Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Lived Experience and Risk Reduction Behaviors Among Sero-Negative Discordant Male Partners Living with HIV-Positive Women in Addis Ababa, Ethiopia, 2019: A Qualitative Phenomenological Study
Authors Bantigen K, Kitaw L ![]() , Negeri H
, Negeri H ![]()
Received 9 December 2021
Accepted for publication 9 March 2022
Published 19 March 2022 Volume 2022:14 Pages 119—128
DOI https://doi.org/10.2147/HIV.S353286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Kerebih Bantigen, Leul Kitaw, Hawine Negeri
Nursing and Midwifery, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Kerebih Bantigen, Nursing and Midwifery, Addis Ababa University, Addis Ababa, Ethiopia, Tel +251-912-248621, Email [email protected]
Objective: This study aimed to explore lived experience and risk reduction behaviors among sero-negative, discordant male partners living with HIV-positive women in Addis Ababa, Ethiopia, 2019.
Methods: A phenomenological study was conducted to explore lived experience and risk reduction behaviors. The study participants were purposively selected 13 sero-negative male partners living with HIV-positive women. An in-depth interview was used to explore important information. A semi-structured interview guide was used to execute the in-depth interview. The in-depth interview was analyzed thematically through the support of ATLAS-ti 7 software.
Results: Scientific explanation of discordant result is not well understood rather, it is associated with religious, cultural, natural resistance, and passive carrier explanations. Sero-negative partners faced several challenges and lived dilemmatic life related to partner mood or behavioral change, maintaining the marital relationship, the desire of child, psychosocial, sexual life, and lack of support system. Risk reduction behaviors like condom use, safe sex practice, preventing sexually transmitted infection, avoiding substance use, continuous checkup and follow-up were not well reflected in their lived experience and were poorly understood. Personalized use of sharp materials to avoid blood contact and support of a partner in the proper use of ART drugs were positively reported risk reduction behaviors.
Conclusion: Sero-negative partners need special attention just as HIV-positive partners in couples with the discordant result. Life suffering is not limited to HIV-positive partners, rather sero-negative partners also faced several challenges and dilemmatic life. HIV transmission risk reduction behavior is not well established and understood.
Keywords: HIV discordant, lived experience, risk reduction behavior, Addis Ababa, Ethiopia
Background
The overall burden of HIV/AIDS and sero-discordance result become an important issue in Africa, especially in sub-Saharan Africa.1 The prevalence of HIV discordance in Africa accounts for about one-half to two-thirds among cohabitating couples of HIV patients.2 In Africa, among discordant couples, women and men account for 47% and 53% of HIV index partners, respectively.3 In Ethiopia, the prevalence of HIV/AIDS among couples is about 1.1%; of which around 0.8% are sero-discordant couples.4 The risk of HIV transmission in a discordant couple is high unless consistent protective measures should be taken. Only a few couples can remain discordant for a long period.5 World Health Organization (WHO) focuses on the reduction of HIV transmission in discordant couples by enhancing couple and partner voluntary HIV testing, early initiation of ART, and consistent condom use.6 In developing countries, HIV discordant couples confronted complicated socio-economic challenges. Risk reduction measures are almost neglected.7,8
Risk reduction measures are behaviors acted by HIV discordant couples to minimize the risk of HIV sero-conversion. Risk reduction behaviors are determinant factors to prevent HIV transmission in a discordant couple.9 Male partners’ unwillingness and misconception are reasons for inconsistent condom use or total refusal.8 Women who live with HIV/AIDS experience various social, emotional, and behavioral changes like social isolation and depression. This behavioral change directly or indirectly affects the life of their sero-negative partners.10
Compared to concordant, couples with discordant results encountered various dilemmatic issues in their life. Maintaining marital relationships, fertility desire, social isolation, and sexual issues are a headache for discordant couples.11
Research reports showed that discordant couples end up with divorce and only a few couples maintain their relationship. Most of the time, the initiative of divorce comes from sero-negative male partners.12 It is usual that, HIV-positive partners faced different psychosocial and economic challenges, and stakeholders try to support them.7
However, the painful dilemmatic life of sero-negative partners in a discordant couple is almost ignored or lacks attention. Despite the high risk of HIV transmission and several life challenges, couple-based intervention and continuous follow-up are still limited in discordant couples. Especially, sero-negative partners carry many socio-economic burdens and continued with dilemmatic life situations. So, sero-negative partners need special health care support and follow-up besides the index case.11,13 Therefore, this study aimed to explore lived experience and risk reduction behaviors among sero-negative male partners living with HIV- positive women in Addis Ababa, Ethiopia, 2019.
Methods
Study Setting, Design, and Period
This phenomenological study was conducted from February 20 to May 20, 2019, in Addis Ababa, which is the capital city of Ethiopia. Addis Ababa used as the center of diplomacy for Africa, the seat of the African Union and Economic Commission for Africa. It has a population size of 7.178 million, as estimated in 2018.14 Addis Ababa is one of the cities with a high prevalence of HIV/AIDS.15
Study Participants
The study participants were purposively selected 13 sero-negative male partners living with HIV-positive women in Addis Ababa public health institutions. Participants were purposively selected based on the recommendation of health workers working at PMTICT and ART clinics by considering maximum variation in age, educational background, and duration of diagnosis as discordant. Volunteer participants were selected from the respective health institution by communicating with health workers working at PMTICT and ART clinics. Then, four participants were interviewed from Zewditu Memorial Hospital and three participants were interviewed from each health center (Kotebe Health Center, Bole Health Center, and Addis Ketema Health Center). The sample size was determined by data saturation when the interviewer had no longer heard or seen new information from new study participants. The richness of theoretical saturation was decided through the discussion of all the three investigators based on the themes of the interview guide when there is no new information able to form a new code or theme.
Data Collection Method
An in-depth interview was used to discover important information. A semi-structured interview guide was used to execute the in-depth interview (supplementary material). The interview guide was organized under three themes; understanding discordancy, 75 challenges faced, and risk reduction behaviors. An information sheet and informed consent form were delivered to all participants. An in-depth interview was performed among participants who voluntarily took part in the study and signed the consent form. The face-to-face in-depth interview was conducted by principal investigators. The interview was conducted in the respective health institution specifically in the HIV counseling room. The duration of the interview ranges from 40 minutes to 80 minutes. The interviewers had no relation with the participant other than this research 80 interview event. Two of the interviewers had previous experience in qualitative research since they are Ph.D. fellows and the third has also experience in qualitative data collection. A probe was used throughout the interviews to offer a clarification and inspire elaboration from the participant on specific issues that were a domain of interest to the investigator. A tape recorder was used to support the data collection. A type note was taken throughout the interview for cross-validation with the audio recordings and final interview transcripts.
Data Analysis and Trustworthiness of Data
Data analysis was done alongside with data collection. Investigators transcribed the audio record and written field notes verbatim after repeated listening and reading of the interviews. Then, the transcribed interview was translated from the local language (Amharic) into English. The translated data was entered into ATLAS-ti 7 software and analyzed by extracting important concepts into codes and then to themes. The manuscript was coded by the three investigators in English language. There were no significant code discrepancies between coders. Then, similar codes are grouped into themes. Identified themes presented with detailed description and results discussed. An inductive analysis approach was used. For the trustworthiness of the data, the interview guide was translated from English to Amharic and back to English, and the interview was performed by using the Amharic version. Type notes were taken throughout the interview for cross-validation with the audio recordings. Peer debriefing was used, colleagues reviewed the transcribed document and extracted concepts. All field notes, recorded interviews, and transcripts were checked each day for errors, and a correction was made. The audio record and typed notes were transcribed verbatim and translated carefully.
Result
Socio-Demographic Characteristics
The age of the participant ranges from 27 to 40 years. Participants’ educational status was from literate to degree level. More than half of them were completed secondary school and above. Regarding to religion, the majority of the participant were Orthodox and Muslim followers. Concerning employment status, participants were mixed from a government employee, private employee, and daily laborer. Duration of diagnosis as discordant during the study time was from one year to five years. The monthly family income ranges between 1500–5000 Ethiopian birr, which is grouped under the low level to medium level income category (Table 1. Socio-demographic characteristics of sero-negative discordant male partners living with HIV-positive women in Addis Ababa, Ethiopia, 2019).
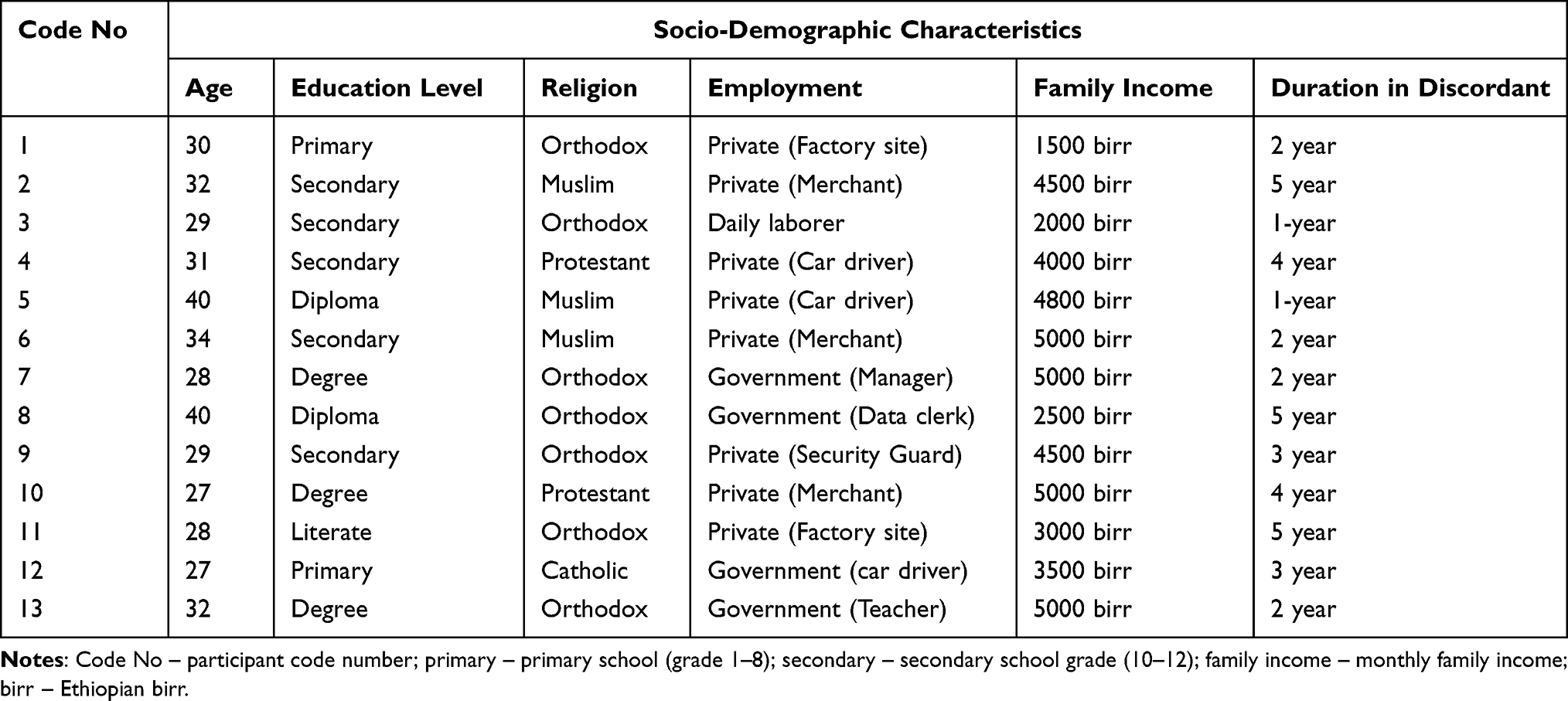 |
Table 1 Socio-Demographic Characteristics of Sero-Negative Discordant Male Partners Living with HIV-Positive Women in Addis Ababa, Ethiopia, 2019 |
Themes
Important concepts identified and organized into codes; then conceptually similar codes further organized into three themes. Theme I: understanding discordancy, theme II: challenges faced, and Theme III: risk reduction behaviors.
Theme I: Understanding Discordancy
Most of the participants explain discordant results as a new thing, uncertain of the description, and muddled by their discordant result. They also associated it with special natural immunity or blood type that can prevent HIV infection. As stated by (Participant-7);
I do not know about discordancy … and am really confused by the condition. I heard from other people that some blood types are resistant to HIV and this may be the reason, but I do not know the exact reason.
Some of the IIP (in-depth interview participant) reports that discordant result occurs due to the resistance of the negative partner. Some participants considered themselves as the carrier of the virus and perceive as the virus will express itself in the future. Due to this, they stated as they get into trouble to accept the result and end up with a denial of the test result. As stated by (Participant-1)
The doctor told me as I am free from the virus. But I can’t express myself as HIV negative and I believe the virus has been concealed inside my blood since we married two years ago and we have had free sexual intercourse….
Others also associated discordancy results with a religious explanation. It is explained as the miracle of God or the will of God.
I believe that we humans are the creature of God, and the entire world is under the control of God. So, if God loves me or wants to save me from the virus… he can;
statement from (participant-4). Only one participant gave a scientific explanation. Describe discordancy condition related to viral load, direct blood contact, presence of sexually transmitted infection, and other lesions in the genital area.Theme II: Challenges They Faced
It is usual that HIV-positive partners faced different psychosocial and economic challenges. But this life suffering is not limited to sero-positive partners. All of the participants report various challenges they faced because of their discordancy results.
Partner Behavioral or Mood Change
The majority of participants report that their seropositive partners develop irritable behavior and mood fluctuation. This situation gets worse in the first half-year of discordancy result. Participants get confusion and experience the same behavior. Subsequently, they suffer mood changes and show misbehavior within the family.
More than the event, I suffer more by her behavioral change. Most of the time she has become in a silent mood… and sometimes she showed irritable behavior to the family. I told her to ignore the issue and to live as before, but she has no interest… this condition also affects my behavior
as reflected by (participant-9).
Participants Felt Confused Due to Lack of Support System
The majority of the participants complain that there was no special support system, even if ART and PMTCT clinics are open in health institutions. Participants felt confused by the event. Discordant partners speech as they need a special support system to get clear information since they are full of a dilemma but health workers give more attention to index partners than sero-negative partners. Saying from (participant-12);
I am still confused. There is no support system for us. I need clear information since I necessity more children, but the health worker can’t tell me the exact time. They simply told me to use a condom and to have a checkup every three months. However, I want a method that can avoid my stress and support me to live the same as before.
Participants cannot get clear information about the risk of transmission, the desire of a child, and sexual life, even from health professionals. Health professionals simply teach condom use and the time of the next checkup.
Maintain Marital Relationship
All of the study participants report that maintaining a marital relationship was the major challenge faced. After the couple knew their status, almost all sero-negative male partners pass through the dilemmatic situation to decide on future life, to maintain the relationship, or to divorce. Life becomes a hardship, especially in the first few months of knowing their discordant result. But eventually, they struggle to cope and ignore the situation. As stated by respondents:
I faced a hard time to decide on our marriage, to live together or to divorce with my HIV positive wife. Especially, it was difficult in the first six months of our discordancy time,
(Participant-7). Fear of HIV transmission, loss of trust, and desire for children were reasons for initiation to divorce. On the other way, love from a partner, marital promise, and considering a child’s life were reasons that positively influence maintaining the relationship.Desire for Child
Desire for children and thinking about the health of children was the other challenge that discordant couples confronted.
The very sensitive issue is to have or not to have a child. Sometimes I decide to have a child with the help of God, but I become restless when I think about the health of my child. Our child may scarify by our luck. (Participant-1)
Couples who have no child plan to have a child for the continuation of their race and couples who have only one child want to have one or two more children. The pressure of desire of child also came from the family and society. The dilemma is the risk of HIV transmission during free sexual intercourse. On the other way, the major cause of headaches and stress is thinking about the risk of HIV transmission to the child.
I am now 40 years old; it is enough for me… and I don’t care about myself. I feel stress and headache when I think about the health of my child. Never, I can’t see when my child is HIV positive, and I prefer my death;
(participant −5). Participants also complain since they cannot get clear information about the best time to have a child, even from health professionals.Psychosocial and Economic Challenge
Psychosocial challenges were other critical issues related to discordancy status. As reported by participants, fear of stigma and social isolation is the major factor that affects their life. Since the community is networked with many social lives, it is difficult to live out of this culture. So, they try to hold their status as secret as possible even from their child. As evidenced by (participant-2);
Yes, I scarify depression and stress for a long time associated with the situation. I didn’t imagine such an event in my life, but it happens. You know our culture and society… how I can live with… if I disclosed to the nearby society. It is a headache to think about it. You are the second next to health workers knows my case.
They experience depression and stress associated with their discordancy result. They confront life hardship especially in the first few months of knowing their status. As reported, thinking about the risk of transmission, fertility desire, child health, fear of social isolation, and behavioral change of positive partner leads them into depression and stress. All sero-negative partners experienced hopelessness, negligence, and loss of self-confidence.
I feel as I am unlucky in my life. I became hopeless and careless in my life. I am not happy in all my life. I simply live for only my child. I have three children, one male, and two female. (participant-8)
Some participants also encounter economic burdens in relation to their discordancy status. HIV-positive partners need improved nutrients to enhance their immunity level, this increases family expenditure. Couple productivity and the family monthly income decreased due to different reasons. So, sero-negative partners faced economic challenges related to child school fees, house rent, and family expenditure. Speech from (Partner-11);
Thanks to God we live better till now… however, the family depends on my income. Because my wife stopped her regular job when she went to the monastery to use holy water. It is hard to continue in this way….
Sexual Life
Most sero-negative partners had decreased sexual initiation because of their psychological trauma, loss of happiness, and loss of love to their wives. They lose trust and love for their wife since they consider as their wife lacks honesty. The behavioral change and mood fluctuation also affect the sexual interest of the male partner.
It is not easy to think about the event. Sometimes I feel bad as I lose something in my life. I lost trust and love in my wife after I knew our discordancy result. I do not know the reason… my sexual desire is not the same as before. (Participant-1)
Some of the participants report as they continue as usual in a normal sexual relationship. Surprisingly, one partner reports, they live together without a sexual relationship simply to help each other and to grow the child. This is due to fear of HIV transmission and loss of interest.
We have no sexual contact after we knew our discordant result. We live together simply to help each other and to care for the child. I have no moral for such thing and I am really disappointed…. (Participant-8)
Theme III: Risk Reduction Behaviors
In this study, risk reduction behaviors like condom use, safe sex practice, avoiding blood contact, personalized use of sharp materials, partner support for proper use of ART drug, preventing STI, substance use, and continuous checkup or follow-up were explored. Unexpectedly, most of the respondents were not exercise HIV transmission risk reduction measures. Only a few participants report consistent or inconsistent condom use. Participants mentioned that positive partner influence, health workers’ advice, and fear of HIV transmission were the major reason for condom use. However, most of the participants were not interested or do not use condom totally during their sexual relationship.
I use condom inconsistently. Sometimes we have sexual intercourse without a condom. This is mainly because of condom absenteeism in our home when we are ready for sexual intercourse. Moreover, I feel hopeless and most of my life is unplanned. (Participant-10)
Male partners are usually reluctant to use a condom even the woman tries to negotiate. Majority of the participant associated condom use with religious thought and cultural norms. They report as condom is not allowed in their religion and culture. They believe in the power or will of GOD and become ignorant to use a condom.
I never used a condom. She is my wife, if God keeps me, the condom is not above God. The doctor advises me to use a condom but I am not happy to use it. I discussed with my wife to give all our life for Jesus Christ;
(Participant-7). The desire of a child, absence of a condom at hand during sex, feeling of sloppiness, and hopelessness were other reasons reported by the participant to avoid condom use.Misconception about the risk of transmission was explored by the respondents. Some of the participants believe as they are naturally resistant to the virus. Others simply consider themselves as the career of the virus. (Participant-7) stated as;
we had married two years ago, and we never used a condom but I am still free from the virus. I heard from other people that some blood types are resistant to HIV and this may the reason, but I do not know the exact reason.
Most of the respondents were not substance dependent. Substance dependency, contextually explored by interviewing the obligatory frequent and high dose use of substances, and history associated with intoxication problems in the use of substances like alcohol, chat, and smoking cigarette. Some of them use alcohol and/or chat during holidays and special days. Some of the participants report alcohol use to be free from stress when they encountered stress. Nevertheless, they have no idea, how substance use increases the risk of seroconversion.
I have no substance dependency, but sometimes I drink alcohol. I used alcohol to avoid stress in my life when I become full of stress. I have no information about the relationship between substance use and HIV transmission. I do not remember any event that the alcohol intoxication disturbs my sexual life…. (Participant-9)
Most of sero-negative partners did not continue with their follow-up. Respondents report that the follow-up has no significant importance to their life. Lack of a special support system was also mentioned as one factor to discontinue their follow-up. When the research team trace participants together with ART and PMTCT clinicians, most of them had no follow-up after the first visit. The important thing explored as good practice in the risk reduction behavior were personalized use of sharp materials, avoiding blood contact, and support of positive partner for proper use of ART drugs. As explored from the interview, still their intention and focus are the health of their child and partners than themselves. Moreover, they have no clear information about safe sex practice and prevention techniques of STI. Evidence from (participant-3); “Yes, I heard about sexually transmitted infection … I know as it causes infection in the genital area, but I don’t know how I can prevent it”. Speaks from (participant-13); “It is difficult to answer your question. I have no idea about safe sex practice … I am not sure how can apply it”.
Discussion
This study explored the lived experience and risk reduction behaviors of male sero-negative partners who lived with HIV-positive women. Besides index partners, sero-negative partners should get attention to support their life, clear dilemmas, reduce divorce, and reduce the risk of HIV transmission. Even though the existence of HIV passes a few decades, the scientific explanation of discordancy status is not still well established among discordant couples. Discordant partners were confused by their discordant result. It is misunderstood and associated with religious belief, naturally resistant immunity, and the hidden career of the virus. This is also evidenced by a study done in Uganda.16 Understanding, the scientific explanation aids to apply risk reduction measures.
It is usual that seronegative partners are understood as they can live a healthy life. However, as explored from the participants, discordant partners faced several dilemmatic lives or challenges. The desire for a child, maintaining a marital relationship, fear of social isolation and stigma, loss of trust, and love to the wife were explored factors related to psychosocial challenges. This finding is also supported by other studies.17–19 Likewise, positive partner behavioral or mood change and lack of support system were among the challenges that affect the behavior and emotion of the participants. It is associated with aggravating factors like poor counseling, the desire for a child, fear of transmission to the family, and hopelessness. Research reports also showed that men are more affected by depression than women.20 In the Ethiopian context, the majority of family income is expected from male partners besides partners’ HIV stage.21 Being discordant intensifies the economic burden of male partners together with loss of hope and extra demand related to partner HIV infection. The economic burden is another headache of discordant couples.7 Loss of sexual interest was the other challenge that discordant partners encountered. Even most did not know the exact reason; loss of trust, disappointment by the event, fear of transmission, and partners’ mood change were reported as the major cause.11 Deciding to maintain a marital relationship or to divorce is the immediate mind conflict in a discordant couple. In Ethiopia, research reports showed that most discordant couples end up with divorce and only a few couples maintain their relationship. Most of the time, the initiative of divorce comes from sero-negative male partners.12 All the above-explored life challenges should alert stakeholders as sero-negative partners felt confused and should have a special support system.
Related to risk reduction behaviors, sero-negative male partners’ lived experience showed that HIV transmission risk reduction methods were not well-practiced. Misconception and ignorance about discordancy results make them reluctant to take protective measures. Some consider as they are naturally resistant to the virus. Others ignore the issue and want to live by the will of God. They ignore condom use associated with their religious belief, cultural value, and misconception. A similar study also reported that misconception and fertility desire hinder condom use.8 Almost all participants did not exercise safe sex practice and did not apply STI prevention method and even they have no clear information about it. However, unsafe sex practices and the presence of STIs increase the risk of seroconversion.22–24
Participants report wonderful experiences in the use of personalized sharp material to avoid blood contact even if their caution is the health of children than themselves. Participants also showed optimistic support towards partners’ ART use. However, this effort was for the health of partners, not understanding its advantage in the reduction of the risk of seroconversion. Evidence showed that early initiation and proper use of ART minimize the risk of virus transmission in discordant couples.5,25 Accessing sero- negative male partners was tough during the study since most of the seronegative partners had no follow-up. Most of the participants also have no continuous follow-up and checkups after the first visit. Lack of interest, not understanding the advantage or misconception, and lack of a special support system were reasons to miss their follow-up. However, being ignorant is risky for the family, the community, and for themselves as well. WHO recommended regular follow-up and couple-based approach treatment for discordant couples.6
Limitation of the Study
- Participants were only male partners since participants accessed better via PMTCT clinics. Because most of the discordant diagnoses occur in the PMTCT unit since partner HIV tests offer during antenatal care.
- The study did not include the rural area as a result educational level, access to information, and way of life may show substantial variation.
Conclusion and Recommendation
Sero-negative partners need special attention equally as HIV-positive partners in couples with a discordant result. In discordant couples, life suffering is not limited to HIV-positive partners, rather seronegative partners also faced several challenges and dilemmatic life. HIV transmission risk reduction behavior is not well established and poorly understood by discordant couples. Therefore, a special psychosocial support system and continuous follow-up should be one of the strategies to support non-index partners. Health education and counseling session should include seronegative partners addressing risk reduction behavior and misconceptions parallelly with general life support. The health worker should have a clear discussion and counseling session with a couple on the issue of fertility desire.
Ethical Consideration
The proposal was submitted to Addis Ababa University, College of health science. The ethical review board approved and gave ethical clearance in reference to institutional review number /IRB of 047/19/SNM. Informed consent was taken after provision of all necessary information, asking willingness to participate in the study, and getting permission for audio recording. The participant’s informed consent also encompassed the publication of anonymized responses. Before conducting the interview, confidentiality, anonymity, voluntary participation, and freedom to withdraw from the study were assured. The information is taken from the participant accessed only by the research team. It was locked with a password and placed in a private computer. The coding system was used to maintain confidentiality and anonymity. The investigators assure that the audio recorded should be used secretly and will be deleted after transcription and translation. We authors approve that this study was conducted in accordance with the declaration of Helsinki.
Acknowledgment
The authors thankfully acknowledge Addis Ababa University, College of health science, school of Nursing, and Midwifery for offering such an opportunity to undertake this study. We would like to express our heartfelt gratitude Addis Ababa health bureau for its cooperation in the success of this study. We are also grateful to all clinicians working on the ART adherence office, PMTCT clinic, and ART Clinic of selected health institutions for their support. Finally, we have honor and appreciation for study participants for their kind participation.
Author Contributions
All authors made significant contributions to this paper and they fulfill the criteria of authorship based on your guideline. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. They took part in drafting the article or revising it critically for important intellectual content and agreed to submit it to the current journal. Gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Funding
Addis Ababa University was the funder of the study. The funder had no role in the study design, data collection, analysis, interpretation of data, the decision to publish, and preparation of the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Awad SF, Chemaitelly H, Abu-Raddad LJ. Estimating the annual risk of HIV transmission within HIV sero-discordant couples in sub-Saharan Africa. Int J Infect Dis. 2018;66:131–134. doi:10.1016/j.ijid.2017.10.022
2. Mehra B, Bhalla P, Rawat D, Kishore J. A study of HIV-concordant and -discordant couples attending voluntary counselling and testing services at a tertiary care center in North India. Indian J Public Health. 2015;59(4):306–309. doi:10.4103/0019-557X.169664
3. Eyawo O, de Walque D, Ford N, Gakii G, Lester RT, Mills EJ. HIV status in discordant couples in sub-Saharan Africa: a systematic review and meta-analysis. Lancet Infect Dis. 2010;10(11):770–777. doi:10.1016/S1473-3099(10)70189-4
4. Koye DN, Zeleke BM. Mother-to-child transmission of HIV and its predictors among HIV-exposed infants at a PMTCT clinic in northwest Ethiopia. BMC Public Health. 2013;13:398. doi:10.1186/1471-2458-13-398
5. Curran K, Baeten JM, Coates TJ, Kurth A, Mugo NR, Celum C. HIV-1 prevention for HIV-1 serodiscordant couples. Curr HIV/AIDS Rep. 2012;9(2):160–170. doi:10.1007/s11904-012-0114-z
6. World Health Organization. World Health Organization: guidance on couple HIV testing and counseling, including antiretroviral therapy for treatment and prevention in serodiscordant couples, recommendations for a public health approach; April 2012.
7. Nega Jibat M, Berihanu Nigussie M, Selamawit Tesfaye M. Original article socioeconomic challenges and coping mechanisms of HIV serodiscordant couples in Jimma Town, Oromia/Ethiopia. Eur Sci J. 2014;10(23).
8. Ngure K, Mugo N, Celum C, et al. A qualitative study of barriers to consistent condom use among HIV-1 serodiscordant couples in Kenya. AIDS Care. 2012;24(4):509–516. doi:10.1080/09540121.2011.613911
9. Jones D, Kashy D, Chitalu N, et al. Risk reduction among HIV-seroconcordant and-discordant couples: the Zambia NOW2 intervention. AIDS Patient Care STDS. 2014;28(8):433–441. doi:10.1089/apc.2014.0039
10. Subramoney R. The lived experiences of Indian women with HIV/AIDS in South Africa: a phenomenological inquiry. Int J Health Sci. 2015;3(2):61–121.
11. Mwakalapuka A, Mwampagatwa I, Bali T, Mwashambwa M, Kibusi S, Mwansisya T. Emotional and relationship dynamics between HIV serodiscordance and concordance couples: a narrative literature review and theoretical framework. ARC J Public Health Community Med. 2017;2(2):1.
12. Porter L, Hao L, Bishai D, et al. HIV status and union dissolution in sub-Saharan Africa: the case of Rakai, Uganda. Demography. 2004;41(3):465–482. doi:10.1353/dem.2004.0025
13. Mashaphu S, Burns JK, Wyatt GE, Vawda NB. Psychosocial and behavioural interventions towards HIV risk reduction for serodiscordant couples in Africa: a systematic review. S Afr J Psychiatr. 2018;24:1136. doi:10.4102/sajpsychiatry.v24i0.1136
14. Aynie M. Land use land cover change in Addis Ababa since 2003, 2011 and 2018 in case of Addis Ketema sub city kebele 04&05. Addis Ababa; 2019.
15. Kibret GD, Ferede A, Leshargie CT, Wagnew F, Ketema DB, Alebel A. Trends and spatial distributions of HIV prevalence in Ethiopia. Infect Dis Poverty. 2019;8(1):90. doi:10.1186/s40249-019-0594-9
16. Bunnell R, Nassozi J, Marum E, et al. Living with discordance: knowledge, challenges, and prevention strategies of HIV-discordant couples in Uganda. AIDS Care. 2005;17(8):999–1012. doi:10.1080/09540120500100718
17. Hailemariam TG, Kassie GM, Sisay MM. Sexual life and fertility desire in long-term HIV serodiscordant couples in Addis Ababa, Ethiopia: a grounded theory study. Biomedical. 2012;12:1–12.
18. Paulos M. Couples with different HIV status: understanding the experience of sero-discordant married couples in Addis Ababa; 2011.
19. Beyeza-Kashesya J, Kaharuza F, Mirembe F, Neema S, Ekstrom AM, Kulane A. The dilemma of safe sex and having children: challenges facing HIV sero-discordant couples in Uganda. Afr Health Sci. 2009;9(1):2–12.
20. Cherayi S. Life of discordant couples living with HIV in Puducherry, India: psychological distress and coping strategies. Life. 2013;1. Available from: https://www.iiste.org/Journals/index.php/JHMN/article/view/9191. Accessed March 17, 2022
21. United Nations Women. Preliminary gender profile of Ethiopia. Addis Ababa, Ethiopia; 2014.
22. Wall KM, Kilembe W, Vwalika B, et al. Risk of heterosexual HIV transmission attributable to sexually transmitted infections and non-specific genital inflammation in Zambian discordant couples, 1994–2012. Int J Epidemiol. 2017;46(5):1593–1606. doi:10.1093/ije/dyx045
23. Ruzagira E, Wandiembe S, Abaasa A, et al. HIV incidence and risk factors for acquisition in HIV discordant couples in Masaka, Uganda: an HIV vaccine preparedness study. PLoS One. 2011;6(8):e24037. doi:10.1371/journal.pone.0024037
24. Getachew T. A Struggle to Maintain Relationship” - Sexual Life and Fertility Desire in Long-term HIV Sero-discordant Couples: a Grounded Theory Study [doctoral dissertation]. Addis Ababa University; 2011.
25. Baggaley RF, White RG, Hollingsworth TD, Boily MC. Heterosexual HIV-1 infectiousness and antiretroviral use: systematic review of prospective studies of discordant couples. Epidemiology. 2013;24(1):110–121. doi:10.1097/EDE.0b013e318276cad7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.