Back to Journals » Patient Related Outcome Measures » Volume 9
Long-term safety and real-world effectiveness of fingolimod in relapsing multiple sclerosis
Authors Druart C ![]() , El Sankari S, van Pesch V
, El Sankari S, van Pesch V ![]()
Received 8 July 2017
Accepted for publication 3 November 2017
Published 21 December 2017 Volume 2018:9 Pages 1—10
DOI https://doi.org/10.2147/PROM.S122401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Charlotte Druart, Souraya El Sankari, Vincent van Pesch
Neurology Department, Cliniques Universitaires Saint-Luc, Université Catholique de Louvain, Brussels, Belgium
Abstract: With a growing number of disease-modifying therapies becoming available for relapsing multiple sclerosis, there is an important need to gather real-world evidence data regarding long-term treatment effectiveness and safety in unselected patient populations. Although not providing as high a level of evidence as randomized controlled trials, and prone to bias, real-world studies from observational studies or registries nevertheless provide crucial information on real-world outcomes of a given therapy. In addition, evaluation of treatment satisfaction and impact on quality of life are increasingly regarded as complementary outcome measures. Fingolimod was the first oral disease-modifying therapy approved for relapsing multiple sclerosis. This review aims to summarize current knowledge on the long-term effectiveness and safety outcomes of multiple sclerosis patients on fingolimod. Impact on treatment satisfaction and quality of life will be discussed according to available data.
Keywords: multiple sclerosis, fingolimod, quality of life, safety, effectiveness, long-term, real-world evidence, patient-reported outcomes
Introduction
Multiple sclerosis (MS) is a chronic inflammatory demyelinating and neurodegenerative disease of the central nervous system (CNS).1 It affects over 2.3 million people worldwide, and is the most common cause of atraumatic disability in young adults. Its most common clinical presentation is relapsing–remitting MS (RRMS; 85%–90%), in which subacute bouts of neurological worsening seem to be driven at least partly by invasion of the CNS by adaptive immune cells.2,3 As the disease evolves over time, there is disability progression (DP), resulting in reduced quality of life (QoL).4 There is an increasing armamentarium of disease-modifying treatments (DMTs), both injectable and oral, with different mechanisms of action approved for relapsing MS. It is now recognized that the overall objective in treating MS includes preventing relapses, DP, and increase in CNS-lesion burden as seen on magnetic resonance imaging (MRI). These outcomes are included in the composite measure of no evidence of disease activity (NEDA).5,6 NEDA 4 also includes follow-up of brain-volume loss as surrogate marker for neurodegeneration and disability worsening.
Phase III randomized controlled trials assess the short-term efficacy and safety of DMTs in a strictly preselected patient population. Real-world evidence (RWE) is defined as data regarding a treatment that are not collected in a randomized controlled trial.7 RWE is gathered in unselected patient populations and can provide more generalizable data and also long-term evidence on a wide variety of end points such as effectiveness, safety or other outcomes, such as patient-reported outcomes (PROs). Despite existing bias, due to the non-randomized setting in which data is collected, RWE can still provide evidence that can be used for post-marketing decision making by health care providers or regulatory authorities.8 There is however an unmet need for RWE data, regarding long-term outcomes on more recently introduced DMTs, to understand their comparative benefits in this complex and evolving landscape.
PROs are increasingly recognized as complementary outcomes measures to classical end points not captured by classical measures, such as the Expanded Disability Status Scale (EDSS). They can provide additional insight on disease status by evaluating mood, fatigue, treatment satisfaction, and QoL.9 In the setting of MS, a large-scale European survey recently showed that reported decreases in QoL were correlated with increasing disease severity in the domains of mobility, self-care, usual activities, and pain/discomfort.10
Traditional injectable DMTs, such as IFNβ and glatiramer acetate, have been the mainstay of first-line RRMS treatment for the past two decades and have overall good safety profiles. However, the efficacy of these agents may be limited in some patients.11,12 In addition, the need for long-term self-administration of injections imposes a significant burden on patients, because of tolerability issues and injection-site-related side effects.13,14 This can be responsible for reduced treatment persistence in the long run and potentially affects QoL.15
Fingolimod (Gilenya; Novartis International AG, Basel, Switzerland) is a sphingosine 1 phosphate-receptor modulator that selectively and reversibly retains naïve and central memory T-lymphocytes within lymph nodes, thereby preventing them from circulating to other tissues, including the CNS.16 It was the first oral therapy approved to treat relapsing MS by the US Food and Drug Administration (FDA) in September 2010. The European Medicines Agency approved fingolimod for rapidly evolving severe MS or failure of first-line therapy in RRMS in January 2011. In total, three Phase III studies – FREEDOMS, FREEDOMS II, and TRANSFORMS – demonstrated the efficacy of fingolimod in reducing the annualized relapse rate (ARR) and improving MRI outcomes, including slowing of brain-volume loss compared with placebo or intramuscular IFNβ1a.17–19
By May 31, 2017, it was estimated that over 213,000 patients worldwide had been treated with fingolimod, resulting in 453,000 patient-years of exposure (Novartis International AG, data on file, September 2017). This underscores the importance of gathering RWE concerning the long-term outcomes of treatment with fingolimod. This review aims to summarize current knowledge on the long-term effectiveness and safety outcomes of MS patients on fingolimod. Impact on treatment satisfaction and QoL is discussed according to available data.
Materials and methods
A bibliographic search was performed in PubMed (https://www.ncbi.nlm.nih.gov/pubmed) and on published abstracts from the following international congresses: Annual Congress of the European Committee for Treatment and Research in Multiple Sclerosis, Annual Meeting of the American Academy of Neurology, Annual Meeting of the European Neurological Society, European Academy of Neurology Congress, and congresses of the International Society for Pharmacoeconomics and Outcomes Research. Keywords used were fingolimod, multiple sclerosis, effectiveness, safety, open-label, extension, quality of life, patient-reported outcomes, long-term, and observational.
Only studies reporting effectiveness or safety with a follow-up of more than 2 years were selected for review. Studies including PROs and QoL measures were retained regardless of fingolimod-treatment duration. Figure 1 illustrates the process of selection of published papers and congress abstracts for this review.
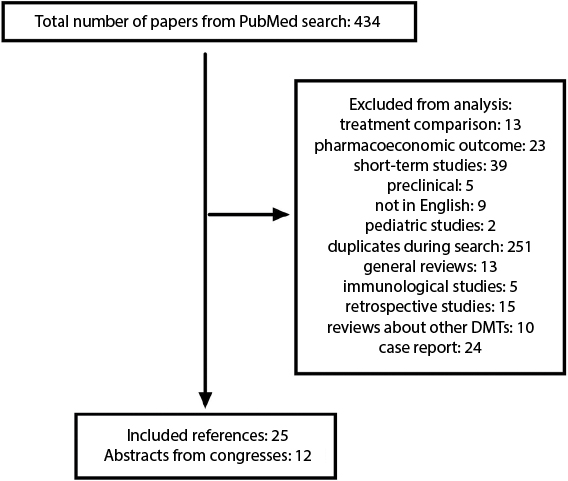 | Figure 1 Selection process for published papers. Note: In addition to papers and abstracts selected, 21 additional references were included for the Introduction and Discussion sections. Abbreviation: DMTs, disease-modifying treatments. |
Efficacy from clinical trials and real-world effectiveness of fingolimod
Efficacy from pivotal Phase III clinical trials
FREEDOMS, FREEDOMS II, and TRANSFORMS were three large, randomized, double-blind, multicenter, pivotal Phase III clinical trials for fingolimod in patients with RRMS.17–19 In the 24-month FREEDOMS trial,17 daily 0.5 mg fingolimod significantly reduced the ARR by 54% (P<0.001) and risk of 6-month confirmed DP (CDP) by 37% (P=0.01) relative to placebo. Across the study duration, the number of gadolinium-enhancing lesions (GELs) was reduced by 79%, number of new or enlarged T2 lesions by 74%, and brain-volume loss by 36% (P<0.001 for all).
In TRANSFORMS,18 the ARR at 1 year was reduced by 52% in 0.5 mg fingolimod-treated patients compared to those treated with intramuscular IFNβ1a (P<0.001). GELs were reduced by 55% (P<0.001), new or enlarged T2 lesions by 35% (P<0.004), and brain-volume loss by 31% (P<0.001). The risk of DP was reduced by 29% (nonsignificant versus active comparator).
The FREEDOMS II trial19 was similar in design and objectives to FREEDOMS, except that it included additional outcome measures at the request of the FDA. The ARR was reduced by 48% in 0.5 mg fingolimod-treated patients relative to placebo (P<0.0001), number of GELs by 70% (P<0.0001), number of new or enlarged T2 lesions by 74% (P<0.0001), and brain-volume loss by 31% (P<0.0002). A post hoc analysis showed that the 3 month CDP was reduced by 30% (P=0.04) in patients with an EDSS score above 0.
Efficacy from the Phase II and III extension trials
In the Phase II extension study, patients receiving placebo were rerandomized to daily fingolimod 5 mg or 1.25 mg. At month 24, patients on fingolimod 5 mg were switched to fingolimod 1.25 mg, and at month 60 all patients were switched to fingolimod 0.5 mg, due to safety considerations.20 Median treatment duration was 5.1 years, and 122 patients completed the study with over 7 years of treatment (Table 1). Overall, in patients treated for at least 6 months (n=243), the ARR remained low (0.17), 60.9% were free from relapse, and 82% from 6 month CDP. MRI outcomes were also favorable, with 84%–96% of patients free of GELs between years 1 and 7, regardless of initial randomization (Table 2). Throughout the study period, 68%–88% of patients were free from new or enlarging T2 lesions.
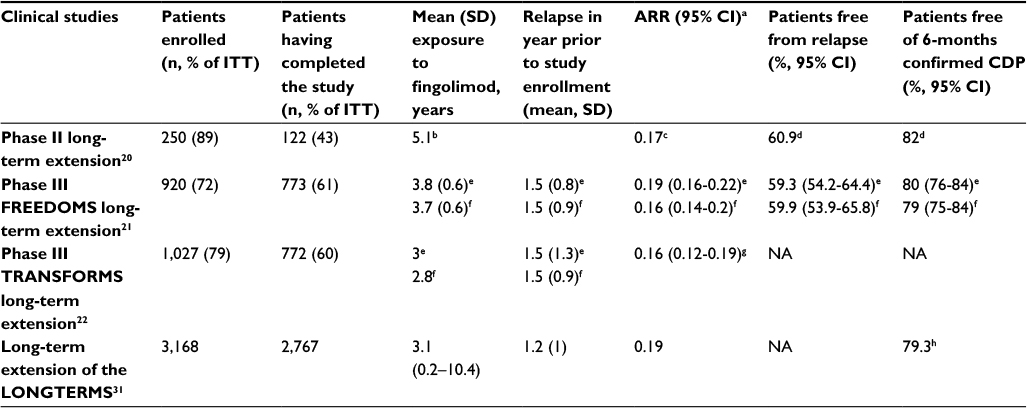 | Table 1 Clinical end points from the fingolimod extension studies Notes: aOver entire duration of observation period; bmedian; cin patients having received at least 6 months of fingolimod; dKaplan–Meier estimates adjusted for dropouts in patients exposed to fingolimod for 6 months at least; ein continuous fingolimod 0.5 mg group; fin continuous fingolimod 1.25 mg group; gbetween month 13 (beginning of extension phase) and end of study; hat month 60 for 729 patients. Abbreviations: ITT, intent to treat; ARR, annualized relapse rate; CDP, confirmed disease progression. |
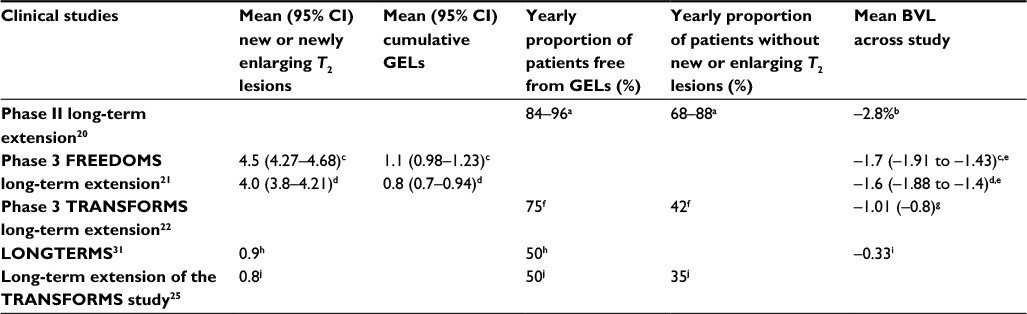 | Table 2 Radiological endpoints of fingolimod extension studies Notes: aRegardless of initial randomization group, yearly percentages from year 1 to year 7; bcalculated over 84 months; cin continuous fingolimod 0.5 mg group over 48 months; din continuous fingolimod 1.25 mg group over 48 months; e95% CI; ffor fingolimod 0.5 mg group between month 13 (beginning of extension phase) and end of study; gSD; h between months 0 and 60 (n=605)31; iannualized rate of BVL between months 0 and 60 (n=548)31; jbetween months 0-60 (n=924).25 Abbreviations: GELs, gadolinium-enhancing lesions; BVL, brain-volume loss. |
The extensions of the three pivotal fingolimod Phase III trials also provided evidence of the prolonged efficacy of the treatment. It must be noted that both 0.5 mg and 1.25 mg fingolimod doses were initially evaluated in the extension studies. In FREEDOMS and FREEDOMS II, patients on placebo who were enrolled in the extension phase were initially rerandomized to either daily fingolimod 0.5 mg or 1.25 mg.21 Similarly, in the extension of the TRANSFORMS study, patients on fingolimod remained on the same dose, although blinding was maintained, while patients on IFNβ1a were rerandomized at a 1:1 ratio to either fingolimod 0.5 mg or 1.25 mg.22 Ultimately, all remaining patients were switched to fingolimod 0.5 mg in the open-label extension (LONGTERMS, NCT01201356) upon implementation of a protocol amendment in 2009. Dropout rates and reasons for drug discontinuation from these studies are listed in Table 3. Overall, retention rates were 76%–93%, including the long-term extension study. Of note, only 13% of patients discontinued fingolimod during the LONGTERMS extension. During the Phase III trials and their extensions, 19%–36% of patients stopped fingolimod due to adverse events.
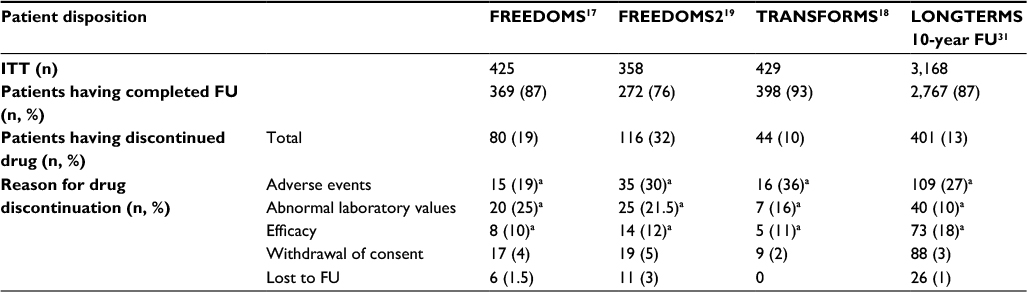 | Table 3 FU and treatment-discontinuation rates in Phase III clinical trials and the LONGTERMS extension Note: aOf total number of patients having discontinued the study drug. Abbreviations: FU, follow-up; ITT, intent to treat. |
In the 2-year extension of FREEDOMS, in patients continuously treated with fingolimod 0.5 mg per day, the ARR remained low (Table 1): 59.3% of patients (95% CI 54.2%–64.4%) remained free of relapse, while 80% (95% CI 76%–84%) were free of 6-month CDP. The mean number of GELs measured during 48 months was 1.1 in comparison to 1.6 at baseline, before randomization (Table 2). Analysis of individual measures of disease activity in the extension study of the pooled cohorts of the pivotal FREEDOMS and FREEDOMSII trials at 4 years showed better outcomes in treatment-naïve patients compared to those previously exposed to DMTs.23
In the 4.5-year extension of TRANSFORMS, in patients who received 0.5 mg of fingolimod throughout the study, the ARR during study extension was 0.16 (95% CI 0.12–0.19); 75% of patients remained free of new GELs and 42% of new or enlarging T2 lesions (Tables 1 and 2). Preliminary results from the LONGTERMS study show that 50% of patients remain free of GELs (n=924) and that 35% remain free of new or enlarging T2 lesions (n=595) up to year 5 (Table 2).24 Post hoc analysis of the TRANSFORMS and extension studies showed that 44.6%–78.3% of patients continuously on fingolimod or switching from IFNβ1a achieved NEDA 3 status from year 1 through year 8. NEDA 4 status, including mean yearly brain-volume loss ≤0.4%, was also sustained in 26.6%–53.2% of patients during the same yearly intervals.25
Long-term real-world effectiveness of fingolimod
Although a number of studies have been published regarding the effectiveness of fingolimod in an real-world (RW) setting, most report outcomes at 1 or 2 years and have recently been reviewed elsewhere.26 PANGAEA is a large-scale postmarketing study aiming to provide long-term safety and effectiveness data on 4,229 MS patients treated with fingolimod in Germany.27 A pharmacoeconomic substudy is ongoing, including 800 patients, that collects QoL, treatment-satisfaction, and health-resource consumption data through PROs. Interim results have already been communicated regarding certain outcomes of the study in a population of 4,016 patients, with mean exposure to fingolimod of 2.8 (SD 1.7) years.28 Regarding effectiveness, the reported year 3–5 ARR in patients is 0.27 (Table 4). During this interval, 76%–78.4% of patients were free of relapses and 85% free from 6-month CDP. Overall, 42.3%–44.4% of patients remained free of clinical disease activity during years 3 and 4 of treatment. No imaging outcomes have yet been communicated in this study.
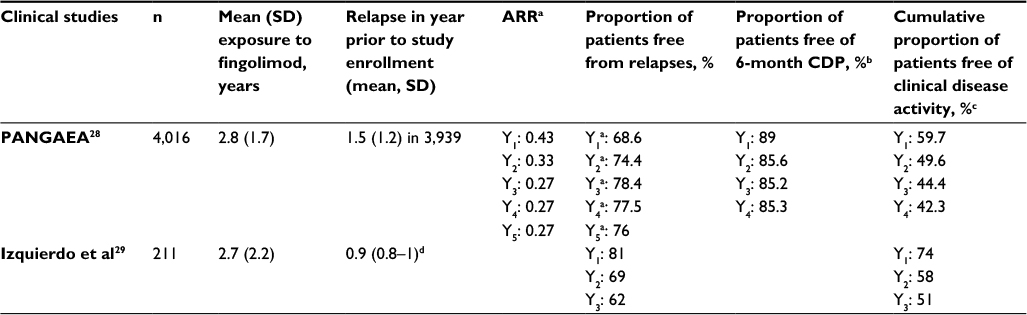 | Table 4 Clinical effectiveness in patients treated with fingolimod for more than 2 years Notes: aY1, n=3,363; Y2, n=2,690; Y3, n=1,996; Y4, n=1,139; Y5, n=474. bY1, n=2,483; Y2, n=1,913; Y3, n=1,300; Y4, n=688. cY1, n=2,670; Y2, n=2,129; Y3, n=1,463; Y4, n=763. d95% CI. Abbreviations: ARR, annualized relapse rate; CDP, confirmed disability progression. |
A retrospective study reported RW results on fingolimod effectiveness in a cohort of 249 patients, with mean treatment duration of 2.7 (SD 2.2) years.29 At year 3, 62% of patients were relapse-free and 51% remained free of clinical disease activity (Table 4). Regarding MRI outcomes, 74% of patients remained free of GELs during year 3 and 23% were free of new or enlarging T2 lesions. As a whole, 36% of patients still fulfilled the NEDA 3 criteria at that time point.
Long-term safety of fingolimod
The safety profile of fingolimod up to 2 years was defined during the Phase II and III clinical trials, and includes (among others) first-dose-related bradycardia, macular edema, hypertension, severe lymphopenia, and elevation of liver enzymes. An integrated analysis of safety data from clinical studies, their extension, and postmarketing safety data up to December 2011 has not identified any unexpected or new safety signals.30 Table 5 shows the incidence of adverse events of special interest or serious adverse events during the Phase III trials and the LONGTERMS extension up to 10 years, as well as in the large-scale RW studies PANGAEA and VIRGILE.31–33 Overall, incidence rates of the reported events were consistent with the known safety profile of fingolimod, except for cryptococcal infections and progressive multifocal leukoencephalopathy (PML), which emerged in the postmarketing setting.
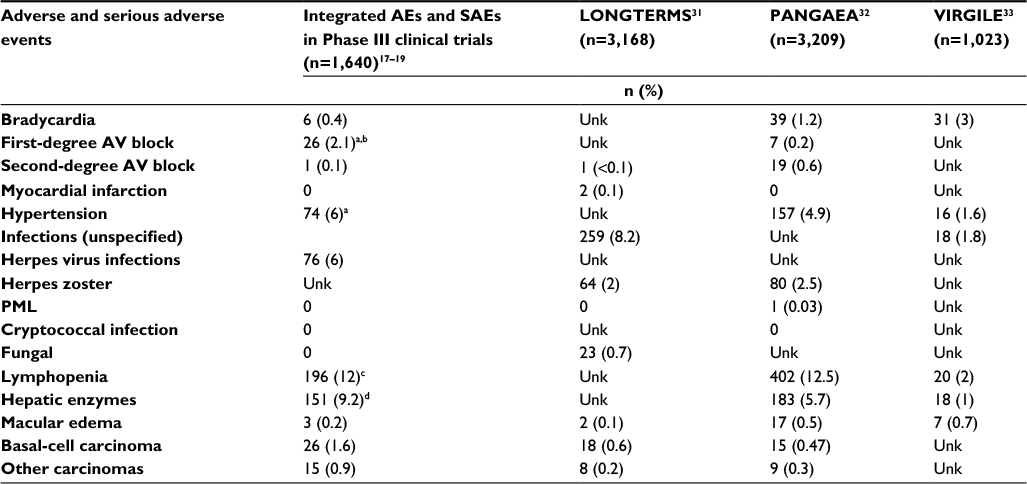 | Table 5 AEs of special interest and SAE rates during the Phase III trials, the LONGTERMS extension, and the real-world studies PANGAEA and VIRGILE Notes: aCalculated from the 1,212 patients on fingolimod 0.5 mg in the Phase III clinical trials (FREEDOMS, FREEDOMS2, and TRANSFORMS); b22 of the 26 events were classified as SAEs during the Phase III trials; cnumber of AEs, of which three (0.2%) were classified as SAEs; dnumber of AEs of which none was classified as an SAE. Abbreviations: AEs, adverse events; AV, atrioventricular; PML, progressive multifocal leukoencephalopathy; SAE, serious AE; Unk, unknown. |
Infections
In the extension of the FREEDOMS study, herpes virus infections (n=99) were reported in 9%–12.1% of patients across treatment groups.21 Similar rates were recorded during the extension of the TRANSFORMS study (10.1%–15% across treatment groups in six patients).22 In the postmarketing setting, there have been 13 confirmed cases of PML in patients on fingolimod not attributed to previous treatment with natalizumab (Novartis, data on file). Twelve cases occurred after 2 years of treatment. Over 79,000 patients worldwide have been treated for 2 years or longer with fingolimod. Therefore, the PML risk in patients treated with fingolimod for more than 2 years is estimated to be 0.152 per 1,000 patients (95% CI 0.078–0.265), corresponding roughly to one in 6,000 patients. Cases of carryover PML following switches from natalizumab to fingolimod have been reported, but no precise estimate is available on their incidence.34
Rare cases of cryptococcal infection have been reported in patients on fingolimod, either cutaneous, meningeal or disseminated.35–37 Prescribing physicians should also be aware of the risk of herpes zoster or herpes simplex reactivation while on fingolimod therapy.38–41 The risk does not increase with the duration of exposure to fingolimod, and the reactivation is not necessarily more severe, but exposure to intravenous corticosteroids for relapse might be a risk factor.42 Before initiating fingolimod treatment, it is mandatory to verify whether the patient has been immunized for the varicella zoster virus, and if not to vaccinate accordingly.
Malignancies
In the extension of the FREEDOMS study, 17 cases of malignancy occurred, among which there were ten cases of basal-cell carcinoma (0–1.4% across treatment groups).21 Similar rates were also reported during the extension of the TRANSFORMS study.22 In total, 105 cases of basal-cell carcinoma have been reported within the fingolimod clinical trials and 111 cases in the postmarketing setting (Novartis, data on file). Clinical vigilance for suspicious skin lesions is thus warranted while patients are on fingolimod therapy, and should prompt referral to a dermatologist if needed.
Up to now, apart from basal-cell carcinoma, reported malignancy rates have been within the range of expected malignancies in the general and MS populations, but have prompted the inclusion of this adverse event in the prescribing information. Long-term safety data is however still needed collected from RW observational studies, especially regarding the use of the product in an unselected patient population, with possible comorbidities and potential interactions with other medications.
Cardiovascular safety
The adverse-event profile of fingolimod includes cardiovascular events, for which practical guidelines for treatment initiation and monitoring have been implemented. Expression of the S1P1 receptor is not restricted to lymphocytes, but is also present on atrial myocytes, thereby explaining the transient negative chronotropic effect seen upon first-dose intake of fingolimod.43
In the Phase III FREEDOMS and FREEDOMS2 trials, bradycardia, first-degree atrioventricular (AV) block, and second-degree AV block were reported in 1.4%, 2.8%, and 0.1%, respectively, of patients upon treatment initiation with fingolimod 0.5 mg.17,19 Mean elevations of 3 mmHg systolic and 1 mmHg diastolic blood pressure were also reported. This has prompted open-label studies (FIRST, START) on the outcome of cardiac monitoring upon first-dose intake (Table 6).44,45 These studies have provided evidence that bradycardia is a transient, mostly asymptomatic event and that AV-conduction abnormalities are infrequent and recover spontaneously. In the FIRST study, the incidence of Mobitz type I second-degree AV block (4.1%) and 2:1 AV block (2%) was higher in patients with preexisting cardiac conditions versus those without (0.9% versus 0.3%), warranting precaution in these patients. Concomitant medications, such as selective serotonin-recapture inhibitor antidepressants or other drugs known to prolong the QT interval, β-blockers, or calcium-channel blockers did not show an effect on the incidence of cardiac adverse events.44–46
 | Table 6 Adverse events during first-dose heart-rate monitoring Notes: aFour were symptomatic; b123 (1.78%) patients had asymptomatic first-degree AV block on the ECG performed 1 week after initiating fingolimod treatment; ctiming of these adverse events was not communicated. Abbreviations: AV, atrioventricular; PR, pulse rate; NA, not available. |
Among the five patients who presented with cardiac adverse events during the 4-month follow-up of the FIRST study, 80% occurred within 48 hours of fingolimod initiation. Only two events led to drug discontinuation (unconfirmed angina pectoris and asymptomatic Mobitz I second-degree AV block).44 Longer-term follow-up in the LONGTERMS or RW PANGAEA studies did not show new safety signals regarding cardiovascular safety.31,32
MS relapses with tumefacient demyelinating lesions
The occurrence of tumefacient demyelinating lesions in individual cases following either initiation or withdrawal of treatment with fingolimod has recently been comprehensively reviewed.47 It demonstrates that in some patients, the redistribution of immune cells can have adverse effects promoting unusual disease activity. Immunological profiling studies are needed to understand the underlying mechanisms better.
Impact of fingolimod on quality of life and patient-reported outcomes
Clinical trial data
In the FREEDOMS II study, at 24 months no statistically significant differences in the EuroQol utility score, the Patient Reported Indices in Multiple Sclerosis nor the modified Fatigue Impact Scale were reported between fingolimod- and placebo-treated patients.19
Real-world evidence
The EPOC study was a 6-month, randomized, open-label, multicenter trial with an optional 3-month extension, in which 1,053 patients were randomized at a 1:3 ratio to either fingolimod or an injectable DMT.48 Patients (33.3%) were switched from glatiramer acetate to fingolimod and the remainder from subcutaneous or intramuscular IFNβ preparations. Patient satisfaction was measured by changes in the Treatment Satisfaction Questionnaire for Medication between baseline and 6 months. It improved significantly with fingolimod compared with the injectable DMT. The least-squares ± SE treatment difference was –17.5±1.68 (P<0.001).The improvement was also seen on the questionnaire subscales for effectiveness, side effects, and convenience. QoL measured with the SF-36 scale showed significant improvement in all components (physical health, bodily pain, vitality, social functioning, role limitation due to emotional problems, and general mental health). Only score increases in the domains of physical functioning and general health perceptions were nonsignificant.
A substudy of PANGAEA collecting QoL, treatment satisfaction, and health-resource consumption data is ongoing. Preliminary results of this study have been reported on 662 patients, showing that 71.2% of patients estimated their overall state of health as stable or improved (16.9%) using the EQ-5D.28 Individual (effectiveness and convenience) and overall treatment-satisfaction scores were increased up to 2 years in comparison to baseline. Recently, a substudy of PANGAEA on a small subset of patients showed improvements in cognition between 0 and 24 months using the single-digit modality test (n=83). The neuropsychological, mood, and fatigue subscores of the UK neurological disability score were also slightly improved during the first 2 years on fingolimod (n=187).49
A 12-month study performed on 172 subjects treated with fingolimod and 75 with other DMTs assessed health-related QoL using the MusiQoL questionnaire at baseline and 6 and 12 months. For both treatment cohorts, there was no significant improvement in overall MusiQoL score versus baseline. There was, however, a slight improvement in the “psychological well-being subscore” for fingolimod-treated patients at months 6 and 12 (P=0.002 and P<0.01 versus baseline, respectively).50
The VIRGILE study is an ongoing prospective observational study aiming to collect effectiveness and safety data in an RW setting. It also includes pharmacoepidemiological outcomes and assessment of the impact of fingolimod on QoL with the MusiQoL and EQ-5D questionnaires. The recruitment target is 1,200 fingolimod-treated patients, with a planned follow-up of 5 years. In addition, 600 patients on natalizumab will be recruited and followed for 3 years. Interim results show that all domains analyzed by the MusiQoL questionnaire are sustained between 6 and 24 months relative to baseline.33,51
Discussion
RWE is needed, to gain knowledge on long-term safety and effectiveness for recently introduced DMTs for MS. As the data are gathered in unselected populations, it can lead to several biases, which have been extensively reviewed by Kalincik and Butzkueven.52 However, despite not providing the same level of evidence as a randomized controlled trial, RW studies can still inform health-care practitioners and other stakeholders of long-term clinical benefits and rare adverse events. In addition, postmarketing studies can include other unconventional measures, such as pharmacoeconomic evaluations of health-care resource utilization and impact of a given intervention on patient-reported outcomes, such as QoL.
With regard to fingolimod, long-term effectiveness comes from extension studies of the pivotal trials or from observational postmarketing studies or retrospective analysis of patient cohorts. The extension studies for fingolimod have shown sustained benefit on clinical and radiological outcomes in a significant proportion of patients. However, the results should be interpreted with caution, because of the bias introduced by patient dropouts due to adverse events, lack of efficacy, or termination of a study before all patients had reached a defined treatment duration. For example, only 60% of the intent-to-treat patients completed the Phase III fingolimod extension studies (Table 1). Follow-up has been extended to 10 years now and is ongoing in the LONGTERMS study. However, only 41.3% of the 3,168 patients enrolled in LONGTERMS have reached more than 2 years of treatment and only 25 have been treated continuously for 10 years. Results concerning brain-volume loss show an advantage for early versus late treatment with fingolimod, and annualized brain-atrophy rates reported up to 5 years in the LONGTERMS study show almost normalized rates of between –0.38 and –0.33.
Short-term RW-effectiveness studies have been extensively reviewed by Ziemssen et al.26 The present review highlights the paucity of data available for treatment longer than 2 years. However, both interim results of PANGAEA and of the retrospective study by Izquierdo et al provide evidence for sustained effectiveness of fingolimod.27,29 In the latter study, 36% of patients fulfilled the NEDA 3 criteria at year 3 and more than 40% of patients in the PANGAEA study were free of clinical disease activity during years 3 and 4 of treatment (n=1,463 and n=763, respectively). Ongoing initiatives include PANGAEA and VIRGILE. Other national or international registries, such as MSBase, also aim at gathering long-term effectiveness data.53 It should be noted, however, that these studies or others should include not only clinical but also radiological evidence of treatment effectiveness. In addition to conventional imaging outcomes, such as the number of GELs and T2 lesions, the rate of brain-volume loss could also be measured. MS-MRIUS is an ongoing multicenter observational study of patients treated with fingolimod in the US. It captures MRI data acquired in routine clinical practice during 24 months that will also be used for brain-volumetric analysis. The purpose of this study is to evaluate the proportion of patients achieving NEDA 3/4 status at 12 and 24 months.54
Safety is an important concern for long-term DMT in MS. Until now, extension studies and PANGAEA have reported adverse events consistent with the known profile of fingolimod.55 It must be noted, however, that rare adverse events having occurred while on fingolimod therapy are published as case reports. PML, Cryptococcus infection, hemophagocytic syndrome, Kaposi’s sarcoma, vasculopathy, or encephalopathy have been individually reported and reviewed recently by Fragoso.56 These rare occurrences have (to our knowledge) not been captured in the long-term studies discussed herein. The primary end point of the international observational PASSAGE study (NCT01442194) is the incidence of collected adverse events. Other ongoing registries capturing safety data, such as BELTRIMS, might also contribute to collection of safety data on the long-term use of fingolimod in a RW setting.59
This review of literature and congress abstracts shows that although the collection of PROs and QoL data is advocated as useful and complementary for a comprehensive multimodal assessment of treatment response, data on these outcomes remain scarce, notably for the RW use of fingolimod. The EPOC study demonstrated in a large cohort of patient transitioning from injectable DMTs to fingolimod an increase in all aspects of treatment satisfaction (effectiveness, convenience, and side effects) as well as a significant improvement in all QoL components of the SF-36 scale, except the physical functioning and general health domains.48 These results were replicated in an independent cohort. Preliminary results of the PANGAEA substudy show 88% of patients estimated that their overall state of health was stable or improved on fingolimod at 2 years of treatment.28 As in the EPOC study, treatment satisfaction was increased in comparison to baseline. The VIRGILE study, with enrolment of 1,200 patients on fingolimod planned, is another ongoing large-scale prospective study that includes QoL outcomes using other scales, such as the MusiQoL.
In conclusion, more data are needed on the long-term effectiveness and safety of fingolimod in unselected patient cohorts, as most postmarketing observational studies published until now have reported outcomes of 2 years or less. Several national or international initiatives are ongoing, gathering these data prospectively. There is, however, a lack of data on PROs. In the short term, EPOC provided evidence on treatment satisfaction and QoL after 6 months of treatment with fingolimod. The ongoing PANGAEA and VIRGILE studies will also provide information on QoL outcomes in an RW setting at 2 and 3 years, respectively. In order to obtain complete and informative data on long-term use of fingolimod, study protocols should comprehensively assess all relevant clinical and radiological outcome measures, in accordance with current recommendations.57,58
Disclosure
V van Pesch has received travel grants from Biogen, Bayer Schering, Sanofi Genzyme, Merck, Teva, Novartis Pharma and Roche. His institution receives honoraria for consultancy and lectures from Biogen, Bayer Schering, Sanofi Genzyme, Merck, Roche, Teva and Novartis Pharma as well as research grants from Novartis Pharma, Roche and Bayer Schering. S El Sankari has received travel grants from Biogen, Sanofi Genzyme, Merck and Teva. The authors report no other conflicts of interest in this work.
References
Sospedra M, Martin R. Immunology of multiple sclerosis. Annu Rev Immunol. 2005;23:683–747. | ||
Tullman MJ. Overview of the epidemiology, diagnosis, and disease progression associated with multiple sclerosis. Am J Manag Care. 2013;19(2 Suppl):S15–S20. | ||
Frischer JM, Bramow S, Dal-Bianco A, et al. The relation between inflammation and neurodegeneration in multiple sclerosis brains. Brain. 2009;132(Pt 5):1175–1189. | ||
Janardhan V, Bakshi R. Quality of life in patients with multiple sclerosis: the impact of fatigue and depression. J Neurol Sci. 2002;205(1):51–58. | ||
Ziemssen T, Derfuss T, de Stefano N, et al. Optimizing treatment success in multiple sclerosis. J Neurol. 2016;263(6):1053–1065. | ||
Banwell B, Giovannoni G, Hawkes C, Lublin F. Editors’ welcome and a working definition for a multiple sclerosis cure. Mult Scler Relat Disord. 2013;2(2):65–67. | ||
Garrison LP Jr, Neumann PJ, Erickson P, Marshall D, Mullins CD. Using real-world data for coverage and payment decisions: the ISPOR Real-World Data Task Force report. Value Health. 2007;10(5):326–335. | ||
Trojano M, Tintore M, Montalban X, et al. Treatment decisions in multiple sclerosis: insights from real-world observational studies. Nat Rev Neurol. 2017;13(2):105–118. | ||
Sonder JM, Balk LJ, van der Linden FA, Bosma LV, Polman CH, Uitdehaag BM. Toward the use of proxy reports for estimating long-term patient-reported outcomes in multiple sclerosis. Mult Scler. 2015;21(14):1865–1871. | ||
Kobelt G, Thompson A, Berg J, Gannedahl M, Eriksson J. New insights into the burden and costs of multiple sclerosis in Europe. Mult Scler. 2017;23(8):1123–1136. | ||
Qizilbash N, Mendez I, Sanchez-de la Rosa R. Benefit-risk analysis of glatiramer acetate for relapsing-remitting and clinically isolated syndrome multiple sclerosis. Clin Ther. 2012;34(1):159–176.e5. | ||
Oliver BJ, Kohli E, Kasper LH. Interferon therapy in relapsing-remitting multiple sclerosis: a systematic review and meta-analysis of the comparative trials. J Neurol Sci. 2011;302(1–2):96–105. | ||
Brandes DW, Callender T, Lathi E, O’Leary S. A review of disease-modifying therapies for MS: maximizing adherence and minimizing adverse events. Curr Med Res Opin. 2009;25(1):77–92. | ||
Menzin J, Caon C, Nichols C, White LA, Friedman M, Pill MW. Narrative review of the literature on adherence to disease-modifying therapies among patients with multiple sclerosis. J Manag Care Pharm. 2013;19(1 Suppl A):S24–S40. | ||
Treadaway K, Cutter G, Salter A, et al. Factors that influence adherence with disease-modifying therapy in MS. J Neurol. 2009;256(4):568–576. | ||
Hofmann M, Brinkmann V, Zerwes HG. FTY720 preferentially depletes naive T cells from peripheral and lymphoid organs. Int Immunopharmacol. 2006;6(13–14):1902–1910. | ||
Kappos L, Radue EW, O’Connor P, et al. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med. 2010;362(5):387–401. | ||
Cohen JA, Barkhof F, Comi G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010;362(5):402–415. | ||
Calabresi PA, Radue EW, Goodin D, et al. Safety and efficacy of fingolimod in patients with relapsing-remitting multiple sclerosis (FREEDOMS II): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Neurol. 2014;13(6):545–556. | ||
Montalban X, Comi G, Antel J, et al. Long-term results from a phase 2 extension study of fingolimod at high and approved dose in relapsing multiple sclerosis. J Neurol. 2015;262(12):2627–2634. | ||
Kappos L, O’Connor P, Radue EW, et al. Long-term effects of fingolimod in multiple sclerosis: the randomized FREEDOMS extension trial. Neurology. 2015;84(15):1582–1591. | ||
Cohen JA, Khatri B, Barkhof F, et al. Long-term (up to 4.5 years) treatment with fingolimod in multiple sclerosis: results from the extension of the randomised TRANSFORMS study. J Neurol Neurosurg Psychiatry. 2016;87(5):468–475. | ||
Hohlfeld R, Kappos L, Tomic D, et al. Early fingolimod treatment improves disease outcomes at 2 and 4 years in patients with relapsing-remitting multiple sclerosis. Neurology. 2017;88(16 Suppl):P6.332. | ||
Cohen J, Tenenbaum N, Bhatt A, Pimentel R, Kappos L. Radiological evidence of the long-term effect of fingolimod treatment in patients with relapsing-remitting multiple sclerosis. Neurology. 2017;88(16 Suppl):P4.409. | ||
Cohen J, Hartung H, Khatri B, et al. Early switch to fingolimod for achieving no evidence of multiple sclerosis disease activity: 8-year analysis of data from the TRANSFORMS study. Neurology. 2017;88(16 Suppl):P4.390. | ||
Ziemssen T, Medin J, Couto CA, Mitchell CR. Multiple sclerosis in the real world: a systematic review of fingolimod as a case study. Autoimmun Rev. 2017;16(4):355–376. | ||
Ziemssen T, Kern R, Cornelissen C. The PANGAEA study design: a prospective, multicenter, non-interventional, long-term study on fingolimod for the treatment of multiple sclerosis in daily practice. BMC Neurol. 2015;15:93. | ||
Ziemssen T, Albrecht H, Haas J, et al. 5 Years effectiveness of fingolimod in daily clinical practice: results of the non-interventional study PANGAEA documenting RRMS patients treated with fingolimod in Germany. Neurology. 2017;88(16 Suppl):P6.345. | ||
Izquierdo G, Damas F, Paramo MD, Ruiz-Pena JL, Navarro G. The real-world effectiveness and safety of fingolimod in relapsing-remitting multiple sclerosis patients: an observational study. PLoS One. 2017;12(4):e0176174. | ||
Kappos L, Cohen J, Collins W, et al. Fingolimod in relapsing multiple sclerosis: an integrated analysis of safety findings. Mult Scler Relat Disord. 2014;3(4):494–504. | ||
Cohen J, Tenenbaum S, Bhat R, Pimentel R, Kappos L. Long-term efficacy and safety of fingolimod in patients with RRMS: 10-year experience from LONGTERMS study. Mult Scler J. 2017;23(3 Suppl):P1879. | ||
Ziemssen T, Albrecht H, Haas J, et al. 5 Years safety experience with fingolimod in real world: results from PANGAEA, a non-interventional study of RRMS patients treated in Germany. Mult Scler J. 2017;23(3 Suppl):P1192. | ||
Lebrun-Frenay C, Papeix C, Kobelt G, et al. Long-term efficacy, safety, tolerability and quality of life with fingolimod treatment in patients with multiple sclerosis in real-world settings in France: VIRGILE two-year results. Mult Scler J. 2017;23(3 Suppl):EP1716. | ||
Killestein J, Vennegoor A, van Golde AE, Bourez RL, Wijlens ML, Wattjes MP. PML-IRIS during fingolimod diagnosed after natalizumab discontinuation. Case Rep Neurol Med. 2014;2014:307872. | ||
Achtnichts L, Obreja O, Conen A, Fux CA, Nedeltchev K. Cryptococcal meningoencephalitis in a patient with multiple sclerosis treated with fingolimod. JAMA Neurol. 2015;72(10):1203–1205. | ||
Forrestel AK, Modi BG, Longworth S, Wilck MB, Micheletti RG. Primary cutaneous Cryptococcus in a patient with multiple sclerosis treated with fingolimod. JAMA Neurol. 2016;73(3):355–356. | ||
Seto H, Nishimura M, Minamiji K, et al. Disseminated cryptococcosis in a 63-year-old patient with multiple sclerosis treated with fingolimod. Intern Med. 2016;55(22):3383–3386. | ||
Hagiya H, Yoshida H, Shimizu M, et al. Herpes zoster laryngitis in a patient treated with fingolimod. J Infect Chemother. 2016;22(12):830–832. | ||
Pfender N, Jelcic I, Linnebank M, Schwarz U, Martin R. Reactivation of herpesvirus under fingolimod: a case of severe herpes simplex encephalitis. Neurology. 2015;84(23):2377–2378. | ||
Issa NP, Hentati A. VZV encephalitis that developed in an immunized patient during fingolimod therapy. Neurology. 2015;84(1):99–100. | ||
Kawiorski MM, Viedma-Guiard E, Costa-Frossard L, Corral I. Polydermatomal perineal and gluteal herpes zoster infection in a patient on fingolimod treatment. Enferm Infecc Microbiol Clin. 2015;33(2):138–139. | ||
Arvin AM, Wolinsky JS, Kappos L, et al. Varicella-zoster virus infections in patients treated with fingolimod: risk assessment and consensus recommendations for management. JAMA Neurol. 2015;72(1):31–39. | ||
Subei AM, Cohen JA. Sphingosine 1-phosphate receptor modulators in multiple sclerosis. CNS Drugs. 2015;29(7):565–575. | ||
Gold R, Comi G, Palace J, et al. Assessment of cardiac safety during fingolimod treatment initiation in a real-world relapsing multiple sclerosis population: a phase 3B, open-label study. J Neurol. 2014;261(2):267–276. | ||
Limmroth V, Haverkamp W, Dechend R, et al. First dose effects of fingolimod: final results of an in-depth ECG and Holter study in 6,998 German RRMS patients. Mult Scler J. 2017;23(3 Suppl):P764. | ||
Bermel RA, Hashmonay R, Meng X, et al. Fingolimod first-dose effects in patients with relapsing multiple sclerosis concomitantly receiving selective serotonin-reuptake inhibitors. Mult Scler Relat Disord. 2015;4(3):273–280. | ||
Yoshii F, Moriya Y, Ohnuki T, Ryo M, Takahashi W. Neurological safety of fingolimod: an updated review. Clin Exp Neuroimmunol. 2017; 8(3):233–243. | ||
Fox E, Edwards K, Burch G, et al. Outcomes of switching directly to oral fingolimod from injectable therapies: results of the randomized, open-label, multicenter, Evaluate Patient OutComes (EPOC) study in relapsing multiple sclerosis. Mult Scler Relat Disord. 2014;3(5):607–619. | ||
Ziemssen T, Albrecht H, Haas J, et al. 5 Years effectiveness of fingolimod in daily clinical practice: results of the non-interventional study PANGAEA. Mult Scler J. 2017;23(3 Suppl):P745. | ||
Achiron A, Aref H, Inshasi J, et al. Effectiveness, safety and health-related quality of life of multiple sclerosis patients treated with fingolimod: results from a 12-month, real-world, observational PERFORMS study in the Middle East. BMC Neurol. 2017;17(1):150. | ||
Papeix C, Lebrun-Frenay C, Leray E, et al. Long-term efficacy, safety, tolerability and quality of life with fingolimod treatment in patients with multiple sclerosis in real-world settings in France: VIRGILE one-year results. Mult Scler J. 2016;22(3 Suppl):P1234. | ||
Kalincik T, Butzkueven H. Observational data: understanding the real MS world. Mult Scler. 2016;22(13):1642–1648. | ||
Flachenecker P, Buckow K, Pugliatti M, et al. Multiple sclerosis registries in Europe: results of a systematic survey. Mult Scler. 2014;20(11):1523–1532. | ||
Weinstock-Guttman B, Medin J, Khan N, et al. Assessing no evidence of disease activity status in patients with relapsing-remitting multiple sclerosis receiving fingolimod: results from a longitudinal, multicenter, real-world study. Neurology. 2017;88(16 Suppl):P4.388. | ||
Ziemssen T, Albrecht H, Haas J, et al. 5 Years safety of fingolimod in real world: first results from PANGAEA, a non-interventional study of RRMS patients treated with fingolimod, on safety and adherence after 5 years of fingolimod in daily clinical practice. Neurology. 2017;88(16 Suppl):P5.365. | ||
Fragoso YD. Multiple sclerosis treatment with fingolimod: profile of non-cardiologic adverse events. Acta Neurol Belg. 2017;117(4):821–827. | ||
Ziemssen T, Kern R, Thomas K. Multiple sclerosis: clinical profiling and data collection as prerequisite for personalized medicine approach. BMC Neurol. 2016;16:124. | ||
Giovannoni G, Tomic D, Bright JR, Havrdová E. “No evident disease activity”: the use of combined assessments in the management of patients with multiple sclerosis. Mult Scler. 2017;23(9):1179–1187. | ||
van Pesch V, BELTRIMS: First results from a Belgian registry for treatments in Multiple Sclerosis. Newsletter of the Belgian Charcot Foundation. 2017;42:5. Avaialble from: http://www.fondation-charcot.org/en/newsletters/35/ms-research-beltrims-registry-fund-charcot-belgian. Accessed November 22, 2017. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.