Back to Journals » Journal of Pain Research » Volume 15
Long-Term Clinical Results of Percutaneous Cervical Nucleoplasty for Cervical Radicular Pain: A Retrospective Cohort Study
Authors de Rooij JD, Gadjradj PS, Aukes H, Groeneweg G, Speksnijder CM, Huygen FJ
Received 26 January 2022
Accepted for publication 6 April 2022
Published 17 May 2022 Volume 2022:15 Pages 1433—1441
DOI https://doi.org/10.2147/JPR.S359512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishnan Chakravarthy
Judith Divera de Rooij,1,2 Pravesh Shankar Gadjradj,3 Hans Aukes,4 George Groeneweg,1 Caroline Margina Speksnijder,5 Frank Johannes Huygen1
1Department of Anesthesiology, Center for Pain Medicine, Erasmus MC University Medical Center, Rotterdam, the Netherlands; 2Department of Orthopedics, Physiotherapy Unit, Erasmus MC University Medical Center, Rotterdam, the Netherlands; 3Department of Neurological Surgery, Weill Cornell Brain and Spine Center, New York-Presbyterian Hospital, New York, NY, USA; 4Department of Anesthesiology, Albert Schweitzer Hospital, Dordrecht, the Netherlands; 5Department of Oral and Maxillofacial Surgery, Utrecht Medical Center, Utrecht, the Netherlands
Correspondence: Judith Divera de Rooij, Department of Anesthesiology, Center for Pain Medicine, Erasmus MC University Medical Center, Dr. Molenwaterplein 40, Rotterdam, 2040 CA, the Netherlands, Tel +31 (010) 704 01 40, Email [email protected]
Purpose: Percutaneous cervical nucleoplasty (PCN) is a minimally invasive treatment for cervical radicular pain due to a disc herniation. Preliminary results show equivalent patient-reported outcomes of PCN as compared to conventional anterior cervical discectomy. However, there is a paucity of long-term outcome data. Therefore, the primary objective of this study is to investigate the long-term clinical results of PCN.
Patients and Methods: A retrospective analysis was conducted on patients who underwent PCN at a secondary referral center between 2010 and 2014. Before surgery and five days after surgery, numeric rating scales (NRS) for arm pain and neck pain and data on complications were collected. To determine long-term follow-up outcomes, patients were sent a questionnaire booklet containing the Core Outcome Measures Index-Neck (COMI-Neck), NRS for arm pain and neck pain, Likert-scales on patient satisfaction and questions regarding the incidence of reoperations and complications.
Results: The baseline characteristics were collected for 158 patients. At a median follow-up of 41.5 months (interquartile range (IQR) 27.0 to 57.5), data were available for 118 patients (74.7%). At short-term follow-up, patients that underwent PCN had a mean decrease of 3.0 on the NRS for arm pain (95% CI 2.5 to 3.6) compared to baseline, while at long-term follow-up, a mean decrease of 2.8 (95% CI 1.0 to 3.6) was observed. At the long-term follow-up, 67.8% of the patients were fully recovered from all symptoms and 93.3% remained satisfied with the PCN treatment results. The reoperation rate for recurrent disc herniation was 21.4% at long-term follow-up.
Conclusion: PCN appears to be a safe and effective treatment at short-term and long-term follow-up of a specific selection of cervical herniated discs, with an acceptable long-term reoperation rate. These study results suggest a potential role of PCN as a less invasive treatment option for cervical radicular pain due to a soft disc herniation, before anterior cervical discectomy should be considered.
Keywords: percutaneous cervical nucleoplasty, minimally invasive treatment, cervical radicular pain
Introduction
Symptomatic herniated cervical discs cause neck and radiating arm pain as a result of compression of the cervical spinal nerve.1 Cervical radicular pain has a high impact on the patient’s quality of life2 and the natural course appears to be favourable.3 At six months, 42% of the patients who received conservative treatment recovered from neck pain and 59% of the patients reported no or only slight arm pain.3 At 12 months, almost 50% of the patients recovered from both neck and arm pain.3 When the severe pain persists and does not improve with conservative care, surgery may be considered.
In the 1940s and the 1950s the posterior cervical foraminotomy and the anterior cervical discectomy with fusion (ACDF) techniques were developed to treat cervical disc herniation.4 ACDF is nowadays the preferred technique to treat symptomatic cervical disc herniation,5,6 however two recent trials revealed that anterior cervical discectomy (ACD) seems to achieve similar results as ACDF.6,7 Although ACDF is a safe and effective procedure to treat cervical radicular pain, rare but potentially dangerous risks can occur during or after surgery such as oesophageal injury, postoperative hematoma and mortality.8–10 To reduce these risks of surgery, new minimally invasive techniques and instruments for spine surgery have been developed in the last two decades.11 Compared to conventional anterior open methods, these minimally invasive techniques in spine surgery have several advantages such as smaller incisions, less soft tissue injury, shorter hospital stay, less blood loss and faster return to normal daily activities.11–13 One of the minimally invasive techniques that could potentially answer this need is percutaneous cervical nucleoplasty (PCN). PCN uses coblation technology for ablating and coagulating the soft tissue of the herniated disc.14,15 Strict patient selection, however, is important for a successful outcome after PCN.16,17 In particular, patients with minimally degenerated discs, the absence of central canal stenosis, and unilateral radicular pain will benefit most from this procedure.16,17
PCN is an effective and safe technique in the reduction of pain in patients with cervical radicular pain due to a disc herniation.16,18–21 The efficacy of PCN has been demonstrated from two months up to two years of follow-up.16,18–21 Long-term evidence on the effectiveness and safety of PCN, however, is lacking. Therefore, the primary objective of this retrospective cohort study was to evaluate the clinical long-term effects of PCN on arm pain in patients with cervical radicular pain due to disc herniation. The secondary aim was to evaluate long-term function, symptom-specific well-being, quality of life, disability and patient satisfaction in patients with cervical radicular pain due to disc herniation.
Materials and Methods
Patient Population and Indication
Consecutive patients who received PCN for cervical radicular pain due to a contained soft disc herniation between 2010 and 2014 were included in this single-center retrospective cohort study at Albert Schweitzer Hospital, Dordrecht, the Netherlands. Before referral for a PCN-procedure, patients were evaluated by a neurologist. In the work-up, patients underwent an MRI-scan of their cervical spine and a conventional X-ray aside from neurological examination. In order to be eligible for PCN, patients had to satisfy the following inclusion criteria: (1) have cervical radicular pain due to disc herniation, which did not respond to conservative treatment; (2) have an MRI-confirmed contained, soft disc herniation at levels C4 to C7. PCN was not performed if the following exclusion criteria were present: (1) previously performed surgery in the cervical spine area; (2) osteophytes or loss of more than 50% of disc height at the affected level as determined on conventional X-ray and (3) the concomitant myelopathy at the level of the disc herniation. The local institutional review board of the Albert Schweitzer Hospital, Dordrecht, the Netherlands approved the conduction of this study (MEC-2014.81). All patients gave written informed consent before filling in questionnaires. This study complies with the Declaration of Helsinki.
Surgical Procedure
In the Netherlands, PCN is performed by dedicated pain specialists. The step-by-step operative procedure of PCN has been published elsewhere.12 In brief, PCN was performed under antibiotic prophylaxis and local anesthesia. After identifying the correct level of the cervical spine using fluoroscopy, an entry point for the needle was marked next to the medial part of the sternocleidomastoid muscle. After applying lidocaine locally, a needle and subsequently a trocar were inserted into the annulus fibrosis. After verifying the level of disc herniation again, the SpineWand (ArthroCare) was inserted and used for thermal ablation. After the ablation procedure, the instruments were removed, and a plaster was applied. Patients were discharged a few hours after surgery.
Outcomes and Outcome Collection
Through chart review, data on demographics and scores on the numeric rating scale (NRS) for arm pain and neck pain were collected retrospectively before surgery. Both NRSs were scored from 0 to 10 with ‘0’ indicating no pain and ‘10’ indicating the worst pain possible. The NRS is a valid and reliable Patient Reported Outcome Measure (PROM) in patients with cervical radiculopathy.22 According to the local protocol, all patients had a short-term follow-up phone call scheduled 5 days after the PCN-procedure. During this phone call, the NRS for arm pain and neck pain were evaluated, and information regarding occurring reoperations or complications was collected. To measure long-term follow-up, patients received a questionnaire booklet containing the Core Outcomes Measures Index (COMI) for the neck, questions regarding reoperations and occurrence of late complications and Likert-scales on recovery of symptoms and satisfaction with treatment with an informed consent form.23 The COMI-neck is a seven-question survey, which measures five outcome domains, namely (neck and arm) pain, function, symptom-specific well-being, quality of life and disability on a scale from 0 to 10.23 Based on these outcome domains, a summary score can be calculated in with a “0” indicating the “best score” and a “10” the “worst score”.23,24 If patients indicated in the questionnaire booklet that they had experienced any complication or underwent any reoperation, they were contacted by phone to clarify these. The Likert-scales on recovery and treatment satisfaction were 5-point Likert scales ranging from ‘complete recovery’ or ‘very satisfied’ to “made things worse” or “very dissatisfied”. The COMI-neck is a valid and reliable PROM in patients with an indication for surgery due to cervical radiculopathy or myelopathy caused by degenerative disease.23 Figure 1 depicts a graphical overview of the study procedures and the measurements performed.
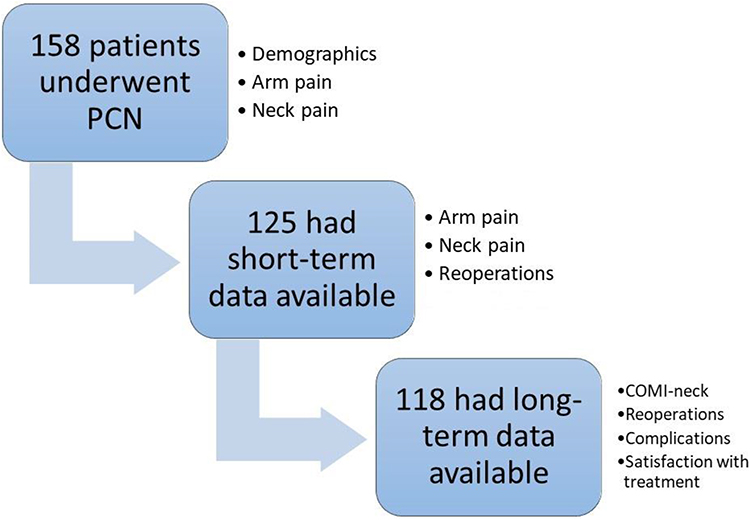 |
Figure 1 Graphical overview of the study procedures and the measurements performed. |
Statistical Analysis
Categorical data were summarized with valid percentages (%); continuous data that are normally distributed are summarized with mean (standard deviation (SD)). Ordinal and non-normally distributed data are summarized with medians and interquartile ranges (IQRs). Normality was verified with Shapiro–Wilk Test. For the COMI-neck, no missing data were accepted for the individual items. Scores on the NRS for neck pain and arm pain were compared pre- and postoperatively using paired t-test. For analyzing purposes, the Likert-scales of the COMI-neck were dichotomized, meaning that the first two options were scored as a “good outcome” and the remaining three options as a “bad outcome”. All analyses were conducted with SPSS version 27.0. A P value <0.05 indicated statistical significance.
Results
Patients
In total 158 patients underwent PCN between 2010 and 2014. Figure 1 gives a graphic overview of the follow-up of the included patients. Short-term follow-up data were available for 79% (N = 125) of the patients, while long-term data were available for 75% (n = 118). Median duration of follow-up was 41.5 months (IQR 27.0 to 57.5). Table 1 gives an overview of the baseline demographics of the patients included. In brief, patients had a mean age of 47.3 ± 9.1, and a mean BMI of 26.6 ± 4.6. Furthermore, most disc herniations were located at C5-6 (48.1%) and C6-7 (48.1%). Prior to PCN, 43.0% of the patients had undergone physical therapy, 75.3% had received pain medication and 7.5% received transcutaneous electrical nerve stimulation. At baseline, the mean NRS for arm pain was 6.3 ± 2.5 and for neck pain 6.0 ± 2.7. Of the included patients, 62.7% had paresthesia, while 17.1% had subjective motor loss.
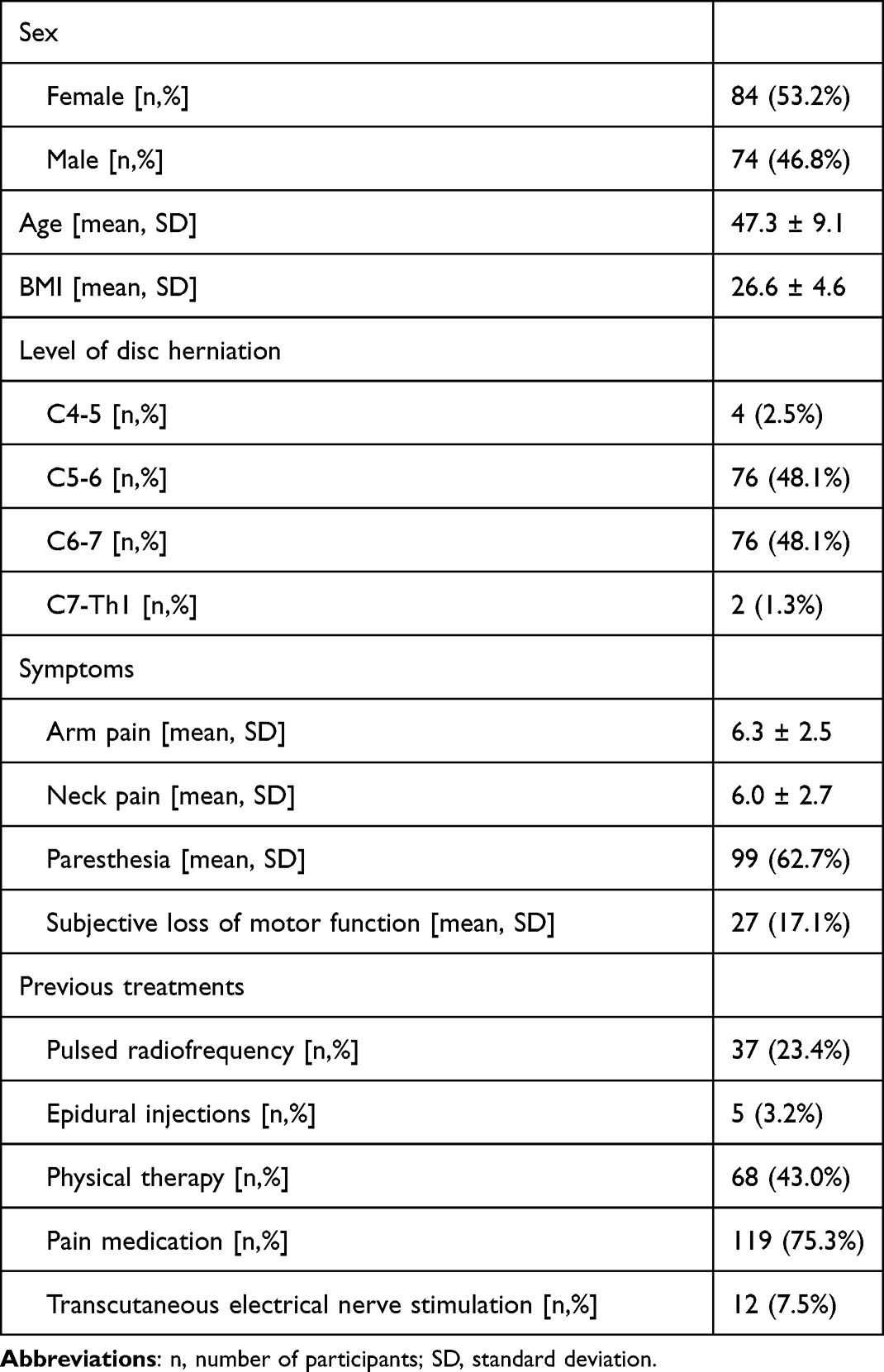 |
Table 1 Demographic and Clinical Characteristics of Patients Who Underwent Cervical Nucleoplasty Treatment at Baseline (N = 158) |
Clinical Outcomes at Short and Long-Term Follow-Up
Table 2 gives an overview of the long-term outcomes of arm pain and neck pain of the included patients. At short-term follow-up patients had a decrease in arm pain (difference of 3.0, 95% Confidence Interval (CI) 2.5 to 3.6, p < 0.001) compared to baseline (Table 2). This decrease was sustained at long-term follow-up (difference with baseline 2.8, 95% CI 1.9 to 3.6, p < 0.001). Neck pain showed similar decrease at short-term (2.8, 95% CI 2.3 to 3.3, p < 0.001) and long-term (2.7, 95% CI 1.9 to 3.5, p < 0.001) follow-up (Table 2). COMI-summary scores showed comparable results. On the Likert scale of recovery, eventually 67.8% of the patients had fully recovered of symptoms and 93.2% was still satisfied with the PCN-treatment results (Table 2).
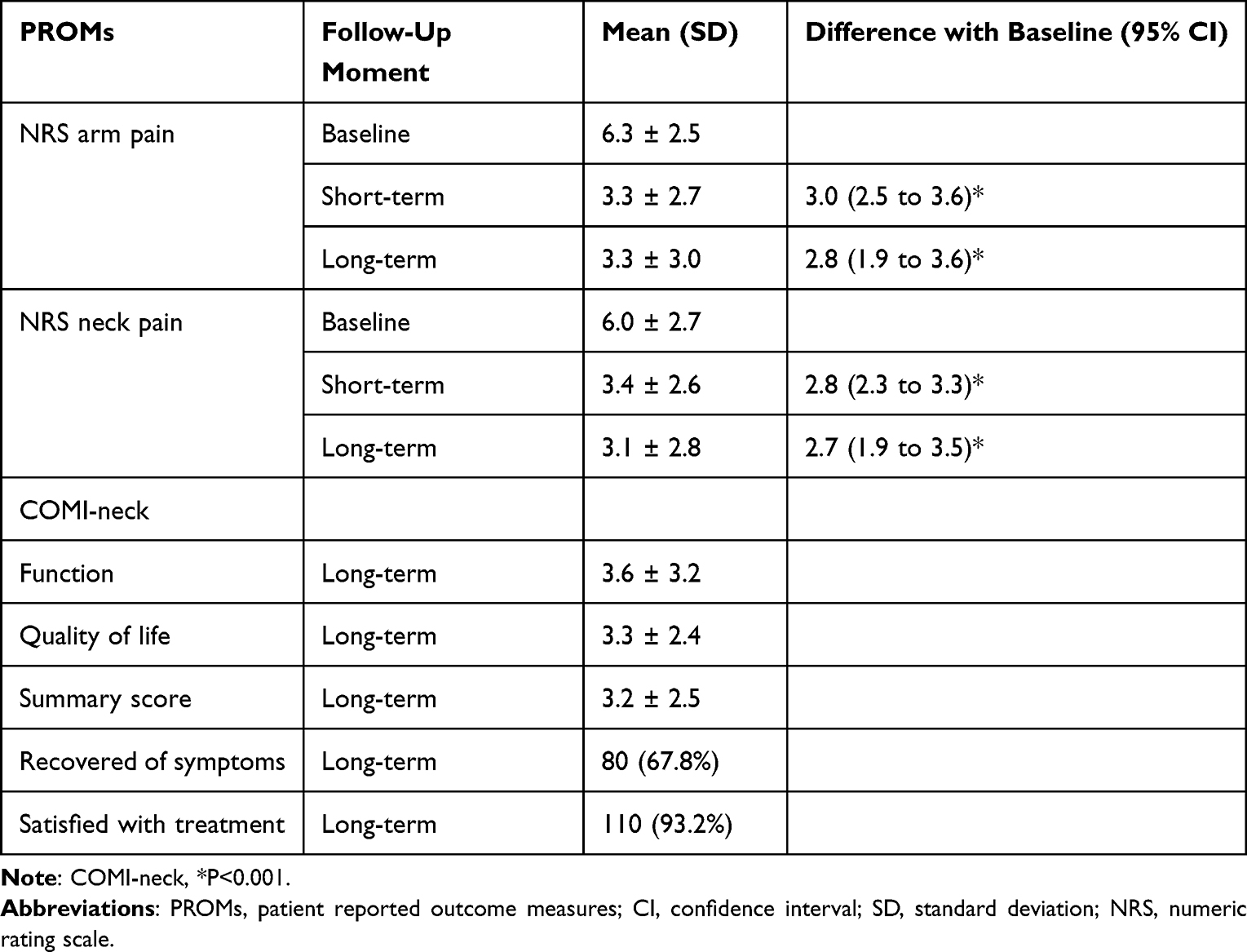 |
Table 2 Clinical Outcomes at Short-Term and Long-Term Follow-Up |
Surgical Outcomes and Complications
Table 3 gives an overview of the surgical outcomes and complications. At short-term follow-up, there were two cases of hoarseness (1.3%), 20 cases of dysphagia (12.7%), 3 cases of wound edema (1.9%) and one case of subcutaneous hematoma (0.6%). All complications are resolved spontaneously over time. At long-term follow-up, 24 patients (21.4%) underwent a reoperation of the cervical spine; 8 (6.8%) due to a disc herniation at another level and 16 (13.6%) due to a disc herniation at the same level as the PCN. Furthermore, 29.9% of the patients had no symptoms of cervical radicular pain at long-term follow-up. Neck pain, arm pain and sensory disturbances were the main complaints for 22.4% to 24.3% of the patients.
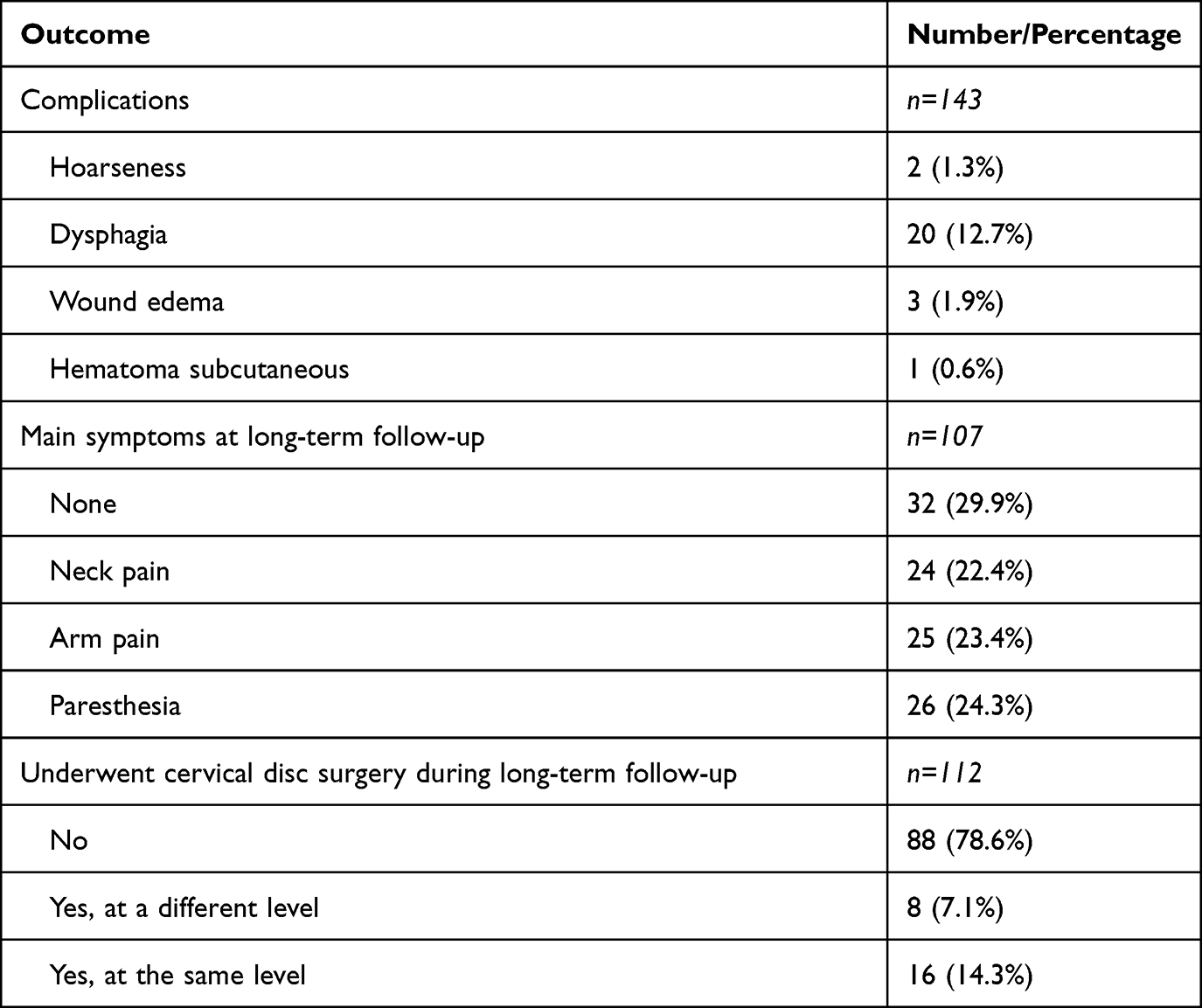 |
Table 3 Surgical Outcomes and Complications |
Discussion
Summary of Findings
The current study presents the results of a retrospective cohort study of 158 patients who underwent PCN due to cervical radicular pain caused by disc herniation. At a median long-term follow-up of 41.5 months, data were available for 75% of the patients. PCN has a low complication risk, and all complications were transient. Based on the patient-reported outcomes, patients experienced a reduction of at least 2.7 on the NRS for arm pain and neck pain at both short- and long-term follow-up. This reduction in arm pain and neck pain exceeds commonly defined thresholds for minimally clinically important differences in the treatment of cervical radiculopathy.25,26 A commonly mentioned concern of applying minimally invasive approaches is the limited working area required to remove enough tissue, and therefore a potential increased risk of recurrent disc herniation.
Comparison with Literature
In the literature, some studies can be identified measuring clinical outcomes or long-term data on PCN. In a retrospective cohort study of 69 patients, Halim et al looked at PROMs at a mean follow-up of 24 months.16 Twenty-seven patients fulfilled ideal selection criteria for PCN, ie patients with a single-level contained cervical herniated disc, which did not resolve with conservative treatment, diagnosed on preoperative MRI and confirmed by a diagnostic selective nerve root block, and 42 patients did not meet these criteria.16 Even though patients who fulfilled the ideal criteria were less likely to use medication postoperatively and were more likely to be satisfied with the treatment, no differences were found in pain scores or the neck disability index.16 This study results suggest that perhaps more patients, than those that were deemed ideal, may benefit from a PCN treatment. Nevertheless, the results of Halim et al appear to be in line with the results of the current study.
Aside from pain and our self-perceived success with interventions, the COMI-neck also measured symptom-specific well-being, quality of life, social disability and work disability. When we compare the results of these outcome domains of the current study, with the outcomes reported in observational studies among patients undergoing anterior cervical spine surgery, we can see comparable decreases in pain scores and the COMI-summary score, showing an overall increase in the different COMI-domains.23,27
Kim et al also looked at predictors for the success of PCN.16,17 In their retrospective study of 201 patients, factors such as unilateral radiculopathy and the use of a specific technique of PCN (curved-tip technique) were identified as predictors of success, while longer pain duration and concurrent spinal canal stenosis were identified as negative predictors. To be noted, the success rate of PCN was 66.7% in the study of Kim et al, though they used a more broader applied indication for PCN, their results appear to be in line with our study.
Li et al published the results of a prospective study among 126 patients undergoing PCN for a symptomatic cervical disc herniation.28 The procedure was successful for 83.7% of the patients and pain treatment reached minimally clinical important differences. There was one case of a device, ie partial Perc-D Spine Wand, that broke in the disc space. The rate of recurrent disc herniations was zero, which was lower than in our case series. Perhaps, the length of follow-up in the study by Li et al,28 ie 12 months, may explain the difference somewhat.
In our study, a total of 16 (13.6%) patients underwent a revision procedure for a “recurrent” disc herniation at the index level at long-term follow-up. In other words, ACD(F) was prevented in 86.4% of the patients. This reoperation rate is comparable with the reoperation rates of ACDF, ie 7.8% to 15%.29,30 Kessinger studied the rate of reoperation after PCN and identified a reoperation rate of 19.5% in his study population of 133 patients.31 This rate appears to be somewhat higher than the rate we found in our study. This difference may be attributed to a difference in the length of the follow-up between both studies. However, it is up to debate how clinically important revision procedures are at, for instance, ten years of follow-up. Although our study did not have a control group, ie surgery or conservative therapy, there are studies who compared PCN with surgery. In a recently published randomized controlled trial, 48 patients with cervical radicular pain as a result of a single-level contained soft disc hernia were randomized between PCN and ACD.21 In this study, it was shown that at short-term follow-up, ie 3 months, the ACD group performed significantly better on arm pain reduction than the PCN group. However, the difference between the groups was 17.2 mm on a VAS scale of 100 mm, this difference can be disputed for its clinical importance.21 At long-term follow-up, ie one year after PCN, no significant differences between the groups were found, suggesting a place for PCN in the treatment of cervical radicular pain. Another recently performed RCT compared the effects of PCN to posterior decompression in 35 patients suffering from single-level disc-herniation with an indication for surgery.32 In this trial, no significant differences were found between the groups on radicular arm pain and neck pain 3 and 6 months after the intervention. Finally, one study made a retrospective comparison in 50 patients who either underwent a PCN or a percutaneous cervical discectomy for a contained cervical disc herniation.33 This study also showed that PCN had comparable results in terms of clinical success or complications, compared to cervical discectomy.
Strengths and Limitations
Advantages of this study are the long follow-up duration after treatment and the relatively large sample size of patients undergoing PCN. Another advantage of our study is the 25% of loss to follow-up at a median of 41.5 months seems to be comparable to the long-term follow-up rates of prospective studies (18% to 37% loss to follow-up).34–36 Furthermore, missing data analyses suggest that data was missing completely at random and therefore we expect a low impact of the missing data on the study results. Finally, several studies show that the amount of missing data may not be related to the quality of the study.37,38
Some limitations, however, must be acknowledged. First, it is the design of the study. Since this study is retrospective, recall bias might have been introduced. Furthermore, at baseline, only a selected number of variables were available, such as pain scores. Another limitation may lie in the generalizability of the study results. PCN is only performed in patients with cervical radicular pain due to contained soft disc herniations without the presence of osteophytes or significant loss of disc height. Therefore, PCN would only be a treatment alternative for a selected group of patients.
Implications
Based on our data, PCN appears to be a safe and effective treatment at short-term and long-term follow-up for primary patients with cervical radicular pain due to a contained soft disc herniation. It prevented the need for ACD(F) in 86.4% of the patients, showing potency of PCN as a treatment option alongside ACD(F) to treat arm pain. Even though in our study population patients experienced a statistically significant decrease in neck pain, PCN is not recommended to be applied to solely treat neck pain in our practice. As aforementioned, PCN was only performed in a strongly selected patient population. Therefore, in our opinion ACD(F) will remain as the standard treatment in cases of osteophytes, myelopathy or other cases not suited for PCN. Another important area, which is underreported in the literature, is the cost-effectiveness. As PCN shows equivalent results to ACD on the short-term and long-term follow-up in the literature,21,32 the height of the costs of the surgery, primary care, secondary care and work loss productivity will determine if PCN is cost-effective compared to ACD.
Conclusion
PCN appears to be a safe and effective treatment for a specific selection of cervical herniated discs, with an acceptable long-term reoperation rate. This study results suggest a potential role of PCN as a less invasive treatment option for cervical radicular pain due to a contained soft disc herniation before surgery should be considered.
Acknowledgments
We would like to thank Tanja Hamm-Faber (Nurse Practitioner Chronic Pain, Department of Anesthesiology and Pain Medicine, Albert Schweitzer Hospital) for her support in collecting the patient data and Ingrid de Rooij for administrative contribution.
Disclosure
Dr Frank Johannes Huygen reports personal fees from ABBOTT, Boston Scientific, Grunenthal, and Pfizer, grants from Saluda, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Bogduk N. On the definitions and physiology of back pain, referred pain, and radicular pain. Pain. 2009;147(1–3):17–19. doi:10.1016/j.pain.2009.08.020
2. Daffner SD, Hilibrand AS, Hanscom BS, Brislin BT, Vaccaro AR, Albert TJ. Impact of neck and arm pain on overall health status. Spine. 2003;28(17):2030–2035. doi:10.1097/01.BRS.0000083325.27357.39
3. Sleijser-Koehorst MLS, Coppieters MW, Heymans MW, Rooker S, Verhagen AP, Scholten-Peeters GGM. Clinical course and prognostic models for the conservative management of cervical radiculopathy: a prospective cohort study. Eur Spine J. 2018;27(11):2710–2719. doi:10.1007/s00586-018-5777-8
4. Liu WJ, Hu L, Chou PH, Wang JW, Kan WS. Comparison of anterior cervical discectomy and fusion versus posterior cervical foraminotomy in the treatment of cervical radiculopathy: a systematic review. Orthop Surg. 2016;8(4):425–431. doi:10.1111/os.12285
5. Yang X, Janssen T, Arts MP, Peul WC, Vleggeert-Lankamp CLA. Radiological follow-up after implanting cervical disc prosthesis in anterior discectomy: a systematic review. Spine J. 2018;18(9):1678–1693. doi:10.1016/j.spinee.2018.04.021
6. Donk RD, Verbeek ALM, Verhagen WIM, Groenewoud H, Hosman AJF, Bartels R. What’s the best surgical treatment for patients with cervical radiculopathy due to single-level degenerative disease? A randomized controlled trial. PLoS One. 2017;12(8):e0183603. doi:10.1371/journal.pone.0183603
7. Vleggeert-Lankamp CLA, Janssen TMH, van Zwet E, et al. The NECK trial: effectiveness of anterior cervical discectomy with or without interbody fusion and arthroplasty in the treatment of cervical disc herniation; a double-blinded randomised controlled trial. Spine J. 2018;19:965–975.
8. de Rooij JD, Gadjradj PS, Soria van Hoeve JS, Harhangi BS. Anterior cervical discectomy without fusion for a symptomatic cervical disk herniation. Acta Neurochir. 2017;159(7):1283–1287. doi:10.1007/s00701-017-3189-x
9. Nanda A, Sharma M, Sonig A, Ambekar S, Bollam P. Surgical complications of anterior cervical discectomy and fusion for cervical degenerative disk disease: a single surgeon’s experience of 1576 patients. World Neurosurg. 2014;82(6):1380–1387. doi:10.1016/j.wneu.2013.09.022
10. Bovonratwet P, Fu MC, Tyagi V, et al. Incidence, risk factors, and clinical implications of postoperative hematoma requiring reoperation following anterior cervical discectomy and fusion. Spine. 2018;44:543–549.
11. Lykissas MG, Giannoulis D. Minimally invasive spine surgery for degenerative spine disease and deformity correction: a literature review. Ann Transl Med. 2018;6(6):99. doi:10.21037/atm.2018.03.18
12. Gadjradj PS, Rubinstein SM, Peul WC, et al. Full endoscopic versus open discectomy for sciatica: randomised controlled non-inferiority trial. BMJ. 2022;376:e065846. doi:10.1136/bmj-2021-065846
13. Gadjradj PS, Broulikova HM, van Dongen JM, et al. Cost-effectiveness of full endoscopic versus open discectomy for sciatica. Br J Sports Med. 2022. doi:10.1136/bjsports-2021-104808
14. de Rooij JD, Gadjradj PS, Soria van Hoeve JS, Huygen FJ, Aukes HA, Harhangi BS. Percutaneous nucleoplasty for the treatment of a contained cervical disk herniation. Clin Spine Surg. 2017;30(9):389–391. doi:10.1097/BSD.0000000000000583
15. Gerges FJ, Lipsitz SR, Nedeljkovic SS. A systematic review on the effectiveness of the Nucleoplasty procedure for discogenic pain. Pain Physician. 2010;13(2):117–132.
16. Halim W, Wullems JA, Lim T, et al. The long-term efficacy and safety of percutaneous cervical nucleoplasty in patients with a contained herniated disk. Pain Pract. 2013;13(5):364–371. doi:10.1111/papr.12003
17. Kim MK, Sim SE, Kim YC, et al. Predictive factors of successful percutaneous cervical nucleoplasty for the treatment of pain with cervical herniated disk. World Neurosurg. 2018;114:e654–e662. doi:10.1016/j.wneu.2018.03.046
18. Birnbaum K. Percutaneous cervical disc decompression. Surg Radiol Anat. 2009;31(5):379–387. doi:10.1007/s00276-009-0462-6
19. Cesaroni A, Nardi PV. Plasma disc decompression for contained cervical disc herniation: a randomized, controlled trial. Eur Spine J. 2010;19(3):477–486. doi:10.1007/s00586-009-1189-0
20. Nardi PV, Cabezas D, Cesaroni A. Percutaneous cervical nucleoplasty using coblation technology. Clinical results in fifty consecutive cases. Acta Neurochir Suppl. 2005;92:73–78.
21. de Rooij J, Harhangi B, Aukes H, Groeneweg G, Stronks D, Huygen F. The effect of percutaneous nucleoplasty vs anterior discectomy in patients with cervical radicular pain due to a single-level contained soft-disc herniation: a randomized controlled trial. Pain Physician. 2020;23(6):553–564.
22. Young IA, Cleland JA, Michener LA, Brown C. Reliability, construct validity, and responsiveness of the neck disability index, patient-specific functional scale, and numeric pain rating scale in patients with cervical radiculopathy. Am J Phys Med Rehabil. 2010;89(10):831–839. doi:10.1097/PHM.0b013e3181ec98e6
23. Gadjradj PS, Chin-See-Chong TC, Donk D, Depauw P, Tulder MWV, Harhangi BS. Cross-cultural adaptation and psychometric validation of the Dutch version of the core outcome measures index for the neck in patients undergoing surgery for degenerative disease of the cervical spine. Neurospine. 2021;18(4):798–805. doi:10.14245/ns.2142682.341
24. Fankhauser CD, Mutter U, Aghayev E, Mannion AF. Validity and responsiveness of the Core Outcome Measures Index (COMI) for the neck. Eur Spine J. 2012;21(1):101–114. doi:10.1007/s00586-011-1921-4
25. Andresen AK, Paulsen RT, Busch F, Isenberg-Jorgensen A, Carreon LY, Andersen MO. Patient-reported outcomes and patient-reported satisfaction after surgical treatment for cervical radiculopathy. Global Spine J. 2018;8(7):703–708. doi:10.1177/2192568218765398
26. Parker SL, Godil SS, Shau DN, Mendenhall SK, McGirt MJ. Assessment of the minimum clinically important difference in pain, disability, and quality of life after anterior cervical discectomy and fusion: clinical article. J Neurosurg Spine. 2013;18(2):154–160. doi:10.3171/2012.10.SPINE12312
27. Staub LP, Ryser C, Röder C, et al. Total disc arthroplasty versus anterior cervical interbody fusion: use of the Spine Tango registry to supplement the evidence from randomized control trials. Spine J. 2016;16(2):136–145. doi:10.1016/j.spinee.2015.11.056
28. Li J, Yan DL, Zhang ZH. Percutaneous cervical nucleoplasty in the treatment of cervical disc herniation. Eur Spine J. 2008;17(12):1664–1669. doi:10.1007/s00586-008-0786-7
29. Emami A, Coban D, Changoor S, et al. Comparing mid-term outcomes between ACDF and minimally invasive posterior cervical foraminotomy in the treatment of cervical radiculopathy. Spine. 2021. doi:10.1097/BRS.0000000000004140
30. van Eck CF, Regan C, Donaldson WF, Kang JD, Lee JY. The revision rate and occurrence of adjacent segment disease after anterior cervical discectomy and fusion: a study of 672 consecutive patients. Spine. 2014;39(26):2143–2147. doi:10.1097/BRS.0000000000000636
31. Klessinger S. The frequency of re-surgery after cervical disc nucleoplasty. World Neurosurg. 2018;117:e552–e556. doi:10.1016/j.wneu.2018.06.075
32. Abrishamkar S, Salimi S, Pirmoradi H. Comparison the postoperation results of discectomy with nucleoplasty in single cervical disc herniation. Adv Biomed Res. 2018;7(1):29. doi:10.4103/abr.abr_159_15
33. Ierardi AM, Carnevale A, Cossu A, et al. Percutaneous cervical discectomy: retrospective comparison of two different techniques. Radiol Med. 2020;125(6):569–577. doi:10.1007/s11547-020-01133-x
34. Lequin MB, Verbaan D, Jacobs WC, et al. Surgery versus prolonged conservative treatment for sciatica: 5-year results of a randomised controlled trial. BMJ Open. 2013;3(5):e002534. doi:10.1136/bmjopen-2012-002534
35. Overdevest GM, Peul WC, Brand R, et al. Tubular discectomy versus conventional microdiscectomy for the treatment of lumbar disc herniation: long-term results of a randomised controlled trial. J Neurol Neurosurg Psychiatry. 2017;88(12):1008–1016. doi:10.1136/jnnp-2016-315306
36. Schenck CD, Terpstra SES, Moojen WA, et al. Interspinous process device versus conventional decompression for lumbar spinal stenosis: 5-year results of a randomized controlled trial. J Neurosurg Spine;2021. 1–9. doi:10.3171/2021.8.SPINE21419
37. Groves RM. Nonresponse rates and nonresponse bias in household surveys. Public Opin Q. 2006;70(5):646–675. doi:10.1093/poq/nfl033
38. Livingston EH, Wislar JS. Minimum response rates for survey research. Arch Surg. 2012;147(2):110.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.