered from infection of hepatitis B virus, and 58.72% progressed to the advanced BCLC stage (B-C). Moreover, most of the HCC patients exhibited normal liver function, which was presented by Child-Pugh.
Prognostic Significance of AISI in HCC Patients
We divided the 109 HCC individuals into low AISI group (n=36) and high AISI group (n=73) based on the 33rd percentile of AISI. Results from survival analysis (Figure 1A) revealed that HCC patients in low AISI group (36.975±2.152 month) tend to experience relatively longer survival time compared with those in high AISI group (28.994±1.675 month), and log rank test also validated this result (P=0.035). Univariate and multivariate Cox regression revealed that AISI is a reliable independent prognostic biomarker of HCC (Table S2). Then, we employed ROC analysis to measure the predictive performance of AISI for the survival outcome, and ROC curve showed that levels of AISI had good predictive performance for the survival status with an AUC of 0.771 (95%CI: 0.671–0.871, Figure 1B). Hence, we could conclude that AISI is a reliable biomarker for the prognostic prediction of HCC individuals.
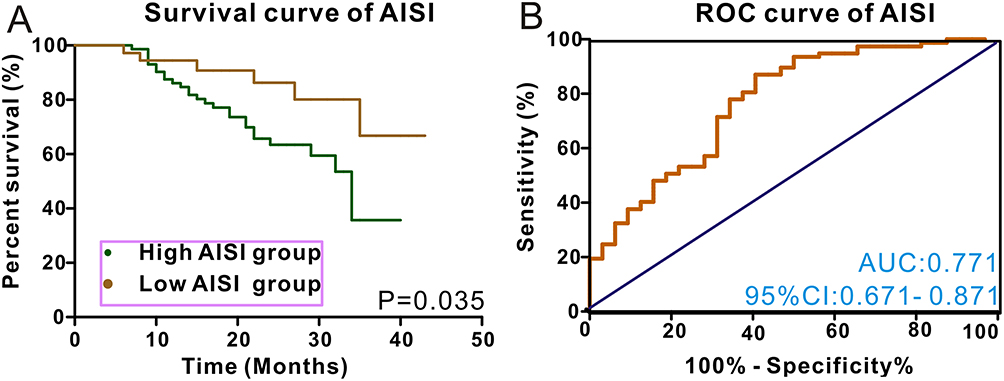 |
Figure 1 Low levels of AISI were correlated with relatively favorable overall survival in HCC individuals (A). ROC analysis exhibits the good performance for predicting survival status of HCC patients (B). |
Correlation Between Levels of AISI and Gut Microbes
16S rRNA sequencing technology was used to determine the most significant gut microbes which are closely associated with the levels of AISI in HCC. Venn plot (Figure 2A) displayed that 139 OTUs are unique to the low AISI group and 428 OTUs are specific to the high AISI group. Alpha diversity measured by Chao index and ACE index demonstrated the significant difference between the two groups (Figure 2B). Microbial community analysis revealed that the abundance of Firmicutes, Actinobacteriota, and Proteobacteria were significantly different between the two groups at the phylum level (Figure 2C). At the genus level, the levels of Blautia, Escherichia-Shigella, Streptococcus, and Bifidobacterium were also different between the two groups (Figure 2D). Further statistical analysis identified that levels of Parabacteroides were up-regulated in the low AISI group (P=0.03736), and levels of Fusicatenibacter were up-regulated in the high AISI group (P=0.02714, Figure 2E). The network between gut microbes and AISI groups are listed in Figure 3A. LEfSe analysis was adopted for the identification of significant bacterium between the two groups (Figure 3B), and Parabacteroides obtained the biggest LDA score in the low AISI group. KEGG enrichment analysis showed that the significant intestinal bacterium between the two groups were most likely to participate in metabolic pathways and biosynthesis of secondary metabolites (Figure 3C). In summary, the correlation between levels of AISI levels and increased abundance of Parabacteroides indicates a potential role of the gut microbiota in modulating systemic inflammation in HCC.
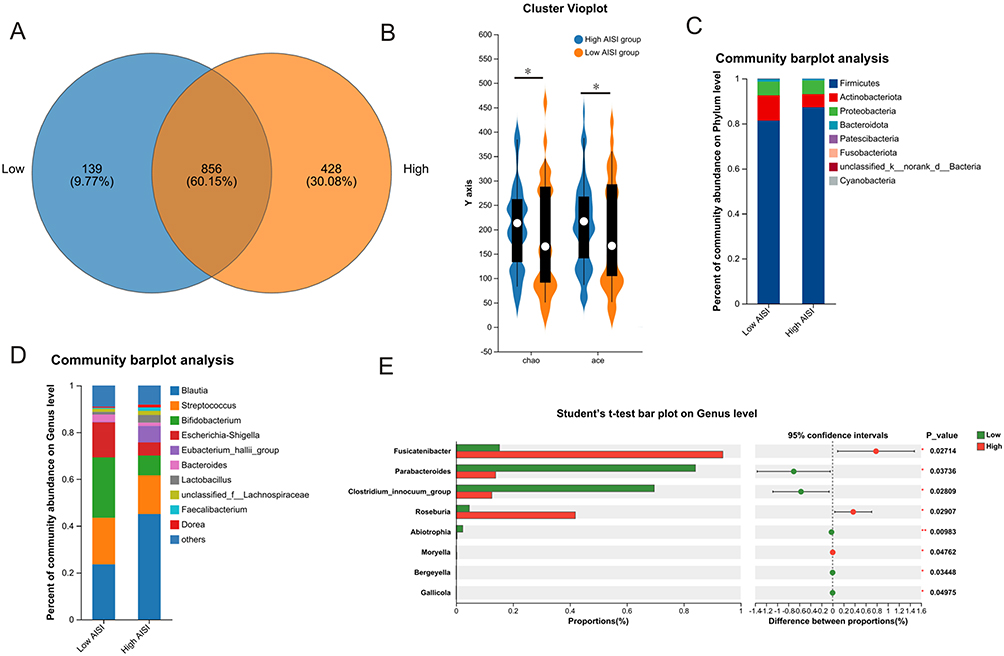 |
Figure 2 Venn plot show the OTUs in the low AISI and high AISI groups (A). The alpha diversity between the two groups measured by Chao and ACE indexed was significantly different (B). The microbial compositions between the two groups at the phylum level (C) and genus level (D). Statistical analysis shows that levels of Parabacteroides were up-regulated in the low AISI group and levels of Fusicatenibacter were up-regulated in the high AISI group (E). Notes: * stands for P<0.05, ** stands for P<0.01. |
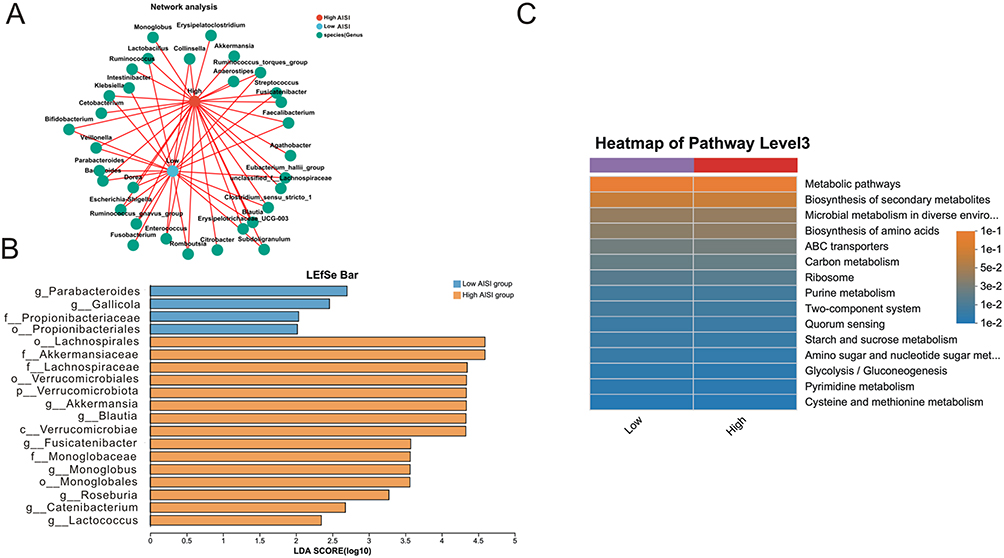 |
Figure 3 (A) Network analysis displayed the distributions of gut microbes between the low AISI and high AISI groups. (B) LEfSe analysis identified the most significant microbes in the low AISI and high AISI groups. (C) KEGG enrichment analysis showed that the significant intestinal bacterium between the two groups were most likely to participate in metabolic pathways and biosynthesis of secondary metabolites. Notes: enviro. stands for environments, met. stands for metabolism. |
Relationship Between Levels of AISI and Metabolites
The fecal metabolites between the low and high AISI groups were determined via metabolic analysis. The low AISI group and high AISI group was basically divided into two parts, which was exhibited in the PCA analysis (Figure 4A). A total of 3568 fecal metabolites were identified from the 109 cases of HCC samples, and the detailed numbers of metabolites between the low AISI group and high AISI group are listed in Figure 4B. The differential metabolites between the low AISI group and high AISI group are exhibited in Figure 4C, and 10 metabolites were up-regulated in low AISI group and 972 metabolites were down-regulated in low AISI group. According to the VIP value, 5 significant metabolites (VIP>2) were cavipetin A, pemptoporphyrin, 8-Oxo-dGMP,(2S)-2-Amino-N-(1S)-7,7-dimethyl-1-4-(2-methylphenyl)pip, Avenestergenin A1, and 5-Penthytetrahydro-2-oxo-3-furancarboxylic acid were the most important fecal metabolites between the two groups (Figure 4D). The levels of five down-regulated metabolites and four up-regulated metabolites in the low AISI group are vividly displayed in Figure 5. The significant fecal metabolites between the low AISI group and high AISI group were mainly involved in biosynthesis of phenylpropanoids and tyrosine metabolism (Figure 6). In brief, levels of AISI were significantly correlated with some metabolites in HCC, such as cavipetin A, pemptoporphyrin, and 8-Oxo-dGMP. The correlation between levels of AISI and the specific faecal metabolites, indicate a potential role of the host metabolism in modulating systemic inflammation in HCC.
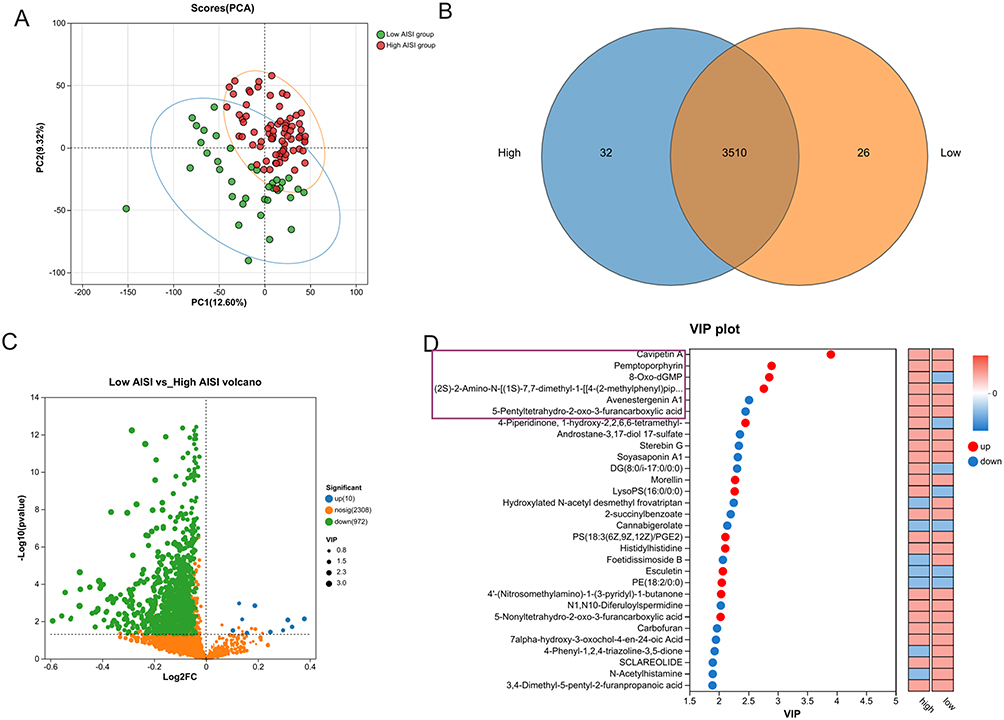 |
Figure 4 PCA demonstrated that the low AISI group and high AISI group was basically divided into two parts (A). Venn plot displayed the fecal metabolites between the low AISI and high AISI groups (B). Hot map shows the up-regulated and down-regulated metabolites between the two groups (C). VIP analysis identified the most important metabolites between the two groups (D). Notes: purple stands for down-regulation, and red stands for up-regulation. |
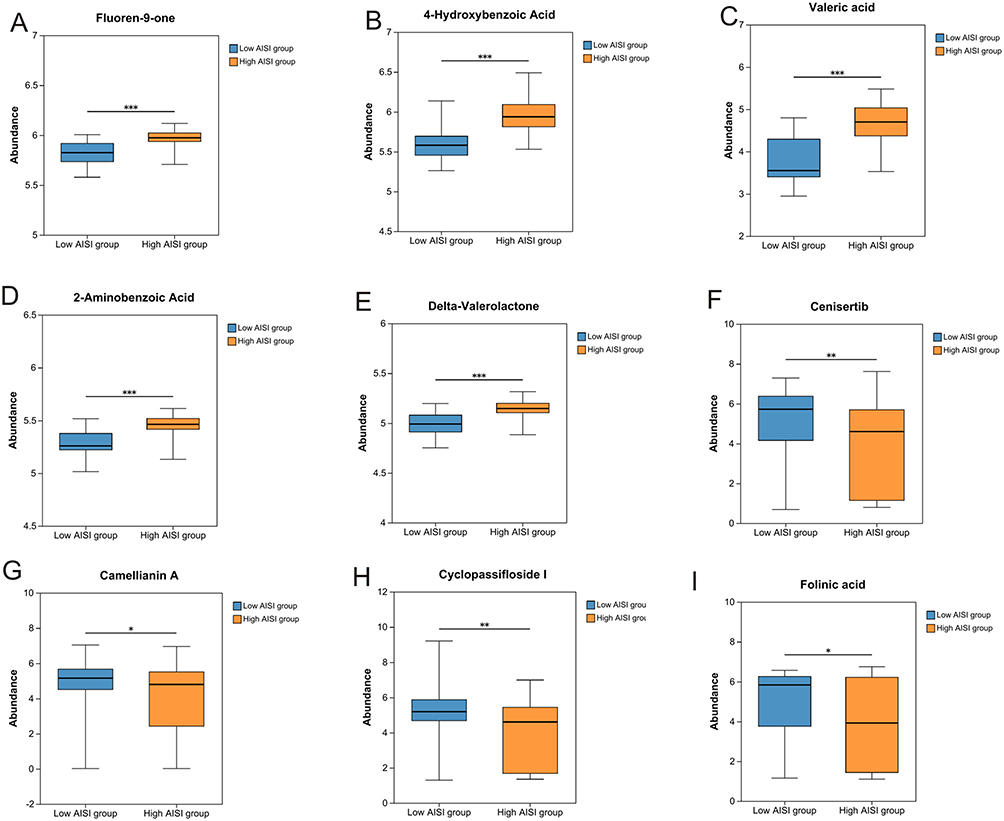 |
Figure 5 The top 9 significant metabolites with down-regulation or up-regulation between the low and high AISI groups. (A) Fluoren-9-one. (B) 4-Hydroxybenzoic acid. (C) Valeric acid. (D) 2-Aminobenzoic acid. (E) Delta-valerolactone. (F) Cenisrtib. (G) Camellianin A. (H) Cyclopassifloside I. (I) Folinic acid. Notes: * stands for P<0.05, ** stands for P<0.01, *** stands for P<0.001. |
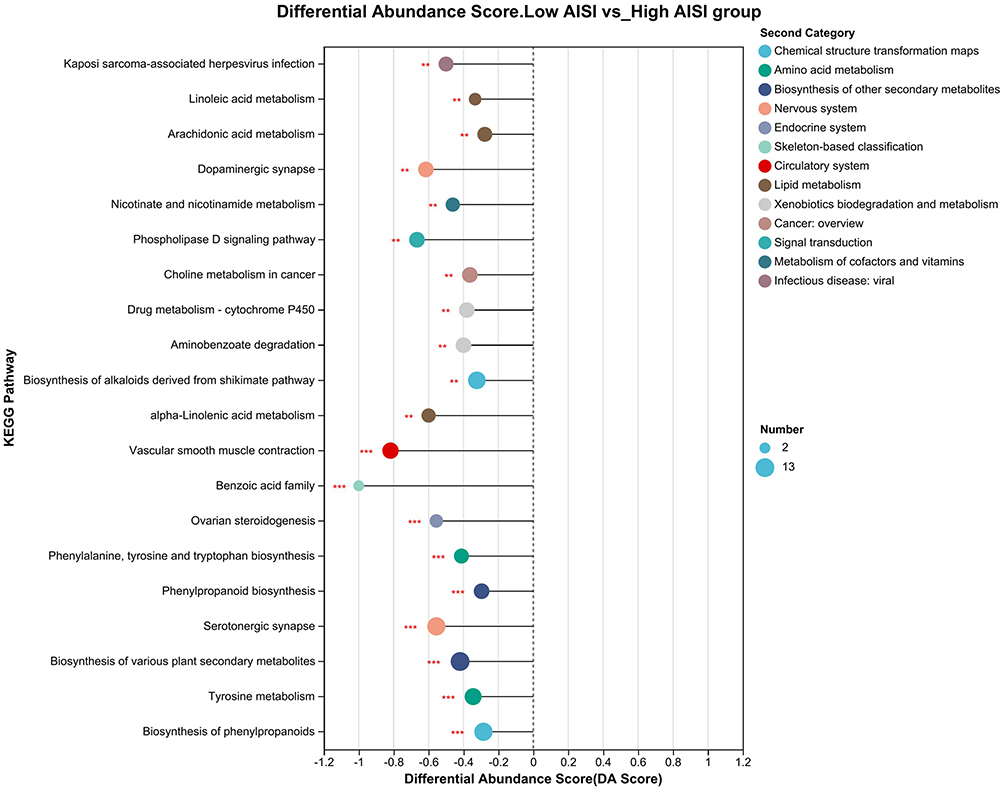 |
Figure 6 KEGG analysis revealed that the significant fecal metabolites between the low AISI group and high AISI group were mainly involved in biosynthesis of phenylpropanoids and tyrosine metabolism. Notes: ** stands for P<0.01, *** stands for P<0.001. |
Discussion
In the present study, we found that HCC patients with high AISI were significantly correlated with unfavorable OS. Subsequent 16S rRNA sequencing revealed that low levels of AISI were significantly correlated with the increased abundance of Parabacteroides. Metabolic analysis identified a panel of fecal metabolites were significantly different between the low and high AISI groups, and low levels of AISI were closely associated with cavipetin A, pemptoporphyrin, 8-Oxo-dGMP. KEGG enrichment analysis identified biosynthesis of phenylpropanoids and tyrosine metabolism as the most important pathways in HCC. Hence, the present study not only identified AISI as a possible prognostic indicator for HCC individuals, but also explored the alterations of gut microbes and fecal metabolites between the low and high AISI groups. Our study indicated a potential role of the gut microbiota and host metabolism in modulating systemic inflammation in HCC.
AISI, a novel systemic inflammation index, was based on four immune cells from blood routine, which is very feasible and convenient in the clinical practice. A series of clinical researches have investigated the survival value of AISI in cancer individuals. Xie et al14 deemed that high levels of AISI were correlated with an increased risk for prostate cancer. A Romania research demonstrated that levels of AISI were significantly correlated with the recurrence of colorectal cancer.15 Huang et al16 reported that high AISI was an independent risk factor for locally advanced intrahepatic cholangiocarcinoma. Feier et al17 found that AISI was a valuable prognostic biomarker for lung cancer individuals, which was validated by a recent Chinese cohort with 266 cases of non-small cell lung cancers.18 To our knowledge, this is the first clinical research revealing the role of AISI in HCC. Consistent with the above findings, AISI is also a possible indicator for predicting the prognosis of HCC individuals.
Although some clinical researches have highlighted the prognostic role of AISI in cancer, the possible mechanism between high AISI and worse survival is still uncertain. As mentioned above, AISI index is consisted of monocyte, platelet, neutrophil and lymphocyte. On the one hand, circulating monocytes have been reported to enhance the growth and migration of tumor cells, and facilitate cancer cells evade from immune surveillance.18 Platelets could promote platelet-tumor cell aggregates, and thus facilitate their entrapment by neutrophil extracellular traps and subsequent remote metastasis of cancer cells.19 Neutrophils play a negative role in anti-tumor immune response via suppressing the activity of effective T lymphocytes and natural killer cells.20 On the another hand, lymphocyte cells are the main force for anti-tumor immune response in the tumor microenvironment, and tumor associated lymphocyte is the key to the efficacy of immunotherapy in HCC.21 Low levels of lymphocytes signify the immunosuppressive tumor microenvironment,22 which facilitates the proliferation and migration of tumor cells.
Gut microbes play a key role in gut homeostasis and the pathophysiology of cancer.23 The complex interplay between gut microbes and systemic inflammation is the research direction in the field of cancer. 16S rRNA sequencing revealed that the microbial compositions between the low and high AISI groups were significantly different, and statistical analysis identified that parabacteroides was the most abundant bacterium in low AISI group. Parabacteroides has been shown to modulate the host mucosal immune system, reduce inflammation, participate in carbon metabolism.24 Parabacteroides may exert a competitive advantage by coordinating the degradation of complex polysaccharides. In addition, Parabacteroides could secret short-chain fatty acids, such as acetate and propionate, which play a positive role in anti-tumor immune response. Hence, we deemed that HCC patients in low AISI groups possessed favorable survival outcome partly due to the high abundance of Parabacteroides.
Both the VIP and differential analysis of metabolomics revealed that cavipetin A is an up-regulated metabolite in patients with low AISI. Cavipetin A belongs to the class of organic compounds known as acyclic diterpenoids. Cavipetin A was involved in the regulation of lipid peroxidation and fatty acid metabolism. A previous study reported that cavipetin could decrease the levels of ROS and oxidative stress.25 Hence, we deemed that cavipetin A plays a protective role in the progression of HCC. In summary, the correlations between levels of AISI and the specific faecal metabolites, indicate a potential role of the host metabolism in modulating systemic inflammation in HCC.
This study also has several shortcomings. First, this was a single-center HCC cohort with only 109 HCC cases, and no external HCC cohorts were available for validation, which may cause various biases. Then, due to the differences in inclusion criteria, the cut-of value of AISI may vary in different cohort. How to gain a unified threshold of AISI for clinical use is an urgent issue. Finally, although we explored the clinical association between levels of AISI and gut microbes, how the gut microbes affect the cancer-associated inflammation is still unknown. Hence, further multi-center clinical trials related to the prognostic role of AISI in HCC and mechanical investigation are still needed in the future.
Conclusion
AISI is a possible prognostic biomarker in HCC patients. The correlations between levels of AISI and increased abundance of Parabacteroides, and the specific faecal metabolites, indicate a potential role of the gut microbiota and host metabolism in modulating systemic inflammation in HCC. Our findings related to AISI needs further research in the future.
Data Sharing Statement
The original data of this study was accessible on reasonable request to the corresponding authors (Xufeng Guo & Zhihai Wang).
Ethics Approval
Ethical approval for the present study was obtained from the Tongji Medical College (2023-S117) and written informed consent was gotten from all the HCC individuals.
Acknowledgments
We thank all the HCC patients in this research.
Funding
This work was supported by Hubei Natural Science Foundation (2021CFB417).
Disclosure
All authors have no conflicts of interest to report for this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
3. Liu X, Lu Y, Zhou W, et al. Chinese multidisciplinary expert consensus on immune checkpoint inhibitor-based combination therapy for hepatocellular carcinoma (2023 edition). Liver Cancer. 2024;13(4):355–375. doi:10.1159/000535496
4. Xie D, Shi J, Zhou J, et al. Clinical practice guidelines and real-life practice in hepatocellular carcinoma: a Chinese perspective. Clin Mol Hepatol. 2023;29(2):206–216. doi:10.3350/cmh.2022.0402
5. Shi Y, Wang Y, Niu K, et al. How CLSPN could demystify its prognostic value and potential molecular mechanism for hepatocellular carcinoma: a crosstalk study. Comput Biol Med. 2024;172:108260. doi:10.1016/j.compbiomed.2024.108260
6. Rossi JF, Lu ZY, Massart C, et al. Dynamic immune/inflammation precision medicine: the good and the bad inflammation in infection and cancer. Front Immunol. 2021;12:595722. doi:10.3389/fimmu.2021.595722
7. Kern L, Mittenbuhler MJ, Vesting AJ, et al. Obesity-induced TNFalpha and IL-6 signaling: the missing link between obesity and inflammation-driven liver and colorectal cancers. Cancers. 2018;11(1):24. doi:10.3390/cancers11010024
8. Luo Y, Lin H. Inflammation initiates a vicious cycle between obesity and nonalcoholic fatty liver disease. Immun Inflamm Dis. 2021;9(1):59–73. doi:10.1002/iid3.391
9. Tian S, Guo Y, Lan Q, et al. Association between ascites Gustave Roussy immune score and the intratumoural microbiome in malignant ascites secondary to hepatocellular carcinoma. Int Immunopharmacol. 2024;133:112097. doi:10.1016/j.intimp.2024.112097
10. Carr BI, Ince V, Bag HG, et al. CRP is a superior and prognostically significant inflammation biomarker for hepatocellular cancer patients treated by liver transplantation. Clin Pract. 2021;18(2):1626–1632.
11. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
12. Feng D, Xiang X, Guan Y, et al. Monocyte-derived macrophages orchestrate multiple cell-type interactions to repair necrotic liver lesions in disease models. J Clin Invest. 2023;133(15). doi:10.1172/JCI166954.
13. Wang HK, Wei Q, Yang YL, et al. Clinical usefulness of the lymphocyte-to-monocyte ratio and aggregate index of systemic inflammation in patients with esophageal cancer: a retrospective cohort study. Cancer Cell Int. 2023;23(1):13. doi:10.1186/s12935-023-02856-3
14. Xie W, Xu Z, Qiu Y, et al. A novel nomogram combined the aggregate index of systemic inflammation and PIRADS score to predict the risk of clinically significant prostate cancer. Biomed Res Int. 2023;2023:9936087. doi:10.1155/2023/9936087
15. Feier C, Muntean C, M FA, et al. An exploratory assessment of pre-treatment inflammatory profiles in gastric cancer patients. Diseases. 2024;12(4):78.
16. Huang G, Xi P, Yao Z, et al. The conditional recurrence-free survival after R0 hepatectomy for locally advanced intrahepatic cholangiocarcinoma: a competing risk analysis based on inflammation-nutritional status. Heliyon. 2024;10(13):e33931. doi:10.1016/j.heliyon.2024.e33931
17. Feier C, Muntean C, Faur AM, et al. Exploring inflammatory parameters in lung cancer patients: a retrospective analysis. J Pers Med. 2024;14(6):552. doi:10.3390/jpm14060552
18. Ma M, Luo M, Liu Q, et al. Influence of abdominal fat distribution and inflammatory status on post-operative prognosis in non-small cell lung cancer patients: a retrospective cohort study. J Cancer Res Clin Oncol. 2024;150(3):111. doi:10.1007/s00432-024-05633-5
19. Ren J, He J, Zhang H, et al. Platelet TLR4-ERK5 axis facilitates NET-mediated capturing of circulating tumor cells and distant metastasis after surgical stress. Cancer Res. 2021;81(9):2373–2385. doi:10.1158/0008-5472.CAN-20-3222
20. Xue R, Zhang Q, Cao Q, et al. Liver tumour immune microenvironment subtypes and neutrophil heterogeneity. Nature. 2022;612(7938):141–147. doi:10.1038/s41586-022-05400-x
21. Zheng C, Zheng L, Yoo JK, et al. Landscape of infiltrating T cells in liver cancer revealed by single-cell sequencing. Cell. 2017;169(7):1342–1356. doi:10.1016/j.cell.2017.05.035
22. Oura K, Morishita A, Tani J, et al. Tumor immune microenvironment and immunosuppressive therapy in hepatocellular carcinoma: a review. Int J Mol Sci. 2021;22(11):5801. doi:10.3390/ijms22115801
23. Jackson DN, Theiss AL. Gut bacteria signaling to mitochondria in intestinal inflammation and cancer. Gut Microbes. 2020;11(3):285–304. doi:10.1080/19490976.2019.1592421
24. Cui Y, Zhang L, Wang X, et al. Roles of intestinal Parabacteroides in human health and diseases. FEMS Microbiol Lett. 2022;369(1). doi:10.1093/femsle/fnac072.
25. Kamo T, Sato K, Sen K, et al. Geranylgeraniol-type diterpenoids, Boletinins A−J, from boletinus c avipes as inhibitors of superoxide anion generation in macrophage cells. J Nat Prod. 2004;67(6):958–963. doi:10.1021/np030535g
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of Predictive Machine Learning Models for Postoperative Recurrence and Microvascular Invasion in Hepatocellular Carcinoma Using Nuclear Magnetic Resonance Metabolomics
Tan H, Xu Y, Liu W, Wen Y, Zhang C, Wang C, Chi L, Liao H, Fu S, Cai L, Guo H, Pan M
Journal of Hepatocellular Carcinoma 2026, 13:589098
Published Date: 13 April 2026