")
Back to Journals » Patient Preference and Adherence » Volume 17
Long-Term Safety, Efficacy, and Patient-Centered Outcomes of Filgotinib in the Treatment of Rheumatoid Arthritis: Current Perspectives
Authors Tanaka Y , Genovese MC, Matsushima H
Received 21 April 2023
Accepted for publication 1 August 2023
Published 6 October 2023 Volume 2023:17 Pages 2499—2516
DOI https://doi.org/10.2147/PPA.S417677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Yoshiya Tanaka,1 Mark C Genovese,2,3 Hironori Matsushima4
1The First Department of Internal Medicine, School of Medicine, University of Occupational and Environmental Health Japan, Kitakyushu, Japan; 2Division of Immunology and Rheumatology, Stanford University, Stanford, CA, USA; 3Gilead Sciences, Inc, Foster City, CA, USA; 4Gilead Sciences, Inc, Tokyo, Japan
Correspondence: Yoshiya Tanaka, The First Department of Internal Medicine, School of Medicine, University of Occupational and Environmental Health Japan, 1-1 Iseigaoka, Yahata-nishi, Kitakyushu, 807-8555, Japan, Tel +81-93-603-1611, Fax +81-93-691-7580, Email [email protected]
Abstract: Filgotinib is an orally administered, preferential Janus kinase (JAK) inhibitor indicated for the treatment of moderate-to-severe rheumatoid arthritis (RA). The short-term safety, efficacy, and patient-reported outcomes (PROs) with filgotinib from Phase 2b/3 clinical trials (DARWIN 1 and 2; FINCH 1, 2, and 3) are described in patients who inadequately responded to methotrexate (MTX) and biologic disease-modifying antirheumatic drugs or who were naïve to MTX. This article reviews the safety and efficacy from the long-term extension (LTE) trials, DARWIN 3 (N=739) and FINCH 4 (N=2731), and PROs across the filgotinib development program in RA. Overall, in the DARWIN clinical trials (conducted from 2013– 2023), patients received their LTE treatment for ≤ 8 years, while in the FINCH trials (ongoing from 2016– 2025), patients received filgotinib treatment for ≤ 6 years in the LTE. The longer-term safety profile and consistent, sustained efficacy (American College of Rheumatology 20/50/70, Clinical Disease Activity Index, and Disease Activity Scale in 28 joints with C-reactive protein response rates) of filgotinib were largely similar to those observed in the shorter-term parent trials ≤ 52 weeks. PRO results from the parent trials showed improvements in patients’ quality of life with filgotinib treatment, which compared to or exceeded improvements seen with placebo and active comparators (adalimumab, MTX). Filgotinib has a higher specificity for JAK1 compared with other therapeutic treatments, leading to reduced inhibition of JAK2/3–dependent pathways, potentially providing a distinct safety profile. Filgotinib is approved in Europe and Japan for treatment of people with moderate-to-severe RA, though it has not been approved by the US Food and Drug Administration, due to concerns around the benefit/risk profile of the filgotinib 200-mg dosage and the potential impact on semen parameters.
Keywords: Janus kinase inhibitors, selectivity, JAKi, disease-modifying antirheumatic drug, DMARD, RA
Introduction
Approximately 0.5% of the world’s population has rheumatoid arthritis (RA).1,2 RA is a chronic, systemic, autoimmune, and inflammatory disease characterized by tender, swollen, and stiff joints; high morbidity and mortality; and progressive disability.3–5 While the full spectrum of signaling pathways involved in the pathogenesis of RA remains unclear, abnormalities in cytokines involved in immune and inflammation responses, including interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor-alpha, are implicated in the progression of RA and are targets of disease-modifying antirheumatic drugs (DMARDs).5–10 Janus kinase (JAK) inhibitors (JAKis)—the first class of targeted synthetic DMARDs to gain marketing authorizations—work by blocking JAK-dependent cytokine signaling pathways, interfering with inflammatory responses and subsequently disrupting the pathogenesis of RA.4,5,7,10,11 Filgotinib, an orally administered medication, has been extensively studied for the treatment of moderate-to-severe RA in a series of Phase 2b and 3 clinical trials: DARWIN 1, 2, and 3 and FINCH 1, 2, 3, and 4.12–22 The Phase 2b DARWIN trials were filgotinib dose-finding studies, while the Phase 3 FINCH trials assessed the safety and efficacy of the treatment modality.23–29 The DARWIN and FINCH trials both required an RA diagnosis defined by the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) criteria for RA and an ACR functional class I–III.23–29 These trials included RA patients who had inadequate response (IR) to other treatments, including methotrexate (MTX) and biologic DMARDs (bDMARDs), and those who were naïve to MTX treatment.12–21 Based on the evidence generated by these trials, filgotinib is approved for the treatment of moderately to severely active RA in the European Union, the United Kingdom, and Japan.30–32 This review describes the safety, efficacy, tolerability, and patient-reported outcomes (PROs) of filgotinib treatment in patients with RA.
Filgotinib + MTX (DARWIN 1; NCT01888874) and filgotinib monotherapy (DARWIN 2; NCT01894516) were evaluated in patients with active RA and IR to previous MTX treatment.15,18 Patients meeting key inclusion criteria for DARWIN 1 were ≥18 years of age, had a diagnosis of RA ≥6 months and met the 2010 ACR/EULAR criteria of RA and ACR function class I–III, had ≥6 swollen joints from a 66-joint count and ≥8 tender joints from a 68-joint count at screening and at baseline, had a screening serum C-reactive protein (CRP) ≥0.7 × upper limit of laboratory normal range, and had received MTX for ≥6 months and were on a stable dose of MTX for ≥4 weeks prior to screening and were willing to continue their current treatment regimen for the duration of the study.18,26 Inclusion criteria for DARWIN 2 were the same as DARWIN 1 with the exception that patients were required to have an IR in terms of either lack of efficacy or toxicity to MTX and were required to have an MTX washout period of ≥4 weeks before or during the screening period.15,25 DARWIN 3 (NCT02065700), an open-label extension study, evaluated the long-term safety and efficacy of filgotinib (200 mg once daily or 100 mg twice daily) in eligible patients who had completed either DARWIN 1 (filgotinib and MTX) or DARWIN 2 (filgotinib monotherapy).16 Overall, the DARWIN clinical trials were conducted internationally across 23 countries from 2013 to 2023, and patients received their long-term extension (LTE) treatment in DARWIN 3 for ≤8 years.23,25,26
FINCH 1 (NCT02889796) investigated filgotinib 200 mg or 100 mg once daily, subcutaneous adalimumab (ADA; 40 mg) every 2 weeks, or placebo all in combination with MTX in patients who were MTX-IR.12 Key inclusion criteria for FINCH 1 were patients ≥18 years of age, a diagnosis of RA based on the 2010 ACR/EULAR criteria of RA and ACR function class I–III, ≥6 swollen joints from a 66-joint count and ≥6 tender joints from a 68-joint count at screening and day 1, and ongoing treatment with a stable dose of MTX.12 FINCH 2 (NCT02873936) included adult patients with moderately to severely active RA, similar to FINCH 1; however, additional inclusion criteria were an IR to 1 or more prior bDMARDs (tumor necrosis factor inhibitor [TNFi] bDMARD exposure: ADA, etanercept, infliximab, golimumab, and certolizumab; non-TNFi bDMARD exposure: tocilizumab, abatacept, rituximab, and anakinra) and had active RA despite ongoing treatment with conventional synthetic DMARDs (csDMARDs; 1 or 2 of the following: MTX, hydroxychloroquine or chloroquine, sulfasalazine, and/or leflunomide; however, the combination of leflunomide and MTX was not allowed).14 These patients were treated with once-daily filgotinib (200 mg or 100 mg) or placebo, in combination with csDMARDs.14 Inclusion criteria for FINCH 3 (NCT02886728) were similar to FINCH 1 and 2, with the exception that FINCH 3 required that eligible patients be naïve to MTX and during the trial were treated with either filgotinib 200 mg or 100 mg daily + MTX, filgotinib 200 mg monotherapy, or MTX monotherapy.4,17,21 Patients who completed any of the FINCH parent trials were eligible to enroll in the LTE study FINCH 4 (NCT03025308).24 Patients who had been assigned to filgotinib continued their originally assigned filgotinib dosage while those who had been assigned to control groups in the parent trials were rerandomized (blinded) to filgotinib 200 or 100 mg once daily.20,21,33 Overall, the FINCH clinical trials have been conducted internationally across 34 countries beginning in 2016, with FINCH 4 currently ongoing, with projected completion in 2025.24 Patients received their LTE treatment in FINCH 4 for ≤6 years.24
Filgotinib was safe and well tolerated and showed consistent efficacy for clinical and PRO measures, with significant improvements vs controls ≤52 weeks in the DARWIN and FINCH parent trials.4,12–15,17–21 The LTE studies (DARWIN 3 and FINCH 4) are ongoing as of December 2022, with DARWIN 3 collecting data for ≤8 years and FINCH 4 for ≤6 years.23,24 This paper reviews the findings to date from DARWIN 3 and FINCH 4 regarding long-term safety, tolerability, and efficacy of filgotinib, along with adherence to treatment and PROs, among patients with RA who are MTX-IR, bDMARD-IR, or MTX-naïve. Table 1 summarizes study characteristics of the DARWIN and FINCH clinical trials; Table 2 summarizes patient demographics of the DARWIN and FINCH clinical trial populations.
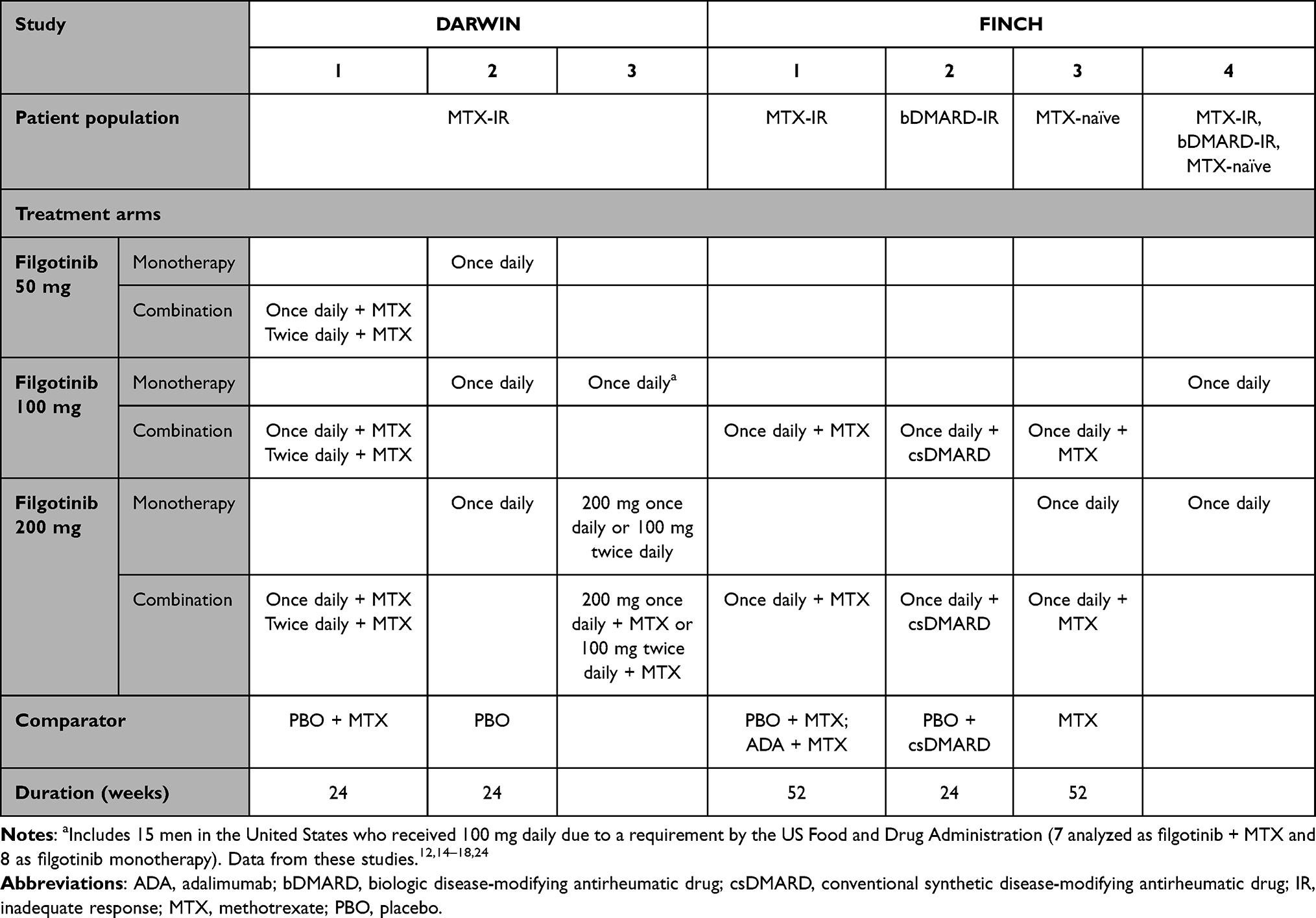 |
Table 1 Trial Characteristics of DARWIN and FINCH |
 |
Table 2 Patient Demographics in the DARWIN and FINCH Programs |
Long-Term Safety and Tolerability of Filgotinib
Filgotinib was generally well tolerated in previous clinical trials, with similar safety profiles ≤52 weeks with active comparators MTX and ADA.12–21,33–35 Safety endpoints such as adverse events (AEs), treatment-emergent AEs (TEAEs) and their exposure-adjusted incidence rates (EAIRs), infections, malignancies, major adverse cardiovascular events (MACE), venous thromboembolisms, and deaths were included for both the FINCH and DARWIN clinical trials.16,19,33–35 EAIRs, representing the number of patients with AEs of interest per patients’ total exposure time, were calculated for TEAEs.16,19,33–35 An integrated safety analysis of data from patients treated a median of 1.6 years (maximum, 5.6 years) in the DARWIN and FINCH studies and a subsequent update at 2.2 years (maximum, 6.8 years) demonstrated that the safety and tolerability of filgotinib 200 and 100 mg were similar, with a lower incidence of infections with filgotinib 200 mg among the long-term, as-treated dataset, and no new safety concerns were identified (Table 3).19,36 EAIRs of TEAEs, including deaths and AEs of special interest (AESIs), decreased or remained stable since the earlier report, while slight increases were noted in rates of nonmelanoma skin cancer (NMSC) and non-NMSC malignancies.36
 |
Table 3 Summary of Safety Results from DARWIN 1–3 and FINCH 1–4 Trials |
Filgotinib in Patients with Inadequate Responses to Methotrexate
DARWIN 3 evaluated safety and tolerability of filgotinib through ≤204 weeks among patients who had IR to MTX. Patients continuing from DARWIN 1 received 200 mg/day of filgotinib in combination with MTX, while patients continuing from DARWIN 2 received 200 mg/day of filgotinib monotherapy (Table 1).16 Overall, DARWIN 3 reported that filgotinib was well tolerated and had a similar safety profile when compared to the 2 parent trials, and the EAIRs for TEAEs were similar between patients receiving filgotinib as a monotherapy or combination therapy.15,16,18 MACE and herpes zoster (HZ) have been reported to be associated with other JAKi treatments; however, the incidence rates for these events are similar to placebo (Table 4).16,19,37–40
 |
Table 4 Safety Results Among MTX-IR Patients from DARWIN 3 |
RA patients were eligible to enroll in the LTE FINCH 4 study if they had completed 1 of the FINCH parent studies. Among patients who were MTX-IR and were rerandomized for the LTE from ADA + MTX to filgotinib + MTX or those who continued their parent-trial treatment with filgotinib 100 or 200 mg with MTX, incidence of TEAEs, serious AEs (SAEs), and ≥3-grade AEs were largely comparable (Table 5).34 Overall incidence of AEs appeared to be lowest among patients who were on ADA + MTX in the parent trial (FINCH 1) and rerandomized to 100 mg of filgotinib + MTX in the LTE (Table 5).34 AESIs occurred at similar rates between treatment groups, with the exception of a higher EAIR of HZ among patients treated with 200 mg filgotinib during the LTE compared with those treated with 100 mg filgotinib, which was also seen in DARWIN 3 (Table 5).34 Deep vein thrombosis, opportunistic infections, and NMSC occurred only in patients who started on and continued filgotinib treatment throughout the entire parent and LTE study (Table 5).34 Overall, the long-term safety of filgotinib in MTX-IR patients was largely comparable and consistent with that observed in FINCH 1, and the safety profiles established in the DARWIN and FINCH trials were similar.16,34
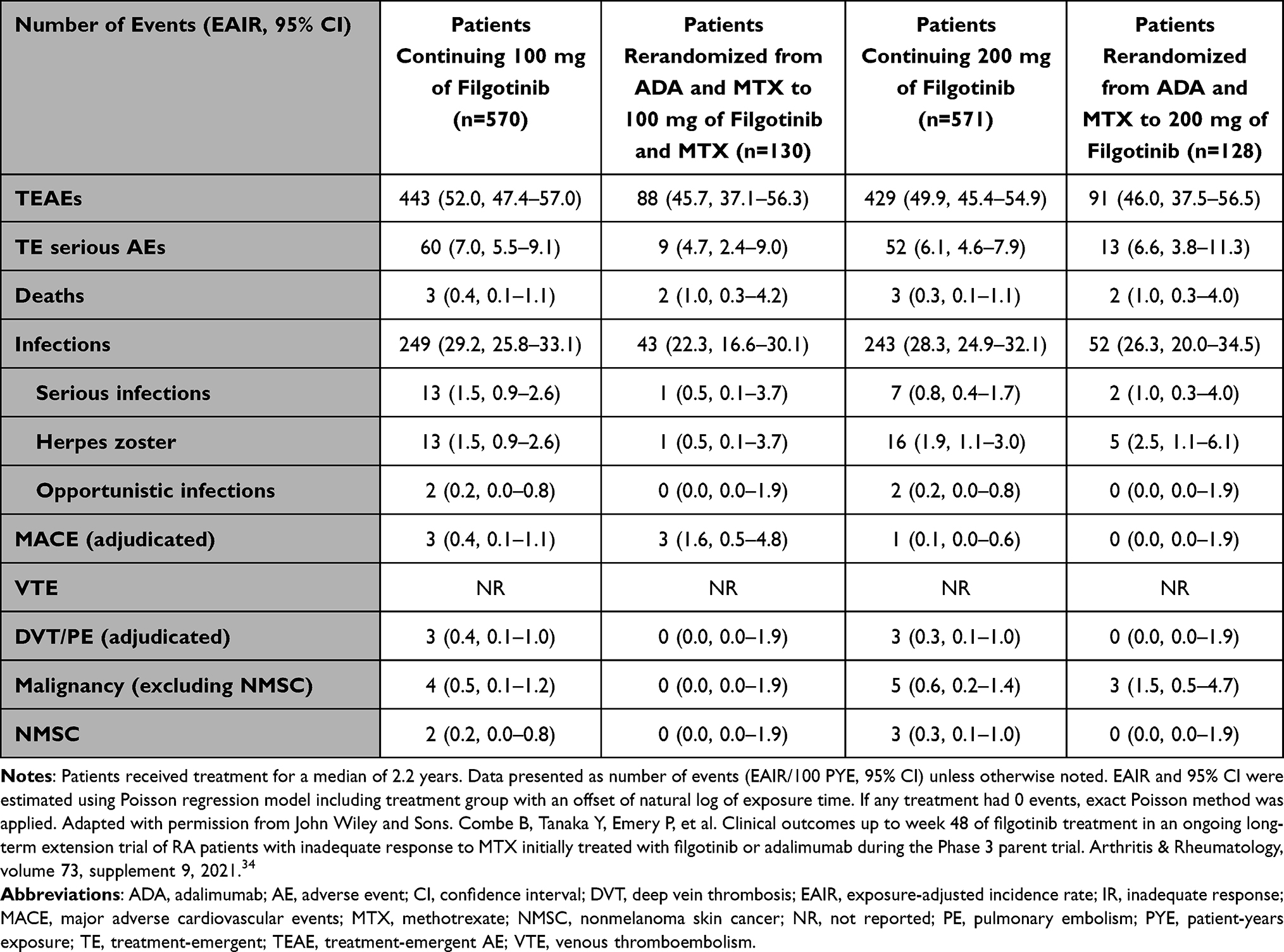 |
Table 5 Safety Results Among MTX-IR Patients from FINCH 4 |
Filgotinib in Patients with Inadequate Responses to bDMARDs
In the FINCH 2 trial, patients who had not met predefined response criteria by week 14 were switched to standard-of-care (SOC) therapy for the rest of the controlled period.14 Patients from FINCH 2 who had been assigned to a filgotinib arm remained on their blinded filgotinib dose (100 mg or 200 mg once daily) for FINCH 4, while those who had been receiving placebo or SOC treatment were rerandomized to 100 mg or 200 mg filgotinib.14,33
In FINCH 4, the safety profile of filgotinib among patients who were bDMARD-IR showed minor deviations from that of patients who were MTX-IR and MTX-naïve. The numbers of SAEs, malignancies, and infections were higher among the bDMARD-IR patient population than what was seen in the MTX-IR or MTX-naïve populations (Table 6).33–35 These differences may be due to longer disease duration, prior immunosuppressive exposures, and the smaller size of the bDMARD-IR population (n=369) compared with the MTX-IR (n=1399) and MTX-naïve (n=960) populations.33–35 EAIRs for SAEs, TEAEs, infections, and serious infection AEs were all higher among patients who had received SOC treatment in the parent trial than among those who received placebo or filgotinib during the parent trial.33 Up to week 48, five deaths were reported in the bDMARD-IR patient groups despite the smaller population size (Table 6).33 Overall, safety profiles were largely consistent between the parent trial and LTE.14,33
 |
Table 6 Safety Results Among bDMARD-IR Patients from FINCH 4 |
Filgotinib in Methotrexate-Naïve Patients
Patients naïve to MTX enrolled into FINCH 4 from the parent trial FINCH 3.17 Patients randomized to MTX in the parent trial underwent a 4-week MTX washout followed by blinded rerandomization to 100 or 200 mg filgotinib.35 The LTE safety profile of filgotinib among the MTX-naïve subpopulation was largely comparable to the parent trial and across treatment arms (Table 7).17,35,36 Six deaths and 5 MACE were reported among patients receiving filgotinib 200 mg in the parent trial and LTE, but there were no deaths or MACE among patients receiving 100 mg filgotinib or among those rerandomized from MTX to 200 mg filgotinib for the LTE (Table 7).35 Incidence of TEAEs, AEs of Grade 3 or higher, SAEs, and infections did not appear to increase among patients rerandomized from MTX to filgotinib for the LTE, while EAIRs of HZ were comparable across treatment arms among MTX-naïve patients, regardless of parent-trial treatment (Table 7).17,35 In general, the rates of AESIs among MTX-naïve patients were low; however, they tended to be higher among patients maintained on filgotinib from the parent study.35
 |
Table 7 Safety Results Among MTX-Naïve Patients from FINCH 4 |
Summary of Long-Term Safety and Tolerability of Filgotinib
The safety profile of filgotinib in RA remained broadly consistent with that of the parent trials in each of the LTE studies. RA inflammation leads to increased cardiac abnormalities and physiologic changes, such as increased arterial stiffness, changes in lipid salvage, and destabilized plaque, leading to an increased risk of cardiovascular events among patients with RA.41–49 MACE were infrequently reported in the LTE studies of filgotinib, which is of particular importance, as careful consideration of cardiovascular risk must inform medication choices for patients with RA.16,33–35,41 Most deaths in the LTE studies were due to cardiovascular events, serious infection, and malignancies.19 All fatal myocardial infarction and strokes reported in the LTE occurred in patients with ≥1 cardiovascular risk factor.19 Patients with RA treated with JAKis can be susceptible to latent viral infections, such as HZ, because JAKis block intracellular signals on the cytokine level modulating the immune response; therefore, HZ infections remain a safety risk for the long-term use of filgotinib.12–21,33–35,50 However, given that other JAKis (tofacitinib, baricitinib, and upadacitinib) are reported to be associated with an increased risk of infection, as well as of reactivation of HZ, it is likely such risk is a class effect rather than unique to filgotinib.19,51–54 A 2020 meta-analysis by Harrington et al suggested that filgotinib had the lowest incidence of HZ among the JAKis.55
Long-Term Efficacy of Filgotinib
The efficacy of filgotinib was measured using the ACR20/50/70 response rate, the Disease Activity Score in 28 joints with CRP (DAS28[CRP]) response rate, and Clinical Disease Activity Index (CDAI) across the clinical trials.12–18,20,21,33–35 The ACR20/50/70 responses are commonly used criteria for measuring response rate and are reported as at least a 20%, 50%, and 70% improvement in at least 3 of 5 ACR core set measures (patient’s pain, patient’s global assessment of disease activity, physician’s global assessment of disease activity, physical function, and highly sensitive quantification of CRP concentration).56 In patients with RA using JAKis, significant advantages for improving the quality of life, reducing inflammation, and efficacy in reducing disease activity have been shown.57 In a meta-analysis of patients treated with JAKis, ACR response rates were considerably higher, and JAKis showed a significant advantage in all disease activity parameters (DAS28[CRP], DAS28-erythrocyte sedimentation rate, simplified disease activity index, and CDAI).57 Improvements in efficacy parameters are seen likely because JAKis interfere with inflammatory responses and disrupt the pathogenesis of RA.4,5,7,10,11 These outcomes were analyzed in the parent trials using the nonresponder imputation (NRI) approach, whereas the outcomes reported from the LTEs are observed cases (OC). As such, the as-observed data from the LTEs may report values higher than that of the parent trials. Data cannot be directly compared between parent trials and LTEs, because the higher values seen in the LTE studies may overestimate the effect of filgotinib.
Filgotinib in Patients with Inadequate Responses to Methotrexate
The ACR20/50/70 responses in DARWIN 3 at week 204, based on the OC analysis, were 89.3%/69.6%/49.1% in the filgotinib + MTX group and 91.8%/69.4%/44.4% in the filgotinib monotherapy group, respectively (Figure 1).16 The observed ACR response rates in the LTE were slightly higher than those reported in the parent trials at week 24.15,18 The proportions of patients who achieved DAS28(CRP) <2.6 were sustained over time: 57.5% of the filgotinib + MTX groups and 49.6% of the filgotinib monotherapy group achieved DAS28(CRP) <2.6 at week 204 of the LTE, suggesting long-term efficacy for those remaining on filgotinib (Figure 1).16
 |
Figure 1 Efficacy results among MTX-IR patients from DARWIN 3. Abbreviations: ACR, American College of Rheumatology; DAS28(CRP), Disease Activity Score for 28 joint count using C-reactive protein; IR, inadequate response; LTE, long-term extension; MTX, methotrexate; OC, observed cases. Notes: ACR20/50/70 response rates (A–C) and DAS28(CRP) response rates (D and E) of MTX-IR patients in DARWIN 3 for the filgotinib monotherapy and filgotinib in combination with MTX treatment arms have been plotted from baseline to week 204 (week 156 of the LTE). Adapted with permission from The Journal of Rheumatology Publishing Co. Ltd. Kavanaugh A, Westhovens RR, Winthrop KL, et al. Safety and efficacy of filgotinib: up to 4-year results from an open-label extension study of Phase II rheumatoid arthritis programs. Journal of Rheumatology, volume 48, issue 8, pages 1230–1238, 2021. Permission conveyed through Copyright Clearance Center, Inc.16 |
In FINCH 4, numerically greater proportions of patients met response criteria (ACR20/50/70, DAS28[CRP], and CDAI) at week 48 of the LTE in the filgotinib 200-mg once-daily group compared with the filgotinib 100-mg group, regardless of their treatment in the parent trial, FINCH 1 (Figure 2).34 ACR20/50/70 response rates among ADA patients rerandomized to 200 mg of filgotinib were slightly higher at LTE week 48 than that achieved with ADA in the parent trial to week 52, and for those who had not achieved CDAI remission at LTE baseline, 22% and 18% were able to achieve such remission with filgotinib 200 or 100 mg, respectively.12,34 Broadly speaking, the proportions of patients achieving ACR20/50/70, DAS28(CRP) ≤3.2 and <2.6, and CDAI ≤10 and ≤2.8 were maintained in all treatment arms up to week 48 of the FINCH 4 LTE, suggesting maintenance of long-term efficacy.4,34
 |
Figure 2 Efficacy results among MTX-IR patients from FINCH 4. Abbreviations: ACR, American College of Rheumatology; ADA, adalimumab; CDAI, Clinical Disease Activity Index; DAS28(CRP), Disease Activity Score for 28 joint count using C-reactive protein; FIL, filgotinib; IR, inadequate response; LTE, long-term extension; MTX, methotrexate. Notes: ACR20/50/70 response rates (A–C), DAS28(CRP) response rates (D and E), and CDAI response rates (F and G) of MTX-IR patients in FINCH 4 for the 4 different treatment arms have been plotted from baseline to week 48 of the LTE (FINCH 4). ACR20 is calculated based on parent study baseline. Analyzed using the logistic regression model including treatment group and stratification factors; no formal comparison of efficacy outcomes was performed. DAS28(CRP) <2.6 or CDAI ≤2.8 signify remission and DAS28(CRP) ≤3.2 or CDAI ≤10 signify low disease activity. Data from Combe et al.34 |
Filgotinib in Patients with Inadequate Responses to bDMARDs
In general, the ACR20/50/70 response rates in bDMARD-IR patients were similar between week 24 of the FINCH 2 parent trial and week 48 of the LTE.14,33 The proportions of DAS28(CRP) responders were maintained among patients continuing filgotinib treatment from the parent trial into the LTE and increased among patients who were rerandomized from placebo or SOC in the parent trial to filgotinib treatment up to week 48 of the LTE (Figure 3).33 However, despite increasing efficacy among patients who had been on SOC in the parent trial, the proportion who achieved DAS28(CRP) response at LTE week 48 was lower than among other groups, potentially revealing a difficult-to-treat population.33 The total number of such patients included in FINCH 4 was low (n=45).33 Further research into this specific subpopulation of patients is warranted, as they may respond differently to therapeutic treatment.
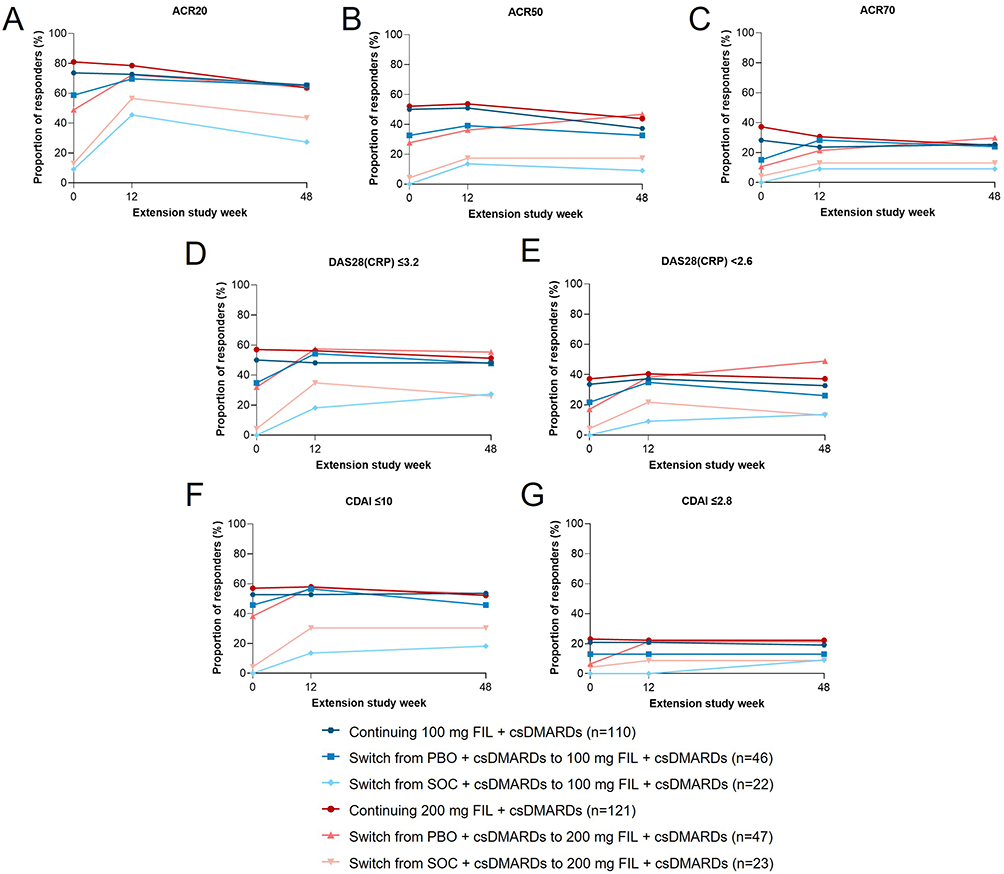 |
Figure 3 Efficacy results among bDMARD-IR patients from FINCH 4. Abbreviations: ACR, American College of Rheumatology; bDMARD, biologic disease-modifying antirheumatic drug; CDAI, Clinical Disease Activity Index; csDMARD, conventional synthetic disease-modifying antirheumatic drug; DAS28(CRP), Disease Activity Score for 28 joint count using C-reactive protein; FIL, filgotinib; IR, inadequate response; LTE, long-term extension; PBO, placebo; SOC, standard-of-care. Notes: ACR20/50/70 response rates (A–C), DAS28(CRP) response rates (D and E), and CDAI response rates (F and G) of bDMARD-IR patients in FINCH 4 for the 4 different treatment arms have been plotted from baseline to week 48 of the LTE (FINCH 4). DAS28(CRP) <2.6 or CDAI ≤2.8 signify remission and DAS28(CRP) ≤3.2 or CDAI ≤10 signify low disease activity. Data from Buch et al.33 |
Filgotinib in Methotrexate-Naïve Patients
Overall, response rates (ACR20/50/70, DAS28[CRP], and CDAI) from LTE baseline slightly decreased to week 12 and then stabilized to week 48 among MTX-naïve patients treated with filgotinib in the FINCH 3 parent trial (Figure 4).35 Patients who were rerandomized from MTX monotherapy (FINCH 3) to filgotinib (FINCH 4) showed increased response rates during the LTE. Further, independent of initial treatment group in the parent study, the response rates at LTE week 48 were comparable across groups.35
 |
Figure 4 Efficacy results among MTX-naïve patients from FINCH 4. Abbreviations: ACR, American College of Rheumatology; CDAI, Clinical Disease Activity Index; DAS28(CRP), Disease Activity Score for 28 joint count using C-reactive protein; FIL, filgotinib; LTE, long-term extension; mono, monotherapy; MTX, methotrexate. Notes: ACR20/50/70 response rates (A–C), DAS28(CRP) response rates (D and E), and CDAI response rates (F and G) of MTX-naïve patients in FINCH 4 for the 4 different treatment arms have been plotted from baseline to week 48 of the LTE (FINCH 4). DAS28(CRP) <2.6 or CDAI ≤2.8 signify remission and DAS28(CRP) ≤3.2 or CDAI ≤10 signify low disease activity. Data from Aletaha et al.58 |
Summary of Long-Term Efficacy of Filgotinib
In summary, filgotinib efficacy was mostly maintained across MTX-IR, MTX-naïve, and bDMARD-IR patient groups in the longer term for those who remained on treatment.16,20,33–35 Improvements in the efficacy outcomes measured during the LTE trials were comparable to those in the parent trials.12–18,20,21,33–35 However, the response rates among bDMARD-IR patients were lower relative to those observed among the MTX-IR and MTX-naïve populations.14,16,20,33–35
Persistence and Patient-Reported Outcomes with Filgotinib
Patient completion of the FINCH parent trials was similar and independent of patient characteristics.59 Completion rates were 82.1%, 86.4%, 85.0% among MTX-naïve, MTX-IR, and bDMARD-IR patients, respectively.59 Of the patients followed into the LTE from the MTX-IR parent study, 91% of patients who continued 200 mg filgotinib, 88% of those who continued 100 mg filgotinib, 92% of those rerandomized from ADA to 200 mg filgotinib, and 89% of those randomized from ADA to 100 mg filgotinib were still on study drug as of June 2020.34 Of patients who entered the LTE from the MTX-naïve parent study, 89% from the filgotinib 200-mg groups and 85% from the filgotinib 100-mg groups were still on study treatment, as were 89% of those rerandomized from MTX to filgotinib 200 mg and 88% of those rerandomized to filgotinib 100 mg.35 Lastly, of the bDMARD-IR patients who entered the LTE, 66% of those receiving 200 mg filgotinib and 69% of those receiving 100 mg filgotinib were still on study treatment as of June 2020.33 Patients still on LTE filgotinib from placebo were 75% for 200 mg filgotinib and 70% for 100 mg filgotinib, while those patients among the SOC group were 57% for 200 mg filgotinib and 59% for 100 mg filgotinib.33 The proportion of patients continuing filgotinib in the bDMARD-IR subpopulation was lower than the proportions of the MTX-IR and MTX-naïve populations.33–35 Given that the bDMARD-IR patients experienced more SAEs and infections, as well as had lower efficacy rates than patients with other treatment backgrounds, this may have contributed to lower treatment persistence over the long term.33–35
The DARWIN 3 LTE included 93.5% of patients who completed the parent trials.16 However, the proportion of patients in DARWIN 3 remaining on the study treatment at week 204 was lower (54.3%) than the completion rate of the parent trials.15,16,18 This may be due to the long duration of the trial for patients on study treatment. The most common reasons for discontinuation were AEs (28.7%, n=212) and patients’ requests to discontinue (10.6%, n=78).16 Of the 212 patients with AEs, latent tuberculosis/positive tuberculosis test accounted for 46.7%.16 The interim data for continuation in FINCH 4 have not yet been reported, and the study is expected to be completed in 2025.24 It is important to note that for the LTEs, patients were rerandomized from active comparators (MTX, ADA, and csDMARDs) to filgotinib by study design rather than for safety, efficacy, or tolerability.20,33 More evidence is needed for the tolerability of filgotinib in real-world settings.
Patient perspectives on treatment can also be assessed directly via PRO measures. PROs provide insight into patient quality of life (QoL) and the impact of disease on patient functionality—important measures to consider when making treatment decisions.60 QoL instruments, including the Short Form Health Survey 36 (SF-36), Health Assessment Questionnaire–Disability Index (HAQ-DI), or Functional Assessment of Chronic Illness Therapy–Fatigue (FACIT-F) scale, were administered throughout the DARWIN and FINCH programs.59,60 Though the PROs from the LTEs are not yet available, data collected from patients in the FINCH parent trials have been reported.59 Outcomes from these trials show that filgotinib improved patient functional status, QoL, fatigue, work productivity and presenteeism, and assessments of disease activity in multiple patient populations.59 MTX-IR patients treated with 200 mg filgotinib + MTX showed greater improvements in PRO measures from baseline than those treated with ADA + MTX, while 100 mg filgotinib + MTX and ADA + MTX patients experienced similar improvements in PRO measures throughout the study.59 Patients treated with either dosage of filgotinib achieved clinically meaningful improvements relative to placebo.59 In DARWIN 1 and 2, patients treated with filgotinib showed improvements in all PROs, with the exception of the SF-36 mental component in the add-on study, compared to placebo.60 Improvements in HAQ-DI, FACIT-F, patient’s global assessment, and pain were maintained or improved to week 24.60 While the FINCH and DARWIN randomized controlled trials provide insight into the potential improvements in PROs with filgotinib treatment, analysis of PROs in the LTEs is needed to determine whether these improvements in QoL persist long term.
To supplement the existing PRO data, the Adelphi RA Disease Specific Programme has provided insight into the management of RA using patient-centric outcomes in real-world settings.61 This large, multinational, point-in-time survey was conducted among rheumatologists and their patients with RA in Europe (Belgium, France, Germany, Italy, Spain, and UK) between January and October 2020.61 Physicians completed record forms for clinical and treatment data including their rationales for current treatment choices. These were then categorized into clinical or patient-centric reasons.61 JAKis were prescribed to 18.5% of patients, with 57.4% receiving treatment as monotherapy.61 When patient-centric, rheumatologist-stated reasons for any advanced therapy choice were investigated, the “acceptability of method of delivery for the patient” was the most commonly selected response at 23%, followed by “ease of product use for the patient” (16%) and “low out-of-pocket cost/affordability for patients” (10%).61 When looking at patients with RA treated with JAKis, higher rates of “acceptability of method of delivery for the patient” (35%) and “ease of product use for the patient” (24%) were reported by rheumatologists (Figure 5).61 Furthermore, improvement or maintenance of QoL was listed more often as a common patient-centric reason for physicians to prescribe JAKis (31.0%) than to prescribe other advanced therapies.61
 |
Figure 5 Patient-centric reasons physicians prescribed JAKis to patients with RA. Abbreviations: JAKi, Janus kinase inhibitor; QoL, quality of life; RA, rheumatoid arthritis. Notes: The top 5 most commonly reported patient-centric reasons for physicians prescribing JAKis in patients with RA from a large, multinational, point-in-time survey conducted among rheumatologists in Europe (Belgium, France, Germany, Italy, Spain, and UK) between January and October 2020. Reproduced with permission from John Wiley and Sons. Taylor P, Fautrel B, Piette Y, et al. Physicians’ reasons for prescribing Janus kinase inhibitors (JAKi) in patients with rheumatoid arthritis, and associated alignment between physicians and patients in a real-world clinical setting. Arthritis & Rheumatology, volume 73, supplement 9, 2021.62 |
Expert Opinions
Filgotinib shows promise to be well tolerated and effective in the long term as a treatment for moderate-to-severe RA. JAKis have similar efficacy in RA with potentially distinct safety profiles, but cross-trial comparisons have inherent limitations and potential biases.63 The safety profiles of JAKis may differ—regarding incidences of HZ, serious infections, venous thromboembolisms, decreased natural killer cell numbers, thrombocytopenia, and anemia—and these differences could be related to JAKi selectivity/preference for cytokine signaling by distinct JAK pairs.63 At therapeutic doses, filgotinib showed similar selectivity as other JAKis in the inhibition of the JAK1 pathway in an in vitro analysis.63
Filgotinib appears to be well tolerated in the longer term, as 85% to 92% of patients across treatment groups were still on filgotinib treatment after a median of 2.2 years.34–36 Better understanding of the effects of filgotinib treatment on semen parameters is needed.64 The Phase 2 MANTA and MANTA-RAy studies are investigating the potential impacts of filgotinib on semen parameters among men with active inflammatory diseases.65 No differences in semen parameters were noted between treatment groups in the proportion of patients who had a 50% or more decrease from baseline in semen parameters at week 13 (pooled primary endpoint: filgotinib 6.7%, placebo 8.3%) and at week 26.22
While controlled clinical trials for filgotinib have provided valuable data, there is an ongoing need to assess whether the trends observed in these settings reflect real-world populations. Ongoing observational studies assessing the safety, effectiveness, persistence, and PROs of filgotinib in real-world settings are underway (FILOSOPHY, NCT04871919; PARROTFISH, NCT05323591).66,67 These studies aim to assess the persistence rate of patients with moderate-to-severe RA remaining on filgotinib after 24 months of follow-up and to assess disease activity and PROs for pain, fatigue, functional assessment, and work productivity.66,67
Conclusion
The international LTEs assessing the efficacy, safety, and tolerability of filgotinib provide a better understanding of filgotinib as a treatment for patients with moderate-to-severe RA. Patients completing one of the parent studies were eligible to participate in the LTEs. Both DARWIN 3 and FINCH 4 demonstrate that the long-term safety and efficacy of filgotinib remain comparable to that shown in short-term data from the parent trials. PROs collected during the parent trials showed marked improvements with filgotinib compared to active comparators, and these PROs are being studied in the FINCH 4 LTE. Patients’ persistence in the LTEs suggests that filgotinib remains tolerable over time. Overall, the data collected from short- and long-term clinical trials have shown filgotinib to be a safe, effective, and tolerable option for patients with moderate-to-severe RA with various treatment backgrounds. However, more evidence is needed to assess whether such trends are observed in a real-world setting.
Acknowledgments
The authors acknowledge Natsumi Fujita, BSc, and Jennifer Evans, PhD, of Costello Medical Singapore Pte Ltd, for medical writing and editorial assistance, along with Danielle Shepherd, PhD, of AlphaScientia, a Red Nucleus company, based on the authors’ input and direction.
Funding
Support for third-party writing assistance for this article was provided by Natsumi Fujita, BSc, and Jennifer Evans, PhD, from Costello Medical Singapore Pte Ltd. Editorial services were provided by Danielle Shepherd, PhD, of AlphaScientia, a Red Nucleus company, and funded by Gilead Sciences, Inc.
Disclosure
Y. Tanaka has received speaking fees and/or honoraria from Boehringer Ingelheim, Eli Lilly, AbbVie, Gilead Sciences, Inc., AstraZeneca, Bristol-Myers Squibb, Chugai, Daiichi-Sankyo, Eisai, Pfizer, Mitsubishi-Tanabe, and GlaxoSmithKline; and received research grants from Asahi-Kasei, AbbVie, Chugai, Eisai, Takeda, Daiichi-Sankyo, and Boehringer Ingelheim. M. Genovese and H. Matsushima are employees of Gilead Sciences, Inc., and may hold stock options. The authors report no other conflicts of interest in this work.
References
1. Almutairi K, Nossent J, Preen D, Keen H, Inderjeeth C. The global prevalence of rheumatoid arthritis: a meta-analysis based on a systematic review. Rheumatol Int. 2021;41(5):863–877. doi:10.1007/s00296-020-04731-0
2. Almutairi KB, Nossent JC, Preen DB, Keen HI, Inderjeeth CA. The prevalence of rheumatoid arthritis: a systematic review of population-based studies. J Rheumatol. 2021;48(5):669–676. doi:10.3899/jrheum.200367
3. Biggioggero M, Becciolini A, Crotti C, Agape E, Favalli EG. Upadacitinib and filgotinib: the role of JAK1 selective inhibition in the treatment of rheumatoid arthritis. Drugs Context. 2019;8:212595. doi:10.7573/dic.212595
4. Tanaka Y, Kavanaugh A, Wicklund J, McInnes IB. Filgotinib, a novel JAK1-preferential inhibitor for the treatment of rheumatoid arthritis: an overview from clinical trials. Mod Rheumatol. 2022;32(1):1–11. doi:10.1080/14397595.2021.1902617
5. Tanaka Y, Luo Y, O’Shea JJ, Nakayamada S. Janus kinase-targeting therapies in rheumatology: a mechanisms-based approach. Nat Rev Rheumatol. 2022;18(3):133–145. doi:10.1038/s41584-021-00726-8
6. Angelini J, Talotta R, Roncato R, et al. JAK-inhibitors for the treatment of rheumatoid arthritis: a focus on the present and an outlook on the future. Biomolecules. 2020;10(7):1002. doi:10.3390/biom10071002
7. O’Shea JJ, Kontzias A, Yamaoka K, Tanaka Y, Laurence A. Janus kinase inhibitors in autoimmune diseases. Ann Rheum Dis. 2013;72(suppl 2):ii111–ii115. doi:10.1136/annrheumdis-2012-202576
8. Scherer HU, Haupl T, Burmester GR. The etiology of rheumatoid arthritis. J Autoimmun. 2020;110:102400. doi:10.1016/j.jaut.2019.102400
9. Smolen JS, Landewe RBM, Bergstra SA, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82(1):3–18. doi:10.1136/ard-2022-223356
10. Tanaka Y, Maeshima K, Yamaoka K. In vitro and in vivo analysis of a JAK inhibitor in rheumatoid arthritis. Ann Rheum Dis. 2012;71(suppl 2):i70–i74. doi:10.1136/annrheumdis-2011-200595
11. Kim ES, Keam SJ. Filgotinib in rheumatoid arthritis: a profile of its use. Clin Drug Investig. 2021;41(8):741–749. doi:10.1007/s40261-021-01055-0
12. Combe B, Kivitz A, Tanaka Y, et al. Filgotinib versus placebo or adalimumab in patients with rheumatoid arthritis and inadequate response to methotrexate: a phase III randomised clinical trial. Ann Rheum Dis. 2021;80(7):848–858. doi:10.1136/annrheumdis-2020-219214
13. Combe BG, Tanaka Y, Buch MH, et al. Efficacy and safety of filgotinib in patients with high risk of poor prognosis who showed inadequate response to MTX: a post hoc analysis of the FINCH 1 study. Rheumatol Ther. 2022;10(1):53–70. doi:10.1007/s40744-022-00498-x
14. Genovese MC, Kalunian K, Gottenberg JE, et al. Effect of filgotinib vs placebo on clinical response in patients with moderate to severe rheumatoid arthritis refractory to disease-modifying antirheumatic drug therapy: the FINCH 2 randomized clinical trial. JAMA. 2019;322(4):315–325. doi:10.1001/jama.2019.9055
15. Kavanaugh A, Kremer J, Ponce L, et al. Filgotinib (GLPG0634/GS-6034), an oral selective JAK1 inhibitor, is effective as monotherapy in patients with active rheumatoid arthritis: results from a randomised, dose-finding study (DARWIN 2). Ann Rheum Dis. 2017;76(6):1009–1019. doi:10.1136/annrheumdis-2016-210105
16. Kavanaugh A, Westhovens RR, Winthrop KL, et al. Safety and efficacy of filgotinib: up to 4-year results from an open-label extension study of phase II rheumatoid arthritis programs. J Rheumatol. 2021;48(8):1230–1238. doi:10.3899/jrheum.201183
17. Westhovens R, Rigby WFC, van der Heijde D, et al. Filgotinib in combination with methotrexate or as monotherapy versus methotrexate monotherapy in patients with active rheumatoid arthritis and limited or no prior exposure to methotrexate: the phase 3, randomised controlled FINCH 3 trial. Ann Rheum Dis. 2021;80(6):727–738. doi:10.1136/annrheumdis-2020-219213
18. Westhovens R, Taylor PC, Alten R, et al. Filgotinib (GLPG0634/GS-6034), an oral JAK1 selective inhibitor, is effective in combination with methotrexate (MTX) in patients with active rheumatoid arthritis and insufficient response to MTX: results from a randomised, dose-finding study (DARWIN 1). Ann Rheum Dis. 2017;76(6):998–1008. doi:10.1136/annrheumdis-2016-210104
19. Winthrop KL, Tanaka Y, Takeuchi T, et al. Integrated safety analysis of filgotinib in patients with moderately to severely active rheumatoid arthritis receiving treatment over a median of 1.6 years. Ann Rheum Dis. 2022;81(2):184–192. doi:10.1136/annrheumdis-2021-221051
20. Tanaka Y, Matsubara T, Atsumi T, et al. Safety and efficacy of filgotinib for Japanese patients with RA and inadequate response to MTX: FINCH 1 52-week results and FINCH 4 48-week results. Mod Rheumatol. 2022:roac084. doi:10.1093/mr/roac084
21. Atsumi T, Tanaka Y, Matsubara T, et al. Long-term safety and efficacy of filgotinib treatment for rheumatoid arthritis in Japanese patients naive to MTX treatment (FINCH 3). Mod Rheumatol. 2022:roac083. doi:10.1093/mr/roac083
22. European Medicines Agency. Jyseleca summary of product characteristics [Annex 1]. European Union: European Medicines Agency; 2022.
23. Galapagos NV. Long-term follow-up study of GLPG0634 in active rheumatoid arthritis patients (DARWIN 3). NLM identifier: NCT02065700. Available from: https://clinicaltrials.gov/ct2/show/NCT02065700.
24. Galapagos NV. Long-term extension study to assess the safety and efficacy of filgotinib in adults with rheumatoid arthritis (FINCH 4). NLM identifier: NCT03025308. Available from: https://clinicaltrials.gov/ct2/show/NCT03025308.
25. Galapagos NV. Dose-finding study of GLPG0634 as monotherapy in active rheumatoid arthritis (RA) participants (DARWIN2). NLM identifier: NCT01894516. Available from: https://clinicaltrials.gov/ct2/show/results/NCT01894516?term=DARWIN+2&draw=2&rank=1&view=results.
26. Galapagos NV. Dose-finding study of GLPG0634 as add-on to methotrexate in active rheumatoid arthritis participants (DARWIN1). NLM identifier: NCT01888874. Available from: https://clinicaltrials.gov/ct2/show/results/NCT01888874.
27. Gilead Sciences, Inc. Filgotinib versus placebo in adults with active rheumatoid arthritis (RA) who have an inadequate response to biologic disease-modifying anti-rheumatic drug(s) (DMARDs) treatment (FINCH 2). NLM identifier: NCT02873936. Available from: https://clinicaltrials.gov/ct2/show/results/NCT02873936?term=Finch+2&draw=2&rank=1&view=results.
28. Gilead Sciences, Inc. Filgotinib alone and in combination with methotrexate (MTX) in adults with moderately to severely active rheumatoid arthritis who are naive to MTX therapy (FINCH 3). NLM identifier: NCT02886728. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT02886728.
29. Gilead Sciences, Inc. Filgotinib in combination with methotrexate in adults with moderately to severely active rheumatoid arthritis who have an inadequate response to methotrexate (FINCH 1). NLM identifier: NCT02889796. Available from: https://classic.clinicaltrials.gov/ct2/show/NCT02889796.
30. Jyseleca. Medicines and healthcare products regulatory agency; 2022. Available from: https://products.mhra.gov.uk/search/?search=Jyseleca&page=1.
31. Anderson K, Zheng H, Kotecha M, et al. The relative bioavailability and effects of food and acid-reducing agents on filgotinib tablets in healthy subjects. Clin Pharmacol Drug Dev. 2019;8(5):585–594. doi:10.1002/cpdd.659
32. Dhillon S, Keam SJ. Filgotinib: first approval. Drugs. 2020;80(18):1987–1997. doi:10.1007/s40265-020-01439-0
33. Buch M, Takeuchi T, Rajendran V, et al. Clinical outcomes up to week 48 of ongoing filgotinib RA long-term extension trial of biologic DMARD inadequate responders initially on filgotinib or placebo in a phase 3 trial. Arthritis Rheumatol. 2021;73(suppl 9):1.
34. Combe B, Tanaka Y, Emery P, et al. Clinical outcomes up to week 48 of filgotinib treatment in an ongoing long-term extension trial of RA patients with inadequate response to MTX initially treated with filgotinib or adalimumab during the phase 3 parent trial. Arthritis Rheumatol. 2021;73(suppl 9):1.
35. Aletaha D, Westhovens R, Atsumi T, et al. Clinical outcomes of MTX-naïve RA patients on filgotinib long-term extension trial initially on FIL or MTX during phase 3 parent trial. Arthritis Rheumatol. 2021;73(suppl 9):1.
36. Winthrop K, Tanaka Y, Takeuchi T, et al. Integrated safety analysis update for filgotinib in patients with moderately to severely active rheumatoid arthritis receiving treatment over a median of 2.2 years.
37. Sunzini F, McInnes I, Siebert S. JAK inhibitors and infections risk: focus on herpes zoster. Ther Adv Musculoskelet Dis. 2020;12:1759720X20936059. doi:10.1177/1759720X20936059
38. Gouverneur A, Avouac J, Prati C, et al. POS0225 Risk of major cardiovascular event across JAK inhibitor treated patients: analysis of a national claim database. Ann Rheum Dis. 2021;80(suppl 1):331–332. doi:10.1136/annrheumdis-2021-eular.2976
39. Burmester GR, Kremer JM, Van den Bosch F, et al. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10139):2503–2512. doi:10.1016/S0140-6736(18)31115-2
40. Genovese MC, Fleischmann R, Combe B, et al. Safety and efficacy of upadacitinib in patients with active rheumatoid arthritis refractory to biologic disease-modifying anti-rheumatic drugs (SELECT-BEYOND): a double-blind, randomised controlled phase 3 trial. Lancet. 2018;391(10139):2513–2524. doi:10.1016/S0140-6736(18)31116-4
41. Chodara AM, Wattiaux A, Bartels CM. Managing cardiovascular disease risk in rheumatoid arthritis: clinical updates and three strategic approaches. Curr Rheumatol Rep. 2017;19(4):16. doi:10.1007/s11926-017-0643-y
42. Aubry MC, Maradit-Kremers H, Reinalda MS, Crowson CS, Edwards WD, Gabriel SE. Differences in atherosclerotic coronary heart disease between subjects with and without rheumatoid arthritis. J Rheumatol. 2007;34(5):937–942.
43. Avalos I, Chung CP, Oeser A, et al. Increased augmentation index in rheumatoid arthritis and its relationship to coronary artery atherosclerosis. J Rheumatol. 2007;34(12):2388–2394.
44. Castañeda S, Nurmohamed MT, González-Gay MA. Cardiovascular disease in inflammatory rheumatic diseases. Best Pract Res Clin Rheumatol. 2016;30(5):851–869. doi:10.1016/j.berh.2016.10.006
45. Charles-Schoeman C, Lee YY, Grijalva V, et al. Cholesterol efflux by high density lipoproteins is impaired in patients with active rheumatoid arthritis. Ann Rheum Dis. 2012;71(7):1157–1162. doi:10.1136/annrheumdis-2011-200493
46. Charles-Schoeman C, Watanabe J, Lee YY, et al. Abnormal function of high-density lipoprotein is associated with poor disease control and an altered protein cargo in rheumatoid arthritis. Arthritis Rheum. 2009;60(10):2870–2879. doi:10.1002/art.24802
47. Libby P. Inflammation in atherosclerosis. Nature. 2002;420(6917):868–874. doi:10.1038/nature01323
48. Wallberg-Jonsson S, Caidahl K, Klintland N, Nyberg G, Rantapaa-Dahlqvist S. Increased arterial stiffness and indication of endothelial dysfunction in long-standing rheumatoid arthritis. Scand J Rheumatol. 2008;37(1):1–5. doi:10.1080/03009740701633238
49. Watanabe J, Charles-Schoeman C, Miao Y, et al. Proteomic profiling following immunoaffinity capture of high-density lipoprotein: association of acute-phase proteins and complement factors with proinflammatory high-density lipoprotein in rheumatoid arthritis. Arthritis Rheum. 2012;64(6):1828–1837. doi:10.1002/art.34363
50. Redeker I, Albrecht K, Kekow J, et al. Risk of herpes zoster (shingles) in patients with rheumatoid arthritis under biologic, targeted synthetic and conventional synthetic DMARD treatment: data from the German RABBIT register. Ann Rheum Dis. 2022;81(1):41–47. doi:10.1136/annrheumdis-2021-220651
51. Cohen SB, Tanaka Y, Mariette X, et al. Long-term safety of tofacitinib for the treatment of rheumatoid arthritis up to 8.5 years: integrated analysis of data from the global clinical trials. Ann Rheum Dis. 2017;76(7):1253–1262. doi:10.1136/annrheumdis-2016-210457
52. Cohen SB, Tanaka Y, Mariette X, et al. Long-term safety of tofacitinib up to 9.5 years: a comprehensive integrated analysis of the rheumatoid arthritis clinical development programme. RMD Open. 2020;6(3):e001395. doi:10.1136/rmdopen-2020-001395
53. Cohen SB, van Vollenhoven RF, Winthrop KL, et al. Safety profile of upadacitinib in rheumatoid arthritis: integrated analysis from the SELECT phase III clinical programme. Ann Rheum Dis. 2021;80(3):304–311. doi:10.1136/annrheumdis-2020-218510
54. Winthrop KL, Harigai M, Genovese MC, et al. Infections in baricitinib clinical trials for patients with active rheumatoid arthritis. Ann Rheum Dis. 2020;79(10):1290–1297. doi:10.1136/annrheumdis-2019-216852
55. Harrington R, Al Nokhatha SA, Conway R. JAK inhibitors in rheumatoid arthritis: an evidence-based review on the emerging clinical data. J Inflamm Res. 2020;13:519–531. doi:10.2147/JIR.S219586
56. Felson DT, Anderson JJ, Boers M, et al. American College of Rheumatology. Preliminary definition of improvement in rheumatoid arthritis. Arthritis Rheum. 1995;38(6):727–735. doi:10.1002/art.1780380602
57. Tóth L, Juhász MF, Szabó L, et al. Janus kinase inhibitors improve disease activity and patient-reported outcomes in rheumatoid arthritis: a systematic review and meta-analysis of 24,135 patients. Int J Mol Sci. 2022;23(3). doi:10.3390/ijms23031246
58. Aletaha D, Westhovens R, Combe B, et al. POS0676 Efficacy and safety of filgotinib in patients aged greater than 75 years: a post hoc subgroup analysis of the FINCH 4 long-term extension (LTE) study. Ann Rheum Dis. 2022;81(1):612–613. doi:10.1136/annrheumdis-2022-eular.1563
59. Bingham CO, Walker D, Nash P, et al. The impact of filgotinib on patient-reported outcomes and health-related quality of life for patients with active rheumatoid arthritis: a post hoc analysis of phase 3 studies. Arthritis Res Ther. 2022;24(1):11. doi:10.1186/s13075-021-02677-7
60. Genovese M, Westhovens R, Meuleners L, et al. Effect of filgotinib, a selective JAK 1 inhibitor, with and without methotrexate in patients with rheumatoid arthritis: patient-reported outcomes. Arthritis Res Ther. 2018;20(1):57. doi:10.1186/s13075-018-1541-z
61. Taylor PC, Fautrel B, Piette Y, et al. Treat-to-target in rheumatoid arthritis: a real-world study of the application and impact of treat-to-target within the wider context of patient management, patient centricity and advanced therapy use in Europe. RMD Open. 2022;8(2):e002658. doi:10.1136/rmdopen-2022-002658
62. Taylor P, Fautrel B, Piette Y, et al. Physicians’ reasons for prescribing Janus kinase inhibitors (JAKi) in patients with rheumatoid arthritis, and associated alignment between physicians and patients in a real-world clinical setting. Arthritis Rheumatol. 2021;73(suppl 9):1.
63. Traves PG, Murray B, Campigotto F, Galien R, Meng A, Di Paolo JA. JAK selectivity and the implications for clinical inhibition of pharmacodynamic cytokine signalling by filgotinib, upadacitinib, tofacitinib and baricitinib. Ann Rheum Dis. 2021;80(7):865–875. doi:10.1136/annrheumdis-2020-219012
64. Food and Drug Administration. Gilead receives complete response letter for filgotinib for the treatment of moderately to severely active rheumatoid arthritis; 2020. Available from: https://wwwam10.gilead.com/en/news-and-press/press-room/press-releases/2020/8/gilead-receives-complete-response-letter-for-filgotinib-for-The-treatment-of-moderately-to-severely-active-rheumatoid-arthritis.
65. Hellstrom WJG, Dolhain R, Ritter TE, et al. MANTA and MANTA-RAy: rationale and design of trials evaluating effects of filgotinib on semen parameters in patients with inflammatory diseases. Adv Ther. 2022;39(7):3403–3422. doi:10.1007/s12325-022-02168-4
66. Galapagos NV. Prospective observational study of filgotinib in subjects with rheumatoid arthritis (FILOSOPHY). NLM identifier: NCT04871919. Available from: https://clinicaltrials.gov/ct2/show/NCT04871919.
67. Galapagos NV. Prospective observational study of filgotinib in female participants with rheumatoid arthritis in France (PARROTFISH). NLM identifier: NCT05323591. Available from: https://www.clinicaltrials.gov/ct2/show/NCT05323591?term=filgotinib&cond=rheumatoid+arthritis&draw=2&rank=1.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.