Back to Journals » Infection and Drug Resistance » Volume 15
Listeria Monocytogenes Meningitis in an Immunocompetent Patient
Authors Magiar O, Vulpie S, Musuroi C, Marincu I ![]() , Murariu A, Turaiche M, Musuroi SI, Muntean D, Licker M
, Murariu A, Turaiche M, Musuroi SI, Muntean D, Licker M ![]()
Received 5 December 2021
Accepted for publication 28 January 2022
Published 10 March 2022 Volume 2022:15 Pages 989—994
DOI https://doi.org/10.2147/IDR.S351132
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Oana Magiar,1 Silvana Vulpie,1,2 Corina Musuroi,1,3 Iosif Marincu,4,5 Alina Murariu,6 Mirela Turaiche,4,5 Silvia Ioana Musuroi,7 Delia Muntean,1,3,8 Monica Licker1,3,8
1Clinical Laboratory, “Pius Brînzeu” County Clinical Emergency Hospital Timisoara, Timis, Romania; 2Doctoral School, “Victor Babeș” University of Medicine and Pharmacy Timisoara, Timis, Romania; 3Microbiology Department, “Victor Babeș” University of Medicine and Pharmacy Timisoara, Timis, Romania; 4”Victor Babeș” Clinical Hospital of Infectious Diseases, Methodological and Infectious Diseases Research Centre Timisoara, Timis, Romania; 5Infectious Diseases Department, “Victor Babeș” University of Medicine and Pharmacy Timisoara, Timis, Romania; 6Neurology II Department, “Pius Brînzeu” County Clinical Emergency Hospital Timisoara, Timis, Romania; 7Internal Medicine Department, Clinical Emergency Municipal Hospital, Timisoara, Romania; 8Multidisciplinary Research Centre for Antibiotic Resistance, “Victor Babeș” University of Medicine and Pharmacy Timisoara, Timis, Romania
Correspondence: Silvana Vulpie, Clinical Laboratory, “Pius Brînzeu” County Clinical Emergency Hospital Timisoara, Liviu Rebreanu, No. 156, Timișoara, Timis, 300723, Romania, Tel +40 727248701, Email [email protected]
Abstract: Listeria monocytogenes (LM), one of the most important foodborne pathogens, is an intracellular bacterium found in food and the environment. It causes listeriosis, a potentially severe disease, particularly for pregnant women, the elderly and immunocompromised patients, but in rare cases, it can cause invasive disease in immunocompetent adults and children. Community-acquired bacterial meningitis caused by LM is rare and difficult to diagnose. It carries a high mortality rate; therefore, it is essential to start appropriate antibiotic treatment as soon as possible. The first case of LM meningitis identified in our hospital over the last 10 years is that of a previously healthy 45-year-old man who presented in the emergency department with a 4-day history of diplopia, left eye medial deviation and left palpebral ptosis, with no history of fever, headache or gastrointestinal symptoms. Because of the atypical symptoms, a suspicion of meningitis vs cerebral aneurysm was raised during the admission process. The patient was diagnosed with LM meningitis and recovered fully after appropriate antibiotic treatment. The purpose of this article is to emphasise the possibility of LM invasive disease (in this case meningitis) occurring in previously healthy individuals and to raise awareness about the need for LM to be considered in the differential diagnosis of atypical presentations.
Keywords: Listeria monocytogenes, meningitis, antibiotics, atypical clinical manifestation, immunocompetent patient
Introduction
Listeria monocytogenes (LM), the main species of the Listeria genus, is a Gram-positive facultative anaerobic intracellular bacterium widely distributed in the environment, which has the ability to grow at refrigeration temperatures (at 4°C). It is generally transmitted to humans through ingestion of contaminated food (ready-to-eat food, deli meats and soft cheeses). The primary bacteraemia, after ingestion, is followed by dissemination in the central nervous system (CNS), endocardium and for pregnant women, invasion of the placenta and foetus.1 It principally affects specific groups of patients: pregnant women, neonates, the immunocompromised (especially if cell-mediated immunity is impaired), and the elderly, potentially causing life-threatening infections such as bacteriaemia and meningoencephalitis. However, there are also case reports of Listeria infections in previously healthy and immunocompetent patients, which may be associated with severe complications and a high mortality rate (for meningitis, 20–50%).2,3 This report presents a case of LM meningitis in an immunocompetent adult without significant past medical history or specific risk factors (the first case identified in our hospital in the last 10 years), discussing the atypical presentation, the diagnostic challenges encountered, the treatment challenges and the final outcome.
Case Presentation
We want to look at the case of a 45-year-old man with no significant past medical history or treatment, a train operator living in an urban area, who attended the Emergency Department (ED) of “Pius Branzeu” County Clinical Emergency Hospital Timisoara being sent by his General Practitioner (GP) with a 4-day history of diplopia, left eye medial deviation and left palpebral ptosis. He also reported an episode of severe frontal headache (10/10 in severity) that ceased 3 days prior to his admission, with no history of fever, diarrhoea, vomiting or other signs or symptoms. On examination, the patient presented normal vital signs, including normal blood pressure, heart rate, oxygen saturation and temperature. The cardiorespiratory and abdominal examinations were also normal. The neurological examination showed an alert and orientated patient with divergent strabismus and left palpebral ptosis, no signs of meningeal irritation and no other neurological findings. Blood tests on admission showed an elevated white cell count (WCC) (15.48 ×109/L) and severe hyponatremia (Na = 128 mmol/L). The computed tomography (CT) of the brain performed showed no acute findings. Considering that the patient presented at the ED during the Covid-19 pandemic, the initial assessment included a SARS-CoV-2 Polymerase Chain Reaction test (PCR) and a CT thorax to rule out a possible Covid-19 infection. The SARS-CoV-2 PCR test being negative and the CT thorax showing no acute findings, the patient was admitted onto the Neurology II ward for further investigation and appropriate treatment.
Because of the lack of any significant improvement in his clinical status, on day 2 of his admission, a suspicion of cerebral aneurysm was raised and the patient underwent a brain Magnetic Resonance Angiography (MRA). The images showed no aneurysm but a few small demyelinating lesions localised in the periventricular white matter of the frontoparietal lobes, bilaterally and in the right cerebellar peduncles, which could not be correlated with the neurological findings. Blood tests were performed regularly during admission (see Table 1).
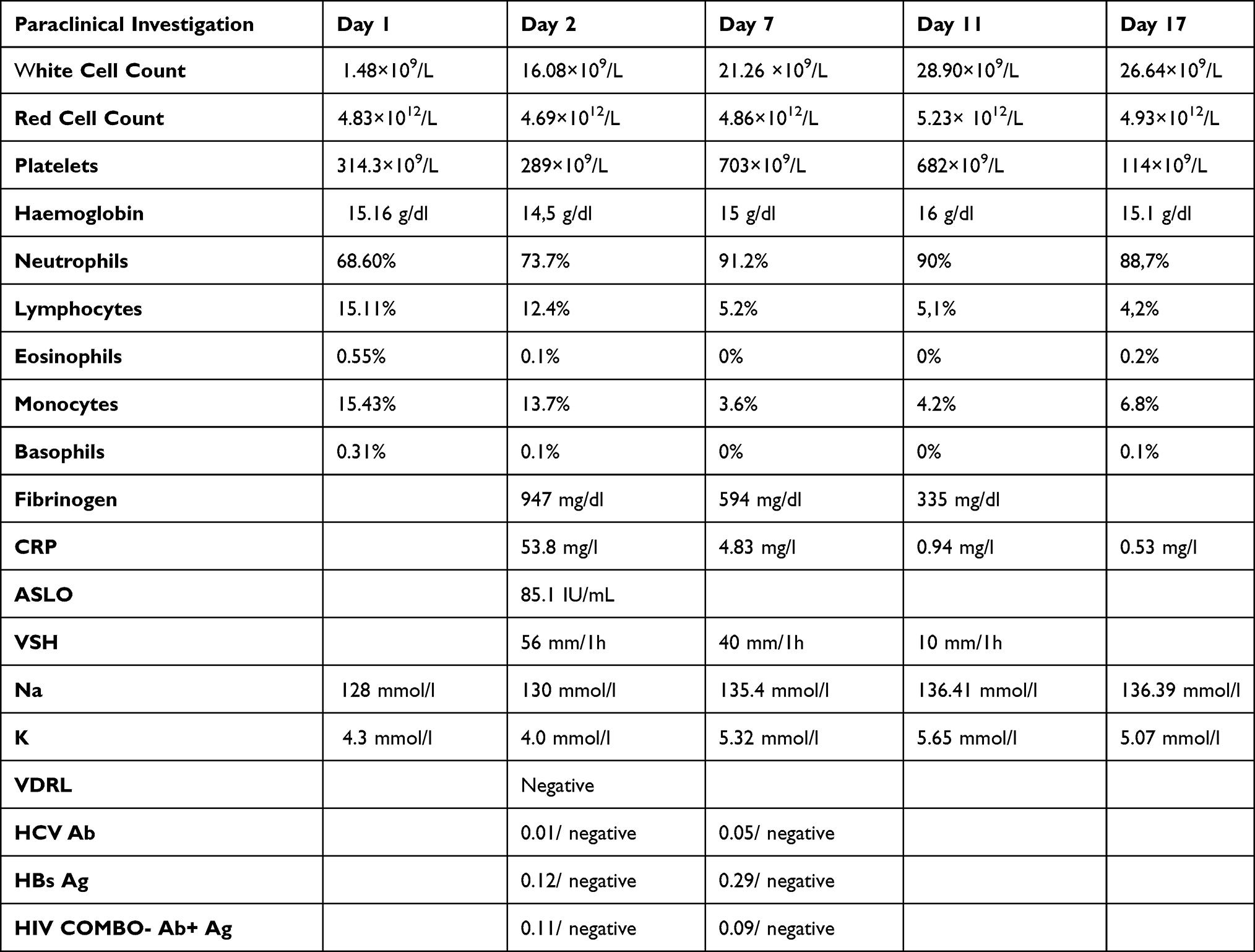 |
Table 1 Blood Investigation Results |
On day 3, the patient developed generalised tremor (on movement) and diaphoresis. As a result of the worsening of his clinical status, a lumbar puncture (LP) was performed and the cerebrospinal fluid (CSF) was sent to the Laboratory for microbiological and biochemical investigations (see Table 2). The CSF sample was inoculated on agar plates (Certifikat Croatia UTI Agar, Certifikat Croatia Blood Agar) and broth (Certifikat Croatia Nutrient Broth) and incubated for 18–24 hours at 35–37°C with ~5% CO2.
 |
Table 2 CSF Results |
Following the preliminary LP results, a diagnosis of bacterial meningitis was suspected and empirical antimicrobial therapy was initiated with ceftriaxone 2g/12h and linezolid 600mg/12h. (Vancomycin was initially prescribed, but due to a shortage in the Hospital’s Pharmacy, linezolid was given instead).4 The patient was also prescribed dexamethasone 8mg/12h. A referral to the Infectious Diseases (ID) team was made requesting a review. After evaluating the patient, the ID team recommended CSF culture, immunology screening (see Table 1) and antibiotic treatment as prescribed. By the end of day 3 of his admission and after receiving the first doses of the above-mentioned therapy, the neurological signs and symptoms improved, and the patient reported the resolution of diplopia.
On day 4, the patient was transferred to “Victor Babes” Infectious Diseases Hospital Timisoara for further management.
The CSF culture results confirmed the diagnosis of Listeria bacterial meningitis. LM was identified using Matrix-Assisted Laser Desorption/Ionisation-Time of Flight (MALDI-TOF) mass spectrometry and VITEK 2 Compact System. For antimicrobial susceptibility testing, disc diffusion method was used (according to the European Committee on Antimicrobial Susceptibility Testing guidelines (EUCAST): 5% sheep blood Mueller–Hinton agar, incubation at 35±1°C for 24 hours, in CO2 atmosphere),5 which showed that the strain was susceptible to amoxicillin-clavulanic acid, ampicillin, erythromycin, linezolid, tetracycline and vancomycin and resistant to clindamycin. (Oxoid™ antimicrobial susceptibility discs and Etest® strip for vancomycin).
The Neurology team and, because by that time the patient had already been transferred, the Infectious Disease team were both informed, and the antibiotic therapy was continued with ampicillin 2g/6h and vancomycin 1g/12h. The Clinical status improved with complete recovery and the patient was discharged on day 21 with the recommendation to continue the antibiotic treatment with oral ampicillin 500mg/12h for seven more days.
The patient was reviewed by the Infectious Disease team in their Outpatient Department 10 days after discharge, finding that he has made a full recovery.
To the best of authors’ knowledge this was an isolated case, not being linked to any outbreaks of listeriosis. The patient did not present an occupational risk, and the dietary history was of no significance for Listeria infection.
This case report was approved by the Ethics Committee of “Pius Brînzeu” County Clinical Emergency Hospital Timisoara, no 241/11.05.2021. Written informed consent, including consent to publish, was obtained from the patient.
Discussions and Conclusion
LM is the third most common cause of bacterial meningitis in adults.4 Typically, patients with LM from the susceptible groups present with signs and symptoms similar to those of meningoencephalitis from other causes: fever, headache, neck stiffness, altered mental status and neurological deficits. Case reports of LM meningitis in healthy individuals occur very rarely. They may atypically present with general “flu-like” illness (fever, diarrhoea, headaches, nausea, vomiting, myalgias) or may be completely asymptomatic.3
This case concerns meningitis in a patient with an atypical presentation, having mainly neurological signs and symptoms that initially led to a suspicion of organic brain lesion, without specific symptoms to support a diagnosis of bacterial meningitis. Ruling out the cerebrovascular pathology by imaging (MRA) guided the diagnosis toward an infectious cause.
The current empirical antibiotic treatment guidelines for community-acquired bacterial meningitis4 does not cover the treatment for LM in immunocompetent patients between 18 and 50 years of age, therefore the appropriate antibiotic treatment for LM meningitis in this case was delayed.
In one study regarding the traits of LM in Romania, Caplan et al showed that a high percentage of young immunocompetent patients without any predisposing conditions were diagnosed with listeriosis, when compared with other European countries, most likely secondary to food products contaminated with high loads of LM.6
This could suggest that LM should be considered in the differential diagnosis of patients presenting with atypical neurological symptoms or those that do not improve on the classical treatment, regardless of age group or past medical history, especially in countries with a higher risk of infection with LM. Furthermore, LM should not be suspected only in immunocompromised patients, as this was reported in 20% of the patients with no specific risk factors. There are only few cases of invasive listeriosis in previously healthy individuals described in the literature. An interesting case of severe LM rhombencephalitis is described by Cao et al, equivalent to our case. The symptomatology was atypical, and the patient presented with only neurological signs on admission.7 Jamal et al presented another interesting case of LM meningitis in an immunocompetent adult with no past medical history and without occupational exposure. Similar to our case, the source of infection could not be determined.8 Another case of meningitis caused by LM in a previously healthy patient is described by Brebenariu et al. In this case, the source of infection was occupational exposure.9 Furthermore, Tiri et al in their case review presented an interesting case of LM brain abscess in an immunocompetent adult patient.10
The treatment of choice for bacterial meningitis caused by LM remains amoxicillin, ampicillin or penicillin G, according to the most recent European Society of Clinical Microbiology and Infectious Diseases (ESCMID) guidelines. Some studies found other antibiotics, such as vancomycin, linezolid, quinolones, gentamycin, meropenem, and chloramphenicol, to also be effective against Listeria species in vitro. However, the clinical data were insufficient to make strong recommendations for any of these agents in Listeria meningitis.4
Jean-Damien Ricard et al did a prospective multicentre observational study showing that the efficient concentration of vancomycin in cerebrospinal fluid can be achieved even when dexamethasone is given simultaneously.11 In another prospective study, Shervin Shokouhi et al concluded that the concentration of vancomycin in CSF does not decrease with the relief of the meningeal inflammation12 and a systematic review by Jessica E Beach et al shows that despite the hydrophilic character and the high molecular weight, vancomycin levels in the CSF were variable.13
The use of linezolid together with dexamethasone is discussed in a previous case report by Yilmaz et al.14 In another study, Tsona et al showed that linezolid has a good penetration into CSF and brain tissue, making it an option to consider in the treatment of bacterial meningitis.15 In our case, the patient’s neurological symptoms improved while he was on linezolid, and we consider this case report an opportunity to contribute to the literature regarding the use of linezolid in Listeria bacterial meningitis.
The patient also received dexamethasone in the first few days of his admission as part of the empirical treatment given for bacterial meningitis. The use of dexamethasone for patients diagnosed with bacterial meningitis is controversial. The meta-analysis by Brouwer et al supports the adjunctive dexamethasone treatment to prevent an inflammatory response, decreasing overall hearing loss and neurologic sequelae, but with no effect on the overall mortality.16 In another systematic review, van de Beek et al concluded that treatment with steroids was associated with a significant reduction in mortality and neurological sequelae.17 Conversely, other studies had no findings to support the benefits of dexamethasone.18
In the literature, there are studies reporting hyponatremia as a common finding in patients diagnosed with bacterial meningitis, especially when caused by LM. In this case, the patient presented with severe hyponatremia of 128 mmol/l, which improved to 133 mmol/l along with the patient’s symptoms, by day 3 of admission, with only gentle intravenous (iv) fluid therapy.19
We presented this case to raise awareness about LM as a possible cause for bacterial meningitis in immunocompetent patients with uncharacteristic clinical symptoms and to confirm that linezolid is a viable treatment option for patients with LM meningitis leading to favourable outcomes.
Acknowledgements
The Authors would like to express their gratitude for the financial support in publishing this paper, provided by “Victor Babes” University of Medicine and Pharmacy Timisoara, Romania.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Buiuc D, Neguţ M. Tratat de Microbiologie Clinică [Manual of Clinical Microbiology].
2. Torok E, Moran E, Cooke F. Oxford Handbook of Infectious Diseases and Microbiology.
3. Murray PR, Rosenthal KS, Pfaller MA. Medical Microbiology.
4. van de Beek D, Cabellos C, Dzupova O, et al. ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin Microbiol Infect. 2016;22:S37–S62.
5. EUCAST disk diffusion method for antimicrobial susceptibility testing Reading guide. Version 9.0 (January 2021). Available from: https://www.eucast.org/ast_of_bacteria/disk_diffusion_methodology/.
6. Caplan M, Pietzka A, Popescu G, et al. Characterization of Romanian Listeria monocytogenes isolates from food and humans. Romanian Biotechnol Lett. 2014;19(3):9319–9329.
7. Cao L, Lin Y, Jiang H, Wei J. Severe invasive Listeria monocytogenes rhombencephalitis mimicking facial neuritis in a healthy middle-aged man: a case report and literature review. J Int Med Res. 2021;49(1):1837.
8. Jamal WY, Al-Shomari S, Boland F, Rotimi VO. Listeria monocytogenes meningitis in an immunocompetent adult patient. Medical Principles Pract. 2005;14(1):765.
9. Brebenariu M, Hogea E, Gheorghiu E, et al. Listeria monocytogenes meningitis. Case report of a patient with occupational exposure. Romanian Biotechnol Lett. 2016;21(3):12.
10. Tiri B, Priante G, Saraca LM, Martella LA, Cappanera S, Francisci D. Listeria monocytogenes Brain Abscess: controversial Issues for the Treatment—Two Cases and Literature Review. Case Rep Infect Dis. 2018;2018:1–9. doi:10.1155/2018/6549496
11. Ricard JD, Wolff M, Lacherade JC, et al. Levels of vancomycin in cerebrospinal fluid of adult patients receiving adjunctive corticosteroids to treat pneumococcal meningitis: a prospective multicenter observational study. Clin Infect Dis. 2007;44(2):250.
12. Shokouhi S, Alavi Darazam I. Determination of vancomycin trough level in serum and cerebrospinal fluid of patients with acute community-acquired meningitis: a prospective study. J Infection. 2014;69(5):424.
13. Beach JE, Perrott J, Turgeon RD, Ensom MHH. Penetration of vancomycin into the cerebrospinal fluid: a systematic review. Clin Pharmacokinet. 2017;56(12):1479.
14. Yılmaz P, Mutlu NM, Sertçelik A, Baştuğ A, Doğu C, Kışlak S. Linezolid and dexamethasone experience in a serious case of listeria rhombencephalitis. J Infect Public Health. 2016;9(5):670–674.
15. Tsona A, Metallidis S, Foroglou N, et al. Linezolid penetration into cerebrospinal fluid and brain tissue. J Chemother. 2010;22(1):17.
16. Brouwer MC, Mcintyre P, Prasad K. Corticosteroids for acute bacterial meningitis. Cochrane Database Sys Rev. 2013;2013(6):12.
17. van de Beek D, de Gans J, McIntyre P, Prasad K. Steroids in adults with acute bacterial meningitis: a systematic review. Lancet Infect Dis. 2004;4(3):139.
18. van de Beek D, Farrar JJ, de Gans J, et al. Adjunctive dexamethasone in bacterial meningitis: a meta-analysis of individual patient data. Lancet Neurol. 2010;9(3):254.
19. Brouwer MC, van de Beek D, Heckenberg SGB, Spanjaard L, de Gans J. Hyponatraemia in adults with community-acquired bacterial meningitis. QJM. 2007;100(1):765.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.