Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Local mild hypothermia therapy as an augmentation strategy for minimally invasive surgery of hypertensive intracerebral hemorrhage: a meta-analysis of randomized clinical trials
Authors Han Y, Sheng K, Su M, Yang N, Wan D
Received 29 September 2016
Accepted for publication 8 November 2016
Published 23 December 2016 Volume 2017:13 Pages 41—49
DOI https://doi.org/10.2147/NDT.S123501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wai Kwong Tang
Yu Han,1 Ke Sheng,1 Meilan Su,1 Nan Yang,1 Dong Wan2
1Department of Neurology, 2Department of Emergency, The First Affiliated Hospital of Chongqing Medical University, Chongqing, People’s Republic of China
Background: Previous studies reported that the mild hypothermia therapy (MHT) could significantly improve the clinical outcomes for patients with hypertensive intracerebral hemorrhage (HICH). Therefore, this meta-analysis was conducted to systematically assess whether the addition of local MHT (LMHT) could significantly improve the efficacy of minimally invasive surgery (MIS) in treating HICH.
Methods: Randomized clinical trials on the combined application of MIS and LMHT (MIS+LMHT) vs MIS alone for treating HICH were searched up to September 2016 in databases. Response rate and mortality rate were the primary outcomes, and the neurologic function and Barthel index were the secondary outcomes. Side effects were also analyzed.
Results: Totally, 28 studies composed of 2,325 patients were included to compare the efficacy of MIS+LMHT to MIS alone. The therapeutic effects of MIS+LMHT were significantly better than MIS alone. The pooled odds ratio of response rate and mortality rate was 2.68 (95% confidence interval [CI]=2.22–3.24) and 0.43 (95% CI=0.32–0.57), respectively. In addition, the MIS+LMHT led to a significantly better improvement in the neurologic function and activities of daily living. The incidence of pneumonia was similar between the two treatment methods.
Conclusion: These results indicated that compared to MIS alone, the MIS+LMHT could be more effective for the acute treatment of patients with HICH. This treatment modality should be further explored and optimized.
Keywords: LMHT, pneumonia, HICH, neurologic function, Barthel index
Introduction
Intracerebral hemorrhage (ICH) is a common cerebrovascular disease with a high mortality and poor outcomes in clinical practice, and also the leading cause of death and disability in elderly patients.1 It was reported to account for about 10% of all strokes and 30% of all cerebrovascular diseases.2,3 The mortality rate could be up to 50%, and the mortality rate in one month could be up to 40%.3,4 Moreover, there could be up to 40% of severely disabled survivors.3 Normally, the edema and hematoma expansion are the two major factors contributing to worsened outcomes and secondary damage.5
Many factors could lead to ICH, but hypertension is the major cause of ICH, and the hypertensive ICH (HICH) is a common neurological disease. To date, there are still no effective drug therapies for HICH.6 Moreover, HICH is characterized by high incidence, high mortality and high morbidity, which seriously endangers the health of patients and causes substantial economic burden for families and society. Therefore, it is urgently necessary to develop an effective therapy for this disease.
During the treatment, the key point is to quickly clear the hematoma and reduce the intracranial pressure.7 Along with minimally invasive technique, minimally invasive surgery (MIS) for HICH is gaining increasing attention. It could effectively decrease the mortality rate in the acute treatment of patients with HICH.8 Additionally, some previous studies reported that the mild hypothermia therapy (MHT) could be useful for neuroprotection and be used to treat cerebral edema after acute brain injury.9–11 Previous study reported that the addition of MHT could significantly improve the efficacy of MIS in treating HICH.12 Therefore, the aim of this study was to review the available published studies and conduct a meta-analysis to systematically assess whether the combined application of MIS and local MHT (LMHT) (MIS+LMHT) could result in a better efficacy than MIS alone.
Methods
Study selection
The first step of this meta-analysis was to obtain the eligible clinical trials. We conducted electronic searches in the following databases: Cochrane Controlled Trails Register, PubMed, Embase, Web of Science, Chinese Biomedical Literature Database on Disc and Chinese National Knowledge Infrastructure (dated up to September 2016). The search terms that we used were “hypothermia”, “minimally invasive” and “hypertensive cerebral hemorrhage”. No language restriction was set to avoid the potential language bias. Reference documents listed in the eligible studies and conference summaries were also reviewed. The inclusion criteria included the following items: 1) randomized clinical trials comparing the MIS+LMHT with MIS alone; 2) patients with hypertensive cerebral hemorrhage over 18 years of age; 3) the outcomes including at least one of these three indexes: response rate, mortality rate and neurologic function; and 4) patients could provide informed consent. The exclusion criteria included the following items: 1) no control group or not used MIS as the control group and 2) case reports, reviews and duplicate studies.
Outcome measures
Response rate and mortality rate were chosen as the primary outcomes. The response rate was defined according to the criteria of the included studies. The neurologic function, Barthel index and side effects were chosen as the secondary outcomes. The neurologic function was assessed according to the China Stroke Scale (CSS). The Barthel index was used to assess the activities of daily living (ADL) after treatment. Because pneumonia might be the main side effect caused by hypothermia,13 we only analyzed the incidence of pneumonia to assess the acceptability of these treatment methods.
Data extraction
In order to ensure the high accuracy of the extracted data, two authors (Yu Han and Ke Sheng) were arranged to independently screen the potential studies according to the aforementioned inclusion/exclusion criteria and extract the data. Any disagreement was resolved by discussion. The extracted data included the demographic data of the patients, the parameters of the MIS and LMHT, the first author and outcomes (primary and secondary outcomes). Good-faith efforts were made to obtain the data which were not available from the included studies.
Statistical analysis
RevMan 5.1 software was used to conduct the meta-analysis. For discontinuous data, the summary odds ratio (OR) was used as the effect size; for continuous data, the weighted mean difference (WMD) was used as the effect size. The chi-square test and I2 index were used to assess the heterogeneity.14 If the corresponding P-value was more than 0.10 and I2 was less than 50%, then the Mantel–Haenszel fixed-effects model was used; otherwise, the random-effects model was used. The potential presence of publication bias was assessed using funnel plot. This meta-analysis was conducted according to the recommendations.15
Results
Literature search
At first, we obtained 157 potentially relevant randomized clinical trials. Based on the inclusion and exclusion criteria, 129 studies were excluded. The reasons for exclusion included the following: 1) no randomization, 2) no control group, 3) compared the MIS+LMHT with the conservative treatment, 4) no available data, 5) did not use MIS and 6) being a retrospective study. Finally, 28 clinical trials composed of 2,325 adult patients with hypertensive cerebral hemorrhage were included in this meta-analysis.16–43 The matched demographic data were observed in the included studies (Table 1). More than half of the included studies used cooling blanket as the device of LMHT. The detailed information of treatment methods is provided in Table 2.
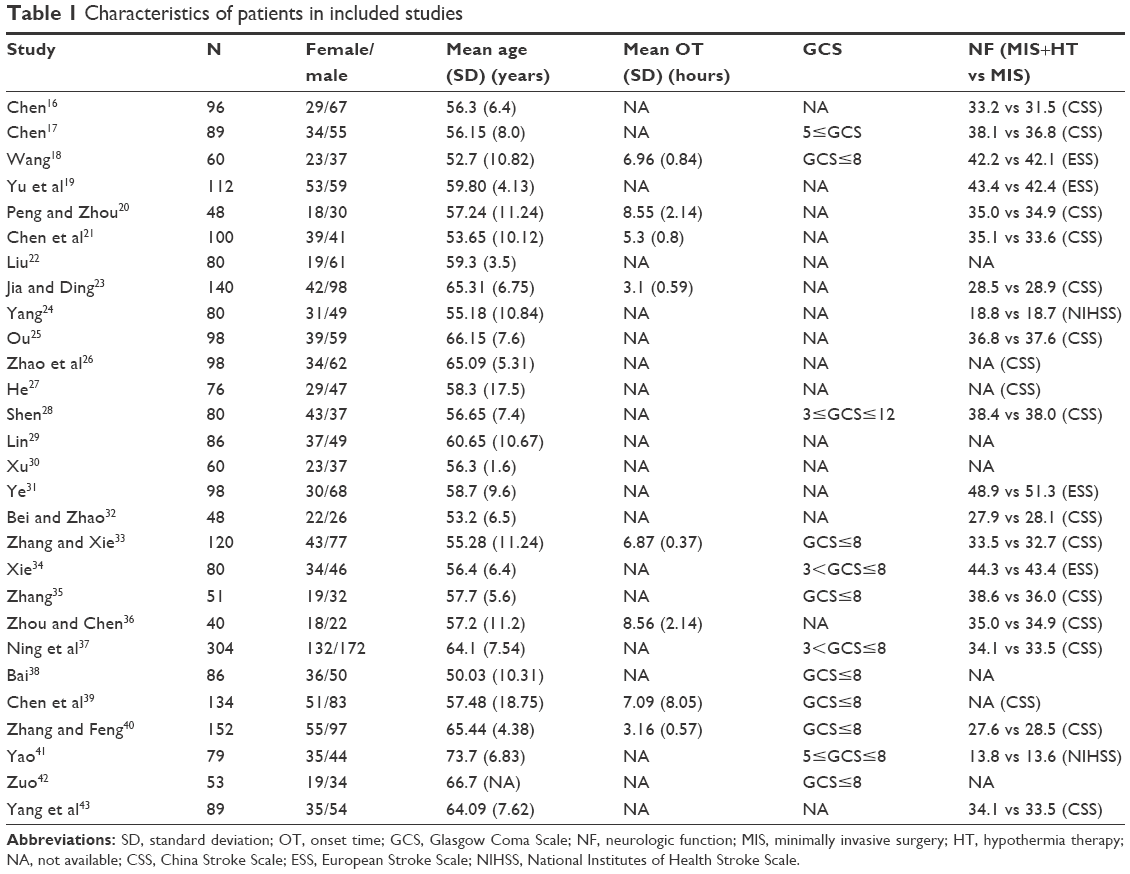 | Table 1 Characteristics of patients in included studies |
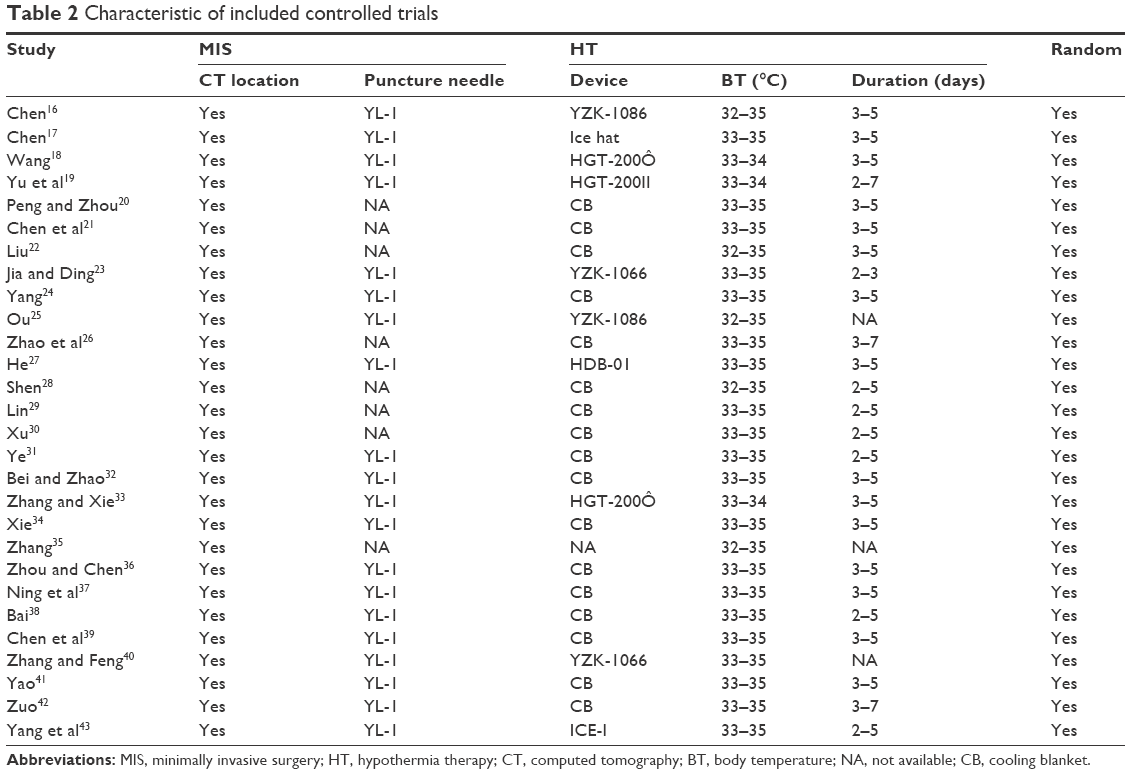 | Table 2 Characteristic of included controlled trials |
Response rates
Response rate was available for 23 trials (Figure 1). Overall, 916 of 1,156 (79.2%) patients receiving the MIS+LMHT and 673 of 1,129 (59.6%) patients receiving MIS alone were classified as responders. No heterogeneity (I2=0%, P=0.63) existed. Then, the fixed-effects model was used. The pooled OR was 2.68 with 95% confidence interval (CI)=2.22–3.24, which indicated that the MIS+LMHT could yield a higher response rate than MIS alone. The funnel plot showed that there was no publication bias (Figure 2).
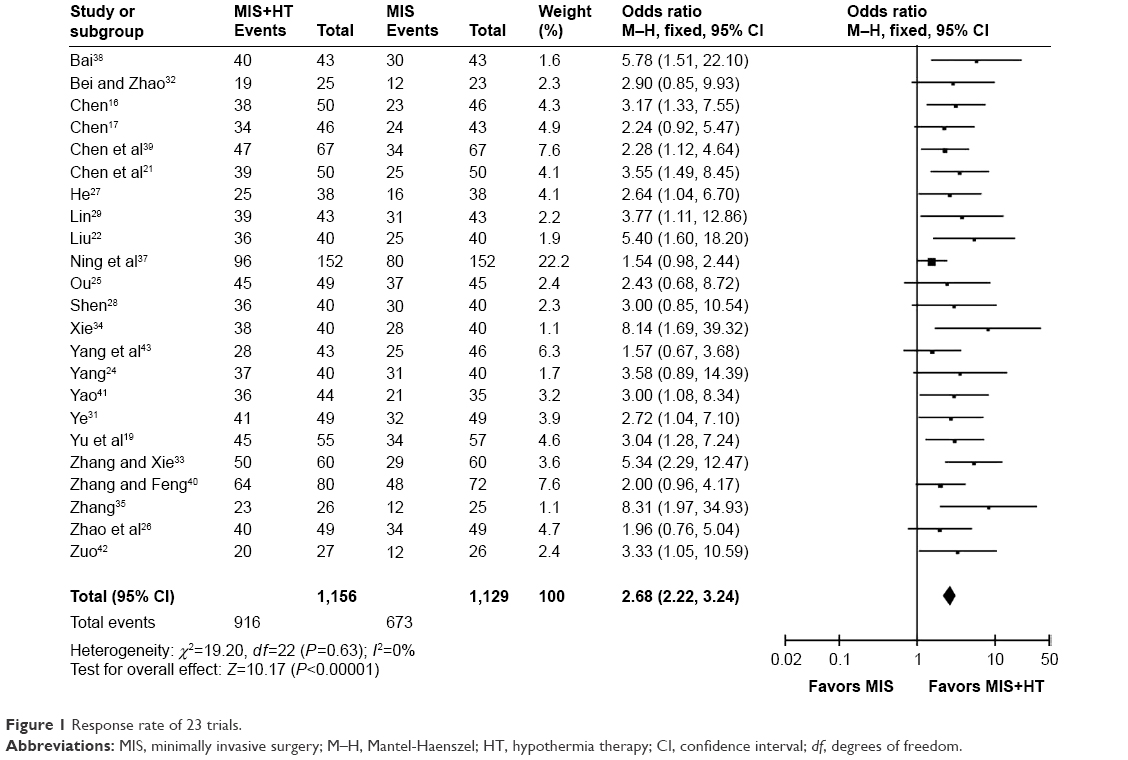 | Figure 1 Response rate of 23 trials. |
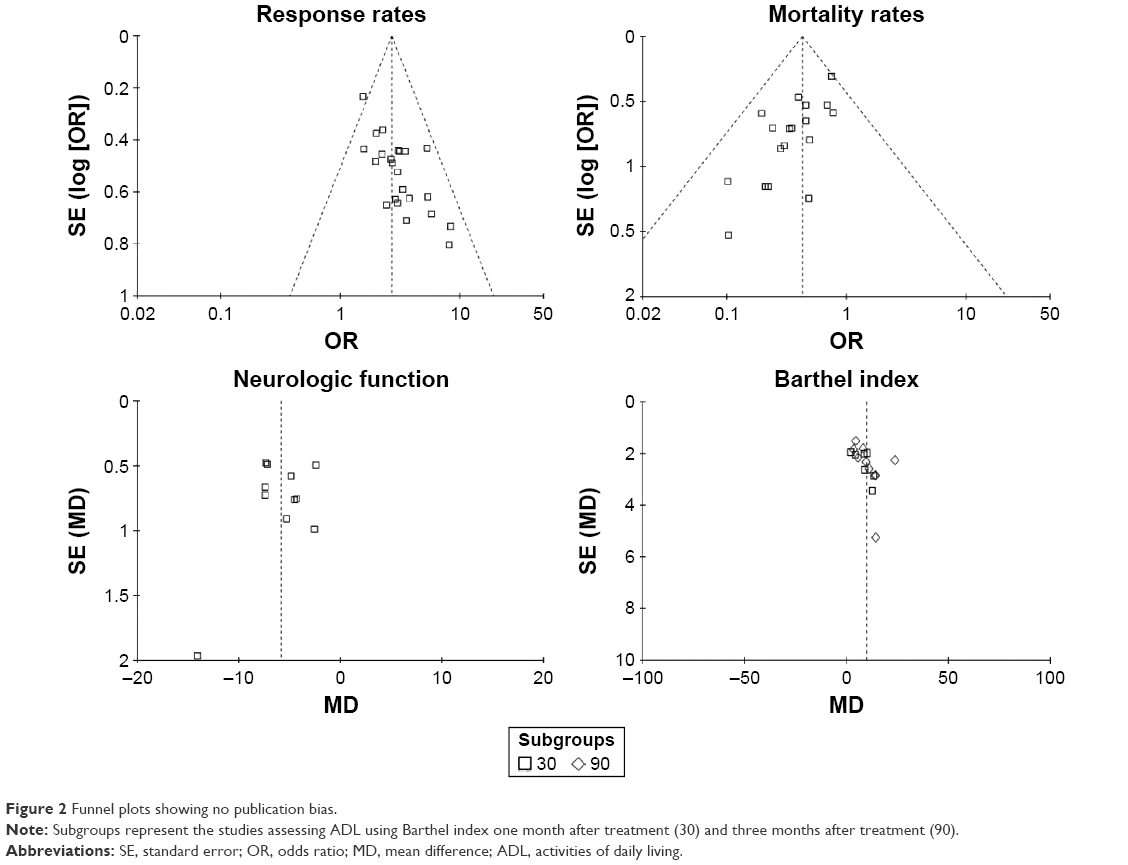 | Figure 2 Funnel plots showing no publication bias. |
Mortality rates
Mortality rate was available for 18 trials (Figure 3). Overall, 79 of 883 (8.9%) patients receiving the MIS+LMHT and 162 of 868 (18.7%) patients receiving MIS alone died after treatment. No heterogeneity (I2=0%, P=0.83) existed. Then, the fixed-effects model was used. The pooled OR was 0.43 with 95% CI=0.32–0.57, which indicated that the MIS+LMHT could yield a lower mortality rate than MIS alone. The funnel plot showed that there was no publication bias (Figure 2).
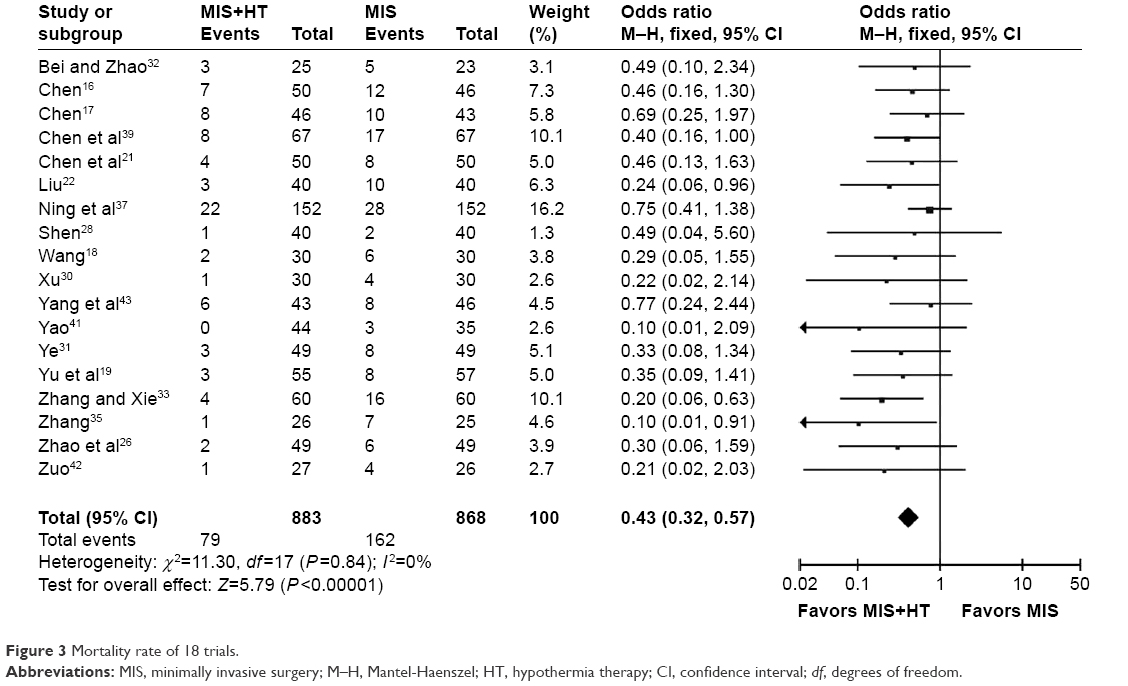 | Figure 3 Mortality rate of 18 trials. |
Neurologic function
Among the included studies, 11 studies used CSS to assess the neurologic function of patients (Figure 4). Eight of 11 studies assessed the neurologic function one month after treatment; two studies conducted the assessment 21 days later and one study 14 days later. Heterogeneity (I2=91%, P<0.0001) existed. Then, the random-effects model was used. The pooled WMD was −5.83 with 95% CI=−7.18 to −4.47, which indicated that the MIS+LMHT could be more effective than MIS alone in improving the neurologic function of patients. The funnel plot showed that there was no publication bias (Figure 2).
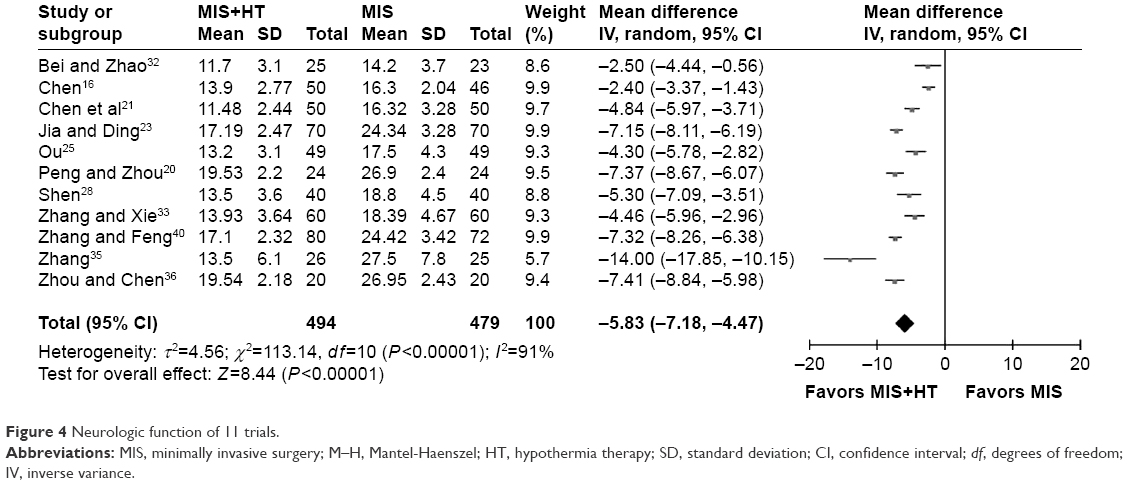 | Figure 4 Neurologic function of 11 trials. |
Barthel index
Seven studies assessed ADL using Barthel index one month after treatment (Figure 5A). Heterogeneity (I2=67%, P=0.006) existed. Then, the random-effects model was used. The pooled WMD was 8.17 with 95% CI=5.16–11.19. Ten studies assessed ADL three months after treatment (Figure 5B). Heterogeneity (I2=87%, P<0.00001) existed. Then, the random-effects model was used. The pooled WMD was 10.75 with 95% CI=6.77–14.73. No publication bias existed (Figure 2). These results indicated that the MIS+LMHT could be more effective than MIS alone in improving the ADL of patients.
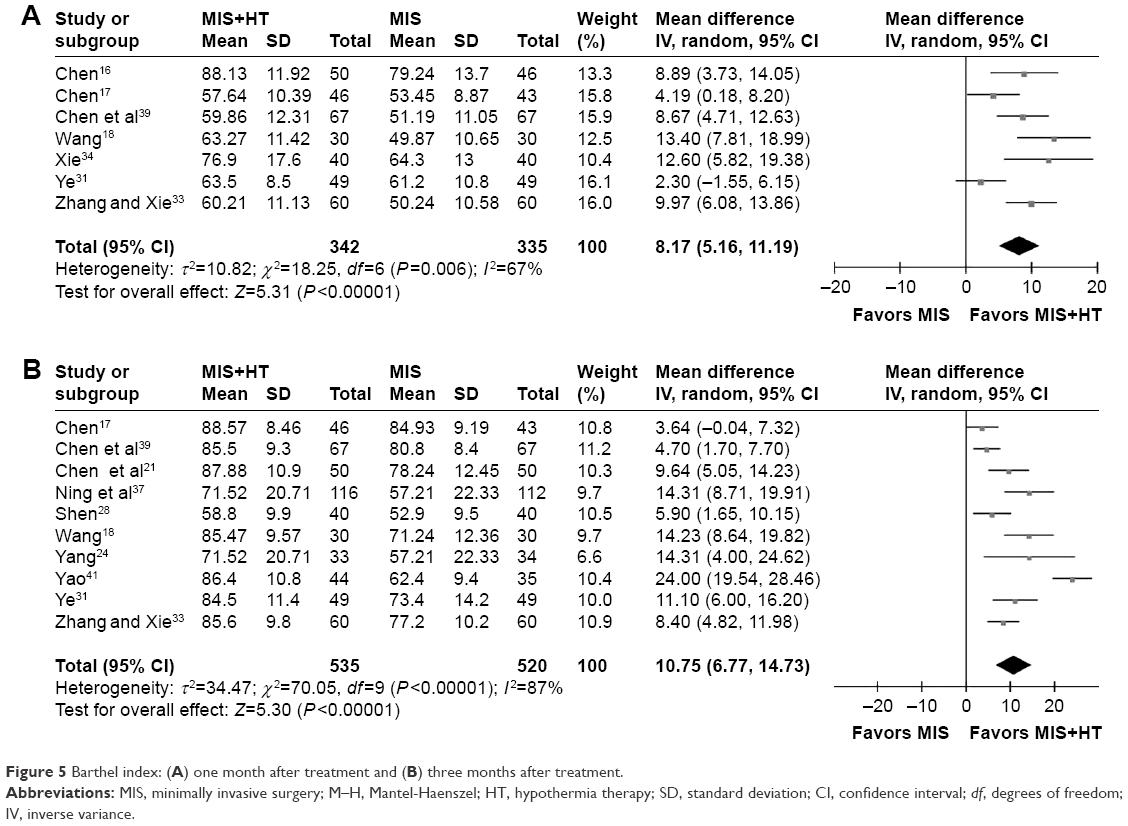 | Figure 5 Barthel index: (A) one month after treatment and (B) three months after treatment. |
Side effects
Only three studies assessed the side effects of the two treatment methods. Overall, 17 of 77 patients receiving the MIS+LMHT and 16 of 76 patients receiving the MIS alone experienced pneumonia. The pooled OR was 1.05 with 95% CI=0.43–2.59, which indicated that the incidence of pneumonia was similar between these two treatment methods.
Discussion
We conducted this meta-analysis of 28 randomized clinical trials to compare the efficacy of MIS+LMHT with MIS alone in the treatment of patients with HICH. The results showed that the MIS+LMHT could yield higher response rate (OR=2.68) and lower mortality rate (OR=0.43). Moreover, this treatment modality could significantly improve the neurologic function and ADL of patients. With respect to the analysis of side effects, only three studies reported the number of patients with pneumonia, which was insufficient to make a robust conclusion on the safety of the MIS+LMHT. However, these results demonstrated that the LMHT could be an effective augmentation strategy for MIS in treating patients with HICH.
In this study, almost all relevant randomized clinical trials were included, but some trials might have been missed, partly because these were published in some journals that are not indexed by international databases. Fortunately, it is likely that these trials are of low quality, and could not significantly affect the results.44 Additionally, there was one trial without the needed data,45 and despite our best efforts, we could not obtain them. However, this trial concluded that the MIS+LMHT could be good at protecting nerve cell and promoting neurofunctional rehabilitation. Therefore, this trial would not affect our conclusion.
Under conditions of mild hypothermia, the oxygen consumption and metabolic rate in brain tissue are decreased, the production of free radicals is reduced and the synthesis of xanthine oxidase is slowed down and then the tissue damage could be alleviated. Meanwhile, the abnormal sodium–calcium exchange between cell membrane and sarcoplasmic reticulum is suppressed, which could alleviate the calcium overload.46 Under normal conditions, vasoactive substances, such as endothelin and vascular vasopressin, are in dynamic equilibrium to maintain the systolic and diastolic function of blood vessels.47 The acute period of ICH is usually accompanied by the disorder of vasoactive substances. The substantial production of endothelin and vascular vasopressin could further aggravate cerebral ischemia. Previous studies reported that the mild hypothermia could reduce the level of endothelin and vascular vasopressin.40,48
Previous studies on ischemic and hemorrhagic stroke subtypes showed that the mild hypothermia (body temperature reduced by 3°C–5°C) was neuroprotective.49,50 But one point should be noticed in clinical practice: systemic mild hypothermia is difficult to perform because of its possible side effects.10,11 Alternatively, local mild hypothermia could quickly obtain the target temperature and overcome the potential side effects.51 Therefore, compared to systemic mild hypothermia, the local mild hypothermia could be more effective in treating patients with HICH.
Limitations
There were several limitations. First, all of the included studies were from the People’s Republic of China, which might limit the applicability of our findings.52 Second, only three studies were used to analyze the side effects; hence, future studies are needed to further assess the safety of the MIS+LMHT. Third, the target temperature and treatment time of LMHT were not consistent, but there were also the general problems for meta-studies to solve.53,54
Conclusion
By pooling analysis of 28 randomized clinical trials, we found that the addition of LMHT could significantly improve the efficacy of MIS in the treatment of patients with HICH. The OR of response rate and mortality rate was 2.68 and 0.43, respectively, which was in favor of the MIS+LMHT. The neurologic function and ADL were also found to be improved. The clinical applicability of this modality showed greater promise and should be further explored and optimized.
Acknowledgments
This work was supported by the medical research subjects from Health and Family Planning Commission of Chongqing (No 20142008) and State Key Clinical Specialties, Department of Neurology, First Affiliated Hospital of Chongqing Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
Juvela S, Kase CS. Advances in intracerebral hemorrhage management. Stroke. 2006;37(2):301–304. | ||
Kreitzer N, Adeoye O. An update on surgical and medical management strategies for intracerebral hemorrhage. Semin Neurol. 2013;33(5):462–467. | ||
Riggs JE, Libell DP, Brooks CE, Hobbs GR. Impact of institution of a stroke program upon referral bias at a rural academic medical center. J Rural Health. 2005;21(3):269–271. | ||
van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–176. | ||
Chen S, Zeng L, Hu Z. Progressing haemorrhagic stroke: categories, causes, mechanisms and managements. J Neurol. 2014;261(11):2061–2078. | ||
Wei S, Sun J, Li J, et al. Acute and delayed protective effects of pharmacologically induced hypothermia in an intracerebral hemorrhage stroke model of mice. Neuroscience. 2013;252:489–500. | ||
Stone JR, Singleton RH, Povlishock JT. Intra-axonal neurofilament compaction does not evoke local axonal swelling in all traumatically injured axons. Exp Neurol. 2001;172(2):320–331. | ||
Broderick J, Connolly S, Feldmann E, et al; American Heart Association; American Stroke Association Stroke Council; High Blood Pressure Research Council; Quality of Care and Outcomes in Research Interdisciplinary Working Group. Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38(6):2001–2023. | ||
Rincon F, Friedman DP, Bell R, Mayer SA, Bray PF. Targeted temperature management after intracerebral hemorrhage (TTM-ICH): methodology of a prospective randomized clinical trial. Int J Stroke. 2014;9(5):646–651. | ||
Staykov D, Wagner I, Volbers B, Doerfler A, Schwab S, Kollmar R. Mild prolonged hypothermia for large intracerebral hemorrhage. Neurocrit Care. 2013;18(2):178–183. | ||
Schwab S, Schwarz S, Spranger M, et al. Moderate hypothermia in the treatment of patients with severe middle cerebral artery infarction. Stroke. 1998;29(12):2461–2466. | ||
Tan YW, Tang BW, Li XJ. Clinical study of minimally invasive aspiration with mild hypothermia in the treatment of hypertensive cerebral hemorrhage. China J Mod Med. 2008;19:49. | ||
Kollmar R, Staykov D, Dörfler A, Schellinger PD, Schwab S, Bardutzky J. Hypothermia reduces perihemorrhagic edema after intracerebral hemorrhage. Stroke. 2010;41(8):1684–1689. | ||
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. | ||
Sacks HS, Berrier J, Reitman D, Ancona-Berk VA, Chalmers TC. Meta-analyses of randomized controlled trials. N Engl J Med. 1987;316(8):450–455. | ||
Chen J. [Efficacy of minimally invasive surgery plus hypothermia treatment for hypertensive intracerebral hemorrhage]. J Minim Invasive Med. 2010;5(5):483–486. Chinese. | ||
Chen G. [Clinical observation of minimally invasive intracranial hematoma plus local mild hypothermia therapy for hypertensive intracerebral hemorrhage]. Med J Natl Defend Forces North China. 2010;22(6):548–550. Chinese. | ||
Wang W. [Combined application of minimally invasive surgery and mild hypothermia therapy for hypertensive intracerebral hemorrhage]. Chin J Pract Nerv Dis. 2015;18(5):96–97. Chinese. | ||
Yu QJ, Gao JL, Jiang J, Wang KJ, He F, Xue YH. [Clinical efficacy observation of minimally invasive surgery and mild hypothermia therapy for hypertensive intracerebral hemorrhage]. J Apoplexy Nerv Dis. 2010;27(3):266–267. Chinese. | ||
Peng W, Zhou P. [Combined application of minimally invasive surgery and mild hypothermia therapy for 24 patients with hypertensive intracerebral hemorrhage]. Chin J Ethnomed Ethnopharm. 2014; 23:107. Chinese. | ||
Chen WX, Li XQ, He ZP, Liu XH. [Clinical efficacy observation of minimally invasive surgery and hypothermia therapy for hypertensive intracerebral hemorrhage]. Contemp Med. 2014;20(32):51–52. Chinese. | ||
Liu R. [Efficacy analysis of minimally invasive surgery plus hypothermia therapy for hypertensive intracerebral hemorrhage]. China Foreign Med Treat. 2012;35:55–56. Chinese. | ||
Jia JF, Ding L. [Effect of minimally invasive surgery plus hypothermia therapy on the neurologic function and vasoactive substances of patients with hypertensive intracerebral hemorrhage]. Chin J Pract Nerv Dis. 2015;18(13):85–87. Chinese. | ||
Yang C. [Clinical analysis of minimally invasive surgery combined with mild hypothermia treatment for hypertensive intracerebral hemorrhage]. J Qiqihar Univ Med. 2015;36(12):1782–1783. Chinese. | ||
Ou ML. [Combined application of minimally invasive surgery and mild hypothermia therapy for 98 elderly patients with hypertensive intracerebral hemorrhage]. China Elderly Med. 2011;31:861–862. Chinese. | ||
Zhao JC, Liu XH, Su YQ, Wang XM, Yang HT. [Mini-invasive evacuation of hematoma and mild hypothermia therapy for hypertensive intracerebral hemorrhage]. Guide China Med. 2013;11(25):90–91. Chinese. | ||
He YY. [Study of minimally invasive surgery plus hypothermia therapy for hypertensive intracerebral hemorrhage]. China J Ctrl Endem Dis. 2014;29(1):141–142. Chinese. | ||
Shen XZ. [Efficacy assessment of the combined application of minimally invasive surgery and hypothermia therapy for hypertensive intracerebral hemorrhage]. China Pract Med. 2015;10(19):72–73. Chinese. | ||
Lin JJ. [Efficacy of minimally invasive surgery plus hypothermia therapy for hypertensive intracerebral hemorrhage and its effect on serum inflammatory factors]. Mod Pract Med. 2016;28(4):456–457. Chinese. | ||
Xu HB. [Effect of the combined application of minimally invasive surgery and hypothermia therapy on serum inflammatory factors and prognosis for patients with hypertensive intracerebral hemorrhage]. Chin J Pract Nerv Dis. 2015;18(21):87–88. Chinese. | ||
Ye Q. [Effect of the combined application of minimally invasive surgery and hypothermia therapy on nervous function and activities of daily living]. Chin Prim Health Care. 2011;25(10):108–109. Chinese. | ||
Bei WW, Zhao SJ. [Combined application of minimally invasive surgery and hypothermia therapy for patients with hypertensive intracerebral hemorrhage]. Guangxi Med J. 2010;32(10):1193–1194. Chinese. | ||
Zhang J, Xie RL. [Clinical study of minimally invasive surgery and Gaja hypothermia in the treatment of hypertensive cerebral hemorrhage]. Chin J Gen Pract. 2014;12(2):225–227. Chinese. | ||
Xie DM. [Curative effect observation of intracranial hematoma minimally invasive hypothermia in the treatment of hypertensive cerebral hemorrhage].Chin Community Doctors. 2014;30(18):22–23. Chinese. | ||
Zhang H. [The clinical efficacy research of micro-invasive evacuation of intracranial hematoma combined with mild hypothermia therapy in hypertensive cerebral hemorrhage patients]. Chin J Pract Nerv Dis. 2016;19(9):19–21. Chinese. | ||
Zhou LS, Chen GR. Observation of minimally invasive removal of intracranial hematoma combined with mild hypothermia for hypertensive intracerebral hemorrhage. Jilin Med J. 2014;35(11): 2276–2278. | ||
Ning HH, Li D, Li T, Li X, Zhao Q. [Combined application of minimally invasive surgery and mild hypothermia therapy for 152 patients with hypertensive intracerebral hemorrhage]. China Foreign Med Treat. 2011;24:16–17. Chinese. | ||
Bai JM. Clinical efficacy of minimally invasive removal of intracranial hematoma combined with mild hypothermia in the treatment of severe hypertensive cerebral hemorrhage. China Contin Med Educ. 2016;8(14):112–113. | ||
Chen JY, Chen J, Zhou K. [Clinical analysis of intracranial hematoma minimally invasive removal combined with mild hypothermia therapy to treat severe hypertensive cerebral hemorrhage]. Asia Pac J Tradit Med. 2012;8(12):131–132. Chinese. | ||
Zhang L, Feng YJ. [Impact of minimally invasive intracranial hematoma elimination combined with mild hypothermia on vasoactive substances and neurological function in patients with hypertensive intracerebral hemorrhage]. Chin J Hypertens. 2015;23(2):436–438. Chinese. | ||
Yao HW. [Observation of curative effect of the minimally invasive removal of intracranial hematoma combined with mild hypothermia treatment for patients with hypertensive cerebral hemorrhage in the elderly]. Chin J Pract Nerv Dis. 2014;17(15):24–26. Chinese. | ||
Zuo J. The clinical nursing of patients of elderly hypertensive cerebral hemorrhage receiving minimally invasive hematoma surgery and mild hypothermia therapy. J Shandong Med Coll. 2009;31(5):330–332. | ||
Yang M, Zhang QS, Gui W. [Clinical analysing on treatment of brain hemorrhage with the minimal access surgery combined mild hypothermia therapy]. HeBei Med. 2009;8:889–891. Chinese. | ||
Deeks JJ, Altman DG, Bradburn MJ. Statistical methods for examining heterogeneity and combining results from several studies in meta-analysis. In: Egger M, Davey Smith G, Altman DG, editors. Systematic Reviews in Health Care: Meta-Analysis in Context. 2nd ed. London: BMJ Publication Group; 2008:285–312. | ||
Wen SK, Yang S, Li Y. Comparison of effect of local mild hypothermia therapy and continuous perfusion of hypothermic liquids therapy on the treatment of hypertension-induced cerebral hemorrhage after micro-invasives evaluatich hematoma. China Pract Med. 2011;6(14):1–4. | ||
Dai M, Freeman B, Bruno FP, et al. The novel ETA receptor antagonist HJP-272 prevents cerebral microvascular hemorrhage in cerebral malaria and synergistically improves survival in combination with an artemisinin derivative. Life Sci. 2012;91(13–14):687–692. | ||
Zweifel C, Katan M, Schuetz P, et al. Growth hormone and outcome in patients with intracerebral hemorrhage: a pilot study. Biomarkers. 2011;16(6):511–516. | ||
Jovanovic V, Pekic S, Stojanovic M, et al. Neuroendocrine dysfunction in patients recovering from subarachnoid hemorrhage. Hormones (Athens). 2010;9(3):235–244. | ||
Fingas M, Penner M, Silasi G, Colbourne F. Treatment of intracerebral hemorrhage in rats with 12 h, 3 days and 6 days of selective brain hypothermia. Exp Neurol. 2009;219(1):156–162. | ||
Theodorsson A, Holm L, Theodorsson E. Hypothermia-induced increase in galanin concentrations and ischemic neuroprotection in the rat brain. Neuropeptides. 2008;42(1):79–87. | ||
Bi M, Ma Q, Zhang S, et al. Local mild hypothermia with thrombolysis for acute ischemic stroke within a 6-h window. Clin Neurol Neurosurg. 2011;113(9):768–773. | ||
Chen JJ, Zhou CJ, Liu Z, et al. Divergent urinary metabolic phenotypes between major depressive disorder and bipolar disorder identified by a combined GC-MS and NMR spectroscopic metabonomic approach. J Proteome Res. 2015;14(8):3382–3389. | ||
Chen J, Zhao L, Liu Y, Fan S, Xie P. Comparative efficacy and acceptability of electroconvulsive therapy versus repetitive transcranial magnetic stimulation for major depression: A systematic review and multiple-treatments meta-analysis. Behav Brain Res. 2016;320:30–36. | ||
Chen J, Liu Z, Zhu D, et al. Bilateral vs unilateral repetitive transcranial magnetic stimulation in treating major depression: a meta-analysis of randomized controlled trials. Psychiatry Res. 2014;219(1):51–57. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.