Back to Journals » Clinical Ophthalmology » Volume 20
Long-Term Clinical Outcomes of nDSAEK and Machine Learning-Based Prediction of Graft Survival in Corneal Endothelial Decompensation
Authors Lin Y ![]() , Hu Y, Xie Z, Fang X, Luo S, Xiao X, Lin Z, Wu H
, Hu Y, Xie Z, Fang X, Luo S, Xiao X, Lin Z, Wu H
Received 31 March 2026
Accepted for publication 12 June 2026
Published 17 June 2026 Volume 2026:20 612110
DOI https://doi.org/10.2147/OPTH.S612110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Yuan Lin,1– 6,* Yiming Hu,7,* Zhiwen Xie,1– 6,* Xie Fang,1– 6 Shunrong Luo,1– 6 Xianwen Xiao,1– 6 Zhirong Lin,1– 6 Huping Wu1– 6
1Xiamen Eye Center and Eye Institute of Xiamen University, School of Medicine, Xiamen, People’s Republic of China; 2Fujian Key Laboratory of Corneal & Ocular Surface Diseases, Xiamen, Fujian, People’s Republic of China; 3Xiamen Key Laboratory of Corneal & Ocular Surface Diseases, Xiamen, Fujian, People’s Republic of China; 4Xiamen Clinical Research Center for Eye Diseases, Xiamen, Fujian, People’s Republic of China; 5Xiamen Key Laboratory of Ophthalmology, Xiamen, Fujian, People’s Republic of China; 6Translational Medicine Institute of Xiamen Eye Center of Xiamen University, Xiamen, Fujian, People’s Republic of China; 7Ophthalmic Center, The Second Affiliated Hospital, Jiangxi Medical College, Nanchang University, Nanchang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhirong Lin; Huping Wu, Email [email protected]; [email protected]
Purpose: To evaluate long-term outcomes of non-Descemet stripping automated endothelial keratoplasty (nDSAEK) in low-vision patients with corneal endothelial decompensation (CED), and to develop a machine-learning framework for predicting graft failure.
Methods: This retrospective study included 114 eyes (Fuchs’ and non-Fuchs’ etiologies) treated with nDSAEK. Best-corrected visual acuity (BCVA), endothelial cell density (ECD), and complications were assessed over a long-term follow-up. Linear mixed-effects models (LMM) analyzed ECD kinetics. An XGBoost model using 10 clinical features was constructed to predict graft failure, interpreted via SHapley Additive exPlanations (SHAP) analysis. Results were compared against established endothelial keratoplasty benchmarks.
Results: The median follow-up was 41.50 months (IQR: 25.65– 55.75 months). Mean BCVA improved significantly from 1.80 logMAR baseline to 1.20 logMAR at 6 months, remaining stable thereafter. At 3 years, mean ECD was 1724 ± 279 cells/mm2.,Subgroup stratification demonstrating a 3-year cumulative ECD loss of 37.9% in the Fuchs’ group compared to a significantly higher long-term depletion rate of 45.3% in the non-Fuchs’ group. LMM analysis showed that femtosecond laser-assisted nDSAEK (FS-nDSAEK) significantly improved long-term ECD maintenance over manual dissection. The predictive framework yielded longitudinal risk-discrimination capability, demonstrating a time-dependent area under the ROC curve (AUC) of 0.917 (95% CI: 0.819– 1.000) at 12 months, 0.920 (95% CI: 0.823– 1.000) at 24 months, and 0.880 (95% CI: 0.765– 0.995) at 36 months, driven by 15 confirmed graft failure events within the 114-eye cohort. SHAP analysis identified FS assistance and preoperative ECD as key protective factors. Compared to literature benchmarks, nDSAEK demonstrated visual and anatomical stability demonstrated visual and anatomical trends that align with historical DSAEK cohorts.
Conclusion: nDSAEK offers stable long-term visual and anatomical outcomes for CED. The integration of AI frameworks offers an exploratory framework for individualized prognostic screening, though further external validation is required before direct clinical integration.
Keywords: non-descemet stripping automated endothelial keratoplasty, corneal endothelial decompensation, post-cataract surgery, endothelial cell density, long-term graft survival
Introduction
Persistent corneal edema and a steady decline in visual acuity are frequently attributable to corneal endothelial decompensation (CED). In advanced stages, this condition can progress to corneal blindness, profoundly compromising patients’ quality of life.1,2 Patients in the early phases typically present with subtle visual impairment. As corneal edema exacerbates, it leads to Descemet’s membrane (DM) folds and stromal thickening, thereby inducing glare and blurred vision. Late-stage disease may manifest as bullae formation, further deteriorating visual function and causing symptoms ranging from foreign body sensation to intractable pain.3 Currently, CED remains a leading cause of visual impairment worldwide and the primary indication for corneal transplantation. While penetrating keratoplasty (PK) once served as the clinical gold standard, its inherent drawbacks including prolonged visual rehabilitation, high postoperative astigmatism, and an increased risk of graft rejection sparked a shift toward more refined lamellar endothelial procedures.4–6
Endothelial keratoplasty (EK) reconstructs the posterior cornea by selectively replacing the DM and the endothelial layer. Over the past two decades, EK has largely supplanted PK for the treatment of endothelial pathologies.7 Descemet’s stripping automated endothelial keratoplasty (DSAEK) and Descemet’s membrane endothelial keratoplasty (DMEK) have become the gold standard EK procedures for treating corneal endothelial dysfunction.8 Compared to PK, DSAEK and DMEK have demonstrated superior visual recovery, enhanced structural stability, and lower rejection rates.9–11 Notably, however, both procedures mandate the stripping of the host’s DM, which may escalate surgical complexity and pose potential risks in eyes with compromised anterior segment anatomy, a history of intraocular surgery, or a tenuous intraocular environment.
Non-Descemet stripping automated endothelial keratoplasty (nDSAEK) is a technique that obviates the need for host DM removal. Previous studies indicated that endothelial grafts could adhere to the host cornea even when the recipient endothelium was retained, and subsequent clinical applications have further validated the efficacy of nDSAEK.12–14 Early animal studies suggested that nDSAEK might compromise graft survival and visual quality due to poor transparency after graft folding and insufficient clarity at the donor-host interface.15 Consequently, nDSAEK has long remained on the periphery of mainstream EK procedures. However, research by Risa Yamazaki et al demonstrated no significant clinical disparities between DSAEK and nDSAEK regarding best-corrected visual acuity (BCVA), refraction, or endothelial cell density (ECD).16
In complex cases involving severe preoperative edema, chronic low vision, or a history of multiple intraocular surgeries, conventional DM stripping may further insult the posterior stroma and increase the risk of interface instability. In contrast, nDSAEK preserves the host’s DM architecture to mitigate surgical trauma and avoid inadvertent traction on posterior stromal fibers. This provides superior conformational adaptability at the donor-host interface, making it potentially better suited for patients with complex CED in the context of global donor tissue scarcity. Although the feasibility of nDSAEK has been confirmed in specific cohorts, systematic evaluations regarding long-term visual improvement, endothelial cell dynamics, and structural stability in low-vision CED patients remain scant. Most existing literature focuses on short-to-medium-term outcomes,17 leaving a notable lack of data regarding extended long-term follow-up survival and Fuchs’ endothelial corneal dystrophy (FECD). Therefore, it is imperative to re-evaluate the expanded indications and long-term durability of the nDSAEK technique.
While the therapeutic efficacy and endothelial dynamics of nDSAEK have been traditionally documented through descriptive registries, an unaddressed clinical blind spot remains regarding individual risk stratification for long-term graft decompensation.18 Recent advances in ophthalmic artificial intelligence from 2024 to 2025 have witnessed a paradigm shift from static deep-learning image classification to multi-modal predictive analytics capable of processing highly heterogeneous clinical variables over extended longitudinal horizons.19
However, existing corneal prognostics often treat algorithmic output as an isolated endpoint, neglecting the emerging paradigm that human-AI collaboration yields vastly superior clinical diagnostic and prognostic efficacy compared to autonomous AI image analysis or clinician intuition alone.20 Furthermore, contemporary machine learning literature in ophthalmology frequently lacks methodological transparency due to non-standardized reporting.21 To bridge these clinical and methodological gaps, this study presents an interpretable machine learning framework engineered as a clinical decision support system. Developed in strict adherence to the TRIPOD+AI statement,22 this framework delivers robust temporal risk-discrimination boundaries to optimize post-keratoplasty surveillance.
Currently, high-quality evidence remains insufficient to define the long-term clinical role of nDSAEK relative to established benchmarks. A comprehensive longitudinal evaluation integrating multi-decadal endothelial survival, anatomical stability, and AI-driven risk stratification is notably absent. This study addresses this critical gap by presenting nDSAEK cohorts to date, featuring a follow-up spanning up to 18 years. We aim to evaluate the clinical utility of nDSAEK in patients with low-vision CED, focusing on visual rehabilitation, endothelial attrition kinetics, and graft-related complications. By leveraging XGBoost and SHAP analysis, we not only assess long-term efficacy but also establish a predictive framework for individualized graft prognosis. Ultimately, these outcomes are interpreted with reference to longitudinal data from major EK studies to offer a benchmarked perspective on the clinical viability of nDSAEK in the modern era of corneal surgery.
Methods
Ethics and Study Population
This study adhered to the ethical principles of the Declaration of Helsinki and received approval from the Human Ethics Committee of Xiamen Eye Center, affiliated with Xiamen University (XMYKZX-KY-2025-057). Due to the retrospective, non-interventional nature of the analysis utilizing de-identified historical medical charts, the IRB officially granted a waiver of dedicated informed consent for this study. Standard written informed consent for the surgical procedures and the subsequent academic utilization of de-identified clinical data had been routinely obtained from all patients prior to surgery. This retrospective cohort study enrolled 114 eyes from 114 patients who underwent nDSAEK at the Xiamen Eye Institute between 2007 and 2025. Comprehensive clinical data, including initial presentation, age, sex, symptoms, treatment protocols, complications, and visual recovery, were extracted from electronic medical records.
Inclusion and Exclusion Criteria
The inclusion criteria encompassed cases of CED secondary to multiple ocular surgeries, such as uncomplicated cataract surgery, corneal transplantation, trabeculectomy, and pars plana vitrectomy, as well as patients with FECD presenting with bullous changes. Conversely, patients were excluded if they presented with CED secondary to severe ocular trauma, ocular hypertension, or infectious keratitis. Other exclusion criteria included severe systemic diseases or the long-term use of systemic immunosuppressants, pre-existing ocular comorbidities that significantly limited visual potential, and a high risk of graft failure requiring systemic immunosuppressive therapy. Furthermore, patients unable to adhere to the designated follow-up protocols were also excluded from the analysis.
Donor Tissue Provenance
All donor corneal tissues utilized in this study (donor age range: 12–30 years) were procured by and obtained from the Affiliated Eye Bank of Xiamen University. Tissue collection, screening, and allocation strictly adhered to national organ and tissue procurement regulations. For all donors, including pediatric cases under 18 years of age, written informed consent for tissue donation and research utilization was legally obtained from their respective parents or immediate next of kin prior to procurement. No tissues were obtained from vulnerable or non-consenting populations.
Surgical Technique
All procedures were performed by a single experienced surgeon (Huping Wu, MD, PhD). Fresh donor corneas, with donor ages ranging from 12 to 30 years, were retrieved from the institutional eye bank and stored in a moist chamber for approximately 12 hours. Posterior lamellar grafts of 7.5 or 8.0 mm in diameter were prepared using either a standard microkeratome or a femtosecond laser, notably without stripping the host’s Descemet’s membrane. Under peribulbar anesthesia, a 5-mm temporal corneal tunnel incision was created to facilitate graft insertion. The graft was then introduced into the anterior chamber using a glide technique similar to intraocular lens implantation. The wound was secured with interrupted 10–0 nylon sutures, followed by an intracameral air injection to promote graft adherence. Patients remained in a supine position for 2 to 3 hours postoperatively.
Clinical Evaluation and Follow-Up
Demographic and clinical parameters were collected, including preoperative diagnosis, BCVA, ECD, central corneal thickness, slit-lamp biomicroscopy findings, graft status, and postoperative complications. Follow-up examinations were conducted at scheduled intervals, focusing on long-term visual improvement, endothelial dynamics, corneal clarity, and graft functionality. A subset of cases completed an extended follow-up period exceeding five years.
Statistical Analysis and Predictive Modeling
Statistical analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY) and R software (version 4.2.0; R Foundation for Statistical Computing). The normality of data distribution was assessed using the Shapiro–Wilk test. Continuous variables are expressed as mean ± standard deviation or median with interquartile range, while categorical variables are reported as frequencies and percentages.
To evaluate the longitudinal trajectory of ECD and BCVA, linear mixed-effects models were employed to account for the correlation between repeated measurements and to adjust for covariates such as age, sex, surgical history, and technique. Comparisons between FECD and non-FECD groups were performed using independent-samples t-tests or Mann–Whitney U-tests as appropriate.
Furthermore, an AI-driven predictive framework was developed to assess the risk of graft failure. An XGBoost algorithm was trained on ten clinical features, including age, surgical history, surgical technique, and preoperative corneal status. To overcome statistical power constraints tied to a small sample size and to maximize data utility, a 5-fold cross-validation technique was utilized instead of a standard train/test split, while applying strict conservative regularization hyperparameters to penalize model complexity.
To enhance model interpretability, SHAP analysis was utilized to quantify the contribution of each feature to the model’s predictions. A gradient-boosted decision tree ensemble was constructed using the XGBoost algorithm to model graft failure risk. To ensure transparency and robust clinical interpretation, a post-hoc explanatory analysis was performed using the TreeSHAP (Tree Shapley Additive exPlanations) algorithm to compute exact local feature contributions. Regarding feature engineering, categorical variables (eg., sex, surgical technique, and baseline ocular history) were systematically converted via one-hot encoding into separate binary indicators before matrix construction.
Model performance was evaluated using time-dependent receiver operating characteristic curves and the area under the curve at 12, 24, and 36 months. A two-sided P < 0.05 was considered statistically significant. Data visualization was performed using GraphPad Prism version 8.0 and the ggplot2 package in R.
To evaluate longitudinal trends, Linear mixed-effects models (LMM) were fitted using the Restricted Maximum Likelihood (REML) estimation via the lmerTest package. The random-effects structure featured random intercepts per patient to account for intrasubject correlation of repeated measurements across the 7 post-operative timepoints, specifying an unstructured covariance matrix. For multiple continuous clinical comparisons in Table 1, the Benjamini-Hochberg False Discovery Rate (BH-FDR) correction was systematically applied to mitigate Type I error inflation.
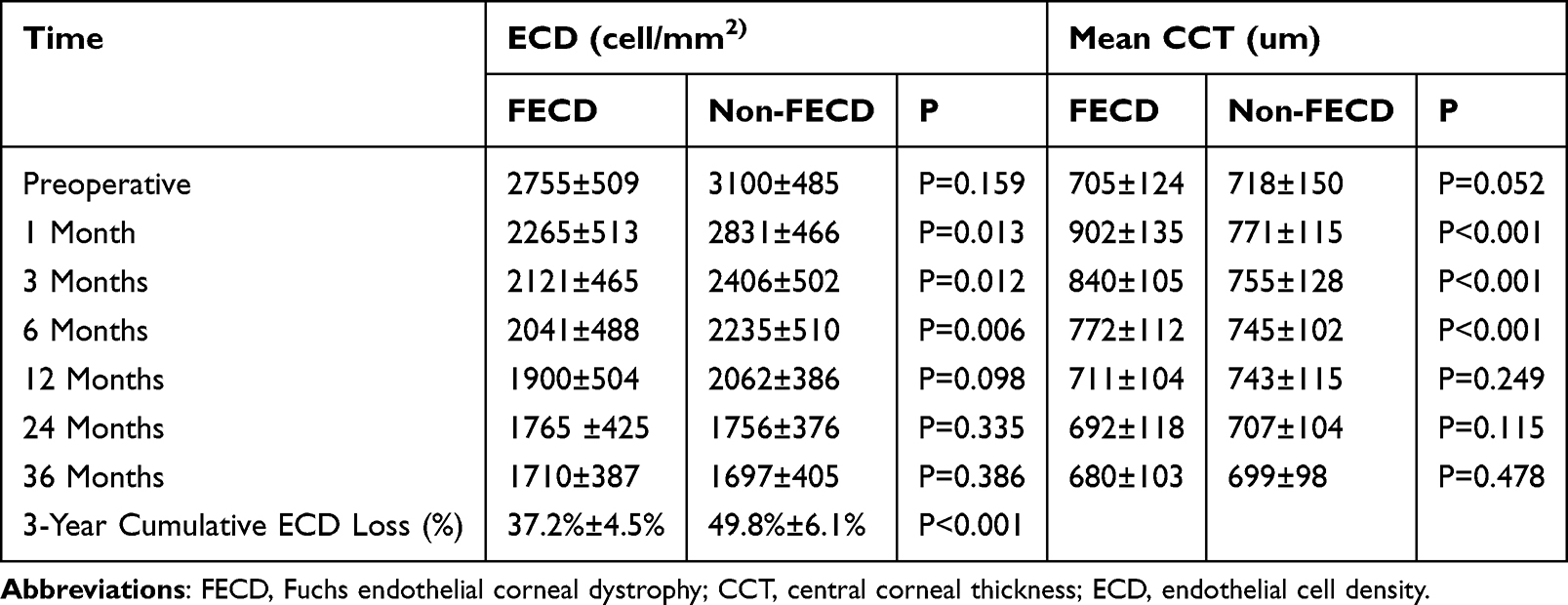 |
Table 1 FECD and Non-FECD Patients Postoperative Corneal and Graft Status |
The XGBoost prognostic framework was governed by conservative regularization hyperparameters to penalize complexity, given the acknowledged constraints of a low event-per-variable ratio. Regarding missing data handling, rather than employing ad-hoc imputation, we leveraged XGBoost’s native sparsity-aware split-finding algorithm, allowing eyes with unrecordable pre-operative ECD due to severe corneal edema to be classified inherently during node splitting. Time-dependent ROC curves were estimated using the Kaplan-Meier non-parametric method for censoring distribution adjustment. The study structure was audited utilizing the TRIPOD+AI statement22 guidelines alongside the PROBAST tool to explicitly evaluate risk of bias and ensure standardized reporting taxonomy.
Benchmark Comparison
To interpret the long-term clinical significance of nDSAEK, the outcomes observed in this study were descriptively compared against established benchmarks from prominent longitudinal studies on conventional endothelial keratoplasty, such as DSAEK and DMEK. This comparative analysis served primarily for contextual interpretation and did not involve statistical pooling or formal meta-analysis.
Results
Patient and Postoperative Graft Status
This study enrolled 114 patients, consisting of 54 males and 60 females with a mean age of 56.2 ± 13.7 years. The cohort comprised 43 cases of FECD and 71 non-FECD cases secondary to cataract surgery, including six eyes with a history of ocular trauma surgery, four post-vitrectomy, and one post-corneal transplantation. All patients successfully underwent nDSAEK, with the median follow-up was 41.50 months (IQR: 25.65–55.75 months). Postoperatively, resolution of corneal edema and bullous epithelial keratopathy was achieved in all subjects. Corneal clarity was sustained throughout the 3-to-5-year follow-up period, even in complex cases with a history of multiple intraocular surgeries (Figure 1).
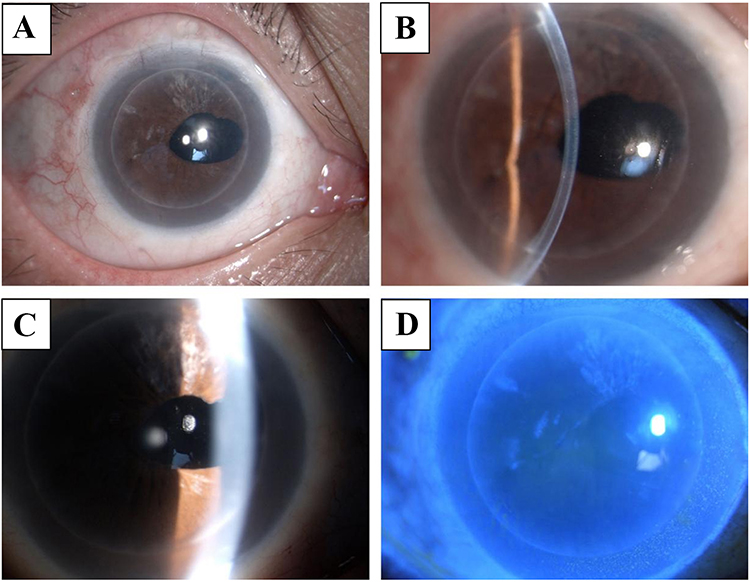 |
Figure 1 Five-year follow-up of a patient post-nDSAEK. Long-term follow-up (3 to 5 years) in a stable anterior segment demonstrates sustained corneal clarity, indicating successful graft survival and maintained endothelial function.(A) Diffuse anterior segment photograph showing a clear to mildly hazy corneal graft. (B) Slit-lamp biomicroscopy highlighting the cornea and anterior chamber, showing the interface between the host cornea and the nDSAEK lenticule. (C) Retroillumination photography demonstrating the extent of the retrocorneal/graft membrane. (D) Cobalt blue light examination with fluorescein staining. |
In vivo confocal microscopy revealed a progressive reduction in stromal edema across both groups. In patients with FECD, primary endothelial lesions at the donor-recipient interface were gradually absorbed, with no recurrence or secondary lesions observed on the donor graft (Figure 2). Furthermore, the donor grafts demonstrated functional stability across various primary etiologies (Figure 3).
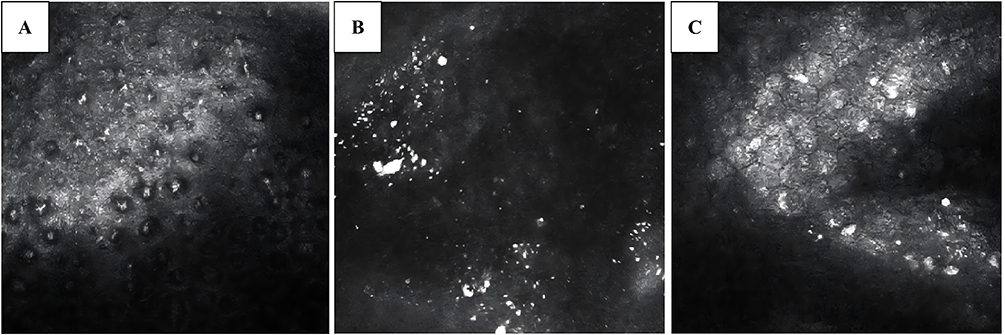 |
Figure 2 IVCM images of a patient with FECD after nDSAEK. (A) Preoperative IVCM image showing typical FECD endothelial lesions. (B) At 12 months post-nDSAEK, the primary lesions gradually dissipated and fused with the donor interface. (C) Donor graft at 12 months shows a slight decrease in endothelial cell count but no recurrence of typical FECD features. |
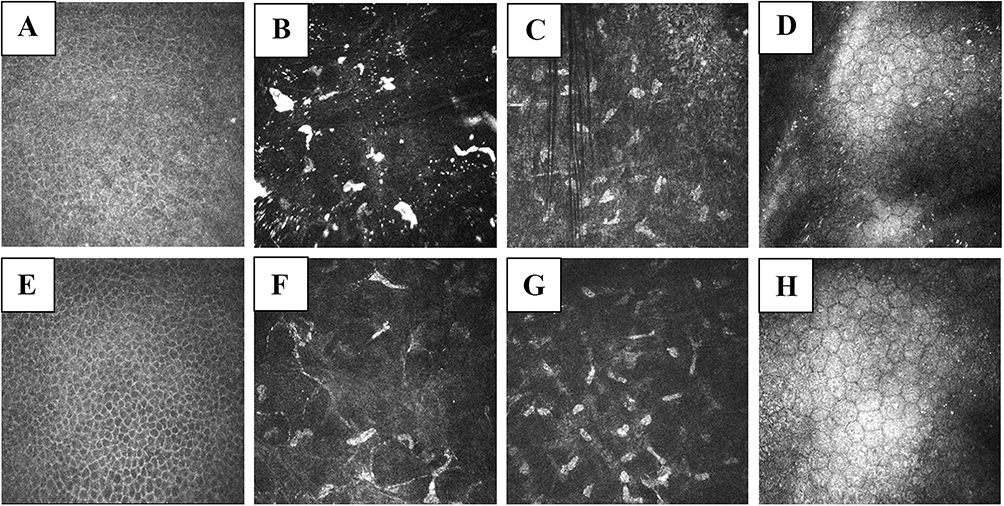 |
Figure 3 IVCM images 12 months postoperatively. (A–D) FECD group: (A) Corneal epithelium showing regular cellular morphology and resolution of epithelial edema. (B) Donor-recipient interface demonstrating reflective particles and gradual remodeling/decomposition of primary endothelial lesions. (C) Donor graft stroma showing quiescent keratocytes and a stable extracellular matrix. (D) Well-preserved donor corneal endothelial layer with distinct hexagonal cell borders. (E–H) Non-FECD group: (E) Normal corneal epithelial layer with regular hexagonal cells. (F) Donor-recipient interface showing a clearer optical zone with fewer micro-precipitations or fibrotic strands compared to the FECD group. (G) Donor graft stroma exhibiting a stable stromal architecture similar to the FECD group. (H) Functional donor endothelial cells demonstrating acceptable cell density and regular morphology. |
Graft Status Comparison: Femtosecond Laser-Assisted Vs. Manual Technique
Assessment of graft morphology and interface quality indicated that femtosecond laser-assisted grafts (F-nDSAEK) exhibited superior adherence and smoother interfaces during the follow-up period compared to grafts prepared using a standard microkeratome (M-nDSAEK) (Figure 4).
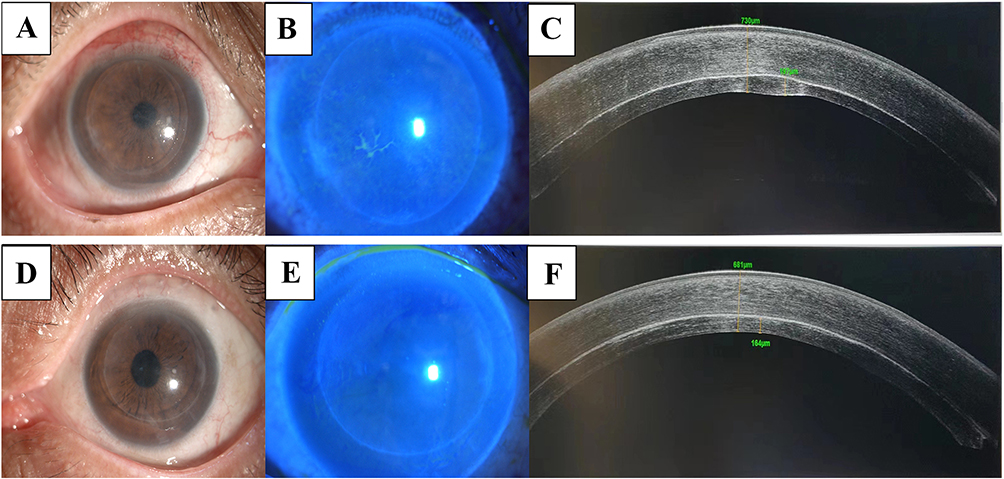 |
Figure 4 Comparison of recovery between manual nDSAEK (M-nDSAEK) and femtosecond-assisted nDSAEK (F-nDSAEK). (A–C) M-nDSAEK group: (A) Slit-lamp photograph showing mild diffuse graft haze. (B) Corneal fluorescein staining revealing localized epithelial defects. (C) Anterior segment OCT (AS-OCT) demonstrating a less uniform graft profile with a total central corneal thickness (CCT) of 730 µm. (D–F) F-nDSAEK group: (D) Slit-lamp photograph showing a clear corneal graft and stable anterior segment. (E) Fluorescein staining showing a smooth, well-epithelialized ocular surface. (F) AS-OCT demonstrating a highly uniform donor lenticule morphology (graft thickness: 164 µm) with a smoother donor-recipient interface and a thinner CCT of 601 µm. |
Postoperative ECD and Corneal Thickness
Preoperative ECD could not be recorded in several cases due to severe corneal edema limiting measurement accuracy. At one month postoperatively, the mean ECD was 2622.58 ± 405.93 cells/mm2. A rapid decline in cell density was observed within the first year, followed by a stabilization phase between the second and third years (Table 1). The mean preoperative CCT was 720.14 ± 25.38 μm, which initially increased to 804.41 ± 57.87 μm at one month before gradually decreasing. While ECD in FECD cases was lower than in non-FECD cases during the first six months, these differences did not remain statistically significant over the long term (Table 1).
Visual Outcomes and Improvement
Preoperatively, all 114 eyes presented with a BCVA worse than 1.0 logMAR. At the final follow-up, six eyes achieved a BCVA better than 0.523 logMAR. Visual acuity improved in both FECD and non-FECD groups, though the non-FECD group demonstrated slightly superior visual outcomes at the three-month postoperative mark compared to the FECD group (Table 2).
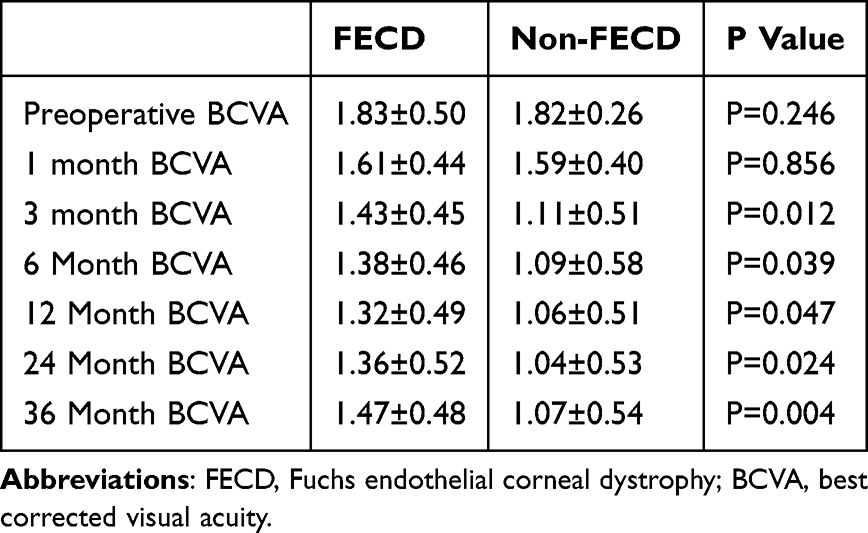 |
Table 2 FECD and Non-FECD Patients Preoperative and Postoperative Follow-Up BCVA (LogMAR) |
Complications and Risk Factors
During the follow-up period, the overall safety profile of this specific cohort was highly favorable. Complications included four cases of graft rejection (3.50%) and seven cases of recurrent bullous changes within five years (6.14%). Secondary glaucoma developed in four cases (3.50%), all of which manifested as transient intraocular pressure (IOP) spikes within the first 2 weeks postoperatively and were successfully managed via topical medication alone, with no further surgical intervention required. Notably, there was a 0% incidence of cystoid macular edema (CME), Urrets-Zavalia syndrome, and interface infections. Graft detachment requiring a rebubbling procedure occurred in only 3 out of 114 eyes (2.63%). No serious adverse events, such as endophthalmitis or systemic reactions, were reported. Mild blurred vision or dry eye symptoms observed during long-term follow-up were successfully managed with artificial tears.
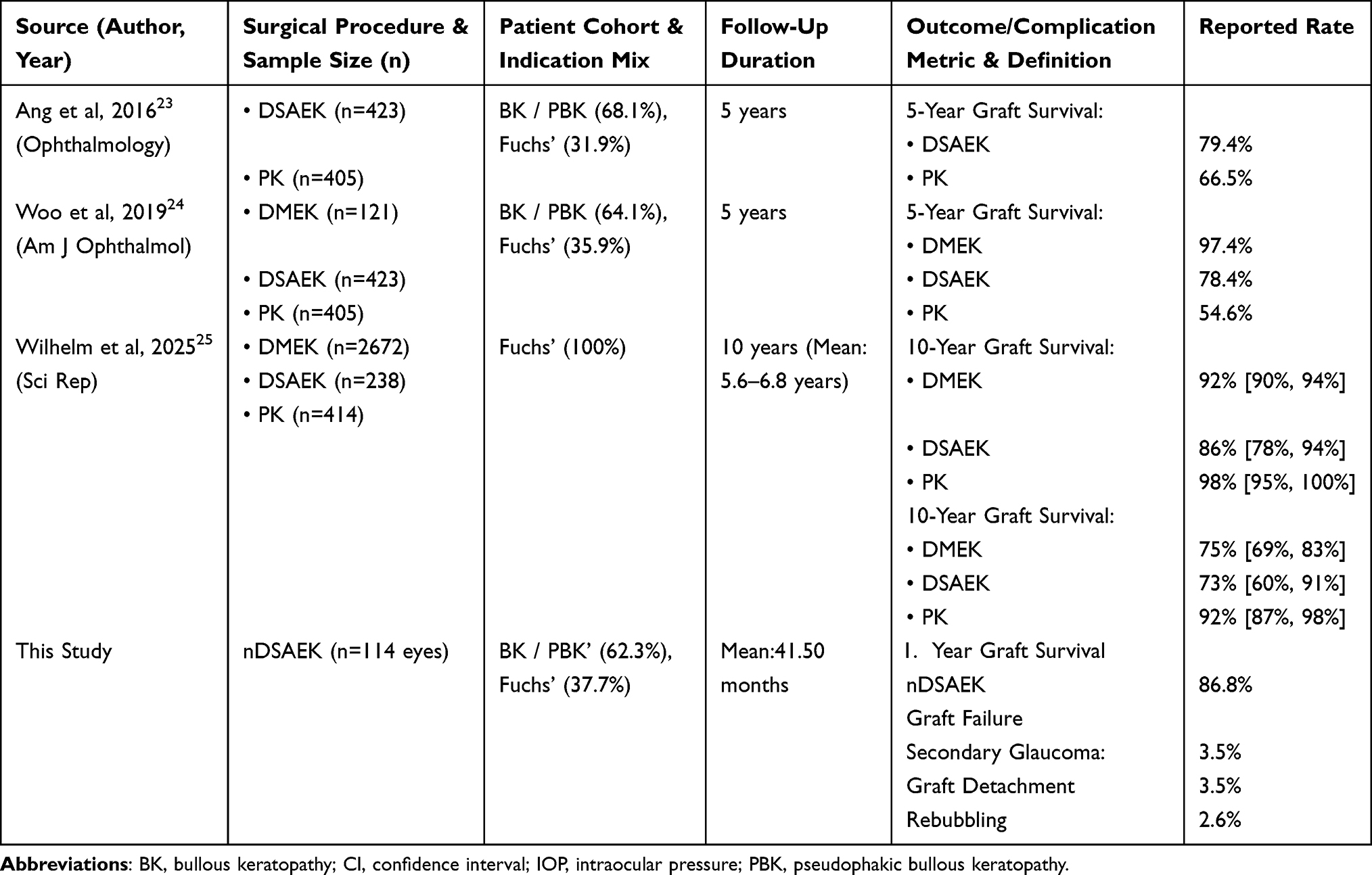 |
Table 3 Comparison of Clinical Outcomes Among Different Endothelial Keratoplasty Techniques |
Benchmarking nDSAEK Against Established EK Techniques
As detailed in Table 3, different EK techniques present distinct clinical profiles. Compared to DMEK, which typically achieves superior visual recovery, nDSAEK provided sustained corneal clarity and functional visual restoration in complex cases, characterized by acceptable ECD loss and a lower rate of rebubbling (Table 3 and Figure 5). Regarding endothelial attrition, nDSAEK exhibited a decline trend consistent with conventional DSAEK, with an overall attrition rate lower than that reported in prominent DMEK literature (Figure 6).
 |
Figure 5 Comparison of visual acuity improvement across EK techniques. BCVA improvement (ΔlogMAR) from baseline to the last follow-up. While DMEK shows the greatest improvement, nDSAEK is clinically demonstrated visual and anatomical trends that align with historical DSAEK cohorts, particularly in patients with poor preoperative vision and complex surgical histories. |
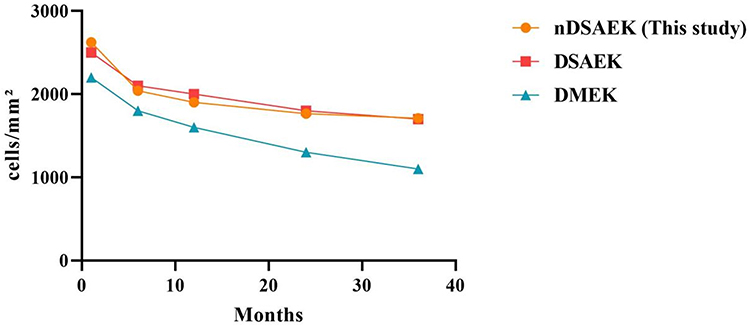 |
Figure 6 Longitudinal changes in endothelial cell density (ECD). nDSAEK demonstrates a more gradual long-term ECD reduction compared to DMEK, maintaining acceptable survival over time in complex eyes. |
AI-Driven Risk Prediction and Long-Term Performance
An XGBoost-based machine learning model utilizing 10 clinical features was developed to predict graft failure. Among the 114 included longitudinal eyes, a total of 15 cases (13.16%) experienced true clinical functional graft failure during the follow-up window. Given the event-per-variable ratio of 1.36, the predictive modeling was prospectively defined as an exploratory and hypothesis-generating framework.
The time-dependent ROC analysis revealed robust predictive accuracy for both short-term and long-term outcomes, demonstrating validated AUC values of 0.917 (95% CI: 0.819–1.000) at 12 months, 0.920 (95% CI: 0.823–1.000) at 24 months, and 0.880 (95% CI: 0.765–0.995) at 36 months (Figure 7). In addition to strong discrimination, the framework exhibited high calibration fidelity. The overall calibration slope was 1.322, a calibration-in-the-large of 0.04, Harrell’s C-index of 0.865 (95% CI: 0.742–0.988), and the 36-month integrated Brier score was exceedingly low at 0.03, indicating minimal residual variance between predicted risk and actual graft failure events.
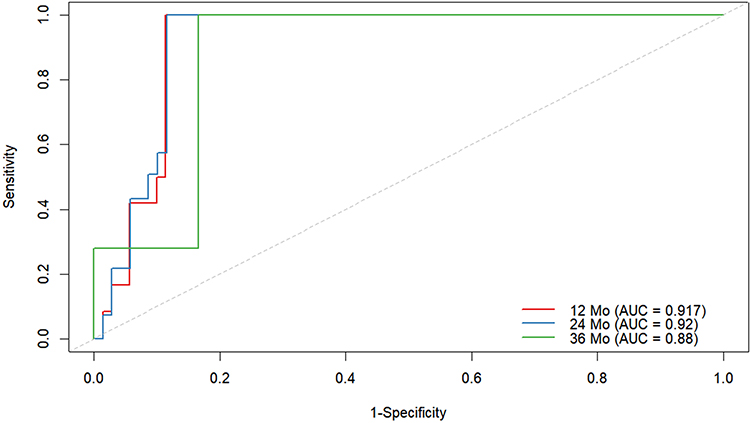 |
Figure 7 Time-Dependent ROC Analysis for Graft Failure. Receiver Operating Characteristic (ROC) curves showing the predictive accuracy of the AI model at 12 months (red, AUC = 0.917, 95% CI: 0.819–1.000), 24 months (blue, AUC = 0.92, 95% CI: 0.823–1.000), and 36 months (green, AUC = 0.88, 95% CI: 0.765–0.995). The dashed diagonal line represents the threshold for chance-level prediction. |
Risk Stratification and Clinical Net Benefit
Using the median AI risk score as a threshold, patients were stratified into High-Risk and Low-Risk groups. Kaplan-Meier analysis demonstrated nearly 100% survival in the Low-Risk group over 60 months, whereas the High-Risk group showed a significant decline in graft survival (log-rank p < 0.0001; Figure 8).
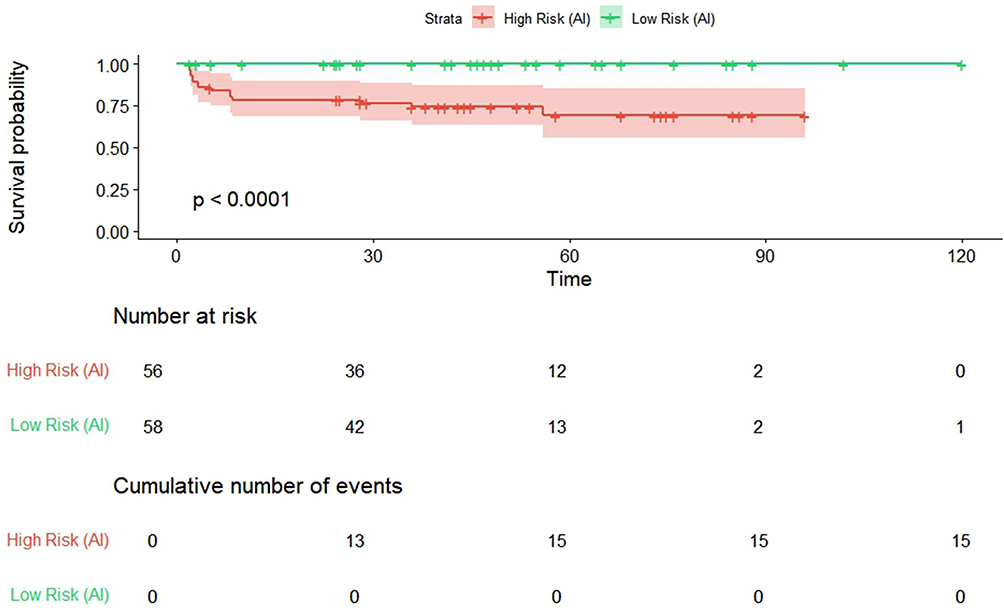 |
Figure 8 AI-Based Risk Stratification for Graft FailureLegend. Kaplan-Meier curves illustrating survival probability for High Risk (red, n = 46) and Low Risk (green, n = 47) patients as identified by the AI model. The shaded areas represent 95% confidence intervals. The significantly different trajectories (p < 0.0001) underscore the model’s ability to identify patients at high risk of failure early in the postoperative course. |
SHAP-Based Mechanistic Insights
SHAP analysis identified FS assistance and the primary disease process as the most influential predictors of graft outcome (Figure 9). A history of prior glaucoma surgery and advanced age correlated with increased risk, whereas FS assistance and higher preoperative ECD were identified as pivotal protective factors. Notably, a simulated sensitivity analysis omitting preoperative ECD completely eliminated the model’s discriminative variance. This highlights that while the algorithm achieves high predictive accuracy, the incorporation of baseline cell density remains an absolute biological prerequisite for reliable long-term graft failure risk stratification.
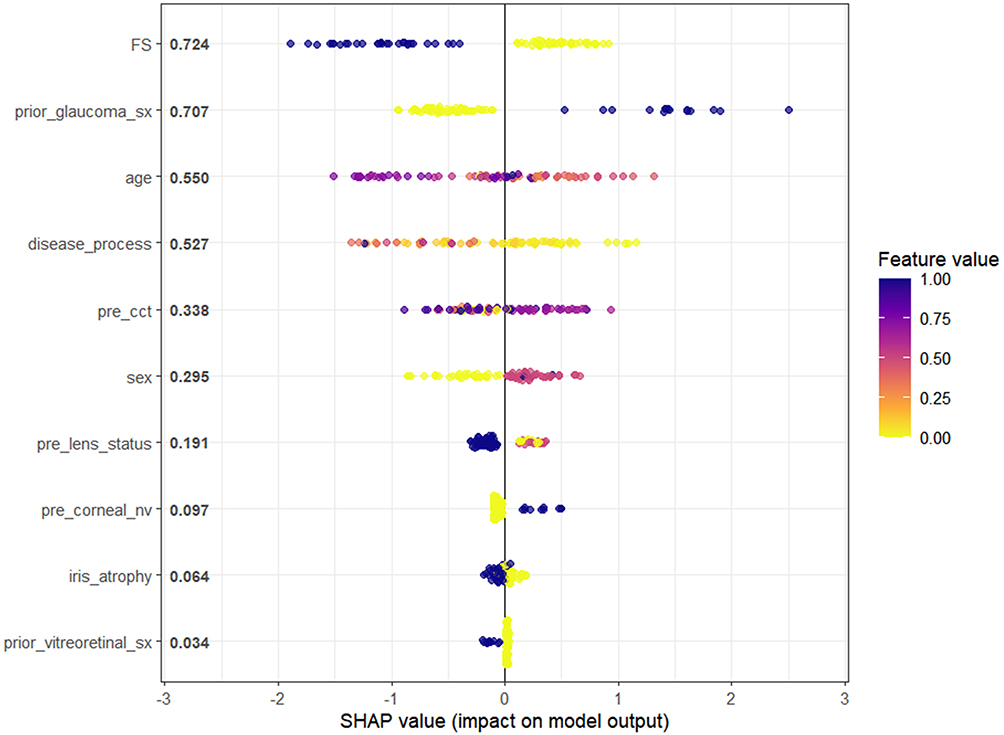 |
Figure 9 SHAP summary plot illustrating the relative importance and directional impact of clinical features on graft failure prediction. Each point represents an individual eye, with the color indicating the relative feature value (purple for high, yellow for low). Feature ranking is derived via the TreeSHAP algorithm. |
LMM demonstrated a significant global postoperative ECD decay rate of −21.55 cells/mm2 per month (p < 0.001). The longitudinal trajectory of cell loss diverged significantly based on the surgical technique; the implementation of F-nDSAEK yielded a substantially higher baseline cellular reservoir (+133.03 cells/mm2, p = 0.0005), although it exhibited a marginally faster monthly attrition rate compared to manual techniques (−4.37 cells/mm2 per month, p = 0.002). Crucially, after adjusting for all covariates, the F-nDSAEK cohort maintained consistently higher predicted ECD levels throughout the 36-month follow-up period compared to the manual group (Figure 10). The longitudinal ECD trajectories modeled by the REML random-intercept linear mixed framework represent marginal predictions over the random effects, treating the variance of the individual random components as zero.
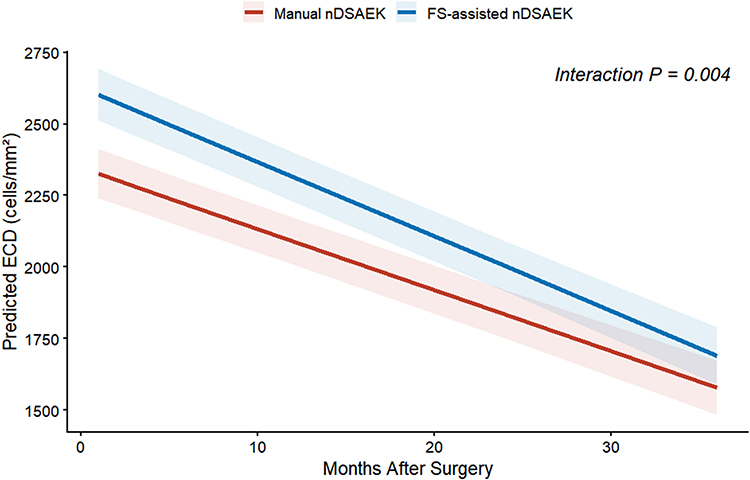 |
Figure 10 ECD Loss Trajectory. Full Covariate-Adjusted Model.Predicted ECD decay over 36 months postoperative, derived from the Linear Mixed-Effect Model. The plot compares FS-assisted nDSAEK (blue line) and Manual nDSAEK (red line), adjusted for age, sex, ocular history, and lens status. Solid lines represent the mean predicted values, shaded areas represent the 95% confidence interval, and background dots show the raw longitudinal data points. |
Furthermore, the LMM identified several independent clinical factors significantly impacting postoperative cell reserves. Preserved preoperative lens status (+87.69 cells/mm2, p = 0.001) and a history of prior glaucoma surgery (+77.90 cells/mm2, p = 0.027) were independent positive predictors of the initial postoperative cellular baseline. Conversely, a history of prior cataract surgery was independently associated with a reduced cellular baseline (−99.47 cells/mm2, p = 0.047).
Discussion
Our long-term data confirm the effectiveness of nDSAEK in consistently clearing the cornea and restoring functional sight for patients with low-vision CED. Unlike surgical techniques that aim for an anatomically ideal interface through stripping, nDSAEK preserves the recipient’s DM to minimize surgical trauma to the posterior stroma. This approach allows the donor-recipient interface to stabilize during long-term follow-up, often reaching a state of near-fusion without compromising corneal transparency or daily visual function. Particularly in complex cases involving post-cataract endothelial decompensation, prior ocular trauma, or vitrectomy, nDSAEK demonstrated favorable tolerance and a controllable complication profile.
However, these long-term outcomes must be interpreted strictly within the specific clinical context of our cohort, which comprised individuals with exceptionally advanced, late-stage disease characterized by multiple dense ocular comorbidities and severely limited baseline visual potential. Consequently, the clinical success of nDSAEK in this specific population should not be benchmarked against the peak visual acuity outcomes typically reported in standard conventional DSAEK or DMEK registries. Instead, the therapeutic objective was primarily tectonic rehabilitation, pain relief, and the restoration of what we operationally define as functional vision. Specifically, this equates to navigational and ambulatory vision which successfully preserves a patient’s independent daily mobility despite their advanced pathology.
Long-term follow-up data further suggest that although ECD in both FECD and non-FECD groups experienced an initial decline, it eventually reached a plateau. Concurrently, corneal thickness gradually normalized as edema resolved, reflecting the sustained functional viability of the transplanted endothelium. Notably, the degree of postoperative visual improvement was closely correlated with preoperative visual status rather than patient age or disease duration. This finding suggests that in low-vision patients, the clinical objective of nDSAEK should focus on restoring and maintaining stable functional vision rather than solely pursuing peak BCVA. We contend that nDSAEK, especially when integrated with femtosecond laser-assisted technology, provides a safe and effective therapeutic option for patients with complex CED.
Research has confirmed that the nDSAEK technique facilitates tight adherence between the donor graft and host cornea even without stripping the host DM.26 While concerns were initially raised regarding postoperative visual outcomes and interface quality, multiple studies have established the non-inferiority of nDSAEK compared to standard DSAEK.27–29 Omoto et al conducted a five-year follow-up of nDSAEK and DSAEK cases and found no statistically significant differences in ECD or BCVA changes between the two groups at any time point.30 Furthermore, Kamiya et al analyzed the impact of both techniques on intraocular forward scattering and higher-order aberrations (HOAs); their findings indicated no significant differences in postoperative Objective Scatter Index (OSI), corneal HOAs, logMAR UCVA, or logMAR BCVA between the DSAEK and nDSAEK subgroups.31 This suggests that the presence or absence of the host DM has no substantial impact on postoperative visual quality, HOAs, or intraocular scattering. A plausible explanation is that the DM is a thin, morphologically uniform structure whose impact on optical quality is minimal.
The pathogenesis of FECD involves complex extracellular matrix abnormalities within the DM, leading to guttata formation and endothelial dysfunction.32 Traditionally, removing the diseased DM was considered an indispensable step in endothelial keratoplasty to influence graft attachment. However, in our nDSAEK cohort for FECD, we observed that primary endothelial lesions gradually dissipated over time and transformed into clinically inactive fibrotic regions, while the donor endothelial grafts maintained stable function without signs of recurrence. These findings suggest that preserving the DM does not necessarily compromise graft adherence or long-term endothelial function. This aligns with the perspective that nDSAEK reduces interference with posterior stromal fibers and maintains the DM’s structural support for the trabecular meshwork, thereby potentially reducing the risk of glaucoma induced by trabecular distortion.33 We hypothesize that nDSAEK alters the local microenvironment by restoring endothelial pump function, which may inhibit further pathological matrix deposition and allow the underlying diseased endothelium to become quiescent.
In this cohort, we observed an early postoperative decline in ECD without significant intraoperative or postoperative complications, a phenomenon commonly seen in other types of endothelial keratoplasty.34 Our three-year follow-up results confirm that nDSAEK maintains adequate ECD to preserve corneal transparency. Surgical technique also significantly influences graft survival. In cases with irregular posterior corneal surfaces or fragile corneas, nDSAEK reduces surgical manipulation and avoids complications such as wound dehiscence or perforation.35 Thus, in the context of donor tissue scarcity, nDSAEK represents a viable option for treating both Fuchs’ and non-Fuchs’ CED. Previous studies have indicated that graft failure following endothelial surgery is associated with a reduction in postoperative endothelial cell counts.36–38
Compared to manual techniques, FS-nDSAEK offers improved visual outcomes and minimizes endothelial cell loss while resulting in minimal refractive changes. The precision of femtosecond technology eliminates the need for enlarged graft diameters, which reduces the area of denuded stroma required for endothelial cell migration.39 Our study indicates that precise cutting with a femtosecond laser creates a smoother donor-host interface to reduce irregularities caused by corneal clearing. This may accelerate the functional recovery of the graft endothelium, subsequently reducing stromal scarring and improving visual prognosis. Consequently, meticulous clinical evaluation is required for patients with good early vision but endothelial decompensation to avoid missing the optimal window for intervention. The incorporation of FS-nDSAEK represented a significant technical evolution in our cohort. Our LMM analysis, which adjusted for ten clinical covariates, confirmed that the FS-assisted group maintained higher predicted ECD levels throughout the follow-up period compared to the manual dissection group. We must also acknowledge that our direct statistical comparison between FS-nDSAEK and manual M-nDSAEK techniques is inherently vulnerable to indication bias, as the selection of the femtosecond laser was likely directed by specific anatomical favorability or varying anterior segment complexities during the long enrollment window. Because the sample size constraints and historical nature of the dataset precluded the robust implementation of propensity score matching, this lack of random allocation remains a major source of selection bias, meaning the superior cellular retention observed in the FS-nDSAEK cohort may partially reflect a less complicated baseline pathology rather than purely technical superiority.
Structurally, AS-OCT imaging demonstrated that FS-assisted grafts achieved superior morphological uniformity and a smoother donor-recipient curvature. We suspect that the ultra-precise nature of femtosecond technology reduces physical stress on the graft, fostering a more stable environment that potentially reduces the initial drop-off of endothelial cells during the healing phase. This anatomical stability is particularly advantageous in the nDSAEK procedure, where the preservation of the host DM necessitates an exceptionally precise graft fit to ensure long-term adherence and transparency.
A key innovation of this study is the integration of an XGBoost-based machine learning framework to address the inherent prognostic uncertainty in complex nDSAEK cases. Our model demonstrated robust predictive performance, achieving AUC values between 0.88 and 0.92 across a 36-month horizon. While traditional clinical assessments often rely on isolated parameters such as ECD, our AI approach synthesizes eleven multidimensional features to provide a personalized risk profile. The high AUC values, particularly in the early postoperative phase from 12 to 24 months, suggest that the model can effectively identify high-risk grafts before clinical decompensation becomes irreversible. This transition from reactive to proactive management allows for intensified follow-up or early therapeutic intervention, which is crucial for low-vision patients with limited secondary treatment options. Furthermore, we employed SHAP analysis to enhance model interpretability, quantifying the specific contribution of each clinical variable to graft failure. SHAP values identified FS-assistance and prior glaucoma surgery as the most influential determinants of long-term survival. The model revealed that complex surgical histories, especially those related to glaucoma, significantly increased the risk trajectory, whereas the use of femtosecond laser technology exerted a profound protective effect. This interpretability is vital for clinical adoption, as it corroborates traditional surgical intuition with data-driven evidence, allowing surgeons to better counsel patients regarding their individualized long-term prognosis.
This study has several limitations. First, all procedures were performed by a single surgeon (HW). While this eliminates inter-operator confounding, it precludes the assessment of inter-rater reproducibility and lacks grader masking for specular microscopy. Second, our donor cohort was exceptionally young (12–30 years) compared to international standards (30–75 years) and preserved via a 12-hour moist chamber rather than Optisol-GS. Although ethically compliant with local regulations, the higher baseline ECD of younger tissue may favor graft survival, limiting immediate generalizability to centers using standard older donor tissue. Third, the exclusion of high-risk cases requiring systemic immunosuppression introduced a selection bias, filtering out patients with a high a priori failure risk; consequently, the downstream machine learning framework represents an optimized predictive model calibrated specifically for standard-risk trajectories. Finally, this study is limited by its retrospective design, which resulted in the unavailability of certain postoperative ocular biomarkers. Standardized quantitative endothelial morphometry such as coefficient of variation (CV) of cell area and hexagonality could not be performed on the chronological IVCM images. While qualitative lesion resolution and structural remodeling were thoroughly captured, the lack of continuous, software-driven quantification limits our ability to model precise ultrastructural dynamics. Future prospective trials with standardized digital IVCM export protocols are warranted to corroborate these morphological transformations. Additionally, data collection from a single tertiary center may limit the sample size and the generalizability of the findings. Although a formal meta-analysis was not conducted, integrating our long-term nDSAEK efficacy data with previously published EK data provides important clinical context. This approach allows for a direct interpretation of the real-world performance of nDSAEK while avoiding the heterogeneity introduced by pooling fundamentally different study designs and patient populations.
Conclusion
nDSAEK provides stable long-term visual and anatomical outcomes in low-vision patients with both FECD and non-FECD. Rather than positioning this technique as a direct equivalent to conventional DSAEK or DMEK, our data support its specific utility in complex or structural rehabilitation cases where the primary goals are tectonic stabilization, pain relief, and the restoration of basic ambulatory and navigational vision. Therefore, for CED patients with recurrent surgeries or damaged recipient tissue structures unsuitable for stripping, nDSAEK is an excellent alternative, particularly in scenarios of corneal donor shortage.
Furthermore, while the integrated machine learning framework demonstrated high internal discriminative capacity for identifying long-term graft failure risk, it remains strictly an internally validated, exploratory tool. Due to the lack of multicenter external validation and a low event-per-variable ratio, this model is not yet ready for clinical deployment and should be viewed solely as a preliminary framework for risk stratification requiring rigorous external benchmarking.
Abbreviations
nDSAEK, non-Descemet stripping automated endothelial keratoplasty; IOP, intraocular pressure; BCVA, best-corrected visual acuity; CED, Corneal endothelial cell dysfunction; OCT, optical coherence tomography.
Data Sharing Statement
The data presented in this study are included within the article. The full datasets are not publicly available due to privacy and ethical restrictions. However, they may be requested from the corresponding authors. To facilitate data access requests, Huping Wu (Email: [email protected]) serves as the designated contact. Data release is subject to approval from the sponsor and compliance with data privacy and ethical guidelines.
Ethics Approval and Informed Consent
The studies involving human participants were reviewed and approved by the Human Ethics Committee of Xiamen University affiliated with the Xiamen Eye Center (XMYKZX-KY-2025-057). All participants provided written informed consent to participate in this study.
Funding
This research was supported by Fujian Provincial Natural Science Foundation of China (2026J0011700), Xiamen city high-quality Development Science and Technology Program youth scientific research project (2024GZL-QN003), Xiamen Medical and Health Guidance Project (3502Z20254ZD1267). The funding sources had no role in the design and conduct of the study; collection, analysis, and interpretation of the data; preparation, review, approval, and submission of the manuscript.
Disclosure
Yuan Lin, Yiming Hu, and Zhiwen Xie are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Peng P, Yu Y, Ma W. et al. Proteomic characterization of aqueous humor in corneal endothelial decompensation after penetrating keratoplasty. Exp Eye Res. 2023;230:109457. doi:10.1016/j.exer.2023.109457
2. Hsu KM, Chang SH, Brothers W, Edelstein SL, Hsu HY, Harocopos GJ. Indications for Keratoplasty at 3 Academic Centers from 2002 to 2012. Eye Contact Lens. 2016;42(6):374–17. doi:10.1097/ICL.0000000000000227
3. Feizi S. Corneal endothelial cell dysfunction: etiologies and management. Ther Adv Ophthalmol. 2018;10:2515841418815802. doi:10.1177/2515841418815802
4. Wu H, Dong N, Xie S, Li C, Li X, Liu Z. Non-Descemet stripping endothelial keratoplasty for treating iridocorneal endothelial syndrome in phakic eyes. Chin J Ophthalmol. 2011;47(5):6.
5. Wajima H, Hayashi T, Kobayashi A, et al. Graft rejection episodes after keratoplasty in Japanese eyes. Sci Rep. 2023;13(1):2635. doi:10.1038/s41598-023-29659-w
6. Tóth G, Váncsa S, Kói T, Kormányos K, Hegyi P, Szentmáry N. Outcomes of Penetrating Keratoplasty Versus Lamellar Endothelial Keratoplasty in Iridocorneal Endothelial Syndrome: a Systematic Review and Meta-Analysis. Am J Ophthalmol. 2025;276:218–229. doi:10.1016/j.ajo.2025.04.017
7. Matthaei M, Hribek A, Clahsen T, Bachmann B, Cursiefen C, Jun AS. Fuchs Endothelial Corneal Dystrophy: clinical, Genetic, Pathophysiologic, and Therapeutic Aspects. Annu Rev Vis Sci. 2019;5(1):151–175. doi:10.1146/annurev-vision-091718-014852
8. Viberg A, Samolov B, Byström B. Descemet Stripping Automated Endothelial Keratoplasty versus Descemet Membrane Endothelial Keratoplasty for Fuchs Endothelial Corneal Dystrophy: a National Registry-Based Comparison. Ophthalmology. 2023;130(12):1248–1257. doi:10.1016/j.ophtha.2023.07.024
9. Ang M, Mehta JS, Lim F, Bose S, Htoon HM, Tan D. Endothelial cell loss and graft survival after Descemet’s stripping automated endothelial keratoplasty and penetrating keratoplasty. Ophthalmology. 2012;119(11):2239–2244. doi:10.1016/j.ophtha.2012.06.012
10. Singh R, Gupta N, Vanathi M, Tandon R. Corneal transplantation in the modern era. Indian J Med Res. 2019;150(1):7–22. doi:10.4103/ijmr.IJMR_141_19
11. Schrittenlocher S, Schlereth SL, Siebelmann S, et al. Long-term outcome of descemet membrane endothelial keratoplasty (DMEK) following failed penetrating keratoplasty (PK). Acta Ophthalmol. 2020;98(7):e901–e906. doi:10.1111/aos.14417
12. Price Jr FW, Price MO. Endothelial keratoplasty to restore clarity to a failed penetrating graft. Cornea. 2006;25(8):895–899. doi:10.1097/01.ico.0000227888.03877.22
13. Masaki T, Kobayashi A, Yokogawa H, Saito Y, Sugiyama K. Clinical evaluation of non-Descemet stripping automated endothelial keratoplasty (nDSAEK). Jpn J Ophthalmol. 2012;56(3):203–207. doi:10.1007/s10384-012-0123-x
14. Chaurasia S, Ramappa M, Sangwan VS. Clinical outcomes of non-Descemet stripping automated endothelial keratoplasty. Int Ophthalmol. 2012;32(6):571–575. doi:10.1007/s10792-012-9615-4
15. Sun JP, Hu FR, Chen YM, Chu HS, Chen WL. Change of recipient corneal endothelial cells after non-descemet’s stripping automated endothelial keratoplasty in a rabbit model. Invest Ophthalmol Vis Sci. 2014;55(12):8467–8474. doi:10.1167/iovs.13-13544
16. Yamazaki R, Nejima R, Ichihashi Y, Miyata K, Tsubota K, Shimmura S. Descemet stripping and automated endothelial keratoplasty (DSAEK) versus non-Descemet stripping and automated endothelial keratoplasty (nDSAEK) for bullous keratopathy. Jpn J Ophthalmol. 2020;64(6):585–590. doi:10.1007/s10384-020-00767-8
17. Zhang T, Li SW, Chen TH, et al. Clinical results of non-Descemet stripping endothelial keratoplasty. Int J Ophthalmol. 2017;10(2):223–227. doi:10.18240/ijo.2017.02.07
18. Vasiliauskaite I, Kocaba V, van Dijk K, et al. Long-Term Outcomes of Descemet Membrane Endothelial Keratoplasty: effect of Surgical Indication and Disease Severity. Cornea. 2023;42(10):1229–1239. doi:10.1097/ICO.0000000000003130
19. Chen S, Bai W. Artificial intelligence technology in ophthalmology public health: current applications and future directions. Front Cell Dev Biol. 2025;13:1576465. doi:10.3389/fcell.2025.1576465
20. Liu X, Faes L, Kale AU, et al. A comparison of deep learning performance against health-care professionals in detecting diseases from medical imaging: a systematic review and meta-analysis. Lancet Digit Health. 2019;1(6):e271–e297. doi:10.1016/S2589-7500(19)30123-2
21. Lekadir K, Frangi AF, Porras AR, et al. FUTURE-AI: international consensus guideline for trustworthy and deployable artificial intelligence in healthcare. BMJ. 2025;388:e081554. doi:10.1136/bmj-2024-081554
22. Collins GS, Moons KGM, Dhiman P, et al. TRIPOD+AI statement: updated guidance for reporting clinical prediction models that use regression or machine learning methods. BMJ. 2024;385:e078378. doi:10.1136/bmj-2023-078378
23. Ang M, Soh Y, Htoon HM, Mehta JS, Tan D. Five-Year Graft Survival Comparing Descemet Stripping Automated Endothelial Keratoplasty and Penetrating Keratoplasty. Ophthalmology. 2016;123(8):1646–1652. doi:10.1016/j.ophtha.2016.04.049
24. Woo JH, Ang M, Htoon HM, Tan D. Descemet Membrane Endothelial Keratoplasty Versus Descemet Stripping Automated Endothelial Keratoplasty and Penetrating Keratoplasty. Am J Ophthalmol. 2019;207:288–303. doi:10.1016/j.ajo.2019.06.012
25. Wilhelm TI, Gauché L, Böhringer D, et al. Ten-year outcomes after DMEK, DSAEK, and PK: insights on graft survival, endothelial cell density loss, rejection and visual acuity. Sci Rep. 2025;15(1):1249. doi:10.1038/s41598-025-85138-4
26. Jovanović V, Nikolić L. Graft stability after endothelial keratoplasty. Vojnosanit Pregl. 2015;72(11):989–995. doi:10.2298/VSP140422100J
27. Hatanaka H, Koizumi N, Okumura N, et al. A study of host corneal endothelial cells after non-Descemet stripping automated endothelial keratoplasty. Cornea. 2013;32(1):76–80. doi:10.1097/ICO.0b013e31825d568a
28. Hirayama M, Yamazaki-Hokama R, Suzuki T, Negishi K. Three-year Outcomes of Endothelial Keratoplasty in Late-Stage Elderly Versus Younger Patients. Clin Interv Aging. 2025;20:2737–2747. doi:10.2147/CIA.S544954
29. Lata S, Asif MI, Kalra N, et al. Mi-OCT assisted endothelial keratoplasty in buphthalmic eyes- 2 year outcomes. Indian J Ophthalmol. 2025;73(Suppl 2):S303–s307. doi:10.4103/IJO.IJO_3112_23
30. Omoto T, Toyono T, Inoue T, et al. Comparison of 5-Year Clinical Results of Descemet and Non-Descemet Stripping Automated Endothelial Keratoplasty. Cornea. 2020;39(5):573–577. doi:10.1097/ICO.0000000000002211
31. Kamiya K, Asato H, Shimizu K, Kobashi H, Igarashi A. Effect of Intraocular Forward Scattering and Corneal Higher-Order Aberrations on Visual Acuity after Descemet’s Stripping Automated Endothelial Keratoplasty. PLoS One. 2015;10(6):e0131110. doi:10.1371/journal.pone.0131110
32. Ong Tone S, Kocaba V, Böhm M, Wylegala A, White TL, Jurkunas UV. Fuchs endothelial corneal dystrophy: the vicious cycle of Fuchs pathogenesis. Prog Retin Eye Res. 2021;80:100863. doi:10.1016/j.preteyeres.2020.100863
33. Mohamed A, Ks AR, Chaurasia S, Ramappa M. Outcomes of endothelial keratoplasty in pseudophakic corneal oedema: with or without Descemet’s membrane stripping. Br J Ophthalmol. 2016;100(6):754–756. doi:10.1136/bjophthalmol-2015-306979
34. Terry MA, Chen ES, Shamie N, Hoar KL, Friend DJ. Endothelial cell loss after Descemet’s stripping endothelial keratoplasty in a large prospective series. Ophthalmology. 2008;115(3):488–496.e483. doi:10.1016/j.ophtha.2007.10.035
35. Shah SG, Shah GY. Non-Descemet stripping automated endothelial keratoplasty for post radial keratotomy corneal edema. Indian J Ophthalmol. 2018;66(9):1333–1335. doi:10.4103/ijo.IJO_1281_17
36. Ishii N, Yamaguchi T, Yazu H, Satake Y, Yoshida A, Shimazaki J. Factors associated with graft survival and endothelial cell density after Descemet’s stripping automated endothelial keratoplasty. Sci Rep. 2016;6(1):25276. doi:10.1038/srep25276
37. Feng Y, Qu HQ, Ren J, Prahs P, Hong J. Corneal Endothelial Cell Loss in Femtosecond Laser-assisted Descemet’s Stripping Automated Endothelial Keratoplasty: a 12-month Follow-up Study. Chin Med J. 2017;130(24):2927–2932. doi:10.4103/0366-6999.220320
38. Patel SV, Lass JH, Benetz BA, et al. Postoperative Endothelial Cell Density Is Associated with Late Endothelial Graft Failure after Descemet Stripping Automated Endothelial Keratoplasty. Ophthalmology. 2019;126(8):1076–1083. doi:10.1016/j.ophtha.2019.02.011
39. Sorkin N, Gouvea L, Din N, et al. Five-Year Safety and Efficacy of Femtosecond Laser-Assisted Descemet Membrane Endothelial Keratoplasty. Cornea. 2023;42(2):145–149. doi:10.1097/ICO.0000000000003019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.