Back to Journals » Infection and Drug Resistance » Volume 14
Listeria Species Occurrence and Associated Factors and Antibiogram of Listeria monocytogenes in Beef at Abattoirs, Butchers, and Restaurants in Ambo and Holeta in Ethiopia
Authors Gebremedhin EZ ![]() , Hirpa G, Borana BM, Sarba EJ, Marami LM
, Hirpa G, Borana BM, Sarba EJ, Marami LM ![]() , Kelbesa KA, Tadese ND
, Kelbesa KA, Tadese ND ![]() , Ambecha HA
, Ambecha HA
Received 2 February 2021
Accepted for publication 31 March 2021
Published 19 April 2021 Volume 2021:14 Pages 1493—1504
DOI https://doi.org/10.2147/IDR.S304871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Endrias Zewdu Gebremedhin,1 Gadisa Hirpa,2 Bizunesh Mideksa Borana,1 Edilu Jorga Sarba,1 Lencho Megersa Marami,3 Kebede Abdisa Kelbesa,1 Nega Desalegn Tadese,3 Hirut Abebe Ambecha3
1Department of Veterinary Sciences, College of Agriculture and Veterinary Science, Ambo University, Ambo, Ethiopia; 2Department of Biology, Ambo Preparatory School, Ambo, Ethiopia; 3Department of Veterinary Laboratory Technology, College of Agriculture and Veterinary Science, Ambo University, Ambo, Ethiopia
Correspondence: Endrias Zewdu Gebremedhin
Ambo University, P.O. Box 19, Ambo, Ethiopia
Tel +251 911894802
Fax +251 112609503
Email [email protected]
Purpose: Listeriosis is one of the globally distributed foodborne diseases with the highest fatality rate. The objectives of this study were to isolate and identify Listeria species, assess factors for contamination of beef, and antibiogram of Listeria monocytogenes in Ambo and Holeta towns, Central Ethiopia.
Materials and Methods: A total of 450 meat samples were collected from abattoirs (n=150), butchers (n=150), and restaurants (n=150) for isolation and identification of Listeria species. Logistic regression analysis was used to assess the association between the occurrence of Listeria species in meat and potential risk factors. The antimicrobial susceptibility test was done using the Kirby Bauer test.
Results: The overall occurrence of Listeria species in Ambo and Holeta towns was 28.4% (128/450; 95% confidence interval [CI]: 24.3– 32.9%). The isolation rate of Listeria monocytogenes was 4.4%, Listeria ivanovii 2.2%, Listeria seeligeri 1.8%, Listeria welshimeri 3.8%, Listeria innocua 6.2%, and Listeria grayi 10.2%. The probability of contamination of meat in butchers and restaurants was higher in Holeta than Ambo [OR=3.4; 95%; p=0.001], in dry than wet season [OR=5.2; p=0.009], and where the hygiene of cutting boards was poor (OR=7.7; p=0.008). Of the 20 Listeria monocytogenes isolates, 80%, 70%, 60%, and 55% were resistant to oxacillin, amikacin, and nalidixic acid, chloramphenicol, and tetracycline, respectively. The Listeria monocytogenes isolates were 95%, 90%, and 85% susceptible to amoxicillin, vancomycin, and clindamycin, respectively. About 95% of Listeria monocytogenes isolates were multidrug-resistant. One isolate (5%) had developed resistance to 10 classes of antimicrobial drugs.
Conclusion: Listeria species are widespread and study towns, season, and hygiene of cutting boards are independent predictors of isolation of Listeria species. Multidrug resistance among Listeria monocytogenes was very high. Therefore, adequate cooking of meat, regular training of beef handlers, prudent use of drugs, and further molecular studies on Listeria species are important.
Keywords: antimicrobial susceptibility, beef, Listeria species, Listeria monocytogenes, multidrug resistance, risk factors, Ethiopia
Introduction
Consumption of raw meat contaminated with pathogenic Listeria species causes foodborne listeriosis.1–3 Foodborne listeriosis is one of the important diseases affecting human health globally related to increasing global trade and travel.2,4,5 Foodborne listeriosis is a sporadic disease epidemiologically associated with the ingestion of contaminated food products.6 Listeriosis causes a spectrum of diseases ranging from milk and self-limiting diseases in healthy people to severe, systemic, and life-threatening infections in susceptible populations such as HIV patients, pregnant women, neonates, people with malignancy, and the elderly.6,7
Based on the phenotypic and genotypic characteristic similarities and differences, Listeria species are grouped into “Listeria sensu lato” and “Listeria sensu strictu”.8,9 Listeria sensu strictu is composed of L. monocytogenes, L. innocua, L. seelgerii, L. welshimeri, and L. marthii. All Listeria sensu strictu are catalase-positive, motile at least at 30°C, and grow below or at 4°C and gram-positive. Listeria sensu lato is composed of 11 species comprising L. grayi as well as L. fleischmannii, L. floridensis, L. aquatica, L. newyorkensis, L. cornellensis, L. rocourtiae, L. weihenstephanensis, L. grandensis, L. riparia, and L. booriae.10 Listeria spp are abundant in nature and can survive diverse types of environmental stresses such as pH, temperature, and salt. Listeria monocytogenes is the main causes of human listeriosis, which is a serious health problem,11 because of severe symptoms and high mortality approximately 20%. Nowadays, other species of Listeria are also known to produce a disease in humans and animals.6,12
Risk factors for food contamination are identified as all factors essential for food contamination/emergence of foodborne infections.13 Contamination of meat by microorganisms occurs in an abattoir during slaughtering and spread from the intestinal tract and the exterior part of animals. Besides, air, workers, knives, clothes, carts, and refrigerators14 may also contaminate meat. Poor food handling and sanitation practices, inadequate food safety laws, weak regulatory systems, lack of financial resources, improper storage, poor personal hygiene during preparation, extended shelf-lives refrigeration, inadequate cooling and reheating create a favorable condition for the spread of foodborne etiologic agents.4,15,16 Socio-demographic factors, worker’s food safety, and hygiene information, knowledge on food safety and hygiene, food safety principles and practices, food source, and others are a few of the food contamination predictors.13
The increased use of antimicrobial agents in food animal production and humans is a significant factor in the emergence of antimicrobial-resistant bacteria. The repetitive use of antimicrobials in food animal production for treatment and as growth promotion is a significant factor for the emergence of multi drugs resistant strains.2,5 Meat is a major source of transmission of antimicrobial-resistant microorganisms to humans.17 As a result, control and treatment of listeriosis are difficult and very hazardous without antimicrobial resistance interventions.18
There have been few studies conducted on the occurrence of Listeria species in food samples and meat sources including poultry, mutton, pork, seafood, and other foods of animal origins in Ethiopia.1,2,4,19,20 However, the occurrence, risk factors, and antibiogram of Listeria species in meat from abattoirs, butchers, and restaurants have not been sufficiently studied. Careful investigation of raw meat samples collected from the three spots of the beef chain (abattoir, butcher, and restaurant) will help to identify the weak links contributing to the contamination. This helps considerably for subsequent interventions in attempts to protect consumers from foodborne illnesses and to reduce economic losses due to food spoilage. Therefore, the objectives of the present study were to generate epidemiological data on occurrence and risk factors of Listeria species as well as the antibiogram of Listeria monocytogenes, isolated from raw beef in abattoirs, butchers, and restaurant of Ambo and Holeta towns of central Ethiopia.
Materials and Methods
Study Area
The research was performed in Ambo and Holeta towns of the Oromia region, central Ethiopia. Ambo town is the administrative center of West Shoa Zone located 114 km West of Addis Ababa at the latitude of 8°59′N 37°51′E and longitude of 8.983°N 37.85°E. The elevation of Ambo town ranges from 1900 to 2275 meters above sea level (m.a.s.l.). Its temperature ranges from 19°C to 29°C with an average annual temperature of 22°C and an average annual rainfall of about 900 mm. The town has a total human population of 74,843 out of which 39,192 are males, and 35,651 are females.21 There are 46 legal butchers with their annexed restaurants and one municipality abattoir in Ambo town.
Holeta is located in Finfine special zone, 44 Kms West of Addis Ababa with a latitude and longitude of 9°3ʹN38°30ʹE/9.050ʹN38.500°E. Its elevation is 2400 masl. It receives 1144 mm annual average precipitation, with an average minimum and maximum temperature of 6°C and 22°C, respectively. The total human population of Holeta town is 25,593, of whom 12,605 are men and 12,988 women.21 There are 20 legal butchers with annexed restaurants and one municipality abattoir in Holeta town.
Study Population
All abattoirs, butchers, restaurants in Ambo and Holeta towns constituted the targets of this study. Carcasses of cattle slaughtered in Ambo and Holeta abattoirs are the study subjects.
Study Design
A cross-sectional study was conducted between October 2017 to April 2018 in abattoirs, butchers, and restaurants of Ambo and Holeta towns, to determine the occurrence of the Listeria species, potential risk factors for meat contamination, and antimicrobial susceptibility profiles of the Listeria monocytogenes from raw beef sampled from three points (abattoir, butcher, and restaurant).
First, the list of all the current legal butchers, restaurants, and abattoirs registered in Ambo and Holeta towns was collected from the towns’ municipality (sampling frame) and then the two abattoirs (one from each town) and those butchers with an annexed restaurant for handling meat were purposively identified.
Sample Size Determination
The required sample size was determined using a 95% confidence limit and a 7% sampling error and an expected prevalence of 25% by Thrusfield22 formula. As a result, a sample size of 147 was calculated. However, 450 samples of meat, consisting of 150 from abattoirs, 150 from butchers, and 150 from restaurants, were sampled. Samples were obtained from all the 20 and 46 butchers in Holeta and Ambo towns, respectively. Eighty-seven samples from the town of Holeta (29 per establishment) and 363 samples from the town of Ambo (121 per establishment) were allocated.
Sample Collection
A systematic random sampling method was used to select animals from the study population. Following slaughtering, meat samples were collected from three spots, ie, Abattoir, butcher, and restaurant. First composite meat samples of about 250 gm were collected from slaughtered cattle from four sites (ramp, flank, brisket, and neck) just after the stage of evisceration. The same procedure was followed on the second sampling spot, ie, butcher house. On the third sampling spot, 250 g raw beef that is prepared to be served for consumption (Kitfo;- a traditional Ethiopian dish made from minced raw beef, chili, spice, and butter blend or Tire siga- cubes of meat cut served raw) was collected. All samples were collected aseptically and labeled with necessary information including the sample code, date of sampling, and sampling place (spot). Samples were kept in separate sterile plastic bags (Seward, England) and immediately transported to the Ambo University Veterinary Microbiology Laboratory in an icebox with ice packs. Samples were processed within 4 hrs of arrival at the laboratory.
During sample collection, demographic data from abattoir personnel, butcher shop workers and restaurant chefs, and waiters who were in charge were collected including the sex, marital status, the residence of origin, educational status, work experience in years, and time on work per day. Besides, an observation was made on the hygiene of the cutting boards, the weighing balance, food handling surfaces, and of butchers and restaurants as a whole. Hygienic variables were categorized as poor if there is gross dirt, undesirable smell, insects and as good if gross dirt, bad smell, and insects are absent.
Isolation and Identification of Listeria Species
For the isolation and identification of Listeria species, the method recommended by the International Standardization Organization (ISO)23 was followed. Accordingly, 25 g of sample was homogenized in 225 mL of Listeria enrichment broth (LEB) containing supplements (HiMedia, India) using a laboratory blender and incubated at 30°C for 24 hrs. Then after 0.1 mL of mixed inoculum was inoculated into a tube containing 10 mL Modified Fraser broth (MFB) and incubated for 24 hrs at 37°C. Following the enrichment procedure, the inoculum was streaked on Oxford agar (OXA) containing manufacturer’s supplements and the plates were incubated at 37°C for 24–48 hrs. After 24 hrs of incubation, the growth of Listeria species on the Oxford agar plate was examined for black halo colonies, which remain the same after 48 hrs of incubation but with a sunken center.
The presumptive colonies were picked up and further purified on Tryptone Soya Yeast Extract agar (TSYEA). Subsequently, pinpoint colonies on TSYEA were subjected to identification procedures, which included Gram’s staining followed by a microscopic examination, catalase test, and oxidase test. The characteristic Gram-positive, coccobacillus, or short rod-shaped organisms, which were catalase-positive and oxidase negative, were sub-cultured in Brain heart infusion (BHI) broth at 25°C for 12–18 hrs. Then, the cultures showing typical tumbling motility were considered as “presumptive” Listeria isolates, which were in turn subjected to detailed biochemical tests viz.; Christe, Atkins, and Munch-Peterson (CAMP) test, methyl red, Voges-Proskauer, and sugar fermentation tests with xylose, rhamnose, and mannitol for identification of Listeria to species level.
Antimicrobial Susceptibility Test
The L. monocytogenes isolates were subjected to an antimicrobial susceptibility test against 16 commercially available antimicrobial discs (Oxoid, UK) selected based on common usage. The antimicrobial discs selected were amikacin (30μg), amoxicillin (10μg), ampicillin (10μg), chloramphenicol (30μg), cefotaxime (30μg), gentamicin (10μg), tetracycline (30μg), oxacillin (1μg), vancomycin (10μg), cotrimoxazole (25μg), nalidixic acid (30μg), ciprofloxacin (5μg), erythromycin (15μg), clindamycin (2μg), penicillin (6μg), and trimethoprim-sulfamethoxazole (23.75μg). An antimicrobial susceptibility test was conducted using the disc diffusion method following the guidelines established by the Clinical and Laboratory Standards Institute (CLSI).24 Two to three pure fresh colonies of the isolates from TSAYE were used to prepare a cell suspension in the Mueller Hinton broth (HiMedia, India) and incubated for 24 hrs at 37°C. Following this, the cell suspension turbidity was attuned to equal 0.5 McFarland Standard. Then, a sterile cotton swab was used to spread the bacterial suspension on the Mueller Hinton agar (HiMedia, India). The discs were firmly placed in the interval of 3 cm spacing from each other onto the medium with sterile forceps and then incubated at 37°C for 24 hrs. Then, the diameter of clear zones around the discs was measured with a ruler against a black background and compared with standards given by CLSI.24 L. monocytogenes ATCC7644, E. coli ATCC25922, and S. aureus ATCC6538 reference strains were used as quality control.
Data Management and Analysis
The collected data were entered into Microsoft Excel spreadsheets (Microsoft Corporation) and analyzed using STATA version 14.2 software (Stata Crop. College Station, USA). Descriptive statistics was used to summarize the occurrence, socio-demographic characteristics of the respondents, and antimicrobial susceptibility data. Univariable and multivariable logistic regression analyses with their Odds Ratio (OR) and 95% confidence Intervals (95% CI) were used to determine potential risk factors associated with meat contamination by Listeria species. During risk factors analysis, for all of the risk factors, the first category of the independent variables (with the lowest prevalence) was considered as a reference category. Non-collinear variables that possessed a p-value of <0.25 in univariable analysis were entered into the multivariable analysis. The model was constructed by a backward exclusion method. Hosmer-Lemeshow goodness-of-fit test was used to assess the model fitness. The reliability of the fitted model was further evaluated using the receiver operating characteristics curve (ROC). The results were considered significant at p<0.05 at all levels of analysis.
Inclusion and Exclusion Criteria
Meats from cattle slaughtered and inspected in the abattoirs, displayed for sale in butcher shops, and used for meat dish preparation in restaurants were included in the study while the meats of other food animals, cattle meat that is not inspected, and cattle meat that is not utilized for raw meat dish preparation were excluded.
Results
Occurrence and Identification of Listeria Species
Out of the total 450 meat samples examined, 28.4% were positive for Listeria species. The occurrence of Listeria species in Ambo town (20.66%) was much lower when compared to Holeta town (60.9%). The highest Listeria species occurrence was recorded in restaurants (30.0%), followed by butchers (29.3%) and then abattoir (26.0%). Listeria species occurrence in abattoir and restaurant samples of Holeta town was relatively higher than similar samples of Ambo town (Table 1).
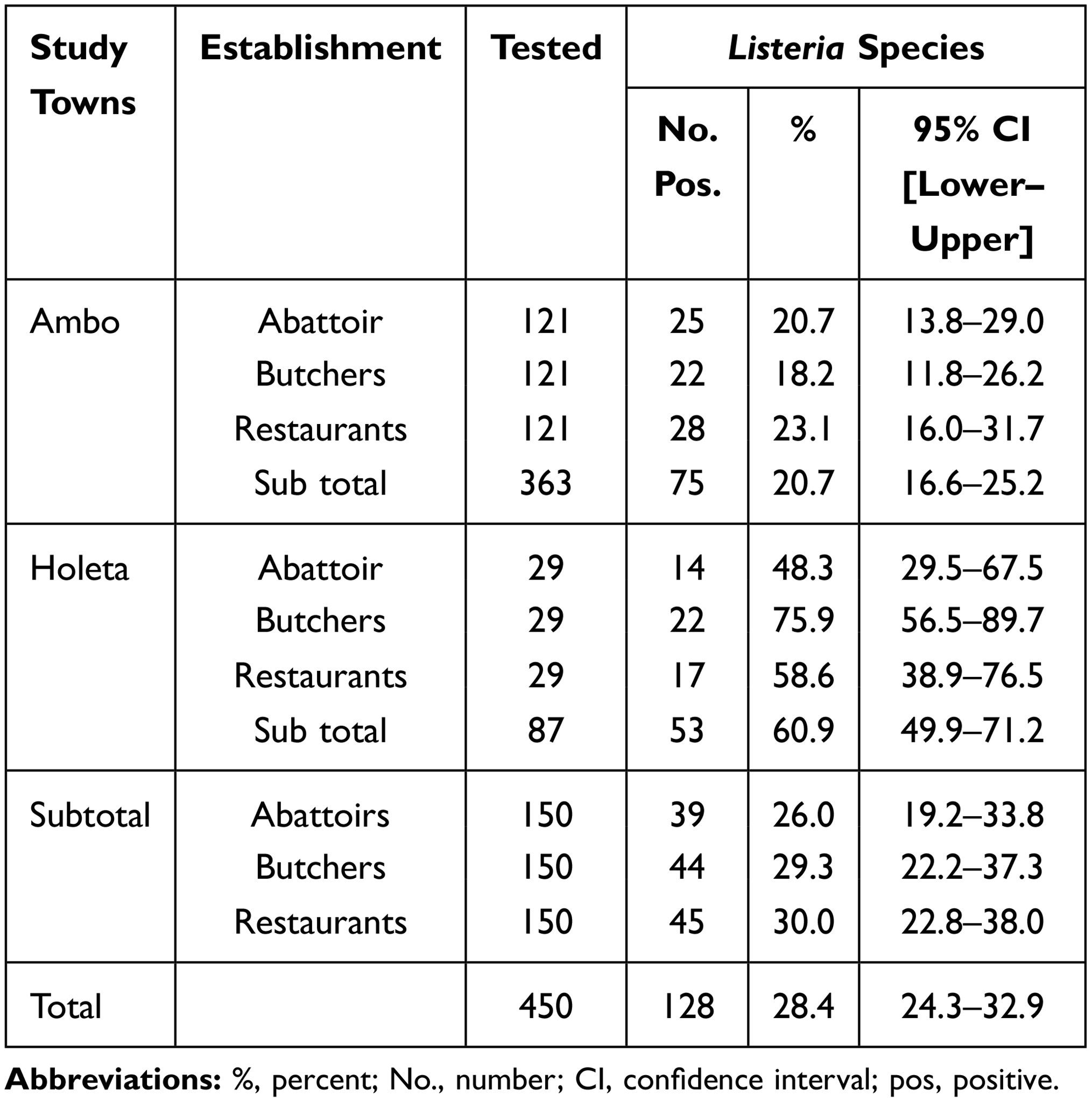 |
Table 1 The Occurrence of Listeria Species in Raw Beef from Abattoirs, Butchers, and Restaurants of Ambo and Holeta Towns of Central Ethiopia |
Out of the total 128 Listeria species isolated, Listeria grayi was the most frequent isolate while Listeria seeligeri was the least. The percentage of L. monocytogenes in abattoirs, butchers, and restaurants raw meat samples of cattle were 33%, 1.6%, and 1.6%, respectively (Table 2).
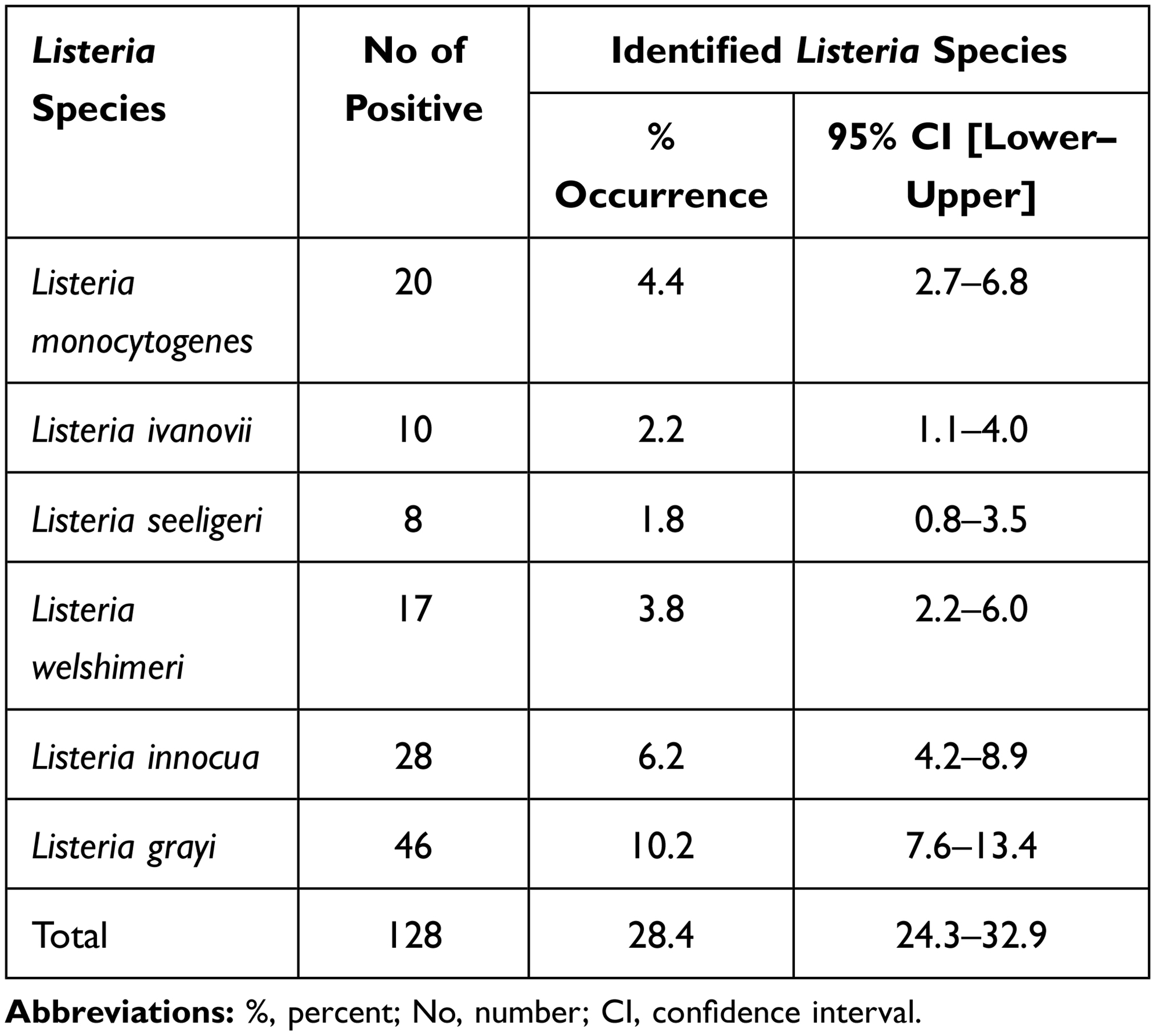 |
Table 2 Listeria Species Identified from Raw Beef in Ambo and Holeta Towns, Oromia, Central Ethiopia (n=450) |
Risk Factors
Socio-Demographic Characteristics, Knowledge, and Practice on Food Safety and Hygiene
The socio-demographic characteristics, knowledge, and practice on food safety and hygiene of respondents are depicted in Table 3.
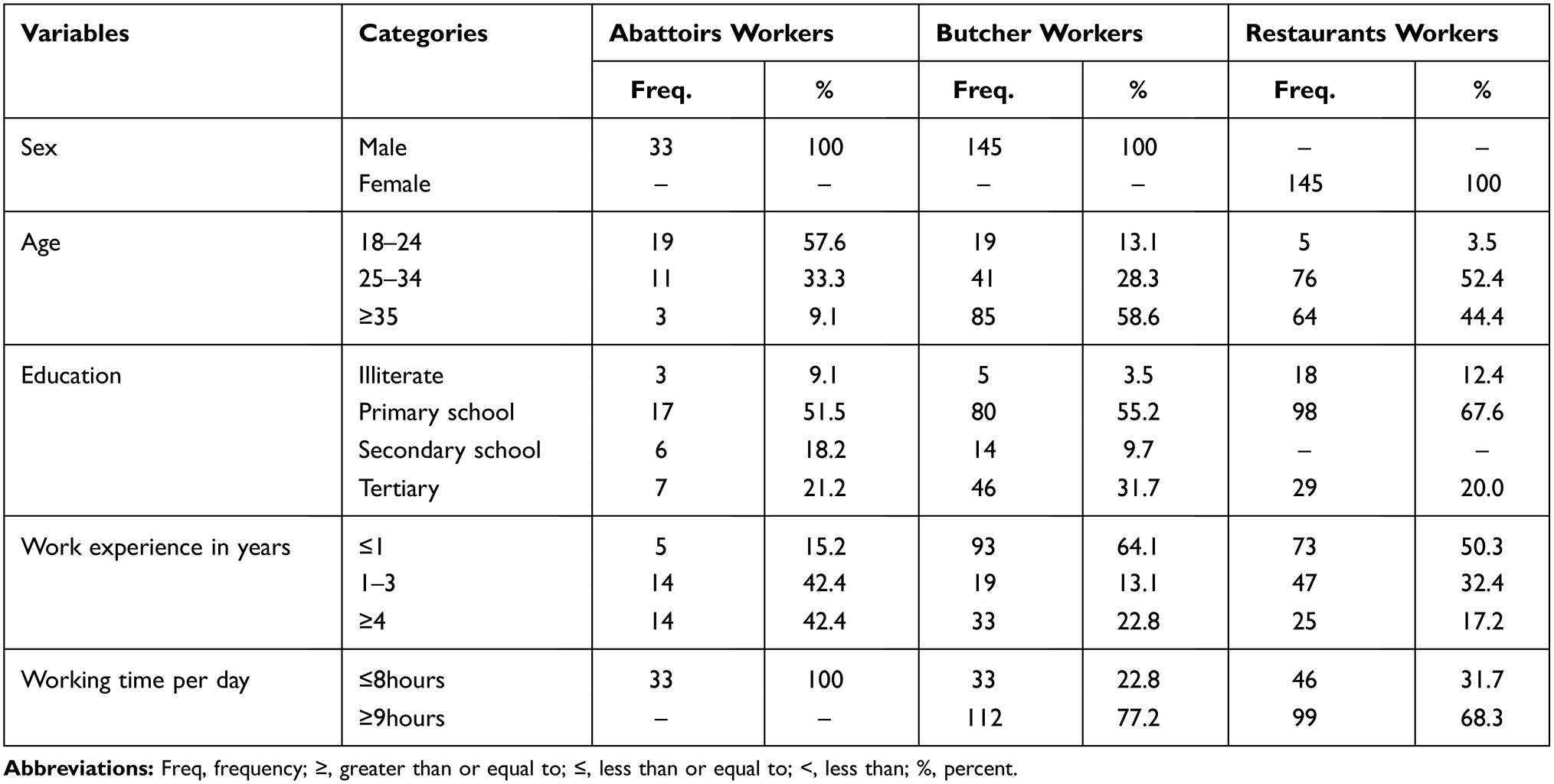 |
Table 3 Socio-Demographic Characteristics of Workers of Abattoirs, Butchers, and Restaurants of Ambo and Holeta Towns |
Logistic Regression Analyses
Univariable logistic regression analysis showed that the occurrence of Listeria species in raw beef was significantly different (p<0.001) between study towns, seasons, information on food hygiene and safety, working times per day, and hygiene of the cutting boards. All the remaining variables did not show a significant association with the risk of raw beef contamination (p>0.05). The risk of raw beef contamination was significantly higher in Holeta town than in Ambo town, in the dry season than wet season, and from butchers and restaurants in which employees working hours per day was ≥ 9 hours as compared to working hours of ≤8 per day (p<0.001) (Table 4).
 |
Table 4 Logistic Regression Analysis of Potential Risk Factors for Listeria Species Isolated from Raw Beef of Butchers and Restaurants in Ambo and Holeta Towns, Central Ethiopia |
Among the studied variables study towns, season, working time per day, hygiene of slicing materials, and hygiene of cutting boards fulfilled the criteria (p<0.25 and (r<0.5) and therefore have been incorporated into the multivariable model. Multivariable logistic regression analysis revealed that study town, season, and hygiene of the cutting boards were independent predictors of contamination of raw beef by Listeria species (p<0.05). Hygiene of the slicing materials (p=0.051), though not significantly associated, was close for association (Table 4). The full model had Hosmer-Lemeshow X2 =4.8, p=0.684, and assessment of model fitness to the observed data indicated that observed and predicted values were not significantly different, ie, the data fitted the model well. Moreover, the sensitivity (32.9%), specificity (92.3%), and receiver operating characteristics (ROC) analysis (0.789) suggest the data fitted the model well. The model had a positive predictive value of 62.8% and a negative predictive value of 77.7%.
Antimicrobial Susceptibility
The results of antimicrobial susceptibility testing of the 20 L. monocytogenesisolates is shown in Table 5.
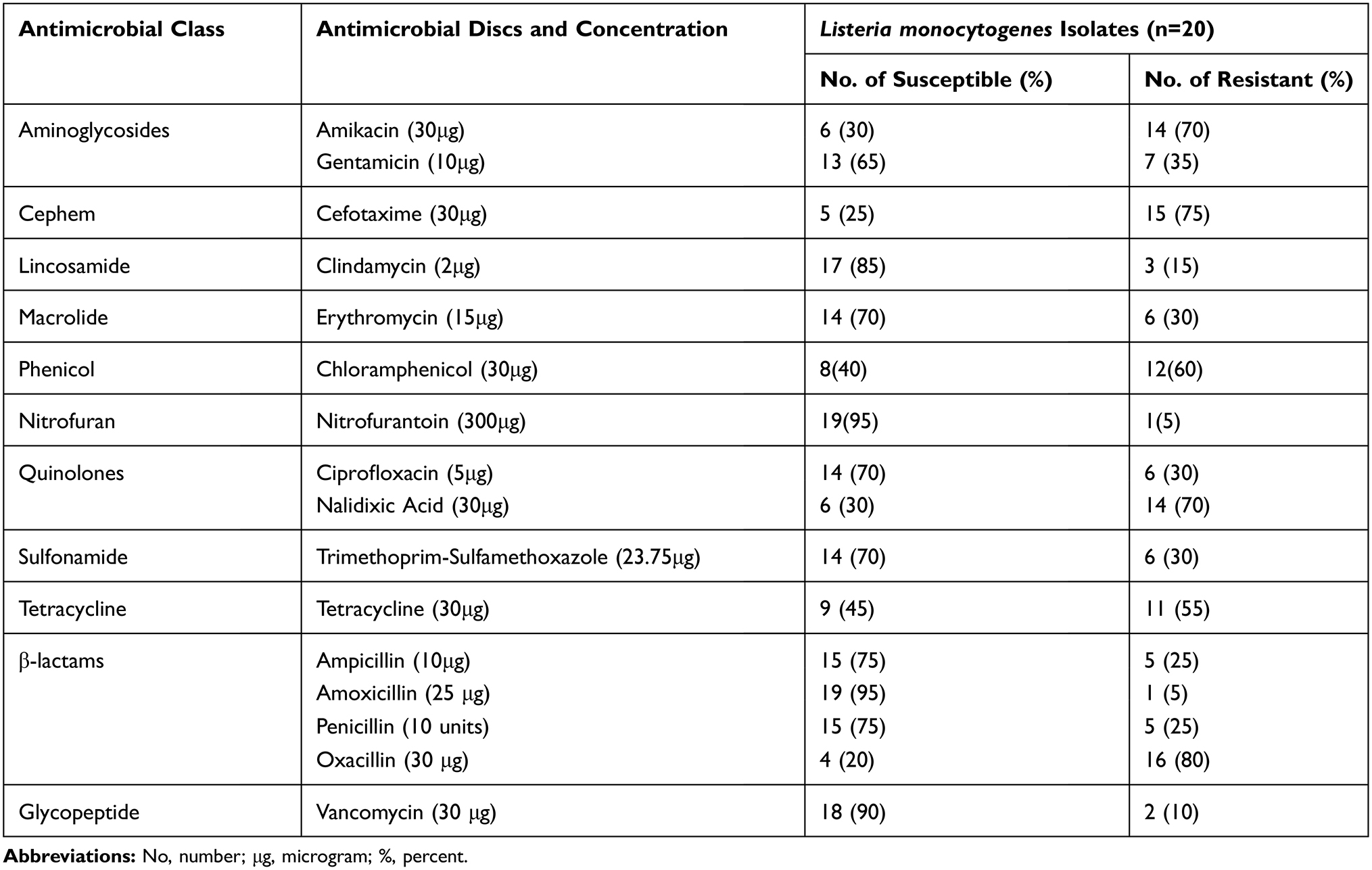 |
Table 5 Results of the Antibiogram of Listeria monocytogenes Isolates (n=20) from Raw Cattle Meat Samples of the Abattoirs, Butchers, and Restaurants |
All identified Listeria monocytogenes had developed resistance to two or more classes of antimicrobial drugs. Nineteen (95%) L. monocytogenes isolates were resistant to three or more classes of antimicrobials (multidrug resistance – MDR). One isolate (5%) had developed resistance to nine classes of antimicrobials. The most common MDR pattern was observed against amikacin, cefotaxime, nalidixic acid, and Oxacillin. The patterns of antimicrobial resistance of L. monocytogenes isolates were shown below (Table 6).
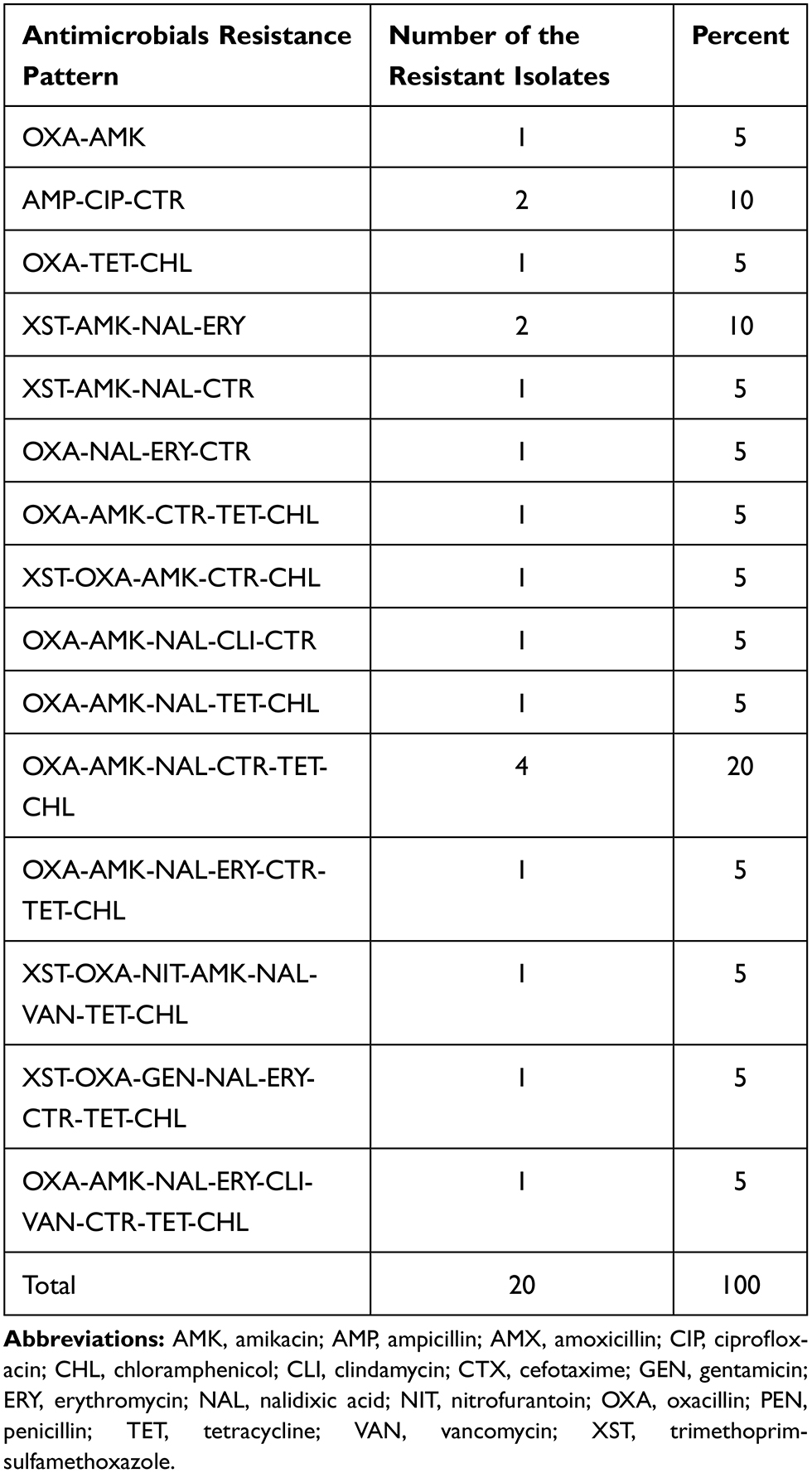 |
Table 6 Antimicrobial Resistance Patterns of Listeria monocytogenes (n=20) |
Discussion
Occurrence of Listeria Species in Raw Beef in Abattoirs, Butchers, and Restaurants
In the present study, an overall occurrence of Listeria species (28.4%) from samples of raw beef from abattoirs, butchers, and restaurants was in agreement with the reports from Addis Ababa (27.5%).1 Other studies have reported significantly higher isolation rates of Listeria species in raw meat such as 95% in Brazil,25 81.5%,26 and 54.1%27 in Turkey, 58% in Nigeria,28 51.3% in Ethiopia,20 and 50% in Jordan.29
The 4.4% isolation rate of L. monocytogenes in this study was comparable with the 4.1% from goat meat in Ethiopia4 and 4.1% in raw beef in Ethiopia.1 However, the current finding was higher when compared to 1.29% from raw cow and goat meats,30 1.6% from minced beef,19 and 2.5% from bovine carcasses in Poland31 and was lower when compared to the 15.6% in Nordic countries,32 15.4% in Bangkok,33 25.5% in Turkey.26 The relatively low percentage of L. monocytogenes (4.4%) in the present study may be attributed to the difference in study season, geographic conditions, and sample size.34,35
Meat can be contaminated by L. monocytogenes at abattoirs by cross-contamination during slaughtering, evisceration, and other processing steps. Additionally, contamination and growth of Listeria at the next chain (butchers and restaurants) could occur due to poor hygienic handling and processing, refrigeration; and the suitability of the meat pH, water activity, and nutrient content.36 The isolation rate of other Listeria species in the present study ranged from 1.8% - 10.2%. The 2.2% isolation rate of L. ivanovii in the present study is by far lower than the 21.9% reported by Al-Nabulsi et al16 and 19.8% by Alsheikh et al37 reported from various types of meat and meat products. However, the isolation rate of L. ivanovii in the present study is comparable to 2% reported from raw meat in Ethiopia.2 The 3.8% isolation rate of the L. welshimeri in this study is in agreement with the 2.8% from Jordan,16 and 4% from Ethiopia2 reported previously. The occurrence of L. seeligeri (1.8%) in the present study disagrees with the 27% reported from Amman, Jordan,16 however, it is in line with the 1% and 2% prevalence of L. seeligeri previously reported by Alsheikh et al37 and Garedew et al,2 respectively. The lower detection rate of L.ivanovii, L. welshimeri, and L. seeligeri in the present study might be linked to the hygienic status of food processing environments and the bacteriological detection method differences.2,37,38
Most research reports indicate that L. innocua is the most common species isolated from different meat samples. For example, in Ethiopia, 83% and 19% of L. innocua have been reported.1,2 In this study, L. grayi (10.22%) and L. innocua (6.2%) were more common than the other Listeria species. Few reports from meat samples showed that L. grayi was the second most abundant Listeria species next to L. ivanovii.16 The relatively high percentage of L. grayi (10.2%) and L. innocua (6.2%) in the current study was in line with the reports of from Ethiopia39 and might be related to the species entrance to the processing environments via as a part of intestinal microbial flora, improper hygienic practices during processing and food handling.40,41
Risk Factors Assessment
The occurrence of Listeria species in raw beef was nearly 5.2 times higher in the dry season (p=0.009) when compared to the wet season. The significantly high occurrence of Listeria species in cattle beef during the dry season might be due to the large sample size (more than 75% of the meat samples) in the dry season and the environmental stress in cattle during the dry season that led to the shedding of the organisms in feces. It is well known that a dry climate harms the persistence of Listeria species.42 Thus, drying is linked to water activity lowering of meat and meat products. As a consequence, the lowered moisture content of the meat enables the organism to persist in (resist) high temperature.43 In addition, the shortage of water during the dry season might impair the hygienic activities of personnel and equipment in the establishments thereby increasing the chance of contamination. The isolation of Listeria species from meat in both dry and wet seasons suggests the existence of natural reservoirs of the bacteria in cattle or the environment. On the other hand, univariable logistic regression showed a significantly high prevalence of Listeria species in butchers and restaurants where the employees work ≥9 hrs as compared to those working ≤8 hrs. This might be related to the change in the hygienic behavior of works as they get exhausted/tired while working ≥9 hrs/day.
In the current study, the place where the study was carried out was the predictor of Listeria species isolation (p=0.001). The significantly high recovery rate of Listeria species from Holeta (57.1%) as compared to Ambo (21.4%) town might be related to the cool temperate of Holeta town favorable for the survival and multiplication of the organisms.
Multivariable logistic regression analysis also identified the hygiene of the cutting boards (p=0.008) as a risk of raw beef contamination by Listeria species. This is in line with the findings of previous workers.44–46 The types or quality of cutting boards and the absence of frequent sanitation of the cutting boards, and the use of unclean water for washing cutting boards might be linked to a higher chance of cutting boards being contaminated with Listeria species.46
Antimicrobial Susceptibility Profile of the L. monocytogenes Isolates
The highest percentage of resistance was noted for oxacillin (75%) followed by 55–70% resistance to amikacin, nalidixic acid, tetracycline, and chloramphenicol. The 75% resistance of oxacillin in the present study is comparable with the 72.2% resistance reported by Wieczorek et al31 and Gomez et al.47 While the 70% resistance to amikacin is contrary to the 100% susceptibility reported by Indrawattana et al.33 The resistance against nalidixic acid and tetracycline in this study is in accord with the reports of Maktabi et al.35
The 30% resistance to ciprofloxacin in this study is lower when compared to the 44.4% and 56% resistance reported from Nigeria.48,49 Similarly, the 30% resistance to erythromycin and trimethoprim-sulfamethoxazole reported in the current study disagrees with the 87.5%49 and 69.4%48 resistance reported previously from Nigeria. Although the resistance to trimethoprim-sulfamethoxazole (30%) and gentamicin (35%) in the present study agrees with the 24%35 and 36.1%48 resistance, it contradicts with the 87.5% trimethoprim-sulfamethoxazole and 72.2% gentamicin resistance.49 The 15% resistance to clindamycin is in line with the 12% resistance reported by Maktabi et al.35 However, 15% of cefotaxime and 25% penicillin resistance in this study is highly divergent from the 77.5% cefotaxime and 66.7% penicillin resistance reported from Ethiopia.2 The low level of resistance (5–15%) to amoxicillin, cefotaxime, vancomycin, and clindamycin in this study might be due to the absence of usage of these drugs in veterinary medicine in Ethiopia which plausibly suggests that these antimicrobials remain an alternative regimen against the organisms.2 The relatively high resistance (≥30%) observed in erythromycin, chloramphenicol, trimethoprim-sulfamethoxazole, oxacillin, tetracycline, gentamicin, and trimethoprim-sulfamethoxazole might be related to the more frequent or improper usage, particularly in the public health sectors. Nevertheless, the study warrants frequent surveillance on the change in the pattern of antibiograms for this organism.
The present MDR L. monocytogenes isolates (95%) was higher when compared to the 72.3% MDR identified from raw foods.50 In agreement with the present study, Odu and Okonko5 also reported L. monocytogenes isolates that are 100% MDR. The MDR patterns of L. monocytogenes in the study towns might be due to the non-prescribed frequent and non-judicious usage of antimicrobials in livestock and public health sectors in the study towns.2 The MDR to L. monocytogenes may occur due to plasmid or chromosomal gene transfer and mutation events in chromosomal genes from other Listeria species and Gram-positive bacteria that may be found in foods.50,51
The high rate of antimicrobial-resistant L. monocytogenes isolates towards the relatively cheaper and commonly available antimicrobials is worrisome as it might lead to the use of mandatory and more expensive drugs.2 This is a problem for listeriosis high-risk groups in developing countries like Ethiopia because the high cost of hospitalization and recent drug treatment leads to an economic burden on families and societies.
The isolation of L. monocytogenes from raw meat is a microbiological hazard for people since the consumption of raw or undercooked meat in the study areas is a widespread food habit. The present findings have also great implications for the public health in Ethiopia because of the high fatality of listeriosis, the abundance of immunocompromised people, and inadequate hygiene and awareness of the community.
The limitations of this study include the following: Firstly, due to the lack of resources and facilities, serotyping and molecular work on Listeria species have not been done. Secondly, antimicrobial susceptibility testing was performed only for L. monocytogenes. Thirdly, samples from meat handlers, equipment, and the environment were not taken to see their association. Fourthly, the questionnaire data collected from abattoir workers were not included in the logistic regression analysis due to the small number of workers (n=33) hard to compare with that of butchers and restaurants and the difficulty of linking responses of workers to a particular sample result as all workers handle the carcasses.
Conclusion
The study confirmed that contamination of raw beef sold for human consumption by Listeria species is widespread in the study area. Six Listeria species (Listeria monocytogenes, Listeria ivanovii, Listeria seeligeri, Listeria welshimeri, Listeria innocua, and Listeria grayi) were identified. The overall occurrence of Listeria species was medium while that of L. monocytogenes was low. The study towns, season, information on food hygiene and safety, and hygiene of meat cutting boards were independent predictors of Listeria species isolation. The high rate of antimicrobial resistance among L. monocytogenes isolates is of great public health importance. Amoxicillin, clindamycin, nitrofurantoin, and vancomycin might be good drugs for the treatment of L. monocytogenes infections in the study areas. Therefore, adequate heat treatment of beef before consumption, regular training for workers in the establishments, and follow-up on the prudent use of antimicrobial drugs in veterinary and public health sectors are important; and subsequently, further serological and molecular studies on Listeria species are proposed.
Data Sharing Statement
All the data supporting our findings were incorporated within the manuscript.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. All study subjects were informed about the study and written informed consents were obtained from all the owners and workers of the Ambo and Holeta town butchers, restaurants, and abattoirs. Confidentiality was assured by using codes. Ethical clearance was obtained from the Ambo University research and ethical review committee.
Acknowledgments
The authors would like to extend their appreciation to Ambo University for financially supporting the project. We thank the workers of the study establishments for their cooperation during the interview.
Author Contributions
All authors made a significant contribution to the work reported either in the conception of the study, study design, execution, acquisition of data, analysis, and interpretation or in all these areas. Moreover, all authors took part in revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Ambo University. The funder had no role in study design, data collection, and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Derra FA, Karlsmose S, Monga DP, et al. Occurrence of Listeria spp. in retail meat and dairy products in the area of Addis Ababa, Ethiopia. Foodborne Pathog Dis. 2013;10(6):577–579. doi:10.1089/fpd.2012.1361
2. Garedew L, Taddese A, Biru T, et al. Prevalence and antimicrobial susceptibility profile of Listeria species from ready-to-eat foods of animal origin in Gondar Town, Ethiopia. BMC Microbiol. 2015;15(1):100. doi:10.1186/s12866-015-0434-4
3. CHP. Scientific Committee on Enteric Infections and Foodborne Diseases. Updated Situation of Listeriosis. Center for Health Protection; 2010:1–13.
4. Mulu S, Pal M. Studies on the prevalence, risk factors, public health implications and antibiogram of Listeria monocytogenes in sheep meat collected from municipal abattoir and butcher shops in Addis Ababa. J Foodborne Zoonotic Dis. 2016;4(1):1–14.
5. Odu NN, Okonko IO. Prevalence and antibiotic susceptibility of Listeria monocytogenes in retailed meats in Port Harcourt Metropolis, Nigeria. Public Health Res. 2017;7(4):91–99. doi:10.5923/j.phr.20170704.02
6. Jalali M, Abedi D. Prevalence of Listeria species in food products in Isfahan, Iran. Int J Food Microbiol. 2008;122(3):336–340. doi:10.1016/j.ijfoodmicro.2007.11.082
7. Ramaswamy V, Cresence VM, Rejitha JS, et al. Listeria - review of epidemiology and pathogenesis. J Microbiol Immunol Infect. 2007;40(1):4–13.
8. Chiara M, Caruso M, D’Erchia AM, et al. Comparative genomics of Listeria sensu lato: genus-wide differences in evolutionary dynamics and the progressive gain of complex, potentially pathogenicity-related traits through lateral gene transfer. Genome Biol Evol. 2015;7(8):2154–2172. doi:10.1093/gbe/evv131
9. Cao X, Wang Y, Wang Y, Ye C. Isolation and characterization of Listeria monocytogenes from the black-headed gull feces in Kunming, China. J Infect Public Health. 2018;11(1):59–63. doi:10.1016/j.jiph.2017.03.003
10. Weller D, Wiedmann M, Strawn LK, Schaffner DW. Spatial and temporal factors associated with an increased prevalence of Listeria monocytogenes in spinach fields in New York state. Appl Environ Microbiol. 2015;81(17):6059–6069. doi:10.1128/AEM.01286-15
11. Fallah AA, Saei-Dehkordi SS, Rahnama M, Tahmasby H, Mahzounieh M. Prevalence and antimicrobial resistance patterns of Listeria species isolated from poultry products marketed in Iran. Food Control. 2012;28(2):327–332. doi:10.1016/j.foodcont.2012.05.014
12. Mazza R, Piras F, Ladu D, Putzolu M, Consolati SG, Mazzette R. Identification of Listeria spp. strains isolated from meat products and meat production plants by multiplex polymerase chain reaction. Ital J Food Saf. 2015;4(4):5498. doi:10.4081/ijfs.2015.5498
13. World Health Organization. Foodborne Disease Outbreaks: Guidelines for Investigation and Control. WHO Press; 2008:47–93.
14. Bhandare S, Sherikar AT, Paturkar AM, Waskar V, Zende R. A comparison of microbial contamination on sheep/goat carcasses in a modern Indian abattoir and traditional meat shops. Food Control. 2007;18(7):854–858. doi:10.1016/j.foodcont.2006.04.012
15. Du Toit L, Venter I. Food practices associated with increased risk of bacterial food-borne disease of female students in self-catering residences at the Cape Peninsula University of Technology. J Consum Res. 2005;33. doi:10.4314/jfecs.v33i1.52864
16. Al-Nabulsi AA, Osaili TM, Awad AA, Olaimat AN, Shaker RR, Holley RA. Occurrence and antibiotic susceptibility of Listeria monocytogenes isolated from raw and processed meat products in Amman, Jordan. CYTA J Food. 2015;13(3):346–352. doi:10.1080/19476337.2014.982191
17. Johnson JR, Murray AC, Gajewski A, et al. Isolation and molecular characterization of nalidixic acid-resistant extraintestinal pathogenic Escherichia coli from retail chicken products. Antimicrob Agents Chemother. 2003;47(7):2161–2168. doi:10.1128/AAC.47.7.2161-2168.2003
18. Olaimat AN, Al-Holy MA, Shahbaz HM, et al. Emergence of antibiotic resistance in Listeria monocytogenes isolated from food products: a comprehensive review. Compr Rev Food Sci. 2018;17(5):1277–1292. doi:10.1111/1541-4337.12387
19. Molla B, Yilma R, Alemayehu D. Listeria monocytogenes and other Listeria species in retail meat and milk products in Addis Ababa, Ethiopia. Ethiop J Health Dev. 2004;18(3):208–212. doi:10.4314/ejhd.v18i3.9962
20. Gebretsadik S, Kassa T, Alemayehu H, Huruy K, Kebede N. Isolation and characterization of Listeria monocytogenes and other Listeria species in foods of animal origin in Addis Ababa, Ethiopia. J Infect Public Health. 2011;4(1):22–29. doi:10.1016/j.jiph.2010.10.002
21. CSA. Population and Housing Census of Ethiopia. Addis Ababa, Ethiopia; 2007.
22. Thrusfield M. Describing Disease Occurrence. Veterinary Epidemiology.
23. ISO. Microbiology of Food and Animal Feeding Stuffs Horizontal Method for the Detection and Enumeration of Listeria Monocytogenes, Part 1: Detection Method. Geneva, Switzerland; 2004.
24. CLSI. Performance standards for antimicrobial susceptibility testing; fifteenth informational supplement, M100_S15. Vol. 25. 2005.
25. Destro MT, de Melo Serrano A, Kabuki DY. Isolation of Listeria species from some Brazilian meat and dairy products. Food Control. 1991;2(2):110–112. doi:10.1016/0956-7135(91)90147-O
26. Arslan S, Baytur S. Prevalence and antimicrobial resistance of Listeria species and subtyping and virulence factors of Listeria monocytogenes from retail meat. J Food Saf. 2019;39(1):e12578. doi:10.1111/jfs.12578
27. Yücel N, Çıtak S, Önder M. Prevalence and antibiotic resistance of Listeria species in meat products in Ankara, Turkey. Food Microbiol. 2005;22(2):241–245. doi:10.1016/j.fm.2004.03.007
28. Oyelami L, Aboaba O, Banjo OA. Prevalence and antibiotics susceptibility profile of Listeria monocytogenes isolated from processed and unprocessed meat products. Fulafia J Sci Technol. 2018.
29. Osaili TM, Alaboudi AR, Nesiar EA. Prevalence of Listeria spp. and antibiotic susceptibility of Listeria monocytogenes isolated from raw chicken and ready-to-eat chicken products in Jordan. Food Control. 2011;22(3):586–590. doi:10.1016/j.foodcont.2010.10.008
30. Eruteya O, Odunfa S, Lahor J. Listeria spp. in raw cow and goat meat in port harcourt, Nigeria. Br Biotechnol J. 2014;4(2):204–214. doi:10.9734/BBJ/2014/6750
31. Wieczorek K, Dmowska K, Osek J. Prevalence, characterization, and antimicrobial resistance of Listeria monocytogenes isolates from bovine hides and carcasses. Appl Environ Microbiol. 2012;78(6):2043–2045. doi:10.1128/AEM.07156-11
32. Gudbjörnsdóttir B, Suihko ML, Gustavsson P, et al. The incidence of Listeria monocytogenes in meat, poultry and seafood plants in the Nordic countries. Food Microbiol. 2004;21(2):217–225. doi:10.1016/S0740-0020(03)00012-1
33. Indrawattana N, Nibaddhasobon T, Sookrung N, et al. Prevalence of Listeria monocytogenes in raw meats marketed in Bangkok and characterization of the isolates by phenotypic and molecular methods. J Health Popul Nutr. 2011;29(1):26–38. doi:10.3329/jhpn.v29i1.7565
34. Marian M, Aminah SS, Zuraini M, et al. MPN-PCR detection and antimicrobial resistance of Listeria monocytogenes isolated from raw and ready-to-eat foods in Malaysia. Food Control. 2012;28(2):309–314. doi:10.1016/j.foodcont.2012.05.030
35. Maktabi S, Pourmehdi M, Zarei M, Fooladgar AA. Detection of antibiotic resistant Listeria spp. in beef burgers distributed in Ahvaz City, Iran. Jundishapur J Health Sci. 2016;8(2). doi:10.17795/jjhs-34780
36. Vitas A, Garcia-Jalon VAEI. Occurrence of Listeria monocytogenes in fresh and processed foods in Navarra (Spain). Int J Food Microbiol. 2004;90(3):349–356. doi:10.1016/s0168-1605(03)00314-3
37. Alsheikh A, Mohammed G, Abdalla M. First isolation and identification of Listeria monocytogenes from fresh raw dressed broiler chicken in Sudan. Res J Microbiol. 2012;7(6):319–326. doi:10.3923/jm.2012.319.326
38. Awaisheh S. Incidence and contamination level of Listeria monocytogenes and other Listeria spp. in ready-to-eat meat products in Jordan. J Food Prot. 2010;73(3):535–540. doi:10.1111/jfs.12578
39. Fisseha S. The occurrence of Listeria monocytogenes in ready-to-eat foods of animal origin and its antibiotic susceptibility profile, Bishoftu and Dukem Towns, Central Ethiopia. World J Adv Healthc Res. 2017;1(2):47–62.
40. Fenlon D, Wilson J, Donachie W. The incidence and level of Listeria monocytogenes contamination of food sources at primary production and initial processing. J Appl Bacteriol. 1996;81(6):641–650. doi:10.1111/j.1365-2672.1996.tb03559.x
41. Gibbons I-S, Adesiyun A, Seepersadsingh N, Rahaman S. Investigation for possible source (s) of contamination of ready-to-eat meat products with Listeria spp. and other pathogens in a meat processing plant in Trinidad. Food Microbiol. 2006;23(4):359–366. doi:10.1016/j.fm.2005.05.008
42. Eslami G, Samadi R, Taherpanah R, Taherpor A, Baseri N. Detection of actA and InlB genes in Listeria monocytogenes isolated from women with spontaneous abortions. Novel Biomed. 2014;2(1):18–21.
43. Sörqvist S. Heat resistance of different serovars of Listeria monocytogenes. J Appl Bacteriol. 1994;76(4):383–388. doi:10.1111/j.1365-2672.1994.tb01644.x
44. Hori K, Matsumoto S. Bacterial adhesion: from mechanism to control. Biochem Eng J. 2010;48(3):424–434. doi:10.1016/j.bej.2009.11.014
45. Jianu C, Chiş C. Study on the hygiene knowledge of food handlers working in small and medium-sized companies in western Romania. Food Control. 2012;26(1):151–156. doi:10.1016/j.foodcont.2012.01.023
46. Ismaïl R, Aviat F, Michel V, et al. Methods for recovering microorganisms from solid surfaces used in the food industry: a review of the literature. Int J Environ Res Public Health. 2013;10(11):6169–6183. doi:10.3390/ijerph10116169
47. Gomez D, Azon E, Marco N, et al. Antimicrobial resistance of Listeria monocytogenes and Listeria innocua from meat products and meat-processing environment. Food Microbiol. 2014;42:61–65. doi:10.1016/j.fm.2014.02.017
48. Usman U, Kwaga J, Kabir J, Olonitola O. Isolation and antimicrobial susceptability of Listeria monocytogenes from raw milk and milk products in Northern Kaduna State, Nigeria. J Appl Environ Microbiol. 2016;4(3):46–54. doi:10.12691/JAEM-4-3-1
49. Ishola OO, Mosugu JI, Adesokan HK. Prevalence and antibiotic susceptibility profiles of Listeria monocytogenes contamination of chicken flocks and meat in Oyo State, south-western Nigeria: public health implications. J Prev Med Hyg. 2016;57(3):E157–E163.
50. Wang G, Qian W, Zhang X, et al. Prevalence, genetic diversity and antimicrobial resistance of Listeria monocytogenes isolated from ready-to-eat meat products in Nanjing, China. Food Control. 2015;50:202–208. doi:10.1016/j.foodcont.2014.07.057
51. Harakeh S, Saleh I, Zouhairi O, Baydoun E, Barbour E, Alwan N. Antimicrobial resistance of Listeria monocytogenes isolated from dairy-based food products. Sci Total Environ. 2009;407(13):4022–4027. doi:10.1016/j.scitotenv.2009.04.010
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.