Back to Journals » Clinical Interventions in Aging » Volume 21
Long-Term Tai Chi Practice Modulates Cortical-Muscular Interactions During Walking in Older Adults: A Cross-Sectional Study
Authors Zhang Y, Song Q, Li X, Sun W, Yv B, Mao D, Mao M
Received 9 April 2026
Accepted for publication 9 June 2026
Published 26 June 2026 Volume 2026:21 615470
DOI https://doi.org/10.2147/CIA.S615470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Yvxi Zhang,1 Qipeng Song,1 Xinru Li,1 Wei Sun,1 Bin Yv,2 Dewei Mao,3 Min Mao4
1College of Sports and Health, Shandong Sport University, Jinan, Shandong, People’s Republic of China; 2Department of Electronic and Communication Engineering, Shandong College of Electronic Technology, Jinan, Shandong, People’s Republic of China; 3Division of Physical Education, The Chinese University of Hong Kong, Shenzhen, Guangdong, People’s Republic of China; 4School of Nursing and Rehabilitation, Shandong University, Jinan, Shandong, People’s Republic of China
Correspondence: Min Mao, School of Nursing and Rehabilitation, Shandong University, No. 44 Wenhua West Road, Jinan, Shandong, 250012, People’s Republic of China, Tel +86-13475999846, Email [email protected]
Purpose: The possible effects of Tai Chi exercise on neural coordination during walking in older adults remain unclear. This study aimed to compare cortical functional connectivity (FC) and corticomuscular coupling (CMC) during walking among older Tai Chi practitioners, older brisk walkers, and non-exercise controls.
Methods: A total of 62 participants were recruited in this study, including older Tai Chi practitioners (n=20), older brisk walkers (n=22), and non-exercise controls (n=20). Participants performed a walking test during which data were collected. The FC was measured using cortical oxygenated hemoglobin (HbO2) concentration via a functional near-infrared spectroscopy device, and CMC was calculated between HbO2 signals and surface electromyography signals.
Results: The Tai Chi practitioners showed greater FC in right primary motor cortex-left supplementary motor area (rM1-lSMA, p=0.006, d=1.081), right primary motor cortex-right supplementary motor area (rM1-rSMA, p=0.003, d=1.318), right primary motor cortex-left primary somatosensory cortex (rM1-lS1, p=0.002, d=1.150), and rM1-rS1 (p=0.011, d=1.015) compared with the non-exercise controls, and greater FC in rM1-rS1 (p=0.015, d=0.856) compared with the brisk walkers. In addition, the Tai Chi practitioners demonstrated greater CMC in the left tibialis anterior-right supplementary motor area (lTA-rSMA, p=0.015, d=0.991), lTA-rS1 (p=0.006, d=1.096), lMG-rSMA (p=0.002, d=1.118), right medial gastrocnemius-right supplementary motor area (rMG-rSMA, p=0.015, d=0.962), and rMG-rS1 (p=0.017, d=0.939) compared to the non-exercise controls.
Conclusion: Older Tai Chi practitioners exhibited greater functional connectivity and corticomuscular coupling, which may contribute to improved postural control and reduced fall risk in older adults.
Keywords: Tai Chi, aged, near-infrared spectroscopy, functional connectivity, corticomuscular coupling
Introduction
Older adults are at a high risk of falls, and falls often occur during locomotor activities such as walking.1 According to the World Health Organization,2 the occurrence of falls in the elderly population is an important public health problem, representing the second leading cause of unintentional injury deaths worldwide. Falls among older adults result in moderate to severe injuries, loss of independence,3 and also cause the economic burden of falls for families and society.4
Falls are generally associated with impaired postural control in older adults.5 Postural control is a complex neuromuscular process that involves integration of sensorimotor information in the central nervous system, and appropriate programming and execution of neuromuscular responses.6,7 In addition, evidence suggests that multiple cortical regions are involved in postural control,8 such as the primary motor cortex, supplementary motor area,9 and prefrontal cortex.10 Furthermore, walking engages a complex brain network, network efficiency and functional connectivity between different cortical regions are considered critical for cortical modulation.11
With aging, declines in postural control are often associated with impairments in the cortical-muscular interaction. Exercise enabled by high-tech may be effective in postponing the decline in postural control.12,13 As a traditional intervention, Tai Chi has been shown to effectively reduce falls and fall risk in older adults with the advantages of easy accessibility and wide population acceptance.14 Proprioceptive training combined with dual-task exercises may have the effect of improving gait speed, an important indicator of fall risk.15 Since Tai Chi practicing involves complex motor-cognitive integration and postural control, which is similar to proprioceptive and dual-task training, this characteristic of Tai Chi may contribute to its enhancement in cortical function and postural control in older adults, which reduces the number of falls and fall risk.16
A previous study reported that Tai Chi practitioners exhibited greater resting-state functional connectivity among the prefrontal cortex, motor cortex, and occipital cortex than the controls without Tai Chi experiences.17 However, most studies have primarily focused on individual cortical functions during resting state, with insufficient emphasis on the coordinated interactions during walking, which is essential for maintaining independence in older adults and is also when most falls occur.
Corticomuscular coupling (CMC) refers to the functional interaction between the cerebral cortex and muscles, characterized by synchronized activity between cortical and neuromuscular signals. A previous study has reported a high consistency between movement related cortical areas and thigh muscle activation during postural control in older adults.18 CMC has been shown to decline with aging, which indicates older adults have poorer neuromuscular control than young adults during voluntary motor tasks.19 To our knowledge, the effects of Tai Chi on neuromuscular control as indicated by CMC during walking in older adults have not been investigated.
The purpose of this study was to compare the differences in the functional connectivity and CMC during walking among older Tai Chi practitioners, older brisk walkers and non-exercise controls. We hypothesized that: (1) the older Tai Chi practitioners would demonstrate significantly greater functional connectivity compared to both the older brisk walkers and non-exercise controls; (2) the older Tai Chi practitioners would demonstrate significantly greater CMC compared to both the older brisk walkers and non-exercise controls.
Materials and Methods
Sample Size Calculation
As no previous study fully comparable to the target population and primary outcome was available, a post hoc power analysis was performed using the observed effect size of the primary outcome in G*Power software (Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). The significance level was to be 0.05, the effect size was calculated to be 0.45. With a sample size of 51, the statistical power was calculated to be 0.81, which was above 0.8.
Participants
A total of 62 participants were recruited by distributing leaflets in the local communities in Jinan, China. The inclusion criteria were (1) ≥ 65 years of age; (2) Without cardiovascular, respiratory, musculoskeletal or neurological diseases; (3) Able to live independently and perform daily activities. Twenty participants with more than 5 years of regular Tai Chi practice were recruited, 22 with more than 5 years of regular brisk walking, and 20 without regular exercise for more than 5 years. The exclusion criteria were (1) visual impairment; (2) Using any medication affecting physical balance or the nervous system in the last 6 months. There was no significant difference in age, sex, height, or weight among the participants (Table 1).
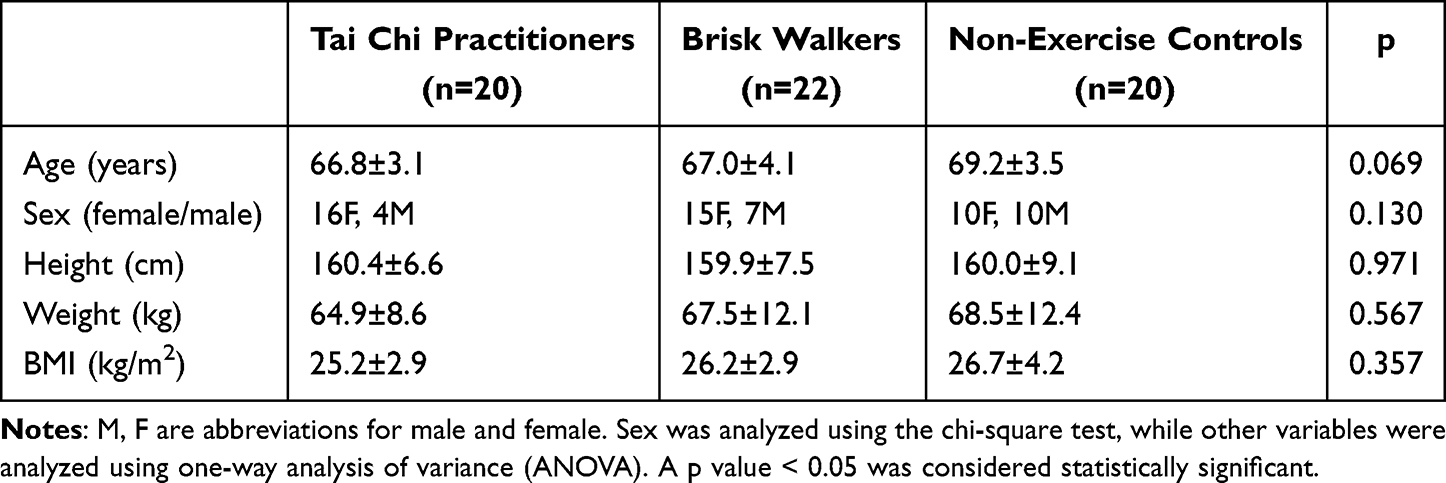 |
Table 1 Basic Information of the Participants (Mean ± Standard Deviation) |
A cross-sectional study was conducted at the Sports Biomechanics Laboratory of Shandong Sport University to investigate differences in measures among groups. The trial was registered in the International Traditional Medicine Clinical Trial Registry under the registration number ITMCTR2025002399. This study was approved by the Ethics Committee of Shandong Sport University (approval number: 2024054, November 5, 2024) and informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki.
Data Collection
fNIRS and sEMG Data Collection
Functional near-infrared spectroscopy (fNIRS) and sEMG data were obtained during walking test, which consisted of a 30-s baseline, a 60-s walking and followed by 30-s rest using an fNIRS system (NirSmartII-3000A, Danyang Huichuang Medical Equipment Co., Ltd., Danyang, Jiangsu, China) and a 16-channel EMG system (Ultium EMG, Noraxon Inc., USA). During the baseline, participants maintained quiet standing and stayed relaxed. During the walking, participants walked back and forth along the walkway at their preferred speed. During the rest, the participants were instructed to sit quietly with eyes closed. Three trials were conducted for the walking test (Figure 1). The fNIRS signals were synchronized with the sEMG data. The sEMG signals were collected from the tibialis anterior (TA), medial gastrocnemius (MG) of both legs. The arrangement of the fNIRS channels is shown in Figure 2.
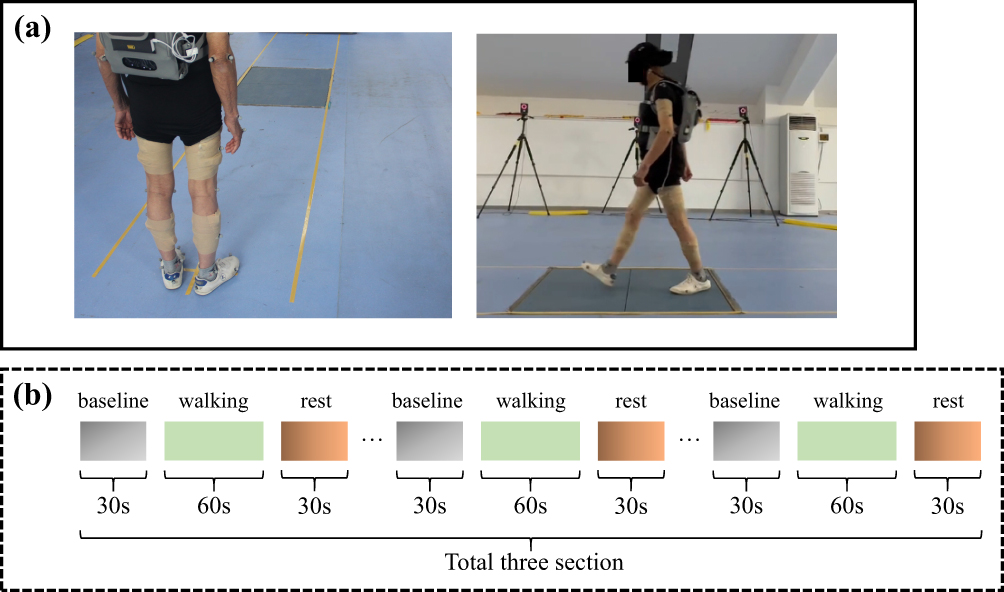 |
Figure 1 Experimental data acquisition paradigm. (a) walking test setup (b) walking test procedure. |
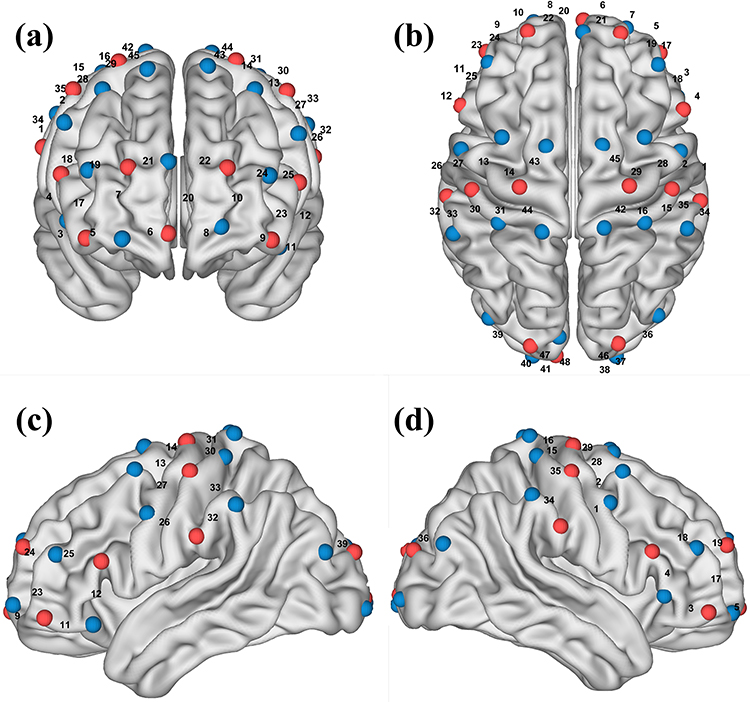 |
Figure 2 Arrangement of the fNIRS channels. The red colour represents the source probes, and the blue colour represents the detector probes. (a) Front, (b) top, (c) left‑lateral, (d) right‑lateral views of the locations of the channels in the MNI brain. |
Data Processing
fNIRS Data Processing
The fNIRS signals were sampled at 11 Hz and processed using NirSpark software20 (Danyang Huichuang Medical Equipment Co., Ltd., Danyang, Jiangsu, China). Eight regions of interest (ROIs) were defined based on the corresponding positions of the channels in the cortex. Channels 8, 9, 10, 11, 20, 22 and 23 corresponded to the left prefrontal cortex (lPFC). Channels 3, 5, 6, 7, 17, 19 and 21 corresponded to the right prefrontal cortex (rPFC). Channels 30, 31 and 44 corresponded to the left primary motor cortex (lM1). Channels 15, 16 and 42 corresponded to the right primary motor cortex (rM1). Channels 32 and 33 corresponded to the left primary somatosensory cortex (lS1). Channels 34 and 35 corresponded to the right primary somatosensory cortex (rS1). Channels 13, 14, 27 and 43 corresponded to the left supplementary motor area (lSMA). Channels 2, 28, 29 and 45 corresponded to the right supplementary motor area (rSMA). All HbO2 concentration signals from the above regions were collected.
Channels with obvious spikes in the time-domain signal and high frequency noise in the frequency-domain were excluded from further analysis. Motion correction was done in the first step, any signal change beyond 5 standard deviations (std_thr > 6) and 0.5 amplitude (amp_thr > 0.5) of the entire time series was considered a motion artifact for tighter control of data quality.21 The signals from each channel were band-pass filtered with cut-off frequencies of 0.01–0.2 Hz to remove physiological noise. The filtered raw light intensity signals were converted to HbO2 concentration data based on the modified Beer-Lambert law. After preprocessing, functional network analysis was performed, and Pearson correlation analysis was applied to calculate correlation coefficients over a 5-min time window (from the first walking to the last sitting) between each pair of channels and ROIs.22 Fisher’s transformation was used to convert the r values into z values, which exhibit better normality for statistical analysis. The resulting z values were used for statistical analysis.
Corticomuscular Coupling Analysis
CMC analysis was performed using Python (Spyder IDE, Anaconda distribution). Before CMC analysis, the sEMG signals were sampled at 2000 Hz and band-pass filtered using a fourth-order Butterworth filter with cut-off frequencies of 20–450 Hz, followed by a 50 Hz notch filter. Subsequently, the filtered fNIRS data from the three walking trials were extracted for CMC calculation with the sEMG data. For segmented data, we mainly focused on the sEMG and fNIRS data for the first 15 seconds of each walking test.23
Time-series causality analysis using transfer entropy (TE) was applied for CMC calculation, allowing the assessment of connectivity strength between physiological signals in various states and providing an objective characterization of information flow direction.24 If given two-time series  and
and  , where N is the length of the time series, the TE from
, where N is the length of the time series, the TE from  to
to  is defined as
is defined as  , the equation is calculated as follows:
, the equation is calculated as follows:

Where  is any point in time (1 ≤ t ≤ N); p represents the probability distribution. In general, the most natural choice for l = k = 1 is computational. At the same time, because TE is inherently asymmetric,
is any point in time (1 ≤ t ≤ N); p represents the probability distribution. In general, the most natural choice for l = k = 1 is computational. At the same time, because TE is inherently asymmetric,  does not equal
does not equal  . Thus, when
. Thus, when  , we call
, we call  cause and
cause and  effect, and thus establish a causal relationship between the two signals.
effect, and thus establish a causal relationship between the two signals.
Considering the hysteresis of physiological signal interaction, the time parameter  can be introduced into the formula of TE. Therefore, the TE from
can be introduced into the formula of TE. Therefore, the TE from  to can be written as:25
to can be written as:25

The resulting TE can measure transmitted information to detect asymmetries in subsystem coupling and measure hysteresis in physiological signal interactions. To distinguish functional connections in muscle and cortex, TE values in the cortico-muscular and muscle-cortical directions were calculated with u from 1 to 50.
Statistical Analysis
Means and standard deviations were calculated for each measure. The normal distribution of data was evaluated with the Shapiro–Wilk test. The one-way ANOVA was used for comparison on measures with normal distribution. The Kruskal–Wallis test for comparison on measures with abnormal distribution. The Bonferroni method was used for post-hoc tests, with the significance level adjusted to 0.017 (p = 0.05/3).
The effect sizes were expressed with Eta squared (η2), η2 < 0.06: small effect size, 0.06 < η2 < 0.14: medium effect size, η2 > 0.14: strong effect size.26 Cohen’s d was used to report effect sizes in post-hoc tests, with the following thresholds: 0.2 to 0.5 indicates a small effect; 0.5 to 0.8 represents a medium effect; and > 0.8 denotes a large effect.27
Results
Functional Connectivity
One-way ANOVA revealed significant differences in the FC of rM1-lSMA (p=0.008, η2=0.153), rM1-rSMA (p=0.004, η2=0.175), rM1-lS1 (p=0.003, η2=0.181), and rM1-rS1 (p=0.005, η2=0.171) among the three groups. Post-hoc analyses using the Bonferroni method indicated that the older Tai Chi practitioners exhibited significantly greater FC than the non-exercise controls in the rM1-lSMA (p=0.006, d=1.081), rM1-rSMA (p=0.003, d=1.318), rM1-lS1 (p=0.002, d=1.150), and rM1-rS1 (p=0.011, d=1.015); the older Tai Chi practitioners had significantly greater FC than the older brisk walkers in rM1-rS1 (p=0.015, d=0.856) (Figure 3).
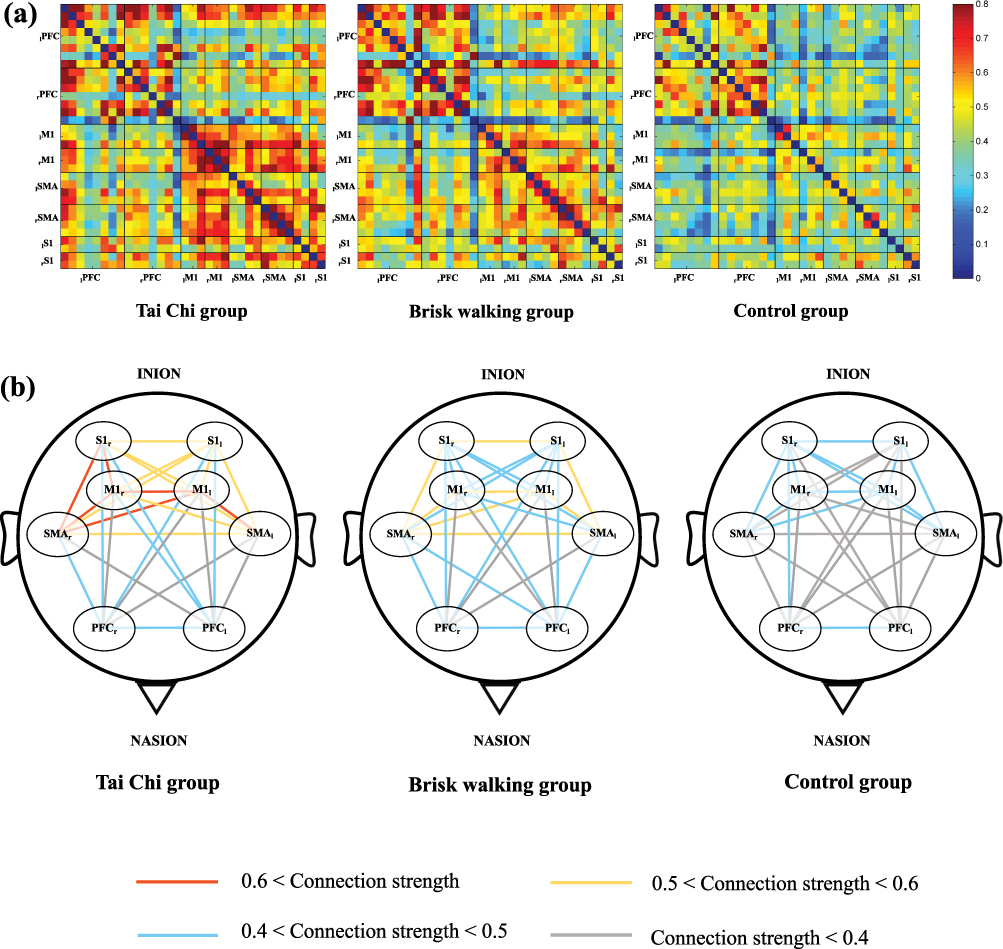 |
Figure 3 (a) Functional connectivity matrices among channels, channels were arranged according to their corresponding cortical regions. The vertical axis (top to bottom) and horizontal axis (left to right) represent the following regions: left prefrontal cortex (lPFC), right prefrontal cortex (rPFC), left primary motor cortex (lM1), right primary motor cortex (rM1), left supplementary motor area (lSMA), right supplementary motor area (rSMA), left primary somatosensory cortex (lS1), and right primary somatosensory cortex (rS1). (b) The intensity of functional connectivity among ROIs, line color indicates the connectivity intensity between two ROIs. |
Corticomuscular Coupling
One-way ANOVA revealed significant differences in the TE between lTA-rSMA (p=0.003, η2=0.194), lTA-rS1 (p=0.006, η2=0.165), lMG-rSMA (p=0.002, η2=0.199), rMG-rSMA (p=0.004, η2=0.173), rMG-rS1 (p=0.020, η2=0.126). Post-hoc analyses using the Bonferroni method indicated that the older Tai Chi practitioners had significantly greater TE in lTA-rSMA (p=0.015, d=0.991), lTA-rS1 (p=0.006, d=1.096), lMG-rSMA (p=0.002, d=1.118), rMG-rSMA (p=0.015, d=0.962), and rMG-rS1 (p=0.017, d=0.939) compared to the non-exercise controls; the older brisk walkers had significantly greater TE in lTA-rSMA (p=0.003, d=1.068), lMG-rSMA (p=0.016, d=0.953), and rMG-rSMA (p=0.009, d=0.940) compared to the non-exercise controls (Figure 4).
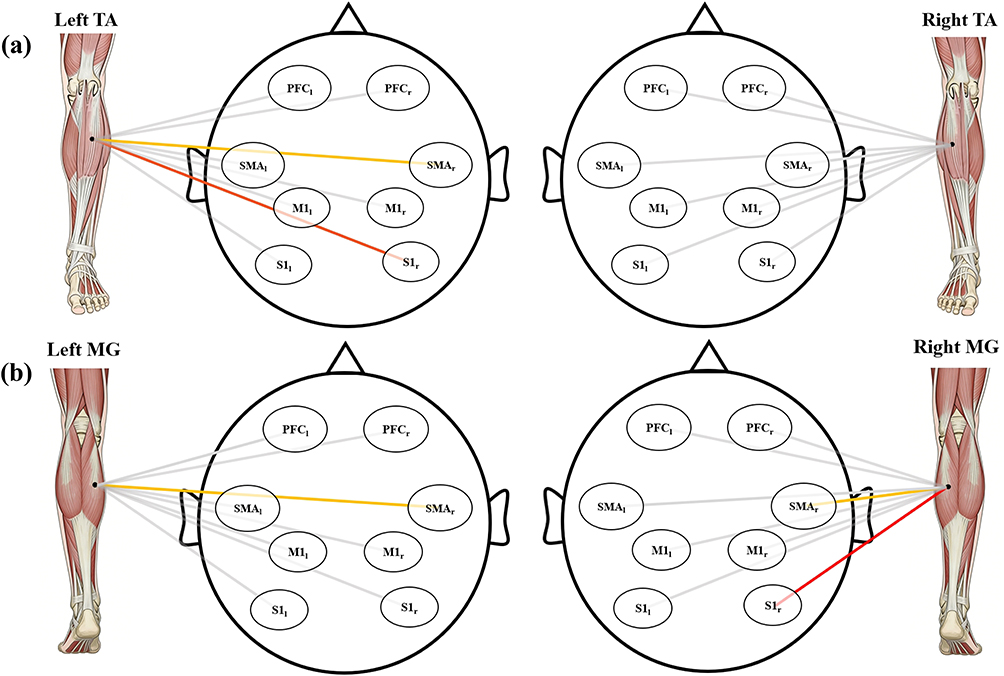 |
Figure 4 Differences in transfer entropy (TE) among the older Tai Chi practitioners, older brisk walkers, and non-exercise controls. (a) Tibialis anterior (TA), (b) medial gastrocnemius (MG). Red lines indicate significantly greater TE in the Tai Chi practitioners than in the non-exercise controls, yellow lines indicate significantly greater TE in the older Tai Chi practitioners and brisk walkers than in the non-exercise controls. The regions of interest are: left prefrontal cortex (PFCl), right prefrontal cortex (PFCr), primary motor cortex (M1), supplementary motor area (SMA), and primary somatosensory cortex (S1). |
Discussion
This study compared the differences in the FC and CMC during walking among older Tai Chi practitioners, older brisk walkers and non-exercise controls. Our results partially support the hypothesis that the older Tai Chi practitioners have greater FC and CMC than the older brisk walkers and non-exercise controls.
Our results indicated that older Tai Chi practitioners exhibited greater functional connectivity than older adults with no exercise habits. According to the hypothesis proposed by Daselaar et al,28 aging brains exhibit “more firing, less wiring.” Due to limited neural resource capacity, older adults appear to recruit neural resources from various ROIs and rely on increased local cortical activation to compensate for age-related declines and maintain task performance.11,29 Compared with non-exercise controls, older Tai Chi practitioners exhibited greater functional connectivity and lower local cortical activation during walking,30 which may reflect a more distributed neural resource recruitment across multiple brain regions.
A possible explanation for our results is that during Tai Chi exercise, spatial orientations and movement directions are often inconsistent, so people need to deal with the conflicting information so as to select the correct action.31 This process includes both cognitive and motor control functions and involves multiple brain regions. Another possible explanation is that Tai Chi exercise emphasizes precise control of body and limb joint positions, and repeated practice may lead to plastic changes in the cortex,32 such as structural changes in the organization and number of connections among neurons.33
Notably, older Tai Chi practitioners exhibited significantly greater FC in the rM1-rS1 than both older adults with no exercise habits and older adults with brisk walking habits. The S1 is responsible for processing various peripheral sensory information from the body,34 among which proprioception plays a critical role in maintaining postural stability, particularly in older adults. A previous study demonstrated that Tai Chi training resulted in better improvements in ankle proprioception compared with brisk walking, and the training effects were maintained after an eight-week detraining period.35 The greater rM1-rS1 functional connectivity observed in older Tai Chi practitioners may reflect more efficient coordination between cortical motor control and peripheral sensory input. Specifically, enhanced proprioceptive input and stronger sensorimotor network connectivity may enable Tai Chi practitioners to achieve superior postural stability and refined motor control during walking, thereby contributing to improved postural control.
The CMC analysis revealed that TE in the cortico-muscular direction was greater than in the muscle-cortical direction (Supplementary Table 1), indicating predominant cortical control over muscle activity. Furthermore, older Tai Chi practitioners exhibited greater TE values in the TA and MG than non-exercise controls, indicating greater neuromuscular information transmission between the cerebral cortex and distal lower-limb muscles. These findings are consistent with previous reports showing greater β-band CMC in older Tai Chi practitioners than in older adults during ankle dorsal flexion and plantar flexion under balance-demanding conditions,36 suggesting that Tai Chi training enhances sensorimotor integration for distal lower-limb muscles. Increased CMC was also found to correlate with decreased medial/lateral postural sway in older adults, suggesting that greater CMC may contribute to improved postural control. Tai Chi has the potential to become a clinically effective intervention for fall prevention and balance enhancement, particularly among older adults. As Tai Chi has effects on improving neuromuscular control, it may be used as a new intervention for neuromuscular control impairments.
This study has some limitations. We only analyzed overground walking rather than more complex conditions (eg., dual-task walking), as it represents a fundamental daily activity in older adults. Although more complex tasks may provide additional insights, this is unlikely to affect the validity of the present findings. Although Tai Chi has demonstrated benefits in cognitive and physical performance, the underlying neurophysiological mechanisms remain unclear. More research is necessary to investigate the long-term changes associated with Tai Chi exercise.
Conclusions
Older Tai Chi practitioners exhibited greater cortical functional connectivity and corticomuscular coupling. These findings suggest that Tai Chi exercise may enhance cortico-muscular information transmission, which may contribute to improved postural control and reduced fall risk in older adults. Further research is needed to clarify the neurophysiological mechanisms underlying these adaptations.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The trial was registered in the International Traditional Medicine Clinical Trial Registry under the registration number ITMCTR2025002399. This study was approved by the Ethics Committee of Shandong Sport University (approval number: 2024054, November 5, 2024) and informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Written informed consent for publication of the image was obtained from the participant.
Acknowledgments
The corresponding author affirms that all individuals who contributed significantly to this work have been appropriately listed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper was supported by the Natural Science Foundation of Shandong Province, China [grant number ZR2023QH433], and the Humanities and Social Sciences Fund of Ministry of Education of China [grant number 25YJCZH185].
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. New Engl J Med. 1988;319(26):1701–10. doi:10.1056/NEJM198812293192604
2. World Health Organization. Falls [fact sheet on the Internet]. Geneva: World Health Organization; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/falls.
3. Biswas I, Adebusoye B, Chattopadhyay K. Risk factors for falls among older adults in India: a systematic review and meta-analysis. Health Sci Rep. 2022;5(4):e637. doi:10.1002/hsr2.637
4. Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C. Medical costs of fatal and nonfatal falls in older adults. J Am Geriatr Soc. 2018;66(4):693–698. doi:10.1111/jgs.15304
5. Dominguez L. Postural control and perturbation response in aging populations: fall risk implications. J Neurophysiol. 2020;124(5):1309–1311. doi:10.1152/jn.00767.2019
6. Scott SH. Optimal feedback control and the neural basis of volitional motor control. Nat Rev Neurosci. 2004;5(7):532–546. doi:10.1038/nrn1427
7. Jeon SY, Han SJ, Jeong JH, Fregni F. Effect of exercise on balance in persons with mild cognitive impairment. NeuroRehabilitation. 2014;35(2):271–278. doi:10.3233/NRE-141120
8. Bolton DA. The role of the cerebral cortex in postural responses to externally induced perturbations. Neurosci Biobehav Rev. 2015;57:142–155. doi:10.1016/j.neubiorev.2015.08.014
9. Herold F, Wiegel P, Scholkmann F, Thiers A, Hamacher D, Schega L. Functional near-infrared spectroscopy in movement science: a systematic review on cortical activity in postural and walking tasks. Neurophotonics. 2017;4(4):041403. doi:10.1117/1.NPh.4.4.041403
10. Holtzer R, Epstein N, Mahoney JR, Izzetoglu M, Blumen HM. Neuroimaging of mobility in aging: a targeted review. J Gerontol a Biol Sci Med Sci. 2014;69(11):1375–1388. doi:10.1093/gerona/glu052
11. Dong Y, Yang C, Chen Y, Pan F, Wang J, Zhang C. How aging impacts cortical dynamics and gait during dual-task turning revealed by fNIRS. GeroScience. 2026;48(1):985–1007. doi:10.1007/s11357-025-01687-6
12. Adliah F, Hall AJ, Goodwin V, Lamb S. Effects of exercise programmes delivered using video technology on physical performance and falls in people aged 60 years and over living in the community: a systematic review and meta-analysis. BMJ open. 2025;15(4):e092775. doi:10.1136/bmjopen-2024-092775
13. Giovannini S, Iacovelli C, Brau F, et al. RObotic-Assisted Rehabilitation for balance and gait in Stroke patients (ROAR-S): study protocol for a preliminary randomized controlled trial. Trials. 2022;23(1):872. doi:10.1186/s13063-022-06812-w
14. Li F, Harmer P, Fisher KJ, et al. Tai Chi and fall reductions in older adults: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. 2005;60(2):187–194. doi:10.1093/gerona/60.2.187
15. Vecchio M, Chiaramonte R, De Sire A, et al. Do proprioceptive training strategies with dual-task exercises positively influence gait parameters in chronic stroke? J Rehabilit Med. 2024;56:jrm18396. doi:10.2340/jrm.v56.18396
16. Leung LYL, Tam HL, Ho JKM. Effectiveness of Tai Chi on older adults: a systematic review of systematic reviews with re-meta-analysis. Arch Gerontol Geriatrics. 2022;103:104796. doi:10.1016/j.archger.2022.104796
17. Chen W, Zhang X, Xie H, He Q, Shi Z. Brain functional connectivity in middle-aged Hong Chuan Tai Chi players in resting state. Int J Environ Res Public Health. 2022;19(19). doi:10.3390/ijerph191912232
18. Ozdemir RA, Contreras-Vidal JL, Paloski WH. Cortical control of upright stance in elderly. Mech Age Develop. 2018;169:19–31. doi:10.1016/j.mad.2017.12.004
19. Bayram MB, Siemionow V, Yue GH. Weakening of corticomuscular signal coupling during voluntary motor action in aging. J Gerontol A Biol Sci Med Sci. 2015;70(8):1037–1043. doi:10.1093/gerona/glv014
20. Yao L, Sun G, Wang J, Hai Y. Effects of Baduanjin imagery and exercise on cognitive function in the elderly: a functional near-infrared spectroscopy study. Front Public Health. 2022;10:968642. doi:10.3389/fpubh.2022.968642
21. Wu YJ, Hou X, Peng C, et al. Rapid learning of a phonemic discrimination in the first hours of life. Nat Human Behav. 2022;6(8):1169–1179. doi:10.1038/s41562-022-01355-1
22. Yang Z, Ye L, Yang L, Lu Q, Yu A, Bai D. Early screening of post-stroke fall risk: a simultaneous multimodal fNIRs-EMG study. CNS Neurosci Ther. 2024;30(9):e70041. doi:10.1111/cns.70041
23. Diao Y, Chen G, Sun Y, et al. Cortico-muscular Information Transfer Based on fNIRS and sEMG During Gait Walking in the Elderly and Young Adults.
24. Wang Y, Chen W. Effective brain connectivity for fNIRS data analysis based on multi-delays symbolic phase transfer entropy. J Neural Engineer. 2020;17(5):056024. doi:10.1088/1741-2552/abb4a4
25. Faes L, Marinazzo D, Montalto A, Nollo G. Lag-specific transfer entropy as a tool to assess cardiovascular and cardiorespiratory information transfer. IEEE Transact Bio Med Engineer. 2014;61(10):2556–2568. doi:10.1109/TBME.2014.2323131
26. Xu G, Zhou M, Chen Y, Song Q, Sun W, Wang J. Brain activation during standing balance control in dual-task paradigm and its correlation among older adults with mild cognitive impairment: a fNIRS study. BMC Geriatr. 2024;24(1):144. doi:10.1186/s12877-024-04772-1
27. Panjeh S, Nordahl-Hansen A, Cogo-Moreira H. Establishing new cutoffs for Cohen’s d: an application using known effect sizes from trials for improving sleep quality on composite mental health. Internat J Method Psych Res. 2023;32(3):e1969. doi:10.1002/mpr.1969
28. Daselaar SM, Iyengar V, Davis SW, Eklund K, Hayes SM, Cabeza RE. Less wiring, more firing: low-performing older adults compensate for impaired white matter with greater neural activity. Cerebral Cortex. 2015;25(4):983–990. doi:10.1093/cercor/bht289
29. Lin CC, Bair WN, Willson J. Age differences in brain activity in dorsolateral prefrontal cortex and supplementary motor areas during three different walking speed tasks. Human Move Sci. 2022;85:102982. doi:10.1016/j.humov.2022.102982
30. Nóbrega-Sousa P, Gobbi LTB, Orcioli-Silva D, Conceição NRD, Beretta VS, Vitório R. Prefrontal cortex activity during walking: effects of aging and associations with gait and executive function. Neurorehabil Neural Repair. 2020;34(10):915–924. doi:10.1177/1545968320953824
31. Yang Y, Chen T, Shao M, Yan S, Yue GH, Jiang C. Effects of Tai Chi Chuan on inhibitory control in elderly women: an fNIRS study. Front Human Neurosci. 2019;13:476. doi:10.3389/fnhum.2019.00476
32. Tsang WW, Hui-Chan CW. Effects of tai chi on joint proprioception and stability limits in elderly subjects. Med Sci Sports Exercise. 2003;35(12):1962–1971. doi:10.1249/01.MSS.0000099110.17311.A2
33. Shumway-Cook A, Woollacott M. Motor Control: Theory and Practical Applications. Baltimore: Williams & Wilkins; 2001.
34. Huang Y, Zhang X, Li W. Involvement of primary somatosensory cortex in motor learning and task execution. Neurosci Lett. 2024;828:137753. doi:10.1016/j.neulet.2024.137753
35. Zhang C, Sun W, Yu B, Song Q, Mao D. Effects of exercise on ankle proprioception in adult women during 16 weeks of training and eight weeks of detraining. Res Sports Med. 2015;23(1):102–113. doi:10.1080/15438627.2014.915835
36. Hu Y, Hsiao-Wecksler ET, Hernandez ME. Exploration of the effects of Tai Chi practice on lower limb corticomuscular coherence during balance-demanding virtual reality conditions in older adults. Front Aging Neurosci. 2025;17:1554000. doi:10.3389/fnagi.2025.1554000
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.