Back to Journals » Infection and Drug Resistance » Volume 15
Long-Term Outcome of Treatment with 2% Topical Ganciclovir Solution in Cytomegalovirus Anterior Uveitis and Corneal Endotheliitis
Authors Chen PJ, Lin IH, Chi YC, Lai CC, Hung JH, Tseng SH, Huang YH ![]()
Received 20 April 2022
Accepted for publication 24 June 2022
Published 29 June 2022 Volume 2022:15 Pages 3395—3403
DOI https://doi.org/10.2147/IDR.S370905
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Po-Jui Chen,1 I-Huang Lin,1 Yi-Chun Chi,2 Chun-Chieh Lai,1 Jia-Horung Hung,1 Sung-Huei Tseng,1 Yi-Hsun Huang1
1Department of Ophthalmology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 2Department of Ophthalmology, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan
Correspondence: Yi-Hsun Huang, Department of Ophthalmology, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan, Email [email protected]
Abstract:
Purpose: This study aimed to evaluate the therapeutic efficacy and long-term outcomes of treatment with topical 2% ganciclovir solution in immunocompetent patients with aqueous humor polymerase chain reaction (PCR)-proven cytomegalovirus (CMV) anterior uveitis and corneal endotheliitis.
Methods: We retrospectively reviewed the findings for immunocompetent patients diagnosed with CMV uveitis or endotheliitis based on clinical manifestations and polymerase chain reaction (PCR) examination results and treated with topical 2% ganciclovir solution at National Cheng Kung University Hospital. Clinical outcome measurements included evaluations of the response rate, relapses, resolution of anterior chamber inflammation, visual acuity, and intraocular pressure.
Results: The study included 38 eyes of 32 patients. Long-term administration of topical 2% ganciclovir significantly decreased keratic precipitates (p = 0.001), anterior chamber cells (p = 0.001), and reduced intraocular pressure (p < 0.001). Only one eye was unresponsive to topical ganciclovir treatment, and the recurrence decreased to 0.13 relapses per year. The presence of keratic precipitates and higher intraocular pressure at the initial presentation were significantly associated with recurrence (p = 0.036 and p = 0.001, respectively).
Conclusions:: Long-term use of topical 2% ganciclovir solution is effective, safe, and applicable when commercialized ganciclovir gel is not available.
Keywords: cytomegalovirus, endotheliitis, ganciclovir, uveitis
Introduction
Cytomegalovirus (CMV) ophthalmic infection has been identified as an etiological factor for Posner-Schlossman syndrome (PSS), Fuchs heterochromic iridocyclitis, retinitis, corneal uveitis, and endotheliitis.1–8 CMV infections involving the anterior segment are characterized by blurred vision, inflammation in the anterior chamber, the presence of keratic precipitates (KP), elevated intraocular pressure (IOP), and corneal endothelial cell damage.1,4
At present, the treatment for CMV anterior uveitis and endotheliitis involves the continuous application of antiviral agents. Since systemic antiviral therapies are associated with various adverse reactions, recent studies have recommended treatment with topical antiviral agents as initial and maintenance therapy to address the high recurrence rates.9,10 In this regard, ganciclovir gel (0.15%, Zirgan®) was approved for acute herpetic keratitis with dendritic ulcers by the US Food and Drug Administration (FDA) in 2009 and was also reported to be eligible for CMV ocular infections in previous studies.11–13 Koizumi et al showed that all CMV patients responded to 0.15% ganciclovir gel,12 and Pavan-Langston et al reported a case refractory to systemic antiviral therapy that improved after application of topical 0.15% ganciclovir gel at 2-h intervals.14 However, 0.15% ganciclovir gel is not available in many countries, including Taiwan. Clinically, a topical 2% ganciclovir solution has been used as a substitute for commercialized ganciclovir gel. However, the long-term efficacy of topical 2% ganciclovir has not been fully studied. Therefore, in this study, we aimed to investigate the long-term efficacy, safety, and predictive factors for CMV uveitis and endotheliitis recurrence treated with 2% ganciclovir solution therapy.
Method
Patient Selection
This retrospective study was approved by the Institutional Review Board of the National Cheng Kung University Hospital (NCKUH). The informed consents were obtained from the study participants prior to the study commencement. Anterior chamber tapping was performed in patients with suspected CMV infection, and the aqueous samples were subjected to polymerase chain reaction (PCR) for analysis of herpes simplex virus (HSV), varicella-zoster virus (VZV), Epstein–Barr virus (EBV), and CMV. We retrospectively reviewed the medical records of patients with positive PCR results for aqueous CMV who had been treated with 2% ganciclovir solution between April 2012 and April 2021 at NCKUH, Tainan, Taiwan.
Inclusion and Exclusion Criteria
All patients were immunocompetent, diagnosed with CMV uveitis or endotheliitis with positive PCR results for the aqueous humor, and treated with 2% ganciclovir solution during initial and maintenance therapy. Patients with a follow-up duration of at least one year were included in the study. We excluded patients showing concurrent infection with HSV, VZV, or EBV and who were lost to follow-up for more than one year.
Treatment Protocol
All patients were treated with 2% ganciclovir solution prepared with intravenous ganciclovir and sterile distilled water. The storage condition of 2% ganciclovir solution was at a temperature between 2°C~8°C, sun exposure should be avoided, and the expiration date was 3 months. The 2% ganciclovir solution treatment was initiated at a dosage frequency of 2 h. The frequency was modified according to the clinical response and maintained at four times daily. Topical steroids (1% prednisolone, 0.1% betamethasone, or 0.1% fluorometholone) and anti-glaucoma medications (carbonic anhydrase inhibitors, alpha-2 adrenergic agonists, or beta-blockers) were prescribed based on the clinical presentation. Similar to previous study,15 if anterior chamber inflammation improved compared to last visit and IOP reduced below 21 mmHg, topical steroids were tapered off according to the clinical response and were finally stopped.
Outcome Measurements
In this study, we set patients to be followed up every three months during maintenance therapy. The follow-up endpoint and primary outcomes were the response to antiviral therapy, resolution of anterior chamber inflammation, intraocular pressure, and the cumulative relapses at the final visit. Response was defined as the resolution of anterior chamber inflammation, including reduction of the anterior chamber cell count, KP, and IOP. Recurrence was defined according to the Standardization of Uveitis Nomenclature (SUN) working group, which was defined as repeated episodes of active inflammation (two-step increase in the level of inflammation or increase from grade 3 to 4), corneal edema, endothelial KP, and elevated IOP separated by periods of 3 months.16 Patients with relapses during maintenance therapy would be classified into the recurrence group. Secondary outcomes were measured using changes in corrected-distance visual acuity (CDVA). All adverse effects were recorded.
Statistical Analysis
Statistical analysis was performed using Statistical Product and Service Solutions (SPSS) software, version 17 (IBM, Armonk, NY, USA). Data are presented as mean ± standard deviation (SD) for quantitative variables and frequencies for categorical variables. Quantitative variables were compared using the independent t-test, paired t-test, and Mann–Whitney U-test. Categorical variables were evaluated using the chi-squared test and McNemar’s test. P values less than 0.05 indicated statistical significance.
Results
Forty-four patients tested positive for CMV in the aqueous humor and were regularly followed up. All patients were treated with a topical 2% ganciclovir solution after diagnosis. Seven patients underwent follow-up assessments for less than one year. One patient each showed concurrent infections with VZV and HSV in the PCR results for the aqueous humor. Two patients were initially treated with oral antiviral medication without a topical 2% ganciclovir solution. One patient with CMV retinitis was immunocompromised and treated with Humira. These patients were excluded to obtain the long-term outcomes of topical 2% ganciclovir solution in isolated CMV anterior uveitis and endotheliitis.
Thirty-two immunocompetent patients with 38 affected eyes were enrolled, and 38 infected eyes were included in this study. The patients’ characteristics are listed in Table 1. Disease recurrence was reported in 17 eyes (44.7%). The study population included 28 male participants (73.7%), and the mean age at diagnosis was 55.68 ± 12.43 years (range, 36 to 83 years). The mean follow-up duration was 45.68 ± 28.47 months (range, 12–105 months). CMV uveitis was diagnosed in 34 eyes (89.5%), and CMV endotheliitis was diagnosed in 4 eyes (10.5%).
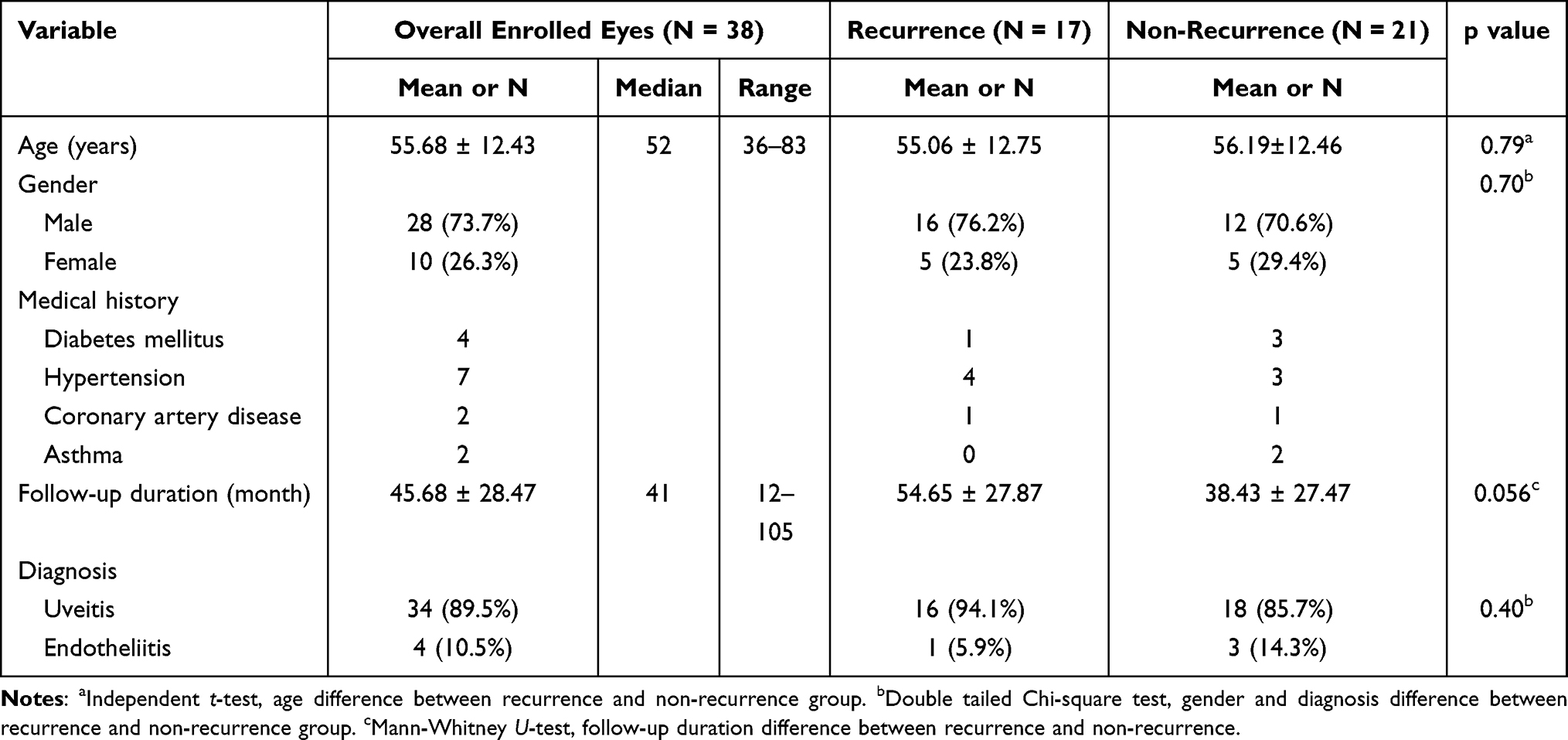 |
Table 1 Patient Demographics |
Comparisons of characteristics between the recurrence and non-recurrence groups are summarized in Table 1. The recurrence and non-recurrence groups showed no significant differences in age (p = 0.79), sex (p = 0.70), follow-up period (p = 0.056), and diagnosis (p = 0.40 in uveitis and endotheliitis). At baseline, most patients reported at least 1–2 uveitis or endotheliitis episodes per year.
As shown in Table 2, the CDVA was 0.41 ± 0.27 (logMAR, ranging from 0 to 1.1), and the cell amount was 1.14 ± 0.73 (+, ranging from 0 to 2) at initial diagnosis. KP was present in 83% of infected eyes. The mean IOP was 27.67 ± 12.46 (mmHg, ranging from 12 to 60). The most affected eyes were treated with topical steroids (86.8%) and topical IOP-lowering agents (84.2%). Only a small proportion of eyes were prescribed systemic IOP-lowering medications, including oral acetazolamide (26.3%) and intravenous mannitol (18.8%).
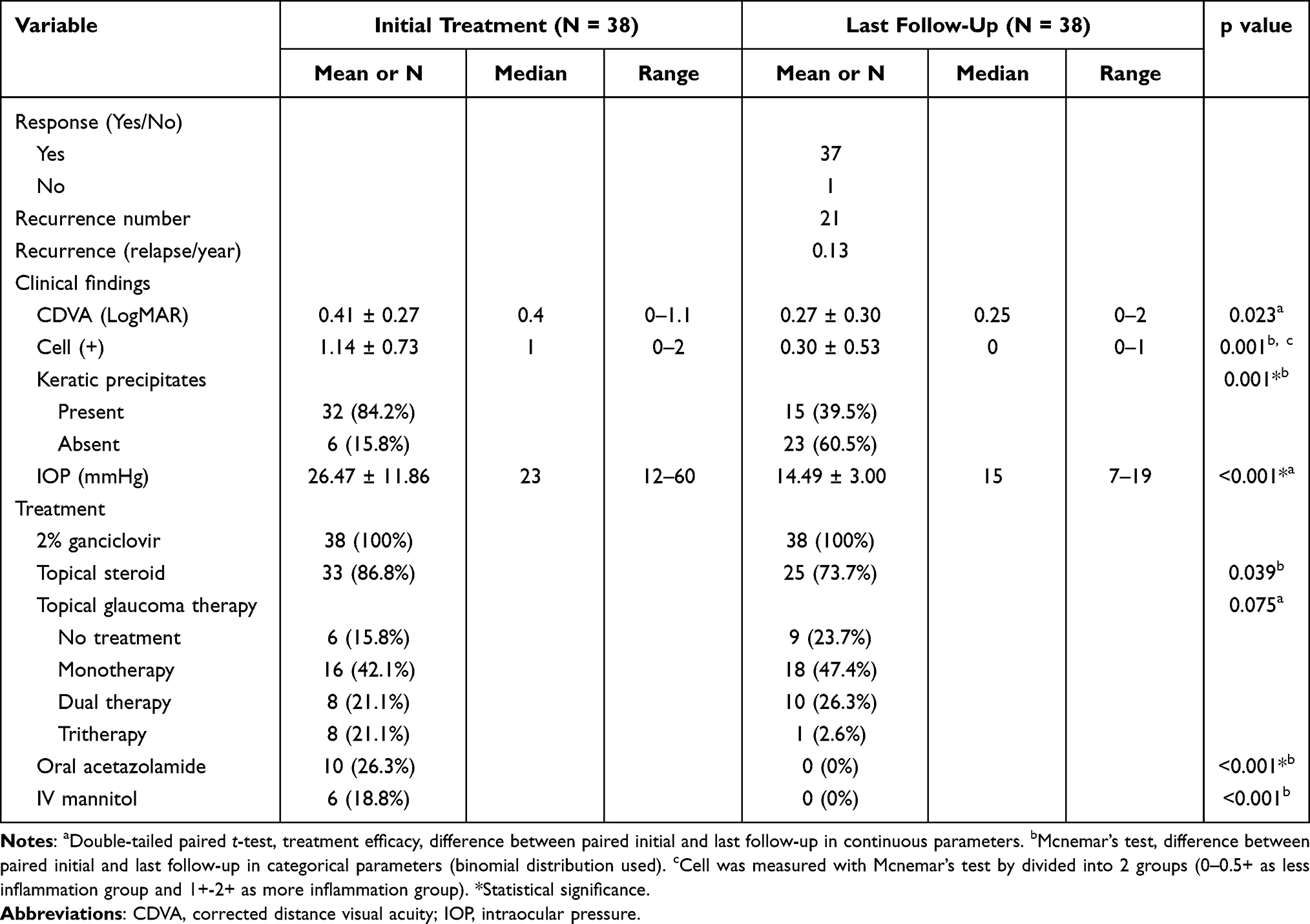 |
Table 2 Treatment Outcomes: Comparison of Primary and Secondary Outcome Parameters in Initial Treatment and Last Follow-Up |
At the last follow-up, only one uveitic eye was unresponsive to topical 2% ganciclovir solution and required further surgical intervention with trabeculectomy. Another eye underwent trabeculectomy due to intractable ocular hypertension when the disease relapsed 19 months after initiation of topical ganciclovir treatment. Both patients showed no episodes of IOP spikes after trabeculectomy. One patient with CMV endotheliitis experienced corneal decompensation and subsequently underwent keratoplasty. AC inflammation parameters and treatment modalities were compared between the time of diagnosis and last follow-up (Table 2). By the last follow-up, there were 21 relapses and 0.13 relapses/year, and significant differences were observed in KP resolution (p < 0.001), the decrease in IOP (p < 0.001), and a reduction in the use of oral acetazolamide (p = 0.008).
The results of the recurrence analysis are shown in Table 3. We attempted to identify the predictive parameters for recurrence by comparing the initial parameters between the recurrence and non-recurrence groups. Only the initial presence of KP and a higher IOP were significantly different (p = 0.036 and p = 0.03, respectively). Adverse effects of ganciclovir treatment were also recorded. One patient had punctate epithelial erosion, which was suspected to be related to ganciclovir toxicity, and one patient had allergic conjunctivitis of uncertain etiology.
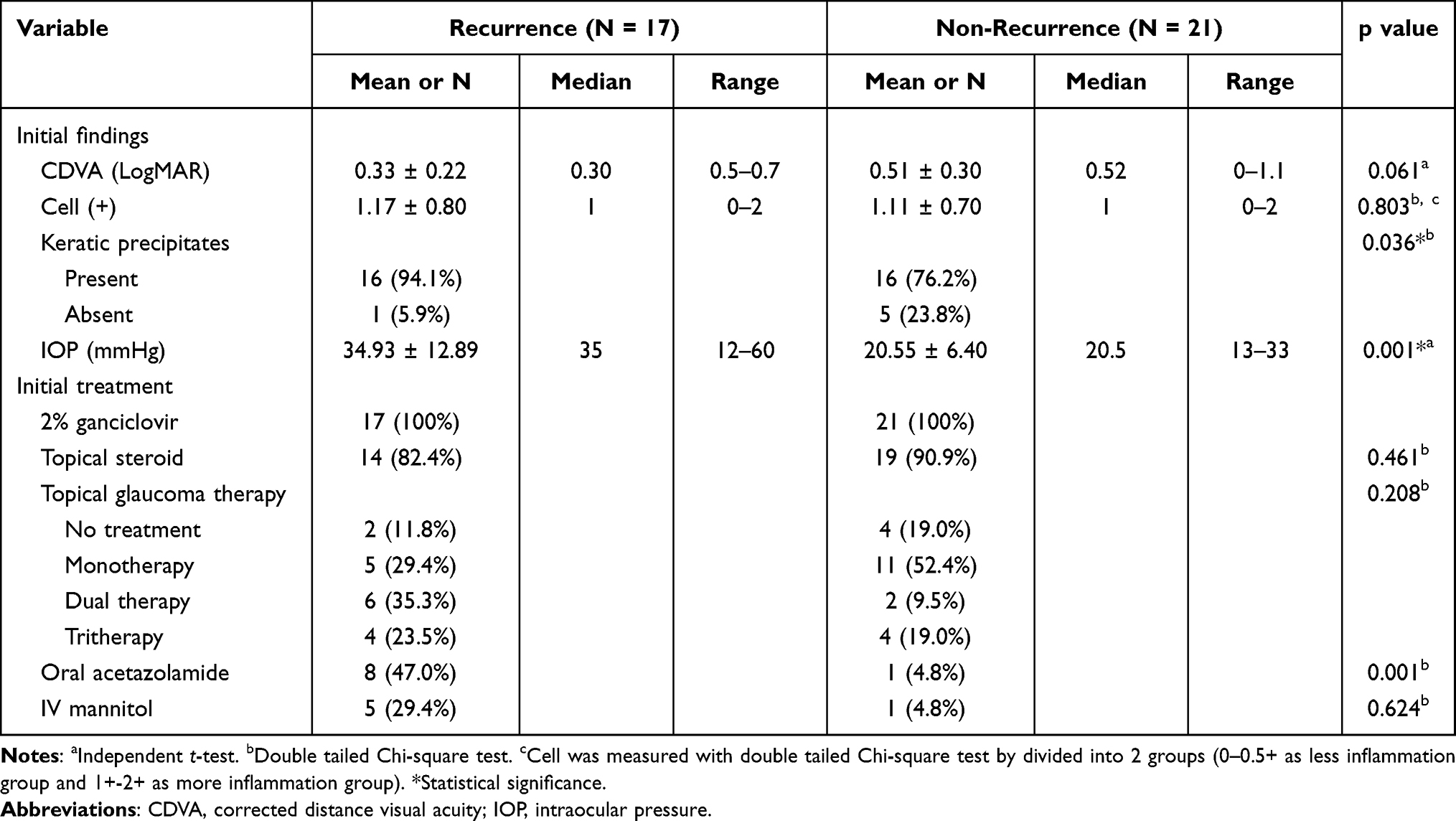 |
Table 3 Recurrence Analysis: Comparison of Initial Findings in Recurrence and Non-Recurrence Group |
Discussion
In this study, we used topical 2% ganciclovir solution that was initiated at a frequency of 2 h and maintained at 4 times daily, similar to a previous study.17 Using a literature review, we have summarized the findings of previous studies that evaluated topical 2% ganciclovir solution therapy (Table 4). In comparison with previous reports, our study had the longest follow-up period and the lowest rate of relapses per year with long-term efficacy and recurrence analysis of topical 2% ganciclovir in aqueous PCR-proven CMV infection.
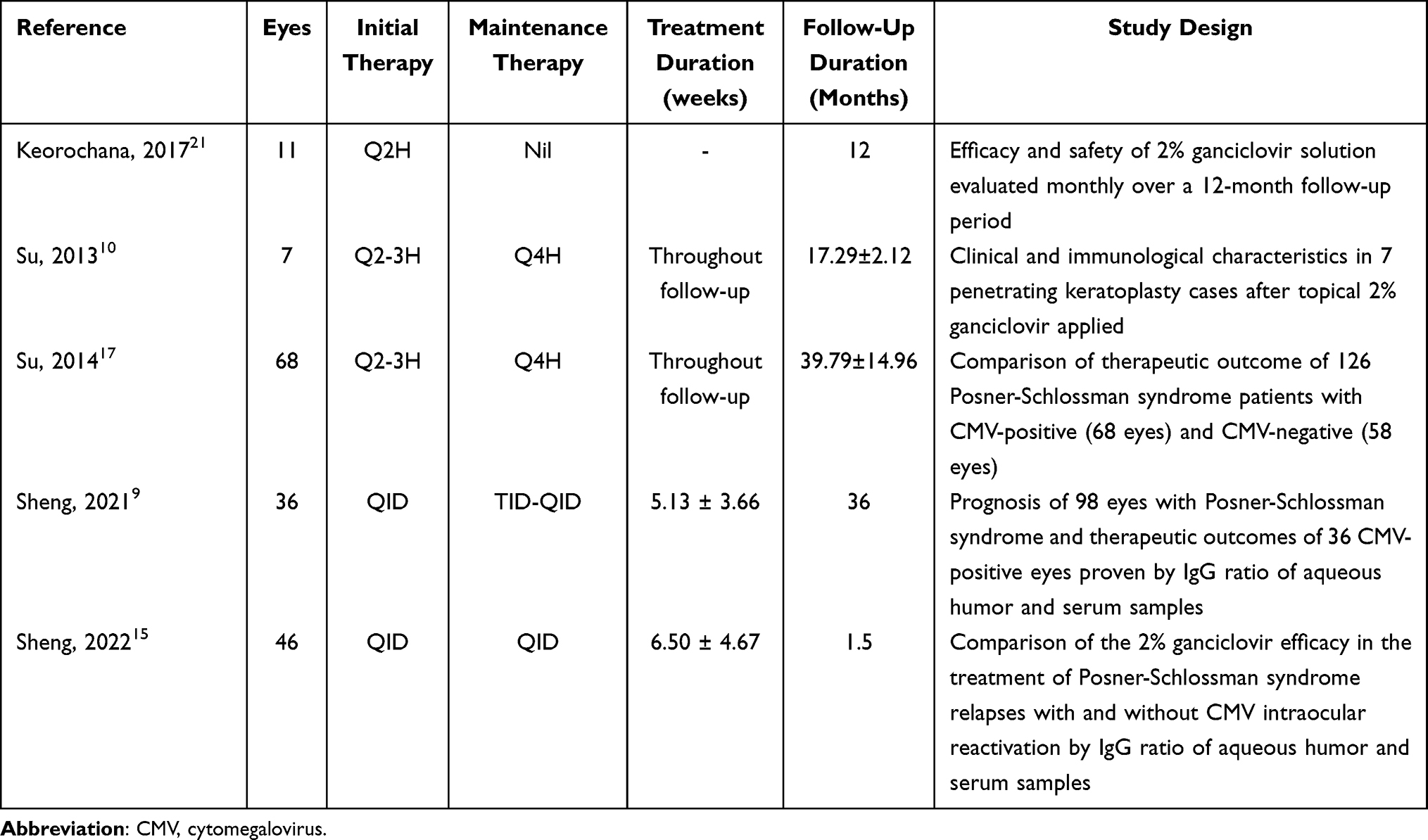 |
Table 4 Literature Review of Topical 2% Ganciclovir Solution in Patients with CMV Anterior Segment Infection |
CMV infection recurrence has been mentioned in several studies, especially when antiviral therapy was discontinued.13,18 In this study, we reported 21 relapses with a total follow-up duration of 1736 months, with 0.13 relapses per year on average. Accorinti et al reported 23 relapses over 714 months of follow-up,19 while Wong et al reported 0.88 episodes per person-year.11 The better results obtained in our study may be due to the long-term application of topical antiviral therapy, but considering the small sample size, the results need to be confirmed in further large-scale studies to obtain more reliable conclusions. The recurrence episodes decreased significantly, and the repeated relapses after antiviral therapy might be attributable to the virostatic rather than the virucidal effect of ganciclovir.13 Moreover, the recurrence could have resulted from the low intracameral inhibitory dose when topical ganciclovir was titrated.12,20 Keorochana et al reported that the recurrence group tended to be present with poorer visual acuity, fewer cells, and more KP, but the differences failed to reach statistical significance.21 In our study, significant differences were observed in the presence of KP and elevation of IOP in recurrence group. However, contrary to a previous study,21 we found that patients with more anterior chamber cells tended to experience recurrence. Therefore, elimination of CMV anterior segment infection remains a challenge, but the reduction of relapse episodes is proof of efficacy, and long-term application of antiviral therapy for virostatic effects still remains the current consensus for CMV uveitis and endotheliitis treatment.15,22
To better understand CMV treatment, we reviewed the findings obtained for previous treatment modalities and outcomes other than topical ganciclovir solution (Table 5). Systemic ganciclovir and valganciclovir treatment is known to cause infertility and bone marrow suppression and can result in severe neutropenia or thrombocytopenia.23 In contrast, topical ganciclovir is less toxic and has shown no obvious side effects.11,21 Thus, topical ganciclovir has been reported to be a safe treatment modality and can ensure better compliance due to the non-invasive nature of treatment and the convenient mode of application. Although oral valaciclovir has been reported to be a successful treatment option for CMV anterior uveitis by Sira and Murray,24 no consensus has been achieved for the use of valaciclovir in patients with CMV. Most studies still focus on the outcomes of oral valganciclovir or different modalities of ganciclovir as antiviral therapy.3,11,13,17,18,25–28 Van Boxtel et al reported five cases of CMV uveitis that were successfully treated with oral valganciclovir for 3 to 12 months.3 Sobolewska et al showed favorable results with combination therapy using topical ganciclovir ophthalmic 0.15% gel (Zirgan®) and oral valganciclovir for a mean duration of 20 months.27 Harada et al used oral valganciclovir followed by 1% ganciclovir eye drops due to the unavailability of the 0.15% gel in Japan.29 Markomichelakis et al reported two cases of acyclovir-resistant CMV uveitis that were controlled by oral ganciclovir without recurrence.26 Treatment with intravitreal ganciclovir injection has also been reported, and it showed reduction of CMV DNA copies and resolution of anterior chamber inflammation.28 Chee et al reviewed four types of ganciclovir therapy, including intravenous, implant, intravitreal, and gel (0.15%, Zirgan® gel), and noted responses in 36 out of 47 patients.13 Among the treatments, intravitreal injection of ganciclovir was not suggested due to the higher rate of treatment failure. Meanwhile, a relatively lower recurrence rate was found in the topical ganciclovir gel group.13 Foscarnet was also applied and but was limited to cases with CMV retinitis.25
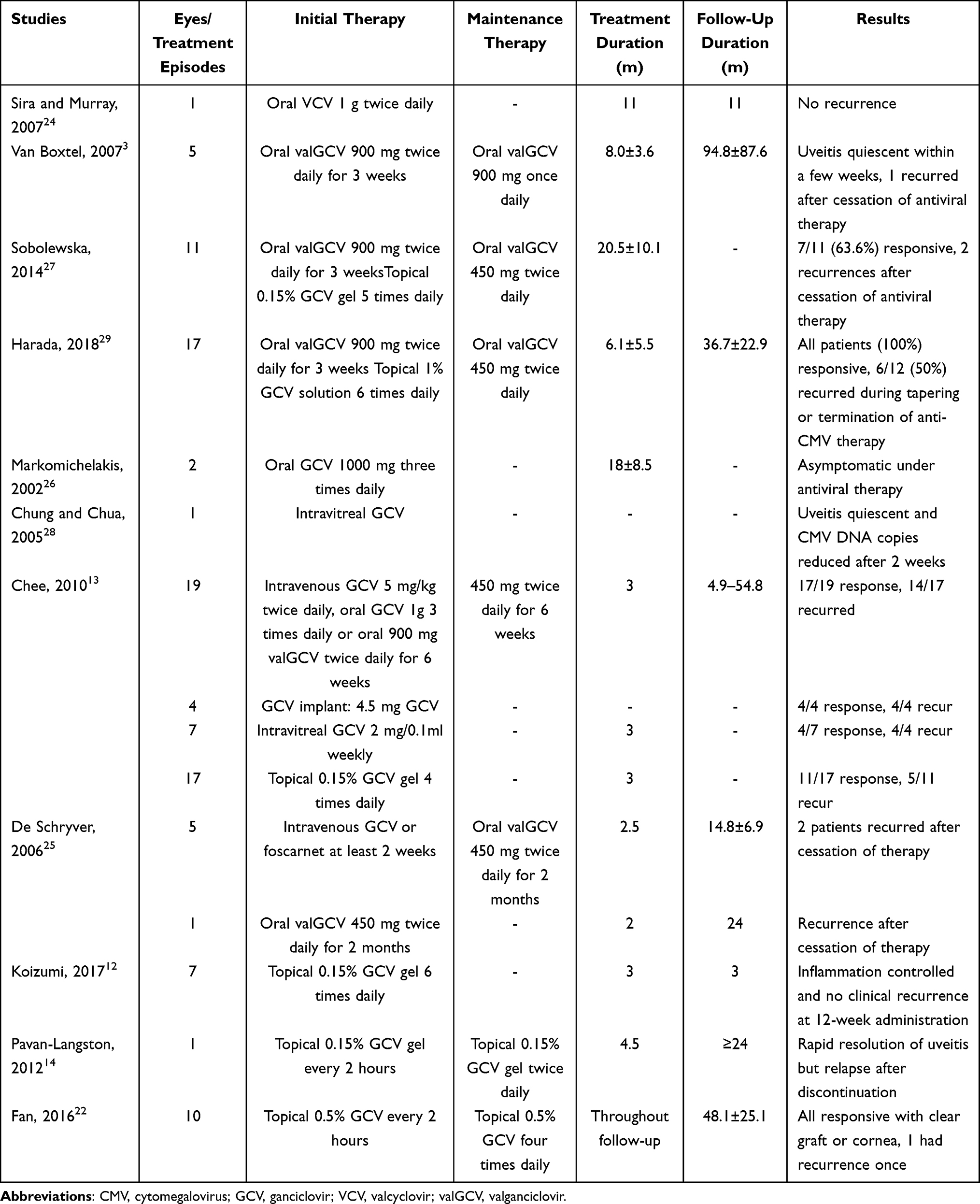 |
Table 5 Literature Review of Other CMV Treatment Modalities and Outcomes |
Although our study revealed promising therapeutic and preventive effects of topical 2% ganciclovir solution, the retrospective nature of the study was a limitation, and the parameters for the analysis were also limited. Moreover, NCKUH is a tertiary referral medical center, and patients who had more complicated symptoms or were refractory to prior treatments at local ophthalmic clinics were referred to this center, which may have resulted in a selection bias. Furthermore, previous study has demonstrated the correlation between viral load and IOP, number of glaucoma medications, and future recurrences.30 However, in this retrospective study, the viral load was not routinely examined in all patients. Besides, we performed paracentesis only once for diagnosis, and no further data from aqueous tapping were obtained to evaluate the therapeutic intracameral level of 2% ganciclovir solution. However, all our patients had PCR-positive results, completed at least one year of follow-up, and had the longest follow-up period in the literature; therefore, the results can be expected to contribute to the current body of knowledge regarding the treatment of CMV infections.
In summary, the long-term application of topical 2% ganciclovir solution was effective, safe, and non-inferior to other treatment modalities. This might be a treatment option when commercialized topical ganciclovir gel is not available. Further large-scale prospective studies are required to evaluate the long-term efficacy and safety of topical 2% ganciclovir solution.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Ministry of Science and Technology Grant (MOST 110-2628-B-006 −018). The sponsor or funding organization had no role in the design or conduct of this research.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chee S-P, Bacsal K, Jap A, Se-Thoe S-Y, Cheng CL, Tan BH. Clinical features of cytomegalovirus anterior uveitis in immunocompetent patients. Am J Ophthalmol. 2008;145(5):834–840.e831. doi:10.1016/j.ajo.2007.12.015
2. Koizumi N, Suzuki T, Uno T, et al. Cytomegalovirus as an etiologic factor in corneal endotheliitis. Ophthalmology. 2008;115(2):292–297.e293. doi:10.1016/j.ophtha.2007.04.053
3. van Boxtel LAA, van der Lelij A, van der Meer J, Los LI. Cytomegalovirus as a cause of anterior uveitis in immunocompetent patients. Ophthalmology. 2007;114(7):1358–1362. doi:10.1016/j.ophtha.2006.09.035
4. Woo JH, Lim WK, Ho SL, Teoh SC. Characteristics of cytomegalovirus uveitis in immunocompetent patients. Ocul Immunol Inflamm. 2015;23(5):378–383. doi:10.3109/09273948.2014.950384
5. Carmichael A. Cytomegalovirus and the eye. Eye. 2012;26(2):237–240. doi:10.1038/eye.2011.327
6. Park SW, Yu HG. Association of cytomegalovirus with idiopathic chronic anterior uveitis with ocular hypertension in Korean patients. Ocul Immunol Inflamm. 2013;21(3):192–196. doi:10.3109/09273948.2012.754908
7. Chee S-P, Bacsal K, Jap A, Se-Thoe S-Y, Cheng CL, Tan BH. Corneal endotheliitis associated with evidence of cytomegalovirus infection. Ophthalmology. 2007;114(4):798–803. doi:10.1016/j.ophtha.2006.07.057
8. Bloch-Michel E, Dussaix E, Cerqueti P, Patarin D. Possible role of cytomegalovirus infection in the etiology of the Posner-Schlossman syndrome. Int Ophthalmol. 1987;11(2):95–96. doi:10.1007/BF00136737
9. Sheng Q, Zhai R, Fan X, Kong X. The analysis of dynamic changes and prognosis of Posner-Schlossman syndrome with cytomegalovirus infection and antiviral therapy. J Ophthalmol. 2021;2021:6687929. doi:10.1155/2021/6687929
10. Su CC, Wang IJ, Chen WL, Lin CP, His B, Hu FR. Topical ganciclovir treatment in patients with cytomegalovirus endotheliitis receiving penetrating keratoplasty. Clin Exp Ophthalmol. 2013;41(4):339–347. doi:10.1111/j.1442-9071.2012.02888.x
11. Wong JXH, Agrawal R, Wong EPY, Teoh SC. Efficacy and safety of topical ganciclovir in the management of cytomegalovirus (CMV)-related anterior uveitis. J Ophthalmic Inflamm Infect. 2016;6(1):10. doi:10.1186/s12348-016-0078-z
12. Koizumi N, Miyazaki D, Inoue T, et al. The effect of topical application of 0.15% ganciclovir gel on cytomegalovirus corneal endotheliitis. Br J Ophthalmol. 2017;101(2):114. doi:10.1136/bjophthalmol-2015-308238
13. Chee SP, Jap A. Cytomegalovirus anterior uveitis: outcome of treatment. Br J Ophthalmol. 2010;94(12):1648–1652. doi:10.1136/bjo.2009.167767
14. Pavan-Langston D, Welch CL, Zegans ME. Ganciclovir gel for cytomegalovirus keratouveitis. Ophthalmology. 2012;119(11):2411. doi:10.1016/j.ophtha.2012.07.024
15. Sheng Q, Zhai R, Fan X, Kong X. 2% ganciclovir eye drops control Posner-Schlossman syndrome relapses with/without cytomegalovirus intraocular reactivation. Front Med. 2022;9:848820. doi:10.3389/fmed.2022.848820
16. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of uveitis nomenclature working G. standardization of uveitis nomenclature for reporting clinical data. Results of the first international workshop. Am J Ophthalmol. 2005;140(3):509–516.
17. Su -C-C, Hu F-R, Wang T-H, et al. Clinical outcomes in cytomegalovirus-positive Posner-Schlossman syndrome patients treated with topical ganciclovir therapy. Am J Ophthalmol. 2014;158(5):1024–1031.e1022. doi:10.1016/j.ajo.2014.08.007
18. Mietz H, Aisenbrey S, Ulrich bartz-schmidt K, Bamborschke S, Krieglstein GK. Ganciclovir for the treatment of anterior uveitis. Graefes Arch Clin Exp Ophthalmol. 2000;238(11):905–909. doi:10.1007/s004170000193
19. Accorinti M, Gilardi M, Pirraglia MP, et al. Cytomegalovirus anterior uveitis: long-term follow-up of immunocompetent patients. Graefes Arch Clin Exp Ophthalmol. 2014;252(11):1817–1824. doi:10.1007/s00417-014-2782-4
20. Waduthantri S, Zhou L, Chee S-P. Intra-cameral level of ganciclovir gel, 0.15% following topical application for cytomegalovirus anterior segment infection: a pilot study. PLoS One. 2018;13(1):e0191850–e0191850. doi:10.1371/journal.pone.0191850
21. Keorochana N, Choontanom R. Efficacy and safety of an extemporaneous preparation of 2% ganciclovir eye drops in CMV anterior uveitis. BMJ Open Ophthalmol. 2017;2(1):e000061. doi:10.1136/bmjophth-2016-000061
22. Fan NW, Chung YC, Liu YC, Liu CJ, Kuo YS, Lin PY. Long-term topical ganciclovir and corticosteroids preserve corneal endothelial function in cytomegalovirus corneal endotheliitis. Cornea. 2016;35(5):596–601. doi:10.1097/ICO.0000000000000791
23. Upadhyayula S, Michaels MG, Ganciclovir F. Cidofovir: antiviral drugs not just for cytomegalovirus. J Pediatric Infect Dis Soc. 2013;2(3):286–290. doi:10.1093/jpids/pit048
24. Sira M, Murray PI. Treatment of cytomegalovirus anterior uveitis with oral valaciclovir. Ocul Immunol Inflamm. 2007;15(1):31–32. doi:10.1080/09273940601174038
25. de Schryver I, Rozenberg F, Cassoux N, et al. Diagnosis and treatment of cytomegalovirus iridocyclitis without retinal necrosis. Br J Ophthalmol. 2006;90(7):852. doi:10.1136/bjo.2005.086546
26. Markomichelakis NN, Canakis C, Zafirakis P, Marakis T, Mallias I, Theodossiadis G. Cytomegalovirus as a cause of anterior uveitis with sectoral iris atrophy. Ophthalmology. 2002;109(5):879–882. doi:10.1016/S0161-6420(02)00961-2
27. Sobolewska B, Deuter C, Doycheva D, Zierhut M. Long-term oral therapy with valganciclovir in patients with Posner-Schlossman syndrome. Graefes Arch Clin Exp Ophthalmol. 2014;252(1):117–124. doi:10.1007/s00417-013-2535-9
28. Chung RSH, Chua CN. Intravitreal ganciclovir injections in aqueous cytomegalovirus DNA positive hypertensive iritis. Eye. 2006;20(9):1080. doi:10.1038/sj.eye.6702112
29. Harada Y, Fukuda K, Nakahira A, Tada K, Sumi T, Fukushima A. Requirement of longer term antiviral therapy in patients with cytomegalovirus anterior uveitis with corneal endothelial cell damage. Clin Ophthalmol. 2018;12:1311. doi:10.2147/OPTH.S164184
30. Kandori M, Miyazaki D, Yakura K, et al. Relationship between the number of cytomegalovirus in anterior chamber and severity of anterior segment inflammation. Jpn J Ophthalmol. 2013;57(6):497–502. doi:10.1007/s10384-013-0268-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.