Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Longitudinal Study on Pre- and Post-Operation CT Imaging for Predicting Pedicle Screw Loosening in Patients with Lumbar Degenerative Disease
Authors Zhang Q, Zhao F, Zhang Y, Gong X
Received 15 December 2023
Accepted for publication 8 February 2024
Published 11 March 2024 Volume 2024:20 Pages 185—194
DOI https://doi.org/10.2147/TCRM.S453639
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Qian Zhang,1– 3,* Fanfan Zhao,2,* Yu Zhang,3 Xiangyang Gong1,2
1Medical College of Soochow University, Suzhou, People’s Republic of China; 2Department of Radiology, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital), Hangzhou Medical College, Hangzhou, People’s Republic of China; 3Department of Radiology, The 901st Hospital of the Joint Logistics Support Force of PLA, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangyang Gong, Department of Radiology, Zhejiang Provincial People’s Hospital, (Affiliated People’s Hospital), Hangzhou, People’s Republic of China, Tel/Fax +86 57187666666, Email [email protected]
Purpose: We conducted a longitudinal study to examine the predictive role of risk factors in the occurrence of pedicle screw loosening, assessed through pre- and post-operative computed tomography (CT) scans.
Methods: A total of 103 patients with degenerative lumbar disease who had undergone L4/5 pedicle screw fixation (involving 412 screws) were included in this study. They were subsequently categorized into two groups—the “loosening group” and the “non-loosening group”. The axial and sagittal angles of the screw trajectory in pre- and post-operative CT images were measured, and the deviation angles were computed. Additionally, measurements were taken of the Hounsfield unit (HU) within the screw entry point area, the pedicle, and the vertebral body in preoperative CT images. Logistic regression analysis was employed to ascertain the risk factors influencing the occurrence of screw loosening.
Results: Elderly patients who experienced screw loosening tended to have bilateral screw issues at the L5 level (p < 0.005). The HU of the pedicle (p < 0.001), age (p < 0.001), and the axial deviation angle (p = 0.014) were identified as independent factors predicting screw loosening. Additionally, when HU of the pedicle < 126.5 or age ≥ 53.5 years, the axial deviation angle was found to be smaller in the group experiencing screw loosening (p = 0.018 and p = 0.019).
Conclusion: Loosening of screws positioned at L5 was found to be more prevalent in elderly patients, particularly exhibiting a bilateral occurrence. Independent predictors of this phenomenon included a low HU value in the pedicle, advanced age in patients, and a substantial axial deviation angle. In the case of elderly patients with a low HU value in the pedicle, a reduced axial surgical deflection was necessitated to prevent the occurrence of screw loosening.
Keywords: computed tomography, lumbar degenerative diseases, Hounsfield unit, pedicle screw loosening, position deviation value
Background
In the field of spinal surgery, the application of pedicle screw fixation is widely acknowledged and employed for diverse clinical indications.1,2 One of the most frequently encountered late complications in this context is pedicle screw loosening, which can potentially lead to a substantial compromise in the surgical outcome or necessitate a reoperation.3,4 Therefore, the early-stage prediction of screw loosening following pedicle screw fixation is deemed crucial.
In the lower lumbar spine, screw loosening incidence was observed across a wide spectrum, spanning from 1% to 60%, with a heightened occurrence of screw loosening.5–8 The field of spinal surgery is witnessing an increasing incidence of patients with degenerative diseases, particularly within an aging demographic. Predominantly, the insertion of screws in the lower lumbar region has been the prevailing practice in spinal fusion procedures.9 In this study, we excluded the impact of confounding variables while focusing on the evaluation of patients subjected to L4–5 instrumentation due to degenerative ailments, with the intention of ascertaining the independent risk factors responsible for predicting screw loosening and examining their interplay.
In previous investigations, it has been demonstrated that the impact of screw loosening is influenced by surgical techniques.10 In this study, a longitudinal examination was undertaken to assess the condition of screws both prior to and following surgery over an extended duration. The factors evaluated in this study encompassed the values representing positional deviations between the optimal preoperative screw trajectory and the postoperative screw parameters, as ascertained through pre- and post-operative computed tomography (CT) scans. This approach was employed to account for the distinctive variations in vertebral body morphology among individual patients and the morphological distinctions among different vertebral bodies to the greatest possible extent. Inclusion in this study necessitated the collection of comprehensive preoperative and postoperative CT images for each patient, along with a minimum of 12 months’ worth of follow-up CT images.
The protracted duration of the follow-up and the requisite completeness of CT image data collection posed challenges in terms of case acquisition and the completion of the longitudinal investigation. Consequently, there was a scarcity of similar studies in the past, although longitudinal studies offer superior means to compare, observe, and analyze the influential factors evident in CT images. The objective of this study is to investigate the risk factors, predicated on pre- and post-operative CT scans, for the prediction of screw loosening in the L4-5 region in patients afflicted with lumbar degenerative disease.
Materials and Methods
Patients
In this longitudinal study, we enrolled patients who had undergone pedicle screw fixation during surgery for lumbar degenerative disease at a single medical center from January 2017 to December 2022. Approval for this study was obtained from the Ethical Committee of our hospital who waived the need for informed consent as only routinely collected clinical data were recorded. The inclusion criteria were as follows: 1) both posterolateral lumbar fusion (PLF) and posterior lumbar interbody fusion (PLIF) procedures were performed on participants with lumbar degenerative disease by the same surgical team; 2) complete preoperative CT images were available for all individuals; and 3) the instrumented vertebrae comprised L4-5, and the fusion with fixation spanned two levels. Exclusion criteria: 1) patients who have undergone lumbar spine surgery; 2) patients with rheumatoid arthritis; 3) patients who used steroids or with osteoporosis; 4) patients who used bone cement during surgery; 5) newly diagnosed tumor patients during follow-up or death during follow-up; 6) patients with recurrent lumbar spine trauma during follow-up period; 7) patients who undergo secondary surgery due to poor efficacy or complications; 8) patients who only received regular X-ray follow-up after the first postoperative CT follow-up; 9) missing visitors. In the end, only 103 patients completed 2 follow-up visits, with a follow-up period of at least 12 months and a maximum of 54 months. They also obtained complete postoperative CT images.
Surgery was performed on all participants by the same surgical team, and complete preoperative and two postoperative follow-up CT images were obtained. All patients were subsequently monitored at our hospital, and their characteristics, such as sex, age, height, weight, body mass index (BMI, kg/m2), diagnosis, and other underlying clinic diseases (diabetes, hypertension), were recorded.
Radiographic Evaluations
Screw loosening was identified as a radiolucent area (≥ 1 mm) surrounding the screw on postoperative CT scans (Figure 1a).11–13 In accordance with this criterion, patients who demonstrated any screw loosening at the L4 or the L5 level during a minimum 12-month follow-up period were categorized as belonging to the loosening group, whereas the remaining patients were classified into the non-loosening group. Based on the same criteria, the 412 screws involved were divided into two groups, specifically, the screw loosening group and the screw non-loosening group. Evaluation of screw loosening was performed by two radiologists with 5 years of experience in imaging diagnosis, and in cases of any interpretational ambiguity, the corresponding author rendered the final decision.
 |
Figure 1 (a) Typical postoperative CT axial image of screw loosening. A radiolucent area encircling pedicle screws with sclerotic bone perimeter indicating screw loosening (white arrow) (b) Techniques for assessing preoperative CT HU The axial image of the corresponding pedicle was used to measure the HU of screw entry point area (ROI 1), pedicle (ROI 2) and vertebral body (ROI 3) excluding cortical bone. (c) The axial angle of the optimal screw trajectory in the preoperative CT (pre-e), namely angle between pedicle and sagittal plane of vertebral body. (d) The axial angle of the screw in postoperative CT (post-e), d is the distance between the screw tip and the anterior edge of the vertebral body (rad point). (e) The sagittal angle of the optimal screw trajectory in the preoperative CT (pre-f). (f) The sagittal angle of screw in postoperative CT (post-f). Reconstruction of the sagittal position along the screw, and measurement of the intraosseous length (l). |
According to the preoperative CT scans of the lumbar spine in both the coronal and sagittal planes, axial images depicting bilateral pedicles passing through their respective median planes were reconstructed. The measurement of Hounsfield units (HU) was conducted by creating three oval regions of interest (ROIs) on this axial CT image. These three ROIs encompassed the following areas: the region corresponding to the screw entry point (ROI 1), the pedicle (ROI 2), and the vertebral body (ROI 3), with exclusion of cortical bone (Figure 1b).
The axial angle (e) and sagittal angle (f) were measured in preoperative CT images of the L4 and L5, and these measurements were denoted as pre-e and pre-f, respectively, given that the optimal screw trajectory had been determined by the surgical team. Similarly, the measurements of e and f for the actual screw in postoperative CT (conducted within two weeks after the operation) were designated as post-e and post-f. Furthermore, the distance between the screw tip and the anterior edge of the vertebral body was labeled as d (with a value of 0 if the screw reached or exceeded the vertebral margin), and the diameter and intraosseous length (l) were determined through sagittal CT along the screw (Figure 1c–f). The difference between the e angle and f angle, measured both before and after the operation, was calculated.
In the assessment of screw loosening and the measurement of all parameters, two independent radiologists conducted preoperative and postoperative CT scans (utilizing the SOMATOM Definition scanner by SIEMENS). HU and screw-related parameters were measured thrice per participant to derive an average value, and subsequently, the mean value for analysis was computed from the measurements conducted by the two radiologists.
Statistical Analysis
In the execution of all statistical analyses, the software SPSS v.21.0 (IBM Corp., Armonk, NY, USA) was employed. The variables were compared between groups through the utilization of Fisher’s exact test and independent t-test. Assessment of intra-observer and inter-observer reliability was conducted by employing Kappa coefficients and the interobserver intraclass correlation coefficients (ICC).
In order to identify predictors of L4-5 screw loosening, a multivariate logistic regression analysis with forward stepwise selection was executed, encompassing variables with p-values < 0.20 from the univariate analysis. The assessment of cut-off values was conducted through receiver operating characteristic (ROC) curve analyses. A p-value < 0.05 was employed to establish statistical significance.
Results
Reproducibility Evaluation
To evaluate the reliability of intra-observer and inter-observer assessments, a random sample of 60 out of the 412 screws was chosen. The assessment of screw loosening was conducted on postoperative follow-up CT images by two radiologists, both possessing over five years of experience in imaging diagnosis. Each screw was assessed and measured by both radiologists in duplicate, with a 2-week time gap. The Kappa test was employed to gauge the consistency in assessing screw loosening. The interobserver reliability demonstrated excellence between the two radiologists, as indicated by a Kappa value of 0.857 (p < 0.05). Reproducibility evaluations of HU and screw-related parameters were executed using the ICC for both intra-observer and inter-observer measurements (averaged across two assessments by each observer). The reliabilities observed in these evaluations were found to be acceptable (Table 1).
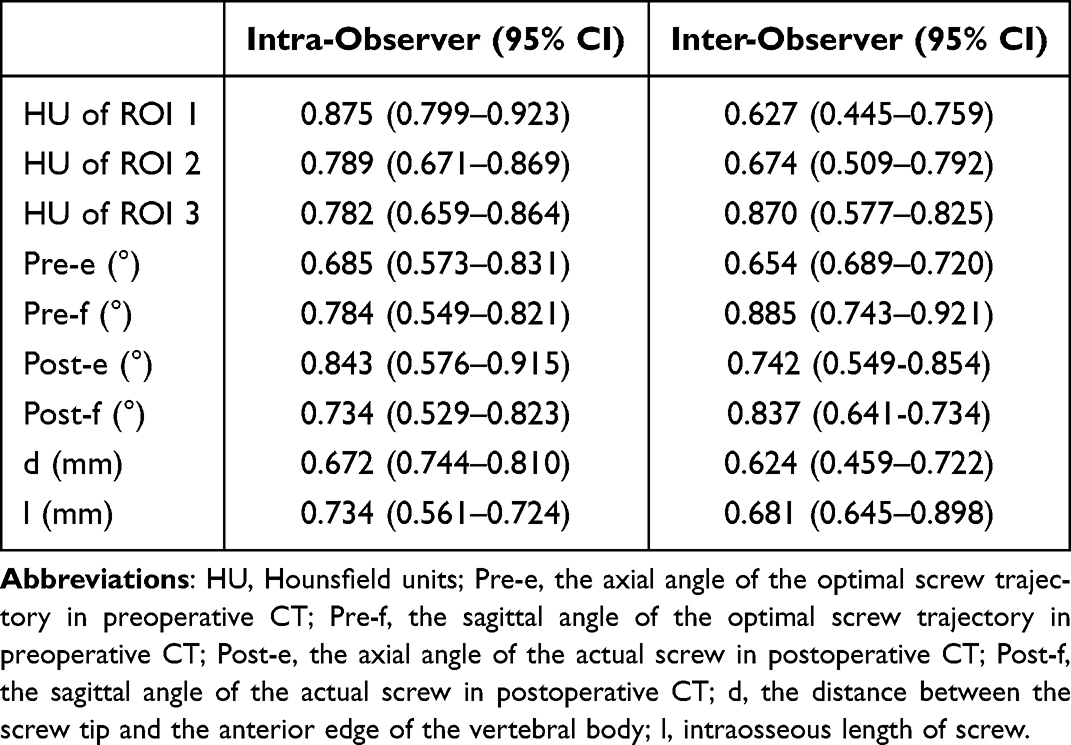 |
Table 1 ICC for Intra-Observer and Inter-Observer Reliability |
Patient Characteristics and Screw Position
The loosening rate of L4-5 instrumentation was found to be 30.1% (31/103). Significantly higher age was observed in the patients in the loosening group when compared to the non-loosening group (p = 0.004); however, no significant differences in other characteristics were discerned between the two groups (Table 2). In the case of all screws, the overall loosening rate was 13.35% (55/412). A notably higher loosening rate was observed for L5 and bilateral screws in comparison to the non-loosening screw group (p = 0.030 and p < 0.001), while no significant distinctions were detected between left and right (Table 3).
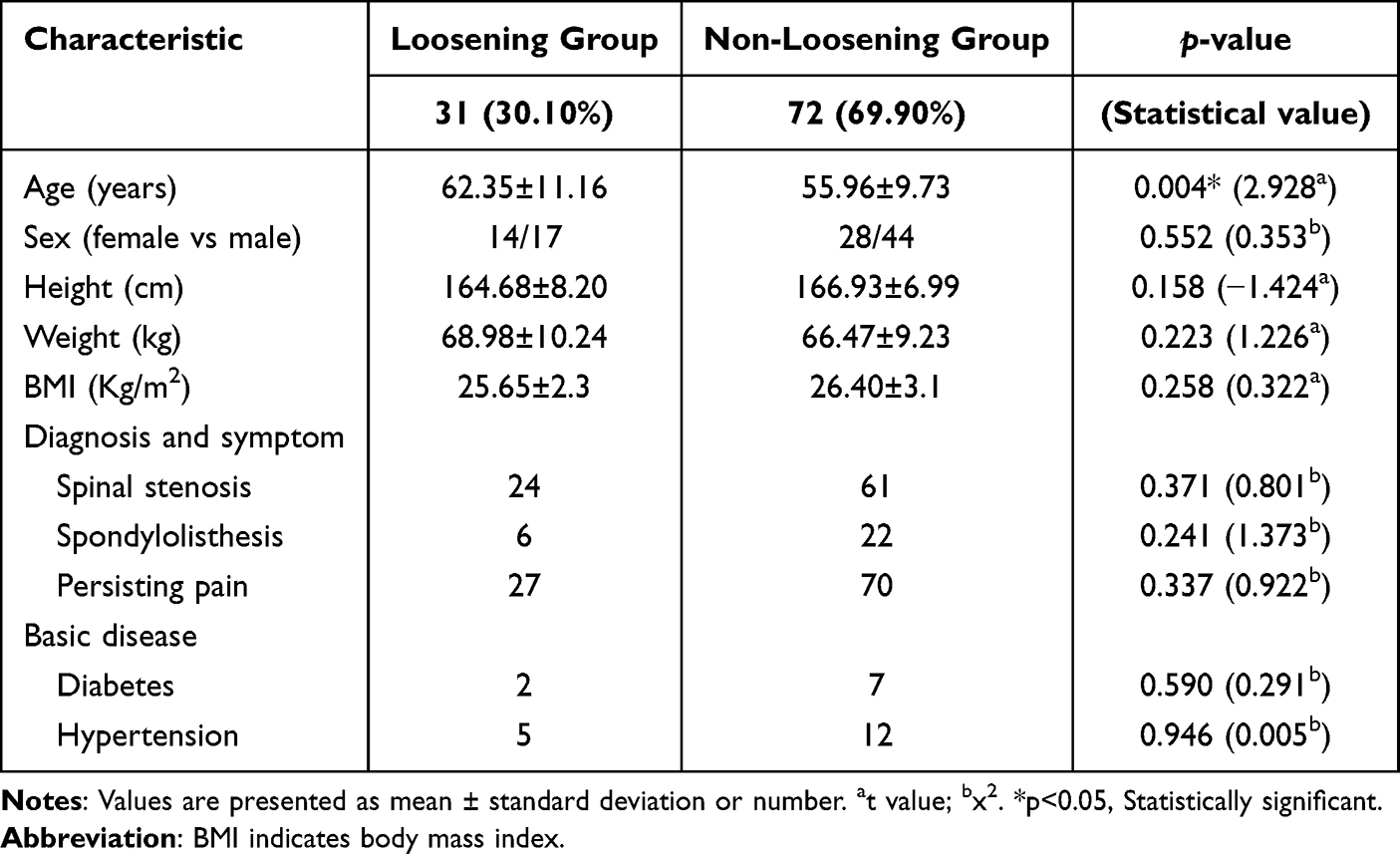 |
Table 2 Patients’ Characteristics |
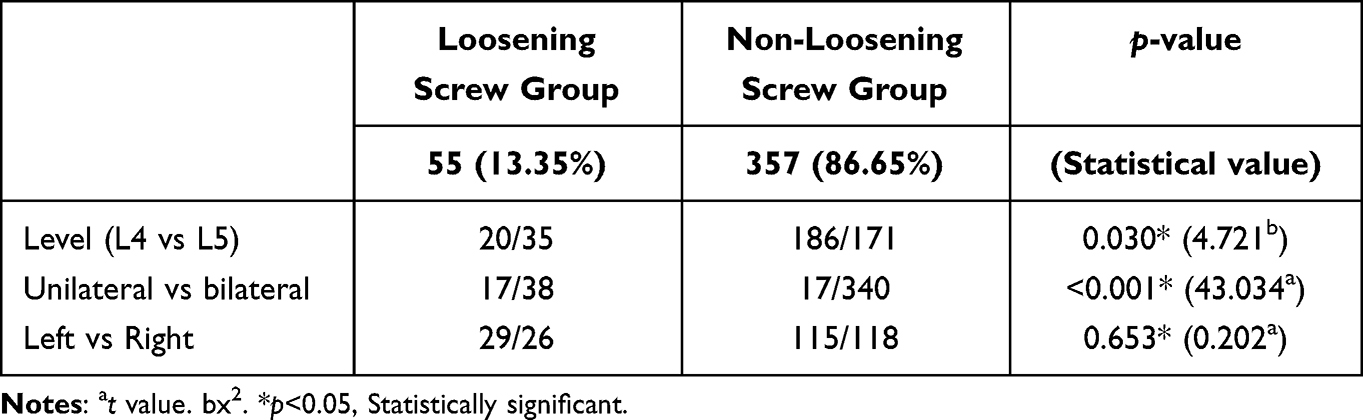 |
Table 3 Screw Position Between the Loosening Screw Group and Non-Loosening Screw Group |
Univariate and Multivariate Analysis of Screw Loosening
Significant differences were observed in terms of age, HU of ROI 2, and deviation angle-e between the loosening screw group and the non-loosening group. However, sex, height, weight, BMI, deviation angle-f, d, l, and HU of ROI1 and ROI3 were not found to be significantly different between the two groups. It was noted that the loosening screw group exhibited lower HU of the pedicle (p = 0.001), a smaller deviation angle-e, and an older age (p < 0.001) compared to the non-loosening group (Table 4).
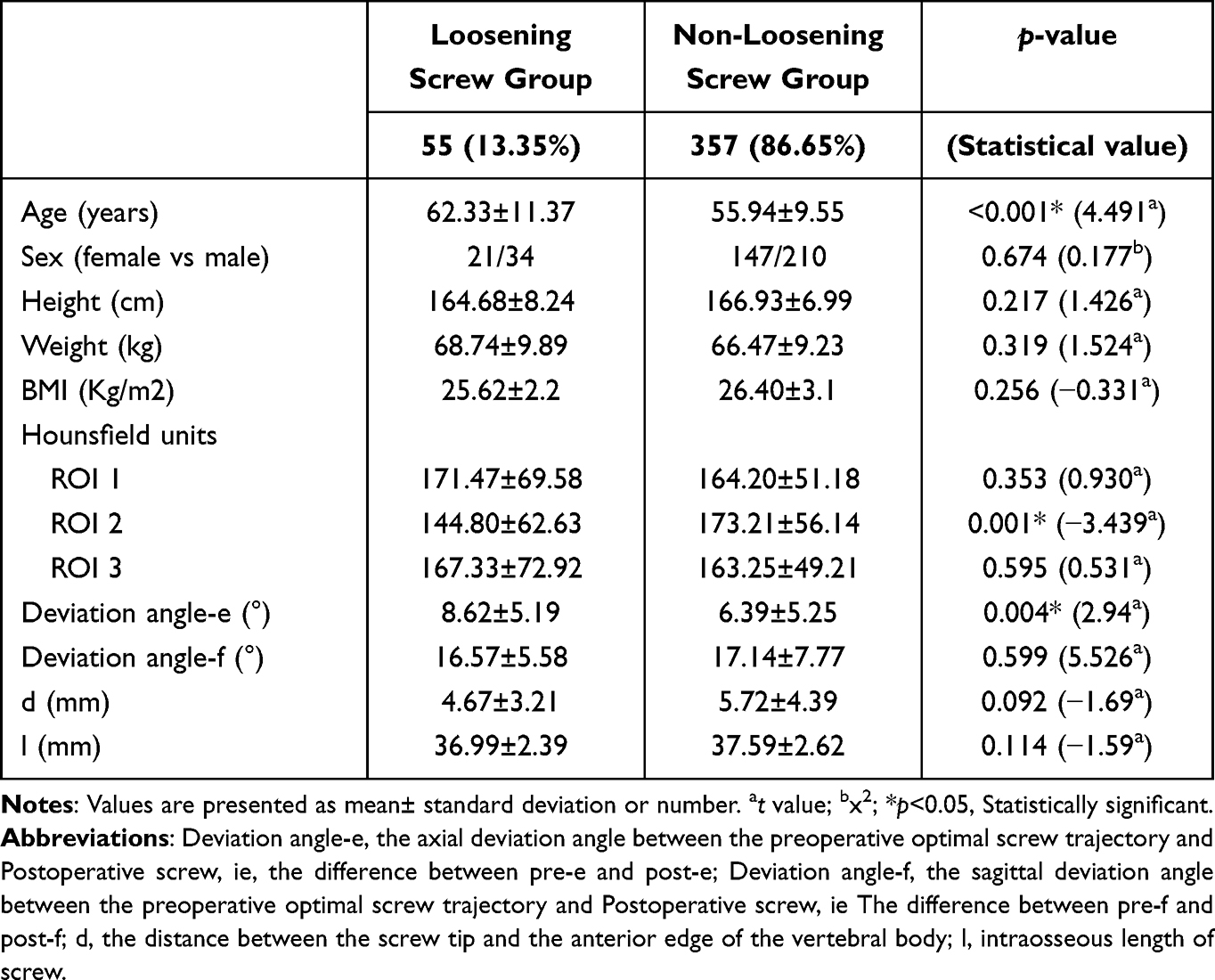 |
Table 4 Univariate Analysis of Screw Loosening |
Nevertheless, in the multivariate analysis involving the aforementioned three predictors (age, HU of ROI 2, deviation angle-e) and two potential predictors (d, with a p-value of 0.092, and l, with a p-value of 0.114), it was revealed that deviation angle-e, age, and HU of ROI 2 were identified as the significant independent risk factors (Table 5).
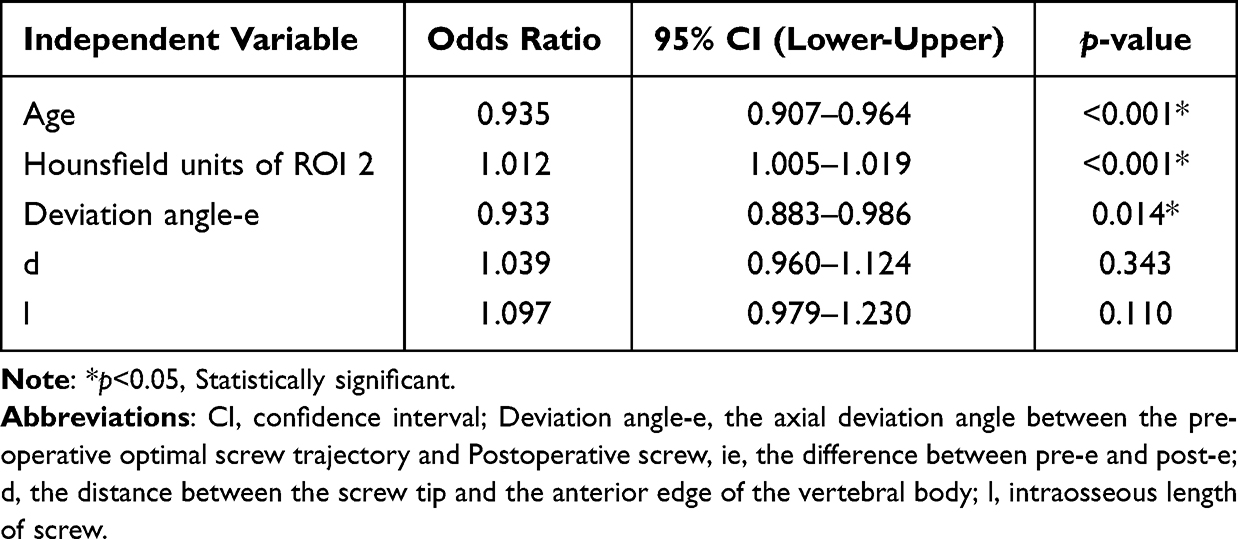 |
Table 5 Multivariate Logistic Regression Analysis of Risk Factors for Screw Loosening |
Relationship Among Pre-Postoperative Independent Risk Factors
In the analysis of independent risk factors, it was found that HU of ROI 2 and age served as predictors before the surgical procedure, while deviation angle-e emerged as the predictor following the operation. ROC curve analyses were carried out for both HU of ROI 2 and age, as these two factors had been identified as predictors prior to surgery in the multivariate analysis. The AUC values for age and HU of ROI 2 with respect to screw loosening were 0.762 (95% CI 0.643–0.809; p < 0.001) and 0.684 (95% CI 0.608–0.760; p < 0.001), respectively. Cut-off values of 126.5 and 53.5 years, respectively, were determined according to the Youden’s index (Figure 2).
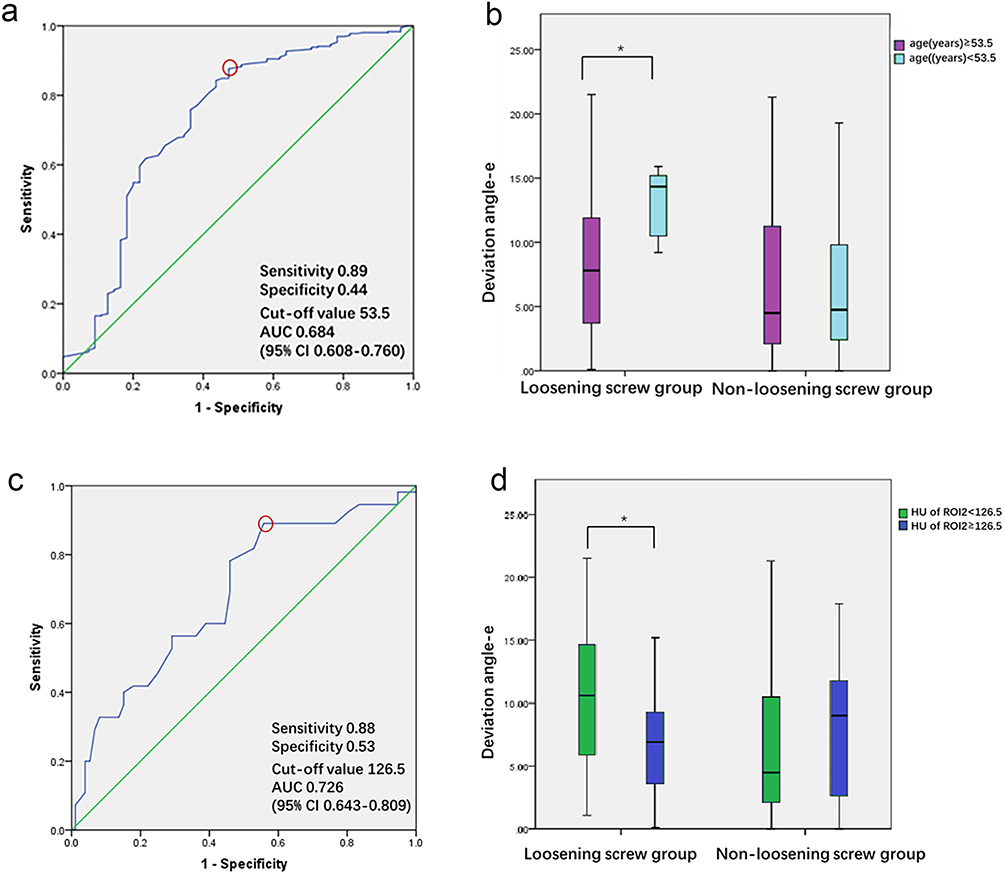 |
Figure 2 Receiver operating characteristic curve for screw loosening due to age (a) and HU of ROI2 (b). Cutoff values determined by the Youden’s index (red circles), and the age and HU of ROI2 were divided according to the threshold, box diagram of the lower age group and slightly higher age group (c) and the lower HU and slightly higher HU group (d) were obtained. In the loosening screw group, the corresponding deviation angle-e was smaller in the lower HU group and slightly higher age group; *Marks significant differences. |
In accordance with the cut-off value for HU within ROI 2, the screws were categorized into two groups, namely the lower HU group and the slightly higher HU group of pedicles. Utilizing the same methodology, the screws were segregated into groups based on the cut-off age value, distinguishing between lower and higher age groups. It was observed that there existed a statistically significant difference between the lower HU group and the higher HU group of pedicles within the screw loosening cohort, while such a difference was not evident in the non-loosening screw group.
Similarly, a statistically significant difference was noted between the lower and higher age groups in the screw loosening group, but not within the non-loosening screw group (Table 6). Within the screw loosening group, the corresponding deviation angle-e was found to be smaller in both the lower HU and higher age groups (Figure 2).
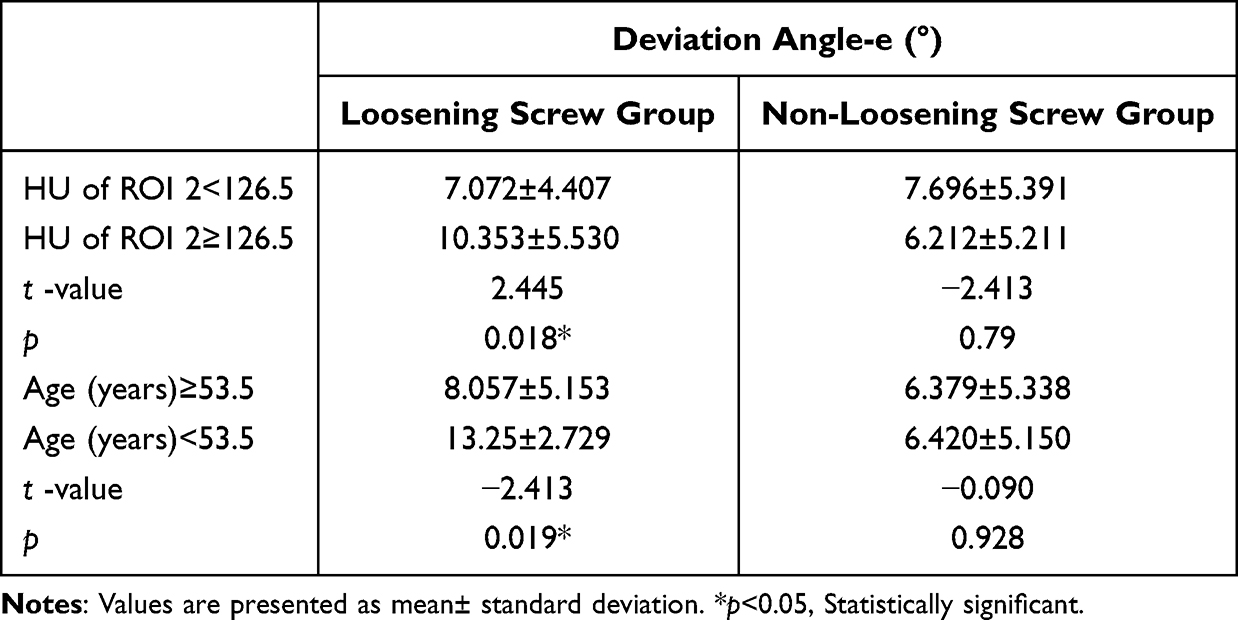 |
Table 6 Relationship Between Risk Factors |
Discussion
The results of this study revealed that screw loosening was observed in patients of advanced age, with a predominant occurrence of loosened screws in the L5 region. Bilateral screw loosening was notably more prevalent than unilateral loosening. By means of multivariate analysis, it was ascertained that the HU value of the pedicle and patient age served as preoperative independent risk factors, while the deviation angle-e represented a postoperative independent risk factor in predicting screw loosening. Through an examination of the interrelationship between preoperative and postoperative independent risk factors via ROC curve analysis and box plots, it was observed that when the HU of the pedicle fell below 126.5 and patient age exceeded 53.5 years, a lesser axial surgical deviation angle could induce screw loosening. This underscores the imperative need for enhanced surgical screw precision among patients with lower HU values in their pedicles and those aged over 53.5 years. In prior research, the primary focus had been either directed towards the entirety of the vertebrae, encompassing the sacrum, or the inclusion criteria were characterized by a broad scope, involving aspects like multi-level fixation or diverse surgical rationales, which frequently led to substantial hindrances in the identification of independent risk factors contributing to screw loosening. For instance, the sacral bone exhibits significant disparities in terms of morphology and bone mass when compared to the lumbar vertebrae. Consequently, the prevalence of screw loosening is noticeably elevated.14,15 Moreover, patients with fracture experience a substantial deterioration in spinal stability, and multi-level fixation also exerts an influence on the mobility of vertebral bodies, resulting in an escalated rate of screw loosening.16 Therefore, the inclusion criteria in this study encompass patients who have undergone internal fixation surgery at the L4-5 level due to degenerative changes. The innovations of this paper, in comparison to prior studies, are characterized by several distinctive features. Firstly, the inclusion of postoperative influencing factors has been predicated upon the utilization of the individual screw as the primary research subject, as opposed to patients. Moreover, it is worth noting that this study stands as the first such study to unveil the risk factors for screw loosening, specifically by disclosing the deviation values between the optimal preoperative screw trajectory and the actual postoperative screw position, as well as establishing the associative relationships among independent risk factors before and after the operation. Notably, while Matsukawa et al,10 exclusively assessed postoperative screw deflection angles and screw lengths following surgery, in our study, we adopted a longitudinal approach, focusing on the disparity between the optimal preoperative screw trajectory and postoperative screw parameters. This approach takes into account the distinctive vertebral body morphology of each patient and inter-patient variations, rendering the factors influencing screw positioning more objective. Thirdly, we utilized long-term CT follow-up, spanning at least 12 months, in order to enhance the precision of screw loosening assessment. Ultimately, the results of our study revealed that the sole independent postoperative predictor of screw loosening is the discrepancy between the optimal preoperative screw trajectory and the horizontal deflection angle of the postoperative screw (deviation angle-e). Osteoporosis has been frequently deliberated upon as a factor with preoperative influence.17,18 Recent studies have focused on the utilization of the HU value for the identification of spinal osteoporosis in patients afflicted with lumbar degenerative diseases. Nevertheless, there was divergence in the selection of measurement areas for CT values.18–21 In the study conducted by Sakai et al,18 the entire segment of screw placement was employed as the ROI to compute the average value, while other studies, including those by Zou et al,19 and Zhou et al,20 opted for the vertebral body area as the ROI for HU value measurement. However, only a limited number of scholars have shed light on the impact of HU values in distinct regions on screw loosening, rendering it an imprecise predictive metric.
Consequently, to enhance the accuracy in depicting the influence of HU values in varying regions concerning screw positions on screw loosening across diverse segments of the vertebral body, three distinct regions of interest were chosen in the preoperative CT images. Subsequently, it was ascertained that the HU values in the pedicle region constituted an independent preoperative predictor for screw loosening. Our investigation aligns with the findings of Matsukawa,22 underscoring that the pull-out strength is primarily determined by the lumbar pedicle as opposed to the vertebral body. It is common knowledge that the utilization of cortical bone trajectory screws and bone cement in lumbar surgery for patients without osteoporosis does not yield conspicuous advantages.23,24 As such, our results can serve as valuable reference points for making informed decisions regarding clinical treatments and surgical approaches.
Some limitations are inherent in this study. Firstly, the relevance between screw loosening and radiolucent zones in the lumbar region on X-rays has been questioned by some scholars, despite the confirmation of screw loosening through radiolucent areas in numerous studies.25,26 This controversy was also addressed in our study, and thus, we opted for the selection of CT image evaluation over X-ray as a means to obtain further supporting evidence. Recently, scholars have begun to study the use of T1 weighted lumbar magnetic resonance imaging based on vertebral bone quality (VBQ) score to evaluate bone quality.27,28 Although reports have shown that this technique is more accurate than CT value evaluation, considering the limited number of patients undergoing magnetic resonance follow-up, this technique has not been introduced for factor assessment of bone quality. Secondly, we only conducted two CT follow-up visits after surgery to measure and observe the screws, and the duration of the two follow-up visits was relatively wide. There was a lack of dynamic measurement during the follow-up period, which failed to reveal the changes in screw parameters before screw loosening. We only studied predictive factors and were unable to further analyze the impact of these factors on the occurrence time of screw loosening. Thirdly, when discussing screw loosening, we did not further explore the mutual influence between each screw in the same patient.
Conclusion
The findings of this study revealed that older patients were more likely to experience screw loosening, with the majority of these loosened screws being located in the L5 region rather than L4. Additionally, bilateral screw loosening was significantly more common than unilateral loosening. Through a multivariate analysis, it can be inferred that the HU of the pedicle and age serve as preoperative risk factors, while the postoperative deviation angle-e is an independent risk factor for predicting screw loosening. Independent predictors of screw loosening include a low HU of the pedicle, advanced age, and a large axial deviation angle. For elderly patients with a low HU of the pedicle, it is advisable to use a smaller axial surgical deflection to prevent screw loosening.
Abbreviations
CT, computed tomography; HU, Hounsfield unit; PLF, posterolateral lumbar fusion; PLIF, posterior lumbar interbody fusion; ROC, receiver operating characteristic; ICC, intraclass correlation coefficient; ROI, regions of interest.
Ethical Statement
This study was conducted with approval from the Ethics Committee of Zhejiang Provincial People’s Hospital. [No. QT2023309] This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
This work was funded by Key Research and Development Project of Zhejiang Province of China (No.2020C01058).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Knezevic NN, Candido KD, Vlaeyen JWS, et al. Low back pain. Lancet. 2021;398(10294):78–92. doi:10.1016/S0140-6736(21)00733-9
2. Varghese V, Saravana Kumar G, Krishnan V. Effect of various factors on pull out strength of pedicle screw in normal and osteoporotic cancellous bone models. Med Eng Phys. 2017;40:28–38. doi:10.1016/j.medengphy.2016.11.012
3. Rometsch E, Spruit M, Zigler JE, et al. Screw-related complications after instrumentation of the osteoporotic spine: a systematic literature review with meta-analysis. Global Spine J. 2020;10(1):69–88. doi:10.1177/2192568218818164
4. Banno T, Hasegawa T, Yamato Y, et al. The incidence of iliac screw-related complications after long fusion surgery in patients with adult spinal deformity. Spine. 2022;47(7):539–547. doi:10.1097/BRS.0000000000004276
5. Xie Y, Ma H, Li H, et al. Comparative study of unilateral and bilateral pedicle screw fixation in posterior lumbar interbody fusion. Orthopedics. 2012;35(10):e1517–e1523. doi:10.3928/01477447-20120919-22
6. Uehara M, Takahashi J, Ikegami S, et al. Pedicle screw loosening after posterior spinal fusion for adolescent idiopathic scoliosis in upper and lower instrumented vertebrae having major perforation. Spine. 2017;42(24):1895–1900. doi:10.1097/BRS.0000000000002305
7. Bredow J, Boese CK, Werner CM, et al. Predictive validity of preoperative CT scans and the risk of pedicle screw loosening in spinal surgery. Arch Orthop Trauma Surg. 2016;136(8):1063–1067. doi:10.1007/s00402-016-2487-8
8. Galbusera F, Volkheimer D, Reitmaier S, et al. Pedicle screw loosening: a clinically relevant complication? Eur Spine J. 2015;24(5):1005–1016. doi:10.1007/s00586-015-3768-6
9. Shin HK, Koo HW, Kim KH, et al. The usefulness of trabecular CT attenuation measurement at L4 level to predict screw loosening after degenerative lumbar fusion surgery: consider number of fused levels and postoperative sagittal balance. Spine. 2022;47(10):745–753. doi:10.1097/BRS.0000000000004330
10. Matsukawa K, Yato Y, Hynes RA, et al. Comparison of pedicle screw fixation strength among different transpedicular trajectories: a finite element study. Clin Spine Surg. 2017;30(7):301–307. doi:10.1097/BSD.0000000000000258
11. Spirig JM, Sutter R, Götschi T, et al. Value of standard radiographs, computed tomography, and magnetic resonance imaging of the lumbar spine in detection of intraoperatively confirmed pedicle screw loosening-a prospective clinical trial. Spine J. 2019;19(3):461–468. doi:10.1016/j.spinee.2018.06.345
12. Zou D, Muheremu A, Sun Z, et al. Computed tomography Hounsfield unit-based prediction of pedicle screw loosening after surgery for degenerative lumbar spine disease. J Neurosurg Spine. 2020;32(5):716–721. doi:10.3171/2019.11.SPINE19868
13. Sandén B, Olerud C, Petrén-Mallmin M, et al. The significance of radiolucent zones surrounding pedicle screws. Definition of screw loosening in spinal instrumentation. J Bone Joint Surg Br. 2004;86(3):457–461. doi:10.1302/0301-620x.86b3.14323
14. Iijima Y, Kotani T, Sakuma T, et al. Risk factors for loosening of S2 alar iliac screw: surgical outcomes of adult spinal deformity. Asian Spine J. 2020;14(6):864–871. doi:10.31616/asj.2020.0100
15. Kim JB, Park SW, Lee YS, et al. The effects of spinopelvic parameters and paraspinal muscle degeneration on S1 screw loosening. J Korean Neurosurg Soc. 2015;58(4):357–362. doi:10.3340/jkns.2015.58.4.357
16. Chen CH, Chen DC, Huang HM, et al. Level-based analysis of screw loosening with cortical bone trajectory screws in patients with lumbar degenerative disease. Medicine. 2020;99(40):e22186. doi:10.1097/MD.0000000000022186
17. Fasser MR, Gerber G, Passaplan C, et al. Computational model predicts risk of spinal screw loosening in patients. Eur Spine J. 2022;31(10):2639–2649. doi:10.1007/s00586-022-07187-x
18. Sakai Y, Takenaka S, Matsuo Y, et al. Hounsfield unit of screw trajectory as a predictor of pedicle screw loosening after single level lumbar interbody fusion. J Orthop Sci. 2018;23(5):734–738. doi:10.1016/j.jos.2018.04.006
19. Zou D, Li W, Xu F, et al. Use of Hounsfield units of S1 body to diagnose osteoporosis in patients with lumbar degenerative diseases. Neurosurg Focus. 2019;46(5):E6. doi:10.3171/2019.2.FOCUS18614
20. Zhou J, Yuan C, Liu C, et al. Hounsfield unit value on CT as a predictor of cage subsidence following stand-alone oblique lumbar interbody fusion for the treatment of degenerative lumbar diseases. BMC Musculoskelet Disord. 2021;22(1):960. doi:10.1186/s12891-021-04833-1
21. Kim KH, Kim TH, Kim SW, et al. Significance of measuring lumbar spine 3-dimensional computed tomography Hounsfield units to predict screw loosening. World Neurosurg. 2022;165:e555–e562. doi:10.1016/j.wneu.2022.06.104
22. Matsukawa K, Yato Y, Imabayashi H, et al. Biomechanical evaluation of lumbar pedicle screws in spondylolytic vertebrae: comparison of fixation strength between the traditional trajectory and a cortical bone trajectory. J Neurosurg Spine. 2016;24(6):910–915. doi:10.3171/2015.11.SPINE15926
23. Kanno H, Aizawa T, Hashimoto K, et al. Novel augmentation technique of percutaneous pedicle screw fixation using hydroxyapatite granules in the osteoporotic lumbar spine: a cadaveric biomechanical analysis. Eur Spine J. 2021;30(1):71–78. doi:10.1007/s00586-020-06451-2
24. Delgado-Fernandez J, García-Pallero MÁ, Blasco G, Pulido-Rivas P, Sola RG. Review of cortical bone trajectory: evidence of a new technique. Asian Spine J. 2017;11(5):817–831. doi:10.4184/asj.2017.11.5.817
25. Kim HJ, Kim SG, Lee HM, et al. Risk factors associated with the halo phenomenon after lumbar fusion surgery and its clinical significance. Asian Spine J. 2008;2(1):22–26. doi:10.4184/asj.2008.2.1.22
26. Tokuhashi Y, Matsuzaki H, Oda H, Uei H. Clinical course and significance of the clear zone around the pedicle screws in the lumbar degenerative disease. Spine. 2008;33(8):903–908. doi:10.1097/BRS.0b013e31816b1eff
27. Ehresman J, Pennington Z, Schilling A, et al. Novel MRI-based score for assessment of bone density in operative spine patients. Spine J. 2020;20:556–562.
28. Ehresman J, Schilling A, Yang X, et al. Vertebral bone quality score predicts fragility fractures independently of bone mineral density. Spine J. 2021;21:20–27.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.