Back to Journals » Clinical Interventions in Aging » Volume 20
Long-Term Bedridden Status as a Predictor of in-Hospital Mortality in Older Adults with Community-Acquired Pneumonia: A Retrospective Cohort Study
Received 16 July 2025
Accepted for publication 13 November 2025
Published 22 November 2025 Volume 2025:20 Pages 2145—2151
DOI https://doi.org/10.2147/CIA.S554154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Zheng Wang, Dong Wu
Department of Geriatrics, Peking University Third Hospital, Beijing, People’s Republic of China
Correspondence: Zheng Wang, Email [email protected]
Background: Long-term bedridden elderly individuals face a high risk of community-acquired pneumonia (CAP) amid China’s aging population, yet the specific mortality impact remains insufficiently studied.
Objective: To compare the clinical characteristics and in-hospital mortality between long-term bedridden and ambulatory elderly patients with CAP, and to identify risk factors for mortality.
Methods: This retrospective study included 453 patients aged ≥ 75 years hospitalized with CAP from March 2016 to March 2019, divided into a bedridden group (n = 162) and a non-bedridden group (n = 291). Data on demographics, comorbidities, frailty (modified Frailty Index-5, mFI-5), functional status (Barthel Index), and laboratory parameters (eg, hs-CRP) were collected. Logistic regression analysis was used to identify predictors of in-hospital mortality.
Results: The bedridden group had a significantly higher mortality rate (27.16% vs 2.06%, P < 0.001) and elevated hs-CRP levels (40.2 ± 44.0 mg/L vs 19.9 ± 20.3 mg/L). Multivariate analysis identified bedridden status (OR = 11.99, 95% CI: 4.31– 33.40), respiratory failure (OR = 6.80, 95% CI: 3.03– 15.28), and renal dysfunction (elevated serum creatinine; OR = 1.01, 95% CI: 1.00– 1.02) as independent risk factors for mortality.
Conclusion: Long-term bedridden status is an independent predictor of in-hospital mortality in elderly CAP patients with inflammatory response potentially playing a critical role.
Keywords: bedridden status, community-acquired pneumonia, frailty, inflammation, hs-CRP, mortality
Introduction
China’s accelerated demographic aging has led to a surge in the geriatric population, exacerbating healthcare challenges in an aging society. Age-related declines in physical function increase the prevalence of multiple comorbidities, frailty, and geriatric syndromes among older adults. Currently, approximately 40 million disabled and semi-disabled older adults exist in China, with mobility limitations rising sharply with age—from 5% in the 60–69 group to over 60% in centenarians.1 During the aging process, the body is often in a state of persistent low-grade inflammation, which is now recognized as a key mechanism underlying aging and functional decline. Furthermore, hs-CRP accelerates the aging process by driving chronic inflammation, which induces alterations in DNA methylation, exacerbates genomic instability, and promotes cellular senescence.2 Long-term bedridden status, often resulting from falls, strokes, or other debilitating conditions, amplifies these issues, causing muscle atrophy, malnutrition, and impaired immunity. Notably, bedridden patients exhibit heightened systemic inflammation, as measured by elevated high-sensitivity C-reactive protein (hs-CRP), a key biomarker of innate immune activation and inflammaging.3 This hyperinflammatory state predisposes them to aspiration pneumonia and severe outcomes from infections like community-acquired pneumonia (CAP). Recent studies confirm that bedridden status significantly increases short-term mortality,4,5 underscoring the need to explore its impact on CAP prognosis. This study aims to compare clinical outcomes between bedridden and ambulatory elderly CAP patients, focusing on hs-CRP as an indicator of inflammatory dysregulation to identify mortality risk factors and guide clinical interventions.
Materials and Methods
This retrospective study included older patients (≥75 years old) admitted to the Department of Geriatrics of Peking University Third Hospital due to community-acquired pneumonia (CAP) from March 2016 to March 2019. Patients were divided into two groups based on their functional status at admission: long-term bedridden group and non-bedridden group. General data for all enrolled patients were collected through the hospital medical record system, including demographic data, comorbid diseases, functional status, and relevant laboratory test results.
Inclusion Criteria
CAP Diagnosis Confirmation: The diagnosis of CAP was primarily based on clinical and radiographic criteria as per the IDSA/ATS guidelines,6 including the presence of acute respiratory symptoms (eg, cough, fever, sputum production) along with new infiltrates on chest imaging. Microbiological identification of pathogens was not routinely performed for all patients as this was a retrospective study based on clinical practice data. Therefore, the analysis of specific viral or bacterial contributors to mortality was not feasible within the scope of this study.
Long-term bedridden status defined as: Inability to walk or stand upright for ≥1 month; All ADL performed exclusively in bed; Dependence on caregiver assistance for self-care.
Exclusion Criteria
Non-CAP diagnoses or severe CAP requiring ventilator support; Malignant tumors with life expectancy <1 year; Acute myocardial infarction, cerebrovascular accident, or other acute infectious diseases; Refusal of informed consent by patients or legal representatives.
Functional Status Assessment
The Barthel Index was used to assess the self-care ability of patients at admission. A score of <60 indicated that the patient was not fully self-reliant in daily activities. Additionally, the modified Frailty Index-5 (mFI-5)7 was used to evaluate the frailty status of patients. The mFI-5 score includes five components: diabetes, hypertension requiring treatment, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), and non-independent functional state (Barthel score <60). Each component is scored as 1 point, with a total score >2 indicating frailty.
Comorbidity Assessment
The comorbidity status of patients was evaluated using the age-corrected Charlson Comorbidity Index (ACCI).8 This index combines an age-equivalent score with the Charlson Comorbidity Index, with each decade of age over 40 years adding 1 point to the cumulative score. The ACCI includes 19 diseases, each assigned a specific point value based on its impact on mortality. A total score ≥5 indicates multiple comorbidities.
Laboratory Tests
Laboratory tests performed at admission included complete blood count, hemoglobin levels, serum albumin, serum creatinine, total cholesterol, and high-sensitivity C-reactive protein (hs-CRP) measured via immunoturbidimetric assay. These tests were used to assess the overall health status, systemic inflammation, and potential complications in patients.
Statistical Methods
Data analysis was performed using SPSS 23.0 software (SPSS, Chicago, IL, USA). Normally distributed continuous data were expressed as mean ± standard deviation (SD), and comparisons between groups were conducted using independent sample t-tests. Categorical data were expressed as counts and percentages, and comparisons were made using chi-square tests. Logistic regression analysis was used to identify the main factors influencing mortality during hospitalization. A p-value of <0.05 was considered statistically significant.
Ethics
This study was approved by the Ethics Committee for Medical Science Research of Peking University Third Hospital (Ethics Number: 2024–370-2) and complies with the Declaration of Helsinki.All data were anonymized to protect patient privacy, and informed consent was obtained from all participants or their legal representatives.
Results
A total of 453 older patients (≥75 years old) admitted to the Department of Geriatrics of Peking University Third Hospital due to CAP from March 2016 to March 2019 were included in this study. The study included 453 patients (mean age 84.03 ± 8.18 years; 62.47% male), comprising 162 in the long-term bedridden group and 291 in the non-bedridden group (Table 1).
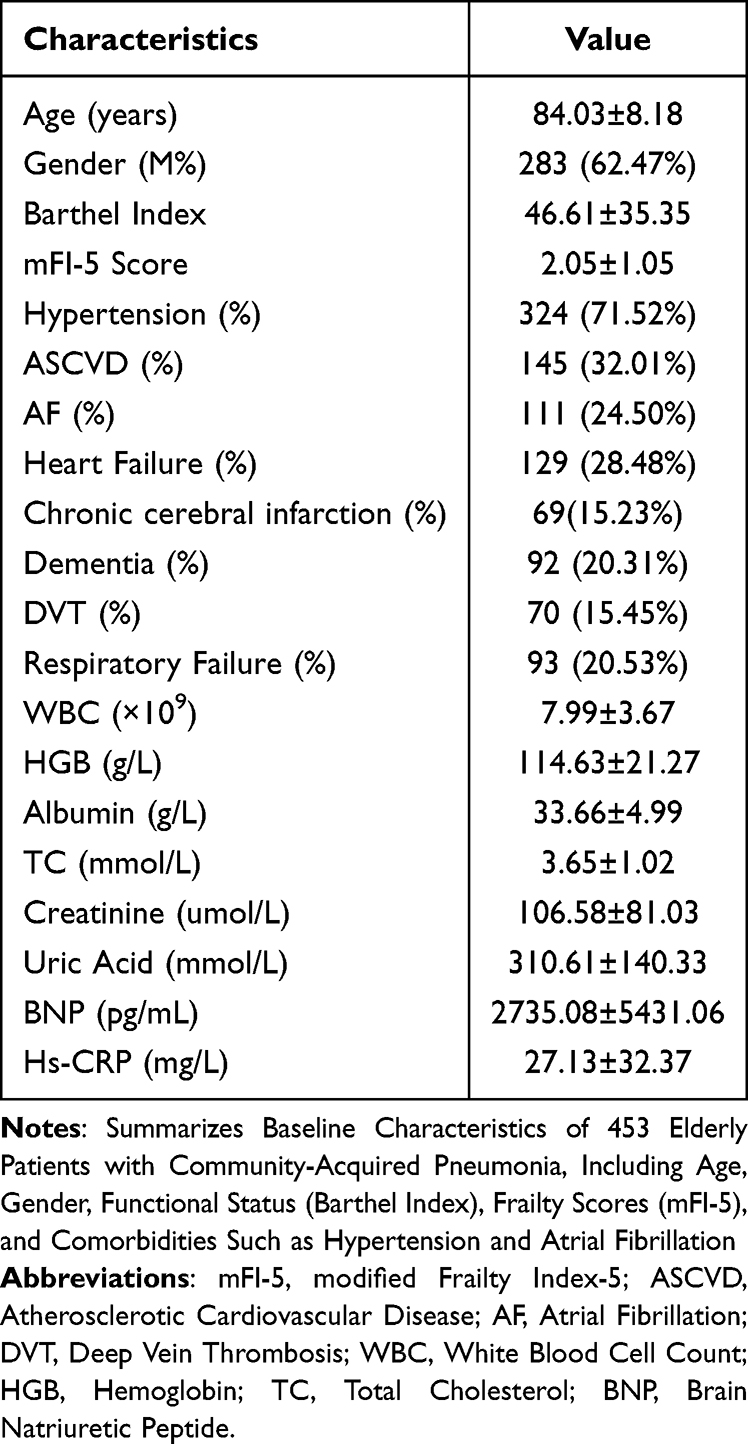 |
Table 1 Baseline Characteristics of the Study Population |
Comparing the long-term bedridden group with the non-bedridden group, the results showed that there were statistically significant differences between the two groups in gender, age, Barthel index, mFI-5 score, and ACCI score (P < 0.05). In terms of comorbid diseases, not only was the ACCI higher in the long-term bedridden group, but there were also its own characteristics in comorbid diseases. The prevalences of atrial fibrillation, cognitive impairment, heart failure, and lower limb deep vein thrombosis had statistically significant differences (P<0.05). While the prevalences of atherosclerotic cardiovascular disease (ASCVD), hypertension, and diabetes had no statistically significant differences (P>0.05). In addition, the laboratory objective test results at admission showed that there were statistically significant differences in white blood cell count, hemoglobin level, total albumin level, and total cholesterol level (P<0.05). Marked differences in inflammatory biomarkers were observed. Bedridden patients presented with significantly higher levels of high-sensitivity C-reactive protein (Hs-CRP) (40.2 ± 44.0 mg/L vs 19.9 ± 20.3 mg/L, p < 0.001) compared to the non-bedridden group, indicating a more severe systemic inflammatory response and a higher likelihood of bacterial infection or sepsis (Table 2).
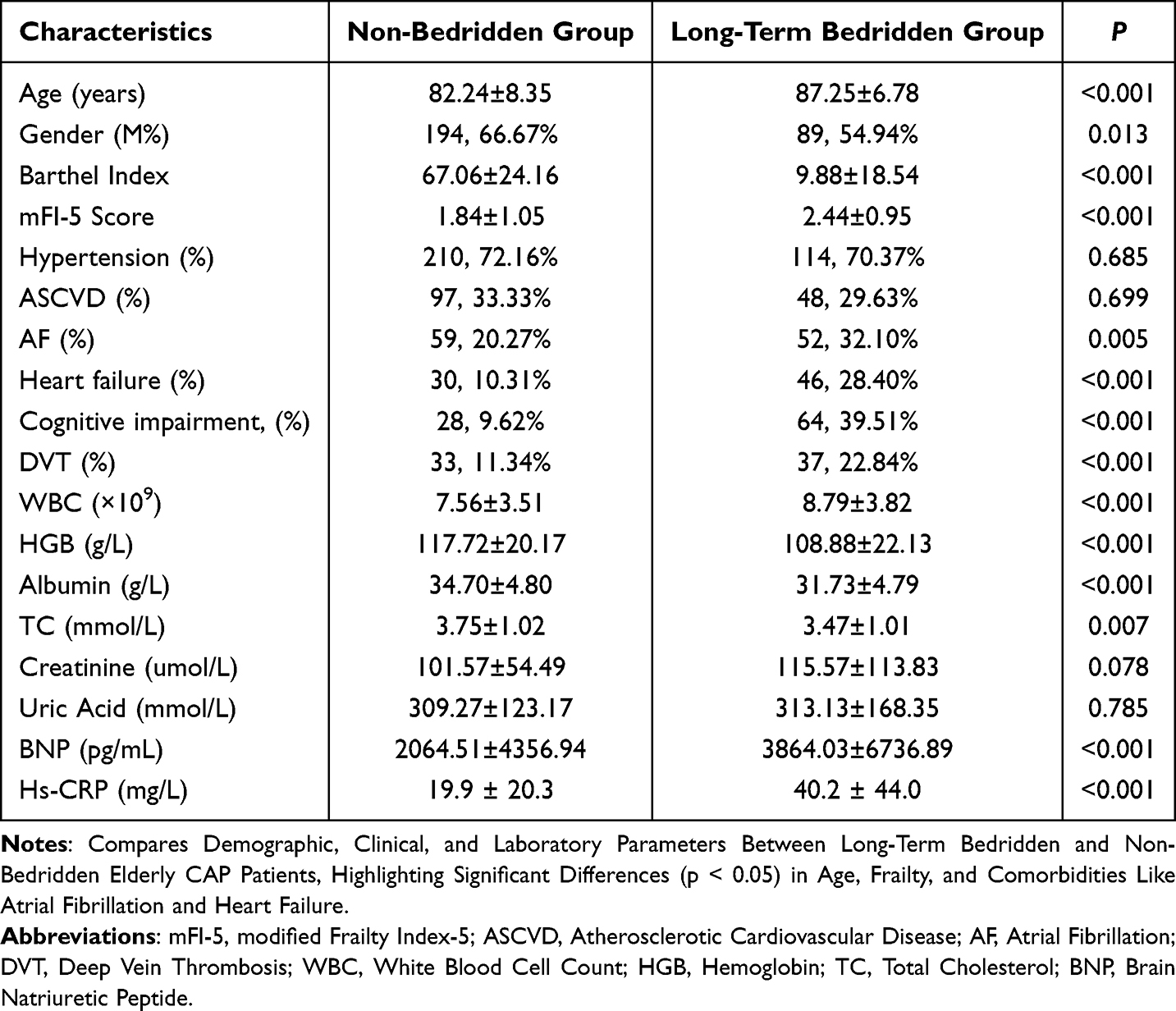 |
Table 2 Comparative Analysis of Clinical Parameters Between Bedridden and Non-Bedridden Older CAP Patients |
Regarding the impact on the mortality rate during hospitalization, a total of 50 patients died for various reasons (11.04%), among which 44 patients died in the bedridden group (27.16%) and 6 patients died in the non-bedridden group (2.06%). The analysis of the causes of death showed that 40 patients died due to aggravated infection, resulting in septic shock and respiratory failure, 4 patients died due to aggravated heart failure, and 6 patients died due to acute myocardial infarction and sudden cardiac death during hospitalization.
Taking the death in hospital event during hospitalization as the observation endpoint for Logistic regression analysis, the results showed that age (OR=1.088, 95% CI =1.017–1.164), admission with respiratory failure (OR=6.799, 95% CI=3.026–15.275), Chronic renal failure (OR=1.009, 95% CI = 1.003–1.015), frailty assessment by mFI-5 score (OR=4.122, 95% CI=1.512–11.238), ACCI score (OR=1.567, 95% CI=0.905–2.654), and long-term bedridden status (OR=11.99, 95% CI=4.305–33.396) were the main influencing factors (Table 3).
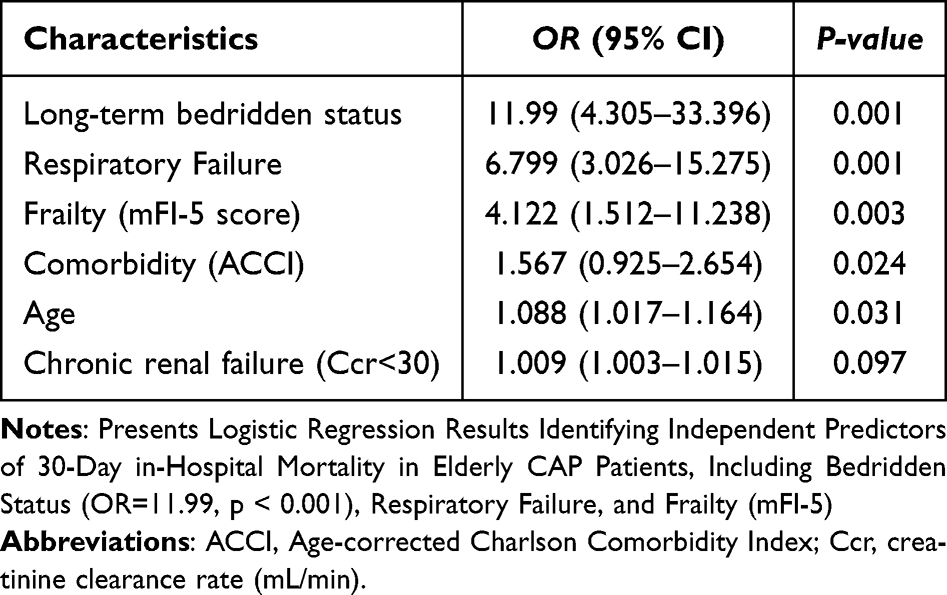 |
Table 3 Logistic Regression Analysis of Factors Influencing in-Hospital Mortality |
Discussion
Our study provides a systematic analysis of clinical characteristics and outcomes in elderly CAP patients who are long-term bedridden. We established bedridden status as a core independent risk factor for adverse CAP-related outcomes. The results demonstrate that long-term bedridden status, defined as the inability to perform basic physiological needs including eating and excretion outside the bed for more than one month, serves as a robust predictor of in-hospital mortality (OR = 11.99, 95% CI: 4.305–33.396). This association is closely linked to a marked inflammatory activation state, evidenced by significantly elevated levels of high-sensitivity C-reactive protein (hs-CRP) (40.2 ± 44.0 mg/L vs 19.9 ± 20.3 mg/L, p < 0.001).
Multivariate analysis further identified respiratory failure (OR = 6.80, 95% CI: 3.03–15.28) and renal insufficiency, reflected by elevated serum creatinine (OR = 1.01, 95% CI: 1.00–1.02), as critical synergistic predictors. These findings indicate that inflammatory response, respiratory dysfunction, and renal impairment collectively contribute to a multifactorial pathophysiological network that exacerbates mortality risk. Notably, bedridden patients exhibited higher frailty scores, as measured by the mFI-5 index, and greater comorbidity burdens, evaluated through ACCI scores, aligning with the “bedridden-disability-elevated mortality” cascade reported by Scarborough et al.9
From a mechanistic perspective, long-term bedridden status aggravates chronic inflammation and organ dysfunction through multiple pathways. Firstly, severely constrained activity space diminishes airway secretion clearance and increases aspiration risk, thereby promoting infection progression. Secondly, bedridden status alters plasma protein profiles, characterized by upregulation of pro-inflammatory mediators, including IL-2, IL-7, and IL-12p70—which are involved in acute T-cell activation and pro-inflammatory responses—and downregulation of anti-inflammatory factors such as IL-9, PDGF-b, and IL-1Ra.10 This leads to immune dysregulation, persistent inflammation, and neurological dysfunction.11 This process strongly resonates with the “inflammaging” concept proposed by Baechle et al,2 wherein chronic low-grade inflammation constitutes a hallmark of aging, and bedridden status acts as a potent accelerator.
Furthermore, renal insufficiency was found to impair drug clearance capacity, intensifying inflammation and multi-organ failure, consistent with the “inflammatory bridge” hypothesis articulated by Singh et al,3 which emphasizes inflammation as a pivotal biological link between aging and disease. Domestic data further validate these mechanisms in the Chinese context: analyses based on the China Health and Retirement Longitudinal Study (CHARLS) database revealed higher prevalences of atrial fibrillation, heart failure, and dementia among bedridden patients in China;12 multicenter studies also confirmed an elevated incidence of hospital-acquired pneumonia (HAP) in this population, with HAP mortality (16.56%) significantly correlated with comorbidity counts and ACCI scores,13,14 underscoring that bedridden status amplifies mortality risk through diverse infectious pathways.
The clinical implications of these findings are substantial: hs-CRP emerges as a practical and sensitive biomarker for early detection of high-risk individuals; for long-term bedridden elderly CAP patients, comprehensive monitoring—encompassing respiratory, renal, and inflammatory parameters—is warranted, coupled with aggressive interventions such as early antimicrobial therapy and inflammation modulation. Future investigations should explore targeted approaches against specific inflammatory pathways, for instance, cytokine manipulation or immune rebalancing, to enhance prognostic outcomes. Additionally, domestic datasets provide a critical foundation for developing risk stratification and precision management strategies tailored to the aging population in China.
Furthermore, our findings are consistent with and extend previous research in this area. Longitudinal data from China has confirmed that bedridden status is a powerful predictor of mortality.1 Similarly, the association between severely restricted life-space mobility (a conceptual cousin to bedridden status) and increased all-cause mortality has been previously established in older cohorts.15 Importantly, the risk factors we identified, such as high comorbidity burden, align with those reported in studies of hospital-acquired pneumonia (HAP) among bedridden patients, underscoring a common pathophysiological pathway toward adverse outcomes regardless of pneumonia acquisition setting.14
Limitations
This study has several limitations. First, while the definition of “long-term bedridden” was based on established functional assessments, the lack of a universally accepted standard may affect the generalizability of our findings. Second, although CAP diagnosis adhered to international guidelines and incorporated hs-CRP to gauge inflammatory response, the absence of pathogen identification and detailed severity stratification might overlook inherent heterogeneity within the patient cohort. Future prospective studies incorporating comprehensive pathogen surveillance are warranted to elucidate the potential interactions between specific infectious agents and the bedridden-induced inflammatory state on mortality outcomes. Third, as a single-center retrospective analysis that focused on in-hospital mortality, our results may not be fully generalizable and likely underestimate the long-term impact of bedridden status. Future prospective, multi-center studies with extended follow-up are warranted to validate our conclusions and explore the long-term outcomes.
Conclusion
Long-term bedridden status, a comprehensive marker of functional dependency, was identified as a strong and independent predictor of in-hospital mortality (OR=11.99) in elderly patients with CAP. Frailty (mFI-5) and multimorbidity burden (ACCI) also significantly contributed to poor prognosis. Clinically, these findings underscore the imperative for vigilant monitoring of systemic inflammation (eg, via hs-CRP) and multi-organ function in bedridden patients, prompting early interventions such as antimicrobial therapy and nutritional support. Future research should prioritize elucidating the underlying inflammatory pathways to facilitate the development of targeted therapeutic strategies.
Data Sharing Statement
The data used in this study are stored at Peking University Third Hospital and are not publicly available due to ethical restrictions and patient confidentiality.
Disclosure
The authors declare no conflicts of interest.
References
1. Cao J, Wang TT, Li Z, et al. Factors associated with death in bedridden patients in China: a longitudinal study. PLoS One. 2020;15(1):e0228423. doi:10.1371/journal.pone.0228423
2. Baechle JJ, Chen N, Makhijani P, et al. Chronic inflammation and the hallmarks of aging. Mol Metab. 2023;74:101755. doi:10.1016/j.molmet.2023.101755
3. Singh A, Schurman SH, Bektas A, et al. Aging and inflammation. Cold Spring Harb Perspect Med. 2024;14(6):a041197. doi:10.1101/cshperspect.a041197
4. Pasina L, Cortesi L, Tiraboschi M, et al. Risk factors for three-month mortality after discharge in a cohort of non-oncologic hospitalized elderly patients: results from the REPOSI study. Arch Gerontol Geriatr. 2018;74:169–173. doi:10.1016/j.archger.2017.10.016
5. Myles PR, Hubbard RB, Gibson JE, et al. Pneumonia mortality in a UK general practice population cohort. Eur J Public Health. 2009;19(5):521–526. doi:10.1093/eurpub/ckp081
6. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and Treatment of adults with community-acquired pneumonia. an official clinical practice guideline of the American Thoracic Society and Infectious Diseases Society of America. Am J Respir Crit Care Med. 2019;200(7):e45–e67. doi:10.1164/rccm.201908-1581ST
7. McGovern J, Grayston A, Coates D, et al. The relationship between the modified frailty index score (mFI-5), malnutrition, body composition, systemic inflammation and short-term clinical outcomes in patients undergoing surgery for colorectal cancer. BMC Geriatr. 2023;23(1):9. doi:10.1186/s12877-022-03703-2
8. Kahl A, du Bois A, Harter P, et al. Prognostic value of the age-adjusted Charlson comorbidity index (ACCI) on short- and long-term outcome in patients with advanced primary epithelial ovarian cancer. Ann Surg Oncol. 2017;24(12):3692–3699. doi:10.1245/s10434-017-6079-9
9. Scarborough JE, Bennett KM, Englum BR, et al. The impact of functional dependency on outcomes after complex general and vascular surgery. Ann Surg. 2015;261(3):432–437. doi:10.1097/SLA.0000000000000767
10. Magliozzi R, Pedrinolla A, Rossi S, et al. Chronic bedridden condition is reflected by substantial changes in plasma inflammatory profile. Biomolecules. 2022;12(12):1867. doi:10.3390/biom12121867
11. Warwick CA, Keyes AL, Woodruff TM, Usachev YM, et al. The complement cascade in the regulation of neuroinflammation, nociceptive sensitization, and pain. J Biol Chem. 2021;297(3):101085. doi:10.1016/j.jbc.2021.101085
12. Xiang Z, Wang H, Li H. Comorbidity risk and distribution characteristics of chronic diseases in the elderly population in China. BMC Public Health. 2024;24(1):360. doi:10.1186/s12889-024-17855-w
13. Jiao J, Yang XY, Li Z, et al. Incidence and related factors for hospital-acquired pneumonia among older bedridden patients in china: a hospital-based multicenter registry data based study. Front Public Health. 2019;(7):221. doi:10.3389/fpubh.2019.00221
14. Jiao J, Li Z, Wu XJ, et al. Risk factors for 3-month mortality in bedridden patients with hospital-acquired pneumonia: a multicenter prospective study. PLoS One. 2021;16(3):e0249198. doi:10.1371/journal.pone.0249198.
15. Mackey DC, Lui LY, Cawthon PM, et al. Life-space mobility and mortality in older women: prospective results from the study of osteoporotic fractures. J Am Geriatr Soc. 2016;64(11):2226–2234. doi:10.1111/jgs.14474
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Correlates of Frailty in Hospitalized Older Adults with Hypertension and Its Influence on Clinical Prognosis

Xu Y, Zhang S, Wang P, Chen Y, Mao Y, Yuan X, Li Y, Li M, Sheng L, Li X, Gao N
International Journal of General Medicine 2024, 17:3373-3385
Published Date: 2 August 2024