Back to Journals » OncoTargets and Therapy » Volume 9
Long-term results of definitive concurrent chemoradiotherapy using S-1 in the treatment of geriatric patients with esophageal cancer
Authors Lv S, Fang M, Yang J, Zhan W, Jia Y, Xu H ![]() , Song T
, Song T
Received 2 March 2016
Accepted for publication 6 July 2016
Published 6 September 2016 Volume 2016:9 Pages 5389—5397
DOI https://doi.org/10.2147/OTT.S107668
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Min Li
Shiliang Lv, Min Fang, Jia Yang, Wenming Zhan, Yongshi Jia, Hong’en Xu, Tao Song
Department of Radiotherapy, Zhejiang Provincial People’s Hospital, Hangzhou, Zhejiang, People’s Republic of China
Objective: The aim of this study was to investigate the efficiency and safety of using S-1 as monotherapy and maintenance therapy combined with definitive concurrent radiotherapy for elderly patients with esophageal cancer.
Patients and methods: From January 2009 to December 2010, 68 elderly patients were included. Radiotherapy was delivered with a daily fraction of 1.8–2.0 Gy to a total radiation dose of 54.0–60.0 Gy. Preplanned concurrent S-1 (80 mg/m2/d) was given on days 1–14, every 3 weeks. After concurrent chemoradiotherapy, maintenance S-1 was repeated up to four cycles.
Results: The median age of the enrolled patients was 76 years (range: 70–88 years), and the clinical stages were stage I (two patients), stage II (24 patients), stage III (28 patients), and stage IV (14 patients). A total of 51 (75.0%) patients finished treatment on schedule, with a median of five cycles of S-1, in which 35 (51.5%) patients achieved complete response. The median follow-up time was 42.7 months, and the median overall survival (OS) and progression-free survival (PFS) times were 25.7 months and 21.5 months, respectively. The 1-year, 3-year, and 5-year OS and PFS rates were 70.6%, 41.8%, and 25.9% and 68.1%, 32.9%, and 15.9%, respectively. Grade ≥3 neutropenia and leukopenia were found in 14 patients and 13 patients, respectively. The most common nonhematologic toxicity was esophagitis including six patients and one patient with grades 3 and 4, respectively. Multivariate analysis revealed that cycles of S-1 and complete response were strong factors for OS and PFS.
Conclusion: For geriatric patients with esophageal cancer, S-1 as monotherapy and maintenance chemotherapy in combination with definitive concurrent radiation therapy yielded satisfactory survival outcomes with tolerable toxicities. More studies are highly warranted to further clarify this issue.
Keywords: esophageal cancer, geriatric, chemoradiotherapy, S-1, survival
Introduction
Despite the great clinical improvement in the treatment of patients with various malignancies, esophageal cancer is still one of the most significant global health problems. The incidence is increasing in the People’s Republic of China, and the 5-year overall survival (OS) rate for the whole stages is dismal with no better than a mere 20%–30%.1–3 Traditionally, esophagectomy plays the pivotal role in the treatment of esophageal cancer, especially for the early-stage patients. However, less surgery was performed for geriatric patients because of safety consideration. A series of reports have revealed that patients older than 70 years have a relatively high postoperative mortality rate (4.5%–60%).4–6 Definitive concurrent chemoradiotherapy (CCRT) has also been considered to be the standard treatment option for patients with localized or locally advanced esophageal cancer who refuse surgery or have no indication for esophagectomy, for which geriatric patients constitute a great proportion as indicated by the Radiation Therapy Oncology Group (RTOG) 85-01 trial.7 5-Fluorouracil (5-Fu) combined with cisplatin has also been confirmed as a standard chemotherapy regimen since then. However, the efficacy of this regimen was only ~25%–35%, and the median survival time was no better than 16 months in patients with advanced esophageal cancer. Thus, exploring other potent radiosensitizers and more tolerable chemotherapy regimens in geriatric patients are gaining momentum.
As an oral pyrimidine fluoride-derived anticancer agent, S-1 combines 5-Fu prodrug (tegafur) and two modulators of 5-Fu metabolism, gimeracil (CDHP) and oteracil.8 S-1 has been widely used in a variety of solid tumors, including colorectal cancer, non-small-cell lung cancer, head and neck cancers, and gastric cancer in Japan and the People’s Republic of China. Compared with tegafur-uracil (UFT), another oral fluoropyrimidine derivative without CDHP, S-1 has been suggested to be more effective on radiosensitivity for human non-small-cell lung cancer xenografts in mice.9 As revealed by clinical studies, S-1 as monotherapy achieved an objective response rate of 34.1% in those patients with progressive or recurrent head and neck cancers,10 while for stage II/III esophageal cancer, S-1 combined with cisplatin led to a complete response (CR) rate of 59.5% (90% confidence interval [CI], 44.6%–73.1%) with favorable toxicity profile.11 To the best of our knowledge, there are few studies regarding the regimen of CCRT using S-1 as monotherapy and maintenance chemotherapy for patients with geriatric esophageal cancer.
Based on these backgrounds, we conducted this study to evaluate the feasibility and efficiency of CCRT with S-1 for elderly patients with esophageal cancer in our institute. We defined an elderly population as subjects aged ≥70 years according to a series of recent studies.12–15
Patients and methods
Ethics statement
The institutional review board of Zhejiang Provincial People’s Hospital approved this study, and written informed consent was obtained from all patients before treatment initiation.
Patients’ workup
Between January 2009 and December 2010, 172 patients with newly diagnosed esophageal cancer who underwent CCRT at the cancer center of Zhejiang Provincial People’s Hospital were screened. Among them, 68 patients aged >70 years and using S-1 as monotherapy and maintenance chemotherapy were retrospectively studied. The main reasons for contraindication of surgery were as follows: rejection of surgery (n=26), advanced age (n=19), tumor location (n=14), and severe comorbidity (n=9).
The inclusion criteria in our study were as follows: 1) histologically proved esophageal cancer; 2) clinical stages according to the 2002 (Version 6.0) American Joint Committee on Cancer staging system; 3) Eastern Cooperative Oncology Group performance status (ECOG PS) 0–2 (for patients with a PS score of 2, CCRT was performed with cautious after being discussed by the multidisciplinary treatment team); 4) no severe bone marrow, hepatic, renal, respiratory, and cardiac dysfunction; and 5) no prior chest chemoradiotherapy received. Patient’s baseline characteristics (dysphagia, weight loss, albumin, and comorbidities) were also collected. Dysphagia degree was evaluated with the Atkinson score,16 while the Charlson score was adopted to analyze the comorbidities of patients, which was based on 19 medical conditions.17
Treatment schedule and dose modification
Typically, the standard S-1 dose was calculated according to the patient’s body surface area with 60–80 mg/m2/d for xanthoderm. One treatment course consisted of consecutive twice daily administration for 4 weeks followed by a period of rest for 2 weeks. However, S-1-related toxicities were suggested to appear ~14–21 days after the initiation of treatment. Further research assessed a new treatment scheme with 2 weeks dosing administration and then a 7-day drug-free interval. This treatment administration was associated with less adverse events and similar treatment response.18 Considering the feasibility of this new treatment drug at that time and accommodating the effectiveness, patients received S-1 with a dose of 80 mg/m2/d twice daily for 2 weeks in our cancer institute.
Radiotherapy was given concurrently on the first day of the fist cycle of S-1 and was delivered with 6–10 Mv X-ray accelerators using the three-dimensional conformal technique. Before radiation, patients were positioned in an immobilization device, and a planning enhanced computed tomography (CT) scan was made. The gross tumor volume included the primary tumor and any enlarged lymph nodes. For regional lymph nodes, the supraclavicular, upper mediastinal, and subcarinal lymph nodes were irradiated for proximal esophagus. The mediastinal and perigastric lymph nodes were included for tumors of the middle or lower esophagus, to which the celiac lymph nodes were included for lower segment cancers. The clinical target volume (CTV) was defined as the gross tumor volume and a 3 cm margin in the superior and inferior directions, 6 mm in the left and right directions, and 6 mm in the anterior and posterior directions. The planning target volume was defined as the CTV and a 5–10 mm margin around the CTV. The total dose was 54.0–60.0 Gy, which was given in 30–33 fractions of 1.8–2.0 Gy once-daily fractions for 5 d/wk. Patients who achieved a response greater than stable disease received maintenance oral S-1 until disease progression, severe side effects, or patient refusal up to a total of six cycles.
The drug dosage was adjusted according to the acute toxicities occurring in the first cycle. S-1 was reduced to 70 mg/m2/d in the following courses: grade 3 neutropenia with infection, or grade 4 leucocytopenia, or grade ≥3 thrombocytopenia, or grade 4 mucositis. Granulocyte colony-stimulating factor was used to treat for the occurrence of febrile neutropenia. Irradiation was suspended for patients with severe esophagitis (grade ≥3), neutropenia (grade 3) with fever, or grade 4 leucocytopenia. Radiation therapy was restarted when toxicities recovered to grade ≤2. The dosage of S-1 was reduced again to 60 mg/m2/d if grade 4 hematological toxicities or grade ≥3 infections still occurred after reducing to 70 mg/m2/d. If patients received more than two dose reductions or there was a treatment delay of >2 weeks because of treatment-related toxicities, S-1 would be terminated.
Evaluation and follow-up
All patients were hospitalized and monitored weekly during the CCRT course for acute treatment toxicity. Toxicity of the treatment was assessed based on the National Cancer Institute Common Terminology Criteria for Adverse Events v3.0. We evaluated clinical response of the patients with the Response Evaluation Criteria in Solid Tumors 2–3 weeks after the completion of CCRT. Follow-up was regularly carried out every 1 month in the first half of 1 year, every 3 months in the second year, and every 6 months after 2 years. Moreover, telephone follow-up was required once a week during the maintenance S-1 treatment to make sure these patients intake S-1 certainly. Any recurrent disease, locoregional and/or distant, was defined as treatment failure. The failure models were evaluated using posttreatment esophagogram, endoscopy, CT, or integrated positron emission tomography/CT (if available) scans. And relevant data were compared with the original CT-based radiation treatment plans.
Statistical analysis
Statistical analyses were conducted using Statistical Package for the Social Sciences 18.0 (SPSS Inc., Chicago, IL, USA). OS was determined as the time (in months) between the first day of therapy and the last follow-up or the date of death. Progression-free survival (PFS) was defined as the internal between the data of CCRT initiation and the data of documented failure or the date of the last follow-up for those remaining without any progressive disease. Kaplan–Meier method was applied for the survival curves. Univariate and multivariate Cox regression analyses were generated to estimate the hazard ratio (HR) with 95% CI for OS and PFS. Significant risk factors identified in univariate analysis were subjected to a multivariate analysis with adjustment for the relevant covariates. P-value <0.05 was considered statistically significant.
Results
Patients and tumor characteristics
Sixty-eight patients were finally included in this analysis. Clinical baseline characteristics are detailed in Table 1. The median age of the patients was 76 years, ranging from 70 years to 88 years old. Fifty-nine patients were male, and nine patients were female. Forty-two (61.8%) patients had a good ECOG PS score (0–1). A total of 38.2% of patients had a severe dysphagia of ≥2, and 30.9% of patients had an initial weight loss of >10% in 6 months. The median Charlson score was 3, and the most common comorbidity for this cohort was hypertension (n=30). Diabetic (35.3%) and peripheral vascular or cerebrovascular disease (14.7%) ranked the second and third places in the data, respectively.
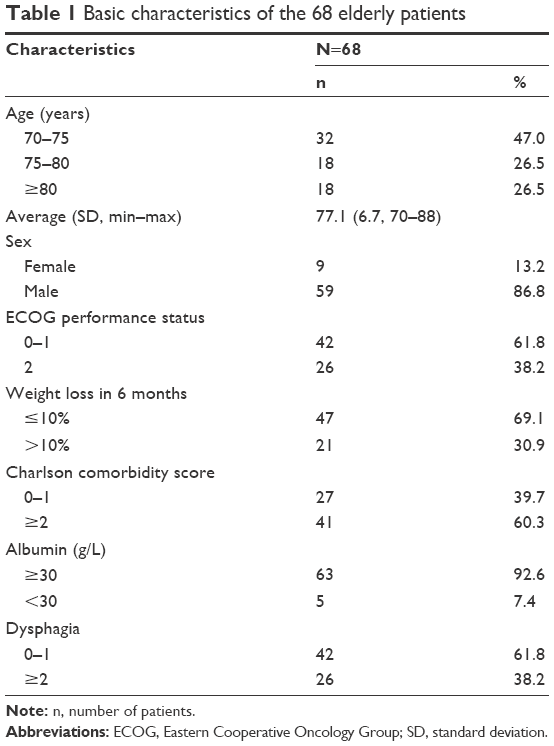 | Table 1 Basic characteristics of the 68 elderly patients |
Detailed tumor characteristics before treatment are shown in Table 2. There were mainly T3–4 stage tumors (80.9%) and squamous cell carcinoma (n=63, 92.6%). A total of 61.8% (n=42) of patients were recorded with stages III and IV and the locations of the tumors were as follows: upper third (20.6%), middle third (47.1%), and lower third (16.2%). Majority of tumors were >5 cm in length (58.8%).
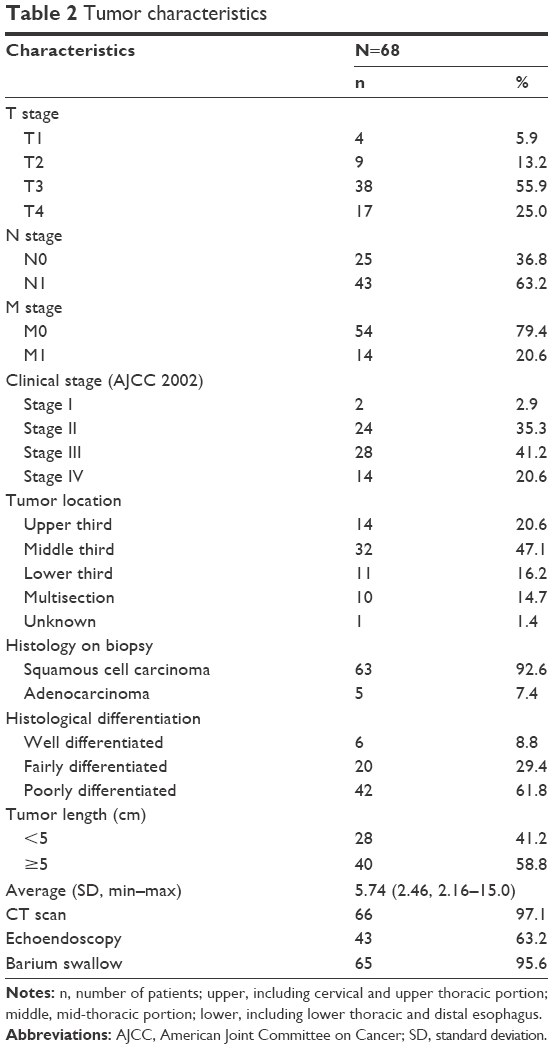 | Table 2 Tumor characteristics |
Treatment compliance and tumor response to CCRT
All patients completed the first cycle of S-1 as planned. One patient refused the second cycle of chemotherapy for occurring grade 4 neutropenia, and this patient also gave up radiation. Eight (11.8%) patients received a reduced dose of S-1 in the second cycle of chemotherapy because of hematological toxicity. A total of 56 (82.4%) patients completed radiotherapy for a total dose of 60 Gy, including five patients with radiation delay. A total of 51 (75.0%) patients finished CCRT on schedule, including 48 (70.6%) patients without changing treatment regimen. Among all patients, the median cycle of S-1 was 5 with a total of 343 cycles. A total of 14 patients completed four cycles of S-1, 14 patients finished five cycles, and 34 patients finished six cycles of chemotherapy. The main reasons for refusing additional cycles of S-1 included intolerable toxic reactions and progression diseases during follow-up time.
All patients received response evaluation, which was conducted after 2–3 weeks following the last radiotherapy session. Thirty-five patients (51.5%) achieved CR, while the overall response rate (ORR; CR + PR) was 88.2%. Meanwhile, three patients had progression diseases. At the end of the last follow-up by December 31, 2015, 55 patients experienced treatment failures. The recurrent sites were as follows: 37 for locoregional and residual disease, eleven for distant metastasis, and seven for both sites.
Acute and late treatment-related toxicities
The acute toxicity profile related to the treatment was listed in Table 3. Toxicity reactions were assessed in all 68 patients. The most common hematologic toxicity during CCRT was grade 4 neutropenia and leucocytopenia in two (2.9%) patients and five (7.4%) patients, respectively. Grade 3 neutropenia and leucocytopenia were seen in twelve (17.6%) patients and eight (11.8%) patients, respectively, and among these patients, 13 patients were aged >75 years. Most patients recovered by using granulocyte colony-stimulating factor. There were three (4.4%) patients with grade 3 thrombocytopenia and two (2.9%) patients with grade 3 anemias. A total of 49 (72.1%) patients received all grade esophagitis including seven patients experiencing grades 3 and 4 (six patients for grade 3 and one patient for grade 4). Other grade 3 nonhematologic toxicities during CCRT included dysphagia (5.9%), nausea/vomiting (7.4%), and fatigue (4.4%). During the maintenance chemotherapy, neutropenia was observed to be the most common grade ≥3 hematologic toxicity (14.7%), while there were only six patients with severe leucocytopenia. Five (7.4%) patients still had grade ≥3 esophagitis during the maintenance treatment course including one patient with grade 4. Nausea/vomiting (5.9%) and dysphagia (4.4%) ranked the second and third places, respectively. There were no patients who died of acute treatment-related toxicities. In terms of late toxicities, ten (14.7%) patients received all grade esophageal stenosis and seven (10.3%) patients experienced radiation-related pneumonitis. Thus, toxicities of this regimen appeared to be well tolerated.
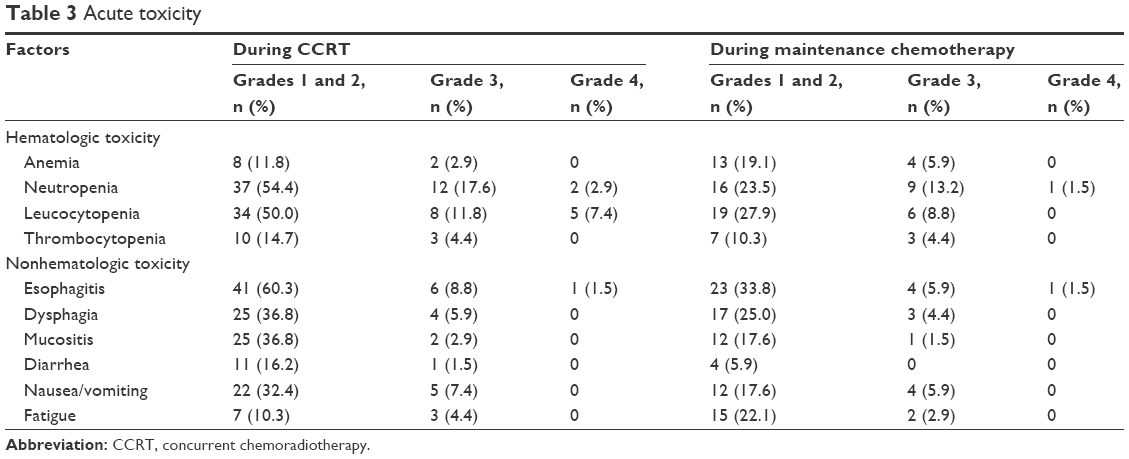 | Table 3 Acute toxicity |
Survival and prognostic analysis
The median follow-up period was 42.7 months (range, 1.9–66.3 months), and the median OS time was 25.7 months (95% CI, 19.7–31.6). The 1-year and 3-year OS rates were 70.6% and 41.8%, respectively, while the 5-year OS rate was 25.9%. At the last regular follow-up, six patients survived >60 months (including four patients without any progression). For patients older than 75 years, the 1-year and 3-year OS rates were 72.4% and 47.6%, respectively. The median PFS was 21.5 months (95% CI, 16.7–26.2), and 1-year, 3-year, and 5-year PFS rates were 68.1%, 32.9%, and 15.9%, respectively (Figure 1). For patients older than 75 years, the 1-year and 3-year PFS rates were 67.9% and 38.9%, respectively.
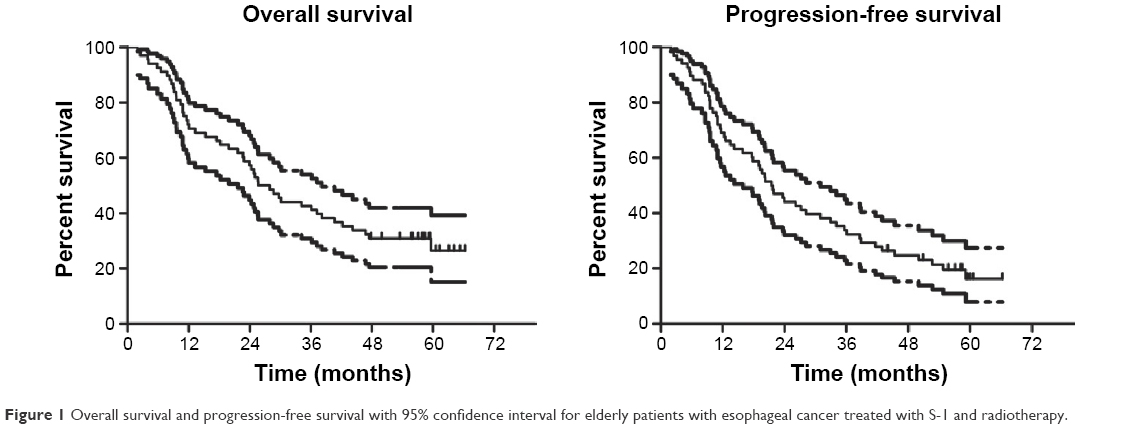 | Figure 1 Overall survival and progression-free survival with 95% confidence interval for elderly patients with esophageal cancer treated with S-1 and radiotherapy. |
We then conducted univariate analyses to identify the association between specific variable and survival of the patients, as shown in Table 4. Several covariates were indicated to be significantly related to OS: ECOG PS (HR 2.185, P=0.007), Charlson comorbidity score (HR 1.886, P=0.039), T stage (HR 2.056, P=0.001), N stage (HR 3.432, P=0.000), M stage (HR 3.880, P<0.001), clinical stage (HR 2.909, P<0.001), tumor length (HR 1.902, P=0.037), dysphagia (HR 1.783, P=0.048), clinical response (HR 2.127, P=0.010), and cycles of S-1 (HR 0.196, P<0.001). The variables significantly associated with the PFS were as follows: ECOG PS (HR 2.102, P=0.007), T stage (HR 1.714, P=0.004), N stage (HR 3.152, P<0.001), M stage (HR 3.746, P<0.001), clinical stage (HR 2.489, P<0.001), cycles of S-1 (HR 0.256, P<0.001), and clinical response (HR 2.081, P=0.007).
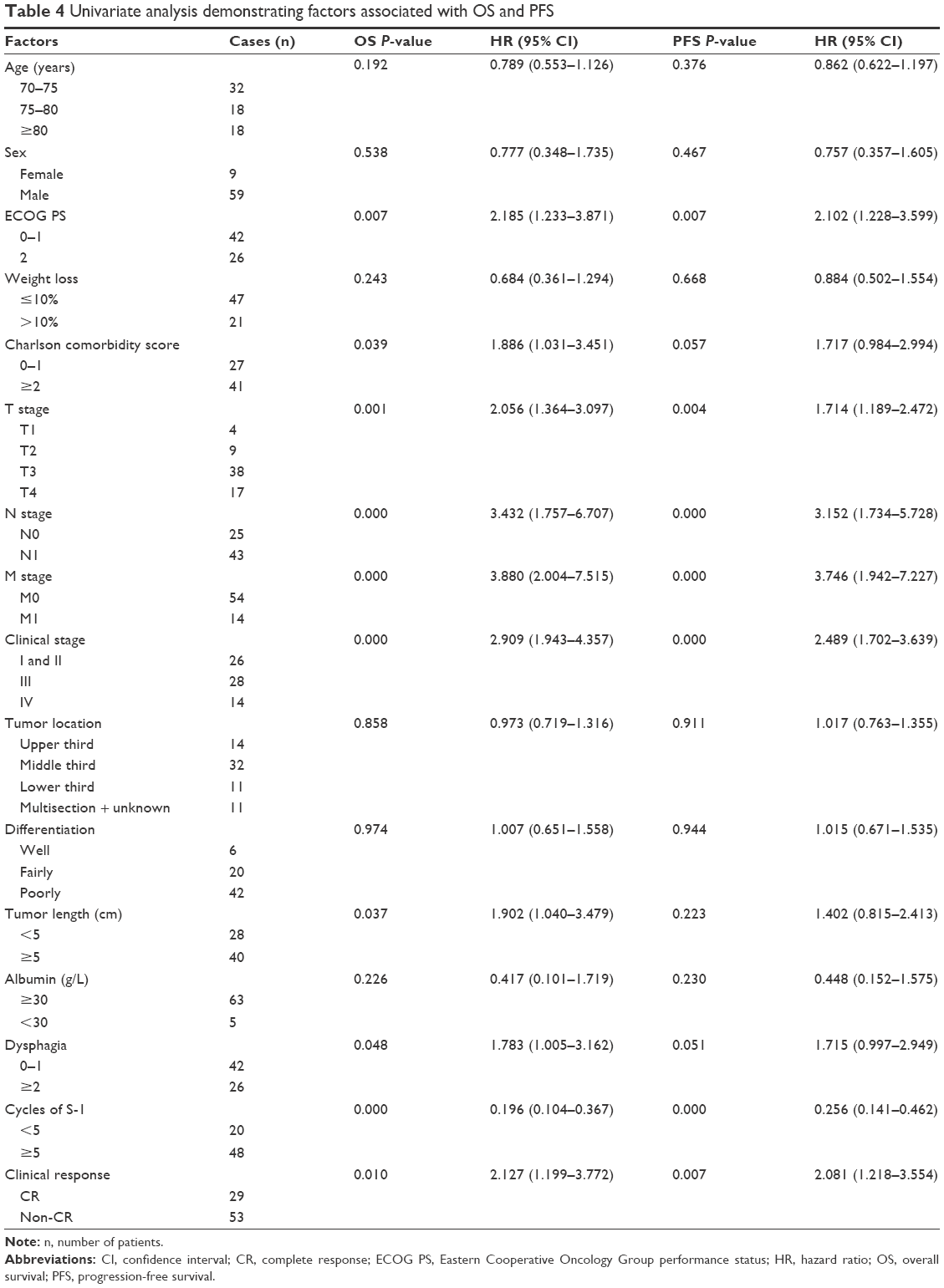 | Table 4 Univariate analysis demonstrating factors associated with OS and PFS |
Multivariate analysis was further performed to explore the possible independent prognostic variables, and the covariates that were significant in the univariate analysis were included. As suggested, the cycles of S-1 (HR 0.305, P=0.004 and HR 0.275, P<0.001, respectively) and clinical response (HR 2.165, P=0.023 and HR 1.872, P=0.040, respectively) were independent prognostic factors for OS and PFS in elderly patients with esophageal cancer (Table 5).
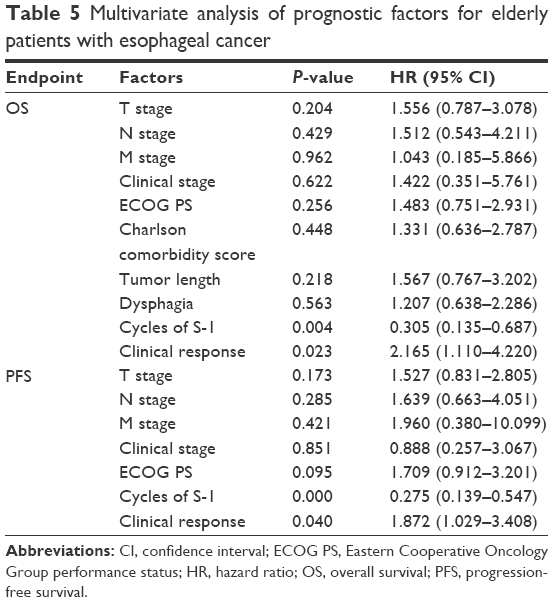 | Table 5 Multivariate analysis of prognostic factors for elderly patients with esophageal cancer |
Discussion
Increasing life expectancy has led to more elderly patients with cancer being referred for treatment, and it must be recognized that they could be acquired invaluable benefits if nonpalliative care could succeed to increasing their lifetime, which would just be an advantage from a broad range of socioeconomic fields, including medical progress. But the fact is that elderly patients with esophageal cancer were often underrepresented in most clinical trials. Traditionally, geriatric patients were considered to have less reserve of body function and more comorbidities compared with younger patients, and CCRT offers us an opportunity to have comparable clinical outcomes with less treatment-related toxicities compared with surgery. Based on the landmark RTOG 85-01 trial,7 5-Fu with cisplatin as a combined treatment regimen has been suggested as the standard radiosensitizers in esophageal cancer. However, in the CCRT arm of the RTOG 85-01 trial, there was one treatment-related death out of the 61 patients occurred, while severe (grade 3) and fatal (grade 4) side effects were observed in 44% and 20% of the included patients, respectively. Moreover, only 26% of elderly patients were enrolled; thus, the suitability of CCRT for the elderly remained unclear. Subsequently, studies have been performed to investigate whether 5-Fu/cisplatin and radiotherapy were suitable for elderly patients, and the results revealed that the proportion of moderate-to-severe side effects and treatment-related deaths for elderly patients was relatively high. Tougeron et al15 retrospectively reviewed 109 elderly patients with nonmetastatic esophageal cancer who mainly treated with 5-Fu/cisplatin with radiotherapy (50–55 Gy). In this study, the 2-year OS rate was 35.5% and grade ≥3 adverse events were observed in 23.8% patients.15 In another retrospective analysis, 22 patients older than 75 years received CCRT consisting of two cycles of platinum/5-Fu with radiation therapy (50–50.4 Gy) and additional chemotherapy when appropriate. The 3-year OS and PFS rates were reported to be 33.3% and 25.9%, respectively. However, there were up to four suspecting treatment-related deaths, and the proportion of patients who had fatal (grade 4) thrombocytopenia and leucocytopenia was 18% and 14%, respectively.19 These studies suggested a possible role of CCRT for elderly esophageal cancer. However, optimal treatment combination and protocol for chemotherapy still needed extensive studies.
As aforesaid, S-1 could inhibit dihydropyrimidine dehydrogenase activity and thus increase therapeutic plasma 5-Fu concentrations, which reduced gastrointestinal side effects among the dose-limiting toxicities of 5-Fu.20 Of the 68 patients included in this study, 75.0% of patients finished CCRT on schedule, including 48 (70.6%) patients without changing treatment regimen. The full dose of CCRT completion rate was much higher than RTOG 85-01 trial, in which all cycles of CCRT could be administered as planned in 33 of the 61 (54%) patients.7 S-1 was also considered to have several advantages over 5-Fu. Pharmacokinetic studies have proven that the half-life of plasma concentrations of 5-Fu after oral S-1 was significantly prolonged compared with that of 5-Fu after intravenous administration.21 In addition, S-1 could be given on a daily basis, which is active for fractionated radiotherapy and is quite convenient for elderly patients.22 The completion rate in this study was also in-line with our recent report which used paclitaxel/cisplatin and 60 Gy radiotherapy for elderly patients with esophageal cancer. In that study, 80.5% of patients completed CCRT on schedule with 67.1% of patients without changing treatment plan.23
In general, favorable complications related to this regimen supported that S-1 with radiotherapy was a promising treatment combination for the geriatric patients. In 2015, Tahara et al11 reported their Phase I/II clinical trial with CCRT using S-1 (60 mg/m2/d in Phase II study) and cisplatin (75 mg/m2 on day 1) to investigate the efficacy and safety for stage II/III esophageal cancer. Their trial showed that the most frequent grade ≥3 toxicity in Phase II trial included leukopenia (57.9%) and neutropenia (50%), while there was no treatment-related death. Although they did not meet the primary endpoint, in respect of the CR rate, authors concluded that the combination of S-1 and cisplatin showed an acceptable toxicity and favorable survival outcomes.11 In 2008, Cho et al20 also conducted a prospective study for locally advanced or metastatic esophageal squamous cell carcinoma. Patients were assigned to receive S-1 (70 mg/m2/d for 2 weeks) and cisplatin (70 mg/m2 on day 1) every 3 weeks with concurrent 54.0 Gy radiotherapy; maintenance chemotherapy was repeated up to six cycles after CCRT. Results showed that the major hematological toxicity was neutropenia and asthenia and vomiting (mostly of grades 1 and 2) appeared to be the main nonhematological toxicities. They also suggested that CCRT with S-1 and cisplatin might be a promising nonsurgical treatment strategy for patients with esophageal cancer.20 Both of the enrolled patients in the above two studies were relatively young patients (mean ages were 62 years and 65 years, respectively), our results showed favorable toxic reactions with 13 (19.2%) grade ≥3 leukopenia and 14 (20.5%) neutropenia observed during CCRT and less frequent myelosuppression in maintenance chemotherapy.
Our findings also showed that in appropriately selected elderly patients, the potential long-term survival benefits were associated with the treatment regimen. Iwase et al24 reported their long-term Phase II trial, which also investigated CCRT comprising a 30 Gy radiotherapy over 3 weeks and S-1 and cisplatin for locally advanced esophageal cancer in 2013. The patients received oral S-1 at a dose of 80 mg/m2/d for 14 days and a 24-hour cisplatin infusion on day 8 at a dose of 70 mg/m2, with an identical course administered after a 2-week break. Their results showed a 1-year OS rate of 78.2% and 5-year OS rate of 29.8%, and the median OS time was 2.3 years, which was in-line with our study.24 Another retrospective study evaluated the efficacy and safety of sequential chemoradiotherapy or CCRT with capecitabine and cisplatin for geriatric patients with esophageal squamous cell carcinoma;25 they reported a median PFS of 19.7 months, and the 3-year PFS rate was 34.1%, while the median OS was 33.6 months with a 3-year OS rate of 46.1%. These data were also comparable with our report.
Clinical response evaluation based on Response Evaluation Criteria in Solid Tumors system showed that CR and ORR in this study was 51.5% and 88.2%, respectively. While comparing with cisplatin-based chemotherapy and 60 Gy CCRT, results in our recent systemic review and pooled analysis, which enrolled 1,915 patients from 26 clinical studies, also showed that the CR and ORR were 50.7% and 86.2%, respectively.26 Iwase et al24 reported that the ORR rate in patients receiving radiotherapy and S-1/cisplatin was 89.7% with a CR of 61.2% and a PR of 28.5%. Furthermore, we confirmed that age was not significantly associated with survival of elderly patients with esophageal cancer, while the clinical response rate of CR and cycles of S-1 were strong prognostic factors for elderly patients receiving combined therapy of S-1 and radiation, as shown in Tables 4 and 5. These findings were consistent with the conclusions of a series of studies.15,27,28
This study is subjected to some limitations. One pitfall of this study is the nature of the retrospective design and some potential and unmeasured factors that might have influences on the final results. Besides, another drawback of this study was the lack of available Phase I data focusing on the application of S-1 as monotherapy and maintenance chemotherapy combined with radiotherapy for elderly patients with esophageal cancer in the literature, but we noticed that a completed Phase I clinical trial (NCT 01175447) had also set its initial dosage of S-1 as 80 mg/m2/d, and we are still waiting for its final reports.
Conclusion
Our results showed the possibility of a convenient and feasible regimen of CCRT for geriatric esophageal cancer with promising survival outcomes and acceptable toxicities. This treatment regimen should be validated in future prospective clinical studies.
Acknowledgments
No funding source was supported this study. We thank Xiaodong Liang for his help with translation and proofreading. SL and MF are the cofirst authors.
Disclosure
The authors report no conflicts of interest in this work.
References
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014;64(1):9–29. | ||
Bray F, Jemal A, Grey N, Ferlay J, Forman D. Global cancer transitions according to the Human Development Index (2008–2030): a population-based study. Lancet Oncol. 2012;13(8):790–801. | ||
Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. | ||
Chino O, Makuuchi H, Machimura T, et al. Treatment of esophageal cancer in patients over 80 years old. Surg Today. 1997;27(1):9–16. | ||
Mohansingh MP. Mortality of oesophagal surgery in the elderly. Br J Surg. 1976;63(8):579–580. | ||
Poon RT, Law SY, Chu KM, Branicki FJ, Wong J. Esophagectomy for carcinoma of the esophagus in the elderly: results of current surgical management. Ann Surg. 1998;227(3):357–364. | ||
Cooper JS, Guo MD, Herskovic A, et al. Chemoradiotherapy of locally advanced esophageal cancer: long-term follow-up of a prospective randomized trial (RTOG 85-01). Radiation Therapy Oncology Group. JAMA. 1999;281(17):1623–1627. | ||
Shirasaka T, Nakano K, Takechi T, et al. Antitumor activity of 1 M tegafur-0.4 M 5-chloro-2,4-dihydroxypyridine-1 M potassium oxonate (S-1) against human colon carcinoma orthotopically implanted into nude rats. Cancer Res. 1996;56(11):2602–2606. | ||
Fukushima M, Sakamoto K, Sakata M, Nakagawa F, Saito H, Sakata Y. Gimeracil, a component of S-1, may enhance the antitumor activity of X-ray irradiation in human cancer xenograft models in vivo. Oncol Rep. 2010;24(5):1307–1313. | ||
Inuyama Y, Kida A, Tsukuda M, Kohno N, Satake B, Group SCS. [Late phase II study of S-1 in patients with advanced head and neck cancer]. Gan To Kagaku Ryoho. 2001;28(10):1381–1390. In Japanese. | ||
Tahara M, Fuse N, Mizusawa J, et al. Phase I/II trial of chemoradiotherapy with concurrent S-1 and cisplatin for clinical stage II/III esophageal carcinoma (JCOG 0604). Cancer Sci. 2015;106(10):1414–1420. | ||
Nallapareddy S, Wilding GE, Yang G, Iyer R, Javle M. Chemoradiation is a tolerable therapy for older adults with esophageal cancer. Anticancer Res. 2005;25(4):3055–3060. | ||
Takeuchi S, Ohtsu A, Doi T, et al. A retrospective study of definitive chemoradiotherapy for elderly patients with esophageal cancer. Am J Clin Oncol. 2007;30(6):607–611. | ||
Feng JF, Huang Y, Chen L, Zhao Q. Prognostic analysis of esophageal cancer in elderly patients: metastatic lymph node ratio versus 2010 AJCC classification by lymph nodes. World J Surg Oncol. 2013;11:162. | ||
Tougeron D, Di Fiore F, Thureau S, et al. Safety and outcome of definitive chemoradiotherapy in elderly patients with oesophageal cancer. Br J Cancer. 2008;99(10):1586–1592. | ||
Atkinson M. Diseases of the alimentary system. Dysphagia. Br Med J. 1977;1(6053):91–93. | ||
Charlson ME, Sax FL, MacKenzie CR, Braham RL, Fields SD, Douglas RG Jr. Morbidity during hospitalization: can we predict it? J Chronic Dis. 1987;40(7):705–712. | ||
Kimura Y, Kikkawa N, Iijima S, et al. A new regimen for S-1 therapy aiming at adverse reaction mitigation and prolonged medication by introducing a 1-week drug-free interval after each 2-week dosing session: efficacy and feasibility in clinical practice. Gastric Cancer. 2003;6(suppl 1):34–39. | ||
Wakui R, Yamashita H, Okuma K, et al. Esophageal cancer: definitive chemoradiotherapy for elderly patients. Dis Esophagus. 2010;23(7):572–579. | ||
Cho SH, Shim HJ, Lee SR, et al. Concurrent chemoradiotherapy with S-1 and cisplatin in advanced esophageal cancer. Dis Esophagus. 2008;21(8):697–703. | ||
van Groeningen CJ, Peters GJ, Schornagel JH, et al. Phase I clinical and pharmacokinetic study of oral S-1 in patients with advanced solid tumors. J Clin Oncol. 2000;18(14):2772–2779. | ||
Ji Y, Qiu G, Sheng L, et al. A phase I dose escalation study of S-1 with concurrent radiotherapy in elderly patients with esophageal cancer. J Thorac Dis. 2016;8(3):451–458. | ||
Song T, Zhang X, Fang M, Wu S. Concurrent chemoradiotherapy using paclitaxel plus cisplatin in the treatment of elderly patients with esophageal cancer. Onco Targets Ther. 2015;8:3087–3094. | ||
Iwase H, Shimada M, Tsuzuki T, et al. Concurrent chemoradiotherapy with a novel fluoropyrimidine, S-1, and cisplatin for locally advanced esophageal cancer: long-term results of a phase II trial. Oncology. 2013;84(6):342–349. | ||
Xing L, Liang Y, Zhang J, et al. Definitive chemoradiotherapy with capecitabine and cisplatin for elder patients with locally advanced squamous cell esophageal cancer. J Cancer Res Clin Oncol. 2014;140(5):867–872. | ||
Song T, Liang X, Fang M, Wu S. High-dose versus conventional-dose irradiation in cisplatin-based definitive concurrent chemoradiotherapy for esophageal cancer: a systematic review and pooled analysis. Expert Rev Anticancer Ther. 2015;15(10):1157–1169. | ||
Zhang P, Xi M, Zhao L, et al. Is there a benefit in receiving concurrent chemoradiotherapy for elderly patients with inoperable thoracic esophageal squamous cell carcinoma? PLoS One. 2014;9(8):e105270. | ||
Umezawa R, Jingu K, Matsushita H, et al. Long-term results of chemoradiotherapy for stage II–III thoracic esophageal cancer in a single institution after 2000-with a focus on comparison of three protocols. BMC Cancer. 2015;15:813. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.