Back to Journals » Biologics: Targets and Therapy » Volume 20
Long-Term TIE2 Inhibition in a TEK-Mutated Venous Malformation: A 3-Year Clinical Experience
Authors Triana P ![]() , Marín E, Mendieta C, Fernández L, Rodriguez-Laguna L, Lopez-Gutierrez JC
, Marín E, Mendieta C, Fernández L, Rodriguez-Laguna L, Lopez-Gutierrez JC
Received 10 March 2026
Accepted for publication 7 May 2026
Published 19 May 2026 Volume 2026:20 606831
DOI https://doi.org/10.2147/BTT.S606831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Paloma Triana,1 Elena Marín,2 Covadonga Mendieta,2 Lucía Fernández,3 Lara Rodriguez-Laguna,4 Juan Carlos Lopez-Gutierrez1
1Pediatric Surgery, La Paz Hospital, Madrid, Spain; 2Vascular Surgery, La Paz Hospital, Madrid, Spain; 3Interventional Radiology, La Paz Hospital, Madrid, Spain; 4Genetics, La Paz Hospital, Madrid, Spain
Correspondence: Paloma Triana, Pediatric Surgery, La Paz Hospital, Paseo de la Castellana 261, Madrid, 28046, Spain, Tel +0034 91 727 70 19, Email [email protected]
Background: Venous malformations (VMs) are slow-flow vascular anomalies frequently driven by somatic activating mutations in TEK/TIE2 receptor. Medical treatment options remain limited; while mTOR inhibition with sirolimus has shown moderate benefit, direct TIE2 inhibition has a strong biological rationale and emerging clinical evidence.
Case Presentation: We report a 51-year-old patient with a diffuse VM involving the right cervical region, thorax, and upper extremity, associated with a somatic mosaic TEK (L914F) variant. The disease was refractory to conventional therapies and complicated by chronic coagulopathy. Compassionate-use treatment with the selective TIE2 inhibitor rebastinib was initiated based on a previously reported patient. Over 3 years of follow-up, the patient experienced sustained clinical benefit with decreased pain and inflammation, partial volume reduction, functional improvement, and stabilization of coagulopathy with manageable toxicity. Unfortunately, the interruption in the production of the drug made it necessary to try other less specific alternatives like PI3K inhibitor alpelisib.
Conclusion: This second long-term clinical experience supports the sustained efficacy and safety of TIE2 inhibition in selected TEK-mutated VMs and highlights the therapeutic gap arised from drug discontinuation, underscoring the need for alternative targeted strategies and prospective evaluation.
Keywords: vascular malformations, venous malformations, targeted therapies, TIE2 inhibitor, rebastinib
Introduction
Vascular malformations comprise a heterogeneous group of disorders characterized by dysplastic vessels that may cause pain, deformity, functional impairment, and other complications. According to the latest update of the ISSVA classification in 2025 (International Society for the Study of Vascular Anomalies), vascular malformations are categorized as slow-flow, fast-flow or developmental anomalies of named vessels.1 These disorders are mainly caused by sporadic postzygotic somatic mutations affecting genes controlling two major signaling pathways regulating cell proliferation, migration and differentiation: PI3K/Akt/mTOR and RAS/MEK/ERK. Many of these mutations are “gain-of-function” or “activating” variants that promote aberrant tissue proliferation, angiogenesis and/or lymphangiogenesis.2
Venous malformations (VMs), which belong to the slow-flow group, are the most frequent subtype and are characterized by ectatic venous channels that progressively enlarge and may associate localized intravascular coagulopathy, with an increased risk of thrombosis and thromboembolic events, especially in adults. All known inherited VMs and approximately half of sporadic VMs harbor activating variants in the endothelial tyrosine kinase receptor TIE2 (encoded by TEK), while around 20% of TEK-negative sporadic VMs present variants in PIK3CA (phosphatidylinositol-4,5-bisphosphate3-kinase catalytic subunit alpha).3,4
Over the last decade, advances in genetic testing have enhanced our understanding of vascular anomalies and enable the repurposing of targeted therapies originally developed for cancer. Sirolimus, an mTOR inhibitor, has emerged as the current backbone of systemic therapy for complex vascular anomalies, although there is no direct inhibition of the known mutations and responses are often partial and variable.
PIK3CA inhibitors, such as alpelisib, have already been used in some selected VMs with partial response. Against this background, direct inhibition of TIE2 represents a logical step although unexplored therapeutic strategy in VMs driven by TEK mutations.
Rebastinib is a potent and selective TIE2 kinase inhibitor with robust preclinical evidence in cancer models and limited clinical experience in vascular anomalies, restricted to a single prior compassionate-use case report describing short-term improvement.5 We present the long-term clinical course of a patient with an extensive symptomatic VM treated with rebastinib in monotherapy for over three years.
Case Presentation
A 51-year-old female with an extensive VM involving the right cervical region, right hemithorax, and right upper limb was referred to our center after a long history of multimodal interventions, including multiple surgical resections and sclerotherapy sessions. She had been diagnosed at birth, after a controlled and uneventful pregnancy, with a cervicothoracic VM involving the dorsal and pectoral regions, right neck, right pleural cavity, mediastinum and right upper limb from shoulder to hand (Figure 1).
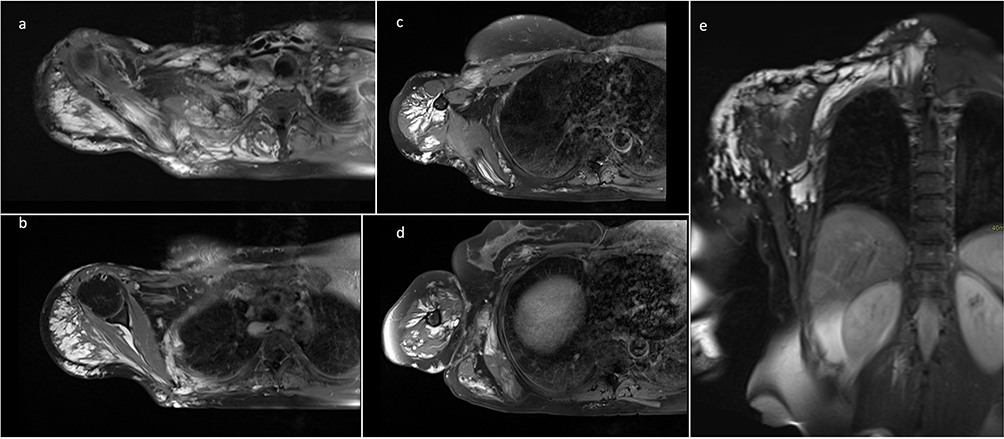 |
Figure 1 Axial post-contrast T1-weighted MRI images (a–d) and a coronal fat-suppressed T2-weighted MRI image (e) demonstrate an extensive vascular malformation involving the cervical region, the posterolateral chest wall, and the right upper extremity, with both superficial and deep components. The malformation involves the latissimus dorsi, subscapularis, supraspinatus, and infraspinatus muscles, as well as the intercostal, paravertebral, and pectoral muscles. |
At our evaluation, the patient exhibited chronic coagulopathy with elevated D-dimer levels (up to 59,000 ng/mL) and mild thrombocytopenia (120,000/µL). Molecular analysis performed on affected tissue identified a somatic mosaic TEK variant (c.2740C>T; p.Leu914Phe) with an allele frequency of 2–8%. Ongoing treatments included intermittent compression therapy, anticoagulation with fondaparinux, sirolimus, and symptomatic management with rehabilitation and extensive analgesic therapy.
Pain control required daily non-opioid analgesics (acetaminophen, metamizole), weak opioids (tramadol), strong opioids (tapentadol, oxycodone) and adjuvant neuropathic agents (pregabalin, amitriptyline, escitalopram). A cervical neurostimulator had been implanted in July 2018 due to chronic pain.
The patient had a history of more than 25 procedures performed during childhood at another institution, in addition to 14 diode laser sessions and 4 sclerotherapy treatments at our facility, all performed by the vascular surgery department. Since December 2015, the patient received sirolimus on a compassionate use basis, showing stability with no progression of the venous malformation, although requiring the same amount of analgesics. She however developed severe mucositis, requiring treatment to be interrupted on three occasions over 7 years.
Despite this regimen, the patient reported daily pain, persistent inflammation with limited mobility and inability to carry loads, and dyspnea, mainly during exercise and occasionally at rest, without postural or Valsalva dependence. There was also a sensory and motor deficit in the first three digits of the right hand consistent with prior radial nerve injury.
Given the progressive deterioration in quality of life, persistent pain despite intensive analgesic treatment, and lack of alternative therapeutic options; compassionate-use with rebastinib was considered over alternative targeted therapies due to the presence of a confirmed activating TEK mutation, making direct TIE2 inhibition a more mechanism-aligned strategy compared to downstream pathway inhibition, and our previous positive clinical experience.5 Institutional approval for compassionate use was obtained from La Paz Hospital (Madrid, Spain), in accordance with local regulatory requirements. After approval by local authorities and informed consent, rebastinib was initiated in October 2022 at 25 mg once daily and gradually escalated to 50 mg twice daily by january 2023, the recommended dose in clinical trials, in the absence of relevant adverse events.
Treatment efficacy was assessed through full physical exam, serial lesion measurements, clinical photographs, pain scores, functional status evaluation, and complete blood analysis at each visit. Safety monitoring included renal and liver function tests and ophthalmologic examination. CT scan of the affected regions was performed after 1 year of treatment (to compare to already performed baseline CT) and magnetic resonance imaging (MRI) was performed after 2 years of treatment.
Within the first month, the patient reported a marked reduction in pain and inflammation, allowing progressive tapering of analgesics. Partial improvement of lymphedema facilitated weekly rehabilitation sessions. A modest but sustained reduction in limb perimeter was documented (arm from 32 to 29 cm, forearm from 26 to 25 cm). Imaging with CT and MRI confirmed a mild decrease in the malformative component of the posterior chest wall and the root of the right upper extremity, affecting both the superficial and deep intramuscular planes, at 2 years of treatment. (Figures 2 and 3).
 |
Figure 2 Clinical evolution of an extensive cervicothoracic and upper limb venous malformation under TIE2 inhibition with rebastinib. Serial photographs obtained at baseline (a and b), 18 months (c and d), and 36 months (e and f) of rebastinib therapy show progressive reduction in congestion and lesion prominence. |
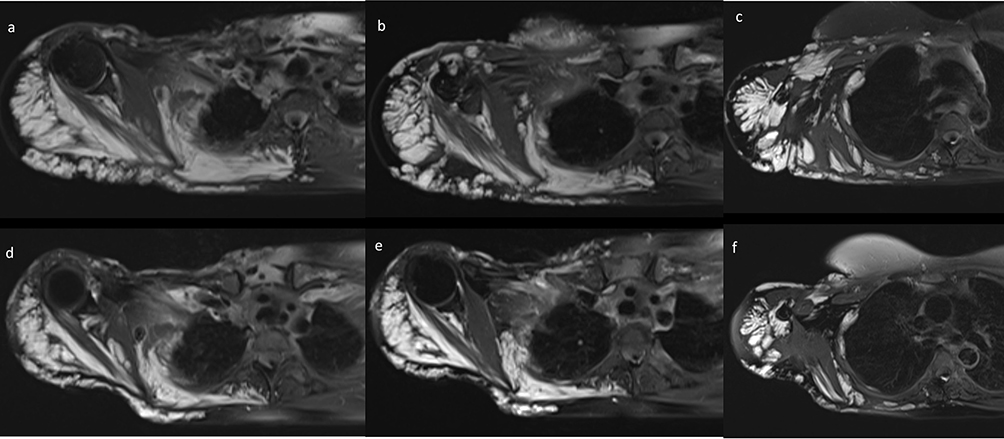 |
Figure 3 Axial fat-suppressed T2-weighted MRI images obtained in 2020 (a–c) [2 years pre-treatment] and 2024 (d–f) [2 years on treatment] show a mild decrease in the malformative component of the posterior chest wall and the root of the right upper extremity, affecting both the superficial and deep intramuscular planes. |
Patient also underwent partial resection of the VM in the axillary region due to a painful phlebolith and one session of sclerosis with ethoxisclerol foam in neck planned prior to rebastinib treatment, while maintaining rebastinib treatment, at 3 years and 1 year of treatment respectively.
The patient’s Karnofsky performance status increased to 90% with notable gains in daily mobility and functional independence. Coagulopathy improved, with a marked initial decrease in D-dimer levels followed by moderate fluctuations over time, while platelet counts remained stably midly reduced. The neurostimulator was turned off in July 2023 and definitively removed in September 2025. At the time of last follow-up, the patient required no analgesic medication. Data on clinical evolution is summarized in Table 1.
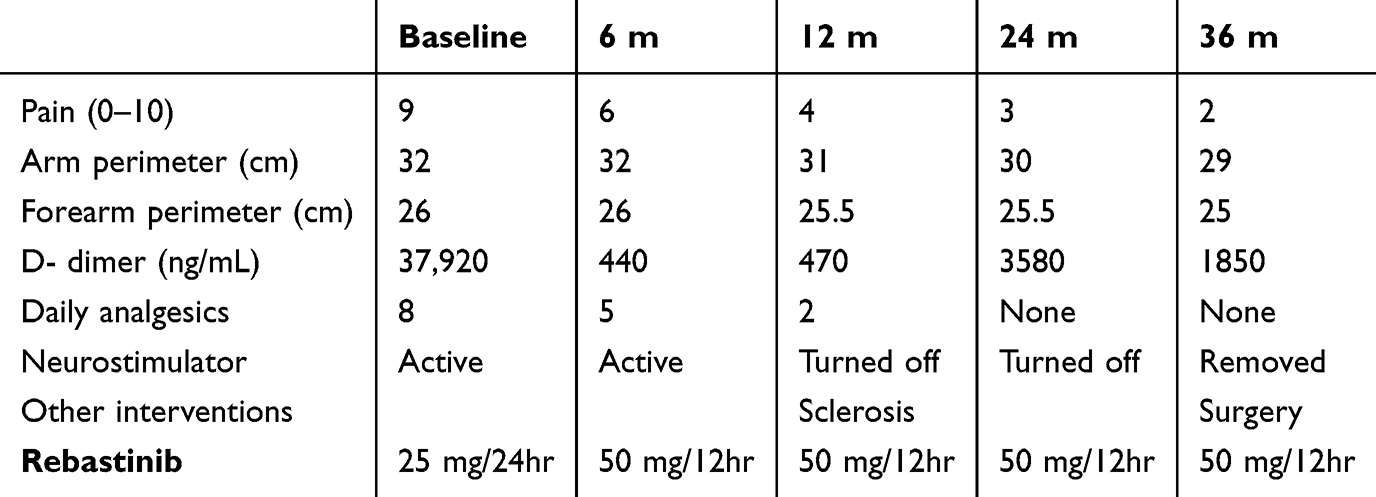 |
Table 1 Clinical Evolution with Rebastinib Treatment |
There was no evidence of severe or dose-limiting toxicity as assessed by heart, liver, kidney function, muscle, eye, and blood testing. Adverse events included transient mucositis early in treatment and grade I self-limited myalgias.
After 3 years of treatment, and due to discontinuation of rebastinib supply, compassionate-use therapy with alpelisib (PIK3CA inhibitor) is planned to start in March 2026.
Discussion
This report extends our previous publication by providing long-term follow-up (3 years), documenting sustained safety an efficacy of TIE2 inhibition in a TEK-mutated VM, and addressing the clinically relevant issue of drug discontinuation and therapeutic transition. The first clinical application of rebastinib in a patient with a vascular malformation was reported in 2023, demonstrating short-term lesion size reduction and quality-of-life improvement.5 This case suggests sustained clinical benefit in terms of symptom control and quality-of-life improvement, with modest lesion size reduction and no major safety concerns over prolonged exposure.
The identification of the specific molecular alterations in vascular anomalies has catalyzed the development of targeted therapies. While mTOR inhibition with sirolimus has become the backbone of medical therapy for complex VMs, demonstrating clinical efficacy especially in refractory patients, it represents downstream pathway modulation of TIE2 signaling.6 In contrast, TIE2 inhibition directly targets the mutant protein driving the lesions, offering a more mechanism-aligned therapeutic approach in TIE2-mutated lesions.
Rebastinib, originally developed as a switch-control kinase inhibitor targeting BCR-ABL1 and FLT3 in hematologic malignancies, has subsequently been identified as a potent and selective TIE2 inhibitor, making it of particular interest for TEK-driven vascular anomalies.7,8 Mechanistically, rebastinib blocks TIE2 receptor phosphorylation and downstream signaling, thereby inhibiting angiopoietin/TIE2-mediated angiogenesis and vascular remodeling.7
In clinical trials for oncologic indications, rebastinib has shown acceptable safety profiles with manageable adverse events. Recent phase Ib trials in metastatic breast cancer have used doses of 50–100 mg twice daily in combination with chemotherapy, demonstrating pharmacodynamic evidence of TIE2 inhibition.9 Common treatment-emergent adverse events include anemia, fatigue, anorexia, leukopenia, hyperglycemia, and muscular weakness, with most events being grade 2 or lower.9,10 Notably, none of these dose-limiting toxicities were observed in our patient despite prolonged exposure, with manageable adverse events. This long-term safety profile is encouraging but requires validation in larger cohorts.
Alternative targeted treatments, such as the PI3Kα inhibitor alpelisib, have shown promising results in cohorts of VMs with TEK or PIK3CA mutations, with marked quality-of-life and radiologic improvements.11,12 Although most VMs are driven by TEK mutations, downstream pathway overlap with PI3K/AKT/mTOR signaling provides a biological rationale for considering PI3K inhibition when direct TIE2 inhibition is unavailable.
This report has several limitations. First, the concurrent use of surgical resection and sclerotherapy during treatment represents a potential confounding factor, limiting the ability to attribute clinical improvement exclusively to rebastinib. Second, the discrepancy between marked clinical improvement and modest radiologic response raises questions regarding the mechanism of action, potentially suggesting a predominant anti-inflammatory or hemodynamic effect rather than substantial structural regression. Lastly, this report remains observational and lacks standardized imaging volumetry or biomarker correlates. Fluctuations in D-dimer and partial lesion changes highlight the complexity of VM response assessment. As this report builds upon prior work from the same group, the potential for observational bias should be acknowledged, although efforts were made to provide objective clinical and laboratory follow-up data.
The convergence of molecular diagnostics and targeted therapeutics represents a paradigm shift in the management of vascular malformations. The identification of TEK mutations in nearly half of sporadic VMs, combined with the availability of selective TIE2 inhibitors like rebastinib, enables a precision medicine approach for patients with refractory or extensive disease. This is particularly relevant given that conventional therapies often provide incomplete responses and require repeated interventions.
The discontinuation of rebastinib production underscores a critical gap between biological rationale and real-world access to targeted therapies in rare diseases. Establishing registries and prospective studies or clinical trials for TIE2-targeted therapies is warranted.
Conclusion
This extended clinical observation illustrates that long-term TIE2 inhibition with rebastinib can be associated with sustained symptomatic improvement, functional recovery, and acceptable safety profile in a patient with a severe, refractory TEK-mutated VM. Although radiologic changes were modest, the durable clinical benefit and stabilization of coagulopathy highlight the relevance of targeting the primary molecular driver of the disease.
Beyond the individual outcome, this case underscores both the potential and the fragility of precision medicine approaches in vascular anomalies, where promising targeted therapies may become unavailable despite clinical benefit. Systematic exploration of TIE2-directed strategies, integration of molecular diagnostics into treatment algorithms, and the development of sustainable access pathways are urgently needed to translate biological rationale into durable clinical care.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Ethical and Informed Consent Statement
Ethical approval was waived by Hospital La Paz due to the retrospective, anonymized nature of the study. Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
Acknowledgment
The authors are grateful to the patient, who with willingness to share her story was crucial to this project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Dr Juan Carlos Lopez-Gutierrez provided educational courses for Alexion Pharmaceutical. The authors declare that they have no other conflicts of interest with regard to the content of this report.
References
1. Goldenberg DC, Vikkula M, Penington A, et al. Updated classification of vascular anomalies. a living document from the international society for the study of vascular anomalies classification group. J Vasc Anom. 2025;6(2):e113. doi:10.1097/JOVA.0000000000000113
2. Li GX, Sebaratnam DF, Pham JP. Targeted therapies for slow-flow vascular malformations. Australas J Dermatol. 2025;66(3):142–6. doi:10.1111/ajd.14451
3. Limaye N, Wouters V, Uebelhoer M, et al. Somatic mutations in angiopoietin receptor gene TEK cause solitary and multiple sporadic venous malformations. Nat Genet. 2009;41:118–124. doi:10.1038/ng.272
4. Limaye N, Kangas J, Mendola A, et al. Somatic activating PIK3CA mutations cause venous malformation. Am J Hum Genet. 2015;97:914–921. doi:10.1016/j.ajhg.2015.11.011
5. Triana P, Lopez-Gutierrez JC. Activity of a TIE2 inhibitor (rebastinib) in a patient with a life-threatening cervicofacial venous malformation. Pediatr Blood Cancer. 2023;70(8):e30404. doi:10.1002/pbc.30404
6. Van Damme A, Seront E, Dekeuleneer V, Boon LM, Vikkula M. New and emerging targeted therapies for vascular malformations. Am J Clin Dermatol. 2020;21(5):657–668. doi:10.1007/s40257-020-00528-w
7. Harney AS, Karagiannis GS, Pignatelli J, et al. The selective Tie2 inhibitor rebastinib blocks recruitment and function of Tie2Hi macrophages in breast cancer and pancreatic neuroendocrine tumors. Mol Cancer Ther. 2017;16(11):2486–2501. doi:10.1158/1535-7163.MCT-17-0241
8. Cortes J, Talpaz M, Smith HP, et al. Phase 1 dose-finding study of rebastinib (DCC-2036) in patients with relapsed chronic myeloid leukemia and acute myeloid leukemia. Haematologica. 2017;102(3):519–528. doi:10.3324/haematol.2016.152710
9. Anampa JD, Flynn DL, Leary C, et al. Phase Ib clinical and pharmacodynamic study of the TIE2 kinase inhibitor rebastinib with paclitaxel or eribulin in HER2-negative metastatic breast cancer. Clin Cancer Res. 2025;31(2):266–277. doi:10.1158/1078-0432.CCR-24-2464
10. Janku F, Hamilton E, Mathews C, et al. Open-label, multicenter, phase 1b/2 study of rebastinib in combination with paclitaxel to assess safety and efficacy in patients with advanced or metastatic endometrial cancer. J Clin Oncol. 2021;39(Suppl 15):5576. doi:10.1200/JCO.2021.39.15_suppl.5576
11. Zerbib L, Ladraa S, Fraissenon A, et al. Targeted therapy for capillary-venous malformations. Signal Transduct Target Ther. 2024;9(1):146. doi:10.1038/s41392-024-01862-9
12. Remy A, Tran TH, Dubois J, et al. Repurposing alpelisib, an anti-cancer drug, for the treatment of severe TIE2-mutated venous malformations: preliminary pharmacokinetics and pharmacodynamic data. Pediatr Blood Cancer. 2022;69(10):e29897. doi:10.1002/pbc.29897
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.