Back to Journals » International Journal of General Medicine » Volume 18
Long-Term Outcomes and Post-Ablation Medication De-Escalation After Catheter Ablation for Premature Ventricular Complexes: A Nationwide Cohort Study
Authors Lin CY ![]() , Chuang CW
, Chuang CW ![]() , Chen M, Shia BC
, Chen M, Shia BC ![]()
Received 18 September 2025
Accepted for publication 21 October 2025
Published 3 November 2025 Volume 2025:18 Pages 6611—6625
DOI https://doi.org/10.2147/IJGM.S568435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Woon-Man Kung
Chung-Yu Lin,1– 3 Chien-Wei Chuang,1,2 Mingchih Chen,1,2 Ben-Chang Shia1,2
1Graduate Institute of Business Administration, Fu Jen Catholic University, New Taipei City, Taiwan; 2Artificial Intelligence Development Center, Fu Jen Catholic University, New Taipei City, Taiwan; 3Department of Cardiology, Fu Jen Catholic University Hospital, New Taipei City, Taiwan
Correspondence: Ben-Chang Shia, Graduate Institute of Business Administration, Fu Jen Catholic University, No. 510, Zhongzheng Road, Xinzhuang Dist, New Taipei City, 242062, Taiwan, Tel +886-2-2905-2901; +886-2-2905-3986, Email [email protected] Mingchih Chen, Graduate Institute of Business Administration, Fu Jen Catholic University, No. 510, Zhongzheng Road, Xinzhuang Dist, New Taipei City, 242062, Taiwan, Tel +886-2-2905-3895, Email [email protected]
Purpose: Frequent premature ventricular complexes are increasingly recognized as a contributor to ventricular dysfunction and progression to heart failure. Current clinical guidelines endorse radiofrequency catheter ablation as an effective treatment for symptomatic or drug-refractory premature ventricular complexes. However, nationwide long-term real-world outcomes, particularly those related to post-ablation medication de-escalation, remain insufficiently characterized.
Patients and Methods: Using Taiwan’s National Health Insurance Research Database, we conducted a nationwide retrospective cohort study of adults who underwent first-time radiofrequency catheter ablation for premature ventricular complexes between 2002 and 2018, with follow-up extending to December 31, 2021, allowing for up to three years of observation. Clinical outcomes included all-cause mortality and heart failure rehospitalization. Antiarrhythmic drug utilization was assessed through both prescription prevalence and defined daily dose, evaluated at baseline, 90 days, and 1 year post-ablation. Subgroup analyses were stratified by baseline heart failure status.
Results: A total of 4195 patients (mean age 53± 15 years; 49% women) were included, of whom 7% had heart failure. Baseline heart failure independently predicted mortality (hazard ratio 3.99, 95% confidence interval 2.71– 5.88) and heart failure rehospitalization (hazard ratio 7.29, 95% confidence interval 5.49– 9.66). Radiofrequency catheter ablation was associated with substantial reductions in antiarrhythmic drug use, declining from 58% before the procedure to 31% at 1 year. Medication analysis confirmed dose de-escalation, particularly for mexiletine, propafenone, and amiodarone. However, patients with heart failure exhibited smaller reductions in beta-blockers and Class III agents.
Conclusion: This nationwide cohort offers real-world insight into radiofrequency catheter ablation outcomes for frequent premature ventricular complexes, highlighting divergent prognoses between patients with and without heart failure. Radiofrequency catheter ablation was associated with meaningful reductions in antiarrhythmic medication use, underscoring its potential therapeutic and economic benefits. These findings support radiofrequency catheter ablation as a component of long-term management strategies, while future prospective studies are needed to refine candidate selection and timing of intervention.
Keywords: premature ventricular complexes, PVC, radiofrequency catheter ablation, RFCA, population-based cohort, health economics
Introduction
Premature ventricular complexes (PVC), also referred to as ventricular premature complexes (VPCs), are among the most common ventricular arrhythmias encountered in clinical practice.1 Although historically considered benign in the absence of structural heart disease, growing evidence indicates that a high PVC burden may contribute to left ventricular dysfunction, adverse remodeling, and, in some cases, PVC-induced cardiomyopathy.1–3 Frequent PVC, affecting approximately 4–5% of the general population, have been independently linked to increased risks of heart failure and all-cause mortality, even in patients without pre-existing structural abnormalities.4–6
Radiofrequency catheter ablation (RFCA) has become the standard therapy for symptomatic, drug-refractory premature ventricular complexes (PVCs) with a burden greater than 10%, as well as for patients at risk of PVC-induced cardiomyopathy, according to current guidelines.7 Acute procedural success rates often exceed 80%, with favorable long-term clinical outcomes and low complication rates.7,8 Prior studies-both in Taiwan and internationally-have demonstrated the benefits of RFCA in symptom control and improvement of left ventricular function.9–12 However, most existing research has focused on short- to mid-term clinical endpoints, with limited data on long-term prognostic outcomes and healthcare resource utilization.
The Taiwan National Health Insurance Research Database (NHIRD) offers a unique opportunity to address these gaps. Encompassing over 99% of Taiwan’s 23 million residents, it provides comprehensive, longitudinal healthcare data across all care levels, including diagnostic codes, procedures, and prescriptions. NHIRD-based research has yielded important insights into arrhythmia management, particularly atrial fibrillation and supraventricular tachycardia.13,14 However, nationwide, population-based evidence specifically evaluating long-term outcomes after RFCA for PVC is lacking.
In addition to rhythm normalization, RFCA may reduce reliance on chronic antiarrhythmic drug (AAD) therapy.15,16 Long-term use of agents such as amiodarone or mexiletine has been linked to drug-related toxicity, including hepatic, thyroid, and pulmonary complications.17,18 Ongoing AAD therapy also necessitates regular laboratory and imaging surveillance, contributing to additional healthcare burden.19
Reducing the prevalence or intensity of AAD prescriptions may therefore yield meaningful clinical benefits, particularly in terms of patient safety and quality of life.20,21 These advantages are especially relevant in healthcare systems with constrained resources, where minimizing medication dependence may help optimize long-term care delivery.22,23 Despite these considerations, changes in AAD utilization following RFCA have not been comprehensively evaluated in large-scale, real-world cohorts.24,25
In this context, we conducted a nationwide cohort study using the NHIRD to investigate long-term outcomes after RFCA for PVC, focusing on both clinical endpoints—such as all-cause mortality and heart failure rehospitalization—and medication-related outcomes, including AAD discontinuation and reductions in defined daily dose (DDD).
Materials and Methods
We conducted a nationwide, retrospective cohort study using data from Taiwan’s National Health Insurance Research Database (NHIRD), a comprehensive claims-based database maintained by the Health and Welfare Data Science Center under the Ministry of Health and Welfare. The NHIRD includes longitudinal healthcare information on more than 99% of the Taiwanese population since the establishment of the National Health Insurance (NHI) program in 1995. It contains detailed records of outpatient and inpatient visits, diagnoses, procedures, prescriptions, and dialysis history. This study was reviewed and approved by the Institutional Review Board of Fu Jen Catholic University (IRB Approval No. C110199). The requirement for informed consent was waived due to the retrospective design of the study. The database used in this research was authorized for use by the national authority and contained only de-identified data provided by the Ministry of Health and Welfare, Taiwan.
The patient selection process is illustrated in Figure 1. We identified adult patients (aged ≥20 years) with a diagnosis of PVC who underwent their first radiofrequency catheter ablation between January 1, 2002, and December 31, 2018; patients with a prior ablation before cohort entry were excluded. The index date was defined as the date of the ablation procedure. Diagnoses were classified using the International Classification of Diseases, 9th and 10th Revision, Clinical Modification (ICD-9-CM and ICD-10-CM), while procedure codes followed the execution coding system established by Taiwan’s Ministry of Health and Welfare.
 |
Figure 1 The flow diagram of patient selection. From the NHIRD, 4195 patients with PVCs undergoing ablation were identified after exclusions. Patients were categorized by baseline heart failure status and analyzed for clinical and economic outcomes using descriptive statistics and logistic regression. Abbreviations: AFL, atrial flutter; Afib, atrial fibrillation; AT, atrial tachycardia; PSVT, paroxysmal supraventricular tachycardia; PVCs, premature ventricular complexes. |
Patients were eligible for inclusion if they had a confirmed diagnosis of PVC and subsequently received RFCA. We excluded individuals who had any documented diagnosis of atrial fibrillation, atrial flutter, paroxysmal supraventricular tachycardia (PSVT), or atrial tachycardia (AT) within 180 days prior to the index ablation, in order to focus on patients undergoing RFCA specifically for PVC. All patients were followed from the index date until the occurrence of study outcomes, loss to follow-up, or the end of the observation period on December 31, 2021, ensuring a maximum follow-up duration of three years.
Baseline demographic data and clinical comorbidities were extracted, including age, sex, and the presence of conditions such as ventricular tachycardia (VT), acute coronary syndrome (ACS), coronary artery disease (CAD), hypertension (HTN), diabetes mellitus (DM), dyslipidemia, heart failure (HF), cerebrovascular accident (CVA), chronic kidney disease (CKD), end-stage renal disease (ESRD), chronic obstructive pulmonary disease (COPD)/asthma, malignancy, moderate-to-severe liver disease, and rheumatic disease.
We examined long-term clinical outcomes, including all-cause mortality and heart failure rehospitalization. In addition, medication utilization was assessed across multiple time points, with a focus on antiarrhythmic drugs (AAD) from different pharmacologic classes—Class I (Ia, Ib, Ic), Class II (beta-blockers), Class III, and Class IV (non-dihydropyridine calcium channel blockers). Changes in prescribing patterns were evaluated by analyzing discontinuation rates and variations in DDD before and after the ablation procedure.
All statistical analyses were performed using R software (version 4.3.2). Categorical variables are presented as counts (percentages) and compared between groups using the Chi-square test. Continuous variables are expressed as mean (standard deviation) and compared using the independent t-test. A P-value < 0.05 was considered statistically significant. A large language model (ChatGPT 5, OpenAI, San Francisco, CA, USA) was used to assist in refining the English grammar, syntax, and overall readability of the manuscript. No new scientific content, data analysis, or interpretation was generated by the model. All outputs from the language model were carefully reviewed, revised, and validated by the authors, who retain full responsibility for the content and conclusions of this work.
To identify clinical predictors of long-term outcomes, including heart failure readmission and all-cause mortality, we conducted multivariable Cox proportional hazards regression analyses. Variables included in the models were selected based on clinical relevance and prior literature, and included age, sex, baseline comorbidities (eg, HF, VT, ACS, CAD, CKD), and medication use. Hazard ratios (HRs) with 95% confidence intervals (CIs) were reported. Kaplan–Meier survival curves were generated to estimate cumulative incidence of outcomes across subgroups, and differences between groups were assessed using the Log rank test.
Results
Baseline Characteristics
We included 4195 patients undergoing RFCA for PVC; 308 (7.3%) had baseline HF and 3887 (92.7%) did not. HF patients were older (61.1±14.7 vs 51.7±14.7 years) and more often male (60.0% vs 48.4%). Cardiovascular comorbidities were higher in HF: VT 12.3% vs 5.0%, ACS 10.1% vs 1.9%, CAD 25.0% vs 7.8%, PAD 2.9% vs 1.1%. Systemic conditions also clustered in HF: HTN 55.2% vs 32.1%, DM 22.4% vs 10.7%, dyslipidemia 32.5% vs 22.8%, CKD 13.3% vs 4.0%, ESRD 10.1% vs 2.8%, COPD/asthma 23.7% vs 9.0%, cerebrovascular disease 14.3% vs 5.3%, liver disease 10.4% vs 7.0%, malignancy 7.5% vs 4.2% (all p<0.05), as shown in Table 1.
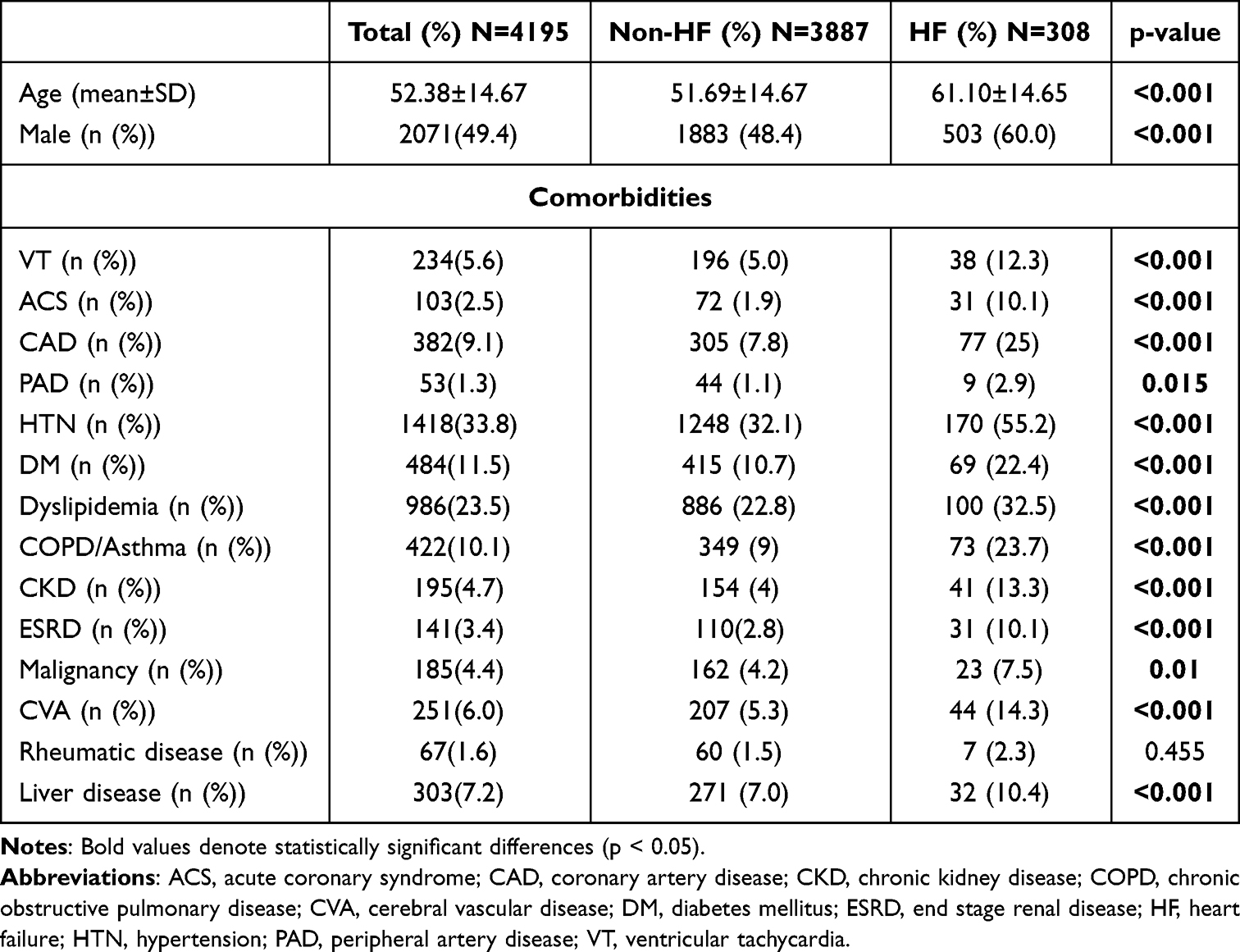 |
Table 1 Baseline Characteristics of Patients Undergoing RFCA for PVCs, Stratified by Baseline Heart Failure Status |
Pre-RFCA medication distribution (overall): beta-blockers 34.1%, Class Ia/Ib 9.8%, Class Ic 13.5%, Class III 4.4%, Non-DHP CCB 25.9%. By HF status, Class III was higher in HF (11.0% vs 3.8%), Class Ic higher in non-HF (13.8% vs 10.7%), and CCB 29.9% vs 25.9%, as shown in Table 2.
 |
Table 2 Changes in Antiarrhythmic Drug Utilization Before and After RFCA, Overall and by Heart Failure Status |
Clinical Outcomes and Predictors
Across 36 months, event curves separated early and remained apart. For HF rehospitalization, the HF group exceeded 30% by year 3, whereas the non-HF group stayed <10% (log-rank p<0.0001; Figure 2). All-cause mortality showed a similar pattern: ~18% in HF vs ~5% in non-HF at 3 years (log-rank p<0.0001; Figure 3).
 |
Figure 2 Kaplan-Meier curve for 3-year heart failure rehospitalization in patients with PVCs after RFCA, stratified by heart failure status. Kaplan–Meier curve illustrating the cumulative incidence of heart failure–related hospitalization in patients with and without pre-existing heart failure during the 3-year follow-up period. Patients with heart failure exhibited a significantly higher hospitalization risk than those without heart failure (log-rank p < 0.0001). The number at risk at each time point is presented below the plot. Abbreviations: HF, heart failure; RFCA, radiofrequency catheter ablation; PVCs, premature ventricular contractions. |
 |
Figure 3 Kaplan-Meier curve for 3-year all-cause mortality in patients with PVCs after RFCA, stratified by heart failure status. Kaplan–Meier survival curve comparing all-cause mortality between patients with and without pre-existing heart failure during the 3-year follow-up period. Patients with heart failure demonstrated significantly higher mortality than those without heart failure (log-rank p < 0.0001). The number at risk at each time point is presented below the plot. Abbreviations: HF, heart failure; RFCA, radiofrequency catheter ablation; PVCs, premature ventricular contractions. |
In multivariable Cox regression analysis, baseline heart failure was the strongest predictor of three-year rehospitalization (HR 7.29, 95% CI 5.49–9.66, p < 0.0001). Other independent predictors included ventricular tachycardia (HR 1.83, 95% CI 1.21–2.75, p = 0.004), acute coronary syndrome (HR 1.95, 95% CI 1.24–3.08, p = 0.004), and coronary artery disease (HR 1.72, 95% CI 1.24–2.41, p = 0.001). Hypertension (HR 1.58) and diabetes mellitus (HR 1.48) were also associated with increased rehospitalization risk. Renal dysfunction, particularly end-stage renal disease, demonstrated a strong association (HR 2.21, 95% CI 1.19–4.11, p = 0.012). Use of Class Ic antiarrhythmic drugs was associated with a reduced risk of rehospitalization (HR 0.52, 95% CI 0.35–0.76, p = 0.0001). Detailed hazard ratios are shown in Figure 4.
 |
Figure 4 Forest Plot of Cox Proportional Hazards Regression for Predictors of Post-Ablation Heart Failure Rehospitalization in 3 years. Forest plot presenting hazard ratios with 95% confidence intervals for clinical comorbidities associated with heart failure–related hospitalization over the 3-year follow-up period. A history of hypertension, heart failure, ventricular tachycardia, acute coronary syndrome, coronary artery disease, diabetes mellitus, and chronic kidney disease was identified as significantly associated with increased risk. Hazard ratios and p-values were calculated using Cox proportional hazards models. Abbreviations: AAD, anti-arrhythmic drug; ACS, acute coronary syndrome; CAD, coronary artery disease; CCB, calcium channel blocker; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular disease; DM, diabetes mellitus; ESRD, end stage renal disease; HF, heart failure; HTN, hypertension; PAD, peripheral artery disease; VT, ventricular tachycardia. |
For all-cause mortality, heart failure was again the most prominent predictor (HR 3.99, 95% CI 2.71–5.88, p < 0.0001), followed by end-stage renal disease (HR 2.82, 95% CI 1.10–7.26, p = 0.031) and malignancy (HR 3.48, 95% CI 2.27–5.34, p < 0.0001). Hypertension (HR 2.24, p = 0.0001) and chronic kidney disease (HR 1.83, 95% CI 1.22–2.75, p = 0.003) were also associated with increased mortality. Class Ia antiarrhythmic drug use was associated with higher mortality (HR 3.49, 95% CI 1.21–10.07, p = 0.04). Other antiarrhythmic drug classes were not independently associated with mortality. Mortality predictors are summarized in Figure 5.
 |
Figure 5 Forest Plot of Cox Proportional Hazards Regression for Predictors of Post-Ablation All-Cause Mortality in 3 years. Forest plot presenting hazard ratios with 95% confidence intervals for factors associated with all-cause mortality over the 3-year follow-up period. A history of hypertension, heart failure, diabetes mellitus, chronic obstructive pulmonary disease, malignancy, and Class Ia antiarrhythmic drug use was identified as significantly associated with increased mortality. In contrast, Class Ic antiarrhythmic drug use was associated with lower mortality risk. Hazard ratios and p-values were calculated using Cox proportional hazards models. Abbreviations: AAD, anti-arrhythmic drug; ACS, acute coronary syndrome; CAD, coronary artery disease; CCB, calcium channel blocker; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; CVA, cerebral vascular disease; DM, diabetes mellitus; ESRD, end stage renal disease; HF, heart failure; HTN, hypertension; PAD, peripheral artery disease; VT, ventricular tachycardia. |
Subgroup Analyses
Medication utilization patterns differed substantially between patients with and without heart failure. In the non-HF subgroup, the proportion of patients receiving beta-blockers decreased from 33.2% before RFCA to 17.6% at 90 days and partially rebounded to 25.5% at one year (both p < 0.001). Class Ia/Ib antiarrhythmic agents also declined markedly, from 10.0% to 2.6% at 90 days and 4.3% at one year (both p < 0.001), as did Class Ic therapy, which decreased from 13.8% at baseline to 5.3% and 7.7% at the respective time points (both p < 0.001).
In contrast, patients with HF exhibited more stable medication use over time. Beta-blocker use decreased initially from 45.8% to 31.5% at 90 days (p = 0.004) but returned to baseline levels at one year (46.1%, p = 0.95). Reductions in Class Ia/Ib and Class Ic prescriptions at 90 days (9.4% to 4.2% and 10.7% to 5.8%, respectively) were not sustained at one year (5.5% and 7.8%, respectively; both p > 0.05). Class III antiarrhythmic drug use showed minimal change in both subgroups throughout follow-up. Non-DHP CCB use decreased from 25.9% pre-RFCA to 10.4% at 90 days and 16.4% at one year in non-HF (both p < 0.001), while in HF it declined from 29.9% to 14.3% at 90 days (p < 0.001) and 18.5% at one year (p = 0.004). Detailed subgroup trajectories are presented in Table 2.
Medication De-Escalation
Changes in antiarrhythmic drug use following RFCA are summarized in Table 2 and visualized in Figure 6A–C. In the total cohort, beta-blocker use declined from 34.1% before RFCA to 18.1% at 90 days and remained lower at 27.0% at one year (both p < 0.001). Class Ia/Ib and Class Ic agents demonstrated similar reductions, decreasing from 9.8% to 2.8% and 13.5% to 5.4% at 90 days, with partial rebound to 4.4% and 7.7% at one year (both p < 0.001). Class III agents showed only a transient decrease (4.4% to 3.0%), returning to baseline by one year (4.5%) (p=0.78). Non-dihydropyridine calcium-channel blockers also declined from 25.9% to 10.4% and remained lower at 16.4% at one year.
Figure 6 Continued. Figure 6 (A) Proportion of patients with PVCs receiving antiarrhythmic drugs before radiofrequency catheter ablation (RFCA), at 90 days, and at 1 year in the total cohort. Comparison brackets indicate pairwise differences over time, with * indicating p < 0.05. (B) Proportion of patients with PVCs without heart failure (HF) receiving AAD before RFCA, at 90 days, and at 1 year. Comparison brackets reflect changes within the same cohort; * denotes p < 0.05. (C) Proportion of patients with HF receiving AAD at baseline, 90 days, and 1 year after RFCA. Significant differences between time points are shown with brackets, with * indicating p < 0.05. Abbreviations: AAD, anti-arrhythmic drug; CCB, calcium channel blocker; PVCs, premature ventricular contractions; RFCA, radiofrequency catheter ablation.

Subgroup analysis revealed sustained medication withdrawal in patients without HF, whereas those with HF demonstrated re-escalation, particularly in beta-blockers, which returned to baseline levels (45.8% to 46.1%) by one year. Class Ia/Ib and Ic use in HF showed no significant long-term reduction.
Dose intensity trends of Class I and Class III AAD, shown in Table 3 and Figure 7, paralleled prescription prevalence. Mexiletine and propafenone exhibited significant decreases in defined daily dose (DDD) at both 90 days and one year, and amiodarone demonstrated a progressive reduction from 1.16 to 0.79 by one year. These findings indicate that RFCA facilitated both discontinuation and dose de-escalation of antiarrhythmic therapy, particularly in patients without HF.
 |
Table 3 Changes in Defined Daily Dose of Class I and Class III AAD Before and After RFCA |
 |
Figure 7 Changes in DDD of antiarrhythmic drug use after RFCA. Mean DDD of individual antiarrhythmic drugs before RFCA, at 90 days, and at 1 year in the total cohort. Comparison brackets indicate within-patient changes over time, with * indicating p < 0.05. Abbreviations: DDD, defined daily dose; RFCA, radiofrequency catheter ablation. |
Discussion
Frequent PVC are increasingly recognized as a potential cause of reversible cardiomyopathy and adverse cardiovascular outcomes, especially when associated with high ectopic burden or structural heart disease.1–3 RFCA uses thermal energy to eliminate abnormal ectopic foci, thereby reducing irregular ventricular activation, mechanical dyssynchrony, and PVC-induced myocardial strain.2 Over the past decade, multiple observational and interventional studies have demonstrated that RFCA can achieve high acute success rates-often exceeding 80%-with sustained suppression of arrhythmia and improvement in left ventricular ejection fraction (LVEF).4–7 In addition to symptomatic relief, successful RFCA has been linked to reversal of PVC-induced cardiomyopathy and improvement in exercise capacity.5,7,26 However, the majority of these studies were conducted in single-center settings or selected populations, limiting their generalizability to broader, real-world clinical practice.27–29
Our nationwide, population-based analysis leveraging the Taiwan National Health Insurance Research Database (NHIRD) offers novel insights into the long-term outcomes of RFCA for PVC in a broad, unselected cohort. Although variables such as ECG characteristics, echocardiographic parameters, PVC burden, and procedural details are essential to fully assess ablation outcomes, these data are not available in the NHIRD administrative database. A non-ablation control cohort was initially considered using propensity score matching; however, substantial baseline imbalances—particularly related to symptom severity, PVC burden, and underlying cardiac dysfunction—limited the feasibility of obtaining a clinically comparable group.30 Rather than introducing additional selection bias, we elected to focus on a homogeneous ablation cohort to ensure validity of the long-term outcome assessment.
Beyond evidence from randomized trials confirming the efficacy of RFCA for PVC,28,29,31 our real-world data refine its prognostic impact. Compared with prior single-center or multicenter studies of idiopathic PVC or VT ablation,2,5,7,11,32,33 our findings provide a more risk-stratified perspective. Baseline heart failure emerged as the key determinant of long-term outcomes: patients without HF experienced marked reductions in mortality and rehospitalization, whereas those with HF continued to face elevated event rates despite procedural success. Notably, divergence in Kaplan–Meier curves appeared as early as 6–12 months post-ablation—earlier than previously reported2,5,11—underscoring the influence of underlying myocardial disease.
From the Taiwan Heart Failure Registry,34 which reported a one-year rehospitalization rate of 38.5% and a mortality rate of 10.5% among heart failure patients admitted in 2014, our study observed comparatively lower one-year rehospitalization (26%) and mortality (7.1%) in patients with HF undergoing RFCA for PVC. However, these differences should be interpreted with caution, as selection bias is likely present among patients who were considered suitable candidates for ablation.
The forest plot analyses highlight the pivotal role of comorbid conditions in shaping long-term outcomes after catheter ablation for premature ventricular complexes. A history of hypertension, heart failure, coronary and metabolic disease was associated with increased risk of heart failure–related rehospitalization and mortality, emphasizing that arrhythmia suppression alone may not fully mitigate adverse prognosis in patients with advanced systemic disease. Notably, Class Ia antiarrhythmic drug use, often reflective of refractory or high-risk substrate, was linked to higher mortality, while Class Ic use, typically restricted to structurally preserved hearts, showed a more favorable profile.18,26,27
Although PVC are distinct from sustained ventricular tachycardia, a high PVC burden may progress to more malignant ventricular arrhythmias, and both conditions often share similar pharmacologic strategies and indications for catheter ablation. The pattern observed in our cohort mirrors findings from scar-related VT ablation trials—such as VANISH, VTACH, and BERLIN-VT11,35,36—where procedural success alone was insufficient to overcome the adverse substrate of advanced cardiomyopathy. Consistent with multicenter VT registries17,37 our stratified analysis further identified chronic kidney disease, cerebrovascular disease, and malignancy as independent predictors of poor outcomes.
Reduction in AAD use after successful PVC ablation has been consistently documented;2,5 however, it may arise from multiple factors rather than arrhythmia suppression alone.38 However, most prior studies focused primarily on discontinuation or examined dose-related pharmacokinetic interactions and potential adverse effects, without quantifying actual dose reduction over time.39 By incorporating DDD analysis, our study provides a more nuanced assessment of medication burden, capturing not only prescription prevalence but also dosing intensity at both 90 days and one year post-ablation.
This is expected, as amiodarone is not a first-line agent for stable patients and is typically reserved for those who are refractory to other AADs or who have significant structural heart disease or heart failure.7 This pattern was reflected in our cohort, where amiodarone use was only 3.8% among patients without HF but reached 11% in those with HF. These findings suggest that RFCA may offer less potential for complete AAD withdrawal in patients already receiving amiodarone, regardless of the underlying indication. Nevertheless, PVC patients undergoing RFCA generally benefited from medication discontinuation or meaningful dose reduction with other AAD classes. Furthermore, compared with non-HF patients, those with HF demonstrated smaller reductions in beta-blocker use, reflecting the continued need for guideline-directed medical therapy irrespective of arrhythmia suppression.35,36,40
Beyond clinical endpoints, our findings have implications for healthcare resource utilization. Reductions in both the proportion of patients on AAD and the DDD of costly agents such as amiodarone can lower direct medication expenditures and decrease the need for long-term toxicity surveillance (eg, hepatic, thyroid, and pulmonary monitoring).23,24,41 Additionally, decreased reliance on chronic AAD therapy may reduce outpatient visits, laboratory monitoring, and unplanned emergency care-benefits supported by health-economic analyses in other arrhythmia management settings.27,28,42–44
Finally, it is important to acknowledge that Taiwan’s healthcare landscape differs substantially from that of other countries. Although Taiwan operates under a single-payer National Health Insurance system with relatively limited reimbursement, approximately 70% of patients also carry supplemental commercial insurance; In contrast, other countries may rely on multi-payer structures or purely commercial insurance systems with broader coverage.45 These differences can influence clinical decision-making and access to treatments such as ablation. Therefore, further research is needed to determine how these variations in healthcare financing may impact the generalizability of our findings.
Limitation
Several limitations should be acknowledged. First, the NHIRD, as an administrative claims database, lacks granular clinical information-such as echocardiographic parameters, PVC burden from Holter monitoring, and electrocardiographic origin-as well as procedural details, including ablation techniques, mapping systems, and repeat procedures. The absence of these data limits our ability to assess arrhythmia mechanisms, stratify clinical severity, and evaluate procedural success. Second, although we analyzed antiarrhythmic drug use and defined daily dose trends, the lack of data on clinical indications, patient adherence, and adverse effects restricts interpretation of prescribing behavior. Third, because this study included only patients who underwent RFCA, the cohort likely represents individuals with more symptomatic or higher-burden PVC, which may not reflect the full spectrum of PVC patients and introduces potential selection bias. Fourth, the absence of a non-ablated control group limits causal inference. Future studies should integrate NHIRD with hospital-based electronic medical records to construct matched cohorts with detailed clinical and procedural variables. Finally, residual confounding from unmeasured factors remains possible despite statistical adjustments.
Conclusion
In this nationwide real-world cohort, RFCA for frequent PVC was associated with meaningful changes in long-term therapeutic profiles, particularly through substantial reductions in antiarrhythmic drug use and dosing intensity. Medication de-escalation, confirmed through both prevalence and defined daily dose analysis, was more pronounced in patients without heart failure, whereas those with HF demonstrated a persistent need for pharmacologic therapy. These findings highlight the potential role of RFCA in facilitating rhythm stabilization and treatment simplification, especially in selected populations. While the study offers clinical and economic insights, interpretation must consider the inherent limitations of claims-based data. Future studies integrating detailed clinical parameters are warranted to optimize timing of intervention and refine post-ablation management strategies.
Acknowledgments
The authors gratefully acknowledge the Artificial Intelligence Development Center, Fu Jen Catholic University, New Taipei City, Taiwan, for their technical support.
Funding
This research was supported by two grants: NSTC112-2622-E-030-001 and A0113252, provided by Ben-Chang Shia and Fu Jen Catholic University, which supported the employment of research personnel for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chung F-P, Lin Y-J, Chang S-L, et al. Long-term follow-up of catheter ablation of ventricular arrhythmias: experiences from a tertiary referral center in Taiwan. Acta Cardiol Sin. 2015;31(1):8–17. doi:10.6515/acs20140721a
2. Latchamsetty R, Yokokawa M, Morady F, et al. Multicenter outcomes for catheter ablation of idiopathic premature ventricular complexes. JACC Clin Electrophysiol. 2015;1(3):116–123. doi:10.1016/j.jacep.2015.04.005
3. Lin CY, Chung FP, Lin YJ, et al. Radiofrequency catheter ablation of ventricular arrhythmias originating from the continuum between the aortic sinus of Valsalva and the left ventricular summit: electrocardiographic characteristics and correlative anatomy. Heart Rhythm. 2016;13(1):111–121. doi:10.1016/j.hrthm.2015.08.030
4. Lee PT, Huang TC, Huang MH, et al. The burden of ventricular premature complex is associated with cardiovascular mortality. Front Cardiovasc Med. 2022;8:797976. doi:10.3389/fcvm.2021.797976
5. Chen YS, Chen WD, Chen YH, et al. Atrial and ventricular response to treatment of premature ventricular complexes. Acta Cardiol Sin. 2020;36(5):475–482. doi:10.6515/ACS.202009_36(5).20200425A
6. Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary. Circulation. 2018;138(13):e210–71. doi:10.1161/CIR.0000000000000548
7. Cronin EM, Bogun FM, Maury P, et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Europace. 2019;21(8):1143–1144. doi:10.1093/europace/euz132
8. Kanat S, Mutluer FO, Tütüncü A, et al. Left atrial function is improved in short-term follow-up after catheter ablation of outflow tract premature ventricular complexes. Medicina (Kaunas). 2019;55(6):241. doi:10.3390/medicina55060241
9. Yen KC, Chan YH, Wang CL. Number of premature ventricular complexes predicts long-term outcomes in patients with persistent atrial fibrillation. Biomedicines. 2024;12(6):1149. doi:10.3390/biomedicines12061149
10. Kusumoto FM, Bailey KR, Chaouki AS, et al. Systematic review for the 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Circulation. 2018;138(13):e392–414. doi:10.1161/CIR.0000000000000550
11. Ju W, Gu K, Yang B, et al. Late cure of focal ventricular arrhythmias post-catheter ablation: electrophysiological characteristics and long-term outcome. J Interv Card Electrophysiol. 2018;52(1):31–37. doi:10.1007/s10840-018-0328-0
12. Dukes JW, Dewland TA, Vittinghoff E, et al. Ventricular ectopy as a predictor of heart failure and death. J Am Coll Cardiol. 2015;66(2):101–109. doi:10.1016/j.jacc.2015.04.062
13. Chan CL, Li AH, Chung HA, et al. Cost Effectiveness Analysis and Payment Policy Recommendation-Population-Based Survey with Big Data Methodology for Readmission Prevention of Patients with Paroxysmal Supraventricular Tachycardia treated with Radiofrequency Catheter Ablation. Int J Environ Res Public Health. 2020,Mar 30;17(7):2334. doi:10.3390/ijerph17072334.
14. Liao KM, Yu CH, Wu YC, et al. Risk of Atrial Fibrillation in Patients with Different Cancer Types in Taiwan. Life (Basel). 2024,May 11;14(5):621. doi:10.3390/life14050621
15. Kochs M, Eggeling T, Hombach V. Pharmacological therapy in coronary heart disease: prevention of life-threatening ventricular tachyarrhythmias and sudden cardiac death. Eur Heart J. 1993;14 Suppl E:107–119. doi:10.1093/eurheartj/14.suppl_e.107
16. Freedman BL, Maher TR, Tracey M, et al. Procedural adaptations to avoid haemodynamic instability during catheter ablation of scar-related ventricular tachycardia. Arrhythm Electrophysiol Rev. 2023;12:e20. doi:10.15420/aer.2022.24
17. Belhassen B, Tovia-Brodie O. Short-coupled idiopathic ventricular fibrillation: a literature review with extended follow-up. JACC Clin Electrophysiol. 2022;8(7):918–936. doi:10.1016/j.jacep.2022.04.013
18. Saikawa T, Nakagawa M, Takahashi N, et al. Mexiletine and disopyramide suppress ventricular premature contractions irrespective of the relationship between the VPC and the underlying heart rate. Jpn Heart J. 1992;33(5):665–678. doi:10.1536/ihj.33.665
19. Sciria CT, Kogan EV, Ip JE, et al. Trends and outcomes of catheter ablation of ventricular tachycardia in patients with ischemic and nonischemic cardiomyopathy. Circ Arrhythm Electrophysiol. 2022;15(4):e010742. doi:10.1161/CIRCEP.121.010742
20. Chen TE, Wang CC, Ho HC, et al. Impact of premature ventricular complex burden on the left ventricle in the structurally normal heart: hemodynamic alterations of idiopathic PVC on echocardiography. Acta Cardiol Sin. 2023;39(5):687–694. doi:10.6515/ACS.202309_39(5).20230119A
21. Benjamin EJ, Virani SS, Callaway CW, et al. Heart disease and stroke statistics—2018 update: a report from the American Heart Association. Circulation. 2018;137(5):e67–492. doi:10.1161/CIR.0000000000000558
22. Zipes DP, Camm AJ, Borggrefe M, et al. ACC/AHA/ESC 2006 guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. J Am Coll Cardiol. 2006;48(5):e247–346. doi:10.1016/j.jacc.2006.07.010
23. Șorodoc V, Indrei L, Dobroghii C, et al. Amiodarone therapy: updated practical insights. J Clin Med. 2024;13(20):6094. doi:10.3390/jcm13206094
24. Vassallo P, Trohman RG. Prescribing amiodarone: an evidence-based review of clinical indications. JAMA. 2007;298(11):1312–1327. doi:10.1001/jama.298.11.1312
25. Baman TS, Lange DC, Ilg KJ, et al. Relationship between burden of premature ventricular complexes and left ventricular function. Heart Rhythm. 2010;7(7):865–869. doi:10.1016/j.hrthm.2010.03.036
26. Zhong L, Lee Y-H, Huang X-M, et al. Relative efficacy of catheter ablation vs antiarrhythmic drugs in treating premature ventricular contractions: a single-center retrospective study. Heart Rhythm. 2014;11(2):187–193. doi:10.1016/j.hrthm.2013.10.033
27. De Silva K, Haqqani H, Mahajan R, et al. Catheter ablation vs antiarrhythmic drug therapy for treatment of premature ventricular complexes: a systematic review. JACC Clin Electrophysiol. 2023;9(6):873–885. doi:10.1016/j.jacep.2023.01.035
28. Willy K, Frommeyer G, Dechering DG, et al. Outcome of catheter ablation in the very elderly—insights from a large matched analysis. Clin Cardiol. 2020;43(12):1423–1427. doi:10.1002/clc.23471
29. Parkash R, Nault I, Rivard L, et al. Effect of baseline antiarrhythmic drug on outcomes with ablation in ischemic ventricular tachycardia: a VANISH substudy. Circ Arrhythm Electrophysiol. 2018;11(1):e005663. doi:10.1161/CIRCEP.117.005663
30. Huang YT, Chen YJ, Chang SH, Kuo CF, Chen MH. Discharge status validation of the Chang Gung Research database in Taiwan. Biomed J. 2022;45(6):907–913. doi:10.1016/j.bj.2021.12.006
31. Bogun F, Crawford T, Reich S, et al. Radiofrequency ablation of frequent, idiopathic premature ventricular complexes: comparison with a control group without intervention. Heart Rhythm. 2007;4(7):863–867. doi:10.1016/j.hrthm.2007.03.003
32. Zeppenfeld K, Tfelt-Hansen J, de Riva M, et al. 2022 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur Heart J. 2022;43(40):3997–4126. doi:10.1093/eurheartj/ehac262
33. Cronin EM, Bogun FM, Maury P, et al. 2019 HRS/EHRA/APHRS/LAHRS expert consensus statement on catheter ablation of ventricular arrhythmias. Heart Rhythm. 2019;16(1):e155–205. doi:10.1016/j.hrthm.2019.01.001
34. Chang HY, Wang CC, Wu YW, et al. One-year outcomes of acute decompensated systolic heart failure in taiwan: lessons from TSOC-HFrEF registry. Acta Cardiol Sin. 2017;33(2):127–138. doi:10.6515/acs20170202a
35. Sapp JL, Wells GA, Parkash R, et al. Ventricular tachycardia ablation versus escalated antiarrhythmic drugs (VANISH). N Engl J Med. 2016;375(2):111–121. doi:10.1056/NEJMoa1513614
36. Kuck KH, Schaumann A, Eckardt L, et al. Catheter ablation of stable ventricular tachycardia before defibrillator implantation in patients with coronary heart disease (VTACH): a multicentre randomised controlled trial. Lancet. 2010;375(9708):31–40. doi:10.1016/S0140-6736(09)61755-4
37. Dinov B, Fiedler L, Schönbauer R, et al. Outcomes in catheter ablation of ventricular tachycardia in dilated nonischemic cardiomyopathy compared with ischemic cardiomyopathy: results from the German VT registry. Circulation. 2014;129(7):728–736. doi:10.1161/CIRCULATIONAHA.113.003063
38. Lamba J, Redfearn DP, Michael KA, et al. Radiofrequency catheter ablation for the treatment of idiopathic premature ventricular contractions originating from the right ventricular outflow tract: a systematic review and meta-analysis. Pacing Clin Electrophysiol. 2014;37(1):73–78. doi:10.1111/pace.12243
39. De Bruin ML, Langendijk PN, Koopmans RP, Wilde AA, Leufkens HG, Hoes AW. In-hospital cardiac arrest is associated with use of non-antiarrhythmic QTc-prolonging drugs. Br J Clin Pharmacol. 2007;63(2):216–223. doi:10.1111/j.1365-2125.2006.02722.x
40. Willems S, Tilz RR, Steven D, et al. Preventive or deferred ablation of ventricular tachycardia in patients with ischemic cardiomyopathy and implantable defibrillator (Berlin VT): a multicenter randomized trial. Circulation. 2020;141(13):1057–1067. doi:10.1161/CIRCULATIONAHA.119.044283
41. Li Y, Hu T, Lin M, et al. Comparison of efficacy and safety between dronedarone and amiodarone used during the blind period in patients with atrial fibrillation after catheter ablation. Clin Pharmacol. 2023;15:113–123. doi:10.2147/CPAA.S440704
42. Porta-Sánchez A, Ha ACT, Wang X, et al. Health care utilization after ventricular tachycardia ablation: a propensity score-matched cohort study. Can J Cardiol. 2019;35(2):169–177. doi:10.1016/j.cjca.2018.10.011
43. Chen Y, Gomes M, Garcia JV, et al. Cost-effectiveness of ablation of ventricular tachycardia in ischaemic cardiomyopathy: limitations in the trial evidence base. Open Heart. 2020;7(1):e001155. doi:10.1136/openhrt-2019-001155
44. Efremidis M, Letsas KP, Sideris A, et al. Reversal of premature ventricular complex-induced cardiomyopathy following successful radiofrequency catheter ablation. Europace. 2008;10(6):769–770. doi:10.1093/europace/eun060
45. Liao JM, Lin -C-CC. Private health insurance in Taiwan: insights from the US medicare program. Perm J. 2025;29(3):111–113. doi:10.7812/TPP/25.064
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.