Back to Journals » Journal of Pain Research » Volume 18
Long-Term Refined Paraspinal Muscle Exercises Combined with ERAS Protocol Enhance Postoperative Recovery Following Lumbar Fusion Surgery
Authors Zhou X, He Z, Qi Y, Zhang X, Li J, Longzhu J, Yang J, Ma Y, Zhou F, Zhang F, Fang T, Zheng F
Received 3 March 2025
Accepted for publication 21 September 2025
Published 15 November 2025 Volume 2025:18 Pages 6097—6107
DOI https://doi.org/10.2147/JPR.S514865
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Xiaohui Zhou,1,2,* Zhao He,1,* Yulin Qi,1 Xin Zhang,1 Jia Li,2 Jiancuo Longzhu,2 Jiancheng Yang,1 Yulin Ma,1 Feng Zhou,3 Fucai Zhang,1 Tianci Fang,2,3,* Feng Zheng1
1Department of Orthopaedics, Qinghai Provincial People’s Hospital, Xining, Qinghai, 810000, People’s Republic of China; 2Department of Orthopaedics, XuZhou Central Hospital, Southeast University, Xuzhou, People’s Republic of China; 3Department of Orthopaedics, The First Affiliated Hospital of Soochow University, Soochow University, Suzhou, 215006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tianci Fang, Department of Orthopaedics, XuZhou Central Hospital, Southeast University, Xuzhou, People’s Republic of China, Email [email protected] Feng Zheng, Department of Orthopaedics, Qinghai Provincial People’s Hospital, Xining, Qinghai, 810000, People’s Republic of China, Email [email protected]
Objective: This study assesses the impact of long-term refined paraspinal muscle exercises on clinical outcomes in patients undergoing posterior lumbar interbody fusion (PLIF) surgery. We hypothesize that the integration of long-term refined paraspinal muscle exercises with ERAS short-term rehabilitation will result in superior musculoskeletal and psychological recovery compared to ERAS short-term exercises alone.
Methods: A total of 298 patients who underwent PLIF surgery between January 2020 and September 2023 were included. Of these, 198 patients (118 males, 80 females) followed the ERAS protocol for short-term recovery, with early mobilization and basic exercises starting within 24 hours post-surgery (ERAS-ST Group). The remaining 100 patients (55 males, 45 females) adhered to ERAS combined with long-term refined paraspinal muscle exercises, beginning within the first week post-surgery and continuing for at least 12 months (ERAS-LT Group). These exercises aimed to strengthen the lumbar and paraspinal muscles, promote long-term functional recovery, and prevent muscle atrophy and related complications. Clinical outcomes were assessed using the Visual Analogue Scale (VAS) for pain, the Oswestry Disability Index (ODI) for functional recovery, and PHQ-9 and GAD-7 to measure depression and anxiety symptoms. Muscle strength was evaluated using hand-held dynamometry (HHD), with measurements taken at baseline, 3 months, 6 months, and 12 months post-surgery.
Results: The ERAS-LT group showed significantly better outcomes in pain reduction (VAS), functional recovery (ODI), and psychological well-being (lower PHQ-9 and GAD-7 scores) compared to the ERAS-ST group. Notably, patients in the ERAS-LT Group demonstrated faster recovery in both physical and psychological domains. Key paraspinal muscles showed significantly improved muscle strength in the ERAS-LT Group.
Conclusion: Combining ERAS short-term functional exercises with long-term refined paraspinal muscle exercises significantly improves postoperative recovery in PLIF patients. The long-term exercise regimen enhanced pain management, functional recovery, muscle strength, and psychological well-being, supporting its incorporation into clinical rehabilitation protocols.
Keywords: lumbar fusion, refined paraspinal muscle exercises, postoperative rehabilitation, pain management, functional recovery, psychological well-being
Introduction
Lumbar degenerative diseases are among the most prevalent musculoskeletal conditions, affecting approximately 5% to 6% of the population.1,2 These conditions are a leading cause of low back pain and are frequently associated with symptoms such as difficulty in standing or walking, restricted spinal mobility, and, in more severe cases, numbness or paralysis in the lower limbs.3 Consequently, lumbar degenerative diseases can significantly impact both the physical and mental health of affected individuals, substantially reducing their overall quality of life.
While mild cases of lumbar degenerative diseases are typically managed with conservative treatments, moderate to severe cases often necessitate surgical intervention. Posterior lumbar interbody fusion (PLIF) is one of the most commonly performed surgical procedures for treating these diseases.3 However, PLIF surgery presents several challenges,4 including increased muscle trauma, postoperative complications, and delayed recovery, particularly in older patients. Moreover, psychological factors such as depression and anxiety are often overlooked during the recovery process, despite their critical role in exacerbating postoperative pain and hindering recovery.5,6
Active rehabilitation training has been shown to alleviate physical pain and improve psychological outcomes, such as depression and anxiety, in patients with spinal disorders.7–9 A key component of spinal rehabilitation is strengthening the paraspinal muscles, which are essential for maintaining spinal stability.10 Functional training targeting these muscles, particularly early lumbar and back muscle exercises, has demonstrated significant benefits in managing conditions like low back pain,11 ankylosing spondylitis,11 and stroke.12 However, many patients remain unaware of the importance of these exercises, which often leads to poor adherence to rehabilitation programs.
Enhanced Recovery After Surgery (ERAS) protocols, which emphasize early mobilization and perioperative care, are designed to minimize surgical trauma and stress responses, thus promoting faster recovery.13 While short-term rehabilitation under the ERAS protocol has demonstrated benefits in early recovery,14 there is a lack of research on long-term exercise interventions, which aim to prevent muscle atrophy, enhance muscle strength, and reduce postoperative pain in the months following lumbar surgery.
In our center, the integration of rehabilitation therapy, nursing measures, and surgical treatment through multidisciplinary collaboration has facilitated the implementation of this long-term, structured paraspinal muscle exercise program.
This study hypothesizes that long-term, refined paraspinal muscle exercises, when combined with early postoperative rehabilitation, will significantly enhance recovery outcomes in patients undergoing PLIF surgery. The aim is to evaluate the comprehensive impact of structured, long-term paraspinal muscle exercises on pain relief, functional recovery, psychological well-being, and flexion/extension muscle strength in PLIF patients, thereby providing practical rehabilitation guidance for clinical practice.
Clinical Data
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Ethics Committee of Qinghai Provincial People’s Hospital (2024073). All participants provided written informed consent after receiving detailed information about the study objectives and procedures. The study population comprised patients who underwent posterior lumbar interbody fusion (PLIF) surgery between January 2020 and September 2023. Patients were divided into two groups based on postoperative rehabilitation preferences and family support capacity: the ERAS-ST group (short-term ERAS rehabilitation only) and the ERAS-LT group (ERAS combined with long-term paraspinal muscle training). Propensity score matching was applied to control for confounders such as age, sex, and baseline pain scores.
Study Population
This study included 298 patients who underwent PLIF surgery between January 2020 and September 2023. The cohort consisted of 173 males and 125 females. Patients were divided into two groups based on the rehabilitation protocol they followed:ERAS Short-Term Functional Exercise Group (ERAS-ST): 198 patients (118 males, 80 females), aged 56–75 years (mean age: 58.42 ± 6.67 years), who adhered to the ERAS protocol with short-term postoperative functional exercises, including early mobilization, pain management, and basic exercises starting within 24 hours after surgery; ERAS + Long-Term Paraspinal Muscle Exercise Group (ERAS-LT): 100 patients (55 males, 45 females), aged 57–78 years (mean age: 60.15 ± 7.53 years), who followed the ERAS protocol and also engaged in long-term, refined paraspinal muscle exercises (starting within the first week post-surgery and continuing for at least 12 months) to enhance muscle strength, improve mobility, and support long-term functional recovery.
Inclusion and Exclusion Criteria
Inclusion criteria for PLIF surgery: 1) Imaging-confirmed diagnoses of disc herniation, degeneration, spondylolisthesis, or spinal stenosis causing nerve root compression. 2) Symptoms that failed to improve or worsened after three months of conservative treatment. 3) No contraindications for surgery.
Exclusion criteria for PLIF surgery: 1) History of prior spinal surgery. 2) Presence of infections, tumors, or severe systemic diseases. 3) Incomplete clinical data.
Inclusion criteria for the back muscle exercise program: 1) Patients fully informed and aware of the rehabilitation process. 2) Ability and willingness to comply with the prescribed exercise regimen.
Exclusion criteria for the back muscle exercise program: 1) Inability to adhere to medical advice or tolerate rehabilitation exercises. 2) Presence of mental or cognitive impairments that hinder cooperation with investigators.
Surgical Procedure and Intervention
Both groups underwent posterior lumbar interbody fusion (PLIF) with a standardized surgical approach.
ERAS Short-Term Functional Exercise Group (ERAS-ST):
Patients in this group followed the Enhanced Recovery After Surgery (ERAS) protocol, which focuses on early mobilization, minimizing surgical trauma, and reducing perioperative stress to promote early recovery.14 Postoperative functional exercises commencedwithin 24 hours after surgery, focusing primarily on pain management, basic mobility, and strengthening exercises to assist patients in regaining functional abilities in the immediate postoperative period.
ERAS + Long-Term Paraspinal Muscle Exercise Group (ERAS-LT):
In addition to adhering to the standard ERAS protocol, patients in this group participated in structured, long-term paraspinal muscle exercises, which began 2–4 weeks post-surgery and continued for at least 12 months. Before discharge, patients were assessed by a rehabilitation therapist, and after discharge, exercises were performed under family supervision. Regular follow-up through phone calls was conducted by nursing staff to monitor progress and address any issues encountered during the training. To ensure adherence to the long-term exercise regimen, ERAS-LT patients received personalized guidance from rehabilitation therapists at discharge, with daily supervision by family members. A rehabilitation log was maintained to record exercise details (eg, type, duration, and perceived exertion using the Borg Scale). The research team conducted monthly telephone follow-ups to verify logs and address training issues. Only patients who completed ≥80% of the exercise plan (ie, ≥38 weeks/year) were included in the final analysis; non-compliant cases (n=12) were excluded.
Paraspinal Muscle Exercise Details
The lumbar spine functions through the coordinated action of multiple muscle groups. Various exercises target specific muscles to achieve comprehensive rehabilitation, such as:15
Five-Point Support and Four-Point Kneeling Alternating to Two-Point Kneeling
This exercise targets the multifidus muscle, crucial for stabilizing the lumbar spine and improving posture. Begin in a quadruped position (hands and knees) and alternate lifting the opposite arm and leg, holding each position briefly before switching sides. This controlled movement enhances spinal stability and balance.
Flying Swallow (Small Swallow Exercise) and Back Extension (Goat Back Lift)
These exercises focus on the erector spinae muscles, which support spinal extension and upright posture. For the Flying Swallow, lie prone and lift the right arm and left leg simultaneously, holding for a few seconds before alternating. In the Back Extension, gently lift the upper torso off the ground while keeping the legs and arms grounded, strengthening spinal muscles.
Pull-Ups and Latissimus Dorsi Stretch
Pull-ups strengthen the latissimus dorsi, a key muscle for spinal stabilization. The Latissimus Dorsi Stretch involves raising both arms overhead and gently leaning to one side, stretching the muscles along the back. Together, these exercises build upper body strength and enhance spinal support.
Supine Alternating Leg Raises
This exercise targets the psoas major, essential for lumbar flexion and core stability. Lie on your back with legs extended, then lift one leg while keeping the other grounded. Alternate between legs to strengthen the core and support lower back stability.
Quadratus Lumborum Stretch
Stretching the quadratus lumborum can alleviate muscle-induced low back pain, as this muscle is often involved in chronic lumbar discomfort. Stand upright, raise one arm overhead, and gently lean to the opposite side to feel the stretch along the lower back.
Recommended Frequency (for all exercises): Perform 3–5 sets of each exercise, with 10–15 repetitions per set; Aim to complete exercises 3–4 times per week for optimal results; For stretching exercises (Latissimus Dorsi Stretch and Quadratus Lumborum Stretch), hold each stretch for 20–30 seconds per side, repeating 3–4 times per week.
Evaluation Indicators
The Visual Analogue Scale (VAS) for low back pain and Oswestry Disability Index (ODI) were used to evaluate clinical outcomes.
PHQ-9 and GAD-7 were utilized to assess depressive and anxiety symptoms.16 The Patient Health Questionnaire-9 (PHQ-9) is a 9-item self-administered tool designed to assess depression, with scores ranging from 0 to 27. Higher scores indicate more severe depression.
The GAD-7 assesses anxiety symptoms through seven questions aimed at identifying the presence of anxiety. Each item is scored from 0 to 3, with a total score ranging from 0 to 21. Higher scores indicate more severe anxiety.
Hand-Held Dynamometry (HHD): to evaluate the strength of paraspinal muscles.17 This method provided objective measurements of muscle strength at various time points post-surgery, specifically for the lumbar and paraspinal regions. The measurements were taken preoperatively and at 3, 6, and 12 months post-surgery to track the improvement in muscle strength.
Statistical Methods
To minimize measurement bias, all outcomes were assessed by evaluators blinded to group allocation. Statistical analysis was performed using SPSS 26.0 software Measurement data were expressed as mean ± standard deviation ( ). For normally distributed data, independent sample t-tests were used for comparisons between the two groups, while paired t-tests were applied for within-group comparisons at two time points. For non-normally distributed data, rank-sum tests and Mann–Whitney U-tests were used. Categorical data were analyzed using the chi-square test or Fisher’s exact test. A p-value of less than 0.05 was considered statistically significant.
). For normally distributed data, independent sample t-tests were used for comparisons between the two groups, while paired t-tests were applied for within-group comparisons at two time points. For non-normally distributed data, rank-sum tests and Mann–Whitney U-tests were used. Categorical data were analyzed using the chi-square test or Fisher’s exact test. A p-value of less than 0.05 was considered statistically significant.
Results
Basic Characteristics
Baseline comparisons revealed no significant differences between the two groups in terms of demographic characteristics, including age, sex, disease duration, occupation, household income, insurance status, and surgical segments (P > 0.05). In the ERAS-LT group, 88% of patients (88/100) completed ≥90% of the exercise plan without encountering significant difficulties. Additionally, 12 patients completed 80–90% of the training program. The 12 dropouts were primarily attributed to insufficient family support (n=7) or health-related issues (n=5, eg, cardiovascular events), none of which resulted in significant adverse effects or complications. Baseline medication use (eg, NSAIDs, antidepressants) showed no significant differences between the two groups (P > 0.05).
Pain and Lumbar Function
Regarding functional recovery, there were no differences in VAS scores between the two groups preoperatively and at 1 and 6 months; however, at 3 months, group LT’s pain scores were higher than those of group ST. A At 12 months postoperatively, the score in group LT was 1.74 ± 1.50, significantly lower than that in group ST (2.19 ± 1.58, P = 0.011). ODI scores showed no statistically significant differences between group LT and group ST preoperatively and at 1 month postoperatively. Group LT significantly outperformed group ST at 3 months (P = 0.007), 6 months (P = 0.002), and 12 months (P = 0.031), with scores of 17.76 ± 7.81, 16.52 ± 8.46, and 18.65 ± 11.14, respectively, compared to group B’s scores of 22.47 ± 8.08, 20.84 ± 5.63, and 23.81 ± 10.42. Figure 1 illustrates representative preoperative and postoperative radiographic findings in a patient undergoing PLIF surgery, demonstrating degenerative changes preoperatively (A), initial hardware placement at 1 month (B), early fusion signs at 6 months (C), and confirmed successful fusion at final follow-up (D).
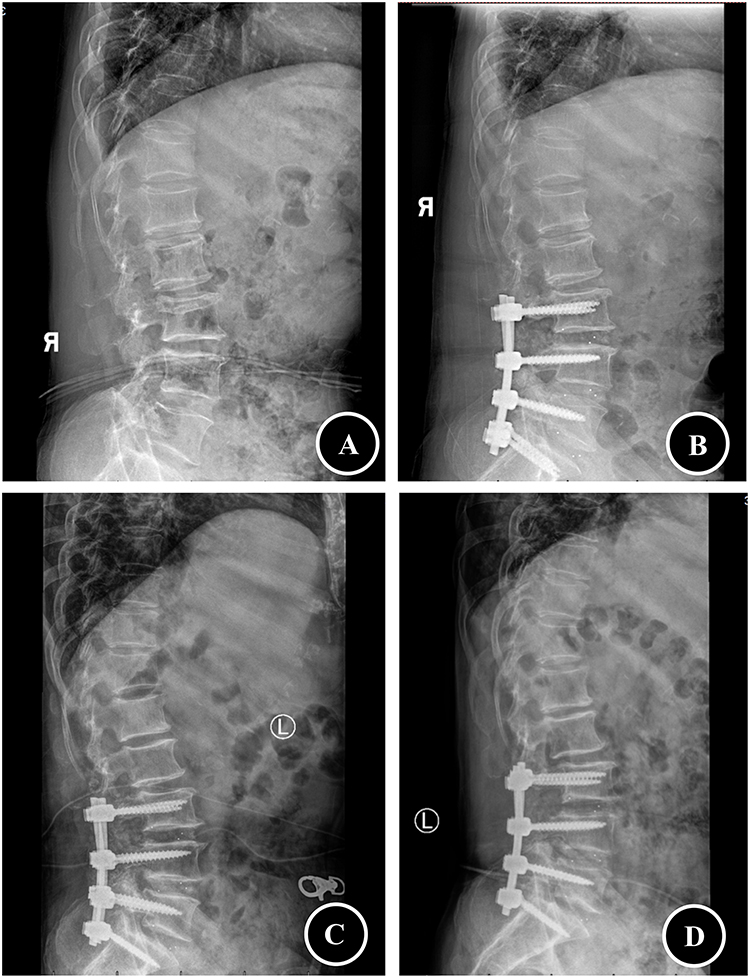 |
Figure 1 Preoperative and Postoperative Imaging of a Patient Undergoing PLIF. (A) Preoperative lateral radiograph showing degenerative changes and spinal instability. (B) Postoperative lateral radiograph at 1 month, demonstrating the initial placement of interbody fusion hardware and spinal alignment. (C) Postoperative lateral radiograph at 6 months, showing early signs of fusion and improved spinal alignment. (D) Final follow-up lateral radiograph, confirming successful fusion, stable hardware, and maintained spinal alignment. This figure illustrates the radiographic progression of a patient who underwent posterior lumbar interbody fusion (PLIF) surgery, highlighting the structural improvements achieved through the procedure and postoperative rehabilitation. |
Depression and Anxiety
In terms of emotional state, the comparison of PHQ-9 scores showed no differences between the two groups preoperatively. There was no statistically significant difference between the two groups at 6 months postoperatively; however, group LT had scores of 4.74 ± 3.93 and 2.39 ± 1.86 at 3 and 12 months postoperatively, respectively, which were significantly lower than group ST’s scores of 6.97 ± 4.19 and 4.28 ± 3.07 (P = 0.009 and P = 0.001). This indicates significant improvement in depressive symptoms for group LT, emphasizing the beneficial effect of consistent exercise on mental health. Although early GAD-7 scores showed no statistical differences, at 12 months postoperatively, group LT’s score was 3.08 ± 1.80, significantly lower than group ST’s score of 4.13 ± 2.08 (P = 0.012), further supporting the role of exercise in alleviating anxiety.
Muscle Strength
The results indicated that between 3 and 6 months postoperatively, patients showed a gradual recovery of both flexor and extensor muscle strength, although these values remained lower than preoperative levels. At 6 months post-surgery, the LT group demonstrated a statistically significant improvement in extensor muscle strength compared to the ST group (P < 0.05). By 12 months, the LT group exhibited more substantial recovery in both extensor and flexor muscle strength (P < 0.05).
Long-Term Complications
Fewer patients in the ERAS-LT group experienced long-term complications such as muscle atrophy and chronic back pain. Only 8% of patients in the ERAS-LT group reported persistent back pain at 12 months, compared to 20% in the ERAS-ST group (P < 0.05).
Discussion
Lumbar degenerative diseases, a leading cause of low back pain, significantly impact patients’ physical and mental health.18 These conditions often lead to reduced spinal mobility, muscle atrophy, and psychological distress, which can significantly impair the quality of life. Posterior lumbar interbody fusion (PLIF) surgery is commonly performed to restore spinal stability, but it presents challenges, including muscle trauma, postoperative complications, and delayed recovery. In this context, enhancing the rehabilitation process, particularly through muscle-strengthening exercises, can play a crucial role in mitigating these challenges.19
This study underscores the significant benefits of incorporating long-term, refined paraspinal muscle exercises into the postoperative rehabilitation of patients undergoing lumbar fusion surgery. Evidence demonstrates that targeted interventions, such as isolated lumbar extension resistance exercises (ILEX), effectively recondition lumbar extensor strength and improve functional outcomes in chronic low back pain populations, with MRI and T2 mapping confirming enhanced paraspinal muscle endurance and morphology after exercise programs.20,21 Our findings align with studies showing that postoperative rehabilitation not only accelerates physical recovery but also reduces pain and improves patient satisfaction by restoring flexor-extensor muscle balance.22,23 For instance, a 12-month home-based exercise program post-lumbar fusion significantly improved trunk muscle strength, with back-specific exercises yielding greater functional gains compared to general rehabilitation protocols.24,25 Furthermore, multidisciplinary collaboration among surgical, rehabilitation, and nursing teams has enabled the development of comprehensive approaches addressing muscle asymmetry and fatty infiltration—key predictors of mechanical complications and reoperation risks.26 This integration is critical, as preoperative paraspinal muscle assessments (eg, cross-sectional area, fat infiltration) have emerged as prognostic indicators for postoperative outcomes, emphasizing the need for tailored rehabilitation.27 Notably, interventions combining motor control training with isolated lumbar strengthening (MC + ILEX) outperformed general exercise in enhancing upper lumbar paraspinal muscle volume and patient-reported outcomes, underscoring the value of biomechanically optimized regimens.28 Psychological well-being improvements are further amplified by addressing muscle strength imbalances, such as reduced extensor/flexor ratios linked to disability indices, which correlate with better Oswestry scores and reduced pain intensity.29 Collectively, these findings validate the necessity of sustained, structured paraspinal exercise programs supported by multidisciplinary strategies to optimize both physiological and psychological recovery trajectories.
Muscle Strength and Recovery Outcomes
A central aspect of this study was the objective measurement of muscle strength using hand-held dynamometry (HHD), a reliable tool validated for assessing isometric strength in both acute and subacute rehabilitation phases. We observed significant improvements in muscle strength across key paraspinal muscle groups such as the multifidus, erector spinae, and psoas major in the ERAS-LT group at both 6 and 12 months post-surgery. Notably, the slower strength gains in extensors compared to flexors may reflect differential biomechanical demands during early spinal stabilization, as the multifidus and erector spinae exhibit higher susceptibility to atrophy and fatty infiltration in degenerative conditions. These improvements were associated with better pain management, as evidenced by lower Visual Analog Scale (VAS) scores, and enhanced functional recovery, reflected by improved Oswestry Disability Index (ODI) scores, consistent with studies linking paraspinal muscle quality (eg, reduced fatty infiltration and increased functional cross-sectional area) to postoperative pain/disability outcomes.30,31
Paraspinal muscle strengthening provides multifaceted biomechanical advantages. Enhanced paraspinal muscles reduce pain related to spinal instability by improving load distribution, as evidenced by the inverse association between psoas mass and mechanical stress in degenerative lumbar conditions.32 Additionally, increased erector spinae muscle quantity correlates with diminished mechanical stress on spinal structures, contributing to sustained pain reduction and disability mitigation.33,34 This aligns with evidence that preserved multifidus integrity decreases dural sac compression and enhances lumbar flexibility, thereby slowing disability progression in degenerative spinal disorders.34 The delayed recovery of extensor strength relative to flexors may reflect distinct neuromuscular activation patterns, with extensors such as the multifidus playing a crucial role in segmental stabilization during dynamic motion.35 This differential underscores the importance of targeted rehabilitation protocols, particularly given the link between early postoperative paraspinal strengthening and reduced complications, including pedicle screw loosening.36 These findings extend prior observations by demonstrating that systematic muscle strengthening not only improves spinal stability but also optimizes force absorption during functional movements, addressing both pain pathogenesis and mechanical overload.37
Psychological Well-Being and Recovery
In addition to physical benefits, our study also underscores the psychological advantages of long-term muscle rehabilitation. We found that patients in the ERAS-LT group showed significant reductions in depression (PHQ-9 scores) and anxiety (GAD-7 scores) over time. These psychological improvements were particularly notable at 12 months post-surgery. The relationship between muscle strength and psychological well-being can be understood through the concept of self-efficacy, where stronger muscles contribute to a sense of control over one’s physical state.38 This sense of control, in turn, enhances psychological resilience, helping to reduce anxiety and depression associated with postoperative recovery.
Our findings corroborate existing evidence emphasizing that enhanced physical strength fosters psychological resilience through improved functional capacity and reduced disability-related distress.39,40 Robust physical function enhances self-esteem and mitigates mental health decline, particularly in chronic pain contexts where pain self-efficacy plays a pivotal role in reducing anxiety.41–43 Since pain and psychological distress often exhibit bidirectional interactions, the concurrent reduction in both domains observed in the ERAS-LT group highlights the critical need for integrated biopsychosocial rehabilitation approaches that address somatic and affective components holistically. Notably, at 3 months postoperatively, the ERAS-LT group displayed higher Visual Analogue Scale (VAS) scores than the ERAS-ST group, followed by a marked decline. This transient pain elevation likely reflects initial muscle adaptation responses involving microtrauma and delayed-onset muscle soreness (DOMS), which resembles exercise-induced discomfort in healthy individuals and may originate from fascial sources rather than muscle tissues.44 Concurrently, psychological barriers or suboptimal exercise technique during early rehabilitation may exacerbate transient pain through increased distress.42,45
As rehabilitation progressed, however, enhanced neuromuscular coordination—facilitated by motor skill adaptation—mediated pain tolerance and score reduction.46 These dynamics underscore the imperative for tailored patient education in early-phase rehabilitation to alleviate anxiety and bolster adherence.39 The psychological benefits of long-term exercise may be mediated through multiple pathways. First, physical activity upregulates brain-derived neurotrophic factor (BDNF), enhancing neuroplasticity and alleviating depressive symptoms.47 Second, improved muscle strength fosters self-efficacy—patients’ confidence in their ability to recover—which reduces helplessness and psychological distress.48 Third, regular exercise modulates the hypothalamic-pituitary-adrenal (HPA) axis, lowering cortisol levels and stabilizing mood.49 These mechanisms synergistically create a “biopsychological positive feedback loop”, amplifying rehabilitation outcomes. Future studies should incorporate biomarkers (eg, serum BDNF, cortisol) to validate these hypotheses.
Muscle Soreness and Adaptation
Our study findings reveal that, although flexor and extensor muscle strength progressively increased postoperatively, the average muscle strength remained lower than preoperative levels due to various factors, such as pain, fear, and stress, as well as the lack of long-term exercise. In the context of long-term back muscle exercises, we observed that extensor muscle strength showed significant improvement at 6 months and may even recover to a level higher than preoperative strength. In contrast, flexor muscle strength only exhibited notable differences at 12 months and ultimately recovered to levels comparable to preoperative strength.
It is also important to note the temporary discomfort and muscle soreness experienced by patients in the ERAS-LT group at the 3-month follow-up. This discomfort, likely stemming from muscle adaptation to the strengthening regimen, was transient and should not be interpreted as a failure of the rehabilitation protocol. On the contrary, this short-term discomfort reflects the necessary adjustments the body makes as muscles strengthen, ultimately contributing to long-term recovery. The absence of significant muscle strength improvements in the ERAS-ST group further underscores the pivotal role that sustained, structured rehabilitation exercises play in enhancing postoperative recovery.
Long-Term Outcomes and Complications
In terms of long-term outcomes, patients in the ERAS-LT group reported fewer complications, such as chronic back pain, compared to those in the ERAS-ST group. Only 8% of patients in the ERAS-LT group experienced persistent back pain at 12 months, whereas 18.2% of patients in the ERAS-ST group reported the same. This finding suggests that the long-term rehabilitation protocol not only promotes functional recovery but also helps prevent long-term complications that could potentially undermine the success of PLIF surgery. However, it is important to acknowledge that the relatively long duration of our study and the exclusion of patients who were unable to adhere to the exercise regimen may limit the comparison of certain long-term complications, particularly severe complications such as reoperation, adjacent segment degeneration, and nerve compression resulting from these conditions.
Study Limitations and Future Directions
Despite the promising findings, this study has some limitations. The observational design and lack of randomization introduce potential selection bias, and the sample size, though adequate, may not fully account for all potential confounding variables. Although propensity score matching controlled for baseline confounders (eg, age, sex), self-selection bias may persist due to patient preferences for long-term exercise. Future randomized controlled trials with larger cohorts and longer follow-up periods are necessary to validate these findings and further explore the mechanisms underlying muscle strength improvements, including neuroplasticity and muscle remodeling.
Additionally, it would be beneficial to investigate the specific biological mechanisms that mediate the improvements in muscle strength and psychological outcomes, potentially leading to more targeted rehabilitation strategies. Understanding these pathways could further optimize rehabilitation protocols for PLIF patients and extend the benefits of muscle training to other spinal conditions.
Conclusion
In conclusion, our study demonstrates that integrating long-term refined paraspinal muscle exercises with the ERAS short-term rehabilitation protocol significantly improves postoperative recovery in PLIF patients. This long-term exercise regimen not only enhances pain management, functional recovery, and muscle strength but also contributes to better psychological well-being. These findings underscore the importance of incorporating long-term, structured muscle exercises into clinical rehabilitation protocols, offering a holistic approach to optimizing recovery outcomes and improving the overall quality of life for PLIF patients. Future research should focus on refining these rehabilitation strategies and exploring the underlying mechanisms to further enhance recovery and long-term health outcomes for this patient population.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request. Restrictions may apply to the availability of some data due to privacy or ethical considerations.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki and was approved by the Ethics Committee of Qinghai Provincial People’s Hospital. Written informed consent was obtained from all participants prior to their inclusion in the study. Participants were fully informed about the study objectives, procedures, potential risks, and benefits.
Consent for Publication
All authors have provided their consent for the publication of this manuscript. The manuscript does not contain any individual person’s data in any form (including images, videos, or other identifiable information).
Acknowledgments
The authors would like to express their gratitude to Qinghai Provincial People’s Hospital for their support and resources throughout this study. Special thanks to the rehabilitation therapists, nursing staff, and patients who participated in this research. Their cooperation and dedication were essential to the successful completion of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Qinghai Provincial Health Commission [2023-wjzdx-09], Soochow University [P112211323], Qinghai Provincial Health Commission [2022-wjzd-02], and Qinghai Province [QHKLYC-GDCXCY-2022-058].
Disclosure
The authors declare that they have no competing interests. No financial or non-financial conflicts of interest influenced the design, execution, or reporting of this study.
References
1. Morlion B. Chronic low back pain: pharmacological, interventional and surgical strategies. Nat Rev Neurol. 2013;9(8):462–473. doi:10.1038/nrneurol.2013.130
2. Modic MT, Ross JS. Lumbar degenerative disk disease. Radiology. 2007;245(1):43–61. doi:10.1148/radiol.2451051706
3. Reid PC, Morr S, Kaiser MG. State of the union: a review of lumbar fusion indications and techniques for degenerative spine disease. J Neurosurg Spine. 2019;31(1):1–14. doi:10.3171/2019.4.SPINE18915
4. Meng B, Bunch J, Burton D, et al. Lumbar interbody fusion: recent advances in surgical techniques and bone healing strategies. Eur Spine J. 2021;30(1):22–33. doi:10.1007/s00586-020-06596-0
5. Bekeris J, Wilson LA, Fiasconaro M, et al. New onset depression and anxiety after spinal fusion surgery: incidence and risk factors. Spine. 2020;45(16):1161–1169. doi:10.1097/BRS.0000000000003467
6. Deshpande N, Hadi M, Mansour TR, et al. The impact of anxiety and depression on lumbar spine surgical outcomes: a michigan spine surgery improvement collaborative study. J Neurosurg Spine. 2024;40(6):741–750. doi:10.3171/2023.12.SPINE23860
7. Lotzke H, Jakobsson M, Brisby H, et al. Use of the PREPARE (PREhabilitation, Physical Activity and exeRcisE) program to improve outcomes after lumbar fusion surgery for severe low back pain: a study protocol of a person-centred randomised controlled trial. BMC Musculoskelet Disord. 2016;17(1):349. doi:10.1186/s12891-016-1203-8
8. Pakarinen M, Vanhanen S, Sinikallio S, et al. Depressive burden is associated with a poorer surgical outcome among lumbar spinal stenosis patients: a 5-year follow-up study. Spine J. 2014;14(10):2392–2396. doi:10.1016/j.spinee.2014.01.047
9. Chin-Hung Chen V, Yang Y-H, Chen P-Y, et al. Factors affecting lumbar surgery outcome: a nation-wide, population-based retrospective study. J Affect Disord. 2017;222:98–102. doi:10.1016/j.jad.2017.06.060
10. Suo M, Zhang J, Sun T, et al. The association between morphological characteristics of paraspinal muscle and spinal disorders. Ann Med. 2023;55(2):2258922. doi:10.1080/07853890.2023.2258922
11. Yildirim P, Gultekin A. The effect of a stretch and strength-based yoga exercise program on patients with neuropathic pain due to lumbar disc herniation. Spine. 2022;47(10):711–719. doi:10.1097/BRS.0000000000004316
12. Cuellar WA, Wilson A, Blizzard CL, et al. The assessment of abdominal and multifidus muscles and their role in physical function in older adults: a systematic review. Physiotherapy. 2017;103(1):21–39. doi:10.1016/j.physio.2016.06.001
13. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
14. Debono B, Wainwright TW, Wang MY, et al. Consensus statement for perioperative care in lumbar spinal fusion: enhanced Recovery After Surgery (ERAS®) society recommendations. Spine J. 2021;21(5):729–752. doi:10.1016/j.spinee.2021.01.001
15. Tian W. Physical exercise for the prevention of low back pain. Chin J Prevent Med. 2023;24(01):2–3.
16. Huang XJ, Ma H-Y, Wang X-M, et al. Equating the PHQ-9 and GAD-7 to the HADS depression and anxiety subscales in patients with major depressive disorder. J Affect Disord. 2022;311:327–335. doi:10.1016/j.jad.2022.05.079
17. Lee YP, Regev GJ, Chan J, et al. Evaluation of hip flexion strength following lateral lumbar interbody fusion. Spine J. 2013;13(10):1259–1262. doi:10.1016/j.spinee.2013.05.031
18. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
19. Skrobot W, Liedtke E, Krasowska K, et al. Early rehabilitation program and vitamin D supplementation improves sensitivity of balance and the postural control in patients after posterior lumbar interbody fusion: a randomized trial. Nutrients. 2019;11(9):2202. doi:10.3390/nu11092202
20. Huang Y, Wei J, Han D, et al. Muscular blood oxygen level-dependent MRI is beneficial to evaluate effectiveness of an exercise prescription. Ann Transl Med. 2021;9(6):470. doi:10.21037/atm-21-279
21. Golonka W, Raschka C, Harandi VM, et al. Isolated lumbar extension resistance exercise in limited range of motion for patients with lumbar radiculopathy and disk herniation-clinical outcome and influencing factors. J Clin Med. 2021;10(11):2430. doi:10.3390/jcm10112430
22. Wu T, Ye Y. The effect of lower-limb exercise on pain management of the patients undergoing posterior lumbar fusion surgery: a retrospective case-control study. Pain Res Manag. 2021;2021:3716696. doi:10.1155/2021/3716696
23. Takahashi S, Hoshino M, Ohyama S, et al. Relationship of back muscle and knee extensors with the compensatory mechanism of sagittal alignment in a community-dwelling elderly population. Sci Rep. 2021;11(1):2179. doi:10.1038/s41598-021-82015-8
24. Ilves O, Neva MH, Häkkinen K, et al. Effectiveness of a 12-month home-based exercise program on trunk muscle strength and spine function after lumbar spine fusion surgery: a randomized controlled trial. Disabil Rehabil. 2022;44(4):549–557. doi:10.1080/09638288.2020.1772383
25. Ilves OE, Neva MH, Häkkinen K, et al. Trunk muscle strength after lumbar spine fusion: a 12-month follow-up. Neurospine. 2019;16(2):332–338. doi:10.14245/ns.1836136.068
26. Han G, Fan Z, Yue L, et al. Paraspinal muscle endurance and morphology (PMEM) score: a new method for prediction of postoperative mechanical complications after lumbar fusion. Spine J. 2024;24(10):1900–1909. doi:10.1016/j.spinee.2024.05.010
27. Cho SM, Kim S-H, Ha S-K, et al. Paraspinal muscle changes after single-level posterior lumbar fusion: volumetric analyses and literature review. BMC Musculoskelet Disord. 2020;21(1):73. doi:10.1186/s12891-020-3104-0
28. Rosenstein B, Rye M, Roussac A, et al. Comparison of combined motor control training and isolated extensor strengthening versus general exercise on lumbar paraspinal muscle health and associations with patient-reported outcome measures in chronic low back pain patients: a randomized controlled trial. Global Spine J. 2025;21925682251324490.
29. Benatto MT, Florencio LL, Bragatto MM, et al. Extensor/flexor ratio of neck muscle strength and electromyographic activity of individuals with migraine: a cross-sectional study. Eur Spine J. 2019;28(10):2311–2318. doi:10.1007/s00586-019-06097-9
30. Ranger TA, Cicuttini FM, Jensen TS, et al. Are the size and composition of the paraspinal muscles associated with low back pain? A systematic review. Spine J. 2017;17(11):1729–1748. doi:10.1016/j.spinee.2017.07.002
31. Halliday MH, Pappas E, Hancock MJ, et al. A randomized controlled trial comparing the mckenzie method to motor control exercises in people with chronic low back pain and a directional preference. J Orthop Sports Phys Ther. 2016;46(7):514–522. doi:10.2519/jospt.2016.6379
32. Choi TY, Chang M-Y, Lee SH, et al. Psoas muscle measurement as a predictor of recurrent lumbar disc herniation: a retrospective blind study. Medicine. 2022;101(26):e29778. doi:10.1097/MD.0000000000029778
33. Ghimire N, Lakhe P, Kumar A, et al. The impact of paraspinal muscle morphology on functional outcome in patients with degenerative lumbar spine disease undergoing surgery - A prospective observational study. Brain Spine. 2024;4:104141. doi:10.1016/j.bas.2024.104141
34. Banitalebi H, Hermansen E, Hellum C, et al. Preoperative fatty infiltration of paraspinal muscles assessed by MRI is associated with less improvement of leg pain 2 years after surgery for lumbar spinal stenosis. Eur Spine J. 2024;33(5):1967–1978. doi:10.1007/s00586-024-08210-z
35. Cheung MC, Yip J, Lai JSK. Biofeedback posture training for adolescents with mild scoliosis. Biomed Res Int. 2022;2022:5918698. doi:10.1155/2022/5918698
36. Wang W, Li W, Chen Z. Risk factors for screw loosening in patients with adult degenerative scoliosis: the importance of paraspinal muscle degeneration. J Orthop Surg Res. 2021;16(1):448. doi:10.1186/s13018-021-02589-x
37. Muellner M, Haffer H, Moser M, et al. Paraspinal musculature impairment is associated with spinopelvic and spinal malalignment in patients undergoing lumbar fusion surgery. Spine J. 2022;22(12):2006–2016. doi:10.1016/j.spinee.2022.07.103
38. Verhoeven JE, Han LKM, Lever-van Milligen BA, et al. Antidepressants or running therapy: comparing effects on mental and physical health in patients with depression and anxiety disorders. J Affect Disord. 2023;329:19–29. doi:10.1016/j.jad.2023.02.064
39. McBride D, Samaranayaka A, Richardson A, et al. Factors associated with self-reported health among New Zealand military veterans: a cross-sectional study. BMJ Open. 2022;12(5):e056916. doi:10.1136/bmjopen-2021-056916
40. Wang Y, Tian S, Yi J, et al. The impact of family burden on the psychological distress of informal caregivers for older adults living with dementia: the role of internal and external coping resources. Geriatr Nurs. 2024;60:92–98. doi:10.1016/j.gerinurse.2024.08.017
41. Woldeamanuel YW, Sanjanwala BM, Cowan RP. Endogenous glucocorticoids may serve as biomarkers for migraine chronification. Ther Adv Chronic Dis. 2020;11:2040622320939793. doi:10.1177/2040622320939793
42. Zhang X, Yue H, Sun J, et al. Regulatory emotional self-efficacy and psychological distress among medical students: multiple mediating roles of interpersonal adaptation and self-acceptance. BMC Med Educ. 2022;22(1):283. doi:10.1186/s12909-022-03338-2
43. Mou Q, Gao M, Liu X, et al. Preoperative anxiety as an independent predictor of postoperative delirium in older patients undergoing elective surgery for lumbar disc herniation. Aging Clin Exp Res. 2023;35(1):85–90. doi:10.1007/s40520-022-02278-7
44. Brandl A, Wilke J, Egner C, et al. Pain quality patterns in delayed onset muscle soreness of the lower back suggest sensitization of fascia rather than muscle afferents: a secondary analysis study. Pflugers Arch. 2024;476(3):395–405. doi:10.1007/s00424-023-02896-8
45. Shahrour G, Dardas LA. Acute stress disorder, coping self-efficacy and subsequent psychological distress among nurses amid COVID-19. J Nurs Manag. 2020;28(7):1686–1695. doi:10.1111/jonm.13124
46. Paladugu P, Kumar R, Ong J, et al. Virtual reality-enhanced rehabilitation for improving musculoskeletal function and recovery after trauma. J Orthop Surg Res. 2025;20(1):404. doi:10.1186/s13018-025-05705-3
47. Kandola A, Ashdown-Franks G, Hendrikse J, et al. Physical activity and depression: towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. 2019;107:525–539. doi:10.1016/j.neubiorev.2019.09.040
48. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037/0033-295X.84.2.191
49. Heijnen S, Hommel B, Kibele A, et al. Neuromodulation of aerobic exercise-a review. Front Psychol. 2015;6:1890. doi:10.3389/fpsyg.2015.01890
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.