Back to Journals » Infection and Drug Resistance » Volume 15
Liver Abscess Combined with Endogenous Endophthalmitis Caused by Genotype ST25 Serotype K2 Hypervirulent Klebsiella pneumoniae: A Case Report
Authors Lin J, Huang Y, Qian L, Pan X, Song Y
Received 31 May 2022
Accepted for publication 2 August 2022
Published 17 August 2022 Volume 2022:15 Pages 4557—4561
DOI https://doi.org/10.2147/IDR.S376443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jian Lin,1 Yize Huang,1 Li Qian,2 Xiaolong Pan,3 Youliang Song1
1Department of Infectious Diseases, Tongling People’s Hospital, Tongling, Anhui, 244000, People’s Republic of China; 2Department of Ophthalmology, Tongling People’s Hospital, Tongling, Anhui, 244000, People’s Republic of China; 3Medical Laboratories, Tongling People’s Hospital, Tongling, Anhui, 244000, People’s Republic of China
Correspondence: Youliang Song, Tel +86 13956250358, Email [email protected]
Abstract: At present, invasive syndrome caused by hypervirulent Klebsiella pneumoniae (HvKp) is a widespread concern, and HvKp strains of different genotypes have been isolated. Here, we report a case of community-acquired liver abscess and endogenous endophthalmitis caused by a genotype ST25 serotype K2 (ST25-K2) HvKp strain in China. A 51-year-old man with diabetes was transferred to our hospital from a local community hospital with persistent fever for > 20 days and blurred vision in his left eye. A detailed examination revealed a liver abscess, endogenous endophthalmitis, and pneumonia. Bacterial cultures of pus from the liver abscess and the vitreous abscess of the left eye yielded Klebsiella pneumoniae (Kp), which was sensitive to the recommended drugs. In addition to positive string tests, a genetic analysis showed that the strain belonged to sequence type 25 (ST25) and serotype K2, and carried already-reported virulence genes, including iucA, rmpA2, rmpA, aerobactin, and entB. The pathogenic agent isolated from this patient was identified as HvKp. The patient’s general condition improved after a combination of treatments, including antimicrobial therapy, abscess drainage, and nutritional support. Unfortunately, the patient lost the vision in his left eye and developed secondary glaucoma, resulting in inevitable enucleation. Sequence 25 serotype K2 HvKp strains have been previously associated with nosocomial infections, but none associated with community-acquired liver abscess combined with endogenous endophthalmitis has yet been reported. Clinicians must be alert to the possibility of genotype ST25-K2 HvKp infection in patients with community-acquired liver abscess combined with an invasive infection, such as ocular discomfort.
Keywords: hypervirulent Klebsiella pneumoniae, liver abscess, endogenous endophthalmitis, sequence type 25, serotype K2
Introduction
Hypervirulent Klebsiella pneumoniae (HvKp) has become one of the most important pathogens in the world. With continuing research, the microbial characteristics of HvKp have gradually emerged, but there are still controversies. Due to its hypermucoviscosity, this bacterium can cause liver abscesses and multiple co-infections, including meningitis, endophthalmitis, and prostate abscesses, which together are known as “invasive syndrome”.1 The treatment strategies for HvKp-induced invasive syndrome vary. Empirical antimicrobial therapy is rarely comprehensive for the treatment of these diseases, and abscess drainage and local targeted therapy are also required. However, clinicians have not sufficiently considered HvKp infection in many medical institutions. Here, we present a case of invasive syndrome caused by a sequence type 25 (ST25) serotype K2 (ST25-K2) HvKp strain to help clinicians in the clinical diagnosis and treatment of HvKp.
Case Presentation
A 51-year-old male patient was admitted to our hospital with persistent fever for >20 days and blurred vision in his left eye. He had a history of untreated diabetes. The patient was aware of abdominal distention, but did not attend the hospital until he developed a fever of 39.5 °C. At the community hospital, he was diagnosed with pneumonia, uncertain intestinal obstruction, uncertain vitreous hemorrhage, and diabetes, and was treated with empirical antibiotics. When his condition became critical, he was transferred to the local tertiary hospital for further treatment. Laboratory tests revealed a white blood cell count of 11.94 × 109/L (normal range = 4–9.5 × 109/L), a neutrophil count of 10.95 × 109/L (normal range = 2–6.5 × 109/L), serum albumin of 25.6 g/L (normal range = 40–55 g/L), serum creatinine of 123 μmol/L (normal range = 35–97 μmol/L), and random blood glucose of 22.4 mmol/L. Inflammatory markers were also measured, with results showing C-reactive protein exceeding 200 mg/L and procalcitonin of 29.82 μg/L. A computed tomographic scan showed multiple nodules in both lungs and intrahepatic cystic lesion with air accumulation (Figure 1), but imaging detected no intestinal obstruction. The clinician considered the patient’s infection to be fatal, although the pathogen had not yet been identified. Meropenem was used for antimicrobial chemotherapy after blood was taken for bacterial culture. Treatment measures such as albumin infusion and nutritional support were implemented simultaneously.
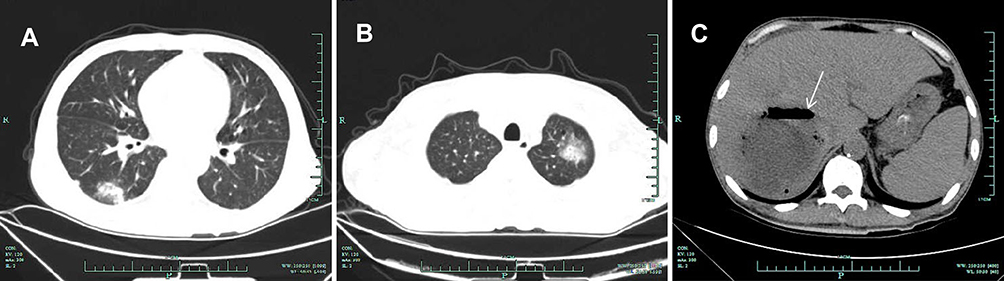 |
Figure 1 Computed tomographic scans of chest and abdomen. (A) and (B) Both lungs showed small scattered nodules and ground glass opacity. (C) A prominent low-density cystic lesion with gas accumulation (97 mm × 75 mm) in the liver (white arrow), which was considered to be ileus on an abdominal radiograph at the community hospital. |
However, the effect of treatment was poor. The patient’s body temperature continued to rise to 40.4 °C, which was attributed to the accumulation of pus in the liver abscess. Under the guidance of color ultrasound, the liver abscess was drained with percutaneous puncture, and 350 mL of brown pus was collected for bacterial culture. After the operation, the patient’s body temperature dropped rapidly and his inflammatory indicators gradually decreased. However, sight in his left eye was still blurry. After consultation with an ophthalmologist, he was diagnosed with endogenous endophthalmitis (EE) (Figure 2A and C) and an emergency vitreous injection was performed. The pus in the vitreous cavity was also aspirated for bacteriological culture.
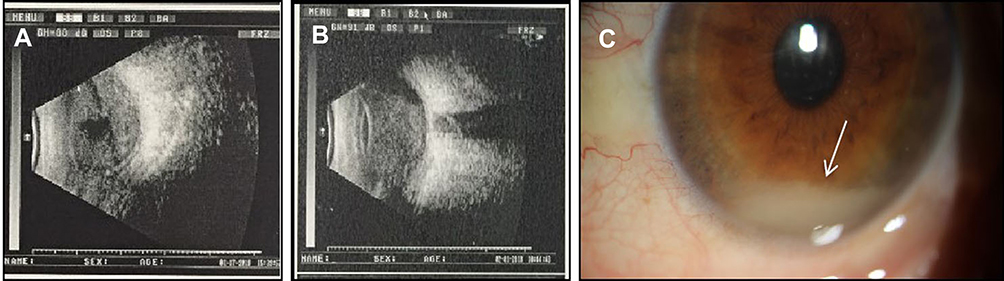 |
Figure 2 Professional medical examination with ophthalmological imaging showed the presence of hypopyon. (A) A color ultrasound image of the eyeball upon admission, with a large volume of pus in the vitreous cavity. (B) Color ultrasound image of the eyeball before enucleation, with extensive pus accumulation in the vitreous cavity, which had worsened significantly. (C) The patient presented with mild swelling of the left eyelid, hyperemia of the eye, mild edema of the left cornea, and an anterior atrial abscess, about 2 mm in depth (white arrow). |
Five days after admission, the bacterial culture of the collected pus samples yielded Klebsiella pneumoniae. In vitro antimicrobial sensitivity tests showed that both strains were sensitive to all the drugs recommended by the Clinical & Laboratory Standards Institute (CLSI). Viscous strings from the colonies were both >5 mm in length, indicating positive string tests (Figure 3). A multilocus sequence typing (MLST) analysis of the isolated strains was performed with PCR amplification, as previously described.2 Seven housekeeping genes (gapA, infB, mdh, pgi, phoE, rpoB, and tonB) were amplified and sequenced. The multiple sequence information was compared with the MLST database and the strains were identified as belonging to ST25. The associated virulence genes and capsule serotypes were also determined, as previously described.3,4 The strains were positive for virulence genes iucA, rmpA2, rmpA, aerobactin, and entB. The serotype of the capsule was K2. Therefore, we diagnosed the patient with invasive syndrome secondary to ST25-K2 HvKp infection, with multiple infected lesions in the liver, lung, and eye.
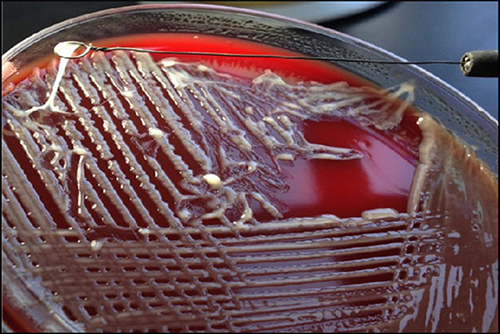 |
Figure 3 A string test was performed to confirm the hypermucoviscous phenotype of the isolated strain. A viscous string of > 5 mm in length was drawn from the colony, in a positive string test. |
Two weeks after admission, the patient had lost all vision in his left eye, accompanied by a very prominent headache and very high intraocular pressure. The ophthalmologist was consulted again and identified secondary glaucoma (Figure 2B). After a comprehensive evaluation and communication with the patient, he finally underwent left eye enucleation. The patient recovered and was discharged from the hospital on day 42 after admission. There was no recurrence of the disease at the 6-month follow-up.
Discussion
Klebsiella pneumonia, a Gram-negative bacterium, is one of the most important pathogenic bacteria associated with community- and hospital-acquired infections. It often causes infections of the bloodstream, respiratory tract, urinary system, abdominal cavity, and even the central nervous system.5 Klebsiella pneumoniae is divided into classical K. pneumoniae (cKp) and hypervirulent K. pneumoniae (HvKp), and the virulence of HvKp is significantly higher than that of cKp. Since its discovery in Taiwan in 1986,6 the clinical isolation of HvKp has been described throughout the world, but predominantly in Asia. At present, the definition of HvKp is still controversial. HvKp is characterized by a hypermucoviscous phenotype and hypervirulence, and can manifest as multiple invasive infections in infected persons, which can include liver abscess, prostate abscess, meningitis, lung abscess, endophthalmia, and so on.7–9 In recent years, the emergence of carbapenem-resistant HvKp (CR-HvKp) has presented great challenges to clinicians.10
Here, we report a patient with liver abscess and EE in the left eye caused by a strain of ST25-K2 HvKp, which to our knowledge, has rarely been reported in the literature. The probability of EE in HvKp-related bacteremia is almost 5.0%.11 Endogenous endophthalmitis is an aggressive manifestation in the eye caused by bacteria or fungi that spread through the bloodstream, and often leads to blindness. It is an ophthalmic emergency requiring urgent treatment. The vascular structure of the eye means that the right eye is usually involved.12 However, in our patient, EE occurred in the left eye. Effective treatment within 24–48 h of onset of the intraocular infection is thought to produce a desirable outcome, although studies have reported an eyeball removal rate of 41%.13 Common treatments for EE include intravitreal injection and vitrectomy. Our patient was treated with an intravitreal infusion soon after admission, but the ocular lesion failed to improve. After repeated consultations with ophthalmologists, it was considered that the patient’s retinal photoreceptor cells had been irreversibly damaged, resulting in irretrievable vision loss in his left eye. His physical condition also showed life-threatening deterioration, and we considered saving his life to be the primary challenge. After comprehensive treatment of the liver abscess, including puncture and drainage, the application of antimicrobial agents, and nutritional support, the patient’s condition improved continuously. However, he was seriously troubled by the anterior atrial abscess and intraocular hypertension, which proved to be secondary glaucoma and required ocular removal. Unfortunately, the patient’s left eye was removed on day 18 after admission.
A lack of awareness about the invasive syndrome caused by HvKp meant that the patient was initially diagnosed with intestinal obstruction and vitreous hemorrhage at the local community hospital, and no bacterial cultures were tested. Furthermore, blood bacterial cultures were negative many times after the patient was transferred to our hospital. However, cultures of pus collected from the liver abscess and vitreous abscess were both positive for K. pneumoniae. Further tests were performed to identify the K. pneumoniae strains.
The microbiology of HvKp is unique, including its hypermucoviscous phenotype and characteristic hypervirulence. Antibiotic sensitivity testing, MLST, string tests, virulence factor detection, and a serum killing test were used to verify this strain.14 A string test is often used to confirm the high viscosity of HvKp, but there are certain limitations in that a negative string test does not always exclude HvKp.15 The colonies of the strains we isolated produced viscous strings of >5 mm in length, in positive string tests. Previous studies have reported that the virulence of HvKp is largely related to the capsular antigen.16,17 The synthesis of the capsule (K antigen) is regulated by the transcription activator RmpA and the mucus-related protein MagA.18,19 The serology of the capsular antigens has been demonstrated in previous studies, and mainly include K1, K2, K5, K20, K57, K64, and KN1, but K1 and K2 are the main serological types.20 Studies have shown that HvKp serotypes K1 and K2 express a variety of virulence genes and play an inevitable role in liver abscess formation and invasive infections. Multilocus sequence typing was performed on our cultured strains, and the results were compared with the MLST database. The strains belonged to ST25 serotype K2, and carried already-reported virulence genes, including iucA, rmpA2, rmpA, aerobactin, and entB. Although the isolated strain showed significantly high viscosity and virulence, it was highly sensitive to microbiological agents, and the infection was eventually controlled with treatment. We defined the isolated strain as an HvKp strain based on the microbiological genotype and its clinical manifestations in the patient.
Invasive infections caused by ST25-K2 HvKp strains have been described in the past, but no association with intraocular invasion has been reported until now. ST25-K2 HvKp has been isolated from the sputum specimens of hospitalized patients only once according to the data published in China in recent decades. It should be noted that the strain in that study was resistant to carbapenems and was not associated with liver abscess or EE.21 In another study based on strains isolated from carriage and infections in mothers and their neonates in Madagascar, two strains were identified as ST25-K2 HvKp, but both were associated with urinary tract infections.22 Therefore, this is the first reported case of liver abscess combined with EE attributed to HvKp ST25-K2.
Conclusion
HvKp-related invasive infection is characterized by rapid progression and a high disability rate, and must be considered by clinicians. Endogenous endophthalmitis is subject to misdiagnosis and missed diagnosis. The possibility of HvKp infection should be considered in cases of ocular discomfort in patients with liver abscess. Multidisciplinary collaboration in both the diagnosis and treatment of these infections will improve the prognoses of patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
This case report was approved by the ethics committee of Tongling People’s Hospital.
Consent for Publication
Written informed consent for publication of his clinical details and clinical images was obtained from the patient.
Acknowledgments
We thank Dr. Juanxiu Qin, at the Department of Laboratory Medicine, Renji Hospital, Shanghai JiaoTong University, for her contribution to the identification of the isolated strains.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Russo TA, Marr CM. Hypervirulent Klebsiella pneumoniae. Clin Microbiol Rev. 2019;32(3):e00001–19. doi:10.1128/CMR.00001-19
2. Diancourt L, Passet V, Verhoef J, et al. Multilocus sequence typing of Klebsiella pneumoniae nosocomial isolates. J Clin Microbiol. 2005;43(8):4178–4182. doi:10.1128/JCM.43.8.4178-4182.2005
3. Brisse S, Passet V, Haugaard AB, et al. wzi Gene sequencing, a rapid method for determination of capsular type for Klebsiella strains. J Clin Microbiol. 2013;51(12):4073–4078. doi:10.1128/JCM.01924-13
4. Russo TA, Olson R, Fang CT, et al. Identification of biomarkers for differentiation of hypervirulent Klebsiella pneumoniae from classical K. pneumoniae. J Clin Microbiol. 2018;56(9):e00776–18. doi:10.1128/JCM.00776-18
5. Effah CY, Sun T, Liu S, et al. Klebsiella pneumoniae: an increasing threat to public health. Ann Clin Microbiol Antimicrob. 2020;19(1):1. doi:10.1186/s12941-019-0343-8
6. Liu YC, Cheng DL, Lin CL. Klebsiella pneumoniae liver abscess associated with septic endophthalmitis. Arch Intern Med. 1986;146(10):1913–1916. doi:10.1001/archinte.1986.00360220057011
7. Zou Q, Li Y. Hypervirulent Klebsiella pneumoniae. N Engl J Med. 2021;385(9):833. doi:10.1056/NEJMicm2101602
8. Salawati EM. Fatal disseminated pyogenic infection due to hypermucoviscous hypervirulent Klebsiella pneumoniae: a case report and literature review. Clin Case Rep. 2021;9(9):e4754. doi:10.1002/ccr3.4754
9. Yu CP, Wang S, Tian SF, et al. Clinical characteristics in patients with hypervirulent Klebsiella pneumoniae infection and its capsular serotypes and multilocus sequence typing. Zhonghua Nei Ke Za Zhi. 2019;58(5):361–365. doi:10.3760/cma.j.issn.0578-1426.2019.05.006
10. Liu C, Du P, Xiao N, et al. Hypervirulent Klebsiella pneumoniae is emerging as an increasingly prevalent K. pneumoniae pathotype responsible for nosocomial and healthcare-associated infections in Beijing, China. Virulence. 2020;11(1):1215–1224. doi:10.1080/21505594.2020.1809322
11. Lee HC, Chuang YC, Yu WL, et al. Clinical implications of hypermucoviscosity phenotype in Klebsiella pneumoniae isolates: association with invasive syndrome in patients with community-acquired bacteraemia. J Intern Med. 2006;259(6):606–614. doi:10.1111/j.1365-2796.2006.01641.x
12. Connell PP, O’Neill EC, Amirul IF, et al. Endogenous endophthalmitis associated with intravenous drug abuse: seven-year experience at a tertiary referral center. Retina. 2010;30(10):1721–1725. doi:10.1097/IAE.0b013e3181dd6db6
13. Hu CC, Ho JD, Lou HY, et al. A one-year follow-up study on the incidence and risk of endophthalmitis after pyogenic liver abscess. Ophthalmology. 2012;119(11):2358–2363. doi:10.1016/j.ophtha.2012.05.022
14. Gao Q, Shen Z, Qin J, et al. Antimicrobial resistance and pathogenicity determination of community-acquired hypervirulent Klebsiella pneumoniae. Microb Drug Resist. 2020;26(10):1195–1200. doi:10.1089/mdr.2019.0439
15. Fang CT, Chuang YP, Shun CT, et al. A novel virulence gene in Klebsiella pneumoniae strains causing primary liver abscess and septic metastatic complications. J Exp Med. 2004;199(5):697–705. doi:10.1084/jem.20030857
16. Zhang ZY, Qin R, Lu YH, et al. Capsular polysaccharide and lipopolysaccharide O type analysis of Klebsiella pneumoniae isolates by genotype in China. Epidemiol Infect. 2020;148:e191. doi:10.1017/S0950268820001788
17. Cubero M, Grau I, Tubau F, et al. Hypervirulent Klebsiella pneumoniae clones causing bacteraemia in adults in a teaching hospital in Barcelona, Spain (2007–2013). Clin Microbiol Infect. 2016;22(2):154–160. doi:10.1016/j.cmi.2015.09.025
18. Sun Y, Wu H, Shen D. Clinical and molecular analysis of Klebsiella pneumoniae causing liver abscess in China. J Mol Microbiol Biotechnol. 2016;26(4):245–251. doi:10.1159/000444367
19. Li B, Zhao Y, Liu C, et al. Molecular pathogenesis of Klebsiella pneumoniae. Future Microbiol. 2014;9(9):1071–1081. doi:10.2217/fmb.14.48
20. Zhu J, Wang T, Chen L, et al. Virulence factors in hypervirulent Klebsiella pneumoniae. Front Microbiol. 2021;12:642484. doi:10.3389/fmicb.2021.642484
21. Li J, Huang ZY, Yu T, et al. Isolation and characterization of a sequence type 25 carbapenem-resistant hypervirulent Klebsiella pneumoniae from the mid-south region of China. BMC Microbiol. 2019;19(1):219. doi:10.1186/s12866-019-1593-5
22. Rakotondrasoa A, Passet V, Herindrainy P, et al. Characterization of Klebsiella pneumoniae isolates from a mother-child cohort in Madagascar. J Antimicrob Chemother. 2020;75(7):1736–1746. doi:10.1093/jac/dkaa107
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.