Back to Journals » Research and Reports in Tropical Medicine » Volume 13
Liver Enzymes and Lipid Profile of Malaria Patients Before and After Antimalarial Drug Treatment at Dembia Primary Hospital and Teda Health Center, Northwest, Ethiopia
Authors Megabiaw F ![]() , Eshetu T
, Eshetu T ![]() , Kassahun Z, Aemero M
, Kassahun Z, Aemero M ![]()
Received 2 December 2021
Accepted for publication 19 March 2022
Published 28 March 2022 Volume 2022:13 Pages 11—23
DOI https://doi.org/10.2147/RRTM.S351268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mario Rodríguez-Pérez
Fentahun Megabiaw,1 Tegegne Eshetu,1 Zeleke Kassahun,2 Mulugeta Aemero1
1Department of Medical Parasitology, School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2College of Medicine and Health Sciences Comprehensive & Specialized Hospital, University of Gondar, Gondar, Ethiopia
Correspondence: Mulugeta Aemero, Email [email protected]; [email protected]
Background: Infection with malaria in humans involves liver cell destruction, which alters the levels of liver enzymes and lipid profiles. A number of studies have been conducted to address the impact of malaria on liver enzymes and lipid profiles but no studies were addressed after antimalarial treatment in Ethiopia. This study is intended to fill this gap.
Methods: An observational cohort study was conducted at Dembia Primary Hospital and Teda Health Center, from June to August 2020. Eighty eight malaria infected study participants were recruited using random sampling techniques. Socio-demographic data, capillary and venous blood samples were collected. Assessment of liver enzymes and lipid profiles was done using Beckman Coulter DC-700 clinical chemistry analyzer. Data were entered using Epi-data and exported to SPSS version 20 for analysis. One way ANOVA, independent t-test, and paired t-test were used to compare the mean liver enzymes and lipid profile. p-value< 0.05 was considered statistically significant.
Results: Before anti-malaria treatment, among 88 study participants, elevated AST (87.5%), ALT (12.5%), ALP (43.2%), and TG (17.2%) and lower HDL (87.5%) and normal LDL and TC were observed. After treatment, 100% AST, ALT, HDL, and LDL and 92% ALP, 94.3% TC, and 86.4% TG levels were in the normal range. The mean level of AST and ALT increased while HDL decreased from low to higher density parasitaemia. Mean level of AST was significantly lower while ALT did not alter. HDL, LDL, and TC level were increased but statistically were insignificant (P> 0.05).
Conclusion: Malaria could be responsible for increased liver enzymes and certain lipids while decreasing some lipid profiles. After anti-malaria treatment, these parameters were reversed to normal from 86.4% to 100%. Hence, prompt treatment is important to improve liver enzymes and lipid profile impairment during malaria infection.
Keywords: malaria, anti-malaria drug, liver enzymes, lipid profiles, Ethiopia
Introduction
Malaria is a vector-borne infectious disease caused by an intracellular protozoan parasite of the genus Plasmodium that infects multiple hosts such as humans and other mammalians.1 Commonly four main Plasmodium species: Plasmodium falciparum, Plasmodium ovale, Plasmodium malariae and Plasmodium vivax have long been known to cause malaria in humans. Nowadays Plasmodium Knowlesi, previously confined to monkeys, is the fifth species that infect humans.2 However, P. falciparum and P. vivax are responsible for the majority of malaria cases and P. falciparum is mainly associated with deaths. Plasmodium is primarily transmitted by the bite of an infected female Anopheles mosquito. Infection can also occur through exposure to infected blood products and through congenital transmission.3
Malaria continuous to have a major health problem worldwide.4 Globally, there were an estimated 229 million malaria cases in 2019 in 87 malaria endemic countries, declining from 238 million in 2000. The World Health Organization (WHO) African Region, with an estimated 215 million cases in 2019, accounted for about 94% of cases.5 Malaria is one of the leading public health problems in Ethiopia. The problem covers 75% of the landmass of the country and 68% of the populations are living in malaria-risk areas.6 Plasmodium falciparum and P. vivax are the two dominant parasite species causing human malaria in Ethiopia, on average, with relative frequencies of about 62.8% and 37.2%, respectively.7 In Ethiopia, malaria transmission is largely determined by altitude and climate. Most of the malaria transmission occurs between September and December, after the main rainy season June to August.8
Though malaria parasite can affect many organs, liver is the major organ which is affected.9 The liver is one of the vital organs of the body and it plays a great role in the proper function of the body. It is involved in the uptake, metabolism, phagocytosis and clearance of microorganisms and endotoxins from the portal blood.10 The liver functions to recognize and generate effective immunoreactivity against pathogens on the one hand, and to generate tolerance to avoid immunoreactivity with “self” and harmless substances as dietary compounds on the other hand.11 During malaria infection, liver plays a protective role against blood stages of malaria. It is more critical than the spleen for mediating suppressive effects of testosterone on resistance to malaria which results difference among males and females in terms of malaria severity.12
The malaria parasite induces certain metabolic and biochemical changes within the host.13 In the liver stage, sporozoites invade the hepatocytes which can cause organ congestion, sinusoidal blockage, and cellular inflammation. These changes in hepatocytes can lead to the leakage of parenchyma and membrane enzymes into the general circulation.3
Liver dysfunction has long been recognized as a clinical feature of malaria.14 Liver failure is one of the major cause of morbidity and mortality.15 Malaria-induced hepatocyte injury may manifest significant elevated serum level enzymes of aspartate transaminase (AST), alanine transaminase (ALT), and alkaline phosphatase (ALP).16 The pathogenesis of hepatic dysfunction is not completely known; however, reduction in portal venous flow as a consequence of micro occlusion of portal venous branches by parasitized erythrocytes, intrahepatic cholestasis due to reticuloendothelial blockage and hepatic microvilli dysfunction, suppression of bilirubin excretion due to effect of parasitaemia or endotoxemia or metabolic acidosis, apoptosis and oxidative stress are all mechanisms involved in hepatic damage.17
Malaria parasites exhibit dyslipidemia due to the parasites use of cholesterol and phospholipids from its host for the increase in surface area and volume of its internal membranes.18 Lipid together with its apoprotein, called lipoprotein, is needed to deliver lipids to and from body tissues to produce energy. Lipoproteins such as chylomicrons, very-low-density lipoproteins (VLDL), low-density lipoproteins (LDL), high-density lipoproteins (HDL), and free fatty acids (FFA) are major lipid components in plasma. Most plasma apolipoproteins, endogenous lipids, and lipoproteins have their origin from the liver. Under normal physiological conditions, the liver ensures homeostasis of lipid and lipoprotein metabolism. Hepatocellular damage is often associated with severe and acute Plasmodium malaria infection that impairs homeostasis leading to alterations in plasma lipid and lipoprotein patterns.13,19,20
Abnormalities in serum lipid profiles play a central role in endothelial functional abnormality which is a major risk factor for atherosclerosis including coronary artery disease, cerebrovascular disease and peripheral vascular diseases.21,22 The extent of serum lipid profile changes during malaria infection and their exact underlying biological mechanisms remain unclear.23 The changes that occur during inflammation and infection are part of the innate immune response and therefore are likely to play an important role in protecting the host. Lipids play a crucial role in the metabolism of Plasmodium life cycle in the human host. These organisms use cholesterol and phospholipids from the host for their metabolic requirements, such as membrane or hemozoin formation. Additionally, the parasite likely modifies metabolic pathways of lipids in the hepatocytes. Moreover, oxidative stress has been associated with the oxidation of lipoproteins, contributing to the abnormalities of lipids level.17,24 Hyperlipidemia of malarial infection may result in depletion of natural antioxidants and facilitates the production of reactive oxygen species which can react with all biological molecules like lipids. Thus increased reactive oxygen species and impaired antioxidant defense contributes to the initiation and progression of micro and macro vascular complications in malaria infection.25 Targeting lipid metabolism has been considered attractive for rational antimalarial chemotherapeutic drug design and development.26
The administration of the right drug against the malaria parasite species to control morbidity and mortality is a very important demand.27,28 Though the list of anti-malarial drugs is long, the most widely known are quinine, chloroquine (CQ), primaquine, and artemisinin and its derivatives. Due to the widespread resistance to monotherapies, the World Health Organization (WHO) recommended the use of Artemisinin-based combination therapies (ACTs) for the treatment of uncomplicated falciparum malaria throughout malaria-endemic areas. Artemether-Lumefantrine (Art-L) having trade names Coartem®, is one of the ACTs. Primaquine is known for its activity against the gametocytes of P. falciparum and hypnozoites of P. vivax or P. ovale.27,29
Drug-induced liver injury remains largely underestimated.30 Following administration of the selected antimalarial drug, the liver enzymes and lipid profiles have a crucial role in giving information about the disease diagnosis, drug interactions assessment, and prognosis.26,31 In this regard, more recently a number of studies have been conducted to address the impact of malaria on liver enzymes; however, their findings have been unclear due to lack of consistency. Moreover, studies conducted so far were not designed to address the impact of antimalarials on liver enzymes and lipid profiles beyond the impact of malaria itself on liver enzymes and lipid profiles in Ethiopia. Considering this gap, this study is aimed to assess liver enzymes and lipid profiles before and after treatment of malaria-infected patients.
Methods
Study Area
The study was conducted at Dembia primary hospital and Teda health center, which are located within the Amhara regional state, central Gondar, Northwest Ethiopia. Dembia primary hospital is found in Dembia district. It is located 729 km north of Addis Ababa at 12°18′30″N and 37°17′30″E. The district has an area of 148,968 sq. km and divided into west and east Dembia woreda. The altitude of the district ranges from 1850 to 2000 m above sea level. The district receives an annual rainfall of 700 to 1160 mm on average. During the last 15 years, the annual mean maximum temperature was 29.6 °C and the minimum mean temperature was 13.2 °C in the District.32 Teda Health Center is found 24km away from Gondar town. Teda town has an average altitude of 1800–2600 meters above sea level, and the mean rainfall is 771–1160 mm. Malaria is the most prevalent seasonal disease in both areas. From October to December is the peak malaria transmission season in the area. Both P. vivax and P. falciparum exist in the area with P. falciparum prevailing all year.33
Study Design and Period
A prospective observational cohort study was conducted from June to August 2020.
Population
Source population
- All clinical malaria suspected participants who are attending Dembia Primary Hospital and Teda health center laboratory during the study period.
Study Population
All individuals who are positive for malaria and satisfy inclusion criteria that are attending Dembia Primary hospital and Teda health center laboratory during the study period were study population.
Inclusion and Exclusion Criteria
Inclusion Criteria
All malarial patients with microscopically confirmed P. falciparum, P. vivax or mixed (both falciparum and P. vivax) infection and both sexes who reside 5-10 km radius in the study area were included in this study.
Exclusion Criteria
Pregnant women, patients with chronic alcoholism, participants having a history of chronic diseases like liver, hepatitis, hypertensive, diabetes mellitus, cardiac disease, renal failure, and other parasitic diseases were excluded in this study. Besides, participants who had been under anti-retroviral therapy, who are positive for HBsAg and HCV at the time of screening were also excluded from this study.
Sample Size Determination
The desired sample size was calculated using the revised 2009WHO protocol. According to the protocol, the sample size calculation assumes the desired precision of 5% and a 95% confidence interval with a minimum of 73 patients. Moreover, considering a potential loss to follow-up,20% as a non-response rate was added. Finally, a minimum of 88 participants sample size was determined.34
N = (z/d) 2 P (1-P)
= (1.96/0.05)2 0.05 (1–0.05)
= 73
Where, N = number of samples, P = the expected population proportion of clinical failure (5%),
z = confidence interval (95%) and d = precision (5%)
Sampling Technique
A random sampling technique was employed to recruit the study participants at Dembia primary hospital and Teda health centers outpatient department (OPD).
Baseline Data Collection and Laboratory methods
Questionnaire
Before study initiation, a standardized questionnaire was developed which was specifically designed to collect socio-demographic characteristics and other previous clinical data of the participant. All relevant personal data were collected using a standard questionnaire after malaria susceptible individuals were confirmed for Plasmodium infections. Socio-demographic (age, gender, and residence, educational and marital status) characteristics and other relevant information were collected via a face-to-face interview technique at Dembia primary hospital and Teda health center OPD by trained data collectors. Following identifying individuals who were parasitologically confirmed for malaria, then the volunteer study participants were linked to laboratory personnel for blood sample collection.
Blood Sample Collection and Processing
After getting informed consent and ascent from the study participants, the blood sample was collected following standard operating procedures (SOPs) by trained laboratory personnel in the first visit on day 0 and the follow-up visiting day on day 14. Capillary blood samples from a finger prick was collected aseptically from each study participant to prepare both thick and thin blood film using pre-labeled microscope slides for detection and identification of Plasmodium species. The prepared blood films were stained using 10% Giemsa solution for 10 minutes and allowed to air dry by putting it horizontally in a slide tray at room temperature. After the stained slides were air-dried both the thick and thin blood film was examined using a high magnification power objective (100X) of the microscope. Thick blood film was used as a screening and quantification of parasitaemia and thin blood film was used primarily for parasite species identification. To determine the density of malaria parasitaemia, two experienced microscopists independently count as Low (+1/1 to 999 /μL), Moderate (+2/1000 to 9999 /μL) and severe or higher (≥+3/10,000 /μL) and the asexual stage of Plasmodium parasite on a slide against 200 WBCs in thick blood film from each of the malaria cases. Then, the results of the two readers were averaged and used for the calculation of parasite density. Finally, the result was expressed by parasites per μL blood. It was calculated by using the formula: Parasite/µL =Parasite counted/200WBC×Total WBC count.35,36
Using an aseptic vein puncture blood sample collection technique, 5 mL of blood sample on day 0 prior to treatment and on days 14 after treatment was collected with a sterile disposable syringe. Then it was delivered into a serum separator test tube for liver enzymes and lipid profile test and kept for1,2 minutes for clotting. Once the blood samples become clot it was centrifuged at 3000rpm for 5 minutes. All participants who were confirmed with Plasmodium infection were tested for hepatitis B surface antigen (HBsAg), hepatitis C (HCV), and intestine parasitic infection to confirm their eligibility. After the study participants were screened for HBsAg and HCV, serum was separated and stored in plain plastic tubes at −20°C until processed. Each participant was reminded to take their drug at home appropriately and instructed to return back 14 days of post-treatment by giving an appointment card for each participant. Fourteen days of post antimalarial drug administration, all relevant parasitological responses were re-assessed. Moreover, participants who were absent during the follow-up data collection period were considered as loss of follow-up. To assess the impact of malaria on the liver, marker enzymes and lipid profiles were evaluated according to International Federation of Clinical Chemistry (IFCC) methods. These biochemical tests were analyzed on separated serum using standard assay kits by using Beckman Coulter DxC-700 chemistry analyzer. All serum parameters were determined using this chemistry analyzer. The Para-Nitrophenyl phosphate method was used for the determination of serum ALP concentration. Besides, serum ALT concentration was determined by the pyruvate method while AST concentration was measured using the oxaloacetate method. Serum HDL, total cholesterol, LDL, and triglycerides were measured by the enzymatic assay method.37–39 The interpretation of test results was based on the manufacturers manual for each analysis to be measured. The enzymes and lipid profiles were done at the University of Gondar compressive specialized hospital laboratory.
Quality Control
To assure consistency and easy understanding, the questionnaire was prepared in English and translated to the Amharic language. The questionnaire was pre-tested for its accuracy and consistency prior to actual data collection. Socio-demographic and clinical data were collected by trained professionals under the supervision of the investigator. Blood sample quality was insured by collecting and processing according to the SOP. Samples were checked whether they are in the acceptable criteria like: no hemolysis, sufficient volume, and correct labeling. The quality control of liver enzymes and lipid profile tests was assessed using clinical chemistry laboratory manuals and standard operating procedures (SOPs) of the University of Gondar hospital laboratory.
Data Management and Analysis
Data was checked for completeness and consistency. After cleaning and coding, the data was entered into Epi-data software and exported into SPSS version 20 software for statistical analyses. The Shapiro–Wilks and the Kolmogorov–Smirnov normality test was conducted to check the distributions of the variables, and it showed the data were normally distributed in both pre- and post-assessment with (p>0.05). Mean, standard deviation, and frequency of quantitative variables were calculated. One way-ANOVA followed by turkey multivariable posthoc test was used to compare the mean liver enzymes and lipid profiles parameters among groups. Independent t-test was used to compare the mean of liver enzymes and lipid profiles parameters between males and females, and paired t-test was applied to compare means of cases pre and post antimalarial treatment. p-value less than 0.05 was considered as statistically significant.
Results
Characteristics of the Study Participants
A total of 1247 clinically malaria suspected individuals visiting Dembia primary hospital and Teda health center were screened for malaria during the study period. Of these, 529 (42.4%) had confirmed malaria positive by microscopic method. Among 529 malaria-infected patients, 430 were excluded since they did not fulfill the inclusion criteria and 99 were eligible for the study. Those who were out of the catchment area, who had taken drugs for chronic disease, pregnant mothers and those who refused to give consent or assent were excluded. Among the 99 who started to participate in the study 11 were lost during the follow-up. Thus, the study participants that successfully completed the 14-day follow-up study were 88 (fifty-one were from Teda health center and thirty-seven were from Dembia primary hospital). Of this 64.8% (57/88) were males and 35.2% (31/88) were females. The mean age of study participants was 26.11±11.044 years (ranges 6–65 years). The age group more affected was 25–34 years (31.8%) followed by 16–24 years (30.7) (Table 1).
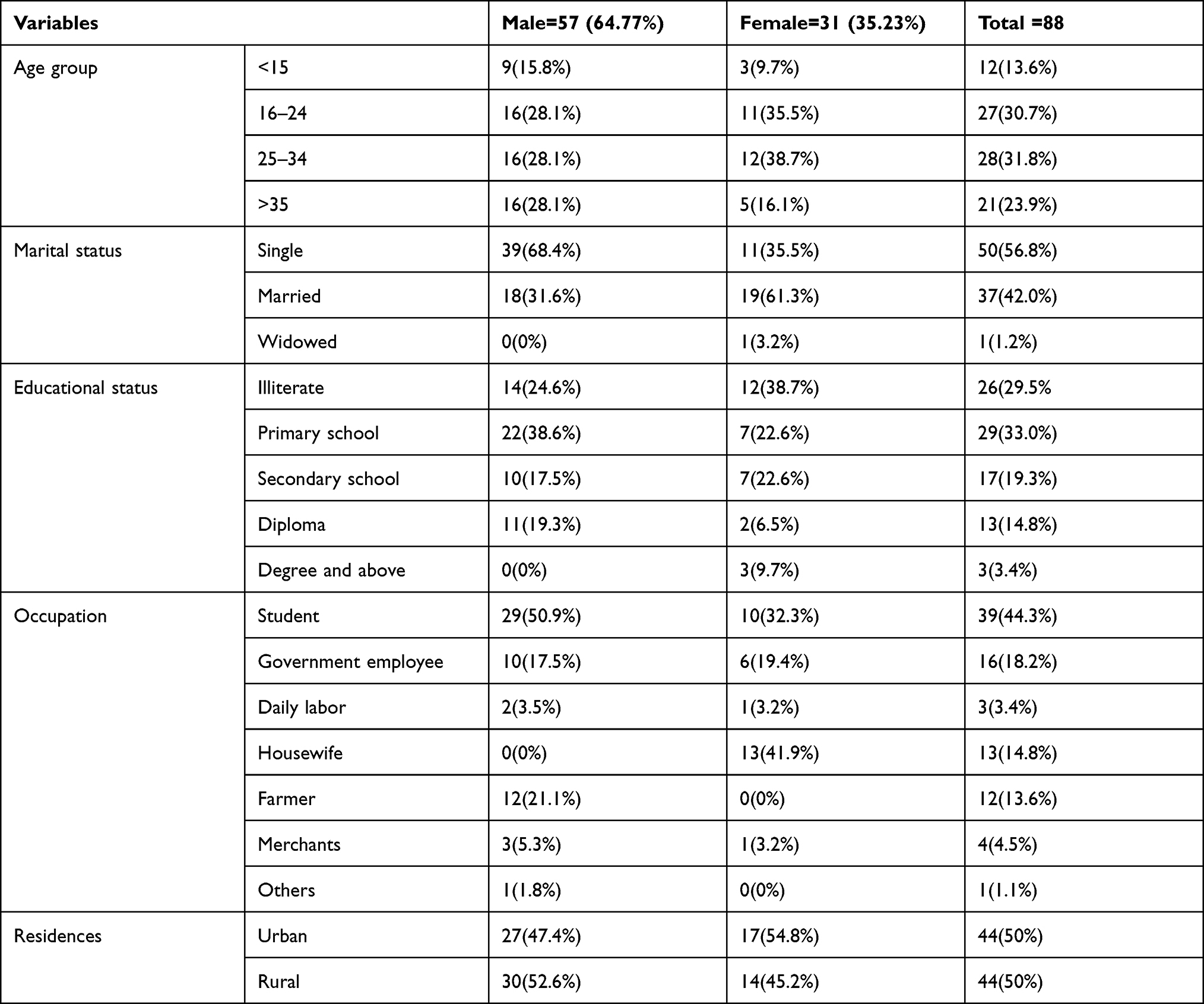 |
Table 1 Socio-Demographic Characteristics of the Study Participants at Dembia Primary Hospital and Teda Health Center, Northwest Ethiopia, 2020 (N=88) |
Among the 88 study participants, 77 (88%) were infected with P. falciparum, 9 (10%) were infected with P. vivax, and 2 (2%) had mixed infection (P. falciparum and P. vivax). In terms of parasitaemia, 42% (37/88) were diagnosed with high parasitaemia, 27% (24/88) with moderate parasitaemia, and 31% (27/88) with low parasitaemia.
Comparison of Liver Enzyme and Lipid Profiles with the Normal Reference Range
Prior to antimalarial drug administration, as compared with the respective normal reference ranges (10–40, 10–55, 32–92, and <150), 87.5% (77/88) AST, 12.5% (11/88) ALT, 43.2% (38/88) ALP, and 17.2% (16/88) TG, deviation was observed. Moreover, the serum level of HDL was found below the lower limit of the normal reference range in 87.5% (77/88) malaria positive study participants when compared to the normal reference range (>40). In contrast to this, the serum level of LDL and TC among all malaria-infected patients were found within the normal range (<100 and<200).
After anti-malaria drug administration, 100% (88/88) of participants’ AST, ALT, HDL, LDL and 92% of participants’ ALP, 94.3% participants’ TC, and 86.4% of participants’ TG were found to be within the normal reference ranges.
Liver Enzymes and Lipid Profiles Before an Anti-Malaria Treatment Based on Sex
Based on the independent t-test analysis the study showed that no statistically significant differences in liver enzymes and lipid profile parameters between male and female study participants in pre-treatment (Table 2).
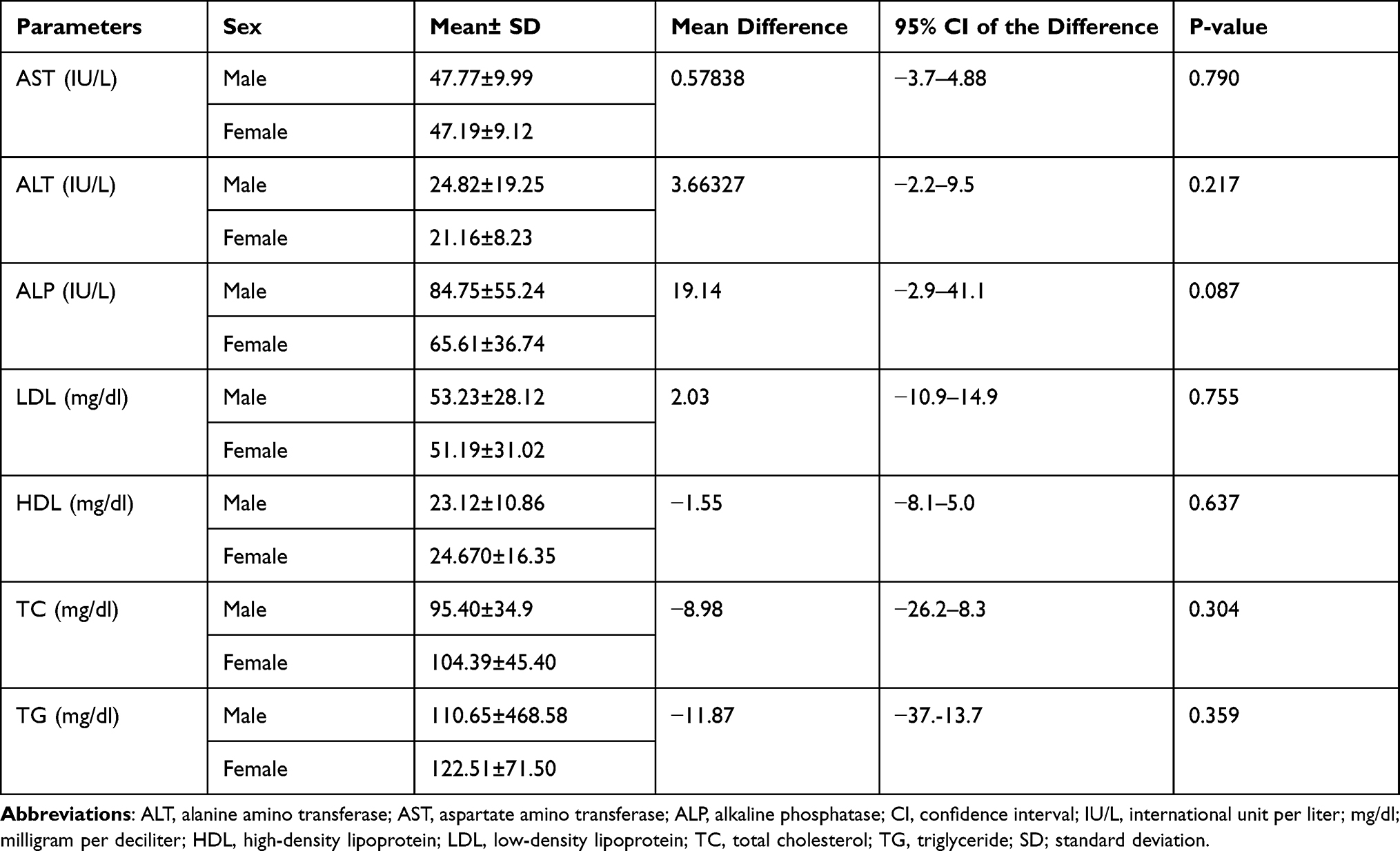 |
Table 2 Liver Enzymes and Lipid Changes Before Anti-Malaria Treatment Based on Sex Among Malaria Infected Patients (N=88) at Dembia Primary Hospital and Teda Health Center, North West Ethiopia, 2020 |
Liver Enzymes and Lipid Profile Parameters Change Before Anti-Malaria Treatment Based on Age Grouping
Based on one-way ANOVA analysis the serum levels of ALP were found to be decreased when the participant’s age groups were increased. These ALP serum measurements were 118.08±58.5, 84.85±52.66, 67.21±48.01, 60.71±28.80 in the age groups of<15yrs, 16–24yrs, 25–34yrs, and >35yrs, respectively (P =0.006). On the other hand, the alteration of serum level of total cholesterol result was found to be associated in the age groups of <15yrs and 25–34yrs. This association showed an increased level of total cholesterol from the age group <15 (71.2500 ± 31.11) to 25–34yrs (111.32 ± 44.07), (P =0.025). Other parameters associations of the participant’s age group are indicated (Table 3).
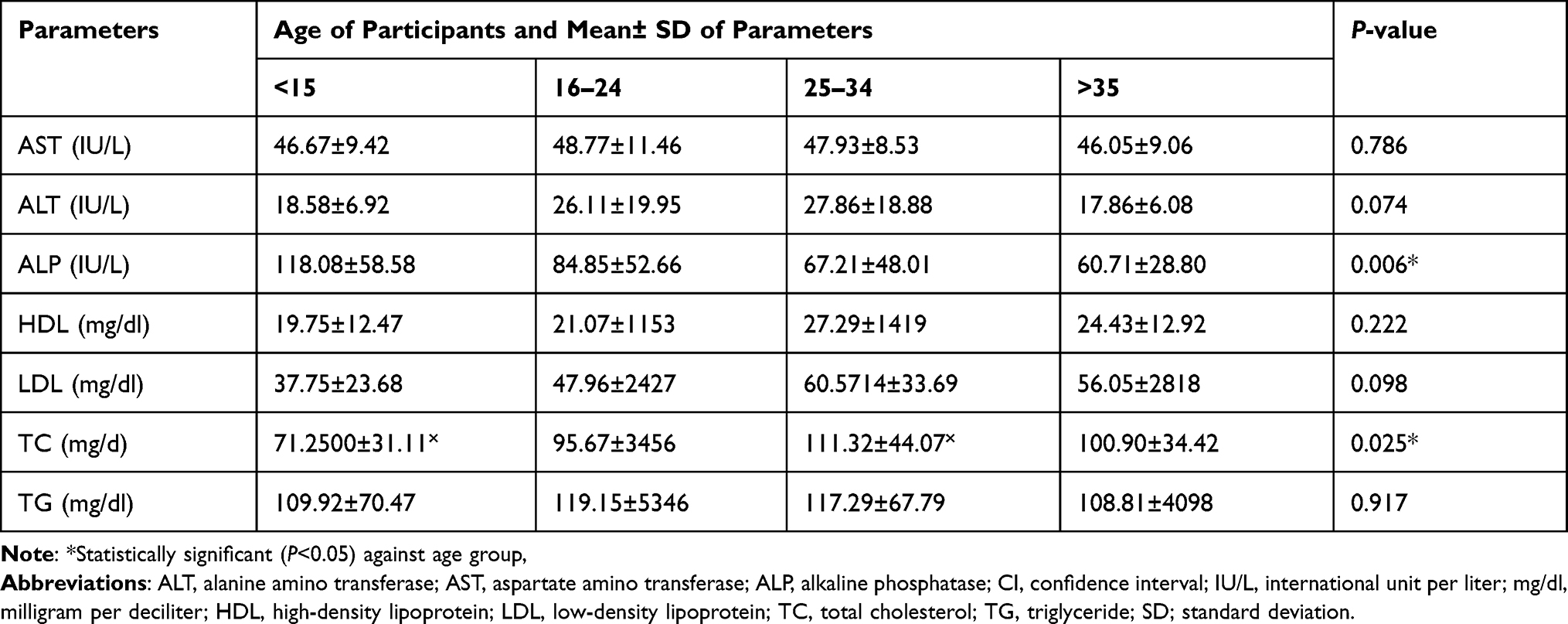 |
Table 3 Some Liver Enzyme and Lipid Profile Measurements in Different Age Groups of Malaria-Infected Participants Before Treatment (N=88) at Dembia Primary Hospital and Teda Health Center, North West Ethiopia, 2020 |
Serum Liver Enzymes and Lipid Profiles in Different Level of Parasitaemia Among Malaria-Infected Patients Before Anti-Malaria Treatments
During the assessment of some liver enzyme measurements in association with the density of malaria parasitaemia, AST, ALT, and ALP measurements showed an increased serum level in proportion to increasing the density of malaria parasitaemia. In this regard, based on one-way ANOVA analysis, the serum level of AST was found to be significantly increased in malaria-infected patients (P<0.001) with the increase in the degree of parasitaemia levels from low, moderate to high (39.70±3.55 IU/L, 44.42±3.22 IU/L and 55.35±9.69 IU/L), respectively. Moreover, ALT and ALP also were found to be increased proportionally with increasing the density of malaria parasitaemia, but the increases were not statistically significant (P>0.05%). On the other hand, serum HDL level was found to be significantly decreased (P =0.024) in malaria-infected patient when the density of parasitaemia increases from low to moderate parasitaemia. Even though HDL decrease was observed when the parasitaemia level increased from moderate to high, there was no statistically significant association (P>0.05) (Table 4).
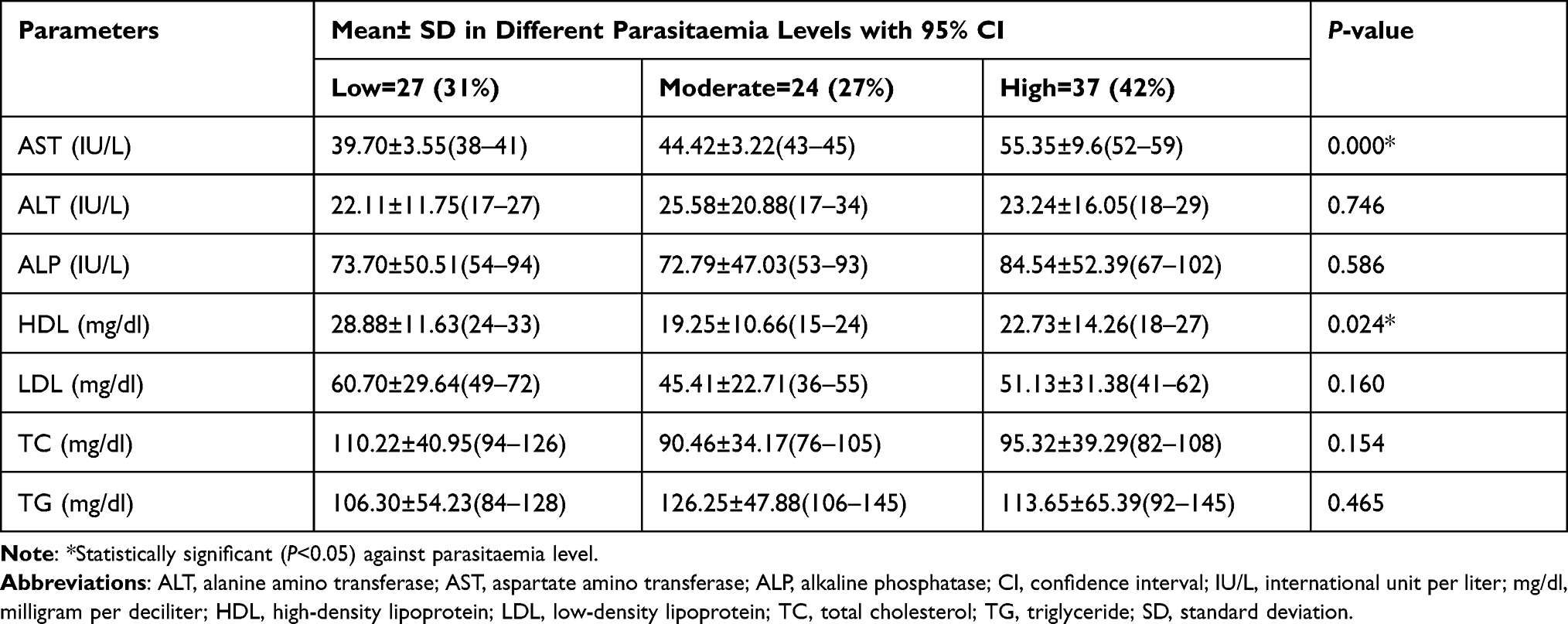 |
Table 4 Baseline Liver Enzymes and Lipid Profiles in Different Levels of Malaria Among Malaria-Infected Patients (N=88) at Dembia Primary Hospital and Teda Health Center, North West Ethiopia, 2020 |
Alteration of Mean Liver Enzymes and Lipid Profiles Before and After Anti-Malaria Treatment: Comparison
According to the paired t-test analysis, the mean pre-treatment concentration for serum AST was 47.60±9.65IU/L and for post- treatment the concentration was 33.90±15.15 IU/L. Comparison of pre-treatment and post-treatment mean concentrations showed a t-value of 7.137 with a p-value of <0.001. This post-treatment mean concentration was significantly lower compared to the pre-treatment level. Mean values for ALP were 78.01±50.14 IU/L and 75.45±37.64IU/L for pre-treatment and post-treatment, respectively. Comparison of these two means showed a t-value of 0.550 with a p-value of 0.581, which was not statistically significant. Moreover, there was no ALT alteration during pre-treatment (23.53±16.28 IU/L) and post-treatment (23.49±11.10IU/L) in the mean value of ALT level while triglyceride showed insignificant decreases at post-treatment (104.27±44.17IU/L) compared with the pre-treatment (114.82±57.57IU/L) measurements. On the contrary, the mean of HDL, LDL, and total cholesterol at post-treatment were found to be increased compared to pre-treatment (P>0.05)(Table 5).
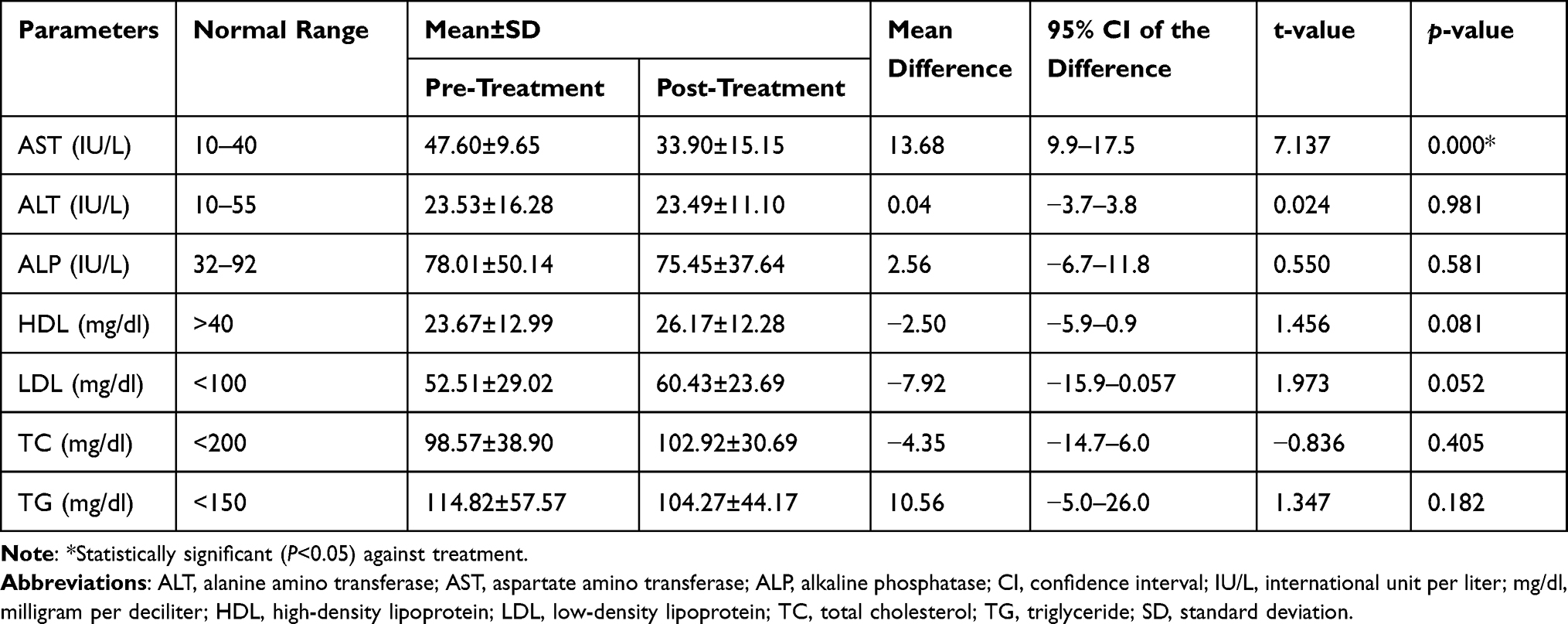 |
Table 5 Alteration of Liver Enzymes and Lipid Profiles Measurement Before and After Ant-Malaria Treatment Among Malaria-Infected Patients (N=88) at Dembia Primary Hospital and Teda Health Center, North West Ethiopia, 2020 |
Liver Enzymes and Lipid Profiles After Anti-Malaria Treatment Based on Types of Treatment
The present study showed that the levels of HDL were significantly high among those study participants treated with ACT only compared with those treated with ACT plus primaquine 39.83±15.10 and 24.79±11.46, respectively (Table 6). The levels of AST, ALT, ALP, LDL TC, and TG does not show statistically significant difference among study participant treated with ACT, ACT plus primaquine, chloroquine, and chloroquine plus primaquine, based on one-way ANOVA analysis.
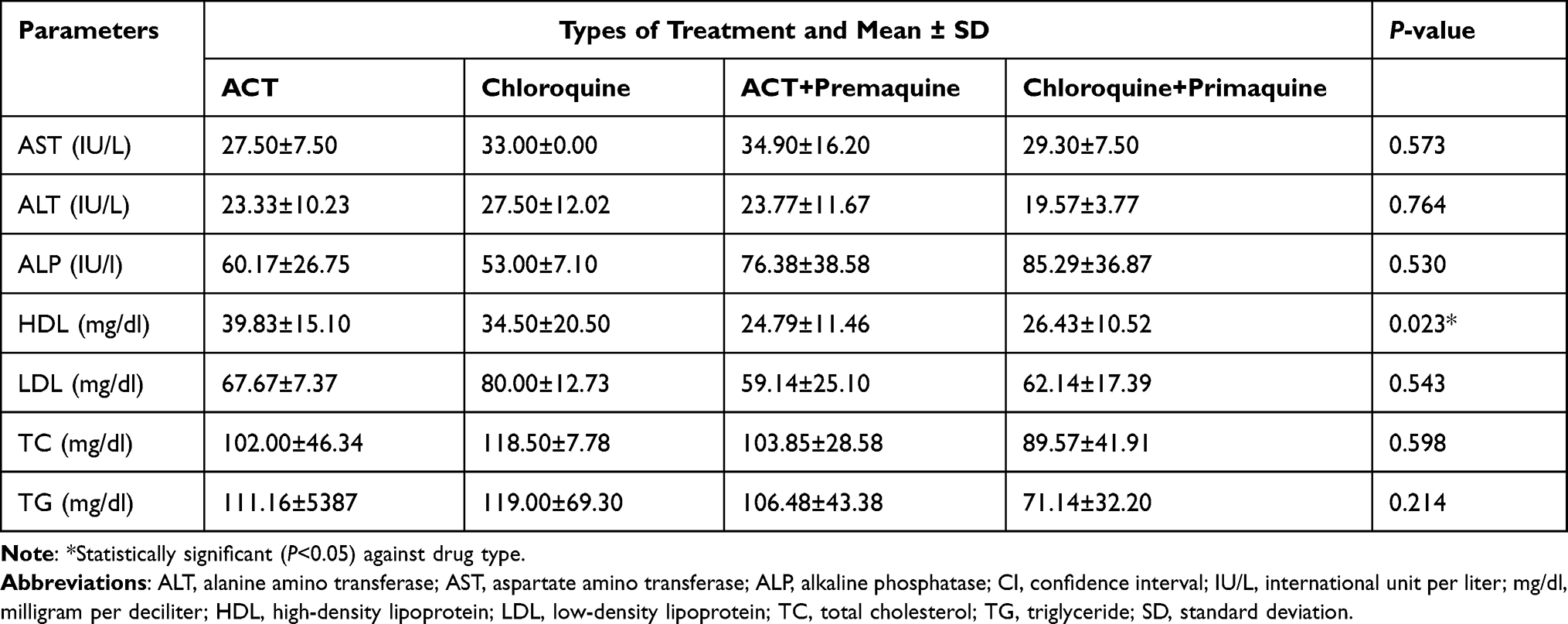 |
Table 6 Comparison of Liver Enzymes and Lipid Changes Based on Anti-Malaria Among Malaria-Infected Patients at Dembia Primary Hospital and Teda Health Center, North West Ethiopia, 2020 |
Discussion
Assessment of liver function tests and lipid profile parameters plays an important role in effective intervention management in malaria infection. Studies have been undertaken to determine the activities of enzymes like AST, ALT, and ALP among patients with Plasmodium malaria that serve as biomarkers of liver disorders and major lipid components in serum.1,26
In this study, during the assessment of some liver enzymes and lipid profile parameters prior to anti-malarial drug administration, 87.5% (77/88) cases of AST, 12.5% (11/88) of ALT, and 43.2% (38/88) of ALP were found to be increased in malaria-infected study participants as compared to normal reference ranges (10–40, 10–55, and 32–92), respectively. A study from India had reported relatively similar ALP (43.33%), lower AST (75%), and higher ALT (65%) levels.40 While 87.5% of HDL in the current study participants was lower than compared with normal reference ranges 17.2% of the study participants’ triglyceride result was higher than the normal reference range. Total cholesterol and LDL levels of the study participants were within the normal reference ranges before anti-malarial treatment was administered. The finding of the present study agreed with a previous study finding conducted in Ethiopia where LDL (34.7±23.5) and TC (88.0±36.3) levels were reported41 and a similar result from India reported a value of LDL (70.45±22.720) and TC (103.52±35), respectively.38 On the other hand, our study findings on the level of TG, HDL and LDL are lower than a study conducted in Brazil where high TG (55.8%), HDL (92.8%), and LDL (97.6%) levels were reported.42 The possible explanation of the difference in liver enzymes and lipid profiles could be due to the utilization of different methods, replicates of samples, malaria species, or the difference of study participants in sociodemographic characteristics such as age and genetic variation.
In the current study, the mean value of ALP with age <15, 16–24, 25–34, and >35yrs range was 118.08±58.58, 84.85±52.66, 67.21±48.01, and 60.71±28.80mg/dl, respectively. Though a statistically significant decrease was observed in the age group between<15 and 25-34, the serum levels of ALP were found to be decreased when the participant’s age groups were increased. This study result is inconsistent with the study conducted in Nigeria where the age group 10–29, 30–49, and 50–69 years mean values of ALP were 84.36±5.75, 90.50±20.84, and 108.00±23.5 (IU/L), respectively.3,43 The genetic and nutritional difference might be the possible reason for this variation of ALP activity difference between malaria-infected individuals.
Furthermore, in our finding during the baseline screening, the mean serum level of AST, ALT, and ALP were found to be increased proportionally, but statistical association (P<0.001) was observed only in AST with increasing the degree of parasitaemia levels from low, moderate to high (39.70±3.5538–41 IU/L, 44.42±3.2243–45 IU/L and 55.35±9.6 (52–59) IU/L with 95% CI, respectively. Similar AST level finding was reported in Yemen on low parasitaemia level which had 28.36 ± 1.04 mean value, but high AST level in moderate (58.63 ± 3.17IU/L) and high (96.03 ± 6.21IU/L) parasitaemia level.16 On the other hand contrary to the current finding, a study conducted in Nigeria had reported low values of AST (32.30±16.40 and 39.74±17.54IU/L) among low and moderate parasitaemia density patients, respectively.3 This variation could be due to the parasite density and the immunity status, age distribution, and sample size difference of the study participants.
In the current study serum HDL level was found to be significantly decreased (P=0.024) when the density of parasitaemia increases from low 28.88±11.63 (95% CI /24-33) mg/dl to moderate 19.25±10.66 (95% CI/15-24mg/dl) parasitaemia level. Though the HDL level was decreased when the parasitaemia level increased from moderate to high 22.73±14.26 (95% CI/18-27), no significant statistical association was found (P>0.05). Similarly no significant association was found on LDL, TC, and TG lipid profiles among the different degrees of parasitaemia. The current study finding of HDL is consistent with a previous study done in Ethiopia that the HDL mean values were (22.4±14.5, 19.90±12.6 and 18.90±14.5mg/dl) in low, moderate, and high parasitaemia levels, respectively.41 The present HDL finding is inconsistent with a study conducted in Nigeria where the HDL mean values were (46.4±11.6 and 23.2±3.9 mg/dl) in mild and severe malaria, respectively.44 The reason for this variation might be difference in parasite load, sample size, immunity status, and genetics of the study participants.
In this study, according to the paired t-test analysis, the mean serum level of AST at post-treatment (33.90±15.15IU/L) was significantly lower when compared with the pre-treatment (47.60±9.65I/L) level which has 13.68 IU/L mean difference of t-value=7.137 (P <0.001) and (95% CI/ 9.9–17.5IU/L). The mean of ALP also showed insignificant decreases at post-treatment (75.45±37.64IU/L) compared with the pre-treatment (78.01±50.14IU/L)(95% CI/-6.7–11.8IU/L), while there were no ALT alterations between pre-treatment (23.53±16.28IU/L) and post-treatment (23.49±11.10IU/L) with (95% CI/-3.7–3.8IU/L). l Our AST result is in line with a study done in India where AST mean value of 67.064±26.027 and 49.606±17.966IU/L is reported for pre-and post-treatment respectively with 17.46IU/L mean difference.45
In the current study, Triglyceride level showed insignificant decrease at post-treatment (104.27±44.17mg/dl) compared with the pre-treatment (114.82±57.57mg/dl) at (95% CI/-5.0–26.0mg/dl). On the contrary, the mean of HDL, LDL and TC at post-treatment were found to be decreased in 2.50, 7.92, and 4.35 with (95% CI/ −5.9–0.9,-15.9-0.057,-14.7–6.0mg/dl) when compared with pre-treatment, respectively. However, the increases were not statistically significant (P>0.05). Except for HDL, these study results are in line with a study reported from Nigeria where TG (0.170), TC (0.18), HDL (2.36), and LDL (−2.7) mg/dl were reported. Similar pre and post treatment result were also reported in Gabon (TC (−12.98), HDL-C (−9.55); LDL (−9.96), and TG levels (0.9).26,46 The mean difference in our findings is inconsistent with the mean difference of other study reports from Nigeria where HDL (1.28), LDL (5.51), TG (4.41), and TC (−6.49),47 and from India where TC (−12.34), HDL (−1.44), LDL (−3.19) and TG (11.42), is reported respectively.48 The possible explanation for this variation might be due to the physiological, environmental, host immunity, and nutritional status differences.
Limitations of the Study
The major limitation of this study is factors that may affect liver enzymes and lipid parameters, such as anthropometric and micronutrient characteristics of patients are not taken into account during the study. The study was only a one round 14 days follow-up. This will have a limitation in the generalization of the findings compared with 28 days follow-up study.
Conclusion and Recommendation
The current study had shown that malaria infection had resulted in the alteration of liver enzymes and lipid profiles. Although TC and LDL levels were within the normal range, there was an increase in AST, ALT, ALP, and TG level and decreased level of HDL as the malaria parasitaemia level increases. After anti-malaria treatment, these parameters which deviate from the normal range were reversed. The pre-treatment and post-treatment mean values showed significant change in AST level and lower mean serum level on ALP and TG. On the contrary, there was no level difference in ALT between pre-treatment and post-treatment mean values. In general, while malaria infection impairs liver enzyme and lipid function, treatment with antimalarial had reversed its function. However, for solid generalization, we recommend 28 days follow-up study accompanied with anthropometric and nutrition assessment in comparison with apparently healthy individuals.
Abbreviations
ALT, alanine amino-transferase; ALP, alkaline phosphatase; ACTs, artemisinin-based combination therapies; AST, aspartate amino-transferase; BF, blood film; CQ, chloroquine; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; HDL, high density lipoprotein; LFTs, liver function tests; LDL, low-density lipoprotein; OPD, outpatient department; SOPs, standard operation procedures; TC, total cholesterol; VLDL, very low-density lipoproteins; WBCs, white blood cells.
Data Sharing Statement
All data is included in the manuscript.
Ethics Approval and Consent to Participate
The study was conducted after ethical approval was obtained from the Research and Ethics Committee of the School of Biomedical and Laboratory Science, College of Medicine and Health Sciences & Specialized Hospital, University of Gondar. Following an explanation on the purpose, benefits, and the possible risks of the study, written informed consent was obtained from adults/guardians and ascents were obtained from all study participants. The participants were informed they were free to withdraw from the study at any time. Compensation for transport was provided for every patient’s scheduled visit. The study complies with the declaration of Helsinki.
Acknowledgments
The authors would like to express deepest gratitude for study participants for their interest to participate in the study. We also acknowledge Dembia primary hospital, Teda health center, and University of Gondar comprehensive specialized hospital clinical chemistry staffs for their contribution to the entire work of data collection and processing. Our gratitude goes to the University of Gondar, College of Medicine and Health Sciences, School of Biomedical and Laboratory Sciences, Department of Medical Parasitology for letting us to do this public health important research work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The research was financially supported by University of Gondar.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Latif A, Mansha M, Saif K, Fatima S. Histopathological effects of different artemisinin derivatives on liver of male albino mice. J Anim Plant Sci. 2018;28(6):1701–1708.
2. Barber BE, Rajahram GS, Grigg MJ, William T, Anstey NM. World malaria report: time to acknowledge Plasmodium knowlesi malaria. Malar J. 2017;16(1):1–3. doi:10.1186/s12936-017-1787-y
3. Onyesom I, Onyemakonor N. Levels of parasitaemia and changes in some liver enzymes among malarial infected patients in edo-delta region of Nigeria. Curr Res J Biol Sci. 2011;3(2):78–81.
4. Sharma C, Awasthi SK. Recent advances in antimalarial drug discovery—challenges and opportunities. In: An Overview of Tropical Diseases. 2015:39.
5. World Health Organization. World malaria report 2020: 20 years of global progress and challenges. J Malar. 2020:2020:1–51.
6. Taffese HS, Hemming-Schroeder E, Koepfli C, et al. Malaria epidemiology and interventions in Ethiopia from 2001 to 2016. Infect Dis Poverty. 2018;7(1):1–9. doi:10.1186/s40249-018-0487-3
7. Deress T, Girma M. Plasmodium falciparum and Plasmodium vivax Prevalence in Ethiopia: a systematic review and meta-analysis. Malar Res Treat. 2019;2019:12.
8. Alemu A, Abebe G, Tsegaye W, Golassa L. Climatic variables and malaria transmission dynamics in Jimma town, South West Ethiopia. Parasit Vectors. 2011;4(1):30. doi:10.1186/1756-3305-4-30
9. Augustine O. Effect of Plasmodium falciparum on liver function parameters of children in Akoko Area of Ondo State, Nigeria. J Diagn. 2018;5(1):1–5. doi:10.18488/journal.98.2018.51.1.5
10. Hoekstra LT, de Graaf W, Nibourg GA, et al. Physiological and biochemical basis of clinical liver function tests: a review. Ann Surg. 2013;257(1):27–36. doi:10.1097/SLA.0b013e31825d5d47
11. Wunderlich F, Al-Quraishy S, Dkhil MA. Liver-inherent immune system: its role in blood-stage malaria. Front Microbiol. 2014;5:559. doi:10.3389/fmicb.2014.00559
12. Krücken J, Dkhil MA, Braun JV, et al. Testosterone suppresses protective responses of the liver to blood-stage malaria. Infect Immun. 2005;73(1):436–443. doi:10.1128/IAI.73.1.436-443.2005
13. Faucher J-F, Ngou-Milama E, Missinou M, Ngomo R, Kombila M, Kremsner PG. The impact of malaria on common lipid parameters. Parasitol Res. 2002;88(12):1040–1043. doi:10.1007/s00436-002-0712-6
14. Kochar D, Agarwal P, Kochar S, et al. Hepatocyte dysfunction and hepatic encephalopathy in Plasmodium falciparum malaria. Int J Med. 2003;96(7):505–512.
15. Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. Cmaj. 2005;172(3):367–379. doi:10.1503/cmaj.1040752
16. Al-Salahy M, Shnawa B, Abed G, Mandour A, Al-Ezzi A. Parasitaemia and its relation to hematological parameters and liver function among patients malaria in Abs, Hajjah, Northwest Yemen. Interdiscip Perspect Infect Dis. 2016:2016. doi:10.1155/2016/5954394
17. Fabbri C, de Cássia Mascarenhas-netto R, Lalwani P, et al. Lipid peroxidation and antioxidant enzymes activity in Plasmodium vivax malaria patients evolving with cholestatic jaundice. Malar J. 2013;12(1):1–7. doi:10.1186/1475-2875-12-315
18. Mohanty S, Mishra S, Das B, et al. Altered plasma lipid pattern in falciparum malaria. Ann Trop Med Parasitol. 1992;86(6):601–606. doi:10.1080/00034983.1992.11812715
19. Jiang J, Nilsson-Ehle P, Xu N. Influence of liver cancer on lipid and lipoprotein metabolism. Lipids Health Dis. 2006;5(1):1–7. doi:10.1186/1476-511X-5-4
20. Sibmooh N, Yamanont P, Krudsood S, et al. Increased fluidity and oxidation of malarial lipoproteins: relation with severity and induction of endothelial expression of adhesion molecules. Lipids Health Dis. 2004;3(1):15. doi:10.1186/1476-511X-3-15
21. Lopes-Virella M, Wohltmann H, Loadholt C, Buse M. Plasma lipids and lipoproteins in young insulin-dependent diabetic patients: relationship with control. Diabetologia. 1981;21(3):216–223. doi:10.1007/BF00252657
22. Pfeifer MA, Brunzell JD, Best JD, Judzewitsch RG, Halter JB, Porte D. The response of plasma triglyceride, cholesterol, and lipoprotein lipase to treatment in non-insulin-dependent diabetic subjects without familial hypertriglyceridemia. Diabetes. 1983;32(6):525–531. doi:10.2337/diab.32.6.525
23. Visser BJ, Wieten RW, Nagel IM, Grobusch MP. Serum lipids and lipoproteins in malaria-a systematic review and meta-analysis. Malar J. 2013;12(1):442. doi:10.1186/1475-2875-12-442
24. Tran PN, Brown SH, Rug M, Ridgway MC, Mitchell TW, Maier AG. Changes in lipid composition during sexual development of the malaria parasite Plasmodium falciparum. Malar J. 2016;15(1):1–13. doi:10.1186/s12936-016-1130-z
25. Khovidhunkit W, Kim M-S, Memon RA, et al. Effects of infection and inflammation on lipid and lipoprotein metabolism: mechanisms and consequences to the host. J Lipid Res. 2004;45(7):1169–1196. doi:10.1194/jlr.R300019-JLR200
26. Edikpo N, Okonkwo PO, Adikwu E. Effect of artemether treatment on plasma lipid profile in malaria. Pharmacol Pharm. 2014;5(07):646. doi:10.4236/pp.2014.57074
27. World Health Organization. Guidelines for the treatment of malaria: World Health Organization; 2015.
28. Enato EF, Okhamafe AO. Plasmodium falciparum malaria and antimalarial interventions in sub-Saharan Africa: challenges and Opportunities. Afr J Biotech. 2005;4:13.
29. Assefa A, Kassa M, Tadese G, Mohamed H, Animut A, Mengesha T. Therapeutic efficacy of artemether/lumefantrine (Coartem®) against Plasmodium falciparum in Kersa, South West Ethiopia. Parasit Vectors. 2010;3(1):1–9. doi:10.1186/1756-3305-3-1
30. Navarro VJ, Senior JR. Drug-related hepatotoxicity. N Engl J Med. 2006;354(7):731–739. doi:10.1056/NEJMra052270
31. Ugokwe C, Asomba H, Onwuzulike I. Hepatotoxicity potential of coartemether on Wistar albino rat using liver enzyme assay. J Pharm Biol Sci. 2015;10:66–70.
32. Alemu A, Muluye D, Mihret M, Adugna M, Gebeyaw M. Ten year trend analysis of malaria prevalence in Kola Diba, North Gondar, Northwest Ethiopia. Parasit Vectors. 2012;5(1):1–6. doi:10.1186/1756-3305-5-173
33. Addisu A, Tegegne Y, Mihiret Y, Setegn A, Zeleke AJ. A 7-year trend of malaria at primary health facilities in Northwest Ethiopia. J Parasitol Res. 2020;2020. doi:10.1155/2020/4204987
34. World Health Organization. Methods for surveillance of antimalarial drug efficacy; 2009.
35. Mathison BA, Pritt BS. Update on malaria diagnostics and test utilization. J Clin Microbiol. 2017;55(7):2009–2017. doi:10.1128/JCM.02562-16
36. Adewoyin A. Peripheral blood film-a review. Ann Ib Postgrad Med. 2014;12(2):71–79.
37. Oyewole I, Senusie S, Mansaray M. Plasmodium falciparum-induced kidney and liver dysfunction in malaria patients in Freetown, Sierra Leone. Sierra Leone J Biomed Res. 2010;2(1):70–74. doi:10.4314/sljbr.v2i1.56611
38. Warjri SB, Ete T, Mishra A, et al. Association between clinical malaria and blood lipids in north eastern India. J Adv Med Med Res. 2016;16:1–7.
39. Bush V, Smola C, Schmitt P. Evaluation of the Beckman Coulter DxC 700 AU chemistry analyzer. Pract Lab Med. 2020;18:e00148. doi:10.1016/j.plabm.2019.e00148
40. Gurjeet Singh R, Maheshwari U, Samant P. Role of liver enzymes in patients infected with Plasmodium vivax and Plasmodium falciparum. Int J Adv Microbiol Health Res. 2018;2(1):650–654.
41. Sirak S, Fola AA, Worku L, Biadgo B. Malaria parasitemia and its association with lipid and hematological parameters among malaria-infected patients attending at Metema Hospital, Northwest Ethiopia. Pathol Lab Med Int. 2016;8:43–50. doi:10.2147/PLMI.S118946
42. Dias RM, Vieira JLF, BdC C, et al. Lipid profile of children with malaria by Plasmodium vivax. J Trop Med. 2016;2016. doi:10.1155/2016/9052612
43. Ebenezer D-IO. Evaluation of some biochemical parameters of Plasmodium falciparum infected inhabitants of Ekpoma Metropolis, Nigeria. Adv Biomed Sci. 2018;3(1):1.
44. Kiru A, Bala R, Abdulazeez A, et al. Lipid profile and electrolyte level in malaria patients attending Muhammadu Abdullahi Wase Specialist Hospital, Kano State, Nigeria. JComplement Altern Med Res. 2018;5(4):1–7. doi:10.9734/JOCAMR/2018/41215
45. Mannu A, Agarwalla SK, Vasudevan J, Subramaniam K, Ahamed Basha A. Hepatic dysfunction in children with complicated malaria. Int J Contemp Pediatr. 2018;5(2):5–28. doi:10.18203/2349-3291.ijcp20180552
46. Visser BJ, de Vries SG, Vingerling R, et al. Serum lipids and lipoproteins during uncomplicated malaria: a cohort study in Lambarene, Gabon. Am J Trop Med Hyg. 2017;96(5):1205–1214. doi:10.4269/ajtmh.16-0721
47. Jacob EA. Assessment of altered plasma lipid pattern in Plasmodium falciparum malaria infected and non infected individuals. Int J Hematol Disord. 2014;1:27–30.
48. Kullu BK, Majhi C, Pradhan B, Swain DK. Lipid profiles among Plasmodium falciparum infected, non malarial febrile patients and volunteers. Int J Adv Med. 2018;5(3):556. doi:10.18203/2349-3933.ijam20181661
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.