Back to Journals » Clinical Epidemiology » Volume 11
Longer distance to specialized treatment centers does not adversely affect treatment intensity or outcomes in adult acute myeloid leukemia patients. A Danish national population-based cohort study
Authors Tøstesen M ![]() , Nørgaard M
, Nørgaard M ![]() , Nørgaard JM
, Nørgaard JM ![]() , Medeiros BC, Marcher CW, Overgaard UM, Severinsen MT
, Medeiros BC, Marcher CW, Overgaard UM, Severinsen MT ![]() , Schoellkopf C, Østgård LSG
, Schoellkopf C, Østgård LSG ![]()
Received 29 March 2019
Accepted for publication 10 July 2019
Published 28 August 2019 Volume 2019:11 Pages 769—780
DOI https://doi.org/10.2147/CLEP.S210456
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Henrik Toft Sørensen
Michael Tøstesen,1 Mette Nørgaard,2 Jan Maxwell Nørgaard,3 Bruno C Medeiros,4 Claus Werenberg Marcher,5 Ulrik Malthe Overgaard,6 Marianne Tang Severinsen,7 Claudia Schoellkopf,8 Lene Sofie Granfeldt Østgård1–3
1Department of Clinical Medicine, Holstebro Regional Hospital, Aarhus, Denmark; 2Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 3Department of Hematology, Aarhus University Hospital, Aarhus, Denmark; 4Department of Hematology, Stanford University, School of Medicine, Stanford, CA, USA; 5Department of Hematology, Odense University Hospital, Odense, Denmark; 6Department of Hematology, University Hospital Rigshospitalet, Copenhagen, Denmark; 7Department of Hematology, Aalborg University Hospital, Aalborg, Denmark; 8Department of Hematology, Herlev University Hospital, Herlev, Denmark
Correspondence: Lene Sofie Granfeldt Østgård
Department of Hematology, Aarhus University Hospital, Palle Juul-Jensens Boulevard 99, 8200 Aarhus N, Denmark
Tel +45 2 972 8127
Email [email protected]
Background: Treatment of acute myeloid leukemia (AML) is widely centralized. Longer distances to a specialized treatment center may affect patients’ access to curative-intended treatment. Especially during outpatient treatment, distance may also affect survival.
Methods and patients: The authors conducted a national population-based cohort study including all AML patients diagnosed in Denmark between 2000 and 2014. We investigated effects of distance (<10 kilometers [km; reference], 10–25, 25–50, 50–100, >100) to the nearest specialized treatment facility on the probability of receiving intensive chemotherapy, HSCT, and achieving a complete remission (CR) using logistic regression analysis (odds ratios; ORs). For overall survival, we used Cox proportional hazards regression (hazard ratios [HRs]) and adjusted (a) for relevant baseline characteristics.
Results: Of 2,992 patients (median age=68.5 years), 53% received intensive chemotherapy and 12% received low-dose chemotherapy outpatient regimens. The median distance to a specialized treatment center was 40 km (interquartile range=10–77 km). No impact of distance to specialized treatment centers was seen on the probability of receiving intensive chemotherapy (10–25 km, aOR=1.1 (CI=0.7–1.7), 25–50 km, aOR=1.1 (CI=0.7–1.7), 50–100 km, aOR=1.3 (CI=0.9–1.9), and >100 km, aOR=1.4 [CI=0.9–2.2]). Overall survival in patients regardless of therapy (<10 km, aOR=1.0 vs >100 km, aOR=1.0 [CI=0.9–1.2]), in intensive therapy patients, or in patients’ choice of post-remission was not affected by distance to specialized treatment center. Distance to a transplant center also did not affect the probability of HSCT or survival post-HSCT.
Conclusion: In Denmark, distance to a specialized treatment facility offering remission-induction chemotherapy and HSCT does not negatively affect access to curative-indented therapy, treatment-response, or survival in AML patients.
Keywords: hematology, allogeneic transplantation, socioeconomics, prognosis, epidemiology
Introduction
Acute myeloid leukemia (AML) is the most common form of acute leukemia in adults. Treatment strategies range from supportive care, over low-dose chemotherapy to high-dose intensive combination chemotherapy, potentially followed by allogeneic stem cell transplantation (HSCT).1 Given the low incidence of only 5,4/100.000 persons-years,2 the disease heterogeneity,3 broad spectrum of patients,4,5 therapeutic modalities, and treatment-related complications, treatment often requires referral to a specialized center. Several studies have shown that patients referred to high-volume centers and academic institutions have fewer treatment-related complications and better long-term outcomes for surgically treated cancers and also hematological cancers than patients treated at low-volume and non-academic centers.6–8
To improve clinical decision-making and outcome, treatment and care of AML patients especially intended for remission-induction therapy and HSCT has, therefore, in Denmark, been centralized at university hospitals.9,10 However, centralized treatment at specialized centers potentially increases the median distance between the patient and nearest treatment center and may affect access to treatment, including allocation to remission-induction chemotherapy and post-remission HSCTs. In addition, prompt initiation of supportive care in cases of treatment-related complications may be delayed or limited in patients living furthest away, ultimately affecting outcomes.
A recent review on the effects of distance to treatment center on health outcomes (defined as survival, length of stay, and non-attendance at follow-up) in different, mostly non-acute patient categories, reported that 77% of studies found an association between increasing distance and travel time to treatment center and worse health outcomes.11 However, only half of the studies included cancer patients, and only one included HSCT patients. We believe that AML patients differ from those included in these studies in terms of acute presentation and the intensive regimens increasing the risk of life-threatening complications.
As such, two previous studies investigated the impact of distance to treatment center in AML patients and found no effect on survival.12,13 Limitations included lack of individual-level socioeconomic-, cytogenetic-, and treatment information, as well as small and selected populations.
Although distance to a specialized treatment center may affect access to treatment and survival in AML more than in chronic diseases and solid cancers, the Danish Healthcare setting may counteract these effects. Denmark is a small country covering only 43,098 square kilometers. It offers universal healthcare, thus patients have full access to free diagnostic workup, treatment, and follow-up within the public hospital system.2 Also, transportation to outpatient visits during periods of myelosuppression and convenient hospital-covered housing for patients and in some cases a relative at ”patient hotels” specially designed for individuals with diseases and disabilities are available during active treatment. No cancer treatment takes place in Danish private hospitals, and patients are referred to hospitals based on geography. Though patients are free to choose another facility, almost all patients are treated at the assigned and nearest specialized treatment center.9,14
To investigate the impact of distance to the nearest treatment center on outcome in AML in a universal healthcare setting, we conducted a nationwide populations-based cohort study using individual-level clinical and socioeconomic data, and estimated the effects of distance to the nearest university hospital treating patients with intensive-chemotherapy on the probability of remission-induction chemotherapy, clinical trial inclusion, treatment response, and overall survival in all Danish AML patients. Second, we estimated the effect of distance to transplant center on the probability of HSCT and overall survival post-transplant.
Methods
In the universal healthcare context, we hypothesized that the overall impact of distance would be negligible. However, if any subgroup effect were to be more pronounced, it would be expected to be during the outpatient course.
The study population included all adult Danish AML patients over the age of 25 years diagnosed between 2000 and 2014 registered in the Danish National Acute Leukemia Registry (DNLR) (coverage >99%).2 We used the Civil Person Registration (CPR) number assigned to all Danish citizens at birth or immigration to link data from different registries on an individual level (Figure 1A).15 Patient selection is shown in Figure 1B.
 |
Figure 1 (A) Registries used to combine administrative, clinical, and outcome data. (B) Flowchart showing the selection of the study population.Abbreviation: AML, acute myeloid leukemia. |
Treatment of AML
Remission-induction therapy and post-remission therapy are centralized at five (six since 2013) specialized treatment centers across Denmark, whereas only two centers are accredited to perform HSCT (Rigshospitalet, Copenhagen and, since 2009, Aarhus University Hospital).9 A national board generates consensus recommendations for treatment of AML, including recommendations for HSCT in CR1 and in the relapse setting.16 No differences in treatment effects across centers have yet been reported after adjusting for unequal distribution of, e.g., age, sex, and cytogenetic features, reducing the incentive to choose another treatment center.17
In AML, the only option to achieve a long-term survival is by remission-induction intensive chemotherapy. Post-remission therapy consisted of one or two courses of consolidation therapy, which was mostly administered in the inpatient setting. However, patients were discharged immediately thereafter, unless complications occurred, followed by close outpatient monitoring and support 1–3 times weekly between chemotherapy cycles. In high-risk cases of AML, HSCT (following 1–2 cycles of consolidation chemotherapy) may be recommended in CR1. Following HSCT in CR1, patients undergoing myeloablative transplantation were managed in the inpatient setting until engraftment, whereas reduced-intensity conditioning patients living closer than 30 minutes from the transplant center were managed as outpatients with daily outpatient visits until neutrophil count >0.5 109/L. In HSCT cases following non-ablative conditioning regimens, patients were followed by 3 weekly visits until day 28 and by 1–2 weekly visits thereafter.
Due to high treatment-toxicity and increasing treatment refractory disease in older patients, treatment options in older and fragile patients are the non-curative treatment options; including supportive care only and low-dose chemotherapy, which may control the leukemia for shorter periods of time. During the study period, patients receiving non-curative treatment options could be followed at regional hematological departments if they were closer to home.18
Socioeconomic information
Individualized socioeconomic information and demographics were retrieved from registries at Statistics Denmark.19–23
The distance from the city center of habitation to the nearest specialized treatment center offering remission-induction therapy was calculated using the shortest route (Google Maps) and grouped according to quintiles (<10, 10–25, 25–50, 50–100, >100 kilometers (km)). The distance to HSCT transplant center was grouped based on quartiles (<10, 10–50, 50–200, >200 km).
Additional information included highest attained education (primary education, secondary/vocational education, and higher education), household income (tertiles), occupation (employed, unemployed, receiving disability or anticipatory pension, and retirement pension), cohabitation (living alone or with an adult partner), marital status (married [including same-sex marriage], never married, divorced, widowed),24,25 and Western/non-Western origin. Western origin was defined as persons born outside of Denmark in a EU country, Andorra, Iceland, Liechtenstein, Monaco, Norway, San Marino, Switzerland, Vatican City, Canada, the US, Australia, or New Zealand.23
Clinical data
We obtained baseline demographics, laboratory results, and treatment information from the DNLR.2 Cytogenetic results were grouped according to MRC’s criteria (favorable, intermediate, adverse).26 Type of AML was grouped into de novo, secondary [s-AML], and therapy-related AML [t-AML].4 Information on non-AML-related comorbidities (according to a modified version of the Charlson Comorbidity Index,5 and cumulative length of hospital admission (day 0–100) were retrieved from The Danish National Patient Registry. Information regarding HSCT (e.g., date and disease stage) was obtained from local registries.
Outcomes
Primary outcomes were treatment with remission-induction chemotherapy, probability of CR defined as morphological CR after up to two cycles of induction therapy,27 HSCT performance in first complete remission (CR1), and overall survival. Remission-induction regimens was defined as standard to high-dose of cytarabine (≥100–400 mg/m) in combination with an anthracycline or anthracycline-like compound.28 Low-dose chemotherapy was defined as hypomethylating agents, low-dose cytarabine, or similar. Supportive care was defined as the absence of chemotherapy (hydroxyurea excluded) and included, e.g., blood products and antibiotics. Information on each patient’s vital status was obtained from the Civil Registration System. Secondary outcomes were pre-specified and included time from diagnosis to initiation of remission-induction therapy, cumulative length of hospital admission (day 0–100; from the DNLR) as a surrogate for complications during the induction phase.
Statistical analyses
We stratified descriptive data by distance to the nearest specialized treatment center.
We used logistic regression analysis to estimate the probability of remission-induction therapy by distance to a specialized treatment center in all patients, the probability of consolidating HSCT in first complete remission (CR1) for transplantation candidates (age<70 years, achievement of CR, non-favorable cytogenetics),16 and the probability of CR in patients receiving remission-induction therapy (crude and adjusted odds ratios [ORs]).
Patients were followed from diagnosis until death, emigration, or end of follow-up (February 18, 2016). We used Kaplan-Meier curves and Cox proportional hazards regression (hazard ratios [HRs] to assess the impact of distance to the nearest specialized treatment center on overall survival in all patients and in remission-induction therapy patients only. In addition, we estimated survival in mainly outpatient patients; patients receiving low-dose chemotherapy only, in patients post-remission (starting follow-up at time of CR1), and in HSCT patients post-transplant (starting follow-up at time of HSCT)). The proportional hazards model assumptions were graphically verified by log minus log plot and accepted.
Potential confounders were identified based on the current literature and drawing and analyzing causal diagrams (DAGs). All results were given crude and adjusted for the patient-related factors (sex, age [continuous], education, income, occupation, cohabitation status, and comorbidity [categorical]) as well as leukemia-related factors (white blood cell count [continuous], cytogenetics risk group, type of AML, and WHO/EGOG performance status [categorical]).29
We used shortest distance as reference. Estimates were given with corresponding 95% confidence intervals (CIs).
To test the robustness of our results, we repeated analyses using the distance to nearest specialized treatment center and HSCT center as continuous variables and stratified by median age (<65, ≥65 years) to address possible effect modification. In HSCT patients, we repeated survival analysis starting follow-up at day 100, to investigate survival effects in the HSCT outpatient setting. Finally, we repeated the primary analysis using a multiple imputation strategy, imputing missing values for possible confounders (WHO PS (0.5%), WBC (3%), comorbidity (8%), and cytogenetic risk group (in intensive therapy patients, 13%)).30–32
Statistical analyses were performed using Stata version 14.1 (Stata Corp., College Station, TX). The study was approved by the Danish Data Protection Agency (jr.nr. 1–16-02–321-18).
Results
Patient characteristics
A total of 2,992 patients diagnosed with AML were included in the study (Figure 1A). The median age at diagnosis was 68.5 years, and the median distance to a specialized treatment center was 40 km (interquartile range=10–77 km). Patients living furthest from a specialized center had a lower income and lower educational level. The median distance to a transplant center was 197 km (IQR=47–293).
Patient characteristics according to distance to nearest specialized treatment center treating patients with intensive chemotherapy are listed in Table 1. Patients originating from non-Western countries (≈2%) tended to live further from a specialized treatment center than patients of Western origin.
 |
Table 1 Patient characteristics according to distance to nearest specialized treatment center in 2,992 adult AML patients |
Effects of upfront AML treatment choice
Overall, 1,588 (53%) received intensive chemotherapy. Table 2 shows the association between the distance to the nearest specialized treatment center and the probability of treatment with intensive chemotherapy.
 |
Table 2 Association between distances to nearest specialized treatment center and probability of intensive chemotherapy in 2,992 acute myeloid leukemia patients. Logistic regression analysis, crude, and adjusted estimatesa |
Overall, distance to a specialized treatment center did not affect the probability of receiving remission-induction chemotherapy. However, patients younger than 65 years living >100 km from a specialized treatment center had a higher absolute probability of receiving intensive chemotherapy compared with patients younger than 65 years with a distance <10 km (95.4% vs 89.2%, aOR=7.5 (95% CI=2.0–27.5).
Of the 1,404 patients treated with non-curative treatment options, 24.7% (n=350) received low-dose outpatient chemotherapy and the remaining supportive care only. The proportion of patients receiving low-dose chemotherapy vs supportive care-only did not vary by distance to a specialized treatment center. In patients receiving low-dose chemotherapy, crude and adjusted survival from time of diagnosis was also not affected by distance to a specialized treatment center (Figure 2).
Treatment response in intensive therapy patients
Of the 1,588 patients receiving intensive chemotherapy, 71% (n=1,045) obtained a CR (75.9% in patients <65 years, 62.6% in patients ≥65 years). The proportion of patients achieving CR did not vary by distance to a specialized treatment center. Crude and adjusted results are shown in Table 3. No effect of distance to specialized treatment center was observed on the probability of achieving a CR after induction chemotherapy.
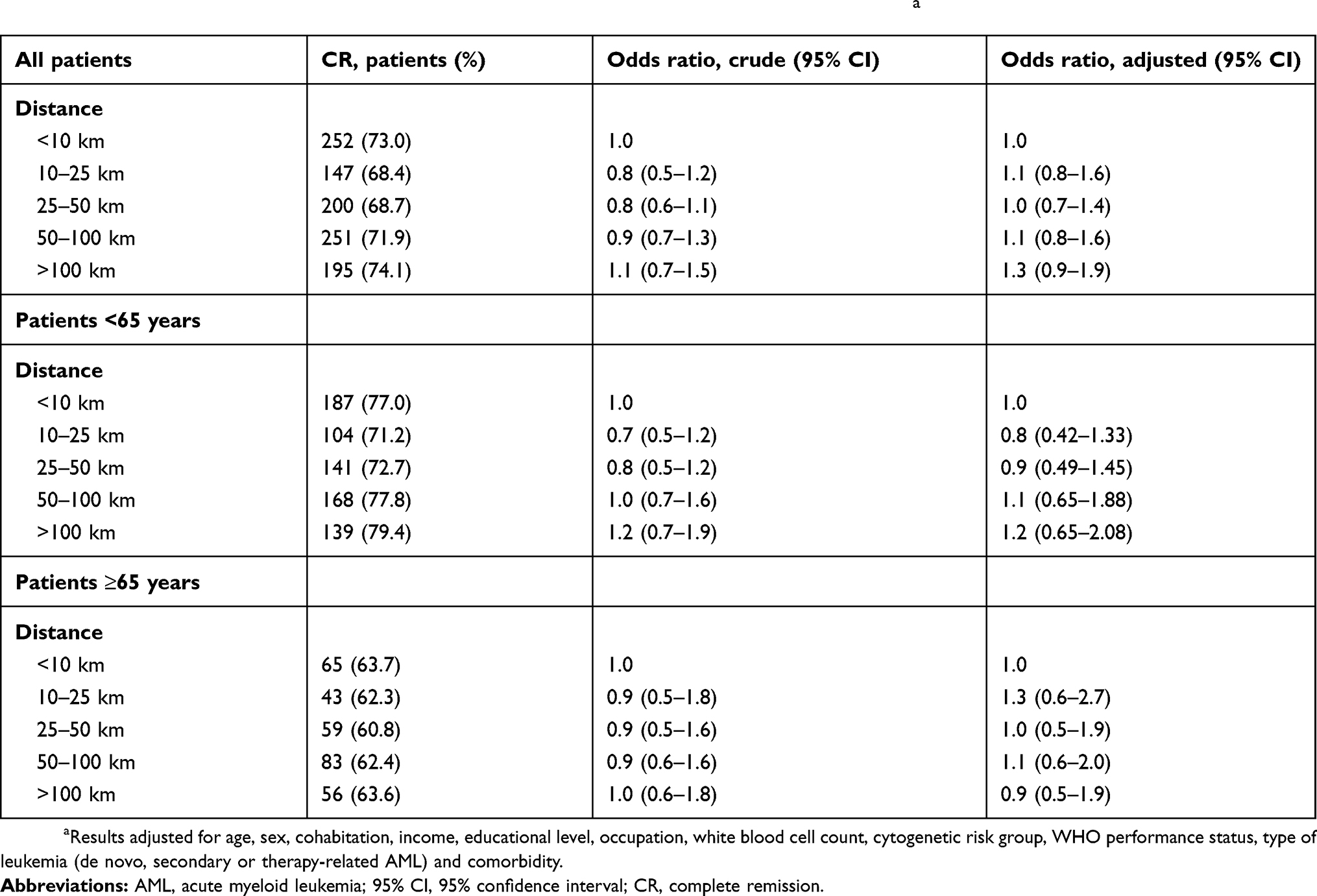 |
Table 3 Association between distances to nearest specialized treatment center and probability of CR in 1,463 AML patients treated with remission-induction therapy. Logistic regression analysis, crude, and adjusted estimatesa |
Probability of HSCT in CR1 and survival from time of HSCT
In the 866 patients younger than 70 years with non-favorable cytogenetic who achieved a CR1, 184 (21%) patients received an HSCT in CR1. Consolidation with a HSCT was more common in patients living closest to a transplant center (distance <10 km, 20.4%; 10–50 km, 17.8% (OR=0.8, CI=0.5–1.3), 50–200 km, 12.4% (OR=0.6, CI=0.3–0.9); >200 km, 14.6% (OR=0.7, CI=0.4–1.1)). However, adjustment for age and other potential confounders weakened this association (10–50 km, aOR=0.9 (CI=0.5–1.5); 50–200 km, aOR=0.7 (0.4–1.2); >200 km, aOR=0.8 (0.5–1.4) compared with distance <10 km). Restricting analysis to patients diagnosed before 2009 when HSCTs were exclusively performed at Copenhagen University Hospital (Rigshospitalet) and the distance, therefore, was extended for patients in the Western half of Denmark, did not change the estimates.
In the patients receiving a HSCT in CR1, the distance to a transplant center did not impact survival from time of transplant (10–50 km, OR=0.9 (CI=0.5–1.8); 50–200 km, OR=1.0 (0.4–2.3); >200 km, aOR=0.9 (0.4–1.8) compared with distance <10 km). Starting follow-up at day 100 post-transplant did not change the interpretation of results.
Overall survival in all patients, in intensive therapy patients, and in CR patients only
The total time from diagnosis to the end of follow-up was 5,544 years. Among patients receiving intensive chemotherapy, the follow-up time was 4,850 years and median follow-up was 514.5 days (interquartile range=179.5–1451 days). Figure 2 shows crude survival by distance to a specialized treatment center for patients overall, in intensive therapy patients only, and by age.
 |
Figure 2 Association between distances to the nearest specialized treatment center and mortality. Results of all AML patients by age and by treatment intensity. Cox regression analysis, crude, and adjusted estimates.a Notes: Patients followed from time of diagnosis to death or end of follow-up. aResults adjusted for age, sex, cohabitation, income, educational level, occupation, white blood cell count, cytogenetic risk group, WHO performance status, type of leukemia (de novo, secondary, or therapy-related AML) and comorbidity. Abbreviations: AML, acute myeloid leukemia; 95% CI, 95% confidence interval. |
Figure 3 shows crude and adjusted estimates (ORs) and Forest plots according to categorical distance overall, by age group, and by treatment intensity. For all patients, irrespective of treatment intensity and age group, no difference in overall survival was observed between groups of varying distance to treating hospital. Adjusting for confounders did not change the interpretation of the results. Also, no effect of distance to a specialized treatment center was observed for intensive therapy patients only. Once in remission following induction chemotherapy (n=959), distance still had no impact on survival.
 |
Figure 3 Crude survival according to categorical distance to the nearest specialized treatment center. Overall survival in all patients (A), in patients <65 years (B), in all patients ≥65 years (C), in all patients receiving intensive chemotherapy (D), and in all patients receiving intensive chemotherapy surviving to achieve a CR (E).Abbreviations: AML, acute myeloid leukemia; CR, complete remission. |
Sensitivity analyses
In general, stratifying analyses by age did not modify any of the results (stratified by median age, <65 and ≥65 years). Analyzing the distance to the nearest treatment center as a continuous variable did not change the interpretation of the probability of CR (aOR=1.0; 95% CI=0.99–1.0). Finally, imputing missing values for clinical and socioeconomic factors did not affect results.
Discussion
In this large population-based study investigating the effect of distance to a specialized treatment center, we did not find increased distance to the treatment center to negatively affect access to intensive chemotherapy or HSCT, the probability of CR, or survival in AML patients neither in the inpatient or outpatient settings when adjusting for potential confounding factors.
In general, distance did not affect access to intensive chemotherapy or HSCT. However, patients younger than 65 years traveling more than 100 km had a higher probability of receiving chemotherapy after adjusting for available confounding factors. The precision of this estimate was low, and this finding may well be explained by chance. The absolute difference in the probability of intensive chemotherapy was only 6% in a high-prevalence cohort, in which case odds ratios cannot be translated into relative risks and may appear inflated.33 Importantly, the findings of a higher probability of remission-induction chemotherapy did not translate into better overall survival.
This study was based on high-quality registries including the CPR-registry, which allowed us to obtain detailed, complete, and up-to-date follow-up data reducing misclassification bias. It was possible to obtain data on important clinical factors, thereby allowing us to investigate a possible effect in several patient sub-groups and at different times during the disease course. Also, detailed information on important prognostic factors made it possible to take most relevant confounders into account. Data was obtained prospectively and unrelated to the study aim, thereby reducing information bias. The median distance was comparable to prior studies both from the US (eg, a median of 24 miles [38 km] for remission-induction therapy and a range of 2–358 minutes for HSCT).12,34
Few previous US studies found longer travel distance to be associated with superior treatment outcomes in other malignancies, likely explained by distance bias associations.11 Differences in AML outcomes have been shown between eg, academic centers and non-academic centers in the US.35 Though under-insured and low-income patients may live furthest from the nearest potential treatment center, well-insured and socioeconomically prosperous with a priori superior prognosis may be motivated and able to travel further to get treatment at the leading academic institutions, which may bias results.
Interestingly, two US acute leukemia studies conducted in completely different settings have previously found comparable results. Master et al.13 examined 67,443 AML patients and found no survival difference between patients living <30 vs >30 miles from the treatment center (HR for OS=0.99; 95% CI=0.99–1.02),whereas Rodriguez et al.,12 in a single center study including only 281 intensive therapy AML patients, found no correlation of OS with an increase in distance to treatment center by 20 mile intervals (HR for OS=0.99; 95% CI=0.98–1.02). Though these studies imply that distance, also in large countries with insurance-based healthcare, does not affect treatment and outcomes in AML, bias and important methodological limitations might explain the results in selected cohorts of patients who are able to make it to these treatment centers.
A lack of associations between effects of distance and survival has also been reported in HSCT patients.36 In contrast, one study reported that distance to the HSCT center negatively affected survival more than 1-year after HSCT,34 but patients with severe complications eg, chronic graft vs host disease, not being referred back to their local oncologist could explain the lack of survival difference in the first year.
We found a clear association between distance >200 km to the HSCT center and a reduced probability of HSCT performance. However, after confounder adjustment this association was less clear and overall survival in intensive therapy patients was not affected.
Our findings may be affected by the Danish universal healthcare system. Still, it is likely that very long distances may affect the probability of “prophylactic” procedures requiring extensive follow-up for months and in the case of GVHD for years. For the same reasons, it is likely that an eventual survival effect of long distance to specialized treatment center would especially affect patients in the outpatient setting, since time and distance may negatively impact access to life-saving procedures and close follow-up. However, we did not find distance to have an effect on survival in these subgroups: low-dose chemotherapy patients, intensive therapy patients in CR, and also not in HSCT patients post-transplant.
We have recently shown that, though Denmark offers universal healthcare, specifically socioeconomic factors do affect access to treatment and survival in AML patients. In contrast to distance to the specialized treatment center, advanced age and living alone have been found to affect Danish patients’ access to intensive chemotherapy and, thus, overall survival.24 Also, education, but not income, has an impact on the probability of undergoing a HSCT and on overall survival in patients younger than 60 years.25 In these patients, adjusting for distance to the treatment center did not affect reported results.
Our study has limitations. We used the shortest distance and not alternative measures of potential barriers to reach a treatment center, such as travel time or costs. Denmark consists of more than 400 islands, 70 of those populated, but most connected by bridges.23 A small percentage of patients living on islands requiring ferry transportation may experience a significant geographical barrier not captured by this study. Patients of non-Western origin tended to live further from a specialized treatment center. Only accounting for 2%, not adjusting for this is unlikely to influence the overall results. Still, it would have been interesting to investigate a potential subgroup effect in these patients. Our analyses did not account for changes in location during the treatment cause, but almost all patients are treated at the closest specialized treatment center, and potential misclassification is thought to be non-differential and neglectable. Despite the high completeness and quality of individual variables, the limitations included the exclusion of patients with missing data on treatment intent (1.4%), education, cohabitation, and income (8.9%). However, median distance and characteristics of these patients did not differ from the final study population, and thus, it is not likely to have affected the overall conclusions.
Conclusion
In a population-based setting, distance, to the specialized treatment facility offering remission-induction chemotherapy or HSCT, does not negatively affect access to care and survival in AML patients. These findings support that the current centralization of specialized treatment aiming to treat AML at high-volume centers only does not negatively affect AML outcomes in a universal healthcare system.
Disclosure
This study was supported by The Danish Cancer Society (COMPAS). The funding source did not contribute to the design, performance, analysis, or reporting of the study. The study has been presented in abstract form (oral presentation) at ASH (December 2018). The authors declare that there are no conflicts of interest to report in relation to the present study.
References
1. Döhner H, Estey E, Grimwade D, et al. Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel. Blood. 2017;129(4):424–447. doi:10.1182/blood-2016-08-733196
2. Østgård LS, Nørgaard JM, Severinsen M, et al. Data quality in the Danish National Acute Leukemia Registry: a hematological data resource. Clin Epidemiol. 2013;5:335–344. doi:10.2147/CLEP.S48411
3. Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues WHO Classification of Tumours. Vol. 2,
4. Granfeldt Ostgard LS, Medeiros BC, Sengelov H, et al. Epidemiology and clinical significance of secondary and therapy-related acute myeloid leukemia: a national population-based cohort study. J Clin Oncol. 2015;33(31):3641–3649. doi:10.1200/JCO.2014.60.0890
5. Ostgard LS, Norgaard JM, Sengelov H, et al. Comorbidity and performance status in acute myeloid leukemia patients: a nation-wide population-based cohort study. Leukemia. 2015;29(3):548–555. doi:10.1038/leu.2014.234
6. Hahn AW, Jamy O, Nunnery S, et al. How center volumes affect early outcomes in acute myeloid leukemia. Clin Lymphoma Myeloma Leuk. 2015;15(11):646–654. doi:10.1016/j.clml.2015.07.646
7. Giri S, Pathak R, Aryal MR, Karmacharya P, Bhatt VR, Martin MG. Impact of hospital volume on outcomes of patients undergoing chemotherapy for acute myeloid leukemia: a matched cohort study. Blood. 2015;125(21):3359–3360. doi:10.1182/blood-2015-01-625764
8. Hillner BE, Smith TJ, Desch CE. Hospital and physician volume or specialization and outcomes in cancer treatment: importance in quality of cancer care. J Clin Oncol. 2000;18(11):2327–2340. doi:10.1200/JCO.2000.18.11.2327
9. [Sundhedsstyrelsen] TDHA. Gældende specialeplan for hæmatologi Maj. 2019. Available from: https://www.sst.dk/da/Viden/Specialeplanlaegning/Gaeldende-specialeplan/Specialeplan-for-intern-medicin-haematologi.
10. Ostgard LS, Norgaard JM, Raaschou-Jensen KK, et al. The Danish National Acute Leukemia Registry. Clin Epidemiol. 2016;8:553–560. doi:10.2147/CLEP.S99460
11. Kelly C, Hulme C, Farragher T, Clarke G. Are differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review. BMJ Open. 2016;6(11):e013059. doi:10.1136/bmjopen-2016-013059
12. Rodriguez CP, Baz R, Jawde RA, et al. Impact of socioeconomic status and distance from treatment center on survival in patients receiving remission induction therapy for newly diagnosed acute myeloid leukemia. Leuk Res. 2008;32(3):413–420. doi:10.1016/j.leukres.2007.07.015
13. Master S, Munker R, Shi Z, Mills G, Shi R. Insurance status and other non-biological factors predict outcomes in acute myelogenous leukemia: analysis of data from the national cancer database. Anticancer Res. 2016;36(9):4915–4921. doi:10.21873/anticanres.11057
14. Danish Regions. https://www.regioner.dk/services/in-english.
15. Schmidt M, Pedersen L, Sorensen HT. The Danish Civil Registration System as a tool in epidemiology. Eur J Epidemiol. 2014;29(8):541–549. doi:10.1007/s10654-014-9930-3
16. The Danish Society of Hematology. [Recommandations for blood and bonemarrow transplatation]. 2017. [updated 2017]. Available from: http://www.hematology.dk/index.php/vejledninger/knoglemarvstransplantation.0.
17. The Danish National Acute Leukemia Group. Annual Report [Årsrapport]. Denmark: The Danish National Acute Leukemia Group; 2017.
18. The Danish National Acute Leukemia Group; Denmark. The Danish Society of Hematology. [Recomandations for Treatment, Diagnostics, and Management of Acute Myeloid Leukemia (AML)]; 2019.
19. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. doi:10.1177/1403494811405098
20. Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7 Suppl):91–94. doi:10.1177/1403494810394715
21. Petersson F, Baadsgaard M, Thygesen LC. Danish registers on personal labour market affiliation. Scand J Public Health. 2011;39(7 Suppl):95–98. doi:10.1177/1403494811408483
22. Sortso C, Thygesen LC, Bronnum-Hansen H. Database on Danish population-based registers for public health and welfare research. Scand J Public Health. 2011;39(7 Suppl):17–19. doi:10.1177/1403494811399171
23. Statistics Denmark. 2017. http://www.dst.dk/en.
24. Ostgard LSG, Norgaard M, Medeiros BC, et al. Associations between cohabitation status, treatment, and outcome in AML patients: a national population-based study. Blood. 2018;131(24):2730–2733. doi:10.1182/blood-2017-11-814327
25. Ostgard LSG, Norgaard M, Medeiros BC, et al. Effects of education and income on treatment and outcome in patients with acute myeloid leukemia in a tax-supported health care system: a national population-based cohort study. J Clin Oncol. 2017;35:3678–3687. doi:10.1200/JCO.2017.73.6728
26. Grimwade D, Hills RK, Moorman AV, et al. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010;116:354–365. doi:10.1182/blood-2009-11-254441
27. Cheson BD, Bennett JM, Kopecky KJ, et al. Revised recommendations of the international working group for diagnosis, standardization of response criteria, treatment outcomes, and reporting standards for therapeutic trials in acute myeloid leukemia. J Clin Oncol. 2003;21(24):4642–4649. doi:10.1200/JCO.2003.04.036
28. Lowenberg B, Pabst T, Vellenga E, et al. Cytarabine dose for acute myeloid leukemia. N Engl J Med. 2011;364(11):1027–1036. doi:10.1056/NEJMoa1010222
29. Oken M, Creech R, Tormey D, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol.
30. Rising B. Multiple Imputation. Bologna (Italy): StataCorp LP; 2010.
31. Sterne JAC, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009 Jun 29;338:b2393. doi: 10.1136/bmj.b2393.
32. White IR, Royston P. Imputing missing covariate values for the Cox model. Stat Med. 2009;28(15):1982–1998. doi:10.1002/sim.3618
33. Jun Zhang MB, PhD KF, Yu P. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. JAMA. 1998;280:1690–1691. doi:10.1001/jama.280.19.1690
34. Abou-Nassar KE, Kim HT, Blossom J, et al. The impact of geographic proximity to transplant center on outcomes after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2012;18(5):708–715. doi:10.1016/j.bbmt.2011.08.022
35. Bhatt VR, Shostrom V, Giri S, et al. Early mortality and overall survival of acute myeloid leukemia based on facility type. Am J Hematol. 2017;92(8):764–771. doi:10.1002/ajh.24767
36. Khera N, Gooley T, Flowers MED, et al. Association of distance from transplantation center and place of residence on outcomes after allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2016;22(7):1319–1323. doi:10.1016/j.bbmt.2016.03.019
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.